Back to Journals » Clinical Interventions in Aging » Volume 18
Functional Connectivity and Anxiety Improvement After Subthalamic Nucleus Deep Brain Stimulation in Parkinson’s Disease
Authors Chang B, Mei J, Ni C, Niu C
Received 23 May 2023
Accepted for publication 23 August 2023
Published 29 August 2023 Volume 2023:18 Pages 1437—1445
DOI https://doi.org/10.2147/CIA.S422605
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Bowen Chang,1,2,* Jiaming Mei,1,2,* Chen Ni,1,2 Chaoshi Niu1,2
1Department of Neurosurgery, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, People’s Republic of China; 2Anhui Province Key Laboratory of Brain Function and Brain Disease, Hefei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chaoshi Niu, Email [email protected]
Background: Anxiety is one of the most common and disturbing non-motor symptoms of Parkinson’s disease (PD). However, few studies have explored the relationship between functional connectivity (FC) and the rate of anxiety improvement after subthalamic nucleus deep brain stimulation (STN-DBS). Therefore, in this study, we aimed to explore the correlation between FC and the rate of anxiety improvement in patients with PD who underwent STN-DBS.
Methods: The resting-state functional magnetic resonance imaging (rs-fMRI) data of 62 patients with anxious PD (aPD), 68 patients with PD without anxiety (naPD), and 64 healthy controls (HCs) were analyzed according to FC. Intergroup comparison and correlation analyses of anxiety improvement rates were performed.
Results: The HC, aPD and naPD groups of zFCs were then used for the ANOVA test, and the results were FDR-corrected. There were 24 significant differences in FCs between the three groups. Post tests were conducted between groups found that 15 significantly different FCs were observed between the naPD and aPD groups. In addition, the two FCs in patients with aPD were significantly correlated with the rate of improvement in anxiety.
Conclusion: We found that the two FCs in patients with aPD (olfactory cortex and inferior frontal gyrus [IFG] pars orbitalis; inferior temporal gyrus and posterior orbital gyrus) were significantly correlated with the rate of improvement in anxiety. Our study may help us understand the underlying mechanisms by which STN-DBS improves anxiety in PD patients and identify more effective treatment strategies.
Keywords: Parkinson’s disease, deep brain stimulation, anxiety, functional connectivity, fMRI
Introduction
Parkinson’s disease (PD) is a progressive degenerative neurological disease that occurs in elderly individuals and has a higher incidence in men than in women. Resting tremor, bradykinesia, and rigidity are the common motor symptoms of patients with most PD.1 In addition, a variety of non-motor symptoms (NMS), such as mood disorders, cognitive impairments, sleep disorders, and autonomic dysfunction, may be observed.2,3 Anxiety is one of the most common NMS of PD. Its prevalence among patients with PD is 31%, which is higher than that in patients with community or other diseases. It has shown to be a common worsening factor of the disease and is associated with a lower quality of life.4–6 With the recent development of neuromodulation therapy, deep brain stimulation (DBS) has become an effective treatment for advanced PD.7,8 It is widely suggested that DBS can significantly improve anxiety and depression in patients with PD, but the mechanism remains unclear.9,10
Although functional magnetic resonance imaging (fMRI) has been developed in recent years, there is an increasing sophistication in the use of functional imaging to study the neural circuitry of brain diseases. However, the exact causal brain network mechanisms by which DBS affects anxiety in PD patients are not known due to the safety and biosafety issues associated with high field strength MRI scanning of DBS equipment in the powered-on state.
Therefore, we used preoperative resting-state fMRI to explore the functional connectivity (FC) of patients with PD to provide some imaging evidence for revealing the mechanism of subthalamic nucleus DBS (STN-DBS) in improving motor symptoms in PD.11,12 Similarly, it is critical to study FC associated with anxiety improvement rates in post-DBS patients with PD. This will help us understand the underlying mechanism and identify more effective treatment strategies. Therefore, in this study, we aimed to explore the correlation between FC and the rate of anxiety improvement in patients with PD who underwent STN-DBS.
Materials and Methods
Patients
Medical records and questionnaire results were retrospectively collected from patients with PD who underwent STN-DBS at the First Hospital of the University of Science and Technology of China between September 2019 and April 2020. The study protocol was approved by the ethics committee of our hospital (2022-RE-154). The included patients had intermediate-to-advanced PD, and the exclusion criteria were moderate/severe cognitive impairment, persistent severe psychiatric disorders, severe atrophy or diffuse ischemic lesions on MRI, or systemic diseases that prevented surgery. None of the included subjects used any anxiolytic drugs. Moreover, the medical records of age- and sex-matched healthy participants who underwent annual physical checkups at the same hospital were collected as healthy controls (HCs).
