Back to Journals » International Journal of Women's Health » Volume 17
Frontier and Inequality Analyses of the Global Burden of Ectopic Pregnancy: Insights from the GBD 2021
Received 10 September 2025
Accepted for publication 25 December 2025
Published 31 December 2025 Volume 2025:17 Pages 5807—5823
DOI https://doi.org/10.2147/IJWH.S566659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Xiaowei Cao, Zhuying Yu, Shengsheng Wu
Department of Gynecology, Meizhou People’s Hospital, Meizhou, Guangdong Province, 514031, People’s Republic of China
Correspondence: Shengsheng Wu, Email [email protected]
Objective: Ectopic pregnancy (EP) is a significant global health concern and is associated with maternal mortality and compromised future fertility. This research aims to refine the assessment of EP’s global impact and its associated inequalities.
Methods: EP’s incidence, prevalence, mortality, and disability-adjusted life years (DALYs) were analyzed using the data from the Global Burden of Disease study from 1990 to 2021. Decomposition analysis was performed to examine the roles of ageing, population growth, and epidemiological changes. Novel frontier and health inequality analyses (Slope Index of Inequality, Concentration Index) were conducted to evaluate socio-demographic disparities.
Results: From 1990 to 2021, the global age-standardized incidence rate (ASIR) decreased from 305.9 to 212.87 per 100,000. However, absolute DALYs increased from 288,083 to 396,856, with the highest burden shifting to the 20– 24 age group. Health inequality analysis revealed a significant but narrowing absolute disparity (SII: − 56.68 to − 36.56), while frontier analysis identified sub-Saharan African nations with the largest unmet potential for health improvement. Decomposition showed that population growth and epidemiological changes were primary drivers of rising DALYs.
Conclusion: Declining EP incidence masks increasing absolute burden and persistent severe inequities. Our findings underscore an urgent public health imperative: to implement equity-focused interventions that enhance early diagnosis, safe management, and the preservation of fertility, particularly in low-resource settings.
Plain Language Summary: EP has posed a considerable health challenge, especially in areas defined by low- and middle-income status. This study analyzes the GBD data from 1990 to 2021 to provide updated estimates related to the incidence, prevalence, mortality, and DALYs associated with EP. Our comprehensive examination indicated a reduction in the occurrence of EP; however, there is an accompanying increase in the overall mortality and years lived with disability, underscoring persistent challenges in this domain. This work reveals significant health disparities across different regions globally and highlights the necessity for enhancing reproductive health services and implementing targeted interventions to improve outcomes for women impacted by EP worldwide.
Keywords: disability-adjusted life years, ectopic pregnancy, global burden of disease, health inequality
Introduction
Ectopic pregnancy (EP) represents a significant concern in the fields of obstetrics and gynecology, characterized by the implantation of a developing blastocyst in a location outside the uterine cavity, most commonly within the fallopian tube.1 The underlying pathophysiology involves functional or anatomical impairment of fallopian tube transport, frequently linked to prior pelvic inflammatory disease, tubal surgery, or endometriosis, which can disrupt embryo migration and lead to ectopic implantation.2,3 It has been estimated that EP occurs in about 1–2% of all pregnancies all over the world.4 Although most EPs originate in the fallopian tubes, they can also be found at other sites such as the cervix, ovaries, abdominal cavity, and even at the site of old cesarean scars.5 The clinical presentation of EP can range from asymptomatic to severe presenting symptoms of abdominal pain to life-threatening complications such as hemodynamic shock; hence, it is considered one of the major challenges faced by obstetricians and gynecologists.1 Diagnosis relies on serial beta-human chorionic gonadotropin (β-hCG) monitoring and transvaginal ultrasonography, with management ranging from medical treatment with methotrexate to surgical intervention, guided by the patient’s hemodynamic stability and desire for future fertility.2,3 However, it is equally important to note that EP accounts for 10–15% of maternal deaths, especially in resource-limited settings.1,6
Critically, the burden of EP extends beyond acute morbidity and mortality. A recent meta-analysis underscores that EP history is related to long-term reproductive sequelae, including a significantly elevated risk of recurrent ectopic pregnancy, infertility, and adverse outcomes in subsequent pregnancies (eg, preterm birth and placental disorders).2 This highlights that the true impact of EP encompasses both immediate safety and long-term reproductive potential, contributing to its substantial disease burden.
Despite the high burden associated with EP, most studies conducted to date have been regional, single-center analyses7–10 with limited generalizability.7–10 In such studies, population sample sizes and temporal spans are typically small, preventing an overview of EP incidence trends over time. Consequently, there is now an urgent need for deeper and broader data to further inform our understanding of this condition. Fortunately, advances in public databases and data mining techniques now enable the extraction of potentially valuable insights from large datasets to further advance clinical applications.11,12 The Global Burden of Disease (GBD) study presently offers comprehensive epidemiological estimates, including the global age-standardized incidence rate (ASIR) and the age-standardized disability-adjusted life years rate (ASDR), for assessing the effects of EP and the effectiveness of associated prevention and treatment strategies.
The disparities in EP outcomes are profoundly influenced by socio-economic determinants. Access to essential healthcare services—including early diagnostic tools like ultrasound, timely surgical intervention for ruptured cases, and comprehensive fertility care—varies dramatically across socio-demographic index (SDI) quintiles.13 These inequities directly contribute to the higher rates of mortality and long-term morbidity observed in low-resource settings. Therefore, addressing this burden is integral to achieve the Sustainable Development Goals (SDGs), particularly SDG 3.1, which aims to reduce the global maternal mortality ratio, and SDG 3.7. This ensures universal access to sexual and reproductive healthcare services.14
EP research is crucial within the GBD framework. These in-depth studies at the global, regional, and national levels of burden will enlighten the present situation and reveal emerging trend to inform public health strategies and reproductive health policies. More particularly, the literature observes limited knowledge regarding global and country-specific epidemiological trends of EP due to scarce available data.15,16 This study aims to address this gap by utilizing GBD data to illustrate trends in the burden of the condition over a period of more than three decades, from 1990 to 2021, focusing on incidence, prevalence, mortality, and disability-adjusted life years (DALYs). This paper represents the first comprehensive global analysis of EP that utilizes the GBD 2021 dataset and integrates novel analytical approaches, including decomposition analysis to quantify the drivers of DALY changes and frontier analysis to identify countries with the largest unrealized health potential. In addition, health inequalities related to EP burden were assessed using the established metrics to illustrate differences across different SDI quintiles. The purpose of this research paper is to present key insights to inform public health responses and clinical practice toward improved reproductive health outcomes and specific interventions to lower the impact of EP on women’s health worldwide.
Methods
Data Source
This study utilized data collected as part of the GBD 2021 initiative. Comprehensive global burden estimates of diseases, injuries, and risk factors were shown in this study. The GBD 2021 study estimated 204 countries and territories using data from various sources. These included vital registration systems, health data from hospitals and outpatient centers, epidemiological surveys, and published studies. Data were categorized for 371 diseases and injuries and 88 risk factors, disaggregated by sex, age group, and geographic region.17 EP is characterized by implantation of the fertilized ovum outside the uterine cavity, predominantly in the fallopian tubes, particularly the ampulla region. Mothers often experience serious illness or even death as a result.18 GBD cause code A.6.1.6, ICD-10 codes O00.0-O00.2, and O00.8-O00.9.
The estimates in GBD 2021 were developed using advanced statistical modeling. The research relied on DisMod-MR and the Cause of Death Ensemble model (CODEm), which are common standardization tools. As a Bayesian meta-regression tool, DisMod-MR improves consistency when analyzing all available data on the incidence, prevalence, remission, and mortality rates of a specific disease, which are important epidemiological parameters.19 For analyzing data on causes of mortality, CODEm is a sophisticated instrument for analyzing data on causes of mortality. A combination of different modeling approaches was used to determine which covariates best suit out-of-sample prediction validity testing and ratio or cause-score analysis.20,21
To achieve this goal, information about GBD 2021 was retrieved from the open-access repository for global health data known as the Global Health Data Exchange (GHDx). Additionally, EP data on incidence, prevalence, mortality, and DALYs for the period of 1990–2021, on a global, regional, and age-stratified national level, were extracted using the GHDx GBD Results Tool (http://ghdx.healthdata.org/gbd-results-tool). This allowed for an accurate portrayal of the disease’s burden. Both the SDI categories and the 21 GBD regions were used to stratify the data.
