")
Back to Journals » Clinical Interventions in Aging » Volume 13
Functionality and Outcome in Older Patients with Severe Aortic Stenosis (FOOPAS): an interdisciplinary study concept for a prospective trial
Authors Vogt F , Wicklein S, Gosch M, Jessl J, Hitzl W, Fischlein T, Pauschinger M, Pfeiffer S, Eckner D
Received 16 October 2017
Accepted for publication 6 December 2017
Published 1 February 2018 Volume 2018:13 Pages 185—193
DOI https://doi.org/10.2147/CIA.S154234
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Ferdinand Vogt,1 Susanne Wicklein,2 Markus Gosch,2 Jürgen Jessl,3 Wolfgang Hitzl,4 Theodor Fischlein,1 Matthias Pauschinger,3 Steffen Pfeiffer,1 Dennis Eckner3
1Department of Cardiac Surgery, Paracelsus Medical University, Nuremberg, Germany; 2Department of Geriatric Medicine, Paracelsus Medical University, Nuremberg, Germany; 3Department of Cardiology, Paracelsus Medical University, Nuremberg, Germany; 4Research Office – Biostatistics, Paracelsus Medical University, Salzburg, Austria
Background: Frailty is a geriatric syndrome that can influence mortality and functional recovery after treatment of severe aortic stenosis (AS). The integration of standardized geriatric assessment (GA) in clinical practice is limited by a lack of consensus on how to measure it.
Objectives: This study aims to compare the incremental predictive value of different frailty scales to predict the outcomes following surgical aortic valve replacement, transcatheter aortic valve implantation, and conservative treatment of severe AS.
Methods: A prospective cohort of 300 older adults with severe AS will be assembled after standard clinical examinations and a comprehensive GA, including 18 different tests and values. Primary outcome parameters are overall mortality, cardiovascular mortality, quality of life, and functionality. Secondary parameters are overall complications, cardiovascular complications, and costs.
Results: Expected results will contribute to the growing body of evidence on frailty based on parameters that influence clinical and functional outcome in elderly patients independent of the method of treatment. The pre-procedural assessment is expected to be valuable in discriminating new post-procedural complications from simple exacerbations of pre-existing conditions. Therefore, a new frailty test which is simple and feasible for application in a clinical routine by most medical professionals, may help in identifying patients for whom further GA should be considered. Finally, such a frailty score could support heart teams to find the right treatment for patients suffering from AS.
Conclusion: Comparison of different frailty scales has not only the goal of finding a predictive value of mortality but also to bring in a meaningful improvement for each individual patient and to avoid disability or fatal outcomes.
Keywords: frailty, aortic valve, geriatric assessment, transcatheter aortic valve implantation, TAVI, aortic valve replacement, AVR
Introduction
Demographic changes have resulted in an increase in the number of old and very old patients in need of heart surgery or invasive cardiological intervention. From 1992 to 2008, the proportion of patients aged >80 years undergoing cardiac surgery in Germany rose from 2.3% to 10.8%. In the 70–80 years age group, it increased from 22.8% to 38.3%.1 In the past 6 years, this development has accelerated. The most frequent indication in this group represents aortic stenosis (AS). Surgical aortic valve replacement (SAVR) has been the gold standard treatment for decades. Transcatheter aortic valve implantation (TAVI) has been established as an alternative treatment option, especially for inoperable patients and in high-risk patients with severe AS.
Both cardiac surgery and TAVIs result in a good outcome among older patients in terms of mortality,2,3 whereas conservative management is limited to symptomatic treatment and results in significantly worse outcome.4 Therefore, conservative treatment is not an option that can replace a surgical or interventional procedure.
Studies on aortic valve replacement in elderly patients showed excellent results, especially with regard to higher mortality. These results contrast with the clinical experience, particularly if mortality is not the only outcome parameter. The decision on the method of aortic valve repair is mainly based on cardiological parameters and the empirical rating, and does not include a standardized assessment with regard to the functional status of a patient. The ‘frailty’ of a patient as an additional criterion was an ‘eyeballing’ of the patient to quantify frailty on a subjective basis by the surgeon or interventionalist. Per se frailty is conceptually defined as a diminished capability to recover from pathological or iatrogenic stressors due to age-related impairments.5 Frailty is a geriatric syndrome influencing potential functional recovery after a TAVI or SAVR procedure.6,7 Although the likelihood of short-term procedural success exceeds 95%,8 2 of 5 patients in the PARTNER I (Placement of AoRTic TraNscathetER Valve Trial) and CoreValve Pivotal trials experienced poor health-related quality of life or death over the ensuing year.9 To optimize patient selection for a certain treatment of aortic valve stenosis, national guidelines strongly recommend an objective evaluation of frailty.
