Back to Journals » International Medical Case Reports Journal » Volume 18
Full-Thickness Macular Hole Formation After Intravitreal Faricimab Injection for Polypoidal Choroidal Vasculopathy
Authors Tavonvunchai F ![]() , Chanwimol K
, Chanwimol K
Received 24 March 2025
Accepted for publication 12 June 2025
Published 23 June 2025 Volume 2025:18 Pages 741—746
DOI https://doi.org/10.2147/IMCRJ.S527975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Fahsiri Tavonvunchai, Karntida Chanwimol
Department of Ophthalmology, Mettapracharak (Wat Rai Khing) Hospital, Nakhon Pathom, Thailand
Correspondence: Fahsiri Tavonvunchai, Department of Ophthalmology, Mettapracharak (Wat Rai Khing) Hospital, 52 Moo 2 Rai Khing Sam Pran, Nakhon Pathom, 73210, Thailand, Email [email protected]
Purpose: To report a case of an Asian man with idiopathic polypoidal choroidal vasculopathy (PCV) who developed a full-thickness macular hole (FTMH) following treatment with intravitreal faricimab, which resolved after vitreoretinal surgery.
Patients and Methods: A 63-year-old man with idiopathic PCV was treated with intravitreal faricimab. Although pigment epithelial detachment (PED) decreased, he developed cystoid macular edema with vitreomacular traction (VMT), which progressed to a FTMH.
Results: Pars plana vitrectomy and internal limiting membrane peeling successfully treated the FTMH. One year after the procedure, the macular hole remains closed, and the PCV was inactive.
Conclusion: Various mechanisms may have contributed to the exacerbation of the preexisting VMT and PED, which finally resulted in the development of a FTMH. Careful attention should be paid to changes in the vitreomacular interface and posterior vitreous detachment before performing intravitreal anti-vascular endothelial growth factor treatment. Nevertheless, FTMHs can be successfully treated with prompt vitreoretinal surgery.
Keywords: anti-vascular endothelial growth factor, pigment epithelial detachment, vitreomacular traction, vitreoretinal surgery
Introduction
Polypoidal choroidal vasculopathy (PCV) is a subset of neovascular age-related macular degeneration (nAMD), characterized by polypoidal aneurysmal vascular lesions in the choroidal vasculature.1 These lesions often lead to recurrent serosanguinous retinal pigment epithelial (RPE) detachments, causing visual impairment.2,3 Although PCV is similar to typical nAMD, it is more prevalent in Asian populations and tend to affect younger individuals.4,5 It is estimated that in 2050, PCV will affect more patients in Asia than in the rest of the world combined.6,7 Vision loss among the working-age population poses a serious threat to the economy, as it reduces the availability of skilled human resources.5
Anti-vascular endothelial growth factor (anti-VEGF) therapy is one of the first line treatments for PCV, due to its ability to reduce exudation from abnormal polyps and choroidal vessels, thus preserving vision.1 Faricimab, a bispecific monoclonal antibody targeting both VEGF-A and angiopoietin-2 (Ang-2), provides dual inhibition of neovascularization and inflammation.8 The development of a full-thickness macular hole (FTMH) is a rare complication of intravitreal anti-VEGF injection.9–11 We present a case of an Asian man with PCV who developed a FTMH following treatment with intravitreal faricimab, which resolved after vitreoretinal surgery.
Case Presentation
A 63-year-old Asian man presented to the hospital with blurry vision of the right eye for two weeks. His best corrected visual acuity (BCVA) measured with a Snellen chart on presentation was 20/50 in the right eye and 20/20 in the left eye. The intraocular pressure (IOP) measured with a pneumotonometer was 12 mmHg and 13 mmHg respectively. The retina of the left eye appears to be within normal limits. However, optical coherence tomography (OCT) of the right macula revealed subretinal fluid (SRF) with pigment epithelial detachment (PED). A fundus fluorescein angiography showed a juxtafoveal hyperfluorescent lesion with a stippled pattern, while an indocyanine green angiography (ICGA) revealed a polyp with a halo. The patient was diagnosed with idiopathic PCV of the right eye and was treated with anti-VEGF injections at 4-week intervals, switching between bevacizumab and ranibizumab. After 10 uneventful intravitreal injections to the right eye, the PED and SRF considerably decreased, and the disease was inactive for the next three years.