Acquisition Clinical Assessment
Patients with anxiety-associated PD were diagnosed by an experienced psychiatrist according to the criteria of the Fifth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-V). Anxiety severity was measured using the 14 Hamilton Anxiety Assessment Scale (HAMA-14). An HAMA-14 score higher than 14 is necessary for a more accurate diagnosis of PD anxiety. PD patients were considered to have anxiety disorders when their HAMA-14 score was higher than 14. Exercise symptoms and disease severity were evaluated using the Movement Section of the Unified Parkinson’s Disease Scale (UPDRS-III) and Hoehn and Yahr (H&Y) scale. All evaluations were performed before the MRI scan. Patients still use the HAMA-14 scale 2 years after surgery to evaluate anxiety and then calculate the rate of anxiety improvement (Improvement rate of HAMA-14 = (HAMA-14 Preop – HAMA-14 Postop)/HAMA-14 Preop). H&Y stage and HAMA-14 were measured in the medication state.
MRI Data and Preprocessing
For patients with PD and HCs, a 3T MRI scanner (Discovery MR750; General Electric Healthcare, Chicago, IL, USA) with an eight-channel phased-array head coil was used. Participants were instructed not to fall asleep during the entire scan. We further confirmed that the participants were awake throughout the scan. Functional and structural MRI data were acquired with a 3T GE (Achieva TX) MRI scanner in the OFF-medication state before DBS surgery, following an 8-h period of medication withdrawal. Structural images were acquired using a sagittal magnetization prepared rapid gradient echo three-dimensional T1-weighted sequence (repetition time [TR] = 8.5 ms, echo time [TE] = 3.2 ms, inversion time [TI] = 450 ms, flip angle [FA] = 12°). Functional MRI images were obtained using the following spin echo–echo planar imaging (SE-EPI) sequence: TR = 2000 ms, TR = 30 ms, slice thickness/gap = 3.6/0 mm, axial slices = 38 layers, FA = 90°, field of view (FOV) = 256 × 256 mm, matrix size = 64 × 64, and scanning time = 484 s.
Data preprocessing was conducted using a Resting-State fMRI Data Analysis Toolkit plus V1.25 (RESTplus V1.25, http://restfmri.net/forum/index.php), which is based on Statistical Parametric Mapping (SPM, https://www.fil.ion.ucl.ac.uk/spm/). Data from 242 volumes were acquired separately as functional scans of patients with PD and HCs. The first 10 volumes of each functional scan were excluded to correct for subject habituation to the scanning environment and magnetization stability. Slice-timing correction was performed to help compensate for differences in acquiring data across all slices with the FOV at any given time point; realignment for head‐motion correction was also considered; data from healthy control/PD subject whose head motion exceeded 3.0 mm or involved rotation exceeding 3.0° during the fMRI scanning was excluded. Individual 3D T1-weighted anatomical images were coregistered to functional images and spatially normalized to the Montreal Neurological Institute template. Each voxel was resampled to 3 × 3 × 3 mm3. Subsequently, the resampled images were smoothed using a 6-mm full-width half-maximum (FWHM) isotropic Gaussian kernel, and a linear trend and bandpass filter (0.01 ~ 0.08 Hz) were used to remove the effect of high-frequency noise. Finally, cerebrospinal fluid signal, white matter, and the Friston-24 head motion parameter model were considered nuisance covariates and regressed from fMRI signals. The resulting data were further analyzed.
Functional Connectivity Analysis Based on Regions of Interest
In this study, each region of interest (ROI) in the AAL3-170 Atlas was extracted as a candidate feature. The AAL3-170 Atlas (www.oxcns.org/aal3.html, accessed June 4, 2022) is an improved version of the AAL2 Atlas that divides the entire brain into 166 ROIs. Two small areas of the AAL3 Atlas (Nos. 133–134) were not defined, as the size of the original 1 × 1 × 1 m3 was resampled to 3 × 3 × 3 m3; therefore, 164 areas remained in the AAL3-170 Atlas. Using these 164 ROIs, we calculated the ROI-wise FC with filtered data and obtained one FC graph each. The FC graph went through Fisher z transformation; we made the data fit normal analysis, obtained the zFC graph, and used the zFC graph for subsequent statistical analysis. The average resting state blood oxygenation level-dependent (BOLD) time series for each ROI was extracted. The BOLD time series for each ROI was then correlated with the BOLD time series of every other ROI (Pearson’s correlation coefficient) for each participant. In calculating FC, we adjusted for sex, age, H-Y classification, and duration variables.
Statistical Analyses
According to the demographic data and the HAMA-14 scale, the participants were classified into three groups: HC, anxiety PD (aPD), and non-anxiety PD (naPD). The groups were tested using one-way analysis of variance (ANOVA) test was performed to compare the FC differences among the HC, aPD and naPD groups (a post hoc test with the post hoc two sample t-tests were used to compare FC between each pair of groups two comparisons was also performed on an ANOVA basis). The All intergroup multiple comparison correction comparisons of all intergroup were performed by using false discovery rate (FDR) correction (q<0.01, q = 0.01). Pearson’s correlation coefficient was used to analyze the correlation between FC and anxiety improvement rates with a significance level of P < 0.05. Multivariate regression was used to analyse the risk factors.