A standardized integration such as geriatric assessment (GA) has been limited by a lack of consensus on how to measure it and has not yet been implemented in clinical practice. According to the GA, the functional status should be assessed by using validated tests regardless of the diagnosis. In other clinical settings, such as orthogeriatric care, different GA tools have proven capable of predicting the clinical outcome.10–12 With regard to cardiac diseases, evidence exists that GA tools can predict the outcome of older patients.13–16 Therefore, GA could be of value in providing an appropriate indication and choice of treatment approach.
The indication for an intervention is currently based on age, cardiological parameters, comorbidities, and the empirical rating of the heart team. Given the surprisingly good outcome of old patients after aortic valve replacement or intervention, we think that many older patients with severe AS are likely to benefit from intervention. To get a closer insight, there is a strong need for data related to indication and the functional status of patients prior to treatment.
Objectives
GA tests have no predictive value as far as outcome in older patients with severe AS are concerned. The aim of this study is to assess functional disabilities of patients aged ≥75 years with severe AS and to search for a predictive value related to outcome. Our primary questions are:
- What is the impact of the functional status on the indication of aortic valve intervention in older patients with severe AS?
- Which assessment tools reveal the highest predictive value?
- Is there a correlation between assessment tools and the empirical judgment of the heart team?
- Is there an option to get a new geriatric score with a high predictive value for older patients?
- Could the implementation of a GA lead to a change from an empirical decision-making process to a standardized approach, resulting in an improvement of the outcome in older patients with severe AS?
Primary outcome parameters are overall mortality, cardiovascular mortality, quality of life, and functionality. Secondary parameters are overall complications such as myocardial infarction, stroke and transient ischemic attack, bleeding complications, acute renal failure, vascular complications, as well as conduction disturbances and arrhythmias following the Valve Academic Research Consortium-2 consensus document criteria.17 New onset conduction disorders such as bundle-branch blocks and arrhythmias, which are known predictors of cardiovascular mortality, will also be evaluated.18 In addition, a cost analysis will also be carried out.
Methods
Study design
The study is a prospective longitudinal case–control study over 12 months. The recruitment of the patients is based on an “all comers”-principle. We expect 2 patients per week in each study group to allow for completion of recruitment within 1 year. The project will run for over 24 months. The additional geriatric evaluation does not include any invasive examination and should improve the quality of care for these patients. Regardless of their treatment approach, all patients will be seen by a geriatrician. The study design will not change the current best clinical practice and has no impact on clinical decisions and indications. Therefore, no negative effects for the patients should be expected. All patients or their legal representatives will provide written informed consent to participate in this study. The ethical approval was given by the Bavarian Medical Association (Bayerische Landesärztekammer-BLAEK, Munich, Germany).
Setting
The interdisciplinarity of the 3 participating university clinics within the Paracelsus Medical University at the Nuremberg General Hospital is working on a daily routine: the geriatric department is the oldest one in Germany and has a history of more than 40 years. The department includes 96 beds for acute geriatric care and a day clinic with 45 places. In 2015, the team cared for 3,225 in-hospital patients, including 40 with severe AS cases. The department of cardiac surgery was implemented 22 years ago. It includes 39 beds, 7 for intermediate and 10 for intensive care. In 2015, 1,046 surgeries were performed. The department of cardiology has a history of more than 30 years. The department includes 113 beds and its own intensive care unit with 36 beds. It provides heart catheters on demand in a 24-hour setup as well as all non-invasive and invasive cardiological procedures. Cardiological examinations are available in both locations, the southern and the northern clinics. Each year, the department cares for about 7,000 in-hospital patients; furthermore, the cardiologists are consultants for all other departments. Together with the cardiologists, the cardiac surgeons are members of the heart team. Since 2009, more than 800 patients have received a TAVI (transfemoral or transapical). In 2016, 156 patients were treated within the heart team (120 underwent a transfemoral procedure, and 36 a transapical one).
Inclusion criteria
Patients with severe AS, aged ≥75 years. Agreement of the patient or their legal representative.