The patient did not return for follow-ups for the following three years due to the COVID-19 pandemic but later revisited the clinic with worsening vision in the right eye. His BCVA on presentation was counting fingers at 3 feet in the right eye and 20/20 in the left eye. The left retina remained within normal limits; however, the OCT scan of the right eye revealed a sharp PED with subretinal hemorrhage (Figure 1). The active PCV was treated with monthly intravitreal faricimab injections for two consecutive months. On the following clinical visit, an OCT scan revealed cystoid macular edema (CME), vitreomacular traction (VMT), RPE changes, and a decreased PED (Figure 2). The patient was treated with a third faricimab injection. One month later, the CME progressed into a FTMH (Figure 3). Pars plana vitrectomy, internal limiting membrane peeling, fluid-air exchange (FAX), intravitreal bevacizumab injection, and installation of 20% SF6 were performed on the right eye. At the one-month postoperative follow-up, the macular hole remained closed, the PED was decreased, and the PCV of the right eye was inactive. One year after the procedure, the macular hole remains closed, and the PCV remains inactive (Figure 4). Cataract surgery was later performed on the right eye, which improved his BCVA from counting fingers at 3 feet to 20/100.
 |
Figure 1 A 63-year-old man with polypoidal choroidal vasculopathy who was lost to follow-up presented with blurry vision in the right eye. (a) A color fundus photograph demonstrating a new submacular hemorrhage (arrow) in the right eye. (b) Spectral-Domain Optical Coherence Tomography (SD-OCT) showing intraretinal hyperreflectivity and subretinal hemorrhage. (c) SD-OCT showing a large serous pigment epithelial detachment with vitreomacular traction. |
 |
Figure 2 Spectral-Domain Optical Coherence Tomography (SD-OCT) imaging after two courses of monthly intravitreal faricimab injections to the right eye. (a) SD-OCT showing a subfoveal intraretinal cyst. (b) SD-OCT showing a slightly decreased pigment epithelial detachment with vitreomacular traction. |
 |
Figure 3 Spectral-Domain Optical Coherence Tomography (SD-OCT) imaging after three courses of monthly intravitreal faricimab injections to the right eye. (a) SD-OCT showing a stage 4, full-thickness macular hole with cystoid macular edema. (b) SD-OCT showing a decreased pigment epithelial detachment. |
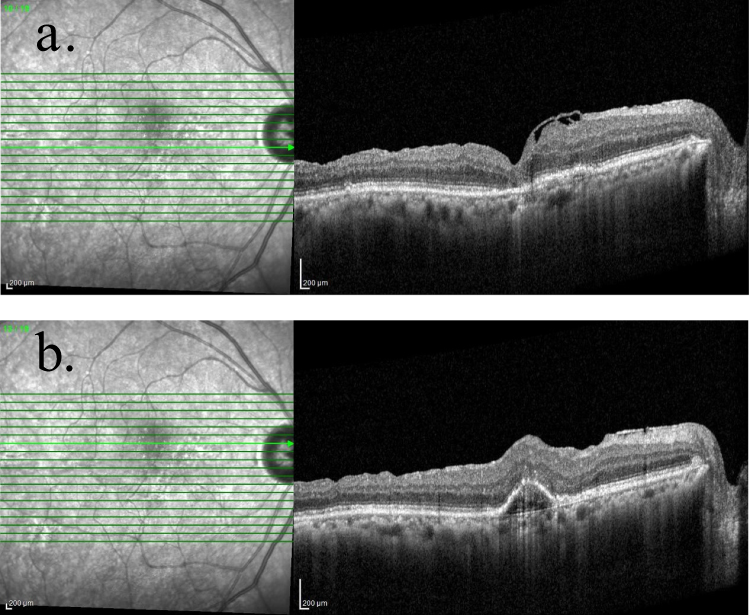 |
Figure 4 Spectral-Domain Optical Coherence Tomography (SD-OCT) imaging of the right eye at one year post-vitreoretinal surgery. (a) SD-OCT showing a closed macular hole. (b) SD-OCT showing a small pigment epithelial detachment. |
Discussion
Developing a FTMH after treating PCV with an intravitreal anti-VEGF injection is rare. Several mechanisms have been hypothesized to explain the process of FTMH formation. Gass suggested that idiopathic FTMH formation occurred due to prefoveal vitreous cortex contraction, causing focal tangential traction on the fovea.12 Gaudric et al demonstrated that posterior hyaloid detachment exerts an oblique tractional force on the foveolar center using OCT.13 Therefore, idiopathic FTMH develops by tangential and anterior–posterior transvitreal traction.
