Back to Journals » Research and Reports in Urology » Volume 18
Fucoidan from Undaria pinnatifida Improves Benign Prostatic Hyperplasia Symptoms in Men: A Randomized, Double-Blind, Placebo-Controlled Study
Authors Wimmer BC ![]() , Dwan CA, Bhalerao SS, Gupta CG, Vaze SV, Kshirsagar SS
, Dwan CA, Bhalerao SS, Gupta CG, Vaze SV, Kshirsagar SS
Received 21 January 2026
Accepted for publication 11 June 2026
Published 15 July 2026 Volume 2026:18 597883
DOI https://doi.org/10.2147/RRU.S597883
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Barbara Caecilia Wimmer,1,* Corinna Anne Dwan,2,* Sagar Sudhir Bhalerao,3,* Chirag Govind Gupta,4,* Sanjay Vishnu Vaze,5,* Shalaka Sharad Kshirsagar5,*
1Marinova Pty Ltd, Cambridge, TAS, Australia; 2Marine Bioproducts Cooperative Research Centre, Kent Town, SA, Australia; 3Department of Urology, Bhalerao Clinics, Pune, MH, India; 4Department of Surgery, JNU Hospital, Jaipur, RJ, India; 5Department of Clinical Development, Vedic Lifesciences Pvt. Ltd, Mumbai, MH, India
*These authors contributed equally to this work
Correspondence: Shalaka Sharad Kshirsagar, Department of Clinical Development, Vedic Lifesciences Pvt. Ltd, Mumbai, MH, India, Tel +91 8082540039, Email [email protected]
Purpose: Benign Prostatic Hyperplasia (BPH) is a common non-malignant prostate enlargement that contributes to bladder outlet obstruction and lower urinary tract symptoms in men as they age.
Patients and Methods: In this 90-day study, ninety-five men aged 45– 80 years with clinically and radiologically confirmed moderate BPH [International Prostate Symptom Score (IPSS) between 8– 19] were randomly allocated (1:1) to receive either Undaria pinnatifida fucoidan (UPF) or placebo. Prostate health was evaluated using the validated IPSS (total and composite sub-scores) on days 30, 60 and 90. Potential clinically meaningful IPSS reductions were assessed as Minimum Clinically Important Difference (MCID). Urinary flow rate, post-void residual volume (PVR) and prostate-specific antigen were also assessed.
Results: By day 60, the UPF group showed significant improvement in total IPSS score compared to placebo (p=0.0234), with further improvements by day 90 (p=0.0015). The mean reduction in total IPSS score from baseline to day 90 was − 3.40 in the UPF group versus − 0.93 in the placebo group. Voiding (p=0.0006) and storage (p=0.0150), sub-scores improved significantly by day 90 in the UPF group. Quality of life related to urinary symptoms improved continuously by day 60 and 90 (both p< 0.05 vs placebo). A higher proportion of UPF-treated participants achieved MCID ≥ 2 (60.0%) and ≥ 3 points (51.1%) compared to placebo (42.2% and 28.9%), with statistical significance for ≥ 3 points (p=0.0314) at day 90. Urinary flow rate improved and PVR decreased in both groups; however, between-group differences, including PSA, were not statistically significant. Importantly, UPF was well tolerated.
Conclusion: UPF supplementation was associated with statistically and clinically significant IPSS improvement, including voiding and storage composite scores, and enhanced prostate-related quality of life when compared to placebo. Secondary outcomes did not differ significantly between groups, and the duration (90 days) limits long-term interpretation. UPF appears safe and potentially beneficial for managing moderate BPH symptoms.
Keywords: benign prostatic hyperplasia, fucoidan, international prostate symptom score, lower urinary tract symptoms, prostate health, Undaria pinnatifida
Introduction
Benign Prostatic Hyperplasia (BPH) is the benign enlargement of the prostate gland that compresses the urethra and hinders urine flow.1 It results from excessive growth of stromal and epithelial cells within the prostate’s transition zone, causing obstruction, insufficient bladder emptying, urine retention, infections, or Lower Urinary Tract Symptoms (LUTS). If untreated, chronic high-pressure retention may damage bladder detrusor muscle and cause serious complications.2 BPH prevalence increases with age, about 10% in men in their 30s to 90% in their 80s, contributing to healthcare expenses and reduced quality of life (QOL).3
BPH and LUTS often coexist in men.4 Symptoms are classified as obstructive (hesitancy, straining, poor urine flow, prolonged voiding, partial or total urine retention or overflow incontinence) and irritative (urinary frequency, urgency with urge incontinence, nocturia, dysuria and small voided volumes), which are bothersome and impair quality of life.5
Managing BPH is complex due to its multifactorial etiology.1 Current therapies include lifestyle modifications, surgery or medications such as α-blockers, 5α-reductase inhibitors (5-ARI), and phosphodiesterase inhibitors6 with 5-ARIs having a slower onset of action than α-blockers. α-blockers quickly improve voiding symptoms but may cause blood-pressure fluctuations and ejaculatory dysfunction.4,6 Despite established efficacy, pharmacological therapies such as α-blockers and 5-ARIs are limited by tolerability and patient acceptability, prompting interest in adjunctive approaches such as fucoidan, which requires rigorous clinical validation.
Currently, several nutraceuticals are marketed for BPH management, including Serenoa repens (Saw Palmetto), Cucurbita pepo (pumpkin), Solanum lycopersicum (tomato) and Urtica dioica (stinging nettle).7 Clinical evidence for these plants is mixed, with limited and inconsistent data on safety and efficacy.8 This emphasizes the need for well-designed clinical studies to assess new treatments with clinically meaningful benefits.
Sargassum horneri is a brown alga rich in polysaccharides such as fucoidan and nutrients. It has been shown to reduce the expression of key markers involved in BPH, including the androgen receptor, prostate-specific antigen (PSA), and 5α-reductase type 2 in vitro and in testosterone propionate-induced BPH models, suggesting its potential for managing BPH.9 However, these findings are based on in vitro and in vivo studies, and their relevance to clinically meaningful outcomes in humans remains uncertain.
Fucoidan, a complex polysaccharide predominantly found in brown seaweeds, has diverse bioactivities, including anti-inflammatory, antioxidant, immune-boosting, and anti-tumor properties.10–12 It blocks selectins and scavenger receptors to reduce inflammation by preventing neutrophil infiltration.13 Fucoidan also inhibits prostate cancer cell growth and enhances human immune cell activity.11 Prior research has demonstrated that consuming fucoidan is safe for both, healthy individuals14 and individuals with cancer.15
In a testosterone-induced rat BPH model, fucoidan from Undaria pinnatifida (UPF) reduced prostate weight, prostate index, testosterone, dihydrotestosterone, PSA, interleukin-1 beta (IL-β), and tumor necrosis factor-alpha (TNF-α) after 28 days. Additionally, UPF demonstrated potential pro-apoptotic qualities by regulating B-cell lymphoma-2 (BCL-2) and BCL-2-associated X protein expression, indicating its activity to alleviate BPH symptoms.16 Although these findings support potential therapeutic relevance, robust clinical data evaluating its efficacy in men with BPH are lacking.
Accordingly, this study was designed to evaluate whether UPF supplementation is associated with clinically meaningful improvements in BPH symptoms in men with moderate condition.
Materials and Methods
Participants
Men aged 45–80 years with clinically and radiologically confirmed BPH were enrolled. Participants had moderate BPH symptoms [International Prostate Symptom Score (IPSS) 8–19] and no prostate cancer symptoms as indicated by Prostatic Acid Phosphatase (PAP) ≤3 U/L], and exclusion of individuals with PSA ≥3.5 ng/mL. The use of PSA ensured exclusion of individuals at risk of prostate cancer, while PAP was included as an additional measure to rule out active or clinically significant disease. Detailed inclusion and exclusion criteria are provided in Table 1. Participants were randomized to UPF or placebo in 1:1 ratio using StatsDirect (v3.1.17). Allocation concealment was maintained using sequentially numbered study product containers prepared by personnel not involved in participant recruitment, assessment, or data analysis.
