Back to Journals » Journal of Pain Research » Volume 18
Functional and Structural Characteristics of the Pelvic Floor in Patients with Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS)
Authors Huang N, Bao K ![]() , Sun W, Yang Z, Shi J, Zha J, Zhang P, Li J, Ma M
, Sun W, Yang Z, Shi J, Zha J, Zhang P, Li J, Ma M
Received 21 August 2025
Accepted for publication 23 December 2025
Published 31 December 2025 Volume 2025:18 Pages 7351—7362
DOI https://doi.org/10.2147/JPR.S558228
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Ningqing Huang,1,* Kaiming Bao,2,* Wudong Sun,3 Zhen Yang,4 Jinjun Shi,3 Jingxian Zha,5 Peng Zhang,3 Jinfei Li,6 Ming Ma3
1Department of Rehabilitation Medicine, Nanjing Drum Tower Hospital, the Affiliated Hospital of Nanjing University Medical School, Nanjing, Jiangsu, People’s Republic of China; 2Sargent College of Health and Rehabilitation Sciences, Boston University, Boston, MA, USA; 3Department of Rehabilitation, Southeast University Zhongda Hospital, Nanjing, Jiangsu, People’s Republic of China; 4Physical Activity, Sports & Health Research Group, Department of Movement Sciences, KU Leuven, Leuven, Belgium; 5Department of Obstetrics, Southeast University Zhongda Hospital, Nanjing, Jiangsu, People’s Republic of China; 6Department of Rehabilitation Medicine, Nanjing Tongren Hospital, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinfei Li, Email [email protected] Ming Ma, Email [email protected]
Purpose: This study aimed to investigate the functional and structural characteristics of the pelvic floor in CP/CPPS patients using surface electromyography (sEMG), pelvic floor ultrasound, and the Psychosomatic Symptom Scale (PSSS).
Methods: Thirty CP/CPPS patients and thirty age-matched healthy males were assessed using the Glazer sEMG protocol and pelvic floor ultrasound to evaluate muscle activity, thickness, and elasticity. PSSS was used to evaluate psychological health. Independent samples t-tests were used for group comparisons.
Results: CP/CPPS patients exhibited significantly higher average EMG values during pre- and post-rest phases, prolonged relaxation time after rapid contractions, and greater variability during endurance contractions (p < 0.05). No significant differences were observed in ultrasound measurements (p > 0.05). PSSS scores were significantly higher in the CP/CPPS group across all subscales (p < 0.05).
Conclusion: CP/CPPS is characterized by increased pelvic floor muscle excitability, reduced coordination, and pronounced somatic and psychological symptom burden, without significant global structural abnormalities. The Glazer sEMG protocol may help identify characteristic pelvic floor abnormalities, while the PSSS offers valuable insights into psychological symptomatology.
Keywords: chronic prostatitis/chronic pelvic pain syndrome, CP/CPPS, male pelvic floor disfunction, surface electromyography, pelvic floor ultrasound, somatic and psychological symptom burden
Introduction
Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) is characterized by urogenital pain or discomfort lasting at least 3 months,1 and is a type of genitourinary pain caused by non-bacterial infections with predominantly pelvic floor muscle involvement.2 It is one of the most prevalent urological conditions in men.3,4 Current assessment tools include the National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI),5 the International Index of Erectile Function,6 the Patient Health Questionnaire-9 (PHQ-9), and digital rectal examination.7 These questionnaires are widely used, but they lack objectivity in evaluating pelvic floor function.
Surface electromyography (sEMG) and pelvic floor ultrasound have attracted increasing interest due to their non-invasive nature, objectivity, and clinical practicality.8,9 However, comprehensive evaluations using these techniques in CP/CPPS populations is still limited.
This study employed the Glazer protocol to assess pelvic floor function via sEMG under different contraction states in both CP/CPPS patients and healthy controls. The aim was to identify sEMG-based muscle activity patterns specific to CP/CPPS. In addition, pelvic floor ultrasound was used to preliminarily explore structural differences. The PSSS was also employed to compare somatic and psychological symptom burden between groups, offering a more holistic understanding of pelvic floor function and mental health in CP/CPPS patients.
Methods
Participants
Participants were recruited from the Pelvic Floor Health Management Center at Zhongda Hospital affiliated to Southeast University. Based on inclusion and exclusion criteria, 30 patients with severe CP/CPPS (as defined by NIH-CPSI scores: 0–15 = mild, 16–29 = moderate, 30–43 = severe,10 the full questionnaire is shown in Figure 1.) were enrolled. 30 healthy adult males without CP/CPPS-related symptoms, matched by age and other demographic characteristics, were recruited as the control group.
