Back to Journals » Nature and Science of Sleep » Volume 18

From Therapeutic Heterogeneity to Precision Neuromodulation: Non-Invasive Brain Stimulation for Chronic Insomnia
Authors Ao WL, Liu Z, Zhao ZY, Zhu WC, Guan SQ, Zheng YS, Huang H ![]()
Received 25 March 2026
Accepted for publication 2 June 2026
Published 24 June 2026 Volume 2026:18 495420
DOI https://doi.org/10.2147/NSS.S495420
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Wu-lan Ao,1,2 Zheng Liu,1,2 Zi-yi Zhao,1,2 Wen-chang Zhu,1 Si-qi Guan,1,2 Yong-su Zheng,1,2 Hao Huang1,2
1Department of Neurology, Affiliated Hospital of Zunyi Medical University, Zunyi City, Guizhou, People’s Republic of China; 2Key Laboratory of Brain Function and Brain Disease Prevention and Treatment of Guizhou Province, Affiliated Hospital of Zunyi Medical University, Zunyi City, Guizhou, People’s Republic of China
Correspondence: Hao Huang, Department of Neurology, Affiliated Hospital of Zunyi Medical University, 149 Dalian Road, Huichuan District, Zunyi, Guizhou, 563000, People’s Republic of China, Email [email protected]
Abstract: Chronic insomnia is linked to impaired daytime functioning, diminished quality of life, and heightened psychiatric and cardiometabolic risks. While cognitive behavioral therapy for insomnia and pharmacotherapy are well-established treatments, their clinical effectiveness may be constrained by limited accessibility, incomplete response, relapse, adherence challenges, or adverse effects. Non-invasive brain stimulation (NIBS) has therefore attracted increasing interest as a potential adjunctive or alternative intervention because it may modulate cortical excitability, large-scale brain networks, sleep-related oscillations, and autonomic function. This narrative review synthesizes current evidence on repetitive transcranial magnetic stimulation (rTMS), transcranial direct current stimulation (tDCS), transcranial alternating current stimulation (tACS), and transcutaneous auricular vagus nerve stimulation (taVNS) for chronic insomnia. Particular attention is given to therapeutic heterogeneity across stimulation targets, parameters, treatment schedules, patient phenotypes, and outcome measures. Available studies suggest potential improvements in subjective sleep quality and selected objective sleep parameters; however, the evidence remains limited by small sample sizes, variable sham designs, short follow-up durations, and inconsistent findings across modalities. We further propose a precision neuromodulation framework based on individualized functional targeting, biomarker-informed patient stratification, closed-loop feedback regulation, and integration with behavioral or pharmacological treatment pathways. This review highlights the translational promise of NIBS and outlines methodological priorities needed to move from heterogeneous evidence toward clinically reliable precision neuromodulation.
Keywords: non-invasive brain stimulation, insomnia, transcranial magnetic stimulation (TMS), transcranial alternating current stimulation (tACS), transcranial direct current stimulation (tDCS), transcutaneous auricular vagus nerve stimulation (taVNS)
Introduction
Insomnia is among the most prevalent health conditions worldwide,1 with chronic insomnia affecting approximately 5–15% of adults,2 particularly women and older individuals.3 It is characterized by difficulty initiating or maintaining sleep, early-morning awakening, or non-restorative sleep, accompanied by daytime impairments such as fatigue, impaired attention, emotional lability, or reduced functioning. These symptoms typically persist for at least 3 months and occur on at least 3 nights per week.4,5
Chronic insomnia imposes substantial individual and societal burdens. It reduces quality of life and is associated with increased risks of cardiovascular disease,6,7 anxiety,8 depression,9 suicide, obesity,10 and diabetes.11 It may also aggravate emotional and cognitive symptoms while increasing socioeconomic costs.
Current first-line management for chronic insomnia and poor sleep quality, including low sleep efficiency and poor sleep satisfaction, mainly involves cognitive behavioral therapy for insomnia (CBT-I) and pharmacotherapy.12 CBT-I is recommended by the American Academy of Sleep Medicine (AASM) and the American College of Physicians (ACP) as a first-line non-pharmacological treatment;13,14 however, its clinical implementation may be limited by the need for trained therapists, poor long-term adherence, variable individual adaptability, a non-response rate of approximately 30%, and complete remission in only about half of patients.15 Sedative-hypnotics, including benzodiazepine and non-benzodiazepine receptor agonists, can rapidly induce sleep but may be associated with falls, cognitive impairment, cardiovascular risks, abuse or dependence,16 anterograde amnesia,17 and rebound insomnia after discontinuation. These limitations highlight the need for safe, sustainable, and clinically feasible alternatives. In addition to efficacy and safety, practical factors such as treatment accessibility, cost, treatment burden, and the feasibility of repeated or home-based interventions are also important for determining whether emerging therapies can be translated into routine insomnia care.
Against this background, non-invasive neuromodulation has attracted increasing attention as an emerging non-pharmacological approach. Its development began in the mid-20th century with cranial electrostimulation (CES), while the introduction of transcranial magnetic stimulation (TMS) in 1985 enabled non-invasive modulation of human brain activity. Since the 21st century, technologies such as transcranial electrical stimulation (tES) and transcutaneous auricular vagus nerve stimulation (taVNS), together with advances in closed-loop systems, multimodal treatment, and wearable devices, have promoted the development of more personalized and potentially home-based interventions, although their clinical implementation remains under active investigation (Figure 1). 18–30
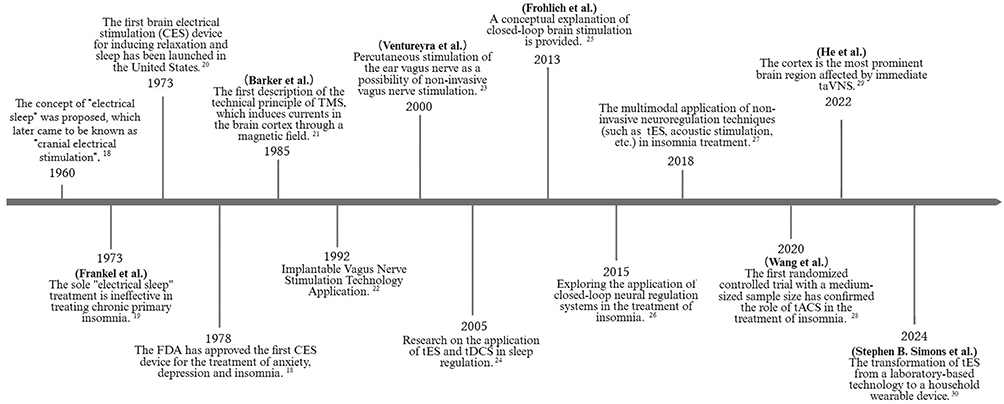 |
Figure 1 Historical evolution of non-invasive neuromodulation techniques (NIBS) in insomnia treatment. |
The pathophysiology of chronic insomnia is increasingly conceptualized within hyperarousal and network-based models.1,31,32 Chronic insomnia is associated with elevated cortical excitability, autonomic imbalance, and abnormal activity within large-scale brain networks, including the default mode network and executive control network.1,31,32 Neuroimaging and electroencephalographic studies have reported disrupted resting-state connectivity among the prefrontal cortex, thalamus, and limbic regions, findings that are consistent with persistent hyperarousal.33,34 Autonomic studies have further identified excessive sympathetic activation and reduced heart rate variability, which may be related to hypothalamic-pituitary-adrenal (HPA) axis activation under chronic stress.31,34 Together, these findings provide a mechanistic rationale for targeting cortical, network-level, oscillatory, and autonomic abnormalities through neuromodulatory approaches.35 Clinically, this mechanistic heterogeneity may be reflected in partially overlapping insomnia phenotypes, such as hyperarousal-dominated sleep-onset difficulties, reduced slow-wave activity, autonomic dysregulation with anxiety symptoms, and refractory or medication-intolerant insomnia, which may require different neuromodulation strategies.1,5,34
Advances in neuroscience and medical technology have supported the investigation of non-invasive neuromodulation, particularly brain stimulation techniques (BSTs), as potential adjunctive interventions for insomnia. These techniques may act through the modulation of neural network activity, cortical excitability, sleep-related oscillations, and autonomic regulation, thereby engaging mechanisms implicated in chronic insomnia.35 In recent years, repetitive transcranial magnetic stimulation (rTMS), transcranial direct current stimulation (tDCS), transcranial alternating current stimulation (tACS), and transcutaneous auricular vagus nerve stimulation (taVNS) have been explored as potential interventions for chronic insomnia management. Their therapeutic relevance may derive from their capacity to modulate aberrant brain networks and hyperarousal-related processes, although the strength and consistency of clinical evidence remain variable across modalities.
For this narrative review, we searched the PubMed and Web of Science electronic databases to obtain relevant articles, without restricting the publication date. We performed a series of literature searches using the following keywords: “insomnia”, “chronic insomnia”, “insomnia disorder”, “sleep initiation and maintenance disorders”, “poor sleep quality”, “non-invasive brain stimulation”, “noninvasive brain stimulation”, “neuromodulation”, “transcranial magnetic stimulation”, “TMS”, “repetitive transcranial magnetic stimulation”, “rTMS”, “transcranial electrical stimulation”, “tES”, “transcranial direct current stimulation”, “tDCS”, “transcranial alternating current stimulation”, “tACS”, “vagus nerve stimulation”, “transcutaneous auricular vagus nerve stimulation”, “auricular vagus nerve stimulation”, “transcutaneous vagus nerve stimulation”, and “taVNS”. Additional searches were conducted using terms related to precision neuromodulation, including “biomarker”, “patient stratification”, “functional targeting”, “closed-loop stimulation”, “EEG”, “neuroimaging”, and “heart rate variability”. Keywords were used alone and in combination, and titles and abstracts from the search results were assessed to identify mechanistic, clinical, and review articles relevant to the scope of this narrative review.
Several recent reviews and meta-analyses have evaluated the efficacy and safety of non-invasive brain stimulation (NIBS) for insomnia and sleep disturbances across neurological and neuropsychiatric conditions.12,35 However, most prior work has primarily summarized treatment effects by modality or pooled clinical outcomes, with less emphasis on why therapeutic responses vary across patients, stimulation protocols, and clinical phenotypes. In addition, the translation of NIBS into routine insomnia care remains constrained by unresolved issues, including target selection, parameter optimization, phenotype-guided patient stratification, accessibility, and long-term feasibility, which are not yet fully incorporated into guideline-based insomnia care.
The present narrative review addresses these gaps by using therapeutic heterogeneity as the organizing framework. Precision neuromodulation is conceptualized here as phenotype- and biomarker-informed selection of stimulation modality, target, parameters, timing, and combination strategy. We synthesize evidence across rTMS, tDCS, tACS, and taVNS; critically appraise positive, negative, null, and inconclusive findings; and propose a translational pathway involving individualized functional targeting, closed-loop adaptive regulation, and integrated treatment strategies.