Results
Demographic and Clinical Characteristics
A total of 68 patients with naPD, 62 patients with aPD, and 64 HCs were included in our analysis. The differences in age, gender, and duration among the three groups were not statistically significant. Differences between the aPD and naPD groups were not statistically significant for UPDRS-III scores, H-Y grades, or levodopa equivalent dose (LED). In addition, the HAMA-14 scores were significantly higher in patients with aPD than in those with naPD or HCs. The improvement rate of anxiety in aPD group was significantly higher than that in naPD group (Table 1).
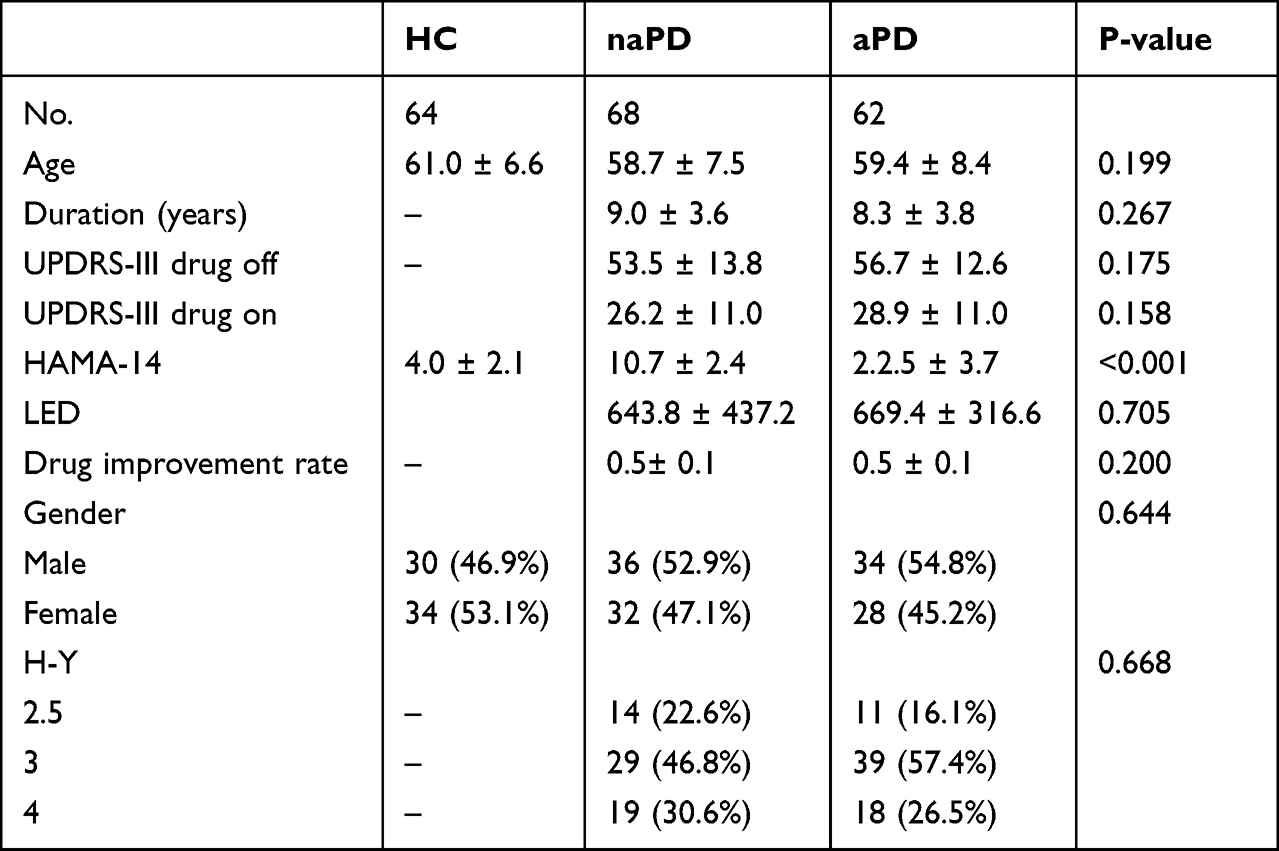 |
Table 1 Demographic and Clinical Information of the Participants |
Functional Connectivity Analysis
The zFC matrix was calculated for each participant by determining the functional connectivity values of the ROIs. Three groups of zFCs were then used for the one-way ANOVA test, and the results were FDR-corrected. A matrix of FCs among the three groups was obtained. Twenty-four ROI-pair FCs (excluding redundant and diagonal elements) in the triangular portion of the matrix were preserved (Figure 1A and Table 2). Significant differences in FCs among the aPD, naPD, and HC groups are shown in Figure 1B. A post hoc test was conducted to compare groups, and we found 15 significantly different FCs between the naPD and aPD groups (Figure 2A and Table 3). Significantly different FCs between the HC and aPD groups are shown in Figure 2B.
