Back to Journals » Advances in Medical Education and Practice » Volume 17
From Stakeholder Expectations to Curriculum Gaps in EMS Education: Implications for Learning-to-Practice Alignment
Authors Tippayanate N, Chaiprom K, Chatuphonprasert W, Khamya A, Sriprow J, Sripol C, Thronsao M
Received 23 January 2026
Accepted for publication 27 April 2026
Published 1 May 2026 Volume 2026:17 593070
DOI https://doi.org/10.2147/AMEP.S593070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Nantawan Tippayanate,1,2 Kiattisak Chaiprom,1 Waranya Chatuphonprasert,3 Ajchara Khamya,1 Jantana Sriprow,1 Chattarin Sripol,1,2 Maitree Thronsao1,2
1Field of Study in Paramedicine, Faculty of Medicine, Mahasarakham University, Maha Sarakham, Thailand; 2International and National Collaborative Network and Innovation for Community Health Development Research Unit (INCHDI), Mahasarakham University, Maha Sarakham, Thailand; 3Field of Study in Medicine, Faculty of Medicine, Mahasarakham University, Maha Sarakham, Thailand
Correspondence: Nantawan Tippayanate, Field of Study in Paramedicine, Faculty of Medicine, Mahasarakham University, Maha Sarakham, Thailand, Tel +66 90 256 2994, Email [email protected]
Background: Preparing emergency medical services (EMS) graduates for real-world practice remains a challenge, particularly in low- and middle-income country settings. Although stakeholder engagement is increasingly used to define desired graduate attributes, how these expectations are translated into curriculum implementation is often unclear.
Methods: This study employed a secondary qualitative content analysis of stakeholder-derived graduate attributes for bachelor-level EMS programs. Identified attributes were mapped against existing curriculum structures, including course learning outcomes and assessment practices, using national qualification and quality assurance frameworks to examine alignment and gaps. A secondary qualitative content analysis was conducted using data from 24 stakeholders, including EMS employers, alumni, and professional representatives.
Results: Stakeholders emphasized attributes related to clinical decision-making under pressure, communication, teamwork, ethical judgment, adaptability, leadership, and handover skills. While several attributes were formally acknowledged in curriculum documents, many were only partially addressed or remained implicit and insufficiently assessed. Non-technical and context-dependent competencies were particularly underrepresented in practice-oriented learning.
Discussion: The persistence of these gaps reflects structural prioritization of easily documented competencies, misalignment between accreditation frameworks and field realities, limited experiential learning opportunities, and assessment practices that undervalue non-technical attributes.
Conclusion: Addressing learning-to-practice misalignment in EMS education requires moving beyond competency documentation toward intentional, practice-oriented curriculum design and assessment. Stakeholder-informed approaches may support educators in strengthening graduate preparedness for real-world EMS practice.
Keywords: emergency medical services education, curriculum mapping, stakeholder engagement, graduate attributes, learning-to-practice alignment, qualitative analysis
Introduction
Ensuring that emergency medical services (EMS) graduates are adequately prepared for real-world practice remains a persistent challenge across many health professions education systems.1,2 EMS professionals are expected to function effectively in time-critical, high-risk, and unpredictable environments, requiring not only technical competence but also sound clinical judgment, communication, teamwork, adaptability, and ethical decision-making. However, concerns regarding gaps between educational preparation and practice readiness have been widely reported, particularly during the early stages of professional practice.
In low- and middle-income country (LMIC) contexts, these challenges may be further amplified by workforce shortages, variability in training quality, and limited opportunities for structured transition from education to practice.2–5 As a result, newly graduated EMS personnel may enter the workforce with strong theoretical knowledge but insufficient preparedness for the complexity of prehospital care environments. Addressing learning-to-practice misalignment has therefore become a key priority in health professions education, including EMS education. In this study, learning-to-practice alignment refers to the extent to which curriculum design, learning experiences, and assessment practices support the development of competencies required for real-world professional practice.