The GBD 2021 study adhered to the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) as standard practice to ensure that modeling of global health metrics is transparent and can be reproduced. The GATHER statement outlines suggested best practices for reporting health estimates, including standardization of data sources and full reporting of methodological approaches.22 Data for this study was retrieved according to the GBD study protocol to ensure the ethical use of publicly available data. No individual-level data were used, and no ethical approval was required for the secondary use of GBD estimates.
Statistical Analysis
The methodology of the 2021 GBD study has been extensively documented in prior research.23 In this analysis, a 95% uncertainty interval (UI) was computed for each metric. Rates are presented as occurrences per 100,000 individuals. P < 0.05 were deemed significant.
Study Population and Age-Standardization
This study focused exclusively on the female population. All estimates, including incidence, prevalence, mortality, and DALYs, are specific to females. The age-standardized rates (ASIR, ASPR, ASMR, ASDR) were calculated using the GBD standard female population to ensure comparability across different regions and over time. Although the burden of EP is concentrated in the reproductive age groups (15–49 years), the age-standardization process accounts for the entire age structure to provide unbiased comparisons.24
Handling of Missing or Sparse Data
The GBD modeling framework, through DisMod-MR and CODEm, is specifically designed to address the challenges of missing, sparse, or heterogeneous data from different sources.25 These models use spatiotemporal Gaussian process regression and covariate analysis to borrow strength from data-rich locations and years to inform estimates in data-sparse settings.26 This approach ensures that all estimates across the study period and across all 204 countries and regions are complete and comparable, even when direct empirical data are unavailable for certain countries or years.
Additional Analytical Methods
Estimated annual percentage change (EAPC) was selected as a metric to monitor the changes in metrics like incidence and prevalence rates across specific time frames. Prevalence, incidence, mortality, and DALY rates of EP from 1990 to 2021 across different regions were estimated. A linear equation including the natural logarithm of each rate was fitted to a regression model using time as the independent variable to compute the EAPC. This procedure determines the EAPC by utilizing the slope of the regression line, which is represented as y = α + βx + ε, where x represents the year, y for the natural logarithm of the rate, α for the intercept, β for the slope, and ε for the random error. The EAPC is further expressed as 100×(exp(β) −1).27 Following this model, the EAPC’s 95% confidence intervals (CIs) was derived. The interpretation of trend results was obtained based on the 95% CIs. If the lower bound of the 95% CI is greater than 0, an increasing trend is indicated; if the upper bound is less than 0, a decreasing trend is suggested. If the 95% CI includes 0, it implies no statistically significant difference in the trend.28
From 1990 to 2021, decomposition analysis was carried out to understand how changes in DALYs were influenced by ageing, population increase, and epidemiological alterations. Here, the changes in mortality and morbidity rates after adjusting for population size are relevant to epidemiology.29 Frontier analysis was used to investigate the correlation between the burden of EP and sociodemographic developments. To establish a nonlinear frontier that represents the minimal feasible load in respect to development state, we followed the approaches in past work and conduct non-parametric data envelope analysis.30,31 Effective differences, defined as the gap between a region’s observed DALY rate and its frontier, measure unrealized health improvements relative to the region’s or country’s current development level.
Inequality was examined using both total DALYs and DALYs rates. Following the recommendations of the World Health Organization, two widely-used measures, the Slope Index of Inequality (SII) and Concentration Index, were employed to evaluate absolute and relative disparities among nations with respect to income.32–34 The slope of the regression line that connects each country’s weighted rank with its DALYs rate for EP was determined by the SII. Dividing the global DALYs rate by the SII yields a relative inequality index, facilitating more equitable distribution of burden levels. To determine how different nations’ EP burdens compare, the Concentration Index uses data fitting techniques on the Lorenz concentration curve, which shows the relationship between cumulative DALYs and cumulative population. A positive concentration index indicates a higher burden of EP in countries with lower SDI; ranging from −1 to 1, it quantifies the area under this curve.
Uncertainty Intervals and Statistical Inference
All estimates are presented with 95% UIs. These UIs are derived from the 2.5th and 97.5th percentiles of the posterior distribution of the GBD models, which inherently propagate uncertainty from all stages of the modeling process, including sampling error, measurement error, and model specification. Therefore, the reported 95% UDIs already account for estimation uncertainty and do not require additional multiple comparison adjustments (eg, Bonferroni correction) as standard practice in GBD analyses. The trends was interpretated based on whether these 95% UIs excluded zero, providing a conservative and well-established approach to statistical inference.28
All statistical analyses and graphics were performed using R version 4.4.1.
Results
Overview of the Global Burden
Figure 1 (panels A and B) presents the ASIR for EP across 204 countries and territories. Over the span from 1990 to 2021, the global incidence of EP, as detailed in Table 1, exhibited a downward trend. In 1990, there were 8,547,903 (95% UI: 6,683,900 to 10,659,847) reported EP cases worldwide, with an ASIR of 305.9 per 100,000 (95% UI: 241.31 to 380.32). By 2021, the cases had decreased to 8,376,810 (95% UI: 6,651,561 to 10,424,089), with an ASIR of 212.87 per 100,000 (95% UI: 169.27 to 264.19). The EAPC in the global EP ASIR from 1990 to 2021 was −0.91 (95% CI −1.03 to −0.79), indicating a slow but consistent decrease in the incidence of EP throughout the study period.
 |
Table 1 Incidence of EP in 1990 and 2021 for Female and All Locations, with EAPC from 1990 and 2021 |
 |
Figure 1 Global burden of EP across 204 countries and territories. (A) ASIR of EP in 2021; (B) EAPC for the ASIR of EP, 1990 to 2021. (C) ASPR of EP in 2021; (D) EAPC for the ASPR of EP, 1990 to 2021. (E) ASMR of EP in 2021; (F) EAPC for the ASMR of EP, 1990 to 2021. (G) ASDR of EP in 2021; (H) EAPC for the ASDR of EP, 1990 to 2021. |
Figure 1C and D and Table 2 display the global prevalence of EP in 1990 and 2021. In 1990, global EP prevalence cases were reported as 70,322 (95% UI: 46,306 to 104,056), with an age-standardized prevalence rate (ASPR) of 2.52 per 100,000 population (95% UI: 1.65 to 3.7). By 2021, this figure had marginally declined to 68,911 (95% UI: 45,381 to 101,997), with the ASPR decreasing to 1.75 per 100,000 population (95% UI: 1.15 to 2.6). The EAPC for the global EP ASPR from 1990 to 2021 was −0.62 (95% CI: −0.7 to −0.53), indicating a slight decrease in prevalence over three decades.