Types and Mechanisms of Non-Invasive Neuromodulation for Improving Chronic Insomnia
Neuromodulation broadly refers to therapeutic strategies that seek to alleviate disease-related symptoms by modulating nervous system activity. Through electrical stimulation, magnetic fields, or biofeedback-based approaches, these interventions can influence neural excitability, network communication, and sleep–wake regulatory circuits.36 Non-invasive neuromodulation is generally distinguished by its non-invasive nature and favorable tolerability, although its targeting precision, safety profile, and clinical efficacy differ substantially across techniques and indications.37 Over recent decades, a growing body of research has explored its potential role in improving sleep and related neurophysiological disturbances.
TMS and Cortical Excitability Modulation
TMS, first introduced as a brain stimulation technique by Barker et al in 1985,21 delivers brief electromagnetic pulses through a coil placed over the scalp, thereby inducing electrical currents in superficial cortical regions. Clinically, TMS-based protocols have been approved or investigated for selected neuropsychiatric indications and are also used to assess cortical inhibitory and excitatory circuits, as well as neurotransmission pathways, in neurological and neuropsychiatric disorders.38–40
Repetitive TMS (rTMS) modulates cortical activity by delivering repeated magnetic pulses that induce electrical currents in brain tissue. Depending on stimulation frequency, rTMS can exert excitatory or inhibitory effects: high-frequency stimulation, usually ≥5 Hz, tends to increase cortical excitability, whereas low-frequency stimulation, usually ≤1 Hz, tends to reduce excitability. These effects are thought to influence synaptic function and neuroplasticity, which may be relevant to insomnia-related hyperarousal and network dysregulation.
In insomnia studies, the dorsolateral prefrontal cortex (DLPFC) is among the most frequently selected stimulation targets because of its involvement in arousal regulation, emotional processing, and large-scale brain networks, including the default mode network (DMN).41 By modulating DLPFC excitability, rTMS may influence insomnia-related network abnormalities (Figure 2). 42 It may also affect hypothalamic-pituitary-adrenal (HPA) axis activity and stress-related neuroendocrine responses, which are relevant to patients with comorbid anxiety or depressive symptoms.43–45
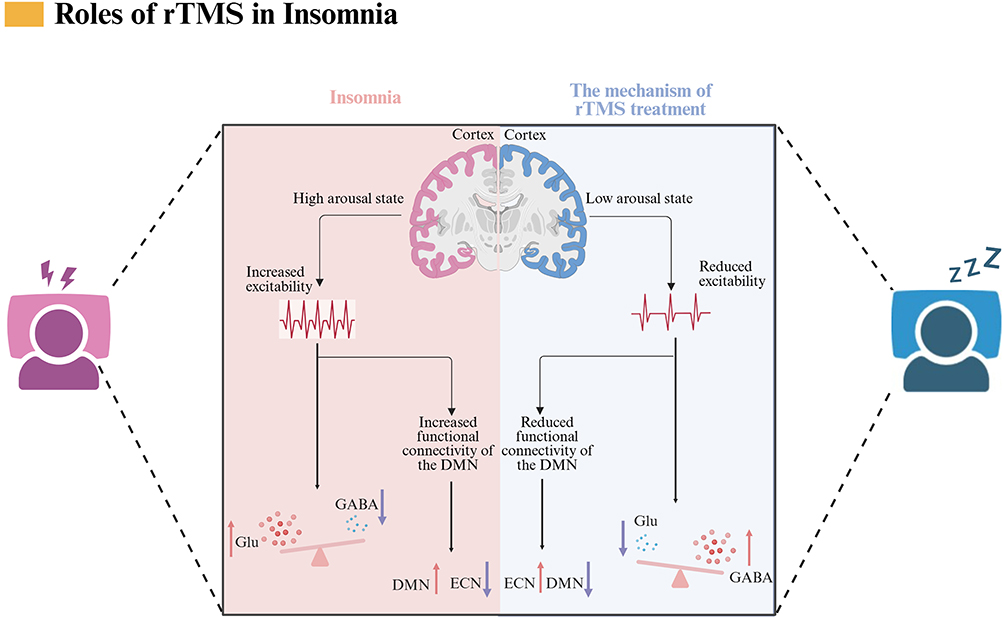 |
Figure 2 Schematic representation of the working principle of rTMS. Abbreviations: Glu, Glutamate; GABA, Gamma-Aminobutyric Acid; DMN, Default Mode Network; ECN, Executive Control Network. |
Several studies have suggested that rTMS may improve cognitive performance, shorten recovery from sleep deprivation-related cognitive impairment, and reduce Pittsburgh Sleep Quality Index (PSQI) scores.40,46 When combined with conventional pharmacotherapy, rTMS has been reported to further improve sleep structure in circadian rhythm disorders and reduce Hamilton Depression Rating Scale (HAMD) and Hamilton Anxiety Rating Scale (HAMA) scores, possibly through serotonin- and γ-aminobutyric acid (GABA)-related mechanisms.42,47 It may also contribute to improvements in sleep continuity, sleep structure, and perceived restorative sleep.48 Nevertheless, these findings should be interpreted cautiously. rTMS may be more suitable for selected patients, such as those with refractory insomnia or comorbid depressive symptoms, and should be avoided or used cautiously in individuals with epilepsy, intracranial metal implants, or other relevant contraindications. Common adverse events include scalp discomfort and transient headache.49,50
Despite its therapeutic promise, the clinical translation of rTMS for insomnia remains limited by substantial methodological heterogeneity. Existing studies differ in stimulation frequency, pulse dose, treatment duration, number of sessions, and outcome assessment, which may lead to inconsistent modulation of target neural circuits.51–54 Target selection also varies across trials. Although the DLPFC remains the most frequently used target, other regions, including the motor and parietal cortices, have also been investigated, often without direct comparative justification.55–57
This heterogeneity is also evident at the study level. Early clinical work by Jiang et al reported improvements in sleep-related outcomes in patients with chronic primary insomnia, whereas later studies examined more specific network-oriented protocols, including 1 Hz rTMS over the left DLPFC and parietal stimulation in patients with comorbid generalized anxiety disorder and insomnia.43,45,57 Other studies have explored EEG or functional-connectivity changes as potential predictors or correlates of treatment response, while combined rTMS–tDCS protocols have begun to examine whether multimodal stimulation provides additional benefit.44,55,56 Patient heterogeneity further complicates interpretation, with some evidence suggesting that response may differ between patients with comorbid depression or anxiety and those with primary insomnia alone.58 A recent systematic review and meta-analysis further summarized randomized evidence for rTMS in insomnia but emphasized the influence of small sample sizes, heterogeneous protocols, and variable study quality.59 Taken together, current findings suggest that rTMS effects are not uniformly observed across insomnia populations and should be interpreted as protocol- and phenotype-dependent rather than uniformly effective.
Although rTMS may alleviate insomnia-related hyperarousal by modulating interactions among the executive control network (ECN), DMN, and corticothalamic circuits, existing studies remain limited by small sample sizes, insufficient blinding, heterogeneous stimulation protocols, and inconsistent polysomnography (PSG)-based outcomes. Future research should clarify optimal stimulation parameters, improve target localization, and examine how different patient subtypes relate to treatment response.59 Larger sham-controlled trials are also needed to establish standardized protocols, expand study populations, and improve the reproducibility of clinical and objective sleep outcomes. In parallel, neuroimaging, electroencephalography (EEG), and machine learning approaches may help identify biomarkers for individualized treatment strategies, supporting more precise intervention across different insomnia phenotypes and potentially improving the clinical stability of rTMS outcomes.
tACS and Brain Rhythm Modulation
tACS is a non-invasive technique that modulates brain activity via low-intensity alternating current to the scalp. It has been investigated as a potential intervention for insomnia because of its capacity to interact with sleep-related neural rhythms and network activity.28,60 Mechanistically, tACS is thought to influence cortical excitability and neural communication by promoting synchronization or desynchronization within frequency-specific oscillatory networks.61 When the stimulation frequency is aligned with endogenous neural oscillations, tACS may entrain specific frequency bands, including slow-wave activity (SWA), which is closely related to deep sleep and sleep restoration (Figure 3).
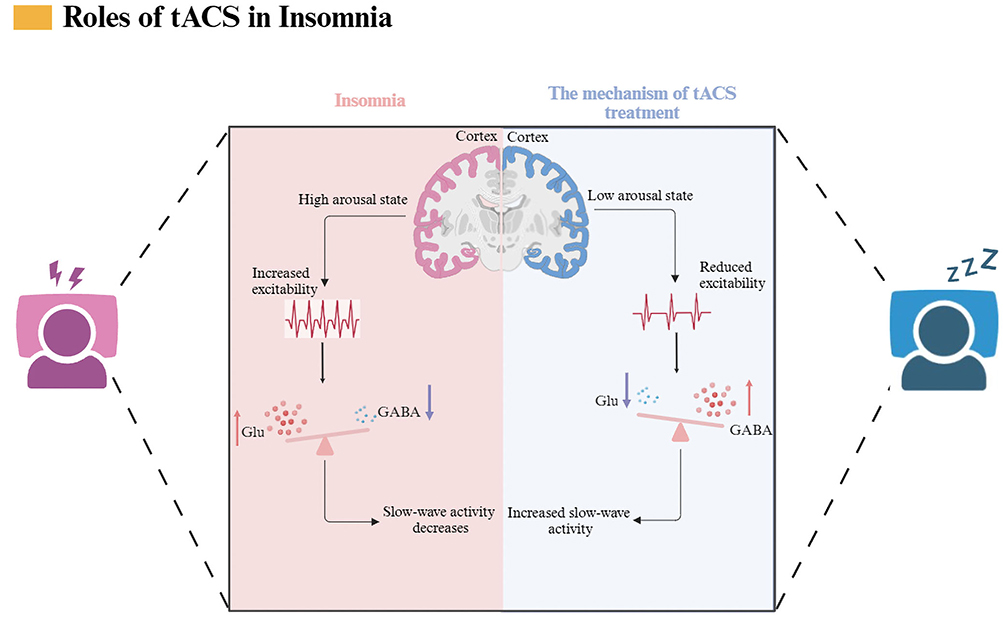 |
Figure 3 Schematic diagram of the transcranial alternating current stimulation (tACS) technique. Abbreviations: Glu, Glutamate; GABA, Gamma-Aminobutyric Acid. |
Experimental studies further suggest that the entrainment effects of tACS may depend on neuronal subtype and network state. Fast-spiking inhibitory interneurons, for example, appear to show stronger phase-locked responses to alternating current because of their distinctive electrophysiological properties.61–63 This cell-type sensitivity may help explain how weak oscillatory stimulation can influence broader network dynamics, although the extent to which these mechanisms translate into clinical sleep improvement remains under investigation.
