Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Functional MRI in Multiple System Atrophy: A Promising Biomarker for Clinical Applications
Authors Xiao S, Ding Y, Weiss A, Cai L, Wang X, Geng X
Received 13 September 2025
Accepted for publication 11 February 2026
Published 18 February 2026 Volume 2026:22 566720
DOI https://doi.org/10.2147/NDT.S566720
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rakesh Kumar
Shuying Xiao,1,2 Yuchuan Ding,3 Alexander Weiss,3 Lipeng Cai,1,2 Xuemei Wang,1 Xiaokun Geng1– 3
1Department of Neurology, Beijing Luhe Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Luhe Institute of Neuroscience, Capital Medical University, Beijing, People’s Republic of China; 3Department of Neurology, Wayne State University School of Medicine, Detroit, MI, USA
Correspondence: Xiaokun Geng, Stroke Center, Department of Neurology, Beijing Luhe Hospital, Capital Medical University, No. 82 Xinhua South Road, Tongzhou District, Beijing, 101149, People’s Republic of China, Email [email protected] Yuchuan Ding, Department of Neurosurgery, Wayne State University School of Medicine, 550 E Canfield, Detroit, MI, 48201, USA, Email [email protected]
Abstract: Multiple system atrophy (MSA) is a neurodegenerative disease characterized by α-synuclein pathology and pronounced clinical heterogeneity, making early diagnosis difficult. Functional magnetic resonance imaging (fMRI) has emerged as a promising tool to enhance diagnostic precision. By identifying disease- and symptom-specific network connectivity abnormalities, fMRI may reflect pathological changes in corresponding brain regions, thereby providing mechanistic insights. Recent work demonstrates that resting-state fMRI (rs-fMRI) can capture subtype-specific patterns, predominant basal ganglia–cortical disruption observed in the parkinsonian subtype of MSA (MSA-P) and cerebellar–cortical disconnection in the cerebellar subtype (MSA-C), reflecting their respective underlying pathologies of striatonigral degeneration and olivopontocerebellar atrophy. Rs-fMRI can also distinguish MSA from related parkinsonian syndromes, including Parkinson’s disease (PD) and progressive supranuclear palsy (PSP), based on characteristic disruptions in cerebellar-cortical network connectivity. These patterns align with pathological features, providing important insights into disease progression. Task-based fMRI (t-fMRI), though less studied, further highlights impairments in motor network integration. Beyond diagnosis, fMRI has shown potential in evaluating treatment effects, with neuromodulatory interventions such as transcranial magnetic stimulation associated with measurable network changes. However, existing studies remain constrained by small sample sizes, single-center designs, and methodological variability. Future directions include large, multicenter trials, standardized imaging protocols, and integration with multimodal and computational approaches to establish robust fMRI-based biomarkers. Collectively, these advances position fMRI as a promising biomarker-oriented tool in MSA, supporting subtype classification, enhancing differential diagnosis from PD and PSP, elucidating symptom-specific network dysfunction, and enabling objective evaluation of therapeutic interventions in clinical and translational settings.
Keywords: synucleinopathy, neurodegeneration, functional connectivity, brain networks
Introduction
Multiple system atrophy (MSA) is a neurodegenerative disorder characterized by autonomic dysfunction, parkinsonism, and cerebellar ataxia. Its pathological hallmark is the deposition of α-synuclein inclusions in oligodendrocytes, leading to degeneration of the striatonigral and olivopontocerebellar systems.1 The peak age of onset is in the sixth decade of life. Current estimates of prevalence and incidence are 1.9–4.9 per 100,000 and 0.6–3 per 100,000 people per year, respectively, with a median survival of 6–10 years from symptom onset.2 Based on core symptoms, MSA is classified into the parkinsonian subtype (MSA-P) and the cerebellar subtype (MSA-C). However, many patients exhibit overlapping features of both subtypes during the disease course, which complicates accurate clinical classification.3
Early diagnosis of MSA remains difficult due to substantial overlap of initial motor symptoms, such as bradykinesia, rigidity, postural instability, and gait disturbance, with other parkinsonian syndromes, including PD and PSP.4,5 This clinical similarity, together with the absence of reliable disease-specific biomarkers,6–8 contributes to high rates of misdiagnosis in early disease stages.9,10 Although structural MRI is routinely used in the diagnostic evaluation of MSA, its utility is limited early in the disease course.11 Characteristic MRI features often emerge only after significant neurodegeneration, while early pathological changes may be masked by compensatory mechanisms or involve subtle microstructural alterations that are not detectable on conventional T1- or T2-weighted imaging.12,13 Consequently, structural MRI findings may fail to reflect evolving clinical phenotypes, highlighting the need for imaging approaches capable of detecting early functional network abnormalities.14,15
Conventional structural MRI can reveal several characteristic features of MSA, including atrophy of the putamen, pons, middle cerebellar peduncle (MCP), and cerebellum, as well as T2 signal abnormalities such as putaminal hypointensity, pontine hyperintensity, and the “hot cross bun” sign.16 Although these findings demonstrate high diagnostic specificity (>80%), their sensitivity in early disease stages is limited,17 and the extent of regional atrophy does not consistently correlate with symptom severity, particularly for non-motor manifestations.18 These limitations suggest that structural degeneration alone cannot fully account for the heterogeneous clinical presentation of MSA.
MSA is a neurodegenerative disorder neuropathologically defined by oligodendroglial and neuronal cytoplasmic inclusions containing pathological insoluble alpha-synuclein aggregates.16 These pathological processes disrupt synaptic function and large-scale network communication through mechanisms such as impaired neuronal signaling, metabolic dysregulation, and abnormal neural synchronization. Importantly, such functional disturbances occur early in the disease course and precede irreversible neuronal loss and gray matter atrophy, ultimately leading to progressive motor and non-motor clinical impairment.8,19,20 In addition to parkinsonism and cerebellar ataxia, patients with MSA frequently develop prominent non-motor symptoms, such as autonomic dysfunction, cognitive impairment, depression, sleep disturbances, which substantially affect quality of life and remain poorly explained by structural imaging alone.21–24
In recent years, fMRI has been increasingly applied in the research of MSA. fMRI approaches include resting-state functional MRI (rs-fMRI) and task-state functional MRI (t-fMRI). Rs-fMRI assesses intrinsic “functional” connectivity by mapping synchronized neural activation patterns across brain regions while subjects remain at rest. This method identifies resting-state networks using blood-oxygen-level-dependent (BOLD) signal fluctuations. In contrast, t-fMRI requires subjects to perform specific tasks (eg, visual, auditory, or motor tasks) or respond to external stimuli (eg, flashes or sounds) while BOLD signal changes are recorded. Through these strategies, researchers can examine neural activity during task execution and stimulus response, providing insights into functional organization and brain network dynamics.25–27
This article aims to systematically summarize advances in fMRI research on MSA, including its role in subtyping, differential diagnosis, and explanation of symptom mechanisms, while also exploring future applications.