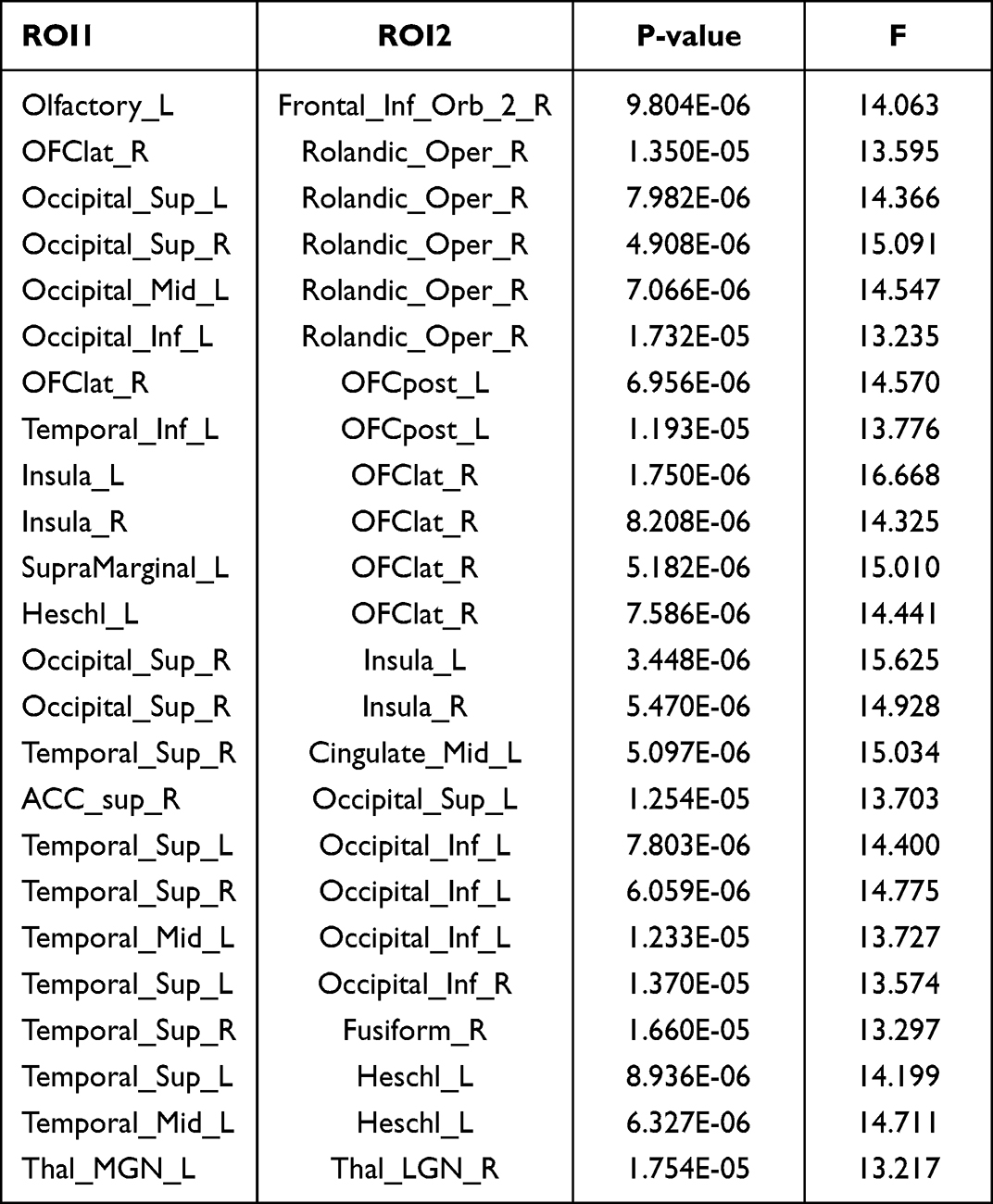 |
Table 2 Significant Differences in FC Between HC, aPD, and naPD Groups |
 |
Table 3 Significant Differences in FC Between aPD, and naPD Groups |
 |
Figure 1 Significant differences in FCs among the aPD, naPD, and HC groups. (A) T-value matrix of functional connectivity between the three groups. (B) Visualization of differential functional connectivity. |
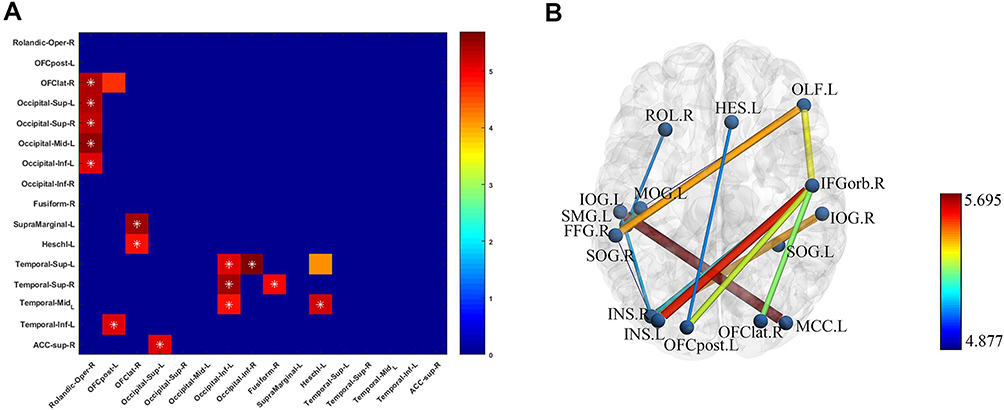 |
Figure 2 Significantly different FCs between the naPD and aPD groups. (A) T-value matrix of functional connectivity between the two groups. (B) Visualization of differential functional connectivity. |
Relationship Between Functional Connectivity and Anxiety Improvement Rate After STN-DBS
In FC with significant differences between naPD and aPD groups, we found that the correlation between the two FCs (Olfactory_L, Frontal_Inf_Orb_2_R; Temporal_Inf_L, OFCpost_L) in the aPD group and the HAMA score improvement rate was significant (Figure 3). We then used multivariate regression model to validate the effect of the two FCs mentioned above on the rate of improvement in HAMA scores. After adjusting for several variables, these two FCs still had a strong effect on the rate of improvement in anxiety in PD patients after STN-DBS (Table 4).
 |
Table 4 Multivariate Regression for Effect of FC on the HAMA Improvement Rate After STN-DBS |
 |
Figure 3 Correlation between FC and anxiety improvement rate after STN-DBS. (A) inferior temporal gyrus and posterior orbital gyrus. (B) Olfactory cortex and inferior frontal gyrus [IFG] pars orbitalis close. |
Discussion
Anxiety is a common NMS of PD that is associated with awakening, reduced visual processing, negative cognition, somatosensory symptoms, and autonomic manifestations.4,13,14 Despite some differences, these manifestations share common neurological abnormalities, mainly characterized by hyperactivation of the amygdala and brain islands and pathological changes in FC.15 In the general population, the current hypothesis is that anxiety results from top-down control impairment of the medial prefrontal cortex (mPFC) in the amygdala, resulting in increased activity and affecting the downstream cortical/subcortical region.16,17