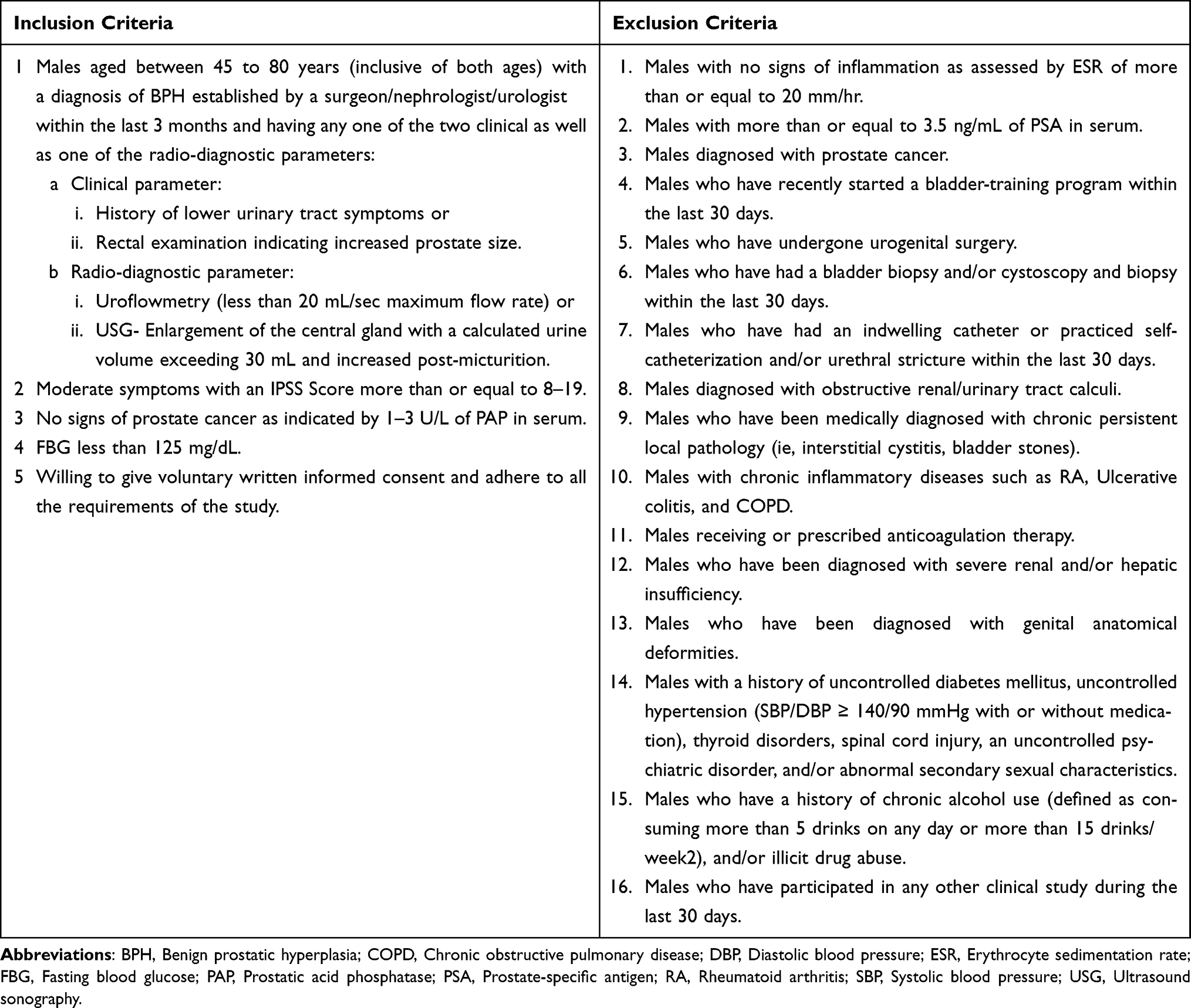 |
Table 1 Inclusion and Exclusion Criteria |
Intervention
UPF (Batch number UPF2023538), manufactured by Marinova Pty. Ltd. (Tasmania, Australia), was provided in capsules matched with placebo for size, shape, color, texture and packaging. Chemical composition and characterization of fucoidan is provided in Table 2.
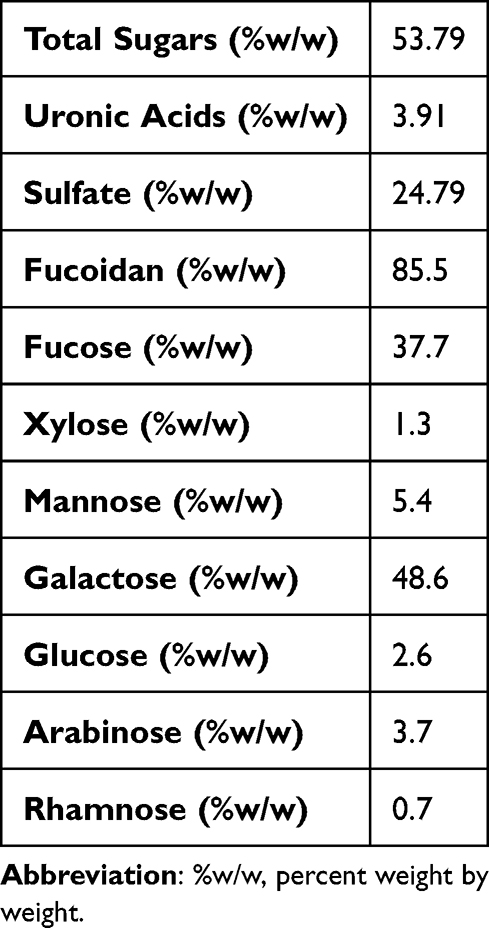 |
Table 2 Absolute Mass Percentages (%w/w) and Carbohydrate Breakdown of Neutral Carbohydrates in UPF Extract |
Each UPF capsule contained 500 mg fucoidan, placebo capsules contained 500 mg hydroxypropyl methylcellulose (Letco Medical, LLC). Participants took two capsules daily after breakfast with water. The selected dose of 1 g/day was based on previous clinical studies demonstrating the safety and biological activity of Marinova-derived UPF at similar doses (approximately 1–1.12 g/day).17–19 Additionally, efficacy of the same UPF extract was demonstrated in a testosterone-induced rat BPH model at 40 mg/kg and 400 mg/kg doses.16 Using the Reagan-Shaw body surface area conversion method, these correspond to approximately 400 mg/day and 4000 mg/day human equivalent doses, respectively.20 Therefore, 1 g/day was considered a biologically relevant and clinically feasible dose for this study. Administration of the full daily dose after breakfast was selected to support participant convenience and compliance during the 90-day intervention period, as current evidence does not indicate additional benefit with divided dosing. Adherence was measured by missed dose diaries and returned capsule counts (< 10% missed doses defined as compliant). Concomitant medications were recorded in source documents and Electronic-Case Record Forms. Participants, the research team, and investigators were blinded to allocation.
Study Conduct
During screening visit (day −14 to −2), procedures were thoroughly explained in plain language. IPSS was completed under investigator’s supervision. Blood samples were collected for Fasting Blood Glucose, Erythrocyte Sedimentation Rate, Prostate Specific Antigen (PSA) and PAP analysis. PSA and PAP assessments were completed using Roche Cobas Kits (Switzerland). Participants on BPH drugs/supplement, received 10-day washout before rescreening.
On day 0 uroflowmetry, Ultrasound sonography (USG) and PSA were conducted. A virtual visit on day 14 ensured IP compliance. Uroflowmetry, USG and PSA were repeated on day 90. IPSS was administered on-site on days 30, 60 and 90. Compliance, vital parameters, and adverse events were monitored throughout.
Outcome Measures
The primary outcome was to assess the effect of UPF on prostate health using the IPSS, a validated seven-item tool with a score for each question ranging from 0 to 5 for evaluating voiding and storage LUTSs linked to BPH.21,22 Additionally, IPSS voiding, storage sub-score and voiding-to-storage ratio were assessed using the formulae below:
Voiding Sub-score = Q1(Incomplete emptying) + Q3(Intermittency) + Q5(Weak stream) + Q6(Straining)
Storage Sub-score = Q2(Frequency) + Q4(Urgency)+ Q7(Nocturia)
IPSS Voiding-to-Storage Ratio= Voiding/Storage
To evaluate clinically meaningful responses from participant-centered perspectives, the study applied Minimum Clinically Important Difference (MCID) criteria. Severity-specific MCID was defined as ≥ 2-point reduction, and overall MCID as ≥ 3-point reduction in total IPSS.21,23
Secondary outcomes included urine flow rate, post-void residual volume (PVR) and PSA. Flow rate and PVR were assessed using uroflowmetry and ultrasonography, respectively.