Several studies have reported potential sleep-improving effects of tACS, but the findings are not uniformly consistent. Garside et al reported that 0.75 Hz tACS reduced slow-wave EEG power, suggesting that stimulation effects may vary according to timing, frequency, and sleep state.64 In contrast, Zhou et al reported that 0.75 Hz tACS was associated with enhanced slow-wave oscillations, lower Insomnia Severity Index (ISI) scores, greater improvement than sham stimulation, an approximately 27-minute reduction in sleep onset latency (SOL), an approximately 13% increase in sleep efficiency (SE), a 47-minute increase in total sleep time (TST), and no reported adverse effects.65
Other clinical studies have also suggested potential benefits. Wang et al reported that tACS reduced ISI scores from 19.5 to 10.3, increased SE to 90% compared with 81% in the sham group, and shortened SOL by approximately 25 minutes; these effects appeared to persist at the 4-week follow-up.28 Simons et al reported improvements in SOL, SE, and TST after 0.75 Hz stimulation, with no serious adverse reactions reported.30 These findings suggest that tACS may be particularly relevant for insomnia phenotypes characterized by reduced slow-wave sleep. Mild scalp paresthesia or local discomfort has been reported in some studies, whereas serious adverse events appear uncommon under conventional stimulation parameters.66,67 Nevertheless, caution is required in individuals with implanted electronic devices because of potential current interference, and the optimal range of stimulation intensity remains to be defined.68
tACS may modulate neural activity through frequency-specific entrainment of endogenous brain rhythms and may be particularly relevant for targeting slow-wave activity (SWA) and deep sleep.69,70 However, the clinical translation of tACS remains constrained by substantial methodological heterogeneity. Existing studies differ in stimulation frequency, intensity, electrode montage, session duration, treatment schedule, and outcome measures, limiting cross-trial comparability.30,35,66,68 Although several trials have reported that slow-wave tACS may enhance deep sleep,30 other evidence suggests that higher-frequency stimulation may shorten sleep latency,71 indicating that optimal frequency selection is likely phenotype-dependent. More recent sham-controlled and GRADE-assessed evidence further suggests that tACS does not consistently outperform sham stimulation across insomnia severity or objective sleep outcomes, reinforcing that its effects are frequency-, timing-, and phenotype-dependent rather than uniformly sleep-promoting.68,72
Despite the favorable safety and portability of tACS, the evidence base is curtailed by small, relatively homogeneous samples, limited validation across age groups and insomnia subtypes, and insufficient long-term follow-up on durability and adverse events.64 Accordingly, future studies should move beyond generic stimulation protocols and define the frequency–efficacy relationship more precisely. Adequately powered, sham-controlled trials are needed to include broader age groups and insomnia subtypes, extend follow-up, systematically monitor adverse events, and incorporate EEG-based biomarkers to guide individualized stimulation parameters.
tDCS and Cortical Excitability Regulation
tDCS is a non-invasive technique that modulates cortical excitability by applying low-intensity direct current through scalp electrodes. The resulting electric field shifts neuronal resting membrane potentials, with anodal stimulation generally increasing cortical excitability and cathodal stimulation tending to reduce it. Experimental evidence suggests that tDCS can modulate human sleep duration,73 with one proposed mechanism involving modulation of excitatory-inhibitory balance in key brain regions (Figure 4).
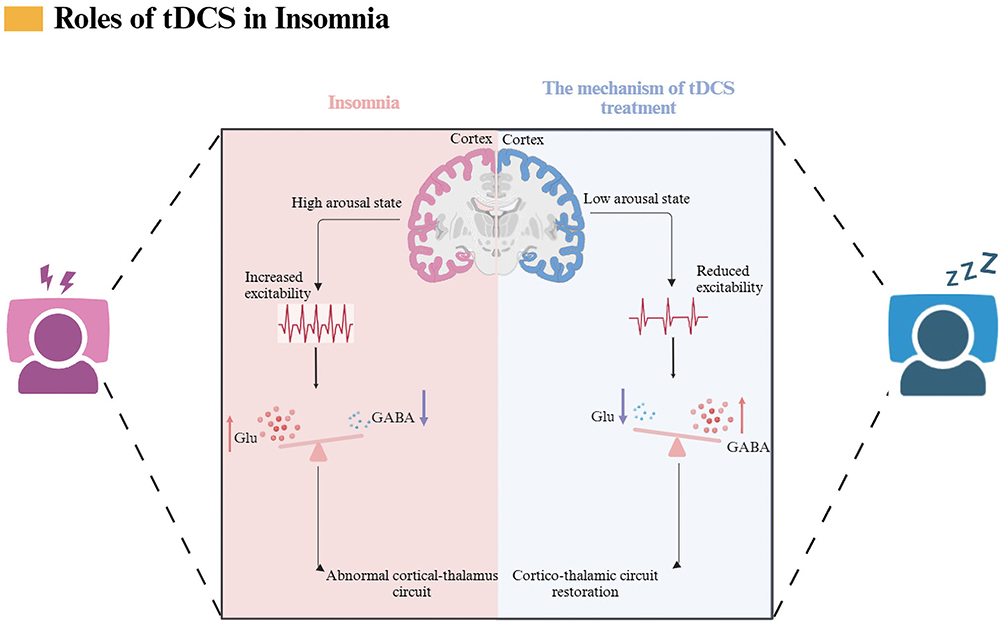 |
Figure 4 Schematic diagram of the tDCS technique. Abbreviations: Glu, Glutamate; GABA, Gamma-Aminobutyric Acid. |
Unlike sedative-hypnotic drugs, which act partly through bottom-up ascending arousal systems, tDCS has been investigated as a way to modulate top-down prefrontal–thalamocortical circuits.74 The DMPFC has been implicated in sleep homeostasis and daytime sleepiness, and tDCS may influence its excitatory–inhibitory balance, thereby contributing to changes in sleep quality and arousal regulation.75,76 At the cellular level, these effects may involve changes in synaptic transmission and long-term potentiation- or depression-like plasticity.
Several lines of evidence have examined the sleep-related effects of tDCS, although the available studies differ in experimental model, stimulation target, and outcome assessment. In a preclinical study, Su et al reported that tDCS prolonged non-rapid eye movement (NREM) sleep in normal mice and improved stress-induced acute insomnia, possibly through activation of the infralimbic cortex–ventrolateral preoptic area (IL–VLPO) pathway.77 In clinical settings, a randomized, double-blind, sham-controlled trial by Li et al reported better sleep quality, shorter sleep onset latency, higher sleep efficiency, and reduced daytime sleepiness after tDCS compared with sham stimulation.75 Dondé et al further reported that anodal tDCS may increase cortical excitability and improve subjective sleep quality in patients with chronic insomnia.78 Taken together, these studies suggest that tDCS may be particularly relevant for insomnia phenotypes characterized by sleep-onset difficulties or cortical hyperarousal. However, the most consistent signal remains centered on subjective sleep improvement, whereas objective sleep architecture, durability of benefit, and dose–response relationships remain less consistently established.
These findings suggest that tDCS may be relevant for insomnia phenotypes characterized by difficulty initiating sleep. However, it should be used cautiously in individuals with scalp dermatoses and in pregnancy, and common adverse events include localized tingling and erythema.79 Although tDCS has practical advantages, including portability, relatively low cost, and potential suitability for supervised home-based use, reproducible efficacy remains constrained by non-standardized protocols and stimulation-related variability.
Targeting the DMPFC for top‑down modulation is conceptually appealing, yet in practice the injected current spreads diffusely through the head—its path heavily dependent on individual anatomy—so that off‑target regions are often co‑activated and spatial specificity is blunted.73,80 This interindividual variability likely contributes to the inconsistent neurophysiological outcomes observed when identical protocols are applied to different participants. The dose–response relationships linking current intensity and treatment duration to neuroplasticity also remain poorly characterized, leaving parameter selection largely empirical.81 An additional methodological concern involves blinding: conventional sham procedures rarely reproduce the cutaneous sensations that accompany active stimulation, making it easier for participants or experimenters to distinguish conditions and introducing possible performance and detection biases.82–84
Accordingly, tDCS findings should be interpreted cautiously. Reported subjective benefits may coexist with inconsistent objective sleep outcomes, and stimulation polarity, timing, current distribution, and sham integrity can substantially influence both the direction and specificity of observed effects.73,78 Larger, well-controlled trials are therefore needed to further evaluate efficacy and mechanisms,78 integrate EEG or fMRI for individualized target localization and dose optimization, and adopt rigorous sham controls and standardized reporting in tele-supervised or home-based settings to improve reliability, reproducibility, and clinical generalizability.
TaVNS and Autonomic Nerve Modulation
The vagus nerve (VN) is a major cranial nerve with bidirectional afferent and efferent signaling and is a central component of autonomic regulation. Through its afferent projections and parasympathetic efferent pathways, the VN participates in the regulation of visceral function, emotional state, and sleep–wake processes.85 Vagus nerve stimulation (VNS) acts partly through activation of vagal afferent fibers, which project to brainstem nuclei and subsequently influence broader autonomic and neuroendocrine networks.
taVNS provides a non-invasive approach to modulating vagal pathways through stimulation of the auricular branch of the VN. Mechanistically, taVNS may influence the locus coeruleus–norepinephrine (LC–NE) system, cholinergic activity, and hypothalamic-pituitary-adrenal (HPA) axis regulation, all of which are involved in arousal, stress responsivity, and sleep–wake regulation (Figure 5). 86,87 Preliminary evidence suggests that taVNS may improve autonomic function, increase vagal tone, and alleviate insomnia-related symptoms.88–90
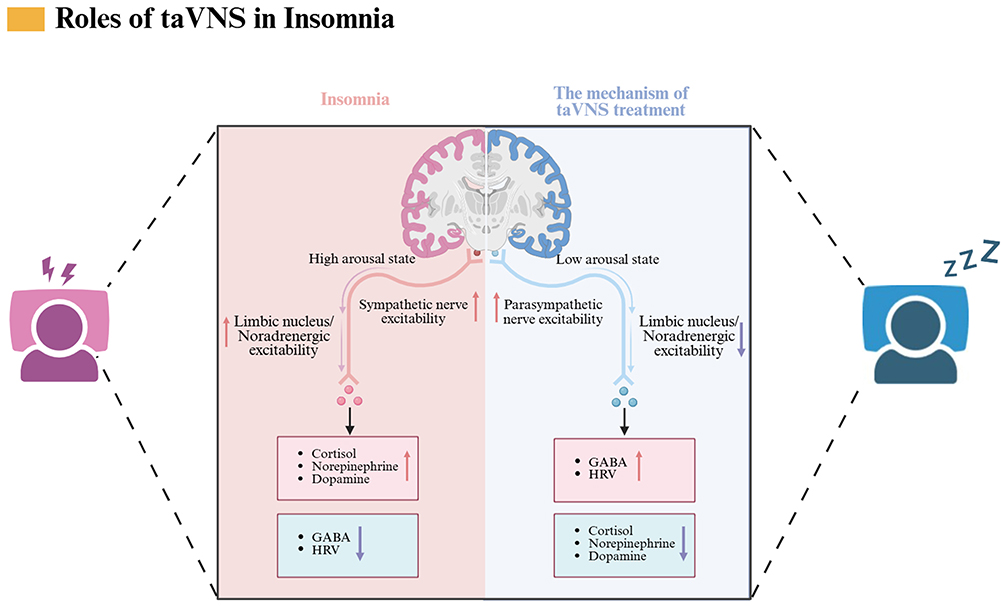 |
Figure 5 Schematic diagram of the taVNS technique. Abbreviations: GABA, Gamma-Aminobutyric Acid; HRV, Heart Rate Variability. |
The available evidence for taVNS also spans heterogeneous study designs and clinical contexts. Kinfe et al reported that non-invasive VNS may enhance autonomic nervous system function through vagus–hypothalamus pathways, supporting the potential relevance of vagal modulation for pain and sleep regulation.91 In a single-center, single-blind randomized controlled trial, Zhang et al reported that 8 weeks of taVNS in patients with chronic insomnia was associated with reductions in Pittsburgh Sleep Quality Index (PSQI), Insomnia Severity Index (ISI), and Generalized Anxiety Disorder-7 (GAD-7) scores, an approximately 22-minute increase in N3 sleep, an approximately 20-minute reduction in sleep onset latency, and no reported adverse reactions.92 Wu et al reported improvements in primary insomnia, particularly high-altitude insomnia, including increased deep sleep and shorter sleep onset latency compared with CBT-I.85 Yeom et al also reported that taVNS may improve sleep and reduce anxiety and depressive symptoms, with no significant side effects reported.89 Collectively, these studies suggest that taVNS may be most relevant for insomnia accompanied by autonomic imbalance, anxiety-related symptoms, or intolerance to pharmacological treatment. Nevertheless, differences in stimulation site, comparator condition, patient population, and follow-up duration limit direct comparison across studies and preclude firm conclusions regarding a unified taVNS protocol.