Thus far, it is unclear whether anxiety in people with PD has the same underlying mechanism as that described in the general population.18 Clinically, anxiety may occur at any stage of the disease, even before motor symptoms. Anxiety in patients with PD is often associated with gait disorders, unstable posture, and freezing gait.19,20 Preliminary studies have revealed impaired connectivity of the amygdala with the basal ganglia, supplementary motor regions (SMA), and other frontal regions in patients with PD.21,22 In our study, between the aPD and naPD groups, we found 15 distinct FCs among the occipital cortex and the rolandic operculum, olfactory and frontal cortex, temporal lobe and occipital cortex, orbital gyrus and superior marginal gyrus, and orbital gyrus and temporal cortex. This is similar to previous findings indicating anxiety in patients with aPD is mainly due to abnormal FC between the limbic system and other brain regions.
This study not only investigated FC differences in HC, naPD, and aPD groups but also explored the correlation of these FCs with the improvement rate of anxiety after STN-DBS. We observed no FCs in the naPD group that were significantly associated with anxiety improvement rates, whereas the two FCs in the aPD group were closely associated with anxiety improvement rates.
Numerous studies have shown that STN-DBS improves anxiety in patients with PD. In a 15-month follow-up study that included 33 patients, anxiety symptoms significantly improved after DBS.23 Similarly, a definitive study published in 2008 included 156 patients with DBS and PD; 123 patients completed multiple NMS scores, showing anxiety symptoms improved after DBS.24 The present study shows several possible reasons for improvement in the mechanism of anxiety. The first is intervention in STN-mediated fear processing, the second is intervention in marginal system loops near the STN, and the third is indirect regulation of the dopamine metabolism.25 In this study, we found significant negative correlations between the anxiety improvement rate and FCs of the olfactory cortex and inferior frontal gyrus (IFG) pars orbitalis and the inferior temporal gyrus and posterior orbital gyrus in the aPD group. These results indicate that these two FCs may affect the anxiety improvement rate of patients with aPD after STN-DBS.