Statistical Analysis
A sample size of 100 (minimum 80 completers; ≥ 40 per arm) was set via F-test-based power analysis [effect size (0.4), power (1-β) of 0.95 and α (0.05)]. A large effect size of Cohen’s f = 0.4 was selected based on Cohen’s conventional classification, where 0.10, 0.25, and 0.40 represent small, medium, and large effect sizes, respectively. Given the limited published clinical data available on fucoidan supplementation in patients with BPH, a large effect size was considered appropriate to detect a clinically meaningful difference in IPSS scores between treatment groups over the 90-day study duration. Continuous variables were summarized by frequency, mean, standard deviation (SD), and 95% confidence interval (CI); categorical variables using frequencies and percentages. Group differences were evaluated using t-test/Analysis of Variance (ANOVA) for continuous variables and Chi-Square/Fisher’s exact test for categorical variables. Changes from baseline to days 30, 60, and 90 were summarized by treatment group using mean, standard deviation, median, minimum, and maximum. A Mixed Model for Repeated Measures (MMRM) assessed between-group differences, including fixed effects for treatment, visit and treatment×visit, with baseline as a covariate when raw values were modeled. The MMRM approach inherently accommodates missing observations under the missing-at-random assumption; therefore, no additional imputation of missing data was performed. The primary efficacy analysis was based on total IPSS, which was predefined as the primary endpoint. Secondary outcomes were considered exploratory; therefore, adjustments for multiple comparisons were not applied. The study was powered to detect changes in the IPSS and not secondary objective outcomes such as urinary flow rate, PVR, or PSA. All statistical tests were performed at 0.05 significance level using the R/R Foundation for Statistical Computing, Vienna, Austria (https://www.r-project.org/version 4.4.1), and XLSTAT Statistical and Data Analysis Solution, New York, USA (https://www.xlstat.com./version [2021.3.1]). Safety and efficacy analyses used the safety set and Full Analysis Set (FAS), respectively.
Results
Demographic Characteristics of Participants
Participants had a mean age of 61.54 (8.55) years and Body Mass Index of 23.85 (3.56) kg/m2, with no statistically significant baseline differences between groups (Table 3).
 |
Table 3 Demographics and Baseline Characteristics |
Out of 134 screened participants, 95 were eligible and randomized and 88 completed the study as the Per Protocol (PP) population (Figure 1). More than 99% of IP compliance was observed throughout the study.
 |
Figure 1 Participant disposition. |
Primary Outcome
Prostate Health- IPSS
By day 60, total IPSS decreased by 1.98 (2.33) and 0.64 (2.66) units in the UPF and control group, respectively. Improvements were more than threefold in the UPF group with a statistically significant difference between the groups (p=0.0234). By day 90, the changes were [−3.40(3.32) units] and [−0.93(3.13) units] in the UPF and placebo group, respectively. The UPF group showed a significant difference between the groups (p=0.0015), suggesting that UPF was associated with improvement in BPH symptoms compared to placebo (Table 4).
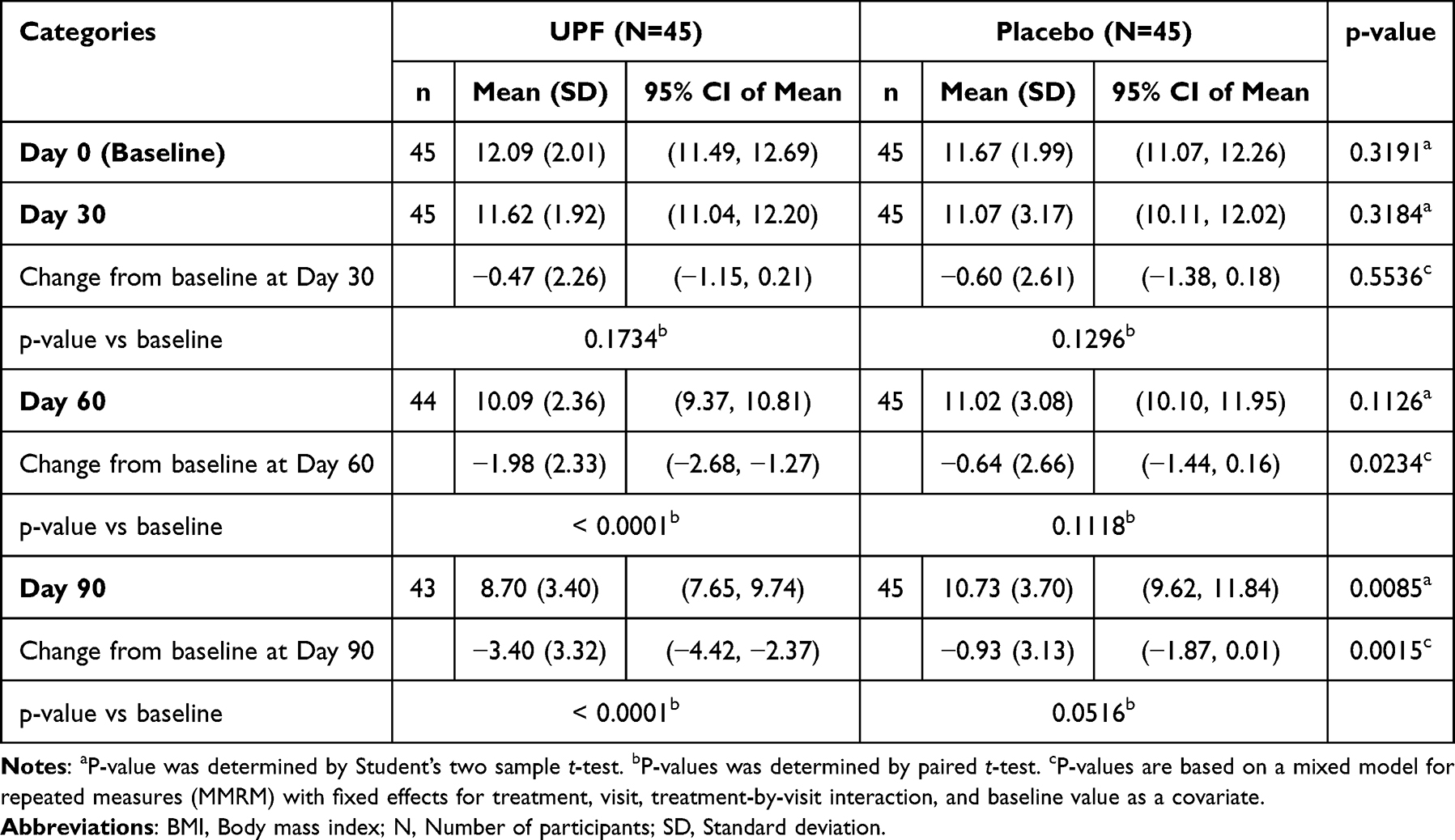 |
Table 4 International Prostate Symptom Score Total |
On day 30, the UPF group showed a statistically significant improvement (p=0.0398) in straining score compared to the placebo group.
On day 60, the UPF group showed statistically significant improvements in symptoms of incomplete emptying (p=0.0272), frequency (p=0.0361) and intermittency (p=0.0354) compared to the placebo group. Improvement in straining also favored the UPF group and approached statistical significance (p=0.0814).
On day 90, the UPF group demonstrated statistically significant improvements in incomplete emptying (p=0.0128), frequency (p=0.0025), intermittency (p=0.0128), and straining (p=0.0097) compared to the placebo group (Figure 2).
 |
Figure 2 Mean IPSS question-wise scores across study visits (UPF and placebo groups) [↔ indicates a significant difference between groups at a specific visit]. |
IPSS Voiding Sub-Score (IPSS-V)
By day 60, IPSS-V scores decreased in the UPF group but increased in the placebo group (p=0.0079). By day 90, voiding symptom reduction was nine-fold greater in the UPF group [−1.77(1.91)] versus placebo [−0.18(2.09)] (p=0.0006), indicating a significant improvement in voiding symptoms (Table 5).