Exclusion criteria
- Missing patient consent
- Combined aortic valve disease
- History of heart surgery
- Acute coronary syndrome within 4 weeks
- Limited life expectancy of ~12 months
Study plan
The study has no impact on routine diagnostic examinations or clinical decision-making. After a decision has been made and further treatment determined, the patient will be informed about the study. Assuming the patient has given his/her consent and all inclusion and exclusion criteria are met, he/she will be included in the study. Regardless of the therapeutic approach, all patients will receive a complex GA and a consultation with a geriatrician with special individual recommendations (eg, adaptation of medication, recommendation for nutrition, and prevention of falls). The results of the GA will have no impact on the treatment decision made by the heart team. Cardiological parameters will be assessed by the heart team following routine clinical standards and complemented by the parameters of the PARTNER 2 trial (Transcatheter or Surgical Aortic-Valve Replacement in Intermediate Risk Patients).19 Table 1 shows an overview of these as well as all geriatric parameters and assessment tests. After the decision of the heart team based on risk stratification and clinical evaluations, the patients will be assigned to undergo SAVR, TAVI, or conservative optimized medical treatment. Further assessments will be planned before discharge (day 3–5) and follow-ups in 3 and 12 months (Figure 1).
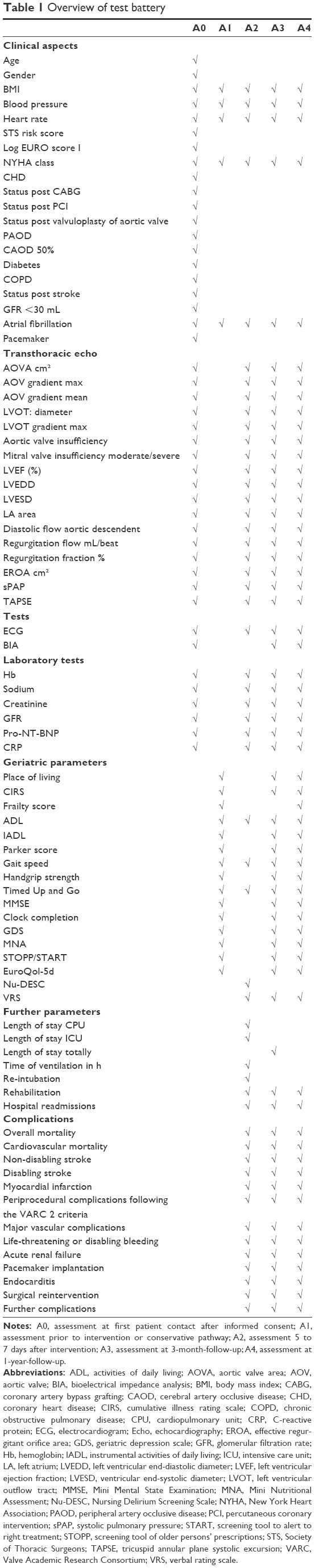 | Table 1 Overview of test battery |
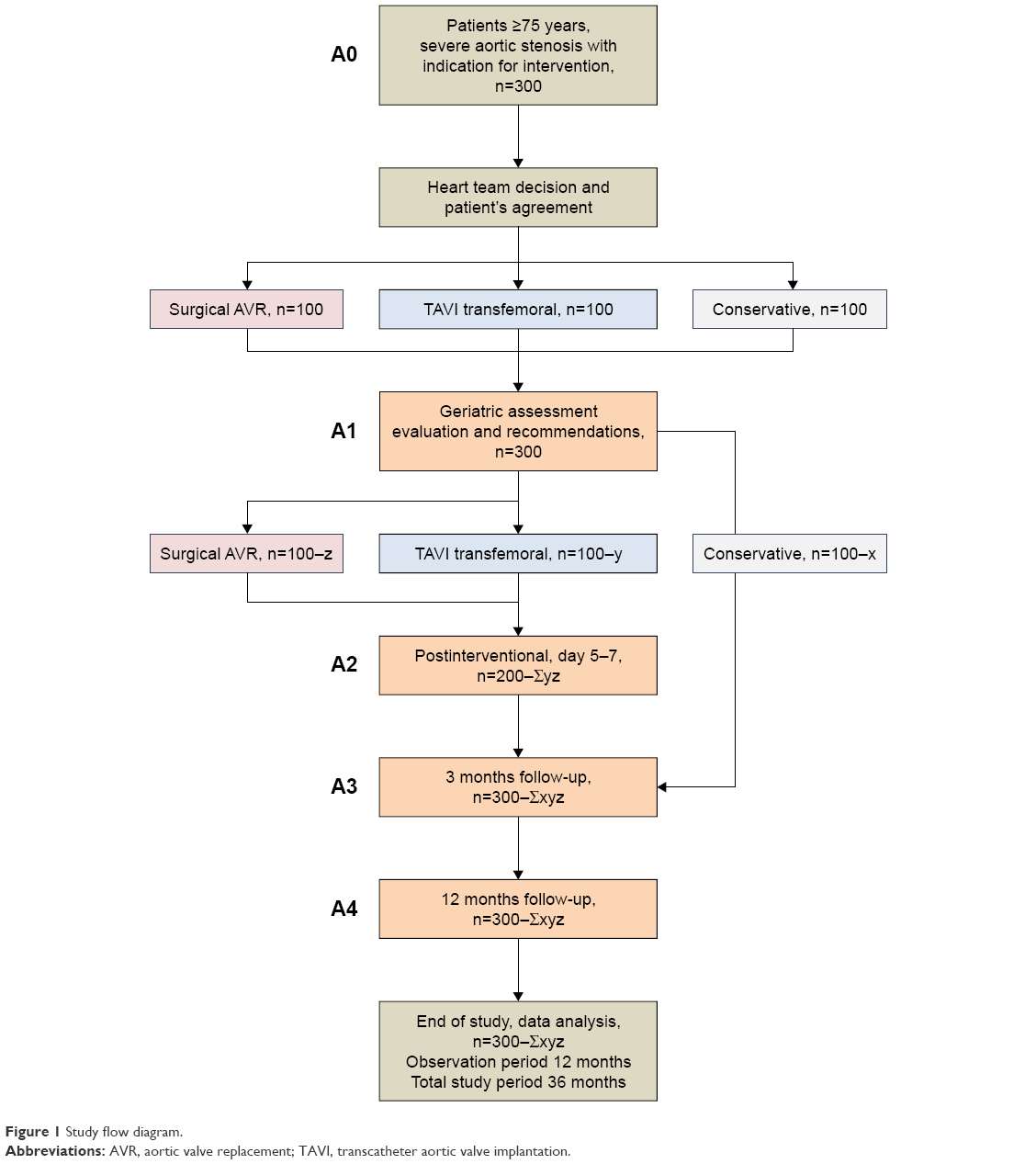 | Figure 1 Study flow diagram. |
GA
Special geriatric parameters include
Place of living: On the one hand, the place of living is a marker for disability and loss of autonomy – long-term care patients have a significantly worse prognosis than community-dwelling elderly patients. On the other hand, it is a very good outcome parameter for older patients as autonomy and independence are the most important overall goals for every geriatric intervention.