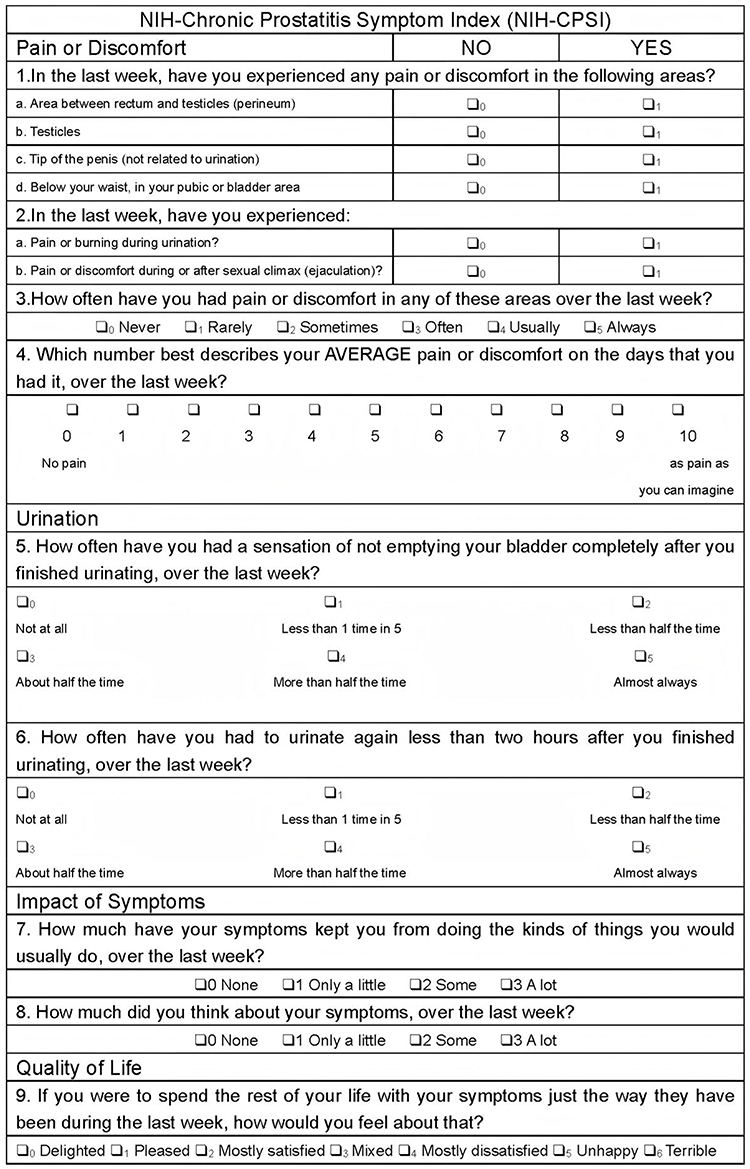 |
Figure 1 NIH-CPSI. |
All participants voluntarily completed a demographic questionnaire and signed informed consent. This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Zhongda Hospital, Southeast University (Approval No.: 2022ZDDSYLL280-P01).
Inclusion and Exclusion Criteria
Inclusion Criteria: (1) Males aged 20–40 years. (2) Diagnosed with CP/CPPS according to NIH criteria (pelvic pain without significant urological abnormalities).10 (3) Chronic pelvic pain persisting for more than 3 months. (4) Provided written informed consent.
Exclusion Criteria: (1) History of coagulation disorders, perineal anatomical anomalies, hormonal imbalances, or neurological disorders. (2) Other identified causes of pelvic pain (eg, infection, trauma, surgery, epididymitis, bacterial prostatitis). (3) Receiving any treatment at the time of recruitment. (4) Presence of urethral lesions. (5) History of lumbar injection or surgery within the past 6 months. (6) Contraindications to physiotherapy.
Assessment Tools and Procedures
Pelvic Floor Surface Electromyography (sEMG)
EMG data were collected using the VISHEE SA9800 biofeedback system. Participants were instructed to empty their bladder and bowel prior to testing. Tests were performed in a supine position following Glazer protocol guidelines to minimize compensatory activation of abdominal, gluteal, or hip muscles. The ground electrode was placed on the anterior superior iliac spine. A lubricated rectal probe was inserted, and recordings began after 10 seconds.
sEMG Testing Phases: 1. Pre-resting phase: 1-minute rest; mean EMG and coefficient of variation recorded. 2. Fast-twitch phase: 5 rapid contractions; peak EMG and relaxation time measured. 3. Slow-twitch phase: 5 sustained 10-second contractions; mean EMG and relaxation time recorded. 4. Endurance phase: 1-minute sustained contraction; mean EMG and coefficient of variation recorded. 5. Post-resting phase: 1-minute post-activity rest; mean EMG recorded.
Pelvic Floor Ultrasound
Ultrasound was conducted by a single experienced sonographer using a Mindray Resona 7S device in a room maintained at 27°C. The following parameters were assessed: 1. Levator hiatus area: Measured in the lithotomy position during rest using transverse and anteroposterior diameters. 2. Levator ani muscle thickness: Measured as the distance between fascial borders in a high-frequency long-axis view; the average of both sides was recorded. 3. Shear wave speed: Measured in the muscle belly during rest; bilateral averages calculated.
PSSS
The PSSS assesses biological and psychological symptom severity over the past four weeks using a 4-point Likert scale (0–3). Total scores range from 0 to 78; scores above 10 in men suggest higher somatic and psychological symptom burden. It consists of: 1. Somatic symptoms: 19 items covering neurological, cardiovascular, digestive, and genitourinary symptoms. 2. Psychological symptoms: 7 items addressing depression, anxiety, obsessive-compulsive behavior, anger, and suicidal ideation.11 The full questionnaire was provided in supplementary table 1.
Statistical Analysis
All statistical analyses were performed using SPSS 23.0. A p-value < 0.05 was considered statistically significant. Normality was tested using the Levene test. Independent samples t-tests were used for normally distributed data; otherwise, non-parametric rank-sum tests were applied.
Results
General Characteristics
Both groups consisted of 30 participants. There were no significant differences in age or body mass index (BMI) between CP/CPPS patients and healthy controls (p > 0.05). As shown in Table 1.