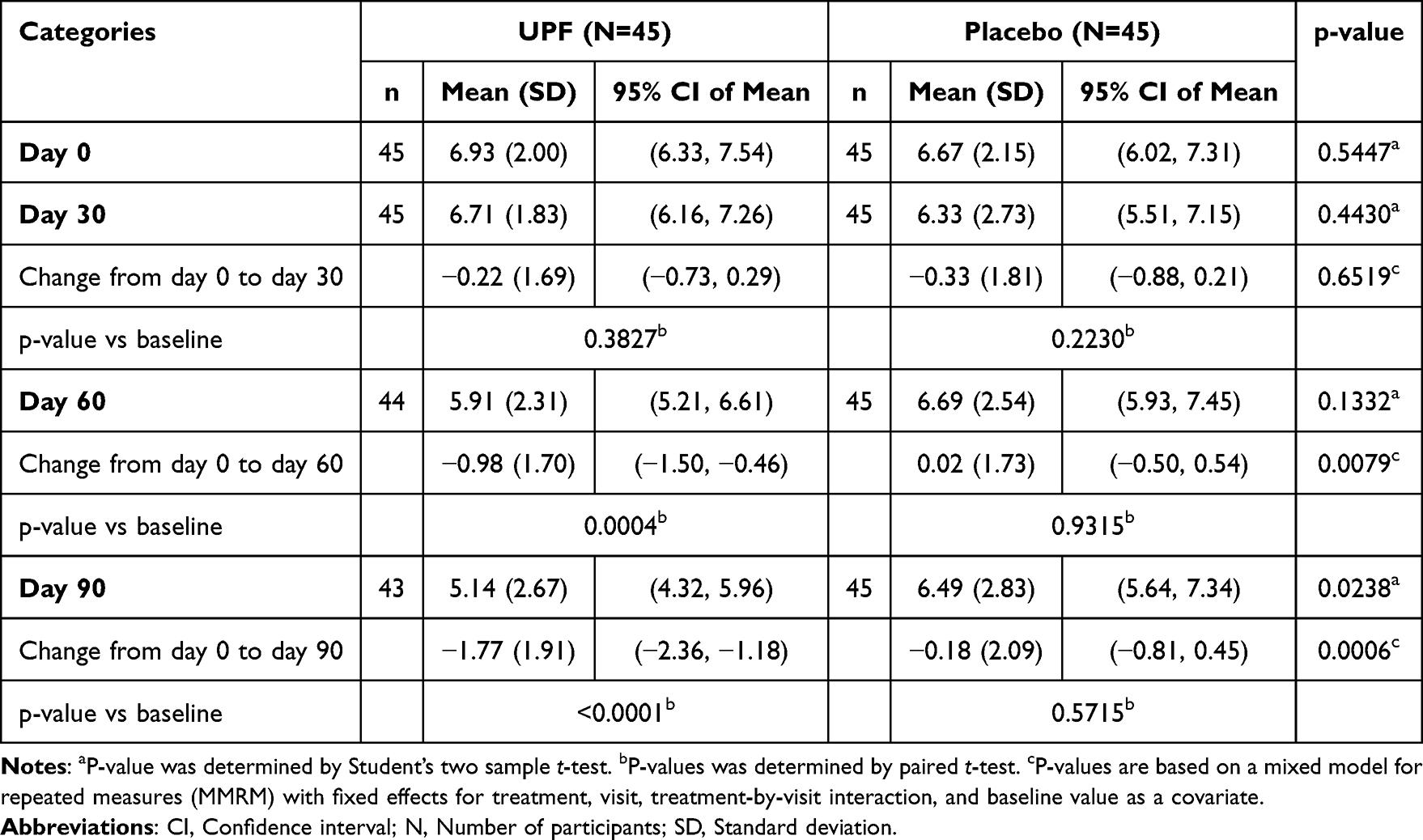 |
Table 5 International Prostate Symptom Score: Voiding Sub-Score |
IPSS Storage Sub-Score (IPSS-S)
The UPF group showed a greater reduction in IPSS-S scores throughout the study. By day 90, the decrease was more than double that of the placebo [−1.63(1.95) vs −0.76(1.64) units] with a significant between-group difference (p=0.0150), indicating improvement in storage symptoms (Table 6).
 |
Table 6 International Prostate Symptom Score: Storage Sub-Score |
IPSS Voiding-to-Storage Sub-Score Ratio (IPSS V/S)
On day 90, the UPF group maintained a stable IPSS V/S ratio of 1.48 units, reflecting balanced improvement in voiding and storage symptoms. The placebo group experienced a 0.25-unit increase, indicating greater improvement in storage than voiding (Table 7).
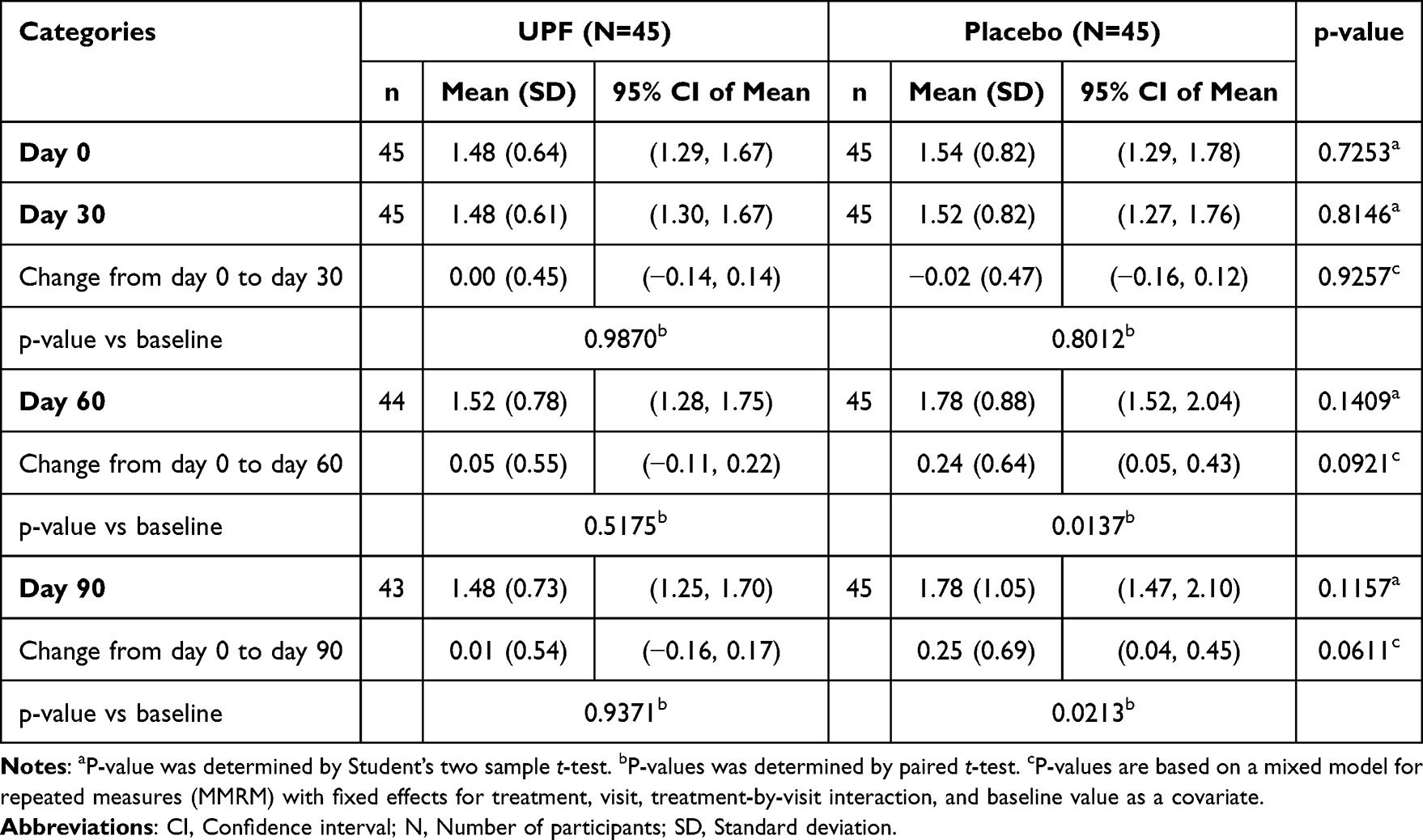 |
Table 7 International Prostate Symptom Score: Voiding-to-Storage Sub-Score Ratio |
IPSS Quality of Life
On day 60, the IPSS QoL scores improved in the UPF group [−0.55(1.15) units] from baseline, versus minimal change with placebo [−0.02(1.20) units], showing a statistically significant difference (p=0.0400). On day 90, the UPF group exhibited a larger reduction [−1.00(1.23) units] compared to no change with placebo [0.00(1.33) units] (p=0.0004), indicating meaningful QoL improvements (Table 8).