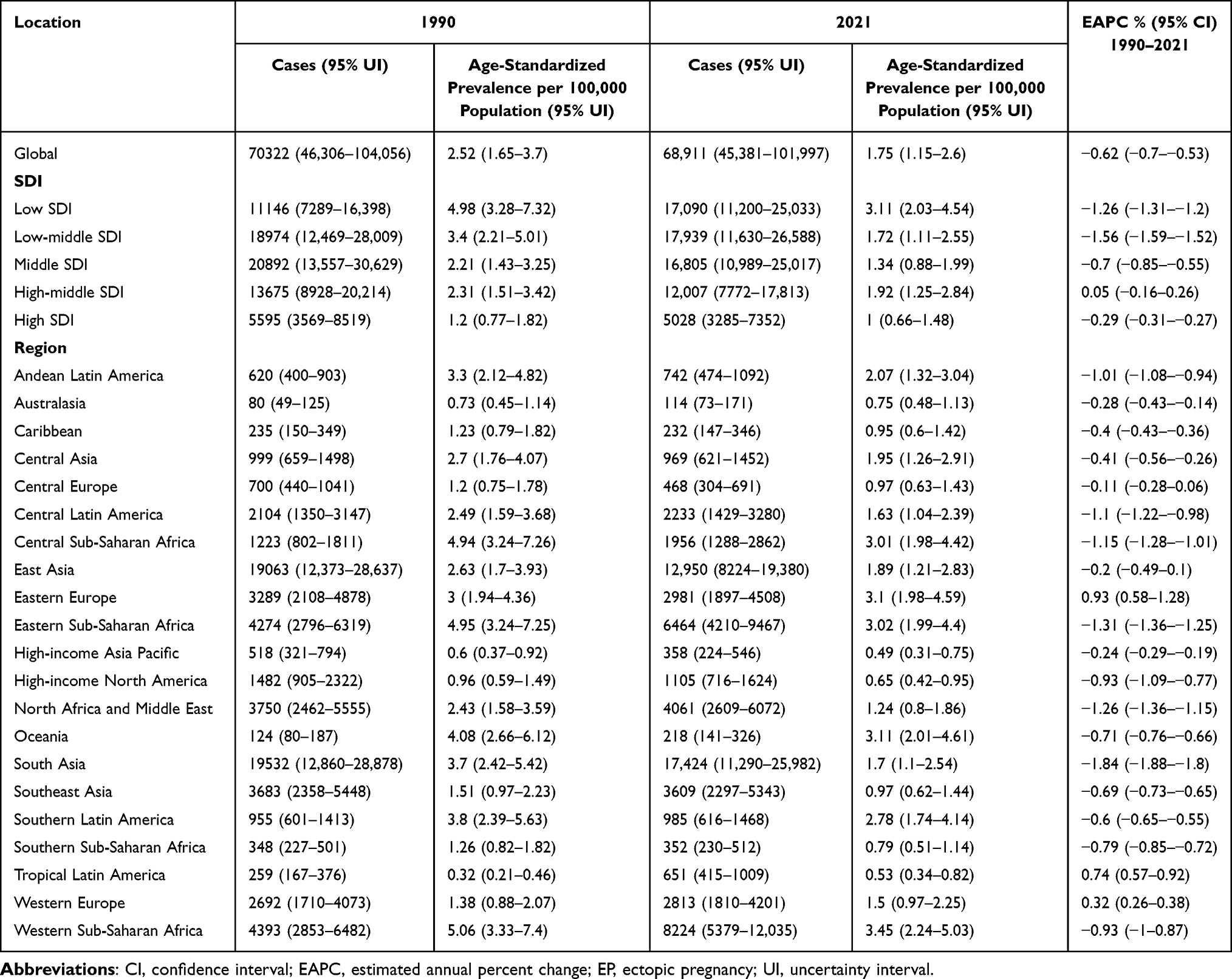 |
Table 2 Prevalence of EP in 1990 and 2021 for Female and All Locations, with EAPC from 1990 and 2021 |
Figure 1E and F and Table 3 illustrate the global age-standardized morality rate (ASMR) for EP. In 1990, the ASMR was 0.17 per 100,000 population (95% UI: 0.15 to 0.19), with 4,636 deaths reported (95% UI: 4,071 to 5,242). By 2021, the ASMR had slightly decreased to 0.16 per 100,000 population (95% UI: 0.14 to 0.20), though the number of deaths had increased to 6,442 (95% UI: 5,368 to 7,796). The EAPC for the global EP ASMR was 0 (95% CI: −0.01 to 0.01), indicating no significant change during this period.
 |
Table 3 Mortality of EP in 1990 and 2021 for Female and All Locations, with EAPC from 1990 and 2021 |
Figure 1G and H and Table 4 present the global DALYs for EP. In 1990, global DALYs for EP totaled 288,083 cases (95% UI: 252,585 to 325,017), with an ASDR of 10.37 per 100,000 population (95% UI: 9.1 to 11.72). By 2021, DALYs had risen to 396,856 cases (95% UI: 332,643 to 479,325), while the ASDR had marginally decreased to 10.21 per 100,000 population (95% UI: 8.56 to 12.34). The EAPC for global EP DALYs from 1990 to 2021 was 0.05 (95% CI: −0.02 to 0.11), reflecting no significant change during this period.
 |
Table 4 DALYs of EP in 1990 and 2021 for Female and All Locations, with EAPC from 1990 and 2021 |
An examination of the age-specific global impact of EP from 1990 to 2021 indicates shifts in patterns. Supplementary Figures S1 and S2 reveal that the peak incidence rates occurred within the 20–24 and 25–29 age brackets in 1990, aligning with the prime reproductive years. By 2021, a rise in incidence was noted across all age demographics, particularly among those aged 30–34 and 35–39. In 1990, the highest mortality rates occurred in those aged 30–34, whereas the greatest DALY rates were in the 25–29 age group. By contrast, in 2021, the highest rates of mortality and DALYs shifted to the 20–24 age group.
EP Burden by SDI Quintile
Figures S3 and S4, along with Tables 1–4, delineate the trends in incidence, prevalence, mortality, and DALYs of EP across SDI quintiles from 1990 to 2021. In 1990, the region with the lowest SDI recorded the highest rates of ASIR, ASPR, ASMR, and ASDR, at 605.11, 4.98, 1.08, and 62.82 per 100,000 respectively, with 95% UIs of 479.53–733.91, 3.28–7.32, 0.91–1.24, and 52.9–72.41. By 2021, these figures had declined to 377.99, 3.11, 0.76, and 44.55 per 100,000, with 95% UIs from 297.61–467.84, 2.03–4.54, 0.61–0.93, and 36–55.03, reflecting substantial reductions in disease burden. Notably, the low-middle SDI region exhibited the most marked decline in ASIR and ASPR, with EAPCs of −2.19% (95% UI: −2.23 to −2.15) and −1.56% (95% UI: −1.59 to −1.52). The High-middle SDI region showed the sharpest decrease in ASDR, with an EAPC of −2.59% (95% CI: −2.69 to −2.49).
EP Burden in 21 GBD Regions
As depicted in Figures S5 to S8 and Tables 1–4, South Asia reported the highest EP incidence in 2021, with 2,118,489 cases (95% UI: 1,614,271–2,712,644). Tropical Latin America saw a rapid increase in ASIR, with an EAPC of 2.47 (95% CI: 1.89 to 3.05). Western Sub-Saharan Africa recorded the highest ASIR and ASPR at 419.8 and 3.45 (95% UIs: 329.87 to 513.53 and 2.24 to 5.03), respectively. Eastern Sub-Saharan Africa noted the highest number of EP-related fatalities, totaling 1,832 cases (95% UI: 1,505 to 2,239). Central Sub-Saharan Africa registered the highest ASDR at 118.34 (95% UI: 83.97 to 163.66). Meanwhile, the Caribbean reported the fastest increases in ASDR, with an EAPC of 4.36 (95% CIs: 3.5 to 5.23).
EP Burden by Country or Territory
In 2021, China reported the highest number of EP incidence cases at 1,525,864 (95% UI: 1,181,694–1,970,718; Table S1) and prevalence cases at 12,556 (95% UI: 7,972–18,792; Table S2). Niger recorded the highest ASIR at 641.3 and ASPR at 5.27 (95% UIs: 498.92–794.53 and 3.46–7.68; Tables S1 and S2). The Democratic Republic of the Congo had the most death cases at 930 (95% UI: 628–1,302; Table S3) and the highest number of DALYs at 54,754 (95% UI: 36,924–75,220; Table S4), along with the highest ASMR at 2.3 and ASDR at 130.8 (95% UIs: 1.55–3.26 and 88.52–184.47; Tables S3 and S4). Meanwhile, Poland exhibited the lowest ASDR at 0.09 (95% UI: 0.06–0.11; Table S4), and Dominica showed the highest EAPC at 6.72 (95% UI: 5.57–7.88; Table S4), indicating the fastest increase in EP ASDR.