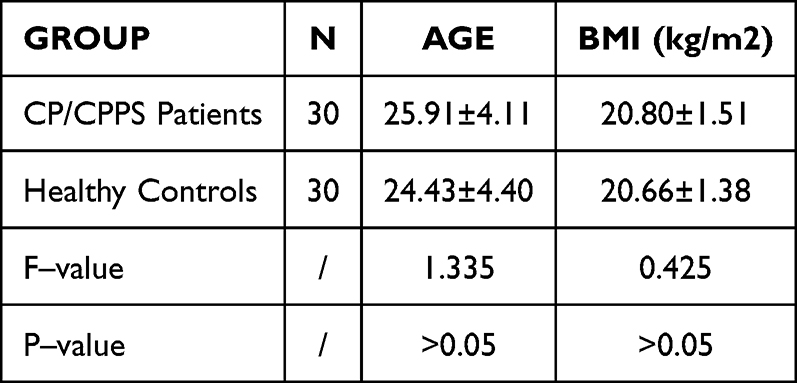 |
Table 1 Comparison of General Information Between the Two Groups [ |

Pelvic Floor sEMG Characteristics in CP/CPPS Patients Vs Healthy Individuals
Significant differences were observed between CP/CPPS patients and healthy controls across various stages of pelvic floor sEMG, as shown in Table 2:
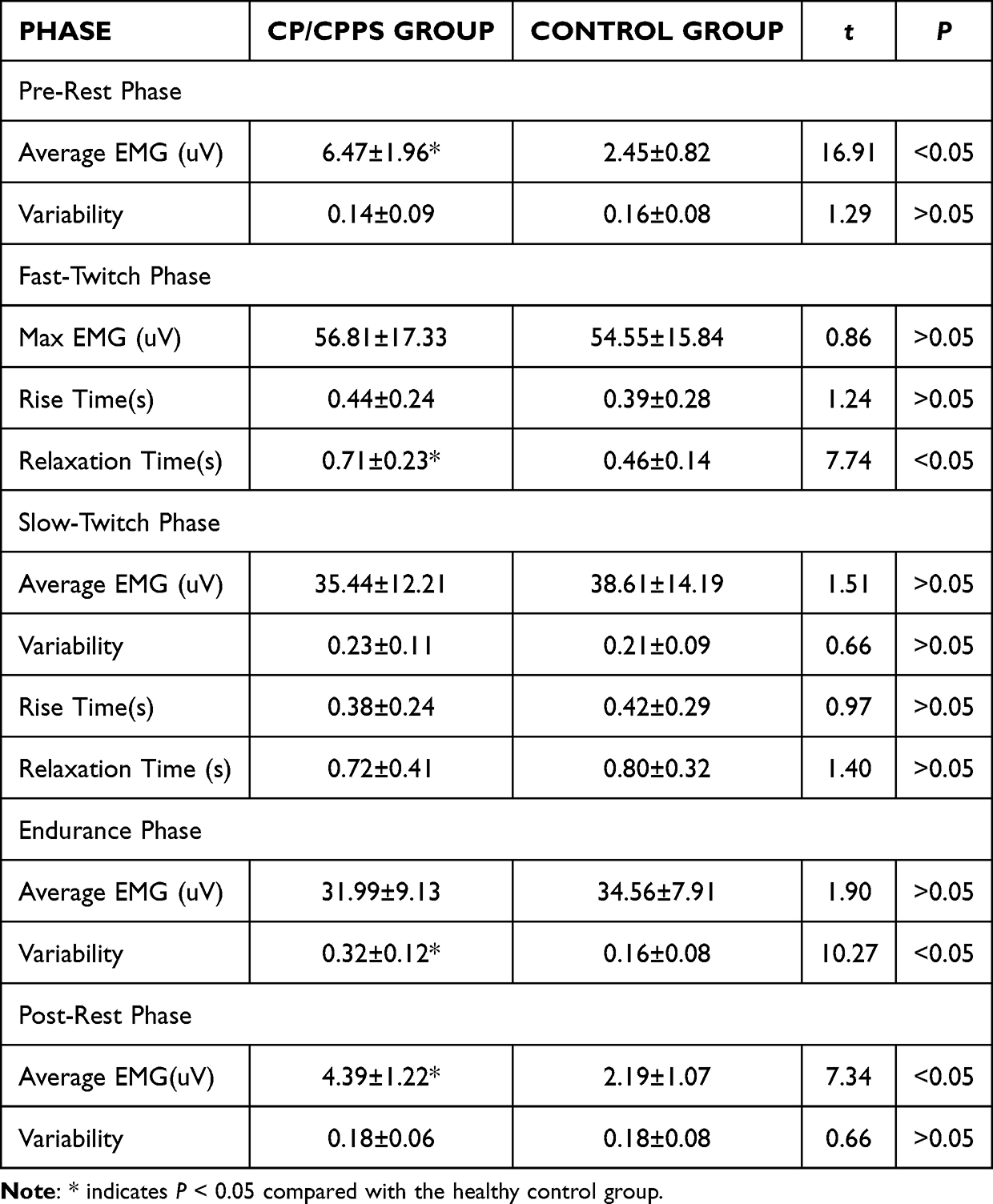 |
Table 2 Comparison of Pelvic Floor sEMG Parameters Between Groups |
Pre-resting phase: The CP/CPPS group demonstrated significantly higher average EMG values compared to controls (p < 0.05), although variability did not differ significantly (p > 0.05).
Fast-twitch contraction phase: Maximum EMG and rise time were comparable between groups (p > 0.05); however, relaxation time was significantly prolonged in the CP/CPPS group (p < 0.05).
Slow-twitch contraction phase: No significant differences were found in average EMG, variability, rise time, or relaxation time (p > 0.05).
Endurance contraction phase: While average EMG values were similar (p > 0.05), the CP/CPPS group showed significantly greater variability (p < 0.05).
Post-resting phase: Average EMG (AEMG) remained elevated in the CP/CPPS group (p < 0.05), with no significant difference in variability (p > 0.05).
Pelvic Floor Ultrasound Characteristics in CP/CPPS Patients Vs Healthy Individuals
In the relaxed lithotomy position, no significant differences were observed between groups in levator hiatus area, levator ani muscle thickness, or average shear wave velocity (p > 0.05), as shown in Table 3 and Figure 2.