Rs-fMRI Alterations in MSA Patients
In MSA, the accumulation of α-synuclein-positive glial cytoplasmic inclusions (GCIs) disrupts widespread brain networks, leading to clinical dysfunction.28 While structural changes such as gray matter atrophy typically appear only in later stages, rs-fMRI can detect disease-related alterations earlier and more sensitively, aiding in the identification of early-stage patients.8
Rs-fMRI Alterations in MSA-C and MSA-P Patients
The cerebellum is the primary region affected in MSA-C, and most fMRI studies therefore focus on its connectivity with other brain regions. Research has demonstrated widespread impairments in cerebellar-cortical functional connectivity (FC) in MSA-C, including disruptions in the default mode network (DMN), sensorimotor network, and visual cortices.29–32 Studies of white matter connectivity further have shown significantly reduced coupling in the superior, middle, and inferior cerebellar peduncles, as well as corticospinal tracts (CSTs),14 consistent with MSA’s pathological hallmarks. However, the reported correlations between cerebellar connectivity loss and disease duration or clinical progression are inconsistent, likely reflecting heterogeneity in patient cohorts with respect to disease stages and severity. Interestingly, MSA-C patients also exhibit enhanced cerebellar-pontine connectivity, which may represent compensatory mechanisms at specific disease phases.28
Compared with MSA-C, fewer fMRI studies have examined MSA-P, but available evidence indicates prominent dysfunction within basal ganglia–cortical motor networks. Rs-fMRI studies have reported reduced fractional amplitude of low-frequency fluctuation (fALFF), reflecting decreased spontaneous neuronal activity in the caudate nucleus and putamen of MSA-P patients. In addition, FC between the putamen and cortical motor regions, including the precentral gyrus, supplementary motor area, and cingulate cortex, is widely weakened, with disrupted interhemispheric basal ganglia connectivity correlating with motor symptom severity. These findings suggest that impaired basal ganglia–cortical communication directly contributes to deficits in motor execution and action sequencing in MSA-P.33 Conversely, increased cerebellar fALFF has been observed, which may represent a compensatory response during early disease stages as basal ganglia–cortical circuits progressively decline.34
Differences in fMRI Findings Between MSA-P and MSA-C Subtypes
The pathological features, treatment responses, and prognoses of MSA subtypes differ significantly. Accurate classification of MSA-P versus MSA-C is therefore critical, not only for understanding of disease pathogenesis and developing targeted therapies but also for improving clinical management. Classification of MSA subtypes is challenging.35 Beyond clinical phenotyping, there remains an urgent need for identifying objective biomarkers to distinguish the two subtypes.3
Recent fMRI studies have revealed several important differences: In MSA-C, markedly reduced connectivity has been observed between the cerebellar dentate nucleus and both the basal ganglia and sensorimotor cortex, whereas in MSA-P patients, reductions were more evident in putamen-cortical connectivity.36 The DMN further demonstrated prominent dysfunction in DMN-cerebellar circuits in MSA-C, while in MSA-P patients, the dominant impairment lies within fronto-basal networks.37 These results are consistent with prior dopamine transporter positron emission tomography (DAT-PET) studies which showed more severe dopaminergic denervation in the basal ganglia of MSA-P patients.38 Another study adopting static and dynamic graph theory metrics attributes added another layer of distinction, as MSA-C patients exhibited greater declines in local efficiency and weighted degree of connectivity in the cerebellum, with stronger correlations with clinical severity scores.39
In summary, MSA-C is primarily characterized by widespread cerebellar-cortical connectivity reduction, while MSA-P patients show predominant basal ganglia-cortical circuit disconnection. Importantly, the median disease duration of patients enrolled in the studies was approximately 3 years, corresponding to the early to mid-stage of MSA. Further longitudinal studies are thus required to investigate how FC differences between subtypes evolve with disease progression. Variability in reported FC changes across studies likely reflects heterogeneity in patient cohorts, disease stage, and imaging methodologies. Future multicenter studies adopting standardized acquisition and analysis protocols are essential to enable meta-analyses and generate robust and reliable conclusions.
Changes in Rs-fMRI of Motor and Non-Motor Symptoms in MSA Patients
Rs-fMRI Alterations in MSA Patients with Depression
Depression is a frequent and clinically significant non-motor symptom in MSA, substantially affecting quality of life of patients.40–42 Increasing evidence suggests that depressive symptoms in MSA are closely linked to dysfunction within distributed limbic–cortical networks, which can be sensitively captured by rs-fMRI. Reduced functional activity in the rostral anterior cingulate cortex (rACC), the right middle temporal lobe, and the right thalamus has been associated with greater depression severity in MSA.43 In addition, aberrant FC between the amygdala and middle frontal gyrus has been linked to emotional dysregulation, further contributing to depression.44 Overall, these findings suggest that depression in MSA arises from disruption within limbic-cortical circuits, particularly those involving the amygdala and prefrontal-thalamic pathways that regulate affective processing.
Rs-fMRI Alterations in MSA Patients with Cognitive Impairment
Cognitive impairment (CI) is not considered a core clinical feature of MSA and is absent from current diagnostic criteria.16 However, studies indicate that approximately 25% of patients exhibit deficits in visuospatial function, attention, and executive functioning,40 while autopsy findings reveal pathological changes in cognition-related regions in up to 32% of cases.45
Structural MRI studies demonstrate that CI correlates with cortical-subcortical atrophy across multiple brain regions,21,46–51 including gray matter atrophy in the bilateral basal ganglia, bilateral thalamus, cerebellum, temporal/frontal lobes,21 and the pericalcarine cortex,48 etc. However, emerging research suggests that early cognitive decline in MSA is more closely related to functional disruption than to structural alterations.52,53 Yang et al identified decreased middle prefrontal cortex activity and altered FC with the precuneus, inferior parietal lobe, and insula were possible biomarkers of cognitive dysfunction in patients with MSA.54 A 2023 Study further demonstrated alterations in spontaneous activity within the dorsolateral prefrontal cortex (DLPFC) and cerebellum, along with disrupted DLPFC-inferior parietal lobule (IPL) and cerebello-cerebral networks, highlighting these regions as potential biomarkers for early cognitive decline.52
Additional work has implicated cerebellar dysfunction: reduced FC between the cerebellum and prefrontal/amygdala regions appears to underlie CI in MSA.53 Intriguingly, enhanced parietal-cerebellar connectivity observed in some patients may represent a compensatory mechanism that delays cognitive deterioration.52 In summary, these results highlight the dual role of the cerebellum in both motor control and higher-order cognitive functions such as executive processing and emotional regulation,55 emphasizing its critical yet understudied involvement in MSA-related CI. The findings from fMRI not only confirm structural damage in key regions but also revealed disrupted connectivity within brain networks.