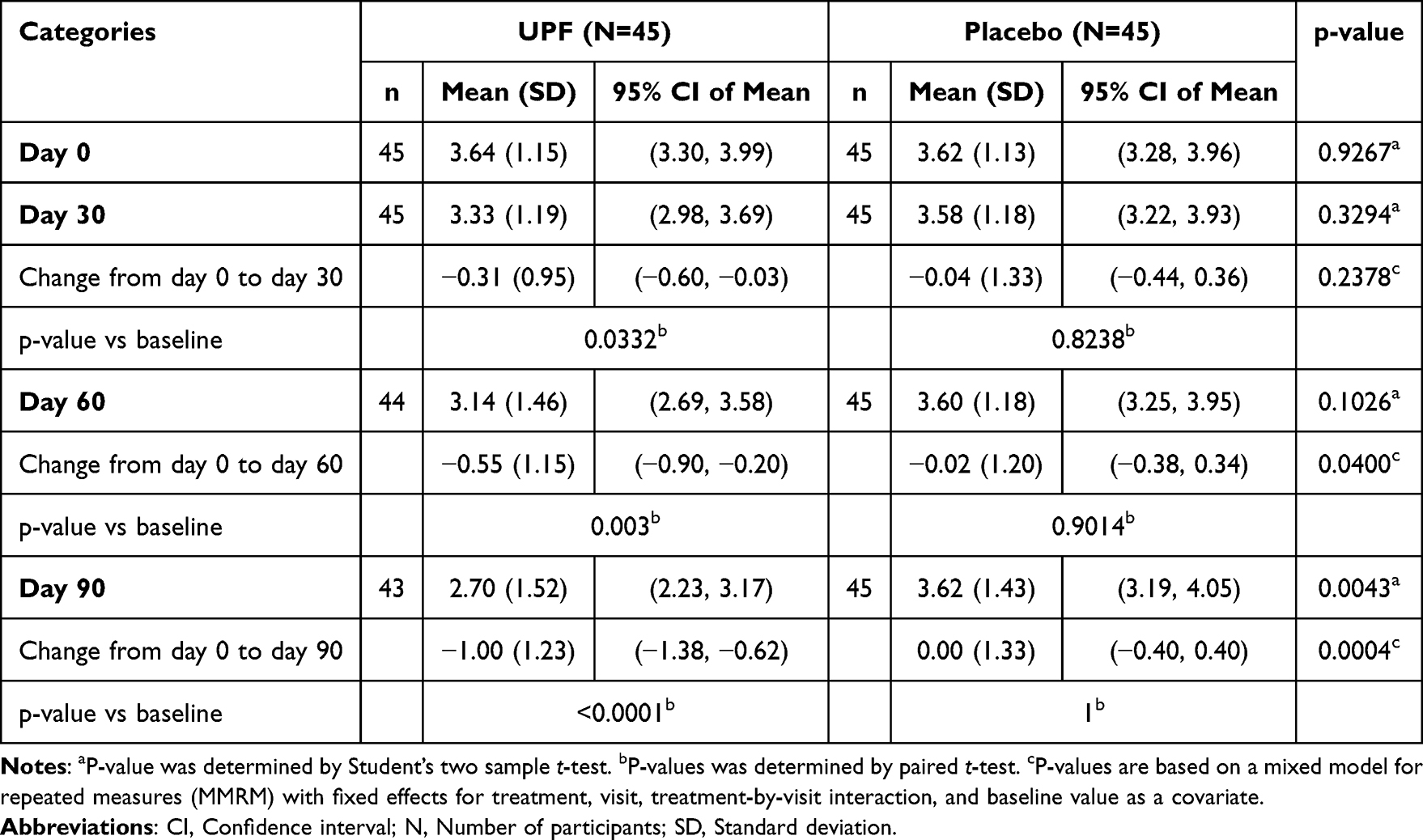 |
Table 8 International Prostate Symptom Score Quality of Life |
Severity MCID (≥ 2-Point Improvement in Total IPSS)
On day 30, 26.7% of UPF participants achieved the MCID vs 17.8% with placebo. By day 60, substantially more UPF participants had ≥2-point improvement (53.3% vs 31.1%; p=0.0328). By day 90, MCID achievement remained higher with UPF (60.0% vs 42.2%), supporting a clinically relevant improvement in LUTS (Figure 3).
 |
Figure 3 Percentage of participants achieving Severity MCID (≥2-point improvement in total IPSS scores) across study visits (UPF vs placebo groups) [* indicates significant difference between groups at a specific visit]. |
Overall MCID (≥ 3-Point Improvement in Total IPSS)
On day 60, the UPF group showed a more than twofold higher proportion achieving a ≥3-point IPSS improvement (35.6%) versus placebo group (15.6%; p=0.0296). On day 90, 51.1% of UPF participants met the MCID criteria with 28.9% in placebo (p=0.0314), suggesting sustained improvement in overall BPH symptom scores with UPF supplementation (Figure 4).
 |
Figure 4 Percentage of participants achieving Overall MCID (≥3-point improvement in total IPSS scores) across study visits (UPF vs placebo groups) [* indicates significant difference between groups at a specific visit]. |
Secondary Outcomes
Urinary Flow Rate
At the end of the study, the UPF group exhibited an increase in urinary flow rate of 1.13 (4.21) mL/s, compared to a minimal change of 0.09 (4.29) mL/s in the placebo group. Although numerical improvement was observed in the UPF group, the difference between groups was not statistically significant (p=0.1704) (Table 9).
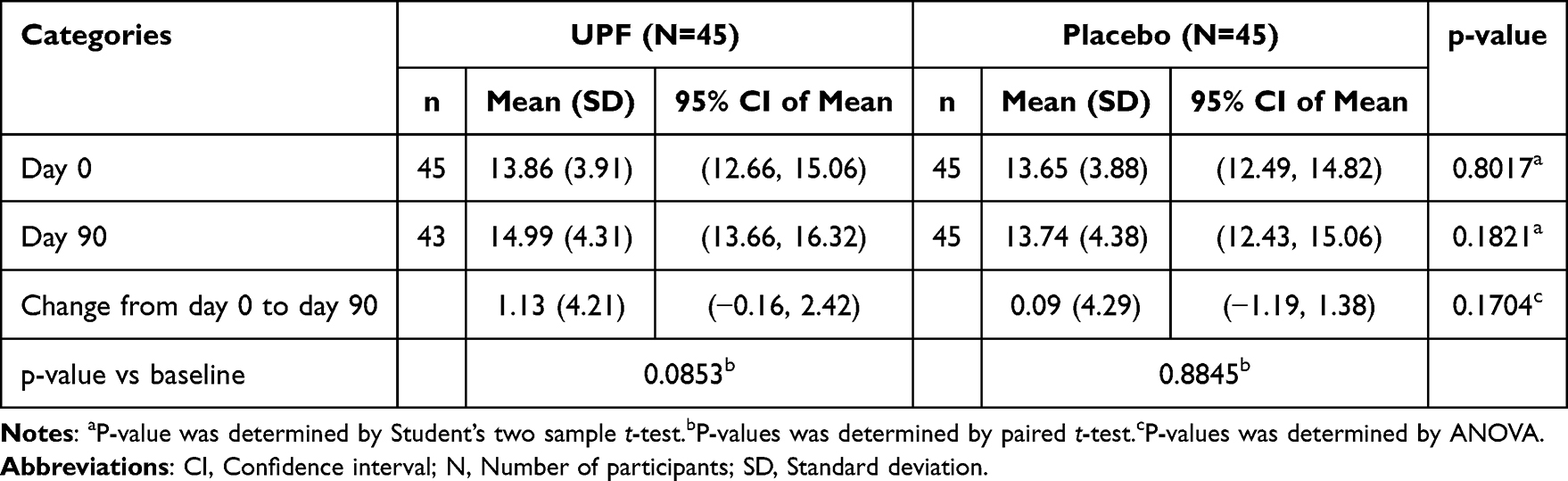 |
Table 9 Urinary Flow Rate |
Post Void Residual Urine (PVR)
At the end of the study, both groups showed reductions in PVR, with mean decreases of 14.26 (27.51) mL in the UPF group and 19.04 (50.86) mL in the placebo group. Within-group analyses revealed statistically significant reductions from baseline in both the UPF (p=0.0015) and placebo (p=0.0158) groups but no significant difference between the groups. The absence of significant between-group differences suggests limited effects of UPF on objective urinary parameters over 90-day study duration (Table 10).