These findings suggest that taVNS may be particularly relevant for insomnia phenotypes characterized by autonomic imbalance, comorbid anxiety, or intolerance to pharmacological treatment.92 However, taVNS should still be regarded as an emerging investigational approach rather than an established treatment for chronic insomnia. It should also be avoided or used cautiously in individuals with cochlear implants, active auricular infection, or other local conditions that may affect stimulation safety and tolerability.
The clinical translation of taVNS is further limited by methodological heterogeneity. Stimulation parameters, including frequency, intensity, pulse width, stimulation duration, and auricular site selection, vary considerably across studies, reducing comparability and making it difficult to define an optimal protocol.92,93 In addition, interindividual variation in the anatomical distribution of the auricular vagus nerve may influence stimulation engagement and treatment response, yet this factor is often insufficiently considered in trial design.85,90 Current taVNS evidence should therefore be interpreted as promising but preliminary. Positive symptom-level findings require confirmation in larger sham-controlled trials with standardized stimulation sites, clearly defined autonomic phenotypes, longer follow-up, and systematic safety reporting.85,90,92,93
To clarify its role in clinical sleep medicine, future research should prioritize evidence-based standardized protocols, large-scale trials, long-term efficacy and safety evaluation, and characterization of response variability across diverse patient populations.
Safety and Contraindications Across Modalities
Although NIBS modalities are generally well tolerated under conventional stimulation parameters, safety considerations remain essential before broader clinical translation.
For rTMS, the most clinically significant acute risk is the induction of seizures. However, expert guidelines suggest that this risk remains low when conventional stimulation parameters, focal coils, and appropriate screening procedures are employed.38,94 rTMS should be avoided or administered with particular caution in individuals with epilepsy or those at elevated risk for seizures, as well as in patients with unstable neurological conditions, intracranial metallic implants, implanted stimulators, or other devices susceptible to magnetic fields.94,95 Common adverse events include scalp discomfort, transient headache, and local pain, whereas serious events are rare when established safety recommendations are followed.38,94
For tDCS and tACS, available safety guidelines indicate that conventional low-intensity transcranial electrical stimulation is generally well tolerated, although adverse events should still be systematically monitored.96,97 Mild adverse effects include tingling, itching, burning sensations, erythema, headache, fatigue, phosphenes, and transient discomfort at electrode sites.98–100 Less common but clinically relevant events, such as skin burns, may occur when electrode–skin contact is suboptimal.99,100 Caution is warranted in patients with implanted electronic devices, skull defects, active scalp disease, skin lesions, or other conditions that may alter current distribution.96,97 Home-based or repeated stimulation protocols also require remote supervision, standardized electrode placement, predefined dose limits, and structured adverse-event reporting.97,101,102
For taVNS, systematic review and pooled safety data suggest a favorable tolerability profile, with common adverse events including ear pain, headache, tingling, and local skin redness or irritation.103,104 However, adverse-event reporting remains inconsistent across studies, and stimulation duration, intensity, site selection, and auricular anatomy may influence tolerability.103,104 In chronic insomnia specifically, randomized clinical evidence has reported that taVNS was generally well tolerated, although larger multicenter trials remain necessary to confirm safety across broader populations.92 taVNS should be avoided or used cautiously in patients with active auricular infection, local skin lesions, cochlear implants, or clinically unstable cardiac conditions unless specialist assessment is available.103,104
Across all modalities, stimulation intensity, session duration, electrode or coil placement, contraindication screening, adverse-event monitoring, and predefined stopping rules should be transparently reported. At the current stage, NIBS should be considered an investigational or adjunctive strategy for chronic insomnia rather than a universally applicable first-line treatment.
Overcoming Heterogeneity: Towards Precise Neuromodulation
A significant challenge confronting traditional NIBS interventions for chronic insomnia is the considerable heterogeneity in treatment responses, which varies markedly among individuals and often proves difficult to replicate consistently.105 This issue largely stems from a disconnect between conventional intervention strategies and the diverse nature of chronic insomnia itself.106 Chronic insomnia does not arise from a singular mechanism; rather, it is sustained by a confluence of interacting processes, including cortical hyperarousal, abnormal coupling within large-scale brain networks, and autonomic imbalance.107 When a uniform protocol with fixed targets and parameters is employed across patients exhibiting different neural abnormalities, treatment effects are likely to differ and may appear unstable
Consequently, advancing toward more precise NIBS may be important for enhancing clinical translation. The clinical merit of this approach lies in aligning target selection, parameter settings, and treatment planning more closely with each patient’s neurophysiological profile.108 The objective is not merely to increase technical complexity but to establish a treatment pathway that is more reproducible and adaptable in a clinical context. By utilizing available neurophysiological data for patient stratification, implementing standardized localization methods to minimize targeting errors, and employing objective indicators to monitor treatment responses, it may be feasible to enhance both intervention accuracy and treatment stability.
From Fixed Anatomical Targets to Individualized Functional Targets
Numerous NIBS studies continue to utilize group-averaged anatomical coordinates for stimulation targets, like the dorsolateral prefrontal cortex.109–112 However, variations in spatial distribution and connectivity patterns of insomnia-related network abnormalities exhibit significant interindividual differences.113 Consequently, the same anatomical site may correspond to diverse dysfunctional circuits among patients, leading to variability in treatment response.114 Enhancing reproducibility necessitates a shift from fixed anatomical locations towards functionally relevant regions that align more closely with each patient’s unique network profile.115,116
This transition relies on integrating multimodal neuro-assessment with computational approaches to enhance target precision and uniformity.111 Individualized connectivity patterns can be characterized using resting-state functional magnetic resonance imaging to pinpoint network hubs more closely associated with the patient’s symptoms.114,117 In this context, target localization seeks to position stimulation at a site more likely to modulate the pertinent dysfunctional network rather than solely relying on a fixed anatomical coordinate.118,119 Initial findings propose that imaging-or connectivity-guided navigated repetitive transcranial magnetic stimulation could ameliorate insomnia symptoms and potentially induce reorganization of relevant functional networks.118,119 Nevertheless, the superiority of this approach over conventional anatomical targeting in chronic insomnia necessitates validation through high-quality comparative studies.119
Electroencephalographic (EEG) biomarkers may also provide a more direct basis for individualizing stimulation parameters.120 Patients with insomnia often show abnormalities in specific neural oscillations.121 Quantifying these features may help adjust the frequency and phase of transcranial alternating current stimulation from generic empirical settings toward protocols that better reflect individual physiological characteristics.110 Selecting stimulation parameters according to slow-wave oscillatory features may improve the specificity of rhythm entrainment and may help explain why previous findings have been inconsistent when stimulation parameters do not match patient phenotype.122
A further step toward clinical implementation is to combine multimodal neural data with clinical information and apply machine learning models to predict response before treatment begins.123 Such models may support patient stratification and reduce trial and error in treatment selection. In practice, this process may begin with more accessible data such as clinical scales and sleep diaries, then expand to EEG, and where feasible, imaging-based indicators. Overall, moving from fixed anatomical targets to individualized functional targets offers a clearer and more implementable way to reduce variability caused by inaccurate targeting, parameter mismatch, and population heterogeneity.
From Static Open-Loop Stimulation to Dynamic Closed-Loop Modulation
Traditional open-loop stimulation relies on fixed parameters and fails to adapt to ongoing fluctuations in sleep stages or brain states. Consequently, its capacity to modulate relevant rhythms and networks may be constrained, leading to unstable efficacy and increased interindividual variability. In contrast, closed-loop neuromodulation integrates physiological monitoring with stimulation delivery within a real-time adaptive framework.124 By continuously acquiring signals, identifying key events or abnormal states associated with sleep instability, and triggering stimulation or adjusting parameters as necessary, this approach may better synchronize stimulation timing and intensity with the patient’s current physiological state.124 This may enhance the consistency and reproducibility of the intervention while providing a more operational pathway for clinical translation.
The EEG serves as one of the most commonly utilized feedback sources in this context.125 Through continuous monitoring and online analysis via wearable EEG systems, it becomes feasible to detect features of arousal intrusion and rhythmic events pertinent to sleep maintenance, thereby optimizing the timing and parameter settings of TMS or tACS.125 When signals indicate sleep fragmentation or diminished spindle activity, stimulation frequency, intensity, or duration may be adjusted within predefined safety limits, potentially enhancing the modulation of sleep architecture.126 For tACS specifically, aligning stimulation timing or key parameters with slow-wave activity is consistent with its reliance on endogenous rhythms.127
In addition to central EEG signals, peripheral physiological indicators may be integrated into the feedback loop to assess autonomic dysfunction, which is particularly pertinent for insomnia patients experiencing anxiety, palpitations, or significant autonomic symptoms.31 Heart rate variability and skin conductance can indicate dynamic fluctuations in sympathovagal balance and may function as potential feedback or process-monitoring biomarkers in interventions such as taVNS; however, direct evidence supporting their application in closed-loop parameter optimization remains scarce.92,128
The transition of closed-loop systems into clinical practice will depend strongly on their reliability and safety. Effective implementation necessitates robust signal acquisition, timely and stable event detection, precise control of trigger delay, and well-defined safety protocols, including intensity limits, trigger rules, stopping criteria, and adverse-event monitoring.129 It should not be assumed that closed-loop stimulation is inherently superior to open-loop stimulation; trigger rules and stimulation dosages must be tailored to the characteristics of the target population and validated through controlled clinical trials. A practical translational pathway may therefore entail a gradual development process, commencing with reliable sleep staging and event detection, followed by the establishment of refined safety boundaries, and subsequently allowing for limited dynamic parameter adjustments. Enhancements in the comfort, stability, and affordability of wearable sensors will also be crucial for long-term and home-based applications.126
From Single-Technology Intervention to Synergistic Integrated Treatment Pathways
Chronic insomnia frequently coexists with cognitive hyperarousal, emotional stress, and autonomic imbalance.117,130,131 Consequently, a single non-invasive brain stimulation (NIBS) technique may be insufficient to address all pertinent dimensions. A more clinically viable approach is to utilize NIBS as a treatment modality that can be administered in combination, with specific pathways chosen based on the insomnia phenotype and comorbidity profile, and assessed through standardized outcome measures and follow-up protocols.56
At the technical level, various NIBS modalities can be integrated to achieve complementary objectives. For instance, tDCS may be employed to modulate baseline cortical excitability,77 tACS to influence sleep-related rhythmic activity,66 and rTMS to target cortical networks associated with arousal and emotion.119 Preliminary studies have begun to assess the feasibility and safety of combined protocols, such as tDCS and rTMS.56 The efficacy of such combinations does not stem from mere additive application; rather, it relies on the precise definition of each technique’s role, sequence, and parameter range to minimize arbitrary variation and enhance comparability and reproducibility.