Rs-fMRI in MSA Patients with Freezing of Gait
Freezing of gait (FoG) is a common and debilitating symptom in MSA,56 yet, rs-fMRI studies addressing FoG in this population remain limited compared to those in PD. A 2022 study demonstrated that FOG severity was negatively correlated with left thalamic degree centrality and found abnormal FC between the thalamus and multiple regions, including the middle temporal gyrus, inferior parietal lobule, and cerebellum.57 Another study found altered topological properties in whole-brain networks, including the dorsal attention network (DAN), the frontoparietal network (FPN), and the DMN, with nodal centrality changes in frontal and limbic regions correlating negatively with FOG severity.58 Together, these findings suggest that FoG in MSA arises from dysfunction across distributed networks involved in motor planning, attention, and executive control, highlighting the potential of rs-fMRI to identify clinically relevant network biomarkers for this disabling symptom.
Rs-fMRI Alterations in the Central Autonomic Network (CAN) in MSA
Autonomic dysfunction is a feature of MSA, such as orthostatic hypotension, urinary symptoms, and constipation.16 Central regulation of autonomic function is mediated by the central autonomic network (CAN) in the human brain, which comprises interconnected cortical and subcortical regions including the posterior midcingulate cortex (pMCC), right anterior insula (RaINS), left posterior insula (LpINS), left amygdala (LAMYG) and ventromedial prefrontal cortex (vmPFC).59 Rs-fMRI studies have demonstrated significant FC alterations within the CAN in patients with MSA. A recent study reported disrupted connectivity between CAN hubs and sensorimotor, limbic, striatal, and cerebellar regions, with these abnormalities correlating with motor symptom severity, selected non-motor symptoms such as urinary dysfunction and cognitive impairment, and overall disease severity.60 These findings suggest that CAN dysfunction in MSA extends beyond isolated autonomic failure and may drive broader clinical deterioration. However, direct correlations between CAN connectivity alterations and specific autonomic features, particularly orthostatic hypotension, remain insufficiently explored and warrant further investigation.
In addition to fMRI, studies have found that changes observed with other imaging techniques, such as dopaminergic radiotracer imaging, are also significantly correlated with certain clinical features in MSA patients, including the severity of symptoms like urinary incontinence and dysphagia.61,62
Rs-fMRI in Differentiating MSA from PD and PSP
PD and MSA, particularly MSA-P, share overlapping motor manifestations in early disease stages, making accurate differentiation difficult. Postmortem studies have shown that 15–38% of clinically diagnosed MSA cases were misclassified, with 16% misdiagnosed as PD.63,64 Conversely, about 35% of PD diagnoses were later revised to MSA after pathological confirmation.63,65 Compared with PD, MSA-P progresses more rapidly, demonstrates poor or absent response to dopaminergic therapy, and is associated with greater disability and shorter survival.66 Accurate distinction between these disorders is crucial for prognosis, clinical trial enrollment, and therapeutic decision-making. Despite the clinical importance, no objective biomarker currently provides definitive discrimination.6 However, recent rs-fMRI studies have offered promising diagnostic insights.29,34,67–74
A multi-modal MRI study incorporating susceptibility-weighted imaging, rs-fMRI, T1-weighted imaging, and diffusion tensor imaging demonstrated that fMRI-derived features had superior discriminative power compared with other MRI modalities differentiating PD from MSA.70 Baggio et al further demonstrated that, compared to PD, MSA patients exhibited reduced FC between the cerebellum and cerebral networks including, the left frontoparietal network (FPN), sensorimotor network, and salience network, as well as reduced cerebellum-striatum connectivity.69 Combined structural and fMRI studies further revealed that MSA patients display significantly lower FC between the bilateral dentate nuclei (DN) and the DMN, alongside cerebellar gray matter atrophy, with both measures correlating cognitive and motor symptom severity.70
Other analytic approaches support these distinctions. One study investigated brain connectome alterations in MSA-P and PD using a variety of methodologies (graph theory, whole-brain FC, and machine learning), and found that MSA-P patients exhibited severe cerebellar-cortical disconnection, whereas PD patients demonstrated basal ganglia-cortical disconnection with relative preservation of cerebellar function. This approach achieved high diagnostic accuracy (AUC>0.90) in distinguishing early-stage MSA-P from PD.74
While PD is characterized by neuronal α-synuclein inclusions (Lewy bodies) that are associated with dopaminergic neuron loss in the substantia nigra, MSA features glial α-synuclein pathology predominantly affecting oligodendrocytes. The oligodendroglial α-synuclein pathology in MSA is associated with a more rapid progression and earlier onset of severe motor and autonomic dysfunction compared to PD.5 These pathological distinctions have direct implications for neuroimaging. While PD shows predominant nigrostriatal dysfunction, α-synuclein-driven glial pathology in MSA leads to more diffuse network disruption, affecting basal ganglia–cortical and cerebellar–cortical circuits. Our fMRI findings of widespread connectivity alterations likely reflect this glial α-synuclein burden Table 1. Thus, these results suggest a mechanistic link between the characteristic pathology of MSA and its functional impairment.
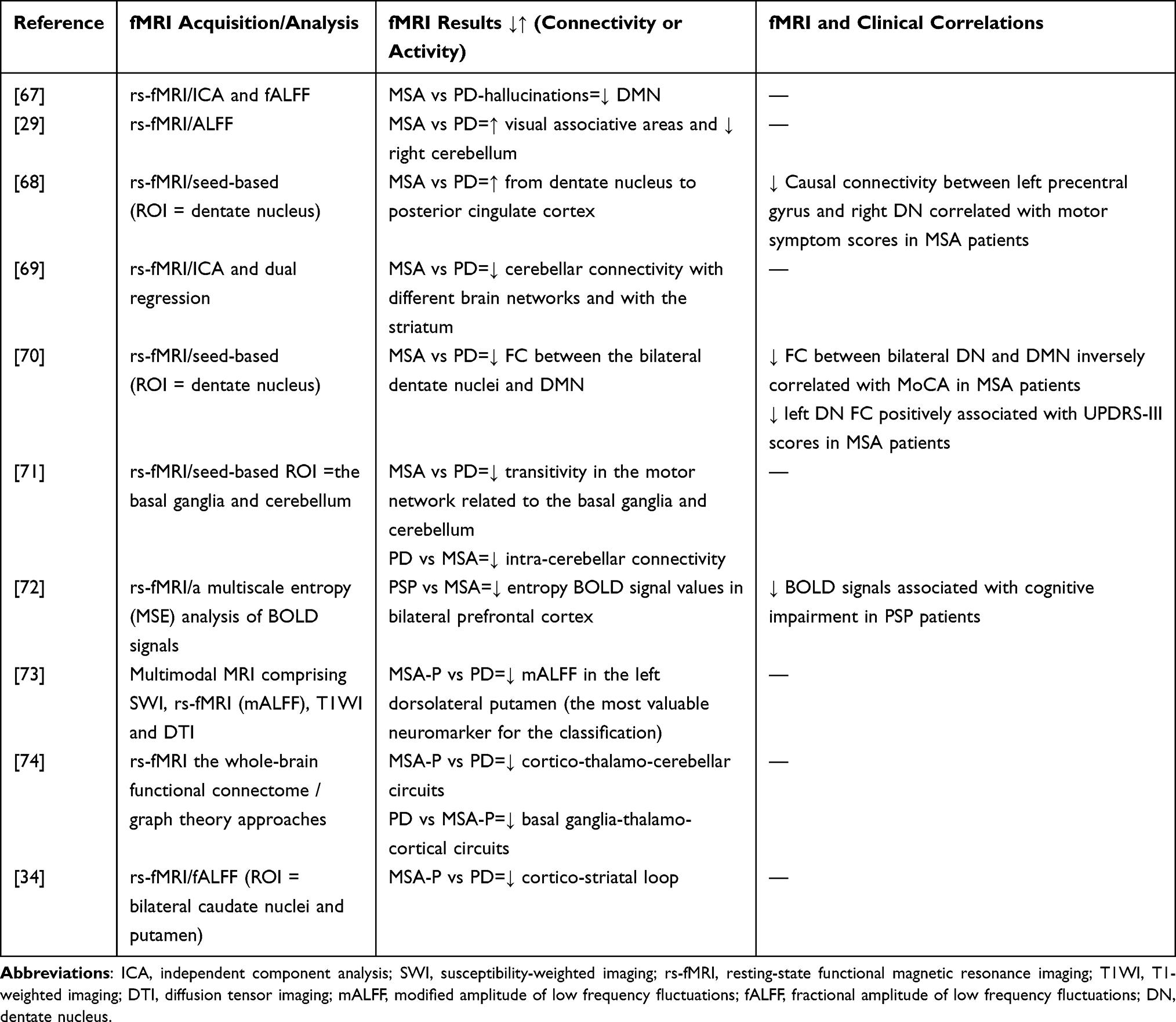 |
Table 1 Resting State fMRI Findings in Differentiating MSA From PD and PSP Patients |