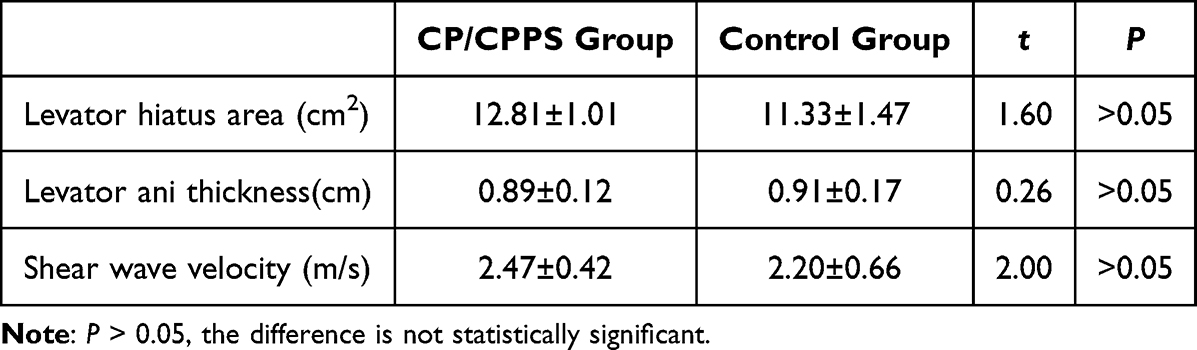 |
Table 3 Comparison of Pelvic Floor Ultrasound Parameters |
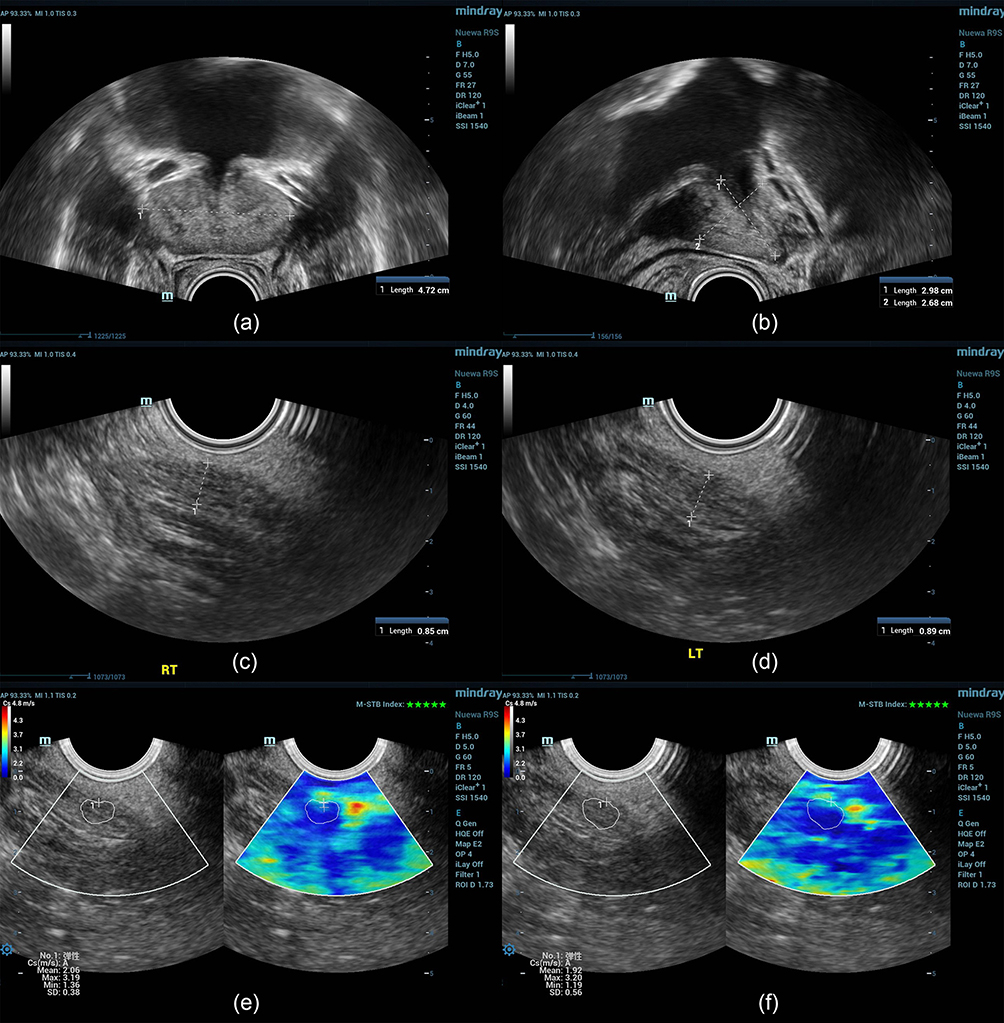 |
Figure 2 Schematic Diagram of Pelvic Floor Ultrasound Measurements. Note: Panels (a–f) illustrate the measurement methods for the following parameters respectively: transverse, vertical, and anteroposterior diameters of the levator hiatus; levator ani muscle thickness (right and left sides); and shear wave velocity for muscle elasticity (right and left sides). |
Somatic and Psychological Symptom Burden of CP/CPPS Patients Vs Healthy Individuals
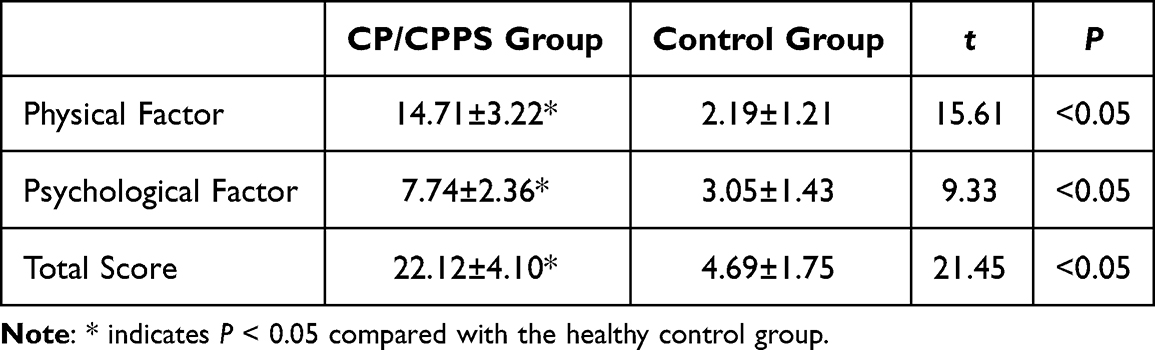
The CP/CPPS patient group scored significantly higher than the healthy control group in all three components of the PSSS: physical symptoms, psychological symptoms, and total score (P < 0.05). Detailed results are shown in Table 4.
 |

Correlation Analysis Between Pre-Rest AEMG and NIH-CPSI Total and Subscale Scores in CP/CPPS Patients
In CP/CPPS patient group, pre-rest pelvic-floor AEMG showed strong positive correlations with NIH-CPSI total score (r = 0.76, p < 0.05). The subscales of NIH-CPSI were examined separately, pre-rest AEMG correlated with Pain (r = 0.65, p < 0.05), Urinary Symptoms (r = 0.62, p < 0.05), and Quality of Life Impact (r = 0.37, p < 0.05). As shown in Figure 3.