In recent years, it has been found that the abnormal structure and function of prefrontal cortex (PFC), amygdala hippocampal loop play an important role in excessive anxiety, each structure plays a unique role in different emotional components, and PFC and hippocampus are key parts regulating positive and negative emotions.26 The PFC is an important part of the emotional central pathway, its function consists of different components, such as the dorsolateral prefrontal cortex (DLPFC), the medial prefrontal lobe (MPFC) and orbitofrontal cortex (OFC), each of which plays different roles in emotional processing. An fMRI-based study showed that social anxiety was positively correlated with cortical gray matter volume of OFC and functional connectivity of OFC-amygdala, indicating that the abnormal structure of OFC and its abnormal connection with amygdala were the neural basis of social anxiety.27 Similarly, a study on cortical morphology in patients with generalized anxiety disorder (GAD) found that bilateral OFC cortical thickness was significantly reduced in GAD patients compared with healthy controls.28 In conclusion, the abnormal structure and function of OFC are the important neural basis of anxiety. In PD patients, previous studies have found that anxiety is associated with changes in the fear loop. In the fear loop of aPD patients, functional connections between amygdala, OFC and hippocampus are increased, while functional connections between MPFC and OFC are decreased.29
Studies have shown that there is a close relationship between the stimulation contact and the location of STN subregion and the stimulation effect after electrode implantation in nuclear mass, that is, different subregions of STN correspond to different stimulation effects.30 STN can be divided into three functional territory: dorsolateral sensorimotor territory, intermediate associative territory and ventromedial limbic territory. Studies have shown that STN, as one of the components of the basal ganglia, plays an important role in the mediation of motor, cognitive and emotional behaviors, and is the link that integrates motor, cognitive and emotional behaviors. Information from the anterior cingulate cortex (ACC), OFC, and hippocampus is transmitted to the STN limbic territory.31
It has been confirmed that patients can obtain the best relief of motor symptoms when stimulating the dorsolateral sensorimotor territory of STN. In terms of emotion, studies based on the neuroanatomy of STN show that the ventral or ventral STN is closely related to afferent and efferent fibers in the limbic territory. Therefore, studies have shown that stimulation of more ventral STN may cause transient manic symptoms, but in the long term, anxiety and depression can be improved better than that of dorsal and intermediate territory.32,33 It can be seen that DBS stimulation of different subregions of STN has different effects on anxiety in PD patients. At the neuroanatomical level, the OFC projects to the middle part of the STN and extends to the lateral hypothalamus. Because of this anatomical connection, STN is also one of the commonly used stimulus targets in the treatment of DBS for obsessive-compulsive disorder. The cortex-thalamic-basal ganglia network consists of a complex set of periodic excitatory and inhibitory loop systems. As a regulatory target of obsessive-compulsive disorder, STN mainly affects circuits related to reward, avoidance and cognitive control in this network, mainly FC of OFC.34 This suggests that regulation of OFC-related brain networks can affect the emotional activity of patients. In conclusion, STN-DBS may regulate anxiety in aPD patients through OFC-related FCs.
There are several new aspects of our research. First, this study is one of few to explore the FC associated with the improvement rate of anxiety after STN-DBS. In addition, we explored the relationship between FC and anxiety improvement rates in patients with PD with different states of anxiety. Our results provide evidence for the mechanisms by which STN-DBS improves anxiety in patients with PD. With the development of DBS devices, we can obtain 3T rs-fMRI images in the DBS power-on state, which will help to further explain the mechanism of anxiety improvement.
The present study had several limitations. First, it was retrospective and lacked reproducibility analysis (testing the same individual under the same conditions at two different time points). This may be a potential confounder of unknown significance. Moreover, the required sample size and statistical efficacy were not estimated at this time due to the study’s retrospective nature, and predictive analyses were performed after the collection of follow-up information. We did not collect postoperative fMRI data because of possible artifacts and MRI heating of the implant. Therefore, for safety reasons, we recommend performing long-term follow-up prior to postoperative data collection.
Conclusion
In this study, we explored the correlation between FC and the rate of anxiety improvement after STN-DBS in patients with PD. We found that the two FCs in patients with aPD (olfactory cortex and IFG pars orbitalis; inferior temporal gyrus and posterior orbital gyrus) were significantly correlated with the rate of improvement in anxiety. Our study may help us understand the underlying mechanisms by which STN-DBS improves anxiety in PD patients and identify more effective treatment strategies.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the First Affiliated Hospital of USTC. Confidentiality of patient data and adherence to the Declaration of Helsinki were maintained. The patients/participants provided their written informed consent to participate in this study.
Disclosure
Bowen Chang and Jiaming Mei are co-first authors for this study. The authors report no conflicts of interest concerning the materials or methods used in this study or the findings specified in this paper.