Integrating NIBS with Cognitive Behavioral Therapy for Insomnia (CBT-I) aligns with guideline-oriented care pathways.132 In patients exhibiting significant hyperarousal or emotional distress, rTMS or tDCS may be employed initially to mitigate excessive arousal, thereby establishing a more stable environment for the behavioral and cognitive elements of CBT-I.75,119 Subsequently, CBT-I can facilitate the consolidation of post-treatment modifications in sleep patterns and cognition, ultimately reducing the risk of relapse. For individuals with heightened sympathetic activity or comorbid anxiety disorders, the integration of taVNS into a comprehensive treatment pathway may be more suitable Additionally, autonomic indicators, such as HRV, could serve as objective metrics for monitoring progress and tailoring interventions.92,131
In cases of severe acute symptoms, short-term pharmacotherapy may be considered to manage symptoms, followed by NIBS to promote sustained improvement and subsequent medication optimization.132 Nonetheless, this sequential approach necessitates further rigorous controlled studies to delineate the patient populations most likely to benefit and to establish the relevant safety parameters.
Summary and Outlook
Summary
The central message of this review is that the clinical value of NIBS for chronic insomnia is unlikely to depend on uniform stimulation protocols applied to broad insomnia populations, but rather on matching stimulation strategies to specific neurophysiological and clinical phenotypes. Current evidence suggests that rTMS, tACS, tDCS, and taVNS engage distinct mechanisms related to cortical and thalamocortical hyperarousal, default mode network dysregulation, sleep-related oscillations, and autonomic imbalance. These modalities may improve selected sleep-related outcomes, particularly in patients who respond inadequately to, or cannot tolerate, conventional therapies. Table 1 summarizes their main mechanisms, advantages, limitations, and phenotype-informed clinical considerations.
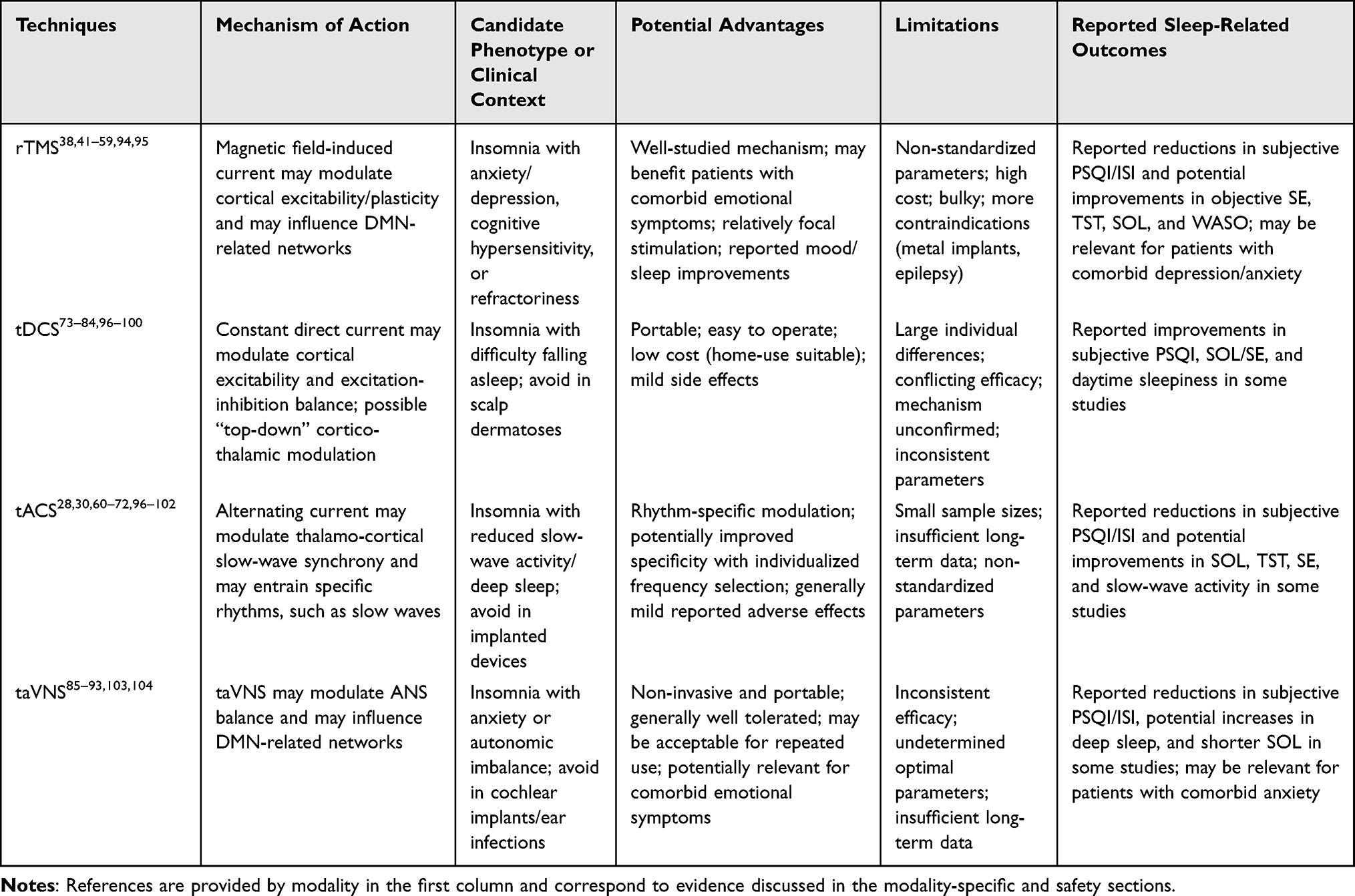 |
Table 1 Comparative Summary of Mechanisms, Potential Clinical Contexts, Advantages, Limitations, and Reported Sleep-Related Outcomes Across NIBS Modalities |
However, these techniques are not interchangeable, and the available evidence remains limited by heterogeneous stimulation parameters, small samples, variable sham designs, short follow-up, and inconsistent outcome reporting. Therefore, NIBS should not currently be regarded as a routine first-line treatment for chronic insomnia. Its future clinical translation will depend on standardized protocols, phenotype-informed patient selection, objective sleep and biomarker-based assessment, and integration with established care pathways such as CBT-I or pharmacotherapy.
Outlook
Future research should prioritize precision, reproducibility, and clinical implementability rather than simply accumulating additional efficacy data. A key task is to define evidence-based stimulation protocols for each modality, including stimulation site, frequency, intensity, session duration, treatment schedule, and sham-control design. Standardized reporting of these parameters will be essential for improving comparability across studies and for determining whether observed effects are reproducible across different insomnia populations.
Another important direction is the integration of biomarkers into patient stratification and treatment optimization. Neuroimaging, electroencephalography, autonomic measures, and machine learning approaches may help identify predictors of response, refine target selection, and clarify the mechanisms underlying treatment variability. Closed-loop systems based on real-time physiological feedback may further support adaptive stimulation delivery, although their superiority over conventional open-loop approaches should be validated in controlled clinical trials.
Clinical translation will also require broader and more rigorous validation. Future studies should include adequately powered sham-controlled designs, longer follow-up periods, diverse age groups, clearly defined insomnia phenotypes, and patients with common psychiatric or cardiometabolic comorbidities. Both subjective and objective sleep outcomes should be incorporated, and adverse events, contraindications, and treatment burden should be systematically reported. In parallel, portable or home-use devices should be evaluated not only for efficacy, but also for usability, adherence, safety, and cost-effectiveness.
Overall, NIBS may move from promising therapeutic signals toward more reliable and clinically applicable interventions only if future studies combine methodological standardization, phenotype-informed selection, biomarker-guided optimization, and integration with established care pathways such as CBT-I, pharmacotherapy, and autonomic monitoring.
Data Sharing Statement
No new datasets were generated or analyzed during the preparation of this narrative review. The evidence summarized in this article is based on previously published studies cited in the reference list. Materials supporting the review, including information used for evidence synthesis where applicable, are available from the corresponding author upon reasonable request.