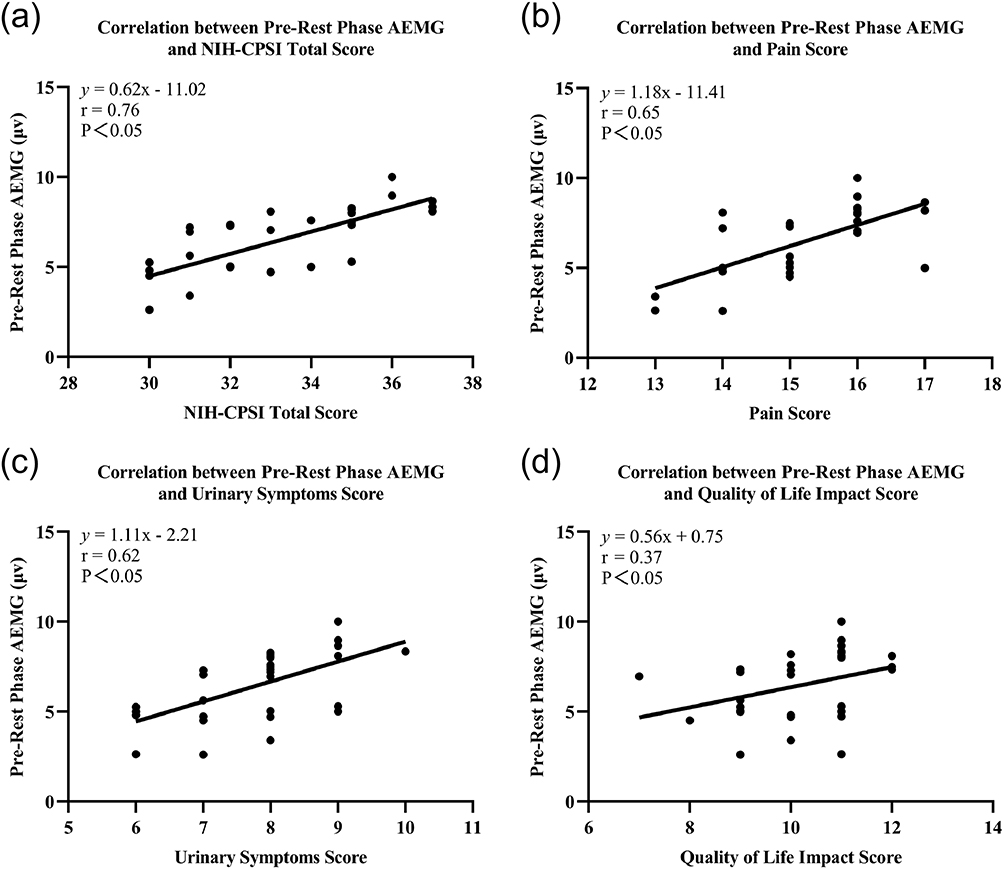 |
Figure 3 Correlations between pre-rest pelvic floor AEMG and NIH-CPSI total and subscale scores in CP/CPPS. Note: Panel (a) shows the correlation between pre-rest pelvic floor AEMG and the NIH-CPSI total score. Panels (b) to (d) show correlations with the NIH-CPSI subscales: (b) Pain, (c) Urinary Symptoms, and (d) Quality-of-Life Impact. |
Discussion
CP/CPPS is defined as chronic idiopathic pelvic pain in men, typically localized to the perineum, pubic region, penis, or testicles, and often prostatitis exacerbated by ejaculation or urinary retention.12,13 Although symptoms may resemble those of chronic bacterial prostatitis, laboratory tests frequently yield negative findings—low white blood cell counts, negative cultures). While earlier theories attributed symptoms to infection or inflammation of the prostate, recent evidence highlights pelvic floor muscle dysfunction as a principal contributor.14 Therefore, identifying the specific dysfunctions that occur during muscle contraction is critically important.
The traditional assessment of the severity and treatment outcomes of CP/CPPS has largely relied on patient report outcome and the clinical experience of therapists—such as the NIH Chronic Prostatitis Symptom Index and manual palpation. These methods are highly subjective and lack scientific rigor and objectivity. Therefore, it is essential to conduct further research to better understand the characteristics of CP/CPPS, develop more objective evaluation methods, and identify more effective clinical interventions based on the manifestations of the condition.15
To enhance clinical precision, this study utilized sEMG, pelvic floor ultrasound, and the PSSS to compare CP/CPPS patients with healthy individuals. Results indicated functional abnormalities and elevated psychosomatic symptomatology in CP/CPPS patients, despite the absence of significant structural changes.
Pelvic Floor sEMG Characteristics
Neuromuscular dysfunction in CP/CPPS patients ultimately showed as impaired contraction and relaxation of pelvic floor muscle fibers. The Glazer protocol offers a comprehensive assessment of PFM activity across five distinct contraction phases: pre-resting, fast-twitch contraction, slow-twitch contraction, endurance contraction, and post-resting phases. Results from this study revealed that patients with CP/CPPS had significantly higher average EMG values during the pre-resting phase compared to healthy controls, suggesting increased excitability of the pelvic floor muscles at rest.
Heightened excitability may result in increased local muscle tension, leading to elevated muscle tone. This in turn can accelerate force transmission and is often associated with pain in regions such as the perineum, penile tip, or during ejaculation. Gentilcore-Saulnier et al reported that women with pelvic pain exhibited higher superficial and deep PFM activation during pressure on the vestibule and vaginal probe insertion compared to women without a history of vulvar pain.16 This implies that, aside from increased excitability at rest, another possible explanation for the elevated pre-resting AEMG in CP/CPPS patients is heightened pelvic floor irritability. Insertion of a rectal probe may trigger a stronger protective muscular response in these patients than in healthy individuals, leading to elevated muscle activation during the initial resting phase.