In summary, in MSA-P patients, there was markedly reduced cerebellar connectivity with the FPN and sensorimotor networks, while PD patients had more pronounced basal ganglia-cortical circuit disconnection. Beyond conventional FC analyses, connectome-based and graph-theoretical approaches have emerged as an important direction in fMRI studies of MSA, enabling whole-brain characterization of network efficiency, nodal centrality, and dynamic connectivity. Recent studies using these methods have demonstrated specific network disruption and correlations with clinical severity, providing complementary systems-level insights into MSA as a network disorder.39,74
Rs-fMRI in Differentiating MSA from PSP
PSP and MSA also present overlapping early clinical features, including bradykinesia, rigidity, postural instability, and cognitive decline, causing further diagnostic challenges.75 In 2021, Kadota et al used rs-fMRI to delineate distinct neural signatures. PSP was characterized by reduced signal complexity in the bilateral prefrontal cortices and prominent frontal lobe dysfunction, while MSA demonstrated cerebellar network abnormalities.72 These findings highlight that rs-fMRI can capture divergent network vulnerabilities-frontally driven dysfunction in PSP versus cerebellar-centric disruption in MSA, providing a potential biomarker for early differential diagnosis. Currently, this is the only study utilizing fMRI to differentiate MSA from PSP, thus the evidence remains preliminary. Further research is required to confirm these findings and to better characterize FC differences between the two disorders.
It is worth noting that fMRI-derived features, especially characteristic patterns of cerebello-cortical disconnection, provide clinically interpretable imaging signatures that can support the differential diagnosis of MSA-P from PD and PSP. Rather than serving as isolated markers, these FC patterns can complement clinical assessment by reflecting disease-specific network vulnerability, thereby enhancing diagnostic precision in routine clinical evaluation.
In recent years, advances in other imaging technologies, such as diffusion tensor imaging (DTI), have further contributed to the differential diagnosis of parkinsonian syndromes.76 DTI has demonstrated high accuracy in distinguishing MSA from related disorders by capturing microstructural white matter degeneration, while cerebral glucose metabolism imaging provides complementary metabolic information.77 Integrating fMRI with DTI and PET may therefore enhance diagnostic capability by combining functional, structural, and metabolic biomarkers.
Rs-fMRI as a Tool for Treatment Effect Evaluation in MSA
Rs-fMRI has emerged as a valuable tool for assessing the effects of neuromodulatory therapies in MSA. Targeted transcranial magnetic stimulation (TMS) applied to the left primary motor cortex (M1) has been shown to enhance functional connectivity with the DMN and cerebello-limbic networks, with these changes significantly correlating with improvements in motor symptoms.78 In a subsequent investigation, a dual-target TMS protocol applied to the cerebellum and bilateral M1 produced positive alterations in motor network connectivity in patients who demonstrated clinical motor improvement, suggesting that rs-fMRI can sensitively track therapy-induced neural reorganization.79
More recently, a clinical trial combined rs-fMRI with electroencephalography (EEG) to generate a more comprehensive mapping of FC across brain regions. This multimodal approach aims to optimize the precision of repetitive TMS (rTMS) efficacy assessment, potentially guiding individualized treatment strategies.80 Overall, these results highlight rs-fMRI’s potential to serve as a biomarker-driven framework for personalizing and monitoring therapeutic interventions in MSA, offering both mechanistic insight and clinical utility.
Task-State Functional MRI (t-fMRI) in MSA
Compared to rs-fMRI, t-fMRI studies in MSA are relatively limited but have revealed distinct functional characteristics. For example, during grip force tasks, MSA-P patients exhibited reduced activation in the basal ganglia and primary motor cortex, along with insufficient compensatory cerebellar activation, indicating impaired motor network integration.81
A longitudinal t-fMRI study that tracked functional changes in the basal ganglia, cerebellum, and motor cortex over one year in patients with PD, MSA-P, and PSP found that MSA patients showed decreased functional activity in the primary motor cortex, supplementary motor area (SMA), and superior cerebellar motor regions (lobules V–VI). In contrast, PSP patients exhibited reductions across all regions of interest, while PD patients demonstrated activity declines only in the putamen and primary motor cortex. These results suggest that functional abnormalities progressed more rapidly in MSA and PSP compared with PD, reflecting distinct pathological spreading patterns among parkinsonian syndromes.82 This longitudinal t-fMRI study further demonstrated that tracking dynamic changes in task-related brain networks can distinguish disease progression patterns among PD, MSA-P, and PSP. From a functional neuroimaging perspective, these findings support fundamentally distinct neuropathological spreading mechanisms, characterized by relatively slow, basal ganglia-centered progression in PD83 versus more rapid and widespread multisystem involvement in MSA-P84 and PSP.85
Overall, the application of t-fMRI in MSA research, though relatively limited compared to rs-fMRI, has revealed distinct patterns of task-related brain functional abnormalities. Future t-fMRI studies may further exploit symptom-specific task paradigms, such as autonomic regulation, balance control, and sleep-wake modulation, to explore the neural mechanisms underlying both motor and non-motor manifestations of MSA.