International literature has emphasized that EMS education plays a critical role in shaping system performance and workforce readiness, particularly through alignment between educational priorities and evolving service demands.6
Stakeholder engagement has increasingly been promoted as a strategy to improve curriculum relevance and workforce alignment.1,2,7 Employers, alumni, and professional bodies provide critical insights into the competencies and attributes required for effective practice, particularly those that may not be fully captured through academic or regulatory perspectives alone. Prior studies have shown that stakeholder-informed approaches can help identify expectations related to non-technical competencies, such as communication, teamwork, professionalism, and leadership, which are essential for safe and effective emergency care.
Despite growing recognition of the value of stakeholder input, less attention has been paid to how stakeholder-identified graduate attributes are translated into curriculum structures, learning activities, and assessment practices.7–9 In many programs, desired attributes may be formally acknowledged within curriculum documents or accreditation reports, yet remain insufficiently operationalized through experiential learning and explicit assessment. This disconnect raises important questions about the extent to which curricula support the development of competencies required for real-world EMS practice.
Quality assurance and qualification frameworks, such as national and regional accreditation systems, provide guidance for defining learning outcomes and ensuring educational accountability. However, these frameworks may also unintentionally encourage emphasis on competencies that are easily documented and assessed,9,10 potentially overlooking context-dependent attributes that are critical in practice. Understanding how stakeholder expectations align—or fail to align—with curriculum implementation is therefore essential for strengthening learning-to-practice alignment.
In Thailand, undergraduate EMS education is typically delivered through university-based paramedic or emergency medical care programs that integrate classroom instruction, simulation-based training, and supervised clinical placements in both hospital and prehospital settings. Graduates are expected to function within a nationally regulated EMS system, often practicing under standardized clinical protocols and medical oversight. EMS personnel commonly operate in team-based response units and are required to perform a range of roles, including patient assessment, initial management, communication, and handover. This educational and service context provides an important backdrop for examining the alignment between curriculum design and real-world practice expectations in EMS education.
Accordingly, this study examines the alignment between stakeholder-expected graduate attributes and curriculum implementation in undergraduate EMS education. Using a secondary qualitative analysis approach, stakeholder-derived attributes are mapped against existing curriculum structures and assessment practices. By identifying areas of alignment and persistent gaps, this analysis aims to provide practical insights for EMS educators and curriculum designers seeking to enhance practice-oriented education and better prepare graduates for real-world EMS practice.
Methods
Study Design
This study employed a secondary qualitative content analysis to examine the alignment between stakeholder-identified graduate attributes and the implemented EMS curriculum. The analysis was based on an existing dataset derived from prior stakeholder consultations. This study can be considered a supplementary secondary analysis, focusing on re-examining stakeholder-derived attributes to address a new research question related to curriculum alignment.
Data Source and Participants
The dataset consisted of responses from 24 stakeholders, including EMS employers (n=10), program alumni (n=10), and professional representatives (n=4), selected based on their direct involvement in EMS practice and familiarity with graduate competencies.
Data Analysis
A qualitative content analysis approach was used to systematically examine the alignment between stakeholder expectations and curriculum implementation. The analysis was conducted using data from 24 stakeholders. Two researchers independently reviewed and coded the stakeholder-derived attributes and mapped them against curriculum documents, including course learning outcomes, teaching strategies, and assessment methods.
For the present analysis, stakeholder-identified graduate attributes were treated as the primary qualitative data. An inductive content analysis approach was applied to identify patterns and categories within the data, following established qualitative analytic principles.11 Initial coding focused on clustering attributes with similar conceptual meaning. Codes were iteratively refined and grouped into higher-order categories through constant comparison.
Subsequently, emergent categories were systematically mapped against existing curriculum structures, including course learning outcomes and assessment descriptions, to examine areas of alignment and misalignment. National and regional education quality frameworks—the ASEAN University Network–Quality Assurance (AUN-QA) and the Thai Qualifications Framework for Higher Education (TQF-HED)—were used as analytic lenses to support transparency and coherence in curriculum mapping.10,12 These frameworks informed interpretation without constraining category development. Curriculum mapping focused on formally documented course learning outcomes, assessment descriptions, and program-level curriculum documents available at the time of analysis.