Modified cumulative illness rating scale:20 This scale is a very good marker for multimorbidity. Every organ system is assessed on a scale of 0–4. A manual is available for its application.
Bioelectrical impedance analysis (BIA):21 Sarcopenia is a frequent syndrome in older adults. BIA provides a good quality to assess body composition and muscle mass. BIA is not allowed to be done in patients with a pacemaker.
Frailty:22 Frailty is a specific geriatric syndrome. The most common definition of frailty was posited by Fried et al. They mentioned 5 criteria. Using these criteria, patients can be split into 3 groups as follows: frail, pre-frail, and fit.
Activities of daily living (ADL):23 The ADL score is a valid tool for assessing overall function in daily living in relation to 10 items (bowels, bladder, grooming, toilet use, feeding, transfer, mobility, dressing, stairs, and bathing). It is especially appropriate for in-hospital or long-term care patients.
Instrumental ADL (IADL):24 The IADL scale of Lawton and Brody is a similar tool and assesses the everyday competence of older adults. It contains 8 central ADL and autonomy (ability to use a telephone, shopping, food preparation, housekeeping, laundry, mode of transportation, responsibility for own medication, and ability to handle finances).
Parker Mobility Score (PMS):25 The PMS assesses the mobility of patients in 3 situations (house, outside, and shopping) and 4 categories. The PMS is well established in orthogeriatric trials and shows a strong correlation with short- and long-term mortality.
Gait speed:21 Gait speed is easy to measure and poses an objective parameter. A reduced gait speed is a predictor of worse outcome for older adults. Usually, gait speed is measured over 6 m; the cutoff is 0.8 m/s.