Discussion
Functional MRI as a Promising Biomarker in MSA
MSA remains one of the most challenging neurodegenerative disorders to diagnose and monitor, particularly in its early stages, due to marked clinical heterogeneity and the lack of reliable biomarkers. In this context, fMRI has emerged as a powerful tool for capturing disease-related alterations in large-scale brain networks that may precede overt structural degeneration. The findings summarized in this review collectively support the concept that fMRI provides sensitive, pathophysiologically meaningful, and clinically relevant biomarkers for MSA, with potential applications spanning early diagnosis, subtype classification, differential diagnosis, mechanistic interpretation of symptoms, and therapeutic monitoring.
fMRI Reveals Early and Subtype-Specific Network Vulnerability in MSA
A central contribution of fMRI in MSA lies in its ability to detect early functional network disruption before irreversible neuronal loss becomes evident on conventional structural imaging.14,19 Available rs-fMRI studies consistently demonstrate distinct and reproducible connectivity patterns corresponding to MSA subtypes. MSA-C is predominantly characterized by widespread cerebellar–cortical disconnection, particularly involving the dentate nucleus, sensorimotor cortex, and DMN, whereas MSA-P shows more pronounced disruption of basal ganglia–cortical circuits with relative cerebellar sparing, at least in early to mid-disease stages.30,32,34 These functional signatures align closely with known neuropathological distributions, olivopontocerebellar degeneration in MSA-C and striatonigral degeneration in MSA-P, thereby reinforcing the biological validity of fMRI-derived biomarkers.
Importantly, several studies suggest that fMRI abnormalities may reflect not only neurodegeneration but also compensatory network reorganization.28,34 Increased cerebellar activity or enhanced cerebellar–pontine connectivity observed in some patients may represent adaptive responses aimed at preserving motor or cognitive function during early disease phases. This dual capacity of fMRI to capture both degenerative and compensatory processes provides unique insight into disease dynamics that cannot be obtained from structural imaging alone.28,34,52
Mechanistic Insights into Motor and Non-Motor Symptoms
Beyond its diagnostic utility, fMRI substantially advances our understanding of the neural mechanisms underlying the diverse motor and non-motor manifestations of MSA.44,53,58 Altered connectivity within limbic-cortical circuits has been linked to depression,44 while disruptions in cerebello-prefrontal and frontoparietal networks correlate with cognitive impairment, even in the absence of significant cortical atrophy.52 Similarly, freezing of gait has been associated with dysfunction across distributed networks involving the thalamus, cerebellum, attention and executive control systems, underscoring its multifactorial neural basis.57,58
Particularly noteworthy is the emerging role of fMRI in characterizing alterations within the central autonomic network (CAN), which provides a mechanistic framework for understanding autonomic failure, a defining feature of MSA. FC changes between CAN hubs and motor, limbic, and cerebellar regions suggest that autonomic dysfunction in MSA is not an isolated phenomenon but is integrated with global network degeneration.60 These findings reinforce the concept of MSA as a network-level disorder rather than a collection of regionally confined pathologies.
Differential Diagnosis and Biomarker for Treatment Monitoring and Clinical Trials
Accurate differentiation of MSA from PD and PSP remains a major unmet clinical need. Accumulating evidence indicates that fMRI-derived network signatures, particularly patterns of cerebellar-cortical disconnection, offer strong discriminative power.69,70,72,74 Compared with PD, which is dominated by basal ganglia–cortical dysfunction with relatively preserved cerebellar connectivity, MSA exhibits early and prominent cerebellar network involvement.69–71 In contrast, PSP is marked by frontal network dysfunction and reduced signal complexity in prefrontal regions, distinguishing it from the cerebellar-centric abnormalities seen in MSA.72
The integration of advanced analytical approaches, including graph theory and machine learning, has further enhanced diagnostic accuracy, with some studies reporting excellent performance in distinguishing early-stage MSA-P from PD.39,74 These findings position fMRI as a key component of future multimodal diagnostic frameworks for atypical parkinsonian syndromes.
Another promising application of fMRI lies in its ability to sensitively track treatment-induced neural reorganization. Changes in resting-state connectivity following neuromodulatory interventions such as transcranial magnetic stimulation have been shown to correlate with clinical improvement, highlighting fMRI’s potential role as an objective outcome measure in therapeutic trials.78,79,86 Given the lack of disease-modifying treatments for MSA, the availability of a non-invasive biomarker capable of capturing subtle functional changes is particularly valuable for early-phase clinical studies and personalized intervention strategies.
Limitations
Despite these advances, several limitations currently hinder the translation of fMRI into routine clinical practice. Most existing studies are cross-sectional, single-center investigations with small sample sizes and heterogeneous patient populations. Variability in imaging acquisition parameters, preprocessing pipelines, medication status, and analytical strategies complicates cross-study comparisons and limits reproducibility. Moreover, longitudinal fMRI studies tracking disease progression remain scarce, leaving the temporal evolution of functional network changes in MSA incompletely understood. Additionally, heterogeneity in patient characteristics, including age, disease duration, and clinical severity, may significantly influence functional network connectivity and contribute to variability across studies. Pharmacological factors, particularly dopaminergic and other symptomatic medications, can also modulate neural activity and resting-state connectivity, potentially confounding disease-related fMRI findings. These sources of variability emphasize the importance of careful group stratification and medication control when interpreting functional imaging results in MSA.
Conclusion and Future Directions
In conclusion, current evidence supports fMRI as a promising and versatile biomarker for MSA. By capturing early, dynamic, and system-level brain dysfunction, fMRI bridges the gap between molecular pathology and clinical phenotype—particularly where conventional MRI measures of atrophy lack sensitivity in early disease stages. Integration with structural MRI, DTI, and PET imaging offers a powerful multimodal approach: while atrophy quantification provides anatomical specificity, fMRI reveals functional disruption preceding structural change. This synergy can address critical gaps in diagnosis (earlier detection and subtype differentiation) and treatment evaluation (monitoring network-level responses to emerging neuroprotective therapies). With continued methodological refinement and validation in longitudinal cohorts, fMRI-based biomarkers have the potential to shift MSA management from symptom-driven care to mechanism-guided, individualized treatment strategies.
Future research should prioritize large, multicenter, longitudinal studies with standardized imaging protocols and careful clinical phenotyping. The integration of fMRI with complementary modalities, such as DTI, high-resolution structural MRI, dopaminergic and α-synuclein PET, and fluid biomarkers, is essential for developing robust, multimodal biomarker panels. In parallel, advanced computational approaches, including network-based modeling and artificial intelligence, may further enhance the sensitivity and specificity of fMRI-derived metrics.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Krismer F, Fanciulli A, Meissner WG. et al. Multiple system atrophy: advances in pathophysiology, diagnosis, and treatment. Lancet Neurol. 2024;23(12):1252–12. doi:10.1016/s1474-4422(24)00396-x
2. Ndayisaba A, Halliday GM, Khurana V. Multiple System Atrophy: pathology, Pathogenesis, and Path Forward. Ann Rev Pathol. 2025;20(1):245–273. doi:10.1146/annurev-pathmechdis-051122-104528
3. Gilman S, Wenning GK, Low PA, et al. Second consensus statement on the diagnosis of multiple system atrophy. Neurology. 2008;71(9):670–676. doi:10.1212/01.wnl.0000324625.00404.15
4. Neurobiology MFJIro, Agosta F, Sarasso E. Functional MRI in Atypical Parkinsonisms. Int Rev Neurobiol. 2018;142:149–173. doi:10.1016/bs.irn.2018.09.002.