Discrepancies in coding were discussed and resolved through consensus to ensure analytic consistency. The analysis focused on identifying patterns of alignment and gaps between expected competencies and documented curriculum practices.
Alignment was categorized into four levels: strong alignment, partial alignment, minimal alignment, and not explicitly addressed, based on predefined criteria (see Alignment Criteria section).
Ethical Considerations
Ethical approval for the original data collection was obtained from the Human Research Ethics Committee, Faculty of Medicine, Mahasarakham University (Approval No. 302–183/2025).
The original study involved an online questionnaire with open-ended questions.
Electronic informed consent was obtained from all participants prior to participation, with consent provided via an online consent page before access to the questionnaire.
Participation was voluntary, and all responses were anonymized prior to secondary analysis.
The present manuscript reports a secondary analysis of anonymized stakeholder data, with no additional data collection.
This study was conducted in accordance with the Declaration of Helsinki.
Alignment Criteria
To enhance analytic transparency, alignment categories were defined a priori based on the degree to which stakeholder-derived attributes were reflected in curriculum documents. Strong alignment was defined as attributes explicitly stated in course learning outcomes and supported by corresponding teaching activities and assessment strategies. Partial alignment referred to attributes implicitly represented in course content or learning activities but not systematically assessed. Minimal alignment indicated attributes that were only indirectly reflected or inconsistently represented across courses. Not explicitly addressed referred to attributes that were absent from documented learning outcomes, teaching strategies, or assessment methods.
Analytic rigor and trustworthiness were supported through iterative review of coding categories and peer discussion among the research team to refine category boundaries and ensure internal consistency. An audit trail documenting analytic decisions and category development was maintained throughout the analysis. Reflexive consideration of researcher positioning and professional background in EMS education informed interpretation and helped mitigate over-interpretation beyond the data. Mapping decisions were reviewed by at least two members of the research team to enhance consistency and reduce individual interpretation bias.
Results
The alignment between stakeholder-expected graduate attributes and current curriculum coverage is summarized in Table 1. Clinical decision-making under pressure emerged as one of the most frequently emphasized attributes across stakeholder groups.
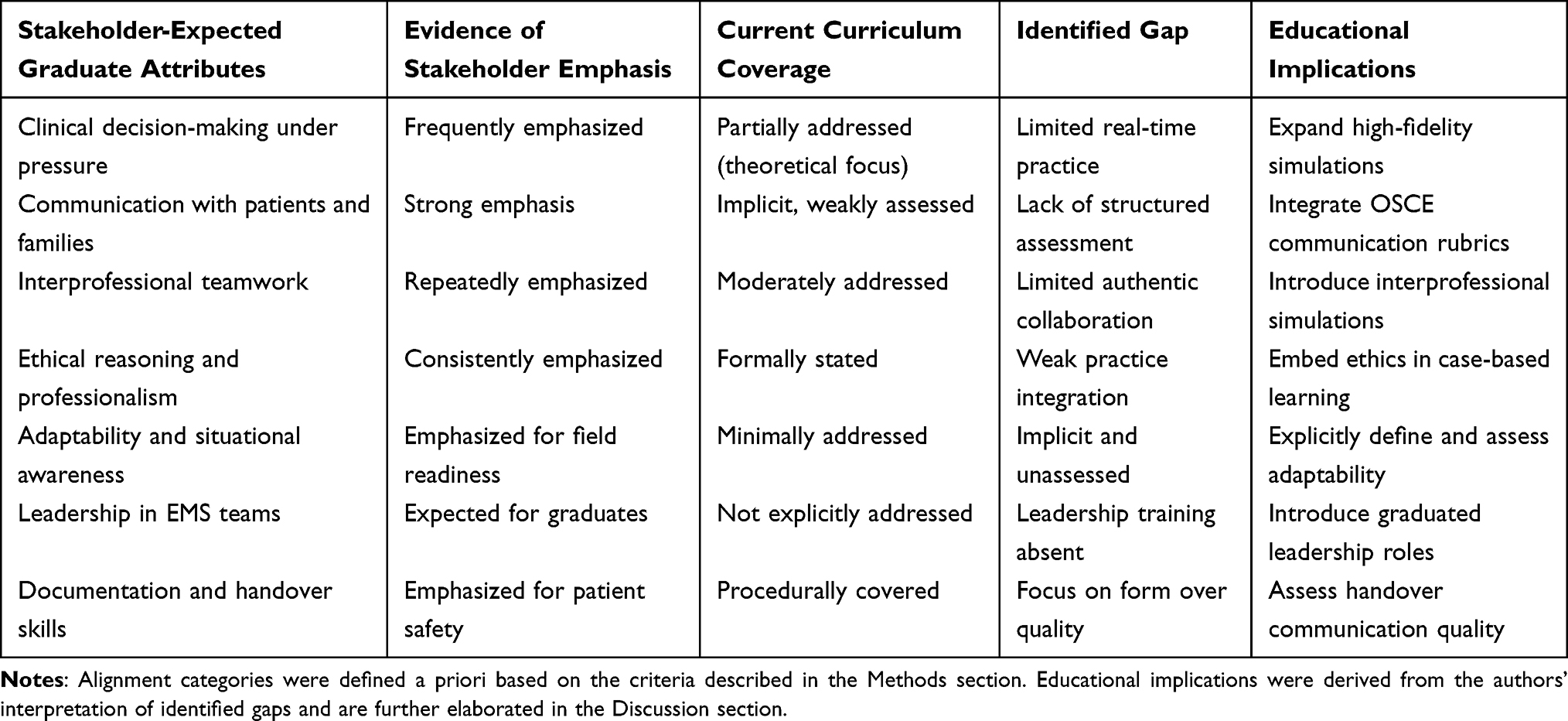 |
Table 1 Alignment Between Stakeholder-Expected Graduate Attributes and Curriculum Implementation in EMS Education |