Decomposition Analysis of DALYs
Over the past three decades, the global landscape has witnessed a marked increase in DALYs, particularly within regions characterized by a low to middle SDI quintile (Figure 2). This rise has been largely shaped by demographic shifts and epidemiological changes in relation to EP. Specifically, population growth and epidemiological shifts contributed 62.73% and 50.75%, respectively, to the global increase in DALYs. Within the five SDI quintiles, both ageing and population growth had substantial effects on DALYs, with ageing’s adverse impact being most marked in the high-middle SDI regions at −374.72%. In contrast, population growth had a positive effect, with DALYs increasing significantly by 183.74% in these regions. Epidemiological changes also produced a marked beneficial impact, particularly in higher SDI quintiles, contributing 115.39%. The impact of these factors on DALYs varied across regions (Table S5).
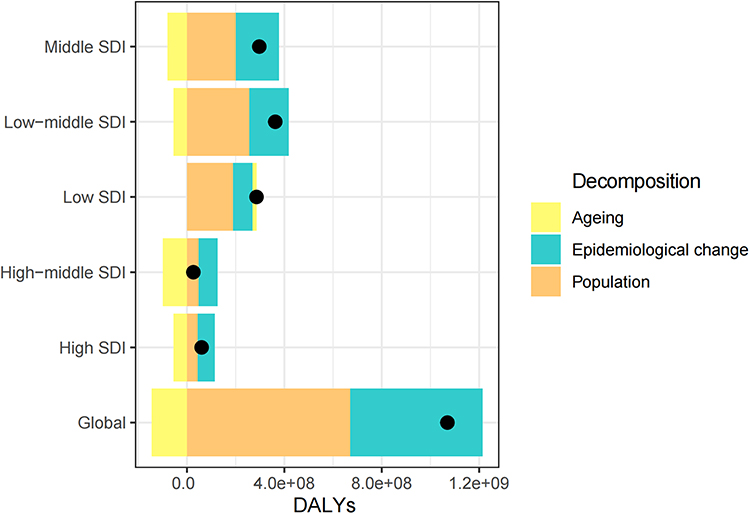 |
Figure 2 Trends in EP’s DALYs from 1990 to 2021 reflect population growth, ageing, and epidemiological shifts globally and across SDI quintiles. The overall impact of these factors is depicted by a black dot. Positive values indicate an increase in EP DALYs due to each factor, while negative values suggest a decrease. |
Frontier Analysis of ASDR
The term “frontier” refers to countries or regions achieving superior health outcomes, manifesting the minimal disease burdens proportionate to their SDI levels. The concept of the “effective difference” is delineated as the deviation from this frontier, representing the discrepancy between the actual observed disease burden and the feasible minimal burden given a country’s or region’s SDI. A substantial effective difference from the frontier indicates unrealized health benefits or opportunities for improvement in reducing the ASDR for EP.
Using 2021 data on ASDR and SDI, the effective difference for each country and region relative to the frontier was calculated. The five countries or regions with the most significant effective differences (range of effective difference: 129.5–103.51, Table S6) included the Democratic Republic of the Congo, The Gambia, Chad, Eritrea, and Angola. Figure 3 describes that ASDR generally decreases as SDI levels rise, and from 1990 to 2021, the overarching trend indicates a decline in ASDR over time. The solid black line denotes the frontier, while the dots represent the countries and regions. Blue dots signify an upward trend in ASDR, and red dots depict a downward trend.
 |
Figure 3 (A) Display the trends in EP’s ASDR from 1990 to 2021. (B) Conducts a frontier analysis based on SDI and ASDR in 2021. The frontier is depicted in solid black, with countries and territories represented by dots. The top 15 countries with the most substantial effective difference are labeled in black. Examples of frontier countries with low SDI (< 0.5) and minimal effective difference appear in blue (eg, Somalia, Timor-Leste, Bangladesh, Nepal, and Bhutan), while those with high SDI (> 0.85) and a relatively high effective difference are shown in red (eg, Sweden, Denmark, Lithuania, Monaco, and Ireland). Red dots denote a reduction in ASDR from 1990 to 2021, whereas blue dots indicate an increase. |
Health Inequality Analysis
In 1990 and 2021, the SII per 100,000 population for DALYs were −56.68 (95% CI: −63.44 to −49.93) and −36.56 (95% CI: −41.84 to −31.28) respectively, as shown in Figure 4 and Table S7. This decrease reflects a reduction in the socioeconomic gradient of the burden of EP, which was statistically significant (p = 1.58e−17), pointing to a narrowing disparity in health outcomes between high-income and low-income countries. Meanwhile, the Concentration Index for DALYs, indicating the distribution of EP-related DALYs across socioeconomic strata, exhibited minimal change, rising slightly from 0.6 in 1990 to 0.66 in 2021. Hence, while some regional disparities have lessened, the global inequality in the burden of EP continues to be a prevalent issue.
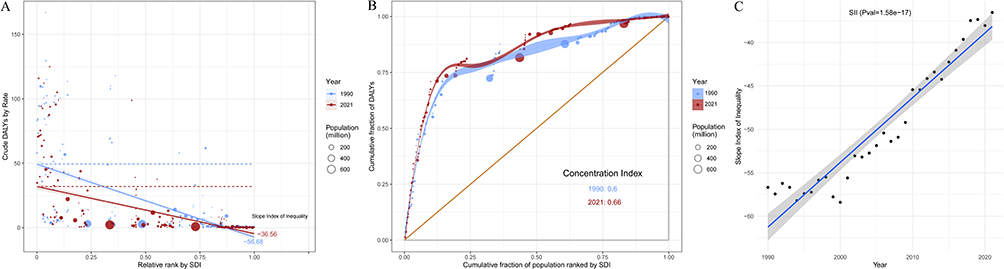 |
Figure 4 Relationship Between Crude DALY Rate and Relative SDI Rank in 1990 and 2021. (A) The relationship between crude DALYs rate for EP and countries’ relative SDI rank in 1990 (blue) and 2021 (red). Each point represents a country, with size indicating population size. The regression lines show a downward trend, suggesting that countries with higher SDI rankings have slightly lower crude DALY rates. (B) Changes in the Concentration Index for EP DALYs Burden from 1990 to 2021. Panel B displays the cumulative distribution of DALYs for EP against the cumulative fraction of the population ranked by SDI for 1990 and 2021. The concentration curve moves closer to the equality line over time, indicating a decrease in inequality. The Concentration Index increases from 0.6 in 1990 to 0.66 in 2021, showing a growing disparity in EP burden across SDI ranks. (C) Temporal Trend of SII from 1990 to 2021. Panel C shows the annual trend of the SII, with black dots representing observed values each year, and a solid blue line showing the fitted regression. The shaded area around the regression line indicates the 95% CI, with the SII showing an upward trajectory over the years, reflecting changes in health inequality over time. |
Discussion
This study systematically evaluated the incidence, prevalence, mortality, and DALYs associated with EP on a global and regional level, covering the period from 1990 to 2021, using the GBD 2021 dataset. The findings reveal a pattern of global disparities in EP, highlighted by significant regional variations and evolving trends over time. Notably, while the global ASIR and ASPR of EP show a decreasing trajectory, variations in ASMR and ASDR are less pronounced; however, absolute numbers of deaths and disability-adjusted life years both increased.