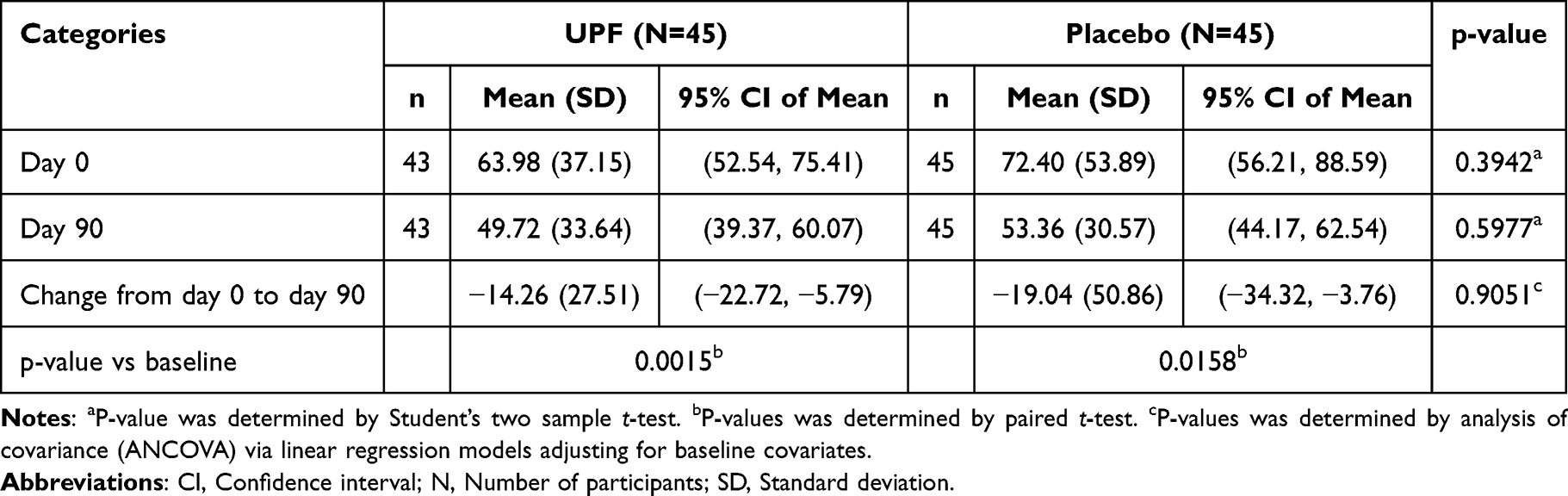 |
Table 10 Post Void Residual Urine |
Serum PSA
On day 90, the UPF group exhibited a minimal increase in PSA levels of 0.07 ng/mL, while the placebo group showed a slight decrease of (−0.14 ng/mL). However, the difference between groups was not statistically significant (p=0.8976), indicating no measurable effect of UPF supplementation on PSA levels during the study period (Table 11).
 |
Table 11 Serum Prostate Specific Antigen |
Safety Evaluations
The vital parameters such as pulse rate and blood pressure remained within normal limits throughout the duration of the study.
Adverse Events
A total of twenty-two adverse events were reported during the study: twelve in the UPF group, and ten in the placebo group. Only three of these events were potentially related to the study product as per investigators’ judgement: two instances of itching in the groin area in the intervention group were classified as “probable” and “possible”, while one case of rashes on the hands, back, and thigh in placebo group was deemed “probable” to the study product. However, all these events resolved without complications.
Discussion
UPF supplementation in this randomized, double-blind, placebo-controlled study significantly improved BPH-related symptoms and QOL. BPH symptoms measured by IPSS improved continuously over the 90-day study period. The UPF group demonstrated a threefold greater reduction in IPSS (16.38% vs 5.48%) by day 60. By day 90, the UPF group had a 28.12% decrease, compared to 7.97% in the placebo group. Importantly, the study was prospectively powered to detect changes in IPSS, the predefined primary endpoint, and clinically meaningful improvements were further supported by MCID analyses.
The IPSS is a standard tool for assessing BPH symptoms and treatment outcomes.21,22 Compared to other nutraceuticals, fucoidan showed strong efficacy. Its 28.12% IPSS reduction at day 90 exceeded 15.90% decrease reported with saw palmetto oil by Sudeep et al24 QOL improvement was also greater than that seen with Pycnogenol (1.0 vs 0.8-unit reduction).25 However, the magnitude of improvement observed in the present study should be interpreted within the context of a nutraceutical intervention and not as equivalent to established pharmacological therapies such as α-blockers or 5α-reductase inhibitors. Fucoidan significantly improved key voiding symptoms, including incomplete emptying, intermittency and straining. Although urgency, weak stream and nocturia did not reach statistical significance, positive trends favored UPF.
IPSS sub-scores assess BPH symptoms through voiding (IPSS-V) and storage (IPSS-S) components, covering incomplete emptying, intermittency, weak stream, straining, frequency, urgency and nocturia.26 UPF significantly reduced IPSS-V by day 60 (p=0.0079) and by 25.54% on day 90, compared with 2.70% observed in placebo (p=0.0006). IPSS-S improved by 31.59% in UPF versus 15.2% in placebo (p=0.0150) on day 90. These findings align with other research on IPSS sub-scores. A single-arm study of prostatic artery embolization in 43 BPH patients reported >50% reductions in both IPSS-V and IPSS-S at 3 months, with maximum improvement at 12 months, indicating benefits of longer follow-up.27 These findings demonstrate that fucoidan meaningfully improved both voiding and storage symptoms, highlighting its potential to address a broad range of LUTS in BPH.
The IPSS V/S ratio helps distinguish symptom patterns and guide treatment in male LUTS.26 Based on Liao et al, a stable IPSS V/S ratio reflects proportional changes in symptom domains. In this study, the maintained ratio of 1.48 on day 90, together with improvements in both voiding and storage sub-scores, indicates balanced improvement across LUTS domains. This aligns with pooled data from four RCTs on tadalafil, where the storage-to-total IPSS ratio remained constant between baseline and 12 weeks.28
Changes in IPSS indicate treatment effectiveness in LUTS or BPH, but the MCID reflects whether improvements are clinically meaningful.29 On day 90, more participants in the UPF group achieved clinically meaningful IPSS reductions than those on placebo: 60.0% reached a ≥2-point improvement (severity MCID) and 51.1% achieved a ≥3-point improvement (overall MCID), compared with 42.2% and 28.9% in the placebo group. The ≥3-point difference was significant (p=0.0314), supporting the clinical relevance of UPF. These findings also enable comparison with other treatments; for example, a study of minimally invasive BPH procedures reported ≥3-point MCID improvement was achieved in 82.2% men undergoing water vapor thermal therapy vs 79.5% of men with prostatic urethral lift after four years, underscoring the need for long-term data.30
Beyond the primary outcomes, the study evaluated urinary flow rate, PVR volume and PSA levels. Uroflowmetry is a standard diagnostic tool used to assess urinary flow, which is often impaired due to prostatic enlargement.31 At the end of the intervention, the UPF group demonstrated a notable rise in urinary flow rate [1.13(4.21) mL/s], approximately twelve times greater than in the placebo group [0.09(4.29) mL/s], indicating a clinically relevant benefit. Although the between-group difference was not statistically significant, the study was not powered to detect differences in these secondary objective measures. Therefore, the absence of statistical significance in secondary outcomes does not diminish the robustness of the primary IPSS findings. These findings align with in vivo evidence by Shanmugasundaram et al16 who found fucoidan administration reduced prostate weight and alleviated urinary obstruction in an animal model.