5. Koga S, Sekiya H, Kondru N, et al. Neuropathology and molecular diagnosis of Synucleinopathies. Molecular Neurodegeneration. 2021;16(1):83. doi:10.1186/s13024-021-00501-z
6. Krismer F, Wenning GK. Multiple system atrophy: insights into a rare and debilitating movement disorder. Nat Rev Neurol. 2017;13(4):232–243. doi:10.1038/nrneurol.2017.26
7. Kanuri SH, Sirrkay PJ. Profiling of microglial-originated microvesicles to unearthing their lurking potential as potent foreseeable biomarkers for the diagnosis of Alzheimer’s disease: a systematic review. Brain Circ. 2024;10(3):193–204. doi:10.4103/bc.bc_113_23
8. Bergantin LB. Ca2+/cAMP ratio in age-related diseases. Brain Circ. 2024;10(3):281–282. doi:10.4103/bc.bc_3_24
9. Miki Y, Tsushima E, Foti SC, et al. Identification of multiple system atrophy mimicking Parkinson’s disease or progressive supranuclear palsy. Brain. 2021;144(4):1138–1151. doi:10.1093/brain/awab017
10. Rissardo JP, Vora NM, Tariq I, et al. Unraveling belly dancer’s dyskinesia and other puzzling diagnostic contortions: a narrative literature review. Brain Circ. 2024;10(2):106–118. doi:10.4103/bc.bc_110_23
11. Saeed U, Compagnone J, Aviv RI, et al. Imaging biomarkers in Parkinson’s disease and Parkinsonian syndromes: current and emerging concepts. Translational Neurodegeneration. 2017;6:8. doi:10.1186/s40035-017-0076-6
12. Fanciulli A, Wenning GK. Multiple-system atrophy. New Engl J Med. 2015;372(3):249–263. doi:10.1056/NEJMra1311488
13. Rissardo JP, Caprara ALF. Movement disorders associated with acetylcholinesterase inhibitors in Alzheimer’s dementia: a systematic review. Brain Circ. 2025;11(1):9–23. doi:10.4103/bc.bc_134_24
14. Lin H, Lin L, Xu L, et al. Combined functional and structural imaging of brain white matter reveals stage-dependent impairment in multiple system atrophy of cerebellar type. NPJ Parkinson Dis. 2022;8(1):105. doi:10.1038/s41531-022-00371-2
15. Zhao W, Ye L, Cao L, et al. A bibliometric review of unilateral neglect: trends, frontiers, and frameworks. Brain Circ. 2024;10(2):94–105. doi:10.4103/bc.bc_72_23
16. Wenning GK, Stankovic I, Vignatelli L, et al. The Movement Disorder Society Criteria for the Diagnosis of Multiple System Atrophy. Mov Disord. 2022;37(6):1131–1148. doi:10.1002/mds.29005
17. Pellecchia MT, Stankovic I, Fanciulli A, et al. Can Autonomic Testing and Imaging Contribute to the Early Diagnosis of Multiple System Atrophy? A Systematic Review and Recommendations by the Movement Disorder Society Multiple System Atrophy Study Group. Mov Disord Clin Pract. 2020;7(7):750–762. doi:10.1002/mdc3.13052
18. Rizzo G, Copetti M, Arcuti S, et al. Accuracy of clinical diagnosis of Parkinson disease: a systematic review and meta-analysis. Neurology. 2016;86(6):566–576. doi:10.1212/wnl.0000000000002350
19. Vemuri P, Castillo AM, Thostenson KB, et al. Imaging biomarkers for early multiple system atrophy. Parkinsonism Related Disord. 2022;103:60–68. doi:10.1016/j.parkreldis.2022.08.028
20. Seeley WW, Crawford RK, Zhou J, et al. Neurodegenerative diseases target large-scale human brain networks. Neuron. 2009;62(1):42–52. doi:10.1016/j.neuron.2009.03.024
21. Kim JS, Yang -J-J, Lee D-K, et al. Cognitive Impairment and Its Structural Correlates in the Parkinsonian Subtype of Multiple System Atrophy. Neuro-Degenerative Diseases. 2015;15(5):294–300. doi:10.1159/000430953
22. Gama RL, Távora DG, Bomfim RC, et al. Sleep disturbances and brain MRI morphometry in Parkinson’s disease, multiple system atrophy and progressive supranuclear palsy - a comparative study. Parkinsonism Related Disord. 2010;16(4):275–279. doi:10.1016/j.parkreldis.2010.01.002
23. Tha KK, Terae S, Yabe I, et al. Microstructural white matter abnormalities of multiple system atrophy: in vivo topographic illustration by using diffusion-tensor MR imaging. Radiology. 2010;255(2):563–569. doi:10.1148/radiol.10090988
24. Watanabe H, Saito Y, Terao S, et al. Progression and prognosis in multiple system atrophy: an analysis of 230 Japanese patients. Brain. 2002;125(Pt 5):1070–1083. doi:10.1093/brain/awf117
25. Biswal B, Yetkin FZ, Haughton VM, et al. Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magnetic Resonance in Medicine. 1995;34(4):537–541. doi:10.1002/mrm.1910340409
26. Cohen MS, Bookheimer SY. Localization of brain function using magnetic resonance imaging. Trends Neurosci. 1994;17(7):268–277. doi:10.1016/0166-2236(94)90055-8
27. Logothetis NK. The neural basis of the blood-oxygen-level-dependent functional magnetic resonance imaging signal. Philosophical Transactions of the Royal Society of London Series B. 2002;357(1424):1003–1037. doi:10.1098/rstb.2002.1114
28. Rosskopf J, Gorges M, Müller H-P, et al. Hyperconnective and hypoconnective cortical and subcortical functional networks in multiple system atrophy. Parkinsonism Related Disord. 2018;49:75–80. doi:10.1016/j.parkreldis.2018.01.012
29. Wang N, Edmiston EK, Luo X, et al. Comparing abnormalities of amplitude of low-frequency fluctuations in multiple system atrophy and idiopathic Parkinson’s disease measured with resting-state fMRI. Psychiatry Res Neuroimag. 2017;269:73–81. doi:10.1016/j.pscychresns.2017.09.002
30. Zheng W, Ren S, Zhang H, et al. Spatial Patterns of Decreased Cerebral Blood Flow and Functional Connectivity in Multiple System Atrophy (Cerebellar-Type): a Combined Arterial Spin Labeling Perfusion and Resting State Functional Magnetic Resonance Imaging Study. Front Neurosci. 2019;13:777. doi:10.3389/fnins.2019.00777
31. Zhang H, Ji S, Ren S, et al. Cerebellar Atrophy in Multiple System Atrophy (Cerebellar Type) and Its Implication for Network Connectivity. Cerebellum. 2020;19(5):636–644. doi:10.1007/s12311-020-01144-4
32. Ren S, Zhang H, Zheng W, et al. Altered Functional Connectivity of Cerebello-Cortical Circuit in Multiple System Atrophy (Cerebellar-Type). Front Neurosci. 2018;12:996. doi:10.3389/fnins.2018.00996