Handgrip strength:21 Handgrip strength is a valid test for estimating muscle strength in older adults. Reduced grip strength is a predictor of falls, further disabilities, and mortality in older age. Handgrip strength is measured by using a vigorimeter.
Timed Up and Go:26 This test assesses the gait speed, gait disabilities, and muscle strength. It is very well established. The time in seconds to get up from a chair, walk 3 m, turn around, and sit down is taken. The Timed Up and Go is a very useful test for observing the course of treatment or rehabilitation.
The Mini Mental State Examination27 and Clock Completion:28 are 2 standard tests for measuring cognitive disorders in older adults. Postoperatively, the prevalence and severity of delirium is assessed using the Delirium Observation Scale.29,30
Geriatric Depression Scale:31 This is a valid screening tool for depression in older adults. The questionnaire includes 15 items.
Mini Nutritional Assessment (MNA):32 Together with body mass index, we will use the MNA to assess the nutrition status of patients. The MNA is a mixture of anthropometric measurements and questions about a patient’s history and eating habits.
Screening tool of older persons’ prescriptions (STOPP) and screening tool to alert to right treatment (START):33 Polypharmacy, including inappropriate medication, as well as undertreatment, is a challenge in the care of older patients. To evaluate the appropriateness of medication, we use the STOPP and START list. This list captures inappropriate medication as well as undertreatment.
EuroQol-5D:34 Quality of life is often under-reported in clinical trials. The EuroQol-5D is a health questionnaire, which assesses quality of life using 5 different items (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression).
Test battery 0 – “A0”
The routine cardiological examinations made during the process of indication and pretesting will be documented as test battery A0. A0 includes no special geriatric parameter because at this stage, geriatric evaluation does not play any role. Table 1 shows an overview of all cardiological tests.
Test battery 1 – “A1”
Test battery A1 follows the indication and the decision about the treatment approach, which has been made by the heart team. Test battery A1 focuses on geriatric aspects and GA. Table 1 shows an overview of the geriatric parameters and tests. After the geriatric evaluation, all patients receive an individual recommendation aimed at optimizing their functionality.
Test battery 2 – “A2”: postinterventional, days 5–7, perioperative outcome
This phase is limited to the hospital stay, particularly the perioperative phase. Table 1 shows an overview of the test program.
Test battery 3 – “A3”: 3 months, short-term outcome
At this point, we want to evaluate the short-term outcome. Table 1 shows an overview of the test program.
Test battery 4 – “A4”: 12 months, long-term outcome
The final test battery will show us the long-term outcome. Table 1 shows an overview of the test program.
Data management
An identification number will be allocated to each proband. Data collection will be done by study nurses and data will be entered in a database (Microsoft Access, Microsoft Corporation, Redmond, WA, USA).
Statistical methods
1) Sample size computation: Currently, neither preliminary data are available from previous studies nor any other information from published studies. A pilot study would last for at least 24–36 months and is not favored due to operating expense. Therefore, the sample size is fixed to n=300 a priori, which will result in an accuracy of ±5.5% for estimating probabilities. This sample size allows usage of 10 input variables for setting up a prediction model, because the ratio of sample size and number of input variables is 30. This is sufficient to end up with statistically sound prediction models, which do not suffer from overlearning. Additionally, it is highly likely that sensitivity, specificity, and negative and positive predictive values observed in the learning and verification sample will remain stable when independently tested in the randomly selected test sample.