Repeated intravitreal anti-VEGF injections may contribute to macular hole formation. Needle insertion can deform the globe or cause vitreous incarceration at the injection site, resulting in vitreoretinal traction.14,15 Meyer et al hypothesized that anti-VEGF chemical compounds promote vitreous gel syneresis, resulting in incomplete posterior vitreous detachment (PVD) and anteroposterior traction on the VMT.16 Intravitreal injections have also been shown to induce PVD in older patients with macular diseases. Geck et al observed a 24% incidence of PVD over 11-weeks post-injection, which correlated with increasing age.17
The contraction of choroidal neovascularization and the flattening of PED may also impose shearing forces on the overlying RPE and retina, leading to a macular hole.9,14,18 Chan et al found that a vascularized PED height of ≥ 400 µm increases the risk of RPE tears after bevacizumab injections, particularly with increased SRF.19 Mukherjee et al presented a case of an 81-year-old woman who was treated with bilateral ranibizumab injections for subfoveal choroidal neovascular membrane with a large dome-shaped PED.20 After six intravitreal injections, a stage 3 FTMH with flattened PED was observed in the left eye. Recurrent flattening and distension of the PED may have exacerbated the instability of the adhesion at the vitreous and neuroretinal interface, which may have ultimately resulted in a FTMH.
In our presented case, the intravitreal faricimab injection may have induced various changes, including globe deformation, modulation of the vitreous, and the rapid resolution of PED and macular edema. Various mechanisms may have contributed to the exacerbation of the preexisting VMT and PED, which finally resulted in the development of a FTMH. However, prompt vitreoretinal surgery successfully repaired and stabilized the macular hole.
This case highlights an occurrence of a FTMH after treatment with a relatively new drug, Faricimab, in PCV. Although this is a single case report and generalizability is limited, it emphasizes the need for clinicians to assess the vitreomacular status prior to initiating anti-VEGF treatment, especially in patients with predisposing factors like VMT or large PEDs.
Conclusion
Macular hole formation is a potential complication of intravitreal anti-VEGF injections; thus, careful attention should be paid to PVD and changes at the vitreomacular interface before treatment. Nevertheless, FTMHs can be treated with prompt vitreoretinal surgery to improve the visual prognosis, as described in the current case.
Ethical Approval
All details, medical records and figures were used with the written consent for publication from the patient. This case report was approved by the Mettapracharak (Wat Rai Khing) Research Ethics Committee in accordance with the International Conference on Harmonization Good Clinical Practice (ICH-GCP) (COA No 005/2567).
Disclosure
Fahsiri Tavonvunchai and Karntida Chanwimol report no conflicts of interest in this work.
References
1. Cps H, Lai TYY. Current management strategy of polypoidal choroidal vasculopathy. Indian J Ophthalmol. 2018;66(12):1727–1735. doi:10.4103/ijo.IJO_975_18
2. Kumar A, Kumawat D, Sundar MD, et al. Polypoidal choroidal vasculopathy: a comprehensive clinical update. Ther Adv Ophthalmol. 2019:11. doi:10.1177/2515841419831152
3. Sen P, Manayath G, Shroff D, Salloju V, Dhar P. Polypoidal choroidal vasculopathy: an update on diagnosis and treatment. Clin Ophthalmol. 2023;17:53–70. doi:10.2147/OPTH.S385827
4. Zhao J, Chandrasekaran PR, Cheong KX, Wong M, Teo K. New concepts for the diagnosis of polypoidal choroidal vasculopathy. Diagnostics. 2023;13(10):1680. doi:10.3390/diagnostics13101680
5. Rai BB, Morley MG, Bernstein PS, Maddess T. Severity of age-related macular degeneration at first presentation in Bhutan: a 3-year national study. BMC Ophthalmol. 2022;22(1):298. doi:10.1186/s12886-022-02520-w