During the fast-twitch contraction phase, CP/CPPS patients demonstrated significantly prolonged relaxation times compared to healthy controls. This indicates impaired muscle coordination, as the pelvic floor failed to relax efficiently following rapid contraction. Normal pelvic floor function depends on precise neuromuscular control, which is mediated by complex afferent and efferent neural pathways. Disruptions in these neural circuits can compromise muscle coordination. Notably, pelvic floor coordination is closely linked to urinary symptoms. For instance, afferent signals from the bladder during urine storage modulate central control pathways at various levels.17,18 In CP/CPPS patients, behaviors such as urinary retention may exacerbate symptoms by altering central nervous system activity. This can manifest as: (1) Spinal reflexes enhancing activity of the bladder base, urethra, and external sphincter while inhibiting the detrusor muscle; (2) Pontine excitation increasing urethral sphincter tone and resistance; (3) Motor cortex modulation of descending signals to pelvic motor neurons via the reticulospinal and corticospinal tracts.19 These changes may explain post-retention symptom worsening in CP/CPPS, such as reduced urinary flow and increased post-void residual volume. Improving pelvic floor coordination may thus offer a pathway to alleviate urinary symptoms.
During the endurance contraction phase, CP/CPPS patients exhibited significantly greater sEMG variability, reflecting an inability to sustain consistent PFM activation. This suggests increased fatigability and unstable muscle output, which may manifest as sudden weakness or spasms during prolonged contraction. These findings indicate both impaired neuromuscular control and reduced muscular endurance. Pelvic muscle spasms may cause erratic pressure changes in the urethral smooth muscle, raising intraluminal pressure and promoting retrograde urine flow—contributing to the sensation of incomplete bladder emptying. Muscles such as the bulbospongiosus and ischiocavernosus (involved in ejaculation), as well as the superficial perineal and levator ani muscles (which transmit pain to the penile tip), are essential for pelvic floor function. Dysfunction in these muscles can directly lead to symptoms such as premature ejaculation, perineal or penile pain, and voiding difficulties. Once pain subsides, CP/CPPS patients should undergo targeted pelvic floor training—such as stabilization exercises—to enhance endurance and control of the deep stabilizing muscles. Activities that significantly increase intra-abdominal pressure (like long-distance running or heavy lifting) should be avoided during rehabilitation.
In the post-resting phase, AEMG in CP/CPPS patients remained significantly higher than in healthy controls, although it was lower than their own pre-resting AEMG. This suggests that although muscle excitability decreases following contraction cycles, it remains elevated overall. Some researchers have proposed that only patients with elevated post-resting AEMG should be diagnosed with CP/CPPS, as elevated pre-resting AEMG alone may produce false positives.19 However, our study indicates that both pre- and post-resting AEMG values are meaningful diagnostic indicators of pelvic floor dysfunction in CP/CPPS.
The pre-resting phase represents an immediate protective response to stimulation, while the post-resting phase reflects the muscle state after routine activity or exercise. In both healthy individuals and CP/CPPS patients, AEMG generally decreases after contraction, with only a minority of patients showing a marked post-exercise increase. The sustained elevation in post-resting AEMG observed in some patients may correlate with greater disease severity and increased muscle spasm. Among the three contraction phases, endurance contraction occurs immediately before the post-resting phase and likely has the most direct influence on post-resting AEMG. Future studies can explore how these contraction types impact pelvic floor electrophysiology in CP/CPPS patients.
Within the CP/CPPS group, pre-rest pelvic floor AEMG showed significant positive correlations with NIH-CPSI total, pain, and urinary symptom scores, and a weaker but still significant association for quality-of-life impact. This pattern supports elevated baseline pelvic floor activity aligns with symptom intensity and voiding complaints. Sustained tonic activity likely increases nociceptive input and output resistance and may therefore contribute to the pain symptoms. The relatively weaker QoL link likely reflects broader, multifactorial influences beyond pelvic floor physiology. In this study, elevated pre-rest AEMG is best viewed as a physiological correlate of symptom severity, not evidence of causation. Clinically, pre-rest AEMG may help guide future treatment, informing the selection and monitoring of approaches that reduce resting tone and improve coordination, with reductions in resting AEMG expected to accompany improvements in pain and urinary symptoms.
Pelvic Floor Ultrasound Characteristics
Studies using musculoskeletal ultrasound elastography have shown that myofascial trigger points appear as oval-shaped, hypoechoic, heterogeneous stiff bands, with stiffness up to 1.5 times greater than that of surrounding healthy tissue.20 Previous research has applied this technique to evaluate muscle conditions in patients with spasticity following stroke,5,21,22 and its application in pelvic floor muscle assessment is gradually being explored.
This study innovatively employed shear wave elastography to evaluate levator ani muscle elasticity in CP/CPPS patients. Greater shear wave velocity indicates increased muscle stiffness, and elasticity varies with contraction state. For instance, a 10 N increase in applied force results in a 0.9 m/s increase in shear wave velocity. Therefore, in this study, measurements were taken while participants were in a relaxed state. Although the average shear wave velocity in the CP/CPPS group was higher than that of the control group, the difference was not statistically significant. This suggests that pelvic floor muscle stiffness in CP/CPPS patients is not markedly increased compared to healthy individuals. This finding implies that the increased stiffness often detected through palpation in CP/CPPS patients may be localized to specific myofascial trigger points and does not reflect a global increase in muscle hardness.