Author Contributions
Wu-lan Ao: Writing - review & editing, Writing - original draft, Investigation, Formal analysis, Data curation, Conceptualization. Zheng Liu: Writing - review & editing, Investigation, Conceptualization. Zi-yi Zhao: Investigation, Data curation. Wen-chang Zhu: Investigation, Data curation. Si-qi Guan: Investigation, Data curation. Yong-su Zheng: Formal analysis, Funding acquisition, Visualization. Hao Huang: Writing - review & editing, Writing - original draft, Supervision, Investigation, Formal analysis, Funding acquisition, Conceptualization. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Medical Research Union Fund for High-quality health development of Guizhou Province (2024GZYXKYJJXM0102). Zunyi City Bureau of Science, Technology and Big Data (Zunshi Kehe HZ Zi (2023) 211).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Riemann D, Benz F, Dressle RJ, et al. Insomnia disorder: state of the science and challenges for the future. J Sleep Res. 2022;31(4):e13604. doi:10.1111/jsr.13604
2. Georgiev T, Paunova R, Todeva-Radneva A, et al. Aberrant effective connectivity within and between the default mode, executive control, and salience networks in chronic insomnia disorder-toward identifying the hyperarousal state. Biomedicines. 2025;13(6). doi:10.3390/biomedicines13061293
3. Medalie L, Cifu AS. Management of chronic insomnia disorder in adults. JAMA. 2017;317(7):762–18. doi:10.1001/jama.2016.19004
4. Riemann D, Nissen C, Palagini L, Otte A, Perlis ML, Spiegelhalder K. The neurobiology, investigation, and treatment of chronic insomnia. Lancet Neurol. 2015;14(5):547–558. doi:10.1016/S1474-4422(15)00021-6
5. Porosnicu Rodriguez KA, Salas RME, Schneider L. Insomnia: personalized diagnosis and treatment options. Neurol Clin. 2023;41(1):1–19. doi:10.1016/j.ncl.2022.07.004
6. Roach M, Juday T, Tuly R, Chou JW, Jena AB, Doghramji PP. Challenges and opportunities in insomnia disorder. Int J Neurosci. 2021;131(11):1058–1065. doi:10.1080/00207454.2020.1773460
7. Li M, Zhang XW, Hou WS, Tang ZY. Insomnia and risk of cardiovascular disease: a meta-analysis of cohort studies. Int J Cardiol. 2014;176(3):1044–1047. doi:10.1016/j.ijcard.2014.07.284
8. Hertenstein E, Feige B, Gmeiner T, et al. Insomnia as a predictor of mental disorders: a systematic review and meta-analysis. Sleep Med Rev. 2019;43:96–105. doi:10.1016/j.smrv.2018.10.006
9. Mirchandaney R, Barete R, Asarnow LD. Moderators of cognitive behavioral treatment for insomnia on depression and anxiety outcomes. Curr Psychiatry Rep. 2022;24(2):121–128. doi:10.1007/s11920-022-01326-3
10. Chan WS, Levsen MP, McCrae CS. A meta-analysis of associations between obesity and insomnia diagnosis and symptoms. Sleep Med Rev. 2018;40:170–182. doi:10.1016/j.smrv.2017.12.004
11. Anothaisintawee T, Reutrakul S, Van Cauter E, Thakkinstian A. Sleep disturbances compared to traditional risk factors for diabetes development: systematic review and meta-analysis. Sleep Med Rev. 2016;30:11–24. doi:10.1016/j.smrv.2015.10.002
12. Herrero Babiloni A, Bellemare A, Beetz G, et al. The effects of non-invasive brain stimulation on sleep disturbances among different neurological and neuropsychiatric conditions: a systematic review. Sleep Med Rev. 2021;55:101381. doi:10.1016/j.smrv.2020.101381
13. Qaseem A, Kansagara D, Forciea MA, Cooke M, Denberg TD. Clinical guidelines committee of the American College of P. management of chronic insomnia disorder in adults: a clinical practice guideline from the American college of physicians. Ann Intern Med. 2016;165(2):125–133. doi:10.7326/M15-2175
14. Edinger JD, Arnedt JT, Bertisch SM, et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2021;17(2):255–262. doi:10.5664/jcsm.8986
15. Morin CM, Vallieres A, Guay B, et al. Cognitive behavioral therapy, singly and combined with medication, for persistent insomnia: a randomized controlled trial. JAMA. 2009;301(19):2005–2015. doi:10.1001/jama.2009.682
16. Kripke DF. Mortality risk of hypnotics: strengths and limits of evidence. Drug Saf. 2016;39(2):93–107. doi:10.1007/s40264-015-0362-0
17. Madari S, Golebiowski R, Mansukhani MP, Kolla BP. Pharmacological management of insomnia. Neurotherapeutics. 2021;18(1):44–52. doi:10.1007/s13311-021-01010-z
18. Shekelle P, Cook I, Miake-Lye IM, et al. The Effectiveness and Risks of Cranial Electrical Stimulation for the Treatment of Pain, Depression, Anxiety, PTSD, and Insomnia: a Systematic Review. 2018. VA Evidence-based Synthesis Program Reports.
19. Frankel BL, Buchbinder R, Snyder F. Ineffectiveness of electrosleep in chronic primary insomnia. Arch Gen Psychiatry. 1973;29(4):563–568. doi:10.1001/archpsyc.1973.04200040103017
20. Brunye TT, Patterson JE, Wooten T, Hussey EK. A critical review of cranial electrotherapy stimulation for neuromodulation in clinical and non-clinical samples. Front Hum Neurosci. 2021;15:625321. doi:10.3389/fnhum.2021.625321
21. Barker AT, Jalinous R, Freeston IL. Non-invasive magnetic stimulation of human motor cortex. Lancet. 1985;1(8437):1106–1107. doi:10.1016/s0140-6736(85)92413-4
22. Hammond EJ, Uthman BM, Wilder BJ, et al. Neurochemical effects of vagus nerve stimulation in humans. Brain Res. 1992;583(1–2):300–303. doi:10.1016/s0006-8993(10)80038-1
23. Ventureyra EC. Transcutaneous vagus nerve stimulation for partial onset seizure therapy. A new concept. Childs Nerv Syst. 2000;16(2):101–102. doi:10.1007/s003810050021
24. Marshall L, Helgadottir H, Molle M, Born J. Boosting slow oscillations during sleep potentiates memory. Nature. 2006;444(7119):610–613. doi:10.1038/nature05278
25. Frohlich F, Schmidt SL. Rational design of transcranial current stimulation (TCS) through mechanistic insights into cortical network dynamics. Front Hum Neurosci. 2013;7:804. doi:10.3389/fnhum.2013.00804
26. Santostasi G, Malkani R, Riedner B, et al. Phase-locked loop for precisely timed acoustic stimulation during sleep. J Neurosci Meth. 2016;259:101–114. doi:10.1016/j.jneumeth.2015.11.007
27. Jones AP, Choe J, Bryant NB, et al. Dose-dependent effects of closed-loop tACS delivered during slow-wave oscillations on memory consolidation. Front Neurosci. 2018;12:867. doi:10.3389/fnins.2018.00867
28. Wang HX, Wang L, Zhang WR, et al. Effect of transcranial alternating current stimulation for the treatment of chronic insomnia: a randomized, double-blind, parallel-group, placebo-controlled clinical trial. Psychother Psychosom. 2020;89(1):38–47. doi:10.1159/000504609
29. He JK, Jia BH, Wang Y, et al. Transcutaneous auricular vagus nerve stimulation modulates the prefrontal cortex in chronic insomnia patients: fMRI study in the first session. Front Neurol. 2022;13:827749. doi:10.3389/fneur.2022.827749
30. Simons SB, Provo M, Yanoschak A, et al. A randomized study on the effect of a wearable device using 0.75 Hz transcranial electrical stimulation on sleep onset insomnia. Front Neurosci. 2024;18:1427462. doi:10.3389/fnins.2024.1427462
31. Kim H, Jung HR, Kim JB, Kim DJ. Autonomic dysfunction in sleep disorders: from neurobiological basis to potential therapeutic approaches. J Clin Neurol. 2022;18(2):140–151. doi:10.3988/jcn.2022.18.2.140
32. Lu Q, Zhang W, Yan H, et al. Connectomic disturbances underlying insomnia disorder and predictors of treatment response. Front Hum Neurosci. 2022;16:960350. doi:10.3389/fnhum.2022.960350
33. Palmer CA, Alfano CA. Sleep and emotion regulation: an organizing, integrative review. Sleep Med Rev. 2017;31:6–16. doi:10.1016/j.smrv.2015.12.006
34. de Zambotti M, Willoughby AR, Franzen PL, Clark DB, Baker FC, Colrain IM. K-complexes: interaction between the central and autonomic nervous systems during sleep. Sleep. 2016;39(5):1129–1137. doi:10.5665/sleep.5770
35. Krone LB, Feher KD, Rivero T, Omlin X. Brain stimulation techniques as novel treatment options for insomnia: a systematic review. J Sleep Res. 2023;32(6):e13927. doi:10.1111/jsr.13927
36. Parpura V, Silva GA, Tass PA, et al. Neuromodulation: selected approaches and challenges. J Neurochem. 2013;124(4):436–453. doi:10.1111/jnc.12105
37. Sabbagh M, Sadowsky C, Tousi B, et al. Effects of a combined transcranial magnetic stimulation (TMS) and cognitive training intervention in patients with Alzheimer’s disease. Alzheimers Dement. 2020;16(4):641–650. doi:10.1016/j.jalz.2019.08.197
38. Stultz DJ, Osburn S, Burns T, Pawlowska-Wajswol S, Walton R. Transcranial magnetic stimulation (TMS) safety with respect to seizures: a literature review. Neuropsychiatr Dis Treat. 2020;16:2989–3000. doi:10.2147/NDT.S276635
39. Santoro V, Hou MD, Premoli I, et al. Investigating cortical excitability and inhibition in patients with schizophrenia: a TMS-EEG study. Brain Res Bull. 2024;212:110972. doi:10.1016/j.brainresbull.2024.110972
40. Lanza G, Fisicaro F, Dubbioso R, et al. A comprehensive review of transcranial magnetic stimulation in secondary dementia. Front Aging Neurosci. 2022;14:995000. doi:10.3389/fnagi.2022.995000
41. Chen J, Li C, Zheng Y, Zhao Z, Deng R, Huang H. Advancements of potential mechanisms of repetitive transcranial magnetic stimulation for refractory insomnia. Current Sleep Med Rep. 2025;11(1):12. doi:10.1007/s40675-025-00329-9
42. Lanza G, Fisicaro F, Cantone M, et al. Repetitive transcranial magnetic stimulation in primary sleep disorders. Sleep Med Rev. 2023;67:101735. doi:10.1016/j.smrv.2022.101735
43. Jiang CG, Zhang T, Yue FG, Yi ML, Gao D. Efficacy of repetitive transcranial magnetic stimulation in the treatment of patients with chronic primary insomnia. Cell Biochem Biophys. 2013;67(1):169–173. doi:10.1007/s12013-013-9529-4
44. Shi X, Guo Y, Zhu L, et al. Electroencephalographic connectivity predicts clinical response to repetitive transcranial magnetic stimulation in patients with insomnia disorder. Sleep Med. 2021;88:171–179. doi:10.1016/j.sleep.2021.10.017
45. Li M, Zhu Y, Zhang X, et al. 1Hz rTMS over left DLPFC rewired the coordination with hippocampus in insomnia patients: a pilot study. Brain Stimul. 2022;15(2):437–440. doi:10.1016/j.brs.2022.02.011