6. Wong CW, Yanagi Y, Lee WK, et al. Age-related macular degeneration and polypoidal choroidal vasculopathy in Asians. Prog Retin Eye Res. 2016;53:107–139. doi:10.1016/j.preteyeres.2016.04.002
7. van Dijk EHC, Mohabati D, Veselinovic S, Chung WH, Dijkman G, Boon CJF. The spectrum of polypoidal choroidal vasculopathy in Caucasians: clinical characteristics and proposal of a classification. Graefes Arch Clin Exp Ophthalmol. 2021;259(2):351–361. doi:10.1007/s00417-020-04844-z
8. Nicolò M, Ferro Desideri L, Vagge A, Traverso CE. Faricimab: an investigational agent targeting the Tie-2/angiopoietin pathway and VEGF-A for the treatment of retinal diseases. Expert Opin Investig Drugs. 2021;30(3):193–200. doi:10.1080/13543784.2021.1879791
9. Sethia A, Sheth J, Gopalakrishnan M, Anantharaman G. Spontaneous formation and closure of full thickness macular hole after treatment with anti-vascular endothelial growth factor therapy in polypoidal choroidal vasculopathy. Indian J Ophthalmol. 2019;67(10):1756–1758. doi:10.4103/ijo.IJO_1597_18
10. Lindeke-Myers A, Kokame GT, Yeh S, Shantha J. Successful treatment of full-thickness macular hole in polypoidal choroidal vasculopathy with anti-VEGF therapy. J Vitreoretin Dis. 2020;4(5):433–436. doi:10.1177/2474126420909706
11. Cho JH, Park SE, Han JR, Kim HK, Nam WH. Macular hole after intravitreal ranibizumab injection for polypoidal choroidal vasculopathy. Clin Exp Optom. 2011;94(6):586–588. doi:10.1111/j.1444-0938.2011.00614.x
12. Gass JDM. Idiopathic Senile macular hole. Arch Ophthalmol. 1988;106(5):629. doi:10.1001/archopht.1988.01060130683026
13. Gaudric A. Macular hole formation. Arch Ophthalmol. 1999;117(6):744. doi:10.1001/archopht.117.6.744
14. Grigoropoulos V, Emfietzoglou J, Nikolaidis P, Theodossiadis G, Theodossiadis P. Full-thickness macular hole after intravitreal injection of ranibizumab in a patient with retinal pigment epithelium detachment and tear. Eur J Ophthalmol. 2010;20(2):469–472. doi:10.1177/112067211002000235
15. Querques G, Souied EH, Soubrane G. Macular hole following intravitreal ranibizumab injection for choroidal neovascular membrane caused by age‐related macular degeneration. Acta Ophthalmol. 2009;87(2):235–237. doi:10.1111/j.1755-3768.2008.01226.x
16. Meyer PS, Kammann MT, Meyer CH. Vitrectomy in full thickness macular holes on top of a pigment epithelial detachment in age-related macular degeneration (AMD). Surgical consideration and review of the literature. Am J Ophthalmol Case Rep. 2021;23. doi:10.1016/j.ajoc.2021.101154
17. Geck U, Pustolla N, Baraki H, Atili A, Feltgen N, Hoerauf H. Posterior vitreous detachment following intravitreal drug injection. Graefes Arch Clin Exp Ophthalmol. 2013;251(7):1691–1695. doi:10.1007/s00417-013-2266-y
18. Kabanarou SA, Xirou T, Mangouritsas G, et al. Full-thickness macular hole formation following anti-VEGF injections for neovascular age-related macular degeneration. Clin Interv Aging. 2017;12:911–915. doi:10.2147/CIA.S135364
19. Chan CK, Abraham P, Meyer CH, et al. Optical coherence tomography-measured pigment epithelial detachment height as a predictor for retinal pigment epithelial tears associated with intravitreal bevacizumab injections. Retina. 2010;30:203–211. doi:10.1097/IAE.0b013e3181babda5
20. Mukherjee C, Mitra A, Kumar NA, Elsherbiny S, Lip PL. Macular hole formation after intravitreal ranibizumab injection in wet age-related macular degeneration. Open Ophthalmol J. 2015;9(1):177–180. doi:10.2174/1874364101509010177
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Short-Term Outcomes of 3 Monthly intravitreal Faricimab On Different Subtypes of Neovascular Age-Related Macular Degeneration
Tanaka A, Hata M, Tsuchikawa M, Ueda-Arakawa NUA, Tamura H, Miyata M, Takahashi A, Kido A, Muraoka Y, Miyake M, Ooto S, Tsujikawa A
Clinical Ophthalmology 2024, 18:507-516
Published Date: 20 February 2024