References
1. Jankovic J. Parkinson’s disease: clinical features and diagnosis. J Neurol Neurosurg Psychiatry. 2008;79(4):368–376. doi:10.1136/jnnp.2007.131045
2. Chang B, Ni C, Mei J, et al. Nomogram for predicting depression improvement after deep brain stimulation for Parkinson’s disease. Brain Sci. 2022;12(7):841. doi:10.3390/brainsci12070841
3. Chang B, Ni C, Zhang W, et al. Nomogram to predict cognitive state improvement after deep brain stimulation for Parkinson’s disease. Brain Sci. 2022;12(6):759. doi:10.3390/brainsci12060759
4. Broen MPG, Narayen NE, Kuijf ML, Dissanayaka NNW, Leentjens AFG. Prevalence of anxiety in Parkinson’s disease: a systematic review and meta-analysis. Mov Disord. 2016;31:1125–1133.
5. Pontone GM, Williams JR, Anderson KE, et al. Anxiety and selfperceived health status in Parkinson’s disease. Parkinsonism Relat Disord. 2011;17:249–254. doi:10.1016/j.parkreldis.2011.01.005
6. Leentjens AFG, Dujardin K, Marsh L, Martinez-Martin P, Richard IH, Starkstein SE. Symptomatology and markers of anxiety disorders in Parkinson’s disease: a cross-sectional study. Mov Disord. 2011;26:484–492. doi:10.1002/mds.23528
7. Chang B, Mei J, Xiong C, Chen P, Jiang M, Niu C. Bilateral globus pallidus interna combined with subthalamic nucleus variable frequency deep brain stimulation in the treatment of young-onset Parkinson’s disease with refractory dyskinesia: a case report. Front Neurosci. 2021;15:782046.
8. Mei J, Chang B, Xiong C, Jiang M, Niu C. A New application of functional zonal image reconstruction in programming for Parkinson’s disease treated using subthalamic nucleus-deep brain stimulation. Front Neurol. 2022;13:916658. doi:10.3389/fneur.2022.916658
9. Cartmill T, Skvarc D, Bittar R, McGillivray J, Berk M, Byrne LK. Deep brain stimulation of the subthalamic nucleus in Parkinson’s disease: a meta-analysis of mood effects. Neuropsychol Rev. 2021;31(3):385–401.
10. Couto MI, Monteiro A, Oliveira A, Lunet N, Massano J. Depression and anxiety following deep brain stimulation in Parkinson’s disease: systematic review and meta-analysis. Acta Med Port. 2014;27(3):372–382. doi:10.20344/amp.4928
11. Horn A, Reich M, Vorwerk J, et al. Connectivity predicts deep brain stimulation outcome in Parkinson disease. Ann Neurol. 2017;82(1):67–78. doi:10.1002/ana.24974
12. Bai Y, Diao Y, Gan L, et al. Deep brain stimulation modulates multiple abnormal resting-state network connectivity in patients with Parkinson’s disease. Front Aging Neurosci. 2022;14:794987. doi:10.3389/fnagi.2022.794987
13. Coakeley S, Martens KE, Almeida QJ. Management of anxiety and motor symptoms in Parkinson’s disease. Expert Rev Neurother. 2014;14(8):937–946. doi:10.1586/14737175.2014.936388
14. Peterson A, Thome J, Frewen P, Lanius RA. Resting-state neuroimaging studies: a new way of identifying differences and similarities among the anxiety disorders? Can J Psychiatry. 2014;59(6):294–300. doi:10.1177/070674371405900602
15. Etkin A, Wager TD. Functional neuroimaging of anxiety: a meta-analysis of emotional processing in PTSD, social anxiety disorder, and specific phobia. Am J Psychiatry. 2007;164(10):1476–1488. doi:10.1176/appi.ajp.2007.07030504
16. He Y, Ting X, Zhang W, Zuo X-N. Lifespan anxiety is reflected in human amygdala cortical connectivity. Hum Brain Mapp. 2016;37(3):1178–1193. doi:10.1002/hbm.23094
17. Justin Kim M, Gee DG, Loucks RA, Caroline Davis F, Whalen PJ. Anxiety dissociates dorsal and ventral medial prefrontal cortex functional connectivity with the amygdala at rest. Cereb Cortex. 2011;21(7):1667–1673. doi:10.1093/cercor/bhq237
18. Prediger RD, Matheus FC, Schwarzbold ML, Lima MM, Vital MA. Anxiety in Parkinson’s disease: a critical review of experimental and clinical studies. Neuropharmacology. 2012;62(1):115–124. doi:10.1016/j.neuropharm.2011.08.039
19. Lintel H, Corpuz T, Paracha SU, Grossberg GT. Mood disorders and anxiety in Parkinson’s disease: current concepts. J Geriatr Psychiatry Neurol. 2021;34(4):280–288. doi:10.1177/08919887211018267