46. Guo J, Chen X, Lyu Z, Xiu H, Lin S, Liu F. Repetitive transcranial magnetic stimulation (rTMS) for post-stroke sleep disorders: a systematic review of randomized controlled trials. Neurol Sci. 2022;43(12):6783–6794. doi:10.1007/s10072-022-06349-5
47. Wu H, Lv J, Liu M, et al. The long-term effect of repetitive transcranial magnetic stimulation in the treatment of intractable insomnia. Sleep Med. 2021;85:309–312. doi:10.1016/j.sleep.2021.07.018
48. Antczak JM, Poleszczyk A, Wichniak A, Rakowicz M, Parnowski TJ. The influence of the repetitive transcranial magnetic stimulation on sleep quality in depression. Psychiatr Pol. 2017;51(5):845–857. Wplyw przezczaszkowej stymulacji magnetycznej seria bodzcow na jakosc snu chorych na depresje. doi:10.12740/PP/68503
49. Tikka SK, Siddiqui MA, Garg S, Pattojoshi A, Gautam M. Clinical practice guidelines for the therapeutic use of repetitive transcranial magnetic stimulation in neuropsychiatric disorders. Indian J Psychiatry. 2023;65(2):270–288. doi:10.4103/indianjpsychiatry.indianjpsychiatry_492_22
50. Oroz R, Kung S, Croarkin PE, Cheung J. Transcranial magnetic stimulation therapeutic applications on sleep and insomnia: a review. Sleep Sci Pract. 2021;5(1):3. doi:10.1186/s41606-020-00057-9
51. Guo Y, Zhao X, Zhang X, et al. Effects on resting-state EEG phase-amplitude coupling in insomnia disorder patients following 1 Hz left dorsolateral prefrontal cortex rTMS. Hum Brain Mapp. 2023;44(8):3084–3093. doi:10.1002/hbm.26264
52. Xu X, Li L, Gao T, Zhang Q, Liu S, Liu X. Clinical study of different frequency transcranial magnetic stimulation combined with paroxetine in the treatment of poststroke depression with insomnia. Medicine. 2024;103(45):e40227. doi:10.1097/MD.0000000000040227
53. Zhao X, Liu J, Shao Z, et al. Restoration of abnormal sleep EEG power in patients with insomnia disorder after 1Hz rTMS over left DLPFC. Front Psychiatry. 2024;15:1431837. doi:10.3389/fpsyt.2024.1431837
54. Zheng H, Zhou Q, Yang J, et al. Altered functional connectivity of the default mode and frontal control networks in patients with insomnia. CNS Neurosci Ther. 2023;29(8):2318–2326. doi:10.1111/cns.14183
55. Zhu L, Dang G, Wu W, et al. Functional connectivity changes are correlated with sleep improvement in chronic insomnia patients after rTMS treatment. Front Neurosci. 2023;17:1135995. doi:10.3389/fnins.2023.1135995
56. Zhou Q, Liu Z, Yu C, et al. Effect of combined treatment with transcranial direct current stimulation and repetitive transcranial magnetic stimulation compared to monotherapy for the treatment of chronic insomnia: a randomised, double-blind, parallel-group, controlled trial. BMC Med. 2024;22(1):538. doi:10.1186/s12916-024-03751-y
57. Huang Z, Li Y, Bianchi MT, et al. Repetitive transcranial magnetic stimulation of the right parietal cortex for comorbid generalized anxiety disorder and insomnia: a randomized, double-blind, sham-controlled pilot study. Brain Stimul. 2018;11(5):1103–1109. doi:10.1016/j.brs.2018.05.016
58. Kweon J, Fukuda AM, Gobin AP, Haq L, Carpenter LL, Brown JC. Effect of sleep quality on repetitive transcranial magnetic stimulation outcomes in depression. Front Psychiatry. 2024;15:1458696. doi:10.3389/fpsyt.2024.1458696
59. Sun N, He Y, Wang Z, Zou W, Liu X. The effect of repetitive transcranial magnetic stimulation for insomnia: a systematic review and meta-analysis. Sleep Med. 2021;77:226–237. doi:10.1016/j.sleep.2020.05.020
60. Kar K, Duijnhouwer J, Krekelberg B. Transcranial alternating current stimulation attenuates neuronal adaptation. J Neurosci. 2017;37(9):2325–2335. doi:10.1523/JNEUROSCI.2266-16.2016
61. Huang WA, Stitt IM, Negahbani E, et al. Transcranial alternating current stimulation entrains alpha oscillations by preferential phase synchronization of fast-spiking cortical neurons to stimulation waveform. Nat Commun. 2021;12(1):3151. doi:10.1038/s41467-021-23021-2
62. Reato D, Rahman A, Bikson M, Parra LC. Low-intensity electrical stimulation affects network dynamics by modulating population rate and spike timing. J Neurosci. 2010;30(45):15067–15079. doi:10.1523/JNEUROSCI.2059-10.2010
63. Pariz A, Trotter D, Hutt A, Lefebvre J. Selective control of synaptic plasticity in heterogeneous networks through transcranial alternating current stimulation (tACS). PLoS Comput Biol. 2023;19(4):e1010736. doi:10.1371/journal.pcbi.1010736
64. Garside P, Arizpe J, Lau CI, Goh C, Walsh V. Cross-hemispheric alternating current stimulation during a nap disrupts slow wave activity and associated memory consolidation. Brain Stimul. 2015;8(3):520–527. doi:10.1016/j.brs.2014.12.010
65. Zhou Q, Qi G, Liu J, et al. Chronic insomnia: treatment with transcranial alternating current stimulation. Brain Stimul. 2021;14(4):848–850. doi:10.1016/j.brs.2021.05.007
66. Zhu X, Ren Y, Tan S, Ma X. Efficacy of transcranial alternating current stimulation in treating chronic insomnia and the impact of age on its effectiveness: a multisite randomized, double-blind, parallel-group, placebo-controlled study. J Psychiatr Res. 2024;170:253–261. doi:10.1016/j.jpsychires.2023.12.037
67. Motamedi GK, Jeliazkov PG, Oyegbile-Chidi TO, et al. Transcranial alternating current stimulation (tACS) as a treatment for insomnia. Can J Neurol Sci. 2023;50(3):446–449. doi:10.1017/cjn.2022.33
68. Lee M, Hong JK, Lee Y, Yoon IY. Transcranial alternating current stimulation in subjects with insomnia symptoms: a randomized, double-blind and controlled study. J Psychiatr Res. 2025;186:129–136. doi:10.1016/j.jpsychires.2025.04.020
69. Shao Z, Guo Y, Yue L, et al. Comparisons of transcranial alternating current stimulation and repetitive transcranial magnetic stimulation treatment therapy for insomnia: a pilot study. Gen Psychiatr. 2024;37(1):e101184. doi:10.1136/gpsych-2023-101184
70. Shi Y, Tian X, Li T, et al. The influence of transcranial alternating current stimulation on EEG spectral power during subsequent sleep: a randomized crossover study. Sleep Med. 2025;126:185–193. doi:10.1016/j.sleep.2024.12.011
71. Wang L, Chen Y, Piao Z, et al. Medial parietal alpha-frequency transcranial alternating current stimulation for chronic insomnia: a randomized sham-controlled trial. Psychol Med. 2025;55:e102. doi:10.1017/S0033291725000625
72. Khan BW, Khattak MH, Khan S, et al. Efficacy of transcranial alternating current stimulation for insomnia: a GRADE-assessed systematic review and meta-analysis of randomized controlled trials. Sleep Sci Pract. 2025;9(1):39. doi:10.1186/s41606-025-00163-6
73. Frase L, Piosczyk H, Zittel S, et al. Modulation of total sleep time by transcranial direct current stimulation (tDCS). Neuropsychopharmacology. 2016;41(10):2577–2586. doi:10.1038/npp.2016.65
74. Frase L, Selhausen P, Krone L, et al. Differential effects of bifrontal tDCS on arousal and sleep duration in insomnia patients and healthy controls. Brain Stimul. 2019;12(3):674–683. doi:10.1016/j.brs.2019.01.001
75. Li J, Li A, Jiao J, et al. Effects of high-definition transcranial direct current stimulation for the treatment of chronic insomnia: a randomized, double-blind, controlled trial. Sci Rep. 2025;15(1):26574. doi:10.1038/s41598-025-09304-4
76. van Boekholdt L, Kerstens S, Khatoun A, Asamoah B, Mc Laughlin M. tDCS peripheral nerve stimulation: a neglected mode of action? Mol Psychiatry. 2021;26(2):456–461. doi:10.1038/s41380-020-00962-6
77. Su YJ, Yi PL, Chang FC. Transcranial direct current stimulation (tDCS) ameliorates stress-induced sleep disruption via activating infralimbic-ventrolateral preoptic projections. Brain Sci. 2024;14(1). doi:10.3390/brainsci14010105
78. Donde C, Brunelin J, Micoulaud-Franchi JA, et al. The effects of transcranial electrical stimulation of the brain on sleep: a systematic review. Front Psychiatry. 2021;12:646569. doi:10.3389/fpsyt.2021.646569
79. Zhou Q, Liu Z, Zhao S, et al. Transcranial magnetic stimulation combined with transcranial direct current stimulation in patients with chronic insomnia: a case report. J Clin Sleep Med. 2022;18(12):2871–2874. doi:10.5664/jcsm.10272
80. Huang Y, Datta A, Bikson M, Parra LC. ROAST: an open-source, fully-automated, realistic volumetric-approach-based simulator for TES. Annu Int Conf IEEE Eng Med Biol Soc. 2018;2018:3072–3075. doi:10.1109/EMBC.2018.8513086
81. Provencher T, Charest J, Bastien CH. Non-invasive brain stimulation for insomnia - a review of current data and future implications. OBM Integrat Compl Med. 2020. doi:10.21926/obm.icm.2001001
82. Greinacher R, Buhot L, Moller L, Learmonth G. The time course of ineffective sham-blinding during low-intensity (1 mA) transcranial direct current stimulation. Eur J Neurosci. 2019;50(8):3380–3388. doi:10.1111/ejn.14497
83. Turner C, Jackson C, Learmonth G. Is the “end-of-study guess” a valid measure of sham blinding during transcranial direct current stimulation? Eur J Neurosci. 2021;53(5):1592–1604. doi:10.1111/ejn.15018
84. El Jamal C, Harrie A, Rahman-Filipiak A, et al. Tolerability and blinding of high-definition transcranial direct current stimulation among older adults at intensities of up to 4 mA per electrode. Brain Stimul. 2023;16(5):1328–1335. doi:10.1016/j.brs.2023.08.025
85. Wu Y, Song L, Wang X, et al. Transcutaneous vagus nerve stimulation could improve the effective rate on the quality of sleep in the treatment of primary insomnia: a randomized control trial. Brain Sci. 2022;12(10). doi:10.3390/brainsci12101296
86. Zhao R, Chang MY, Cheng C, et al. Transcutaneous auricular vagus stimulation (taVNS) improves human working memory performance under sleep deprivation stress. Behav Brain Res. 2023;439:114247. doi:10.1016/j.bbr.2022.114247
87. O’Keane V, Dinan TG, Scott L, Corcoran C. Changes in hypothalamic-pituitary-adrenal axis measures after vagus nerve stimulation therapy in chronic depression. Biol Psychiatry. 2005;58(12):963–968. doi:10.1016/j.biopsych.2005.04.049
88. Bretherton B, Atkinson L, Murray A, Clancy J, Deuchars S, Deuchars J. Effects of transcutaneous vagus nerve stimulation in individuals aged 55 years or above: potential benefits of daily stimulation. Aging. 2019;11(14):4836–4857. doi:10.18632/aging.102074