A total of 24 stakeholders contributed to the dataset, representing perspectives from EMS employers, alumni, and professional bodies. Analysis resulted in three broad categories of alignment between stakeholder-expected graduate attributes and curriculum implementation. Overall, while several core professional attributes were formally acknowledged within curriculum documents, important gaps were identified in how these attributes were operationalized, assessed, and translated into practice-oriented learning experiences.
Attributes with Strong Stakeholder Emphasis but Partial Curriculum Coverage
Clinical decision-making under pressure emerged as one of the most frequently emphasized attributes across stakeholder groups, particularly employers and professional council representatives. Stakeholders highlighted the need for graduates to make rapid, context-sensitive decisions in unpredictable prehospital environments. One employer emphasized that “new graduates must be able to make rapid clinical decisions in unpredictable field situations, often with limited information”. Curriculum review indicated that clinical decision-making was primarily addressed at a theoretical level, with limited opportunities for learners to practice real-time decision-making under simulated stress conditions. This resulted in partial alignment, where conceptual understanding was present but experiential reinforcement was insufficient.
Similarly, effective communication with patients and families was consistently identified as a critical competency, especially during high-stress or emotionally charged situations. An alumnus noted that “communication with patients and their families during stressful situations is often more challenging in practice than what is learned in the classroom”. While communication skills were implicitly referenced within several course learning outcomes, structured assessment of communication performance was limited. Communication competencies were rarely evaluated using standardized rubrics or observed assessments, suggesting a gap between stakeholder expectations and measurable learning outcomes.
Moderately Addressed Attributes with Limited Practice Integration
Interprofessional teamwork was widely emphasized by stakeholders as essential for safe and effective emergency care. A stakeholder highlighted that “effective teamwork in EMS requires real-time coordination and shared understanding, which cannot be fully developed through classroom learning alone”. Curriculum documents demonstrated moderate alignment, with teamwork concepts introduced through classroom-based instruction and group activities. However, opportunities for authentic interprofessional practice—such as joint simulations or collaborative training with other health professions—were limited. As a result, teamwork was addressed conceptually but not consistently reinforced through experiential learning.