2) Data evaluation methods: Data consistency will be checked and data will be screened for outliers. Pairwise deletion of missing variables will be applied. In addition, if more than 15% of values are missing, the number of analyzed cases will be reported in the analysis. Distributions will be evaluated for normal, gamma, Tweedie and Poisson distributions based on quantile plots or Kolmogorov–Smirnov tests. Cross-tabulation tables will be computed for discrete variables and tested by using Fisher’s exact, McNemar’s, Pearson’s chi-square, Kurskal–Wallis tests for singly ordered, marginal homogeneity Jonckheere–Terpstra, and linear-by-linear association tests. Event analyses with Cox-hazard regression models will be performed, generalized estimation equation models. or mixed models will be applied, especially generalized logit, multinomial logit-, Poisson, and normal distribution based models. Corresponding factors as well as interaction effects will be tested and further analyzed by post hoc tests. If model assumptions are not fulfilled, the following nonparametric models will be applied: Wilcoxon signed-rank test, Kruskal–Wallis analysis of variance (ANOVA), Friedman ANOVA, Wilcoxon tests, Wilcoxon–Mann–Whitney tests, and Hodges–Lehmann estimations for medians. Advanced neuronal network models (3-layer perceptron network models) will be used to analyze geriatric scores. To properly set up and test the model, the whole sample will be randomly divided into a learning, verification, and test sample in a ratio of 2:1:1. Instead of using simple 1 cutoff model, 2 cutoff models will be used to generate a gray area. Hence, the model can reject a subject’s prediction if it is highly likely that the prediction fails. The disadvantage of this approach is that not all subjects will receive a prediction. However, the most desirable advantage of this approach is that sensitivity, specificity, and negative and predictive value will rise considerably. The 95% confidence intervals will be computed for means, probabilities (Pearson–Clopper values), hazard ratios, differences of means, and correlations. Whisker plots and histograms will be used for illustration. All tests will be done 2-sided, significance level is set to 5%. No correction will be performed for multiple testing. All statistical analyses will be done using NCSS (NCSS 10, NCSS, LLC. Kaysville, UT, USA), Mathematica 11 (Wolfram Research, Inc., Mathematica, Version 11.1, Champaign, IL, USA), STATISTICA 13 (Hill, T. & Lewicki, P. Statistics: Methods and Applications. StatSoft, Tulsa, OK, USA), PASW 22 (IBM SPSS Statistics for Windows, Version 22.0., Armonk, NY, USA), and StatXact 10 (Cytel Software 2013, Cambridge MA, USA).
Discussion
Frailty per se is a major risk factor for death and disability in patients with severe AS undergoing TAVI or SAVR. To optimize patient selection for a certain treatment of AS, national guidelines strongly recommend an objective evaluation of frailty by the heart team. After many studies about frailty in TAVI and SAVR patients,35 the FOOPAS study is the first in this field to investigate frailty in older people with severe AS run by cardiologists, cardiac surgeons, and geriatricians in one team.
Comparison of different frailty scales gives an idea of both the predictive value for mortality and the meaningful clinical improvement for each individual patient, which gives an idea of disability or fatal outcomes. Future ethical decisions can more easily be made based on this clinical data. Therefore, all frailty assessments are likely to be performed in a comprehensive setup. Expected results are new findings on parameters influencing clinical and functional outcome in elderly patients independent of the method of treatment. A new frailty test, which is simple and feasible to be applied in a clinical routine by most medical professionals, may help in identifying patients for a thorough GA.
Frailty assessment should not only be an ‘eyeballing’ of the patient to quantify frailty on a subjective basis but should confirm disability in general or comorbidities such as sarcopenia, malnutrition, dementia, or depression. The lack of a clear and agreed-upon assessment is a barrier limiting its use.36–38 This lack of consensus surrounding frailty assessment tools is the major reason why frailty is often not measured routinely in clinical practice.39 Across previous studies considering frailty assessment, there are divergent prevalence estimates and effect sizes.40 Gait speed seems to be the most commonly used test to screen frailty. But characterization of frailty with gait speed alone lacks specificity to discriminate between complex patients who may or may not experience poor outcomes following TAVR or SAVR.41,42
Of course, it is in the primary interest of each clinical practitioner to achieve a clinical benefit for his/her patient through an intervention; however, this may presumably result in a consecutive overtherapy, whereas, in return, decompensated patients who are bedridden or severely restricted at the time of the evaluation are rashly rejected.19 Whether such an over- or undertherapy of elderly patients suffering from AS takes place, remains open. Here, by means of valid GAs, facts can be ascertained that would contribute a great deal toward better decision-making; which applies also with regard to ethical issues. For example, in the situation of rejecting a suspected patient.
The aim of this study is not only to add new findings to the growing body of evidence on frailty but also to outline the necessity for geriatric counselling in elderly patients to improve their clinical and functional outcome.
Limitations of the study
Due to ethical reason, the study is a non-randomized trial. Patients with severe AS treated either by TAVI or SAVR have, of course, differing risk profiles. Furthermore, the conservative arm of this study remains as “untreated patients”, of which some declined a treatment against the advice of the team. Finally, the patient’s will is crucial for substantial treatment and a possibly high drop-out rate is expected, especially in the conservative arm of this study, due to lack of adherence of these patients. Conservatively treated patients with severe AS are known to have an impaired prognosis, aggravated by advanced age. Mortality rate increases with age, heart failure, and renal insufficiency. Medical therapy does not seem to affect the survival in the entire group of conservatively treated patients with severe AS.43
Nevertheless a new simple frailty test that is feasible for application in a clinical routine by most doctors or nurses may help in identifying those patients for whom further GA should be considered to improve the outcome. Further research is necessary to define therapeutic consequences and validate their utility in other groups of patients with cardiovascular diseases.