20. de Faria SM, de Morais Fabrício D, Tumas V, et al. Effects of acute cannabidiol administration on anxiety and tremors induced by a simulated public speaking test in patients with Parkinson’s disease. J Psychopharmacol. 2020;34(2):189–196. doi:10.1177/0269881119895536
21. Yu R, Liu B, Wang L, Chen J, Liu X. Enhanced functional connectivity between putamen and supplementary motor area in Parkinson’s disease patients. PLoS One. 2013;8(3):e59717. doi:10.1371/journal.pone.0059717
22. Hu X, Song X, Yuan Y, et al. Abnormal functional connectivity of the amygdala is associated with depression in Parkinson’s disease. Mov Disord. 2015;30(2):238–244. doi:10.1002/mds.26087
23. Soulas T, Sultan S, Gurruchaga J-M, Palfi S, Fénelon G. Depression and coping as predictors of change after deep brain stimulation in Parkinson’s disease. World Neurosurg. 2011;75(3–4):525–532. doi:10.1016/j.wneu.2010.06.015
24. Witt K, Daniels C, Reiff J, et al. Neuropsychological and psychiatric changes after deep brain stimulation for Parkinson’s disease: a randomised, multicentre study. Lancet Neurol. 2008;7(7):605–614. doi:10.1016/S1474-4422(08)70114-5
25. Wolz M, Hauschild J, Koy J, et al. Immediate effects of deep brain stimulation of the subthalamic nucleus on nonmotor symptoms in Parkinson’s disease. Parkinsonism Relat Disord. 2012;18(8):994–997. doi:10.1016/j.parkreldis.2012.05.011
26. Liu WZ, Huang SH, Wang Y, et al. Medial prefrontal cortex input to basolateral amygdala controls acute stress-induced short-term anxiety-like behavior in mice. Neuropsychopharmacol. 2022;2022:1–11.
27. Mao Y, Zuo XN, Ding C, Qiu J. OFC and its connectivity with amygdala as predictors for future social anxiety in adolescents. Dev Cogn Neurosci. 2020;44:100804. doi:10.1016/j.dcn.2020.100804
28. Zhang T, Xie X, Li Q, et al. Hypogyrification in generalized anxiety disorder and associated with insomnia symptoms. Nat Sci Sleep. 2022;14:1009–1019. doi:10.2147/NSS.S358763
29. Carey G, Görmezoğlu M, de Jong JJA, et al. Neuroimaging of anxiety in Parkinson’s disease: a systematic review. Mov Disord. 2021;36(2):327–339. doi:10.1002/mds.28404
30. Kähkölä J, Lahtinen M, Keinänen T, Katisko J. Stimulation of the presupplementary motor area cluster of the subthalamic nucleus predicts more consistent clinical outcomes. Neurosurgery. 2022;2022:2292.
31. van Wouwe NC, Neimat JS, van den Wildenberg WPM, et al. Subthalamic nucleus subregion stimulation modulates inhibitory control. Cereb Cortex Commun. 2020;1(1):tgaa083.
32. Petry-Schmelzer JN, Krause M, Dembek TA, et al. Non-motor outcomes depend on location of neurostimulation in Parkinson’s disease. Brain. 2019;142(11):3592–604.24.
33. Dafsari HS, Petry-Schmelzer JN, Ray-Chaudhuri K, et al. Non-motor outcomes of subthalamic stimulation in Parkinson’s disease depend on location of active contacts. Brain Stimul. 2018;11(4):904–912.
34. Haber SN, Yendiki A, Jbabdi S. Four deep brain stimulation targets for obsessive-compulsive disorder: are they different? Biol Psychiatry. 2021;90(10):667–677.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Detection Analysis of Perioperative Plasma and CSF Reveals Risk Biomarkers of Postoperative Delirium of Parkinson’s Disease Patients Undergoing Deep Brain Stimulation of the Subthalamic Nuclei
Zhou Y, Ma Y, Yu C, Chen Y, Ding J, Yu J, Zhou R, Wang X, Fan T, Shi C
Clinical Interventions in Aging 2022, 17:1739-1749
Published Date: 30 November 2022
The Two Sides of Placebo Analgesia: Differential Functional Connectivity Reveals Mechanisms of Placebo Analgesic Response
Bush NJ, Cushnie AK, Boissoneault J, Aghabeigi S, Alexander C, Staud R, Robinson ME
Journal of Pain Research 2025, 18:189-201
Published Date: 10 January 2025
Updates on Parkinson’s Disease
Bai H, Ma W, Zhu L, Lu Y, Fan J, Chen M, Huang C
Neuropsychiatric Disease and Treatment 2025, 21:1945-1953
Published Date: 4 September 2025
Long-Term Surgical Outcomes and Influential Factors of Subthalamic Nucleus Deep Brain Stimulation for Dyskinesia in Parkinson’s Disease: A 3-Year Longitudinal Cohort Study
Wang S, Xue T, Ma R, Shi L, Zhu G, Jiang Y, Yang A, Meng F, Zhang J
Clinical Interventions in Aging 2026, 21:600031
Published Date: 22 May 2026