33. Caligiore D, Helmich RC, Hallett M, et al. Parkinson’s disease as a system-level disorder. NPJ Parkinson Dis. 2016;2:16025. doi:10.1038/npjparkd.2016.25
34. Wang S, Xiao Y, Hou Y, et al. Comparison of spontaneous brain activity in distinguishing parkinsonian variant of multiple system atrophy from Parkinson’s disease at an early stage. Front Aging Neurosci. 2024;16:1427991. doi:10.3389/fnagi.2024.1427991
35. Rau A, Hosp JA, Rijntjes M, et al. Cerebellar, Not Nigrostriatal Degeneration Impairs Dexterity in Multiple System Atrophy. Movement Disorder. 2024;39(1):130–140. doi:10.1002/mds.29661
36. Yang H, Wang N, Luo X, et al. Altered functional connectivity of dentate nucleus in parkinsonian and cerebellar variants of multiple system atrophy. Brain Imagi Behavior. 2019;13(6):1733–1745. doi:10.1007/s11682-019-00097-5
37. Chen B, He J, Xu M, et al. Automatic classification of MSA subtypes using Whole-brain gray matter function and Structure-Based radiomics approach. Eur J Radiol. 2023;161:110735. doi:10.1016/j.ejrad.2023.110735
38. Bu -L-L, Liu F-T, Jiang C-F, et al. Patterns of dopamine transporter imaging in subtypes of multiple system atrophy. Acta Neurol Scand. 2018;138(2):170–176. doi:10.1111/ane.12932
39. Zheng W, Ge Y, Ren S, et al. Abnormal static and dynamic functional connectivity of resting-state fMRI in multiple system atrophy. Aging. 2020;12(16):16341–16356. doi:10.18632/aging.103676
40. Makawita C, Ananthavarathan P, Silva R, et al. A Systematic Review of the Spectrum and Prevalence of Non-motor Symptoms in Multiple System Atrophy. Cerebellum. 2024. doi:10.1007/s12311-023-01642-1
41. Johnson J. Effect of emotions on learning, memory, and disorders associated with the changes in expression levels: a narrative review. Brain Circ. 2024;10(2):134–144. doi:10.4103/bc.bc_86_23
42. Zhu Y, Simo L, Geng X, et al. Chronic mental stress and ischemic injury: mechanisms and implications - A mini review. Brain Circ. 2025;11(3):171–177. doi:10.4103/bc.bc_88_24
43. Yang HG, Liu WV, Wen Z, et al. Altered voxel-level whole-brain functional connectivity in multiple system atrophy patients with depression symptoms. BMC Psychiatry. 2022;22(1):279. doi:10.1186/s12888-022-03893-4
44. Zhao B, Liu H, Li H, et al. Abnormal functional connectivity of the amygdala is associated with depressive symptoms in patients with multiple system atrophy. Neuropsychiatr Dis Treat. 2018;14:3133–3142. doi:10.2147/ndt.S178657
45. Koga S, Parks A, Uitti RJ, et al. Profile of cognitive impairment and underlying pathology in multiple system atrophy. Mov Disord. 2017;32(3):405–413. doi:10.1002/mds.26874
46. Chang CC, Chang YY, Chang WN, et al. Cognitive deficits in multiple system atrophy correlate with frontal atrophy and disease duration. Eur J Neurol. 2009;16(10):1144–1150. doi:10.1111/j.1468-1331.2009.02661.x
47. Fiorenzato E, Weis L, Seppi K, et al. Brain structural profile of multiple system atrophy patients with cognitive impairment. J Neural Transmission. 2017;124(3):293–302. doi:10.1007/s00702-016-1636-0
48. Lee MJ, Shin J-H, Seoung J-K, et al. Cognitive impairments associated with morphological changes in cortical and subcortical structures in multiple system atrophy of the cerebellar type. Eur J Neurol. 2016;23(1):92–100. doi:10.1111/ene.12796
49. Yang H, Wang N, Luo X, et al. Cerebellar atrophy and its contribution to motor and cognitive performance in multiple system atrophy. NeuroImage Clin. 2019;23:101891. doi:10.1016/j.nicl.2019.101891
50. Zhu X, Zhou Y, Zhong W, et al. Higher Functional Connectivity of Ventral Attention and Visual Network to Maintain Cognitive Performance in White Matter Hyperintensity. Aging Dis. 2023;14(4):1472–1482. doi:10.14336/ad.2022.1206
51. Nasb M, Tao W, Chen N. Alzheimer’s Disease Puzzle: delving into Pathogenesis Hypotheses. Aging Dis. 2024;15(1):43–73. doi:10.14336/ad.2023.0608
52. Li Y, Liu H, Yu H, et al. Alterations of voxel-wise spontaneous activity and corresponding brain functional networks in multiple system atrophy patients with mild cognitive impairment. Human Brain Mapp. 2023;44(2):403–417. doi:10.1002/hbm.26058
53. Kawabata K, Hara K, Watanabe H, et al. Alterations in Cognition-Related Cerebello-Cerebral Networks in Multiple System Atrophy. Cerebellum. 2019;18(4):770–780. doi:10.1007/s12311-019-01031-7
54. Yang H, Luo X, Yu H, et al. Altered resting-state voxel-level whole-brain functional connectivity in multiple system atrophy patients with cognitive impairment. Clin Neurophysiol. 2020;131(1):54–62. doi:10.1016/j.clinph.2019.09.026
55. Habas C. Functional imaging of the deep cerebellar nuclei: a review. Cerebellum. 2010;9(1):22–28. doi:10.1007/s12311-009-0119-3
56. Yang H, Liu WV, Wang S, et al. Freezing of Gait in Multiple System Atrophy. Front Aging Neurosci. 2022;14:833287. doi:10.3389/fnagi.2022.833287
57. Cheng Y, Yang H, Liu WV, et al. Alterations of brain activity in multiple system atrophy patients with freezing of gait: a resting-state fMRI study. Front Neurosci. 2022;16:954332. doi:10.3389/fnins.2022.954332
58. Zhao M, Pang H, Li X, et al. Low and high-order topological disruption of functional networks in multiple system atrophy with freezing of gait: a resting-state study. Neurobiol Dis. 2024;195:106504. doi:10.1016/j.nbd.2024.106504
59. Beissner F, Meissner K, Bär K-J, et al. The autonomic brain: an activation likelihood estimation meta-analysis for central processing of autonomic function. J Neurosci. 2013;33(25):10503–10511. doi:10.1523/jneurosci.1103-13.2013
60. Lyu H, Zhu X, He N, et al. Alterations in Resting-State MR Functional Connectivity of the Central Autonomic Network in Multiple System Atrophy and Relationship with Disease Severity. J Magnetic Resonance Iimag. 2023;58(5):1472–1487. doi:10.1002/jmri.28693