Ethical reasoning and professionalism were formally embedded within curriculum learning outcomes and institutional statements. Stakeholders, however, emphasized the importance of applying ethical judgment in complex field scenarios rather than abstract ethical principles alone. Curriculum analysis revealed limited integration of ethical reasoning into case-based or simulation-based activities, indicating that ethics education remained largely theoretical and insufficiently contextualized within EMS practice.
Underrepresented Attributes and Implicit Expectations
Adaptability and situational awareness were repeatedly described as essential for navigating dynamic and resource-constrained EMS environments. Another respondent stated that “EMS work requires constant adaptation to changing situations, and this flexibility is something that new graduates often struggle with”. These attributes were largely implicit within course descriptions and were not systematically assessed. Their absence from explicit learning outcomes and evaluation frameworks limited opportunities for intentional development and feedback.
Leadership within prehospital teams was another attribute strongly expected by stakeholders, particularly for graduates transitioning into senior or team leader roles. Curriculum review revealed little explicit emphasis on leadership development, with few structured opportunities for learners to assume graduated leadership responsibilities during training. This gap suggests a misalignment between workforce expectations and educational preparation for leadership roles in EMS settings.
Documentation and handover skills were recognized by stakeholders as fundamental to patient safety and continuity of care. While procedural aspects of documentation were covered within the curriculum, emphasis tended to focus on completion of forms rather than the quality of information transfer. Structured assessment of handover communication quality was limited, indicating an opportunity for more comprehensive evaluation approaches.
Summary of Alignment Patterns
Taken together, the findings demonstrate a pattern in which stakeholder-expected graduate attributes are often acknowledged at the curricular level but insufficiently operationalized through practice-oriented learning and assessment. Attributes related to technical knowledge were generally better represented than those requiring contextual judgment, adaptability, leadership, and communication in real-world settings. The identified gaps highlight areas where curriculum design and assessment strategies may be strengthened to better support learning-to-practice alignment and EMS workforce readiness.
Discussion
Historically, EMS education has evolved with strong emphasis on technical and procedural competencies, sometimes at the expense of broader professional and contextual skills required in complex practice environments.13
This analysis demonstrates a persistent gap between stakeholder expectations and curriculum implementation in EMS education. Although many desired attributes are formally acknowledged, their translation into practice-oriented learning remains limited.
One explanation lies in the structural emphasis on competencies that are easily articulated and documented for accreditation purposes.2,9 Attributes requiring contextual judgment—such as adaptability, leadership, and decision-making under pressure—are more difficult to define and assess, leading to their underrepresentation.
Additionally, accreditation and qualification frameworks, while essential for standardization, may inadequately capture the dynamic realities of prehospital care.10,12 Stakeholders emphasized unpredictable field conditions, yet curricula often prioritize compliance over experiential learning.
Limited opportunities for experiential and interprofessional learning further contribute to these gaps.7,8 Resource constraints and logistical challenges restrict authentic practice exposure, resulting in conceptual rather than applied competence. Assessment practices also tend to undervalue non-technical attributes,1,8,14 reinforcing their marginal status within curricula.
Addressing these issues requires intentional alignment between stakeholder expectations, curriculum design, and assessment strategies, particularly for non-technical competencies critical to EMS workforce readiness.
Prior qualitative studies have similarly shown that leadership and team-based behaviours in EMS crews are frequently learned informally in practice rather than through structured educational approaches.15
These findings reinforce the need for more structured integration of non-technical competencies within formal curriculum design and assessment frameworks.