The decline observed in the ASIR and ASPR corresponds to improvements in access to healthcare and contraception, both recognized barriers to unintended pregnancy risk, followed by EP.35,36 This trend underlines the critical role of family planning and reproductive health services in reducing the incidence of EP. Nevertheless, the stability of the ASDR and the increase in the number of DALYs underscore the ongoing necessity for substantial improvements in maternal health outcomes, particularly in areas where the burden of EP remains high. Furthermore, our study indicates that trends in mortality and disability-adjusted life-years rates are highly similar over time. This similarity might be explained by the fact that in EP, DALYs primarily reflect fatal outcomes, this result is similar to previous studies.15 A myriad of elements drives the sustained increase in EP’s disease burden, particularly in rural and economically disadvantaged areas. These factors include an inequitable distribution of medical resources, often resulting in inadequate health services and expertise. This disparity results in significant delays in diagnosing and treating EP.37 Moreover, insufficient awareness among women regarding EP risks and symptoms, coupled with some healthcare providers’ lack of familiarity with specific EP types—such as cesarean scar pregnancy—exacerbates the issue, increasing the likelihood of delayed care and complications.38 Additionally, many women affected by EP may also suffer from chronic conditions or comorbidities, such as pelvic inflammatory disease and endometriosis, which can complicate their overall health and impact their prognosis.39 Furthermore, despite increasing contraceptive use, some women hesitate to use contraceptives during high-risk sexual activity due to concerns about side effects. However, although emergency contraceptives do not increase the incidence of EP beyond that observed in the general population, they are effective in reducing the risk of pregnancy, thereby decreasing the likelihood of EP following unprotected intercourse.35,36 Thus, despite a seeming decline in the incidence and prevalence of EP, these underlying factors may be responsible for the lack of significant improvement in ASMR and ASDR.
The variations in the burden of EP across different SDI quintiles and GBD regions underscore the significant influence of socio-economic factors on health outcomes. The notable reduction in EP rates within low SDI regions may be attributed to global health initiatives that focus on maternal and reproductive health in less affluent nations.40 Decomposition analysis showed that population ageing contributed to the increase of DALYs caused by EP in low SDI areas. This seemingly counterintuitive observation can be explained by the intersecting dynamics of fertility patterns and healthcare access disparities. In many low-SDI settings, high fertility rates mean that women continue childbearing into their later reproductive years. Consequently, an expanding cohort of older reproductive-age women—who inherently face a higher biological risk of EP—are exposed to pregnancy within healthcare systems that lack the capacity for early diagnosis and management.41 Unlike in high-SDI regions where advanced maternal age is often accompanied by enhanced medical surveillance, the increased risks of ageing here are compounded by persistently limited access to high-quality emergency obstetric care, diagnostic ultrasonography, and methotrexate.42 This synergy between undiminished risk and system-level barriers transforms demographic ageing into a driver of EP-related disability and death, as reflected in the rising DALYs. In contrast, the rising EP rates in areas like Tropical Latin America suggest that local factors such as healthcare infrastructure and cultural practices play a role in shaping these trends.43 This situation underscores the need for interventions tailored to align with both global health strategies and the specific contextual factors influencing EP rates in various regions.
Shifts in the age-specific burdens of EP from 1990 to 2021 highlight a transition towards higher incidence and prevalence rate in older demographics, whereas younger cohorts exhibit variations in mortality and DALY rates. This shift mirrors the evolving patterns of age-related health challenges and the effects of delayed childbearing tied to socio-economic advances. As women increasingly prioritize education and careers, they often delay childbearing, resulting in higher maternal age at conception, which is associated with increased EP risks.44–46 Although advanced fertility techniques offer conception opportunities to older women, they also bring heightened risks, especially those associated with physiological changes making older women more susceptible to complications.47–49 Moreover, chronic conditions such as hypertension and obesity, more common in older demographics, may adversely affect pregnancy outcomes or heighten EP risks.50–53 A case-control study indicated that prolonged use of intrauterine devices (IUDs) elevates the risk of EP, a phenomenon possibly linked to increased rates of clinical or subclinical tubal or pelvic infections (eg, due to organisms like chlamydia or actinomyces Israeli) among IUD users, thereby heightening EP risk.54 Although modern contraceptive methods have significantly curtailed unwanted pregnancies, their misuse or failure might still lead to higher EP incidence among older women. Further, evidence suggests an inverse relationship between the Human Development Index and fertility rates, proposing that prolonged educational pursuits among women might defer childbearing, thus delaying the emergence of EP and heightening its incidence at older reproductive ages.46 This evolving trend necessitates targeted healthcare interventions to mitigate the specific risks confronting older pregnant women.
A particularly critical finding that warrants separate emphasis is that by 2021, the highest mortality and disability-adjusted life year rates will shift to the 20–24 age group. Given the overall trend of rising EP incidence among older women, this pattern appears counterintuitive. It is hypothesized that this alarming shift reflects a fundamental disparity in healthcare access intersecting with biological vulnerability. Younger women in high-fertility, low-resource settings often enter their first pregnancies with limited health education and may harbor untreated asymptomatic sexually transmitted infections that cause subclinical tubal damage.55 When combined with the most severe barriers to healthcare access—including delays in seeking care due to limited autonomy, financial constraints, and geographic isolation—this creates a perfect storm where initial pregnancies in young adulthood face the highest risk of progressing to catastrophic outcomes. While advanced maternal age increases the risk of EP occurrence, it currently appears that the convergence of biological risks and severe systemic failures in early adulthood among the most vulnerable populations is the primary driver of EP-related mortality and disability.56–58
Beyond the immediate morbidity and mortality captured in this analysis, our findings on the sustained DALY burden prompt consideration of the long-term reproductive consequences of EP, which are not fully reflected in current burden metrics. A recent meta-analysis provides compelling evidence that EP history is significantly associated with adverse outcomes in subsequent pregnancies, including an elevated risk of recurrent ectopic pregnancy, preterm birth, placental abruption, and low birth weight.2 This underscores that women who survive an EP often face substantial reproductive challenges, including infertility and the risk of further pregnancy complications. Therefore, while the global DALY burden presented in this paper is substantial, it may underestimate the true lifelong impact of EP on women’s health and well-being, as it fails to fully capture these long-term sequelae that extend far beyond the acute event.
In this study, the SII decreased from −56.68 in 1990 (95% CI: −63.44 to −49.93) to −36.56 in 2021 (95% CI: −41.84 to −31.28), suggesting a reduction in health inequalities. However, frontier analysis reveals significant disparities persist in African countries, including the Democratic Republic of the Congo, Gambia, Chad, Eritrea, and Angola, which continue to face substantial health service gaps compared to border regions. This disparity largely stems from inadequate health infrastructure in these areas, marked by insufficient medical facilities and a shortage of healthcare professionals, which limits access to timely and effective treatment.59 Furthermore, poor reproductive health education and limited awareness of contraception and pregnancy risks among women exacerbate the incidence of unwanted pregnancies and, consequently, ectopic pregnancies.44,45,60 Economic and social challenges, such as low-income levels and high poverty rates, further impede access to health services, especially in rural areas where many families cannot afford necessary care. Cultural attitudes also impact women’s reproductive decisions, often delaying medical intervention for complications such as EP.45 Additionally, inadequate transportation and infrastructure deficits hinder timely access to healthcare facilities in emergencies, increasing health risks.61–63 Previous investigations have highlighted several risk factors for ectopic pregnancy, particularly emphasizing reproductive infections caused by mycoplasma and Chlamydia trachomatis, pelvic inflammatory disease, as well as the use of assisted reproductive technologies and IUDs.64,65
Nonetheless, GBD 2019 data underscore that iron deficiency is an emerging prominent risk factor for EP, accounting for over 20% of EP-related mortality and disability-adjusted life years in sub-Saharan Africa. Although the underlying biological pathways remain incompletely elucidated, several plausible hypotheses have been proposed. Iron is crucial for oxygen transport, cellular repair, and optimal immune function. Deficiency could therefore impair the integrity and ciliary function of the fallopian tube epithelium, disrupting embryo transport,66 or increase susceptibility to pelvic infections—a well-established risk factor for EP—through immune dysregulation.67 Alternatively, this association may be confounded by underlying chronic inflammation,68 which can both contribute to functional iron deficiency and independently increase EP risk. Interestingly, in regions designated as high SDI, both iron-deficiency-attributed deaths and disability-adjusted life years exceeded 10%, suggesting new avenues for EP investigation. Other studies indicate that while EP patients often exhibit elevated serum zinc levels, their serum copper levels are reduced, suggesting the copper/zinc ratio may serve as a novel diagnostic marker for EP.15 Thus, additional foundational research is essential to ascertain whether iron deficiency is a direct contributor to EP or if other mineral deficiencies may also be implicated in its causation.