PVR volume, a marker of bladder emptying efficiency,32 reduced in both groups by day 90. The UPF group demonstrated a significant mean decrease of 14.26 mL (p=0.0015), while the placebo group showed a similar significant reduction of 19.04 mL (p=0.0158). These changes align with improvements in the IPSS incomplete emptying domain, suggesting perceived improvement in both groups. An RCT by Sudeep et al reported a 12.76 (14.44) mL PVR reduction after 12 weeks of saw palmetto oil administration.24 PSA, a glycoprotein secreted by the prostate and often elevated in BPH,33 showed increase of 0.07 ng/mL in the UPF group and a minor decrease of 0.14 ng/mL in the placebo group, with the values remaining within the reference range (<4 ng/mL). No significant between-group differences were observed in PSA levels during the study period. Importantly, improvement in BPH symptoms does not necessarily require concomitant reductions in PSA levels, as several interventions may improve LUTS independently of PSA modulation. A review by Grammatikopoulou et al also highlighted that symptomatic or clinical effects may occur without consistent alterations in PSA concentrations.34 Previous in vivo study by Shanmugasundaram et al showed lower PSA levels in fucoidan-treated animals (p<0.05).16
The molecular mechanisms underlying the observed symptomatic improvements with UPF are likely multifactorial. In vitro and in vivo evidence suggests that fucoidan modulates biological pathways relevant to BPH pathogenesis, including androgen signaling, apoptosis, inflammation, and gut microbiome activity. In a testosterone-induced rat model of BPH, UPF reduced dihydrotestosterone levels and modulated apoptosis-related proteins through downregulation of BCL-2 and upregulation of BAX, suggesting reduced prostatic hyperplasia.16 Fucoidan-treated animals also showed reductions in pro-inflammatory cytokines such as IL-1β and TNF-α,16 supporting its anti-inflammatory activity, which has additionally been reported in human and experimental studies.18,34
Emerging evidence further suggests a role for the gut–prostate axis in BPH. Recent in vitro findings demonstrated that UPF may enhance butyrate production through modulation of the gut microbiota.35 Since butyrate has been associated with anti-inflammatory effects and attenuation of prostate enlargement in inflammation-associated BPH models,36,37 these findings provide biologically plausible mechanisms through which UPF may contribute to symptomatic improvement. However, these mechanistic pathways remain exploratory in the context of human BPH and require further investigation.
Safety assessments, based on vital signs (pulse rate, systolic and diastolic blood pressure) and reported adverse events, indicated that UPF was safe and well-tolerated. Vital signs remained within normal limits, and all reported adverse events across both groups resolved by the end of the study.
A key strength of this study is the comprehensive evaluation of clinical outcomes using validated tools such as the IPSS questionnaire and MCID analysis to establish clinical relevance and quantify treatment responders. Additional strengths include the use of a well-characterized natural extract with an excellent safety profile and extensive safety data at doses of 1–3g/day.14,17–19 The 12-week duration was sufficient to identify changes in BPH symptoms, and adherence was high (99%), likely due to participants’ regular visits to urologists. However, the small sample size limits the generalizability, warranting larger, multicenter trials for confirmation. UPF alleviated symptoms, though molecular mechanisms were not explored. Future research should explore the biological pathways behind the symptom improvement.
Conclusion
UPF supplementation was well-tolerated and associated with improvement in BPH-related symptoms during the 90-day intervention period. Compared to placebo, UPF significantly improved total IPSS scores, including both voiding and storage sub-scores and QOL due to urinary symptoms in men. A greater proportion of participants receiving UPF also achieved clinically meaningful reductions in IPSS based on severity and overall MCID thresholds. Although favorable trends were observed for urinary flow rate and PVR, these secondary outcomes did not differ significantly between groups. Collectively, these findings support the potential of UPF as a safe nutraceutical approach for the management of moderate BPH symptoms. However, the relatively short study duration and modest sample size limit broader clinical interpretation, and larger, longer-term studies are needed to further establish its therapeutic role in relation to standard BPH management strategies.
Abbreviations
5-ARI, 5α-reductase inhibitors; ANOVA, Analysis of Variance; BCL-2, B-cell lymphoma-2; BPH, Benign Prostatic Hyperplasia; CI, confidence interval; FAS, Full Analysis Set; IL-β, interleukin-1 beta; IPSS V/S, IPSS voiding-to-storage sub-score ratio; IPSS, International Prostate Symptom Score; IPSS-S, IPSS storage sub-score; IPSS-V, IPSS voiding sub-score; LUTS, Lower Urinary Tract Symptoms; MCID, Minimum Clinically Important Difference; PAP, Prostatic Acid Phosphatase; PP, Per Protocol; PSA, Prostate-specific antigen; PVR, Post-void residual volume; QOL, Quality of Life; SD, standard deviation; UPF, Undaria pinnatifida fucoidan; USG, Ultrasound sonography.
Data Sharing Statement
The data used in the study are available on reasonable request from the corresponding author with due permission from the sponsor.
Ethics Approval and Informed Consent
This study followed the Declaration of Helsinki (2013 revision), International Conference on Harmonization Good Clinical Practice E6(R2) guidelines, and India’s National Ethical Guidelines for Biomedical and Health Research involving Human Participants [Indian Council of Medical Research, 2017] guidelines. The protocol was reviewed and approved by multiple Ethics Committees across India, namely Royal Pune Independent Ethics committee, Gillurkar Hospital Ethics Committee, Rising Medical Care Hospital and IEC, Anand Institutional Ethics Committee, JNU Hospital Institutional Ethics committee, Skinovate Independent Ethics committee. Written informed consent was obtained from all participants before conducting any study-related procedures. The study was registered prospectively with NIH ClinicalTrials.gov (NCT06487871) and Clinical Trials Registry India (Registration Number: CTRI/2024/07/071419) and conducted from August 2024 to April 2025. The study was monitored by Vedic Lifesciences (Mumbai, India) to ensure protocol and ICH-GCP E6(R2) guidelines compliance.
Acknowledgments
The authors are grateful to all participants for their invaluable time and contributions to the study. UPF and funding were provided by the trial sponsor Marinova Pty Ltd., Cambridge, Australia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Marinova Pty Ltd. provided financial support and investigational products for the trial.
Disclosure
At the time the study was planned and conducted, Corinna Dwan and Barbara Wimmer were employees of Marinova Pty Ltd. They were involved in the study conceptualization and manuscript review but were not involved in study conduct, data management or statistical analysis. Sanjay Vaze and Shalaka Kshirsagar are employees of Vedic. Sanjay Vaze was involved in study planning, conduct, data management and statistical analysis, while Shalaka Kshirsagar contributed to manuscript preparation and coordination activities. Sagar Bhalerao and Chirag Gupta are affiliated with clinics that contributed to the study’s conduct under the supervision of Vedic Lifesciences (Contract Research Organization), with incentives provided according to the terms of the clinical research agreement by Vedic Lifesciences. The authors report no other financial or non-financial conflicts of interest related to this work.
References
1. Parsons JK. Benign prostatic hyperplasia and male lower urinary tract symptoms: epidemiology and risk factors. Curr Bladder Dysfunct Rep. 2010;5(4):212–16. doi:10.1007/s11884-010-0067-2
2. Roehrborn CG. Pathology of benign prostatic hyperplasia. Int J Impot Res. 2008;20(Suppl 3):S11–S18. doi:10.1038/ijir.2008.55
3. Bhat SA, Rather SA, Islam N. An overview of benign prostatic hyperplasia and its appreciation in Greco-Arab (Unani) system of medicine. Asian J Urol. 2022;9(2):109–118. doi:10.1016/j.ajur.2021.05.008
4. Park HJ, Won JE, Sorsaburu S, Rivera PD, Lee SW. Urinary Tract Symptoms (LUTS) Secondary to Benign Prostatic Hyperplasia (BPH) and LUTS/BPH with Erectile Dysfunction in Asian Men: a Systematic Review Focusing on Tadalafil. World J Mens Health. 2013;31(3):193–207. doi:10.5534/wjmh.2013.31.3.193
5. Roehrborn CG. Benign prostatic hyperplasia: an overview. Rev Urol. 2005;9(Suppl 9):S3–S14.
6. Sandhu JS, Bixler BR, Dahm P, et al. Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia (BPH): AUA guideline amendment 2023. J Urol. 2024;211(1):11–19. doi:10.1097/JU.0000000000003698
7. Csikós E, Horváth A, Ács K, et al. Treatment of benign prostatic hyperplasia by natural drugs. Molecules. 2021;26(23):7141. doi:10.3390/molecules26237141
8. Antoniou V, Gauhar V, Modi S, Somani BK. Role of phytotherapy in the management of bph: a summary of the literature. J Clin Med. 2023;12(5):1899. doi:10.3390/jcm12051899
9. Kim Y, Kim K, Kim H, et al. Sargassum horneri extract alleviates testosterone-induced benign prostatic hyperplasia in vitro and in vivo. J Aquat Food Prod Technol. 2022;31(10):1049–1060. doi:10.1080/10498850.2022.2132126
10. Ahmad T, Eapen MS, Ishaq M, et al. Anti-inflammatory activity of fucoidan extracts in vitro. Mar Drugs. 2021;19(12):702. doi:10.3390/md19120702
11. Park AY, Nafia I, Stringer DN, Karpiniec SS, Fitton JH. Fucoidan independently enhances activity in human immune cells and has a cytostatic effect on prostate cancer cells in the presence of nivolumab. Mar Drugs. 2021;20(1):12. doi:10.3390/md20010012
12. Yang C, Dwan C, Wimmer BC, et al. Anti-inflammatory and neuroprotective effects of Undaria pinnatifida fucoidan. Mar Drugs. 2025;23(9):350. doi:10.3390/md23090350
13. Baba M, Snoeck R, Pauwels R, De Clercq E. Sulfated polysaccharides are potent and selective inhibitors of various enveloped viruses, including herpes simplex virus, cytomegalovirus, vesicular stomatitis virus, and human immunodeficiency virus. Antimicrob Agents Chemother. 1988;32(11):1742–1745. doi:10.1128/AAC.32.11.1742
14. Irhimeh MR, Fitton JH, Lowenthal RM. Fucoidan ingestion increases the expression of CXCR4 on human CD34+ cells. Exp Hematol. 2007;35(6):989–994. doi:10.1016/j.exphem.2007.02.009
15. Suzuki N, Uebaba K, Han S, et al. The safety and immune-efficacy of fucoidan from Gagome kombu (Kjellmaniella crassifolia) on the elderly. Jpn J Complement Altern Med. 2012;9:149–155.