Acknowledgments
The overall financing of €300,000 was donated by the Schöller-Familienstiftung, a private foundation located in Nuremberg, Germany. The funding source has no influence on selection of data, its evaluation, or the decision to publish the found results.
Disclosure
The authors report no conflicts of interest in this work.
References
Gummert JF, Funkat A, Beckmann A, et al. Cardiac surgery in Germany during 2008. A report on behalf of the German Society for Thoracic and Cardiovascular Surgery. Thorac Cardiovasc Surg. 2009;57(6):315–323. | ||
Eggebrecht H, Mehta RH. Transcatheter aortic valve implantation (TAVI) in Germany 2008–2014: on its way to standard therapy for aortic valve stenosis in the elderly? EuroIntervention. 2016;11(9):1029–1033. | ||
Vasques F, Messori A, Lucenteforte E, Biancari F. Immediate and late outcome of patients aged 80 years and older undergoing isolated aortic valve replacement: a systematic review and meta-analysis of 48 studies. Am Heart J. 2012;163(3):477–485. | ||
Pilgrim T, Englberger L, Rothenbühler M, et al. Long-term outcome of elderly patients with severe aortic stenosis as a function of treatment modality. Heart. 2015;101(1):30–36. | ||
Rodríguez-Mañas L, Féart C, Mann G, et al; FOD-CC group (Appendix 1). Searching for an operational definition of frailty: a Delphi method based consensus statement: the frailty operative definition-consensus conference project. J Gerontol A Biol Sci Med Sci. 2013;68(1):62–67. | ||
Kim DH, Kim CA, Placide S, Lipsitz LA, Marcantonio ER. Preoperative frailty assessment and outcomes at 6 months or later in older adults undergoing cardiac surgical procedures: a systematic review. Ann Intern Med. 2016;165(9):650–660. | ||
Talbot-Hamon C, Afilalo J. Transcatheter aortic valve replacement in the care of older persons with aortic stenosis. J Am Geriatr Soc. 2017;65(4):693–698. | ||
Holmes DR Jr, Brennan JM, Rumsfeld JS, et al; STS/ACC TVT Registry. Clinical outcomes at 1 year following transcatheter aortic valve replacement. JAMA. 2015;313(10):1019–1028. | ||
Lindman BR, Alexander KP, O’Gara PT, Afilalo J. Futility, benefit, and transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2014;7(7):707–716. | ||
Gosch M, Druml T, Nicholas JA, et al. Fragility non-hip fracture patients are at risk. Arch Orthop Trauma Surg. 2015;135(1):69–77. | ||
Gosch M, Wörtz M, Nicholas JA, Doshi HK, Kammerlander C, Lechleitner M. Inappropriate prescribing as a predictor for long-term mortality after hip fracture. Gerontology. 2014;60(2):114–122. | ||
Kammerlander C, Gosch M, Kammerlander-Knauer U, Luger TJ, Blauth M, Roth T. Long-term functional outcome in geriatric hip fracture patients. Arch Orthop Trauma Surg. 2011;131(10):1435–1444. | ||
Schoenenberger AW, Stortecky S, Neumann S, et al. Predictors of functional decline in elderly patients undergoing transcatheter aortic valve implantation (TAVI). Eur Heart J. 2013;34(9):684–692. | ||
Kim CA, Rasania SP, Afilalo J, Popma JJ, Lipsitz LA, Kim DH. Functional status and quality of life after transcatheter aortic valve replacement: a systematic review. Ann Intern Med. 2014;160(4):243–254. | ||
Chen MA. Frailty and cardiovascular disease: potential role of gait speed in surgical risk stratification in older adults. J Geriatr Cardiol. 2015;12(1):44–56. | ||
Stortecky S, Schoenenberger AW, Moser A, et al. Evaluation of multidimensional geriatric assessment as a predictor of mortality and cardiovascular events after transcatheter aortic valve implantation. JACC Cardiovasc Interv. 2012;5(5):489–496. | ||
Kappetein AP, Head SJ, Généreux P, et al; Valve Academic Research Consortium (VARC)-2. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document (VARC-2). Eur J Cardiothorac Surg. 2012;42(5):S45–S60. | ||
Mozos I, Caraba A. Electrocardiographic predictors of cardiovascular mortality. Dis Markers. 2015;2015:727401. | ||