This study notably advances the understanding of EP by offering a comprehensive update on its incidence, prevalence, mortality, and DALYs from 1990 to 2021, thereby providing a global perspective on EP’s burden. By examining disparities across various SDI and age categories, current work elucidates factors influencing EP, providing new perspectives and avenues for subsequent investigations. As the most recent global epidemiological study on EP, this research is crucial for developing management strategies.
Despite its strengths, this study has limitations. First, the accuracy of GBD estimates depends on data quality, which varies across regions and may lead to an underestimation of EP burden, particularly in low- and middle-SDI areas. Second, evolving diagnostic techniques over time may introduce inconsistencies, affecting data comparability. Third, as the GBD does not specify EP by anatomical location, risks associated with different ectopic sites, such as ampulla versus interstitial, remain unclear. This limitation has significant implications. For instance, interstitial pregnancy is associated with higher risks of rupture and life-threatening hemorrhage in early pregnancy compared to ampullary pregnancy.69 The inability to distinguish between these subtypes in our analysis means that the variation in their respective disease burdens, management strategies, and clinical outcomes across different regions and SDI levels could not be investigated. Consequently, our global estimates represent an average that may mask important epidemiological heterogeneity and clinical severity specific to high-risk implantation sites. Fourth, as with all GBD studies, our analysis is constrained by the available data within the framework. The GBD estimates focus on the acute incident of EP and do not capture long-term sequelae, such as subsequent infertility, psychological morbidity, or the detailed outcomes of future pregnancies.2 A key aspect of this limitation is the lack of granular data on initial treatment modalities (eg, salpingectomy vs salpingostomy vs medical management), which are known to significantly influence subsequent fertility outcomes and recurrence risk. The recent literature has aptly highlighted the absence of this longitudinal and management-specific data as a critical evidence gap in understanding the complete burden of EP.2 Future research should incorporate more localized analyses, with improved data sources and collaboration to address these limitations accurately.
This research enhances our comprehension of the worldwide impact of ectopic pregnancy and may guide focused strategies to decrease its occurrence and enhance maternal health results. Local drivers of EP trends in specific regions need to be explored in future studies, while culturally sensitive and contextually appropriate interventions must be developed. Second, there is the need to develop mechanisms for data collection and surveillance systems to further improve the accuracy and reliability of worldwide estimates of the burden of EP. There is also a performance need for long-term health outcomes studies in women who have had EP with respect to impact on future fertility and their mental health. Furthermore, the world’s ageing population, coupled with changing reproductive practices, necessitates research into how these trends influence EP rates and the development of appropriate strategies to mitigate identified risks.
In summary, while there has been a decrease in the global burden associated with EP, the rising absolute number of DALYs and persistent, stark inequalities demand urgent and targeted action. These findings reinforce the message of continued investment in reproductive health services. To effectively reduce the burden and address the hidden long-term consequences, we recommend the implementation of equity-focused interventions. These include: (1) strengthening targeted reproductive health education to prevent pelvic inflammatory disease and mitigate risk factors; (2) enhancing early detection programs through improved access to ultrasound and β-hCG monitoring in primary care settings, particularly in rural and low-income areas; and (3) establishing structured post-EP fertility counseling and follow-up care to support women’s future reproductive goals and manage the risk of recurrence and subsequent complications. These strategies are especially critical in high-burden regions such as sub-Saharan Africa and South Asia, where the convergence of high disease burden and weak health systems creates the greatest need and potential for impact.
Conclusion
This study reveals a critical divergence in the global burden of ectopic pregnancy (1990–2021): while incidence rates have declined, deaths and DALYs have risen, with the heaviest burden shifting to the 20–24 age group in low-SDI regions. These findings underscore a dual challenge: reducing immediate incidence while mitigating long-term reproductive sequelae, necessitating a shift from emergency care alone to integrated, long-term fertility preservation strategies. To address persistent disparities, we recommend equity-focused interventions including targeted reproductive health education, enhanced early detection, and post-EP fertility counseling, particularly in sub-Saharan Africa and South Asia. Future research must bridge current evidence gaps by initiating cohort-based, region-specific follow-up studies that integrate registry data to link population estimates with patient-centered outcomes. These coordinated clinical and research efforts are indispensable for developing targeted interventions to lower the global EP burden and safeguard women’s reproductive futures.
Abbreviations
ASDR, Age-standardized DALYs rate; ASIR, Age-standardized incidence rate; ASMR, Age-standardized mortality rate; ASPR, Age-standardized prevalence rate; β-hCG, Beta-human chorionic gonadotropin; CODEm, Cause of Death Ensemble model; CIs, Confidence intervals; DALYs, Disability-adjusted life years; EAPC, Estimated annual percentage change; EP, Ectopic pregnancy; GATHER, Guidelines for Accurate and Transparent Health Estimates Reporting; GBD, Global Burden of Disease; IUDs, Intrauterine devices; SDG, Sustainable development goal; SDI, Socio-demographic index; SII, Slope index of inequality; UI, Uncertainty interval.
Data Sharing Statement
The original contributions presented in the study are included in the article or Supplementary Materials, further inquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
The institutional ethics committee of Meizhou People’s Hospital granted an exemption for this study, as it did not require approval, given that the data from the 2021 GBD is publicly available. This study adhered to the guidelines for accurate and transparent health assessment reporting. Since publicly accessible data were used, ethical approval and informed consent were not required for this study.
Acknowledgments
We are grateful for the work of the GBD study 2021 collaborators.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this study.