89. Yeom JW, Kim H, Park S, et al. Transcutaneous auricular vagus nerve stimulation (taVNS) improves sleep quality in chronic insomnia disorder: a double-blind, randomized, sham-controlled trial. Sleep Med. 2025;133:106579. doi:10.1016/j.sleep.2025.106579
90. de Oliveira HM, Gallo Ruelas M, Viana Diaz CA, Oliveira de Paula G, da Costa PR F, Pilitsis JG. Transcutaneous auricular vagus nerve stimulation in insomnia: a systematic review and meta-analysis. Neuromodulation. 2025. doi:10.1016/j.neurom.2025.04.001
91. Kinfe TM, Pintea B, Muhammad S, et al. Cervical non-invasive vagus nerve stimulation (nVNS) for preventive and acute treatment of episodic and chronic migraine and migraine-associated sleep disturbance: a prospective observational cohort study. J Headache Pain. 2015;16:101. doi:10.1186/s10194-015-0582-9
92. Zhang S, Zhao Y, Qin Z, et al. Transcutaneous auricular vagus nerve stimulation for chronic insomnia disorder: a randomized clinical trial. JAMA Network Open. 2024;7(12):e2451217. doi:10.1001/jamanetworkopen.2024.51217
93. Qi M, Huang Y, Mai R, et al. Baseline functional connectivity of the basal forebrain-cortical circuit predict taVNS treatment response in primary insomnia: a randomized controlled trial and fMRI study. BMC Med. 2025;23(1):412. doi:10.1186/s12916-025-04126-7
94. Rossi S, Antal A, Bestmann S, et al. Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: expert Guidelines. Clin Neurophysiol. 2021;132(1):269–306. doi:10.1016/j.clinph.2020.10.003
95. Lefaucheur JP, Aleman A, Baeken C, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): an update (2014-2018). Clin Neurophysiol. 2020;131(2):474–528. doi:10.1016/j.clinph.2019.11.002
96. Antal A, Alekseichuk I, Bikson M, et al. Low intensity transcranial electric stimulation: safety, ethical, legal regulatory and application guidelines. Clin Neurophysiol. 2017;128(9):1774–1809. doi:10.1016/j.clinph.2017.06.001
97. Antal A, Bjekic J, Ganho-Avila A, et al. Low intensity transcranial electric stimulation: safety, ethical, legal regulatory and application guidelines (2017-2025: an update) - endorsed by the European Society for Brain Stimulation (ESBS) and by the International Federation for Clinical Neurophysiology (IFCN). Clin Neurophysiol. 2026;184:2111436. doi:10.1016/j.clinph.2025.2111436
98. Brunoni AR, Amadera J, Berbel B, Volz MS, Rizzerio BG, Fregni F. A systematic review on reporting and assessment of adverse effects associated with transcranial direct current stimulation. Int J Neuropsychopharmacol. 2011;14(8):1133–1145. doi:10.1017/S1461145710001690
99. Matsumoto H, Ugawa Y. Adverse events of tDCS and tACS: a review. Clin Neurophysiol Pract. 2017;2:19–25. doi:10.1016/j.cnp.2016.12.003
100. Bikson M, Grossman P, Thomas C, et al. Safety of transcranial direct current stimulation: evidence based update 2016. Brain Stimul. 2016;9(5):641–661. doi:10.1016/j.brs.2016.06.004
101. Latreche C, Mancini V, McGinn N, et al. Safety and feasibility of home-based transcranial alternating current stimulation in youths with 22q11.2 deletion syndrome. Front Neurosci. 2024;18:1453839. doi:10.3389/fnins.2024.1453839
102. Bjekic J, Zivanovic M, Stankovic M, Paunovic D, Konstantinovic U, Filipovic SR. The subjective experience of transcranial electrical stimulation: a within-subject comparison of tolerability and side effects between tDCS, tACS, and otDCS. Front Hum Neurosci. 2024;18:1468538. doi:10.3389/fnhum.2024.1468538
103. Kim AY, Marduy A, de Melo PS, et al. Safety of transcutaneous auricular vagus nerve stimulation (taVNS): a systematic review and meta-analysis. Sci Rep. 2022;12(1):22055. doi:10.1038/s41598-022-25864-1
104. Giraudier M, Ventura-Bort C, Szeska C, Weymar M. A pooled analysis of the side effects of non-invasive transcutaneous auricular vagus nerve stimulation (taVNS). Front Hum Neurosci. 2025;19:1539416. doi:10.3389/fnhum.2025.1539416
105. Soleimani G, Nitsche MA, Bergmann TO, et al. Closing the loop between brain and electrical stimulation: towards precision neuromodulation treatments. Transl Psychiatry. 2023;13(1):279. doi:10.1038/s41398-023-02565-5
106. Ferini-Strambi L, Auer R, Bjorvatn B, et al. Insomnia disorder: clinical and research challenges for the 21st century. Eur J Neurol. 2021;28(7):2156–2167. doi:10.1111/ene.14784
107. Yu L, Gong L, Chen X, et al. Exploratory GABAa-informed control network modulates hyperarousal brain dynamics in chronic insomnia. Commun Biol. 2025;8(1):991. doi:10.1038/s42003-025-08439-4
108. Cao H, Shang L, Hu D, et al. Neuromodulation techniques for modulating cognitive function: enhancing stimulation precision and intervention effects. Neural Regen Res. 2026;21(2):491–501. doi:10.4103/NRR.NRR-D-24-00836
109. Cash RFH, Weigand A, Zalesky A, et al. Using brain imaging to improve spatial targeting of transcranial magnetic stimulation for depression. Biol Psychiatry. 2021;90(10):689–700. doi:10.1016/j.biopsych.2020.05.033
110. Ayanampudi V, Kumar V, Krishnan A, et al. Personalized transcranial alternating current stimulation improves sleep quality: initial findings. Front Hum Neurosci. 2022;16:1066453. doi:10.3389/fnhum.2022.1066453
111. Cash RFH, Cocchi L, Lv J, Wu Y, Fitzgerald PB, Zalesky A. Personalized connectivity-guided DLPFC-TMS for depression: advancing computational feasibility, precision and reproducibility. Hum Brain Mapp. 2021;42(13):4155–4172. doi:10.1002/hbm.25330
112. Choi DS, Lee S. Optimizing electrode placement for transcranial direct current stimulation in nonsuperficial cortical regions: a computational modeling study. Biomed Eng Lett. 2024;14(2):255–265. doi:10.1007/s13534-023-00335-2
113. Reimann GM, Kuppers V, Camilleri JA, et al. Convergent abnormality in the subgenual anterior cingulate cortex in insomnia disorder: a revisited neuroimaging meta-analysis of 39 studies. Sleep Med Rev. 2023;71:101821. doi:10.1016/j.smrv.2023.101821
114. Dworetsky A, Seitzman BA, Adeyemo B, et al. Probabilistic mapping of human functional brain networks identifies regions of high group consensus. Neuroimage. 2021;237:118164. doi:10.1016/j.neuroimage.2021.118164
115. Cao Z, Xiao X, Xie C, Wei L, Yang Y, Zhu C. Personalized connectivity-based network targeting model of transcranial magnetic stimulation for treatment of psychiatric disorders: computational feasibility and reproducibility. Front Psychiatry. 2024;15:1341908. doi:10.3389/fpsyt.2024.1341908
116. Cash RFH, Zalesky A. Personalized and circuit-based transcranial magnetic stimulation: evidence, controversies, and opportunities. Biol Psychiatry. 2024;95(6):510–522. doi:10.1016/j.biopsych.2023.11.013
117. Aquino G, Benz F, Dressle RJ, et al. Towards the neurobiology of insomnia: a systematic review of neuroimaging studies. Sleep Med Rev. 2024;73:101878. doi:10.1016/j.smrv.2023.101878
118. Qi S, Zhang Y, Li X, et al. Improved functional organization in patients with primary insomnia after individually-targeted transcranial magnetic stimulation. Front Neurosci. 2022;16:859440. doi:10.3389/fnins.2022.859440
119. Gong L, Yang X, He Y, et al. Precision targeting of right dorsolateral prefrontal cortex with neuronavigated rTMS alleviates chronic insomnia via functional connectivity reorganization: a randomized neuroimaging trial. Neuroimage Clin. 2025;47:103815. doi:10.1016/j.nicl.2025.103815
120. Kweon W, Lee KH, Choi SH, et al. Amygdala resting-state functional connectivity alterations in patients with chronic insomnia disorder: correlation with electroencephalography beta power during sleep. Sleep. 2023;46(10). doi:10.1093/sleep/zsad205
121. Huang J, Ye J, Gao M, et al. Lateralized differences in power spectra across different frequency bands during NREM sleep in patients with primary insomnia. Front Neurosci. 2025;19:1532011. doi:10.3389/fnins.2025.1532011
122. Takahashi K, Glinski B, Salehinejad MA, et al. Induction and stabilization of delta frequency brain oscillations by phase-synchronized rTMS and tACS. Brain Stimul. 2024;17(5):1086–1097. doi:10.1016/j.brs.2024.09.003
123. Zhu L, Pei Z, Dang G, et al. Predicting response to repetitive transcranial magnetic stimulation in patients with chronic insomnia disorder using electroencephalography: a pilot study. Brain Res Bull. 2024;206:110851. doi:10.1016/j.brainresbull.2023.110851
124. Wang L, Yu Y, Ying S, et al. A personalized closed-loop brain stimulation protocol for difficulty falling asleep. IEEE Trans Neural Syst Rehabil Eng. 2025;33:2368–2380. doi:10.1109/TNSRE.2025.3572851
125. Choi J, Kwon M, Jun SC. A Systematic Review of Closed-Loop Feedback Techniques in Sleep Studies-Related Issues and Future Directions. Sensors. 2020;20(10). doi:10.3390/s20102770
126. Dudysova D, Janku K, Piorecky M, et al. Closed-loop auditory stimulation of slow-wave sleep in chronic insomnia: a pilot study. J Sleep Res. 2024;33(6):e14179. doi:10.1111/jsr.14179
127. Ketz N, Jones AP, Bryant NB, Clark VP, Pilly PK. Closed-loop slow-wave tACS improves sleep-dependent long-term memory generalization by modulating endogenous oscillations. J Neurosci. 2018;38(33):7314–7326. doi:10.1523/JNEUROSCI.0273-18.2018
128. Zhao W, Jiang B. Heart rate variability in patients with insomnia disorder: a systematic review and meta-analysis. Sleep Breath. 2023;27(4):1309–1313. doi:10.1007/s11325-022-02720-0
129. Bressler S, Neely R, Yost RM, Wang D, Read HL. A wearable EEG system for closed-loop neuromodulation of sleep-related oscillations. J Neural Eng. 2023;20(5). doi:10.1088/1741-2552/acfb3b
130. Samea F, Mortazavi N, Reimann GM, et al. Insomnia and emotion dysregulation: a meta-analytical perspective integrating regulatory strategies and dispositional difficulties. Sleep Med Rev. 2025;82:102111. doi:10.1016/j.smrv.2025.102111
131. Ma Y, Mullington JM, Wayne PM, Yeh GY. Heart rate variability during sleep onset in patients with insomnia with or without comorbid sleep apnea. Sleep Med. 2024;122:92–98. doi:10.1016/j.sleep.2024.07.034
132. Riemann D, Espie CA, Altena E, et al. The European insomnia guideline: an update on the diagnosis and treatment of insomnia 2023. J Sleep Res. 2023;32(6):e14035. doi:10.1111/jsr.14035
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.