16. Shanmugasundaram D, Dwan C, Wimmer BC, Srivastava S. Fucoidan Ameliorates Testosterone-Induced Benign Prostatic Hyperplasia (BPH) in Rats. Res Rep Urol. 2024;16:283–297. doi:10.2147/RRU.S478740
17. Cooper R, Dragar C, Elliot K, Fitton JH, Godwin J, Thompson K. GFS, a preparation of Tasmanian Undaria pinnatifida is associated with healing and inhibition of reactivation of Herpes. BMC Complement Altern Med. 2002;2:11. doi:10.1186/1472-6882-2-11
18. Cox AJ, Cripps AW, Taylor PA, Fitton JH, West NP. Fucoidan supplementation restores fecal lysozyme concentrations in high-performance athletes: a pilot study. Mar Drugs. 2020;18(8):412. doi:10.3390/md18080412
19. McFadden BA, Vincenty CS, Chandler AJ, et al. Effects of fucoidan supplementation on inflammatory and immune response after high-intensity exercise. J Int Soc Sports Nutr. 2023;20(1):2224751. doi:10.1080/15502783.2023.2224751
20. Reagan-Shaw S, Nihal M, Ahmad N. Dose translation from animal to human studies revisited. FASEB J. 2008;22(3):659–661. doi:10.1096/fj.07-9574LSF
21. Barry MJ, FJ F Jr, O’Leary MP, et al. The American Urological Association symptom index for benign prostatic hyperplasia. the measurement committee of the American urological association. J Urol. 1992;148(5):1549–1564. doi:10.1016/S0022-5347(17)36966-5
22. Taneja Y, Ram P, Kumar S, et al. Comparison of visual prostate symptom score and international prostate symptom score in the evaluation of men with benign prostatic hyperplasia: a prospective study from an Indian population. Prostate Int. 2017;5(4):158–161. doi:10.1016/j.prnil.2017.04.004
23. Fusco F, D’Anzeo G, Henneges C, Rossi A, Büttner H, Nickel JC. Predictors of individual response to placebo or tadalafil 5mg among men with lower urinary tract symptoms secondary to benign prostatic hyperplasia: an integrated clinical data mining analysis. PLoS One. 2015;10(8):e0135484. doi:10.1371/journal.pone.0135484
24. Sudeep HV, Thomas JV, Shyamprasad K. A double blind, placebo-controlled randomized comparative study on the efficacy of phytosterol-enriched and conventional saw palmetto oil in mitigating benign prostate hyperplasia and androgen deficiency. BMC Urol. 2020;20(1):86. doi:10.1186/s12894-020-00648-9
25. Yagi H, Sato R, Nishio K, Arai G, Soh S, Okada H. Effects of a supplement combining Pycnogenol® and l-arginine aspartate on lower urinary dysfunction compared with saw palmetto extract. J Tradit Complement Med. 2016;7(1):117–120. doi:10.1016/j.jtcme.2016.05.008
26. Liao CH, Kuo HC. Use of the international prostate symptom score voiding-to-storage subscore ratio in assessing lower urinary tract symptoms. Tzu Chi Med J. 2014;26(2):61–63. doi:10.1016/j.tcmj.2014.05.008
27. Maclean D, Kong M, Lim J, et al. Does Prostate Artery Embolization (PAE) Improve Voiding Symptoms, Storage Symptoms, or Both? Cardiovasc Intervent Radiol. 2020;43(1):23–28. doi:10.1007/s00270-019-02298-3
28. Chapple CR, Roehrborn CG, McVary K, Ilo D, Henneges C, Viktrup L. Effect of tadalafil on male lower urinary tract symptoms: an integrated analysis of storage and voiding international prostate symptom subscores from four randomised controlled trials. Eur Urol. 2015;67(1):114–122. doi:10.1016/j.eururo.2014.08.072
29. Babar M, Abramson M, Labagnara K, et al. Predictors of achieving a minimal clinically important difference in lower urinary tract symptoms 3 months after Rezum therapy. Cent European J Urol. 2024;77(2):262–272. doi:10.5173/ceju.2023.256
30. Miller LE, Te AE, Bhattacharyya SK, Lilienfeld S, Dornbier RA, McVary KT. A novel metric for treatment durability in clinical trials of minimally invasive treatments for benign prostatic hyperplasia. Expert Rev Med Devices. 2020;17(4):365–369. doi:10.1080/17434440.2020.1742699
31. Sinha S. The use of uroflowmetry as a diagnostic test. Curr Urol Rep. 2024;25(5):99–107. doi:10.1007/s11934-024-01200-0
32. Chung D, Te A, Tyagi R. Lower urogenital tract dysfunction in men and women. In: Legato MJ, editor. Principles of Gender-Specific Medicine.
33. McNally CJ, Ruddock MW, Moore T, McKenna DJ. Biomarkers that differentiate benign prostatic hyperplasia from prostate cancer: a literature review. Cancer Manag Res. 2020;12:5225–5241. doi:10.2147/CMAR.S250829
34. Grammatikopoulou MG, Gkiouras K, Papageorgiou ST, et al. Dietary factors and supplements influencing prostate specific-antigen (psa) concentrations in men with prostate cancer and increased cancer risk: an evidence analysis review based on randomized controlled trials. Nutrients. 2020;12(10):2985. doi:10.3390/nu12102985
35. Wimmer BC, Dwan C, De Medts J, Duysburgh C, Rotsaert C, Marzorati M. Undaria pinnatifida fucoidan enhances gut microbiome, butyrate production, and exerts anti-inflammatory effects in an in vitro short-term shime® coupled to a caco-2/thp-1 co-culture model. Mar Drugs. 2025;23(6):242. doi:10.3390/md23060242
36. Xu Y, An L, Xie J, Luo C, Huang X, Luo G. The gut-prostate axis in benign prostatic hyperplasia: systematic review of microbial dysbiosis and pathogenic mechanisms. BMC Urol. 2026;26(1):26. doi:10.1186/s12894-025-02003-2
37. Chen J, Chen B, Lin B, et al. The role of gut microbiota in prostate inflammation and benign prostatic hyperplasia and its therapeutic implications. Heliyon. 2024;10(19):e38302. doi:10.1016/j.heliyon.2024.e38302
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The P.R.OS.T.A.T.E Nomogram for the Preoperative Prediction of Clinical Efficacy of Transurethral Resection of the Prostate in Benign Prostatic Hyperplasia Patients
Tian Y, Zhang H, Cao Y, Yang L, Luo G
Clinical Interventions in Aging 2022, 17:845-855
Published Date: 23 May 2022
Correlation Between Benign Prostatic Hyperplasia/Lower Urinary Tract Symptoms and Renal Function in Elderly Men Aged 80 Years and Older
Wang Q, Zhang B, Li B, Yang S, Wang Z, Han C, Wu J, Tian R
Clinical Interventions in Aging 2023, 18:61-69
Published Date: 13 January 2023
The Relationship Between Immune-Inflammatory Indexes and the Severity of Lower Urinary Tract Symptoms/Benign Prostatic Hyperplasia: A Cross-Sectional Study at a Tertiary Hospital in China
Wu Y, Sheng J, Liu X, Huang Y, Zhang Y, Feng N
Journal of Inflammation Research 2025, 18:8509-8523
Published Date: 27 June 2025