References
1. Xu C, Mao Z, Tan M, et al. Prevalence and Related Factors of Rupture among Cases with Ectopic Pregnancy; a Systematic Review and Meta-Analysis. Arch Acad Emerg Med. 2024;12(1):e2. doi:10.22037/aaem.v11i1.2172
2. Papageorgiou D, Sapantzoglou I, Zachariou E, Antsaklis P, Daskalakis G, Pergialiotis V. Impact of Ectopic Pregnancy on the Outcomes of the Subsequent Pregnancy: a Systematic Review and Meta-Analysis. J Clin Med. 2025;14(12):4112. doi:10.3390/jcm14124112
3. Papageorgiou D, Sapantzoglou I, Prokopakis I, Zachariou E. Tubal Ectopic Pregnancy: from Diagnosis to Treatment. Biomedicines. 2025;13(6):1465. doi:10.3390/biomedicines13061465
4. Gerema U, Alemayehu T, Chane G, Desta D, Diriba A. Determinants of ectopic pregnancy among pregnant women attending referral hospitals in southwestern part of Oromia regional state, Southwest Ethiopia: a multi-center case control study. BMC Pregnancy Childbirth. 2021;21(1):130. doi:10.1186/s12884-021-03618-7
5. Tsakiridis I, Giouleka S, Mamopoulos A, Athanasiadis A, Dagklis T. Diagnosis and Management of Ectopic Pregnancy: a Comparative Review of Major National Guidelines. Obstet Gynecol Surv. 2020;75(10):611–623. doi:10.1097/ogx.0000000000000832
6. Orsi M, Janneh FM, Sesay A, Bah AK, Tiru NA. A Clinical and Ethical Dilemma: expectant Management for Ectopic Pregnancy with a Vital Fetus in a Low-Resource Setting. J Clin Med. 2023;12(17):5642. doi:10.3390/jcm12175642
7. Long Y, Zhu H, Hu Y, Shen L, Fu J, Huang W. Interventions for non-tubal ectopic pregnancy. Cochrane Database Syst Rev. 2020;7(7):Cd011174. doi:10.1002/14651858.CD011174.pub2
8. Naveed AK, Anjum MU, Hassan A, Mahmood SN. Methotrexate versus expectant management in ectopic pregnancy: a meta-analysis. Arch Gynecol Obstet. 2022;305(3):547–553. doi:10.1007/s00404-021-06236-y
9. Xiao C, Shi Q, Cheng Q, Xu J. Non-surgical management of tubal ectopic pregnancy: a systematic review and meta-analysis. Medicine. 2021;100(50):e27851. doi:10.1097/md.0000000000027851
10. Mohammad NS, Nazli R, Zafar H, Fatima S. Effects of lipid based Multiple Micronutrients Supplement on the birth outcome of underweight pre-eclamptic women: a randomized clinical trial. Pak J Med Sci. 2022;38(1):219–226. doi:10.12669/pjms.38.1.4396
11. Yang J, Li Y, Liu Q, et al. Brief introduction of medical database and data mining technology in big data era. J Evid Based Med. 2020;13(1):57–69. doi:10.1111/jebm.12373
12. Wu WT, Li YJ, Feng AZ, et al. Data mining in clinical big data: the frequently used databases, steps, and methodological models. Mil Med Res. 2021;8(1):44. doi:10.1186/s40779-021-00338-z
13. Nieto Rey N, Lopez IJ, Quintero MA, Sanabria PL, Villegas-Echeverri JD. Breaking Down Barriers: improving Access to Quality Endometriosis Care. Semin Reprod Med. 2025. doi:10.1055/s-0045-1811188
14. Kurjak A, Stanojević M, Dudenhausen J. Why maternal mortality in the world remains tragedy in low-income countries and shame for high-income ones: will sustainable development goals (SDG) help? J Perinat Med. 2023;51(2):170–181. doi:10.1515/jpm-2022-0061
15. Zhang S, Liu J, Yang L, Li H, Tang J, Hong L. Global burden and trends of ectopic pregnancy: an observational trend study from 1990 to 2019. PLoS One. 2023;18(10):e0291316. doi:10.1371/journal.pone.0291316
16. Qian H, Qian W, Huang H, Wang Y, Jia R. Ectopic pregnancy epidemiology from 1990 to 2021: a global burden of disease (GBD) analysis of 204 countries and territories. Eur J Obstet Gynecol Reprod Biol. 2025;314:114688. doi:10.1016/j.ejogrb.2025.114688
17. GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2100–2132. doi:10.1016/s0140-6736(24)00367-2
18. Panelli DM, Phillips CH, Brady PC. Incidence, diagnosis and management of tubal and nontubal ectopic pregnancies: a review. Fertil Res Pract. 2015;1:15. doi:10.1186/s40738-015-0008-z
19. C Abbafati, DB Machado, B Cislaghi, OM Salman, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/s0140-6736(20)30925-9
20. EM Alvarez, LM Force, R Xu, et al. The global burden of adolescent and young adult cancer in 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Oncol. 2022;23(1):27–52. doi:10.1016/s1470-2045(21)00581-7
21. KL Ong, LK Stafford, SA McLaughlin, et al. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2023;402(10397):203–234. doi:10.1016/s0140-6736(23)01301-6
22. Stevens GA, Alkema L, Black RE, et al. Guidelines for Accurate and Transparent Health Estimates Reporting: the GATHER statement. PLoS Med. 2016;13(6):e1002056. doi:10.1371/journal.pmed.1002056
23. SE Vollset, HS Ababneh, YH Abate, et al. Burden of disease scenarios for 204 countries and territories, 2022–2050: a forecasting analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2204–2256. doi:10.1016/s0140-6736(24)00685-8
24. Huang J, Man Y, Shi Z, Fu X, Shi W, Liang X. Global, regional, and national burden of maternal disorders, 1990–2021: a systematic analysis from the global burden of disease study 2021. BMC Public Health. 2025;25(1):2576. doi:10.1186/s12889-025-23814-w
25. Zou S, Li C. Global and regional trends in male breast cancer burden: a comparative analysis of incidence, prevalence, mortality, and disability-adjusted life years in China and worldwide (1990–2021). Gland Surg. 2025;14(5):818–833. doi:10.21037/gs-2025-10
26. AE Schumacher, HH Kyu, A Aali, et al. Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950–2021, and the impact of the COVID-19 pandemic: a comprehensive demographic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):1989–2056. doi:10.1016/s0140-6736(24)00476-8
27. Deng Y, Zhao P, Zhou L, et al. Epidemiological trends of tracheal, bronchus, and lung cancer at the global, regional, and national levels: a population-based study. J Hematol Oncol. 2020;13(1):98. doi:10.1186/s13045-020-00915-0
28. Bu X, Xie Z, Liu J, et al. Global PM2.5-attributable health burden from 1990 to 2017: estimates from the Global Burden of disease study 2017. Environ Res. 2021;197:111123. doi:10.1016/j.envres.2021.111123
29. Xie Y, Bowe B, Mokdad AH, et al. Analysis of the Global Burden of Disease study highlights the global, regional, and national trends of chronic kidney disease epidemiology from 1990 to 2016. Kidney Int. 2018;94(3):567–581. doi:10.1016/j.kint.2018.04.011
30. Barber RM, Fullman N, Sorensen RJ, et al. Healthcare Access and Quality Index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990–2015: a novel analysis from the Global Burden of Disease Study 2015. Lancet. 2017;390(10091):231–266. doi:10.1016/s0140-6736(17)30818-8
31. Xie Y, Bowe B, Xian H, Balasubramanian S, Al-Aly Z. Rate of Kidney Function Decline and Risk of Hospitalizations in Stage 3A CKD. Clin J Am Soc Nephrol. 2015;10(11):1946–1955. doi:10.2215/cjn.04480415
32. Jiang J, Xia Z, Yao W. Global, regional, and national larynx cancer burden and health inequality analysis from 1990 to 2021 with a prediction from 2022 to 2040. Front Oncol. 2025;15:1617613. doi:10.3389/fonc.2025.1617613
33. Liu W, Rao L, Qiao Z, Wang G, Li B, Shen G. Global disparities in the burden of pancreatic cancer (1990–2021): insights from the 2021 Global Burden of Disease study. BMC Cancer. 2025;25(1):722. doi:10.1186/s12885-025-14110-2
34. Qian N, Lu C, Wei T, et al. Epidemiological trends and forecasts in stroke at global, regional and national levels. J Stroke Cerebrovasc Dis. 2025;34(8):108347. doi:10.1016/j.jstrokecerebrovasdis.2025.108347
35. Zhang J, Li C, Zhao WH, et al. Association between levonorgestrel emergency contraception and the risk of ectopic pregnancy: a multicenter case-control study. Sci Rep. 2015;5:8487. doi:10.1038/srep08487
36. Sapapsap B, Leelakanok N, Boonpattharatthiti K, Siritientong T, Methaneethorn J. A systematic review and meta-analysis of the prevalence and association between levonorgestrel and ectopic pregnancy. Expert Opin Drug Saf. 2023;22(10):929–941. doi:10.1080/14740338.2023.2247965
37. Pak JO, Durfee JK, Pedro L, Osborne A, Larkins-Pettigrew M. Retroperitoneal Ectopic Pregnancy. Obstet Gynecol. 2018;132(6):1491–1493. doi:10.1097/aog.0000000000002965
38. Ravi Selvaraj L, Rose N, Ramachandran M. Pitfalls in Ultrasound Diagnosis of Cesarean Scar Pregnancy. J Obstet Gynaecol India. 2018;68(3):164–172. doi:10.1007/s13224-016-0956-1
39. Farland LV, Prescott J, Sasamoto N, et al. Endometriosis and Risk of Adverse Pregnancy Outcomes. Obstet Gynecol. 2019;134(3):527–536. doi:10.1097/aog.0000000000003410
40. Wu N, Ye E, Ba Y, et al. The global burden of maternal disorders attributable to iron deficiency related sub-disorders in 204 countries and territories: an analysis for the Global Burden of Disease study. Front Public Health. 2024;12:1406549. doi:10.3389/fpubh.2024.1406549
41. Singh S, Gupta V, Jain N, Parihar SS, Jaiswal A, Snigda K. Incidence of Ectopic Pregnancies at a Tertiary Care Center of Tribal India: a Hospital-Based Cross-Sectional Study. Cureus. 2025;17(9):e92319. doi:10.7759/cureus.92319
42. Cordeiro FDE, Alves GJA, Araujo Júnior E, Feitosa LEE. Ectopic pregnancies: a retrospective cohort analysis in a tertiary reference center in the Northeast Region of Brazil. Ceska Gynekol. 2018;83(6):434–439.