Regarding other ultrasound indicators evaluated in this study, no significant average global stiffness differences were found between CP/CPPS patients and healthy controls in levator hiatus area and levator ani muscle thickness. This suggests that these structural parameters may not be closely associated with the onset or progression of CP/CPPS, and that the condition is more likely rooted in functional rather than anatomical changes. Because our shear wave elastography protocol only measured global levator ani stiffness at rest, it may not detect localized focal increases at palpation-positive sites; localized stiffness therefore cannot be excluded. For future measurement considerations, beyond global mean shear-wave values, subsequent studies should employ focal shear wave elastography guided by palpation-positive or patient-designated pain points to evaluate localized stiffness and capture within-muscle heterogeneity.
Psychological Characteristics
Studies have demonstrated that chronic pain significantly reduces patients’ quality of life.22,23 Compared to healthy individuals, patients with CP/CPPS often present with more pronounced psychological issues. A study by the National Institute of Diabetes and Digestive and Kidney Diseases of the US National Institutes of Health reported that 31% of men with CP/CPPS also exhibited somatic syndromes unrelated to the urinary system, which were associated with longer disease duration, more severe urological symptoms, and higher rates of depression and anxiety.24 Another study showed that anxiety, depression, and disease duration were clear negative prognostic factors, while age, NIH-CPSI score, personality, and leukocyte count in EPS had no significant effect.25
In our study, CP/CPPS patients exhibited not only somatic symptoms but also significant psychological disturbances compared to healthy controls. The mean total score on the PSSS in the CP/CPPS group was 22.12 ± 4.10, well above the diagnostic threshold of 10, supporting the classification of CP/CPPS as a biological and psychological disorder. Psychological stress may exacerbate pelvic pain symptoms in CP/CPPS patients, and in turn, the presence of pain can intensify psychological distress. Erectile pain in CP/CPPS patients can result in sexual dysfunction such as premature ejaculation or erectile difficulty. This dysfunction then contributes to negative emotional states. Pain during erection may particularly amplify anxiety and depression.
It has been shown by evidence that within a biopsychosocial model, psychological distress and pain -related cognitions are key contributors to the symptom burden in CP/CPPS.26,27 The EAU 2025 Guidelines classify CPPS as conditions usually associated with negative cognitive, behavioral, sexual, or emotional outcomes. They put emphasis on assessing depression, anxiety, unhelpful coping, and catastrophizing.28 In this study, higher PSSS scores indicate that mood and cognitive factors accompany and may amplify pelvic pain and urinary symptoms, rather than reflecting a purely psychological pain state.
In summary, CP/CPPS is a somatic and psychological symptom burden, and affected individuals are more likely to experience impaired psychological well-being, including emotional disturbances and reduced mental health. Conversely, individuals with poor mental health may be at higher risk of developing this physical condition. However, the current study cannot yet determine whether interventions targeting physical symptoms can alleviate psychological issues in CP/CPPS patients.
Limitations
This study has several limitations. First, the design was cross-sectional, so the observed elevation in pre-rest pelvic-floor AEMG is best interpreted as a physiological correlate of current symptom severity, rather than definitive evidence of causation. Second, although a standardized 10-second post-insertion relaxation period was implemented for all participants to attenuate activation, a probe-induced protective response cannot be excluded. Accordingly, pre-rest AEMG should be interpreted with caution and verified in future studies using less-invasive measurements. Third, our ultrasound shear-wave elastography quantified global levator ani stiffness at rest and may not capture localized focal stiffness. Fourth, our sample consisted exclusively of severe CP/CPPS cases (NIH-CPSI ≥ 30). As a result, findings may not generalize to mild or moderate phenotypes, and severity spectrum effects may have influenced the magnitude of observed associations. Fifth, this was a single-center study with a modest sample size, which may limit external validity and reduce precision. Finally, the participants were restricted to men aged 20–40 years, which may limit applicability to other age groups.
Conclusion
The characteristic indicators of CP/CPPS include average EMG during the pre-resting and post-resting phases, relaxation time following fast contractions, and variability during endurance contractions. These parameters serve as effective tools for assessing pelvic floor function in CP/CPPS patients. Structurally, our ultrasound showed no differences in global resting levator ani measures, but localized hypertonicity or focal stiffness remains possible. The dysfunction appears to stem from physiological impairments. Specifically, pelvic floor muscles in CP/CPPS patients exhibit increased excitability and reduced coordination.
CP/CPPS may be best understood as a somatic and psychological symptom burden, and the PSSS can be used to evaluate the severity of somatic and psychological symptom burden in affected individuals.
Abbreviations
CP/CPPS, Chronic prostatitis/chronic pelvic pain syndrome; PSSS, Psychosomatic Symptom Scale; NIH-CPSI, National Institutes of Health Chronic Prostatitis Symptom Index; PHQ-9, Patient Health Questionnaire-9; sEMG, Surface electromyography; AEMG, Average EMG; BMI, Body mass index.