Practical Implications
The findings offer several practical implications for EMS educators and curriculum designers. First, stakeholder-derived graduate attributes can be used as a reflective tool to review existing course learning outcomes and assessment strategies, particularly for non-technical competencies that are often implicit or underassessed. Second, integrating scenario-based simulation, structured observation, and explicit assessment criteria for communication, adaptability, and leadership may help translate documented competencies into observable practice. Finally, curriculum review processes aligned with quality assurance frameworks should move beyond compliance-oriented mapping toward deliberate consideration of how learning experiences prepare graduates for real-world EMS environments. These approaches may support more meaningful learning-to-practice alignment in undergraduate EMS education.
Limitations
This analysis has several limitations. As a secondary qualitative analysis conducted within a single middle-income country context, the findings may not be directly transferable to all EMS education systems. Curriculum mapping was based on documented learning outcomes and assessment descriptions, which may not fully capture informal or enacted teaching practices. Additionally, stakeholder perspectives reflected the views of key groups involved in EMS education and practice, but may not represent all potential stakeholders. Despite these limitations, the analysis provides contextually grounded insights relevant to educators seeking to strengthen learning-to-practice alignment.
Conclusion
Persistent gaps between stakeholder expectations and curriculum implementation highlight the need to move beyond competency documentation toward practice-oriented educational design. Strengthening experiential learning and assessment of non-technical attributes is essential for improving learning-to-practice alignment and EMS workforce readiness in LMIC contexts. This is particularly important where EMS workforce readiness directly impacts system performance and patient outcomes.
Acknowledgement
This research was financially supported by Mahasarakham University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wynne K, Mwangi F, Onifade O, et al. Readiness for professional practice among health professions education graduates: a systematic review. Front Med. 2024;11:1472834. doi:10.3389/fmed.2024.1472834
2. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems. Lancet. 2010;376(9756):1923–7. doi:10.1016/S0140-6736(10)61854-5
3. World Health Organization. Strengthening Health Systems for Universal Health Coverage. Geneva: World Health Organization; 2022.
4. Quake C, Bibi S, Ahmed H, et al. The current status and challenges of prehospital trauma care in low- and middle-income countries: a systematic review. Injury. 2023;54(9):1918–1929.
5. Delaney PG, King MA, McDonald C, et al. Future directions for emergency medical services development in low- and middle-income countries. Surgery. 2024;176(2):245–252.
6. Maguire BJ, King B, Kist J, et al. Creating the emergency medical services system of the future: the role of the EMS education agenda. JEMS. 2024;18(2):105–118.
7. Jackson D, Wilton N. Developing career management competencies among undergraduates and the role of work-integrated learning. Teach Higher Educ. 2016;21(3):266–286. doi:10.1080/13562517.2015.1136281
8. Gage A, Tanaka K, Fishe JN, et al. Consensus standard for evidence integration into EMS education and high-stakes testing. Prehosp Emerg Care. 2023;27(1):1–9. doi:10.1080/10903127.2021.2000683
9. OECD. The Future of Education and Skills: Education 2030. Paris: OECD Publishing; 2019.
10. Office of the Higher Education Commission, Thailand. Thai Qualifications Framework for Higher Education (TQF:HEd). Bangkok: OHEC; 2019.
11. Lyng HB, Macrae C, Guise V, et al. Balancing adaptation and innovation for resilience in healthcare: a metasynthesis of narratives. BMC Health Serv Res. 2021;21:759. doi:10.1186/s12913-021-06592-0
12. ASEAN University Network. Guide to AUN-QA Assessment at Programme Level Version 4.0. Bangkok: AUN Secretariat; 2020.
13. Brooks SC, Deakin CD, Ahmed N. An historical examination of the development of emergency medical services education in the United States. Adv Med Educ Pract. 2016;7:515–522.
14. Armstrong J, Cusack J, Cairns C, et al. Developing core competencies for paramedics through consensus and evidence: a national approach. Prehosp Emerg Care. 2015;19(1):18–27.
15. Kaššaiová A, Sedlár M. Competencies and behaviours required for membership and leadership of emergency medical service crews: a qualitative study. Paramedicine. 2025;16(1):55–68.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.