43. Elendu C, Amaechi DC, Elendu ID, et al. Global perspectives on the burden of sexually transmitted diseases: a narrative review. Medicine. 2024;103(20):e38199. doi:10.1097/md.0000000000038199
44. Schultheis P, Montoya MN, Zhao Q, Archer J, Madden T, Peipert JF. Contraception and ectopic pregnancy risk: a prospective observational analysis. Am J Obstet Gynecol. 2021;224(2):228–229. doi:10.1016/j.ajog.2020.10.013
45. Kopp-Kallner H, Linder M, Cesta CE, Segovia Chacón S, Kieler H, Graner S. Method of Hormonal Contraception and Protective Effects Against Ectopic Pregnancy. Obstet Gynecol. 2022;139(5):764–770. doi:10.1097/aog.0000000000004726
46. Cheng H, Luo W, Si S, et al. Global trends in total fertility rate and its relation to national wealth, life expectancy and female education. BMC Public Health. 2022;22(1):1346. doi:10.1186/s12889-022-13656-1
47. Vuković P, Kasum M, Raguž J, et al. FERTILITY PRESERVATION IN YOUNG WOMEN WITH EARLY-STAGE BREAST CANCER. Acta Clin Croat. 2019;58(1):147–156. doi:10.20471/acc.2019.58.01.19
48. Kaltsas A, Moustakli E, Zikopoulos A, et al. Impact of Advanced Paternal Age on Fertility and Risks of Genetic Disorders in Offspring. Genes. 2023;14(2):486. doi:10.3390/genes14020486
49. MacArthur T, Bachmann G, Ayers C. Menopausal women requesting egg/embryo donation: examining health screening guidelines for assisted reproductive technology. Menopause. 2016;23(7):799–802. doi:10.1097/gme.0000000000000622
50. Chuang CH, Velott DL, Weisman CS. Exploring knowledge and attitudes related to pregnancy and preconception health in women with chronic medical conditions. Matern Child Health J. 2010;14(5):713–719. doi:10.1007/s10995-009-0518-6
51. Yan X, Xiao X, Kong F, Chen L. Prevalence and outcome of chronic hypertension and its complications with gestational diabetes. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024;49(3):400–407. doi:10.11817/j.issn.1672-7347.2024.230596
52. Berger H, Melamed N, Murray-Davis B, et al. Prevalence of Pre-Pregnancy Diabetes, Obesity, and Hypertension in Canada. J Obstet Gynaecol Can. 2019;41(11):1579–1588.e2. doi:10.1016/j.jogc.2019.01.020
53. Rogne T, Gill D, Liew Z, et al. Mediating Factors in the Association of Maternal Educational Level With Pregnancy Outcomes: a Mendelian Randomization Study. JAMA Netw Open. 2024;7(1):e2351166. doi:10.1001/jamanetworkopen.2023.51166
54. Li C, Zhao WH, Zhu Q, et al. Risk factors for ectopic pregnancy: a multi-center case-control study. BMC Pregnancy Childbirth. 2015;15:187. doi:10.1186/s12884-015-0613-1
55. Wiesenfeld HC, Hillier SL, Krohn MA, et al. Lower genital tract infection and endometritis: insight into subclinical pelvic inflammatory disease. Obstet Gynecol. 2002;100(3):456–463. doi:10.1016/s0029-7844(02)02118-x
56. Correa-de-Araujo R, Yoon SSS. Clinical Outcomes in High-Risk Pregnancies Due to Advanced Maternal Age. J Womens Health. 2021;30(2):160–167. doi:10.1089/jwh.2020.8860
57. Brim ACS, Barretto VRD, Reis-Oliveira JG, da Silveira de Araújo RB, Romeo A. Risk factors for ectopic pregnancy occurrence: systematic review and meta-analysis. Int J Gynaecol Obstet. 2025;168(3):919–932. doi:10.1002/ijgo.15965
58. San Lazaro Campillo IS, Meaney S, O’Donoghue K, Corcoran P. Ectopic pregnancy hospitalisations: a national population-based study of rates, management and outcomes. Eur J Obstet Gynecol Reprod Biol. 2018;231:174–179. doi:10.1016/j.ejogrb.2018.10.054
59. Stulberg DB, Cain L, Dahlquist IH, Lauderdale DS. Ectopic pregnancy morbidity and mortality in low-income women, 2004–2008. Hum Reprod. 2016;31(3):666–671. doi:10.1093/humrep/dev332
60. Hsu JY, Chen L, Gumer AR, et al. Disparities in the management of ectopic pregnancy. Am J Obstet Gynecol. 2017;217(1):49.e1–49.e10. doi:10.1016/j.ajog.2017.03.001
61. Anand S, Ayodele V, Ashraf A, et al. Expanding healthcare access in rural sub-Saharan Africa. Perspect Public Health. 2024;144(6):333–335. doi:10.1177/17579139241263707
62. Sagrestano LM, Clay J, Finerman R, Gooch J, Rapino M. Transportation vulnerability as a barrier to service utilization for HIV-positive individuals. AIDS Care. 2014;26(3):314–319. doi:10.1080/09540121.2013.819403
63. Al-Mamun M, Kalam A, Karim MZ, Alam M, Khan TH. Menstrual hygiene management in flood-affected Bangladesh: addressing socio-cultural barriers, infrastructure gaps, and policy responses. Front Public Health. 2025;13:1538447. doi:10.3389/fpubh.2025.1538447
64. Cirillo F, Paladino I, Ronchetti C, et al. Ectopic pregnancy risk factors in infertile patients: a 10-year single center experience. Sci Rep. 2022;12(1):20473. doi:10.1038/s41598-022-24649-w
65. Pant S, Dimri A, Arora R, Siraj F, Raisuddin S, Rastogi S. Differential expression of matrix metalloproteinases in the fallopian tube of women with Chlamydia trachomatis-associated tubal ectopic pregnancy. Microb Pathog. 2022;165:105468. doi:10.1016/j.micpath.2022.105468
66. Kobak KA, Radwańska M, Dzięgała M, et al. Structural and functional abnormalities in iron-depleted heart. Heart Fail Rev. 2019;24(2):269–277. doi:10.1007/s10741-018-9738-4
67. Cheng WH, Huang KY, Huang PJ, et al. Nitric oxide maintains cell survival of Trichomonas vaginalis upon iron depletion. Parasit Vectors. 2015;8:393. doi:10.1186/s13071-015-1000-5
68. Loftus TJ, Mira JC, Stortz JA, et al. Persistent inflammation and anemia among critically ill septic patients. J Trauma Acute Care Surg. 2019;86(2):260–267. doi:10.1097/ta.0000000000002147
69. Yalçın Y, Tatar B, Erdemoğlu E, Akkurt M, Yavuz A, Erdemoğlu E. Laparoscopic systemic devascularization of uterine cornu for cornual resection in interstitial pregnancy. Turk J Obstet Gynecol. 2015;12(3):182–184. doi:10.4274/tjod.23500
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.