61. Lee R, Shin JH, Choi H, et al. Variability of FP-CIT PET Patterns Associated With Clinical Features of Multiple System Atrophy. Neurology. 2021;96(12):e1663–e1671. doi:10.1212/wnl.0000000000011634
62. Wada T, Sugaya K, Asano Y, et al. Association of dysphagia severity in multiple system atrophy with the specific binding ratio on dopamine transporter SPECT. J Neurol Sci. 2024;463:123116. doi:10.1016/j.jns.2024.123116
63. Hughes AJ, Daniel SE, Ben-Shlomo Y, et al. The accuracy of diagnosis of parkinsonian syndromes in a specialist movement disorder service. Brain. 2002;125(Pt 4):861–870. doi:10.1093/brain/awf080
64. Koga S, Aoki N, Uitti RJ, et al. When DLB, PD, and PSP masquerade as MSA: an autopsy study of 134 patients. Neurology. 2015;85(5):404–412. doi:10.1212/wnl.0000000000001807
65. Schrag A, Ben-Shlomo Y, Quinn N. How valid is the clinical diagnosis of Parkinson’s disease in the community? J Neurol Neurosurg. 2002;73(5):529–534. doi:10.1136/jnnp.73.5.529
66. Stefanova N, Bücke P, Duerr S, et al. Multiple system atrophy: an update. Lancet Neurol. 2009;8(12):1172–1178. doi:10.1016/s1474-4422(09)70288-1
67. Franciotti R, Pizzi SD, Perfetti B, et al. Default mode network links to visual hallucinations: a comparison between Parkinson’s disease and multiple system atrophy. Mov Disord. 2015;30(9):1237–1247. doi:10.1002/mds.26285
68. Yao Q, Zhu D, Li F, et al. Altered Functional and Causal Connectivity of Cerebello-Cortical Circuits between Multiple System Atrophy (Parkinsonian Type) and Parkinson’s Disease. Front Aging Neurosci. 2017;9:266. doi:10.3389/fnagi.2017.00266
69. Baggio HC, Abos A, Segura B, et al. Cerebellar resting-state functional connectivity in Parkinson’s disease and multiple system atrophy: characterization of abnormalities and potential for differential diagnosis at the single-patient level. NeuroImage Clin. 2019;22:101720. doi:10.1016/j.nicl.2019.101720
70. Wang N, Zhang L, Yang H, et al. Similarities and differences in cerebellar grey matter volume and disrupted functional connectivity in idiopathic Parkinson’s disease and multiple system atrophy. Neuropsychologia. 2019;124:125–132. doi:10.1016/j.neuropsychologia.2018.12.019
71. Sako W, Abe T, Furukawa T, et al. Differences in the intra-cerebellar connections and graph theoretical measures between Parkinson’s disease and multiple system atrophy. J Neurol Sci. 2019;400:129–134. doi:10.1016/j.jns.2019.03.022
72. Kadota K, Onoda K, Abe S, et al. Multiscale Entropy of Resting-State Functional Magnetic Resonance Imaging Differentiates Progressive Supranuclear Palsy and Multiple System Atrophy. Life. 2021;11(12):1411. doi:10.3390/life11121411
73. Pang H, Yu Z, Yu H, et al. Multimodal striatal neuromarkers in distinguishing parkinsonian variant of multiple system atrophy from idiopathic Parkinson’s disease. CNS Neurosc Ther. 2022;28(12):2172–2182. doi:10.1111/cns.13959
74. Chen B, Cui W, Wang S, et al. Functional connectome automatically differentiates multiple system atrophy (parkinsonian type) from idiopathic Parkinson’s disease at early stages. Human Brain Mapp. 2023;44(6):2176–2190. doi:10.1002/hbm.26201
75. Litvan I, Bhatia KP, Burn DJ, et al. Movement Disorders Society Scientific Issues Committee report: SIC Task Force appraisal of clinical diagnostic criteria for Parkinsonian disorders. Mov Disord. 2003;18(5):467–486. doi:10.1002/mds.10459
76. Vaillancourt DE, Barmpoutis A, Wu SS, et al. Automated Imaging Differentiation for Parkinsonism. JAMA Neurol. 2025;82(5):495–505. doi:10.1001/jamaneurol.2025.0112
77. Group GPsG.Hopfner F, Höglinger G, et al. Definition and diagnosis of Parkinson’s disease: guideline “Parkinson’s disease” of the German Society of Neurology. J Neurol. 2024;271(11):7102–7119. doi:10.1007/s00415-024-12687-5.
78. Chou Y-H, You H, Wang H, et al. Effect of Repetitive Transcranial Magnetic Stimulation on fMRI Resting-State Connectivity in Multiple System Atrophy. Brain Connect. 2015;5(7):451–459. doi:10.1089/brain.2014.0325
79. Liu Z, Ma H, Poole V, et al. Effects of Multi-Session Repetitive Transcranial Magnetic Stimulation on Motor Control and Spontaneous Brain Activity in Multiple System Atrophy: a Pilot Study. Front Behav Neurosci. 2018;12:90. doi:10.3389/fnbeh.2018.00090
80. Bai J, Bai Y, Li X, et al. A multi-center, randomized, double-blind, sham-stimulation controlled study of transcranial magnetic stimulation with precision navigation for the treatment of multiple system atrophy. Trials. 2024;25(1):640. doi:10.1186/s13063-024-08458-2
81. Planetta PJ, Kurani AS, Shukla P, et al. Distinct functional and macrostructural brain changes in Parkinson’s disease and multiple system atrophy. Human Brain Mapp. 2015;36(3):1165–1179. doi:10.1002/hbm.22694
82. Burciu RG, Chung JW, Shukla P, et al. Functional MRI of disease progression in Parkinson disease and atypical parkinsonian syndromes. Neurology. 2016;87(7):709–717. doi:10.1212/wnl.0000000000002985
83. Braak H, Tredici KD, Rüb U, et al. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24(2):197–211. doi:10.1016/s0197-4580(02)00065-9
84. Wenning GK, Colosimo C, Geser F, et al. Multiple system atrophy. Lancet Neurol. 2004;3(2):93–103. doi:10.1016/s1474-4422(03)00662-8
85. Hauw JJ, Daniel SE, Dickson D, et al. Preliminary NINDS neuropathologic criteria for Steele-Richardson-Olszewski syndrome (progressive supranuclear palsy). Neurology. 1994;44(11):2015–2019. doi:10.1212/wnl.44.11.2015
86. Zubair AS. Utilization of wearable technology to track functional changes in a patient with myopathy. Brain Circ. 2024;10(2):190–191. doi:10.4103/bc.bc_104_23
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Morin Mitigates Methamphetamine-Induced Neurotoxicity: Effects on Motor and Cognitive Function
Anyanwu GE, Umeano AV, Ojiakor VO, Katchy AU, Anyanwu CN, Fakorede S
Journal of Experimental Pharmacology 2025, 17:307-321
Published Date: 11 June 2025