Acknowledgment
We would like thank all the participants who took part in this study. We also acknowledge therapists and medical staff for their support and expertise throughout this research.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Borgert BJ, Wallen EM, Pham MN. Prostatitis: a review. JAMA. 2025;334(11):1003–1013. doi:10.1001/jama.2025.11499
2. Nickel JC, Nyberg LM, Hennenfent M. Research guidelines for chronic prostatitis: consensus report from the first national institutes of health international prostatitis collaborative network. Urology. 1999;54(2):229–233. doi:10.1016/s0090-4295(99)00205-8
3. Yuen KH, Krieger JN, Riley DE, Cheah PY, Liong ML. Epidemiology of prostatitis: new evidence for a world-wide problem. World J Urol. 2003;21(2):70–74. doi:10.1007/s00345-003-0329-0
4. Jackson T, Thomas S, Stabile V, Han X, Shotwell M, McQueen K. Prevalence of chronic pain in low-income and middle-income countries: a systematic review and meta-analysis. Lancet. 2015;385(Suppl 2):S10. doi:10.1016/S0140-6736(15)60805-4
5. Park G-Y, Kwon DR. Sonoelastographic evaluation of medial gastrocnemius muscles intrinsic stiffness after rehabilitation therapy with botulinum toxin a injection in spastic cerebral palsy. Arch Phys Med Rehabil. 2012;93(11):2085–2089. doi:10.1016/j.apmr.2012.06.024
6. Chen X, Zhou Z, Qiu X, Wang B, Dai J, Eldabe S. The effect of chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) on erectile function: a systematic review and meta-analysis. PLoS One. 2015;10(10):e0141447. doi:10.1371/journal.pone.0141447
7. Shulyak A, Gorpynchenko I, Drannik G, Poroshina T, Savchenko V, Nurimanov K. The effectiveness of the combination of rectal electrostimulation and an antidepressant in the treatment of chronic abacterial prostatitis. Cent Euro J Urol. 2019;72(1):66–70. doi:10.5173/ceju.2018.1719
8. Dietz HP. Ultrasound in the investigation of pelvic floor disorders. Curr Opin Obstet Gynecol. 2020;32(6):431–440. doi:10.1097/GCO.0000000000000659
9. Enck P, Vodusek DB. Electromyography of pelvic floor muscles. J Electromyogr Kinesiol. 2006;16(6):568–577. doi:10.1016/j.jelekin.2006.08.007
10. Litwin MS, McNaughton-Collins M, Fowler FJ Jr, et al. The national institutes of health chronic prostatitis symptom index: development and validation of a new outcome measure. chronic prostatitis collaborative research network. J Urol. 1999;162(2):369–375. doi:10.1016/s0022-5347(05)68562-x
11. Li L, Peng T, Liu R, et al. Development of the psychosomatic symptom scale (PSSS) and assessment of its reliability and validity in general hospital patients in China. Gen Hosp Psychiatry. 2020;64:1–8. doi:10.1016/j.genhosppsych.2020.01.008
12. Landis JR, Williams DA, Lucia MS, et al. The MAPP research network: design, patient characterization and operations. BMC Urol. 2014;14:58. doi:10.1186/1471-2490-14-58
13. Krieger JN, Ross SO, Deutsch L, Riley DE. The NIH consensus concept of chronic prostatitis/chronic pelvic pain syndrome compared with traditional concepts of nonbacterial prostatitis and prostatodynia. Curr Urol Rep. 2002;3(4):301–306. doi:10.1007/s11934-002-0054-z
14. Yani MS, Eckel SP, Kirages DJ, Rodriguez LV, Corcos DM, Kutch JJ. Impaired ability to relax pelvic floor muscles in men with chronic prostatitis/chronic pelvic pain syndrome. Phys Ther. 2022;102(7). doi:10.1093/ptj/pzac059
15. Clemens JQ, Kutch JJ, Mayer EA, et al. The multidisciplinary approach to the study of chronic pelvic pain (MAPP) research network*: design and implementation of the symptom patterns study (SPS). Neurourol Urodyn. 2020;39(6):1803–1814. doi:10.1002/nau.24423
16. Gentilcore-Saulnier E, McLean L, Goldfinger C, Pukall CF, Chamberlain S. Pelvic floor muscle assessment outcomes in women with and without provoked vestibulodynia and the impact of a physical therapy program. J Sex Med. 2010;7(2_Part_2):1003–1022. doi:10.1111/j.1743-6109.2009.01642.x
17. Yani MS, Wondolowski JH, Eckel SP, et al. Distributed representation of pelvic floor muscles in human motor cortex. Sci Rep. 2018;8(1):7213. doi:10.1038/s41598-018-25705-0
18. Griffiths D. Neural control of micturition in humans: a working model. Nat Rev Urol. 2015;12(12):695–705. doi:10.1038/nrurol.2015.266
19. Asavasopon S, Rana M, Kirages DJ, et al. Cortical activation associated with muscle synergies of the human male pelvic floor. J Neurosci. 2014;34(41):13811–13818. doi:10.1523/JNEUROSCI.2073-14.2014
20. Brandenburg JE, Eby SF, Song P, et al. Ultrasound elastography: the new frontier in direct measurement of muscle stiffness. Arch Phys Med Rehabil. 2014;95(11):2207–2219. doi:10.1016/j.apmr.2014.07.007
21. Kwon DR, Kwon DG. Botulinum toxin a injection combined with radial extracorporeal shock wave therapy in children with spastic cerebral palsy: shear wave sonoelastographic findings in the medial gastrocnemius muscle, preliminary study. Children. 2021;8(11). doi:10.3390/children8111059
22. Aibel K, Moldwin R. Validation of the ‘Pelvic Pain Map’: anew self-assessment tool for chronic pelvic pain localisation. BJU Int. 2023;131(6):763–769. doi:10.1111/bju.15979
23. Chen N-W, Jin J, Xu H, et al. Effect of thermophilic bacterium HB27 manganese superoxide dismutase in a rat model of chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS). Asian J Androl. 2022;24(3):323–331. doi:10.4103/aja202157
24. Krieger JN, Stephens AJ, Landis JR, et al. Relationship between chronic nonurological associated somatic syndromes and symptom severity in urological chronic pelvic pain syndromes: baseline evaluation of the MAPP study. J Urol. 2015;193(4):1254–1262. doi:10.1016/j.juro.2014.10.086
25. Li H-C, Wang Z-L, Li H-L, et al. Correlation of the prognosis of chronic prostatitis/chronic pelvic pain syndrome with psychological and other factors: a cox regression analysis. Zhonghua Nan Ke xue. 2008;14(8):723–727.
26. Smith KB, Tripp D, Pukall C, Nickel JC. Predictors of sexual and relationship functioning in couples with chronic prostatitis/chronic pelvic pain syndrome. J Sex Med. 2007;4(3):734–744. doi:10.1111/j.1743-6109.2007.00466.x
27. Dybowski C, Lowe B, Brunahl C. Predictors of pain, urinary symptoms and quality of life in patients with chronic pelvic pain syndrome (CPPS): a prospective 12-month follow-up study. J Psychosom Res. 2018;112:99–106. doi:10.1016/j.jpsychores.2018.06.013
28. Fall M, Baranowski AP, Elneil S, et al. EAU guidelines on chronic pelvic pain. Eur Urol. 2010;57(1):35–48. doi:10.1016/j.eururo.2009.08.020
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.