Leon MB, Smith CR, Mack MJ, et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2016;374(17):1609–1620. | ||
Salvi F, Miller MD, Grilli A, et al. A manual of guidelines to score the modified cumulative illness rating scale and its validation in acute hospitalized elderly patients. J Am Geriatr Soc. 2008;56(10):1926–1931. | ||
Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in older people. Age Ageing. 2010;39(4):412–423. | ||
Fried LP, Tangen CM, Walston J, et al; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146–M156. | ||
Mahoney FI, Barthel DW. Functional evaluation: the barthel index. Md State Med J. 1965;14:61–65. | ||
Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(3):179–186. | ||
Parker MJ, Palmer CR. A new mobility score for predicting mortality after hip fracture. J Bone Joint Surg Br. 1993;75(5):797–798. | ||
Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. | ||
Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. | ||
Watson YI, Arfken CL, Birge SJ. Clock completion: an objective screening test for dementia. J Am Geriatr Soc. 1993;41(11):1235–1240. | ||
Schuurmans MJ, Shortridge-Baggett LM, Duursma SA. The Delirium Observation Screening Scale: a screening instrument for delirium. Res Theory Nurs Pract. 2003;17(1):31–50. | ||
Scheffer AC, van Munster BC, Schuurmans MJ, de Rooij SE. Assessing severity of delirium by the Delirium Observation Screening Scale. Int J Geriatr Psychiatry. 2011;26(3):284–291. | ||
Yesavage JA. Geriatric Depression Scale. Psychopharmacol Bull. 1988;24(4):709–711. | ||
Vellas B, Villars H, Abellan G, et al. Overview of the MNA its history and challenges. J Nutr Health Aging. 2006;10(6):456–463; discussion 463–455. | ||
Lozano-Montoya I, Vélez-Diaz-Pallarés M, Delgado-Silveira E, Montero-Errasquin B, Cruz Jentoft AJ. Potentially inappropriate prescribing detected by STOPP-START criteria: are they really inappropriate? Age Ageing. 2015;44(5):861–866. | ||
Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727–1736. | ||
Afilalo J, Lauck S, Kim DH, et al. Frailty in older adults undergoing aortic valve replacement: the FRAILTY-AVR study. J Am Coll Cardiol. 2017;70(6):689–700. | ||
Webb J, Rodés-Cabau J, Fremes S, et al. Transcatheter aortic valve implantation: a Canadian Cardiovascular Society position statement. Can J Cardiol. 2012;28(5):520–528. | ||
Otto CM, Kumbhani DJ, Alexander KP, et al. 2017 ACC expert consensus decision pathway for transcatheter aortic valve replacement in the management of adults with aortic stenosis: a report of the American College of Cardiology Task Force on clinical expert consensus documents. J Am Coll Cardiol. 2017;69(10):1313–1346. | ||
Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2017;70(2):252–289. | ||
Van Mieghem NM, Dumonteil N, Chieffo A, et al. Current decision making and short-term outcome in patients with degenerative aortic stenosis: the Pooled-RotterdAm-Milano-Toulouse In Collaboration Aortic Stenosis survey. Euro Intervention. 2016;11(11):e1305–e1313. | ||
Afilalo J, Alexander KP, Mack MJ, et al. Frailty assessment in the cardiovascular care of older adults. J Am Coll Cardiol. 2014;63(8):747–762. | ||
Afilalo J, Kim S, O’Brien S, et al. Gait speed and operative mortality in older adults following cardiac surgery. JAMA Cardiol. 2016;1(3):314–321. | ||
Alfredsson J, Stebbins A, Brennan JM, et al. Gait speed predicts 30-day mortality after transcatheter aortic valve replacement: results from the society of thoracic surgeons/American College of Cardiology Transcatheter Valve Therapy Registry. Circulation. 2016;133(14):1351–1359. | ||
Varadarajan P, Kapoor N, Bansal RC, Pai RG. Clinical profile and natural history of 453 nonsurgically managed patients with severe aortic stenosis. Ann Thorac Surg. 2006;82(6):2111–2115. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.