Back to Journals » Journal of Healthcare Leadership » Volume 18
From Personal Readiness to Systems Change: Progressive Clinician Cross-Competency Development in the Robert Wood Johnson Foundation Clinical Scholars Program
Authors Caton L ![]() , Rohin W, Adatsi G, Berthiaume R, Corbie G, Fernandez CSP
, Rohin W, Adatsi G, Berthiaume R, Corbie G, Fernandez CSP ![]()
Received 13 December 2025
Accepted for publication 29 April 2026
Published 28 May 2026 Volume 2026:18 588708
DOI https://doi.org/10.2147/JHL.S588708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 7
Editor who approved publication: Dr Pavani Rangachari
Lauren Caton,1,2 Wendy Rohin,2 Georgina Adatsi,2 Rachel Berthiaume,3 Giselle Corbie,3,4 Claudia SP Fernandez2
1Department of Health Policy and Management, Rollins School of Public Health, Emory University, Atlanta, GA, USA; 2Department of Maternal and Child Health, Gillings School of Global Public Health, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; 3Department of Social Medicine, School of Medicine, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; 4Department of Medicine, School of Medicine, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA
Correspondence: Lauren Caton, Emory Rollins School of Public Health, 1518 Clifton Road, Atlanta, GA, USA, 30322, Email [email protected]
Purpose: Clinicians are essential to transforming community health; however, traditional medical training does not provide needed multilevel, sequential, and equity-based leadership skills. The Robert Wood Johnson Foundation (RWJF) Clinical Scholars (CS) program was designed to fill this gap through interdisciplinary and applied competency training alongside an intensive community-based project. However, how clinicians operationalize and implement these competencies temporally and in their own terms has yet to be documented.
Patients and Methods: We conducted a qualitative, retrospective deductive content analysis of 1561 self-described competency entries by 130 clinicians in the CS program from 2016 to 2023. Participants bi-monthly recorded their application of one of 23 leadership self-reported competencies within their community project using STAR (Situation, Task, Actions, and Results), an accepted, structured response format. We also coded cross-competency co-occurrence and project context across personal, interpersonal, organizational, and community/system-level domains to demonstrate individual-level change preceding broader systemic transformation.
Results: Hospital- and clinic-level initiatives made up the largest share of the projects (41.98%). “Communication” was the most coded competency (72.7%) and commonly co-occurred with collaboration, emotional intelligence, and self-awareness competencies. Competencies with the highest cross-domain co-occurrence—innovation, negotiation, social determinants of health, visioning, and advocacy—were distinct from the most prevalent competencies. Certain competencies appear in bundles alongside domain progression such as innovation emerging as a top co-occurring code only for organizational (8.69%) and systems-level (7.83%) domain entries.
Conclusion: The CS program provided clinicians with the opportunity to reflect on and apply equity-centered leadership competencies. The divergence in competencies that were most “prevalent” versus “co-occurring” indicates the complexity of equity-oriented projects that require different, yet integrated bundling of skills. Differences in the prevalence of competencies by domain indicate a need for progressively structured competency development, focusing on personal readiness as a precedent to organizational and community impact. Prioritizing equity-based leadership that acknowledges these bundles and sequenced development is required to address urgent, recalcitrant, and modern healthcare challenges.
Keywords: clinician leadership, community-based research, healthcare workforce, medical training, equity-centered leadership, clinical scholars
Introduction
Healthcare professionals are integral parts of the community health ecosystem and pivotal to enhancing community well-being. Yet, few are positioned with leadership skills required for meaningful community engagement. This gap in preparedness mirrors national disparities in indicators of community health; the US has high clinical spending disproportionate to its high unaddressed health and healthcare needs.1,2 In response to these disparities, many major organizations such as the National Academy of Medicine, Robert Wood Johnson Foundation (RWJF), the Institute for Healthcare Improvement, and The Commonwealth Fund have called for integration of health, social, and community care in clinical training to better address root causes.1,2 Leadership capacity-building efforts, such as those employed by the RWJF Clinical Scholars (CS) program, often intend to equip clinicians with requisite skills for clinic-community integration. However, few provide necessary structural support alongside training, center equity, and systematically track competency acquisition.3
Trends in the US healthcare system have shifted to address a high chronic disease burden (eg, diabetes, heart disease, and obesity) which demand more dynamic training. These inequitable trends are driven, in part, by social, economic, and systemic determinants that extend beyond the reach of the biologic, physiologic, and medical model training received by clinicians.4 Healthcare professionals therefore need more comprehensive, equity-based, and multi-level training to effectively address embedded inequities and re-envision these systems.5–7 However, leadership and equity trainings that target these systemic inequities are rarely provided in clinical training or other post-graduate settings.8–10
To move beyond clinical skills to systems change, healthcare professionals must have structured opportunities to apply leadership skills. While some clinical training integrates social determinants into the curriculum and trainees report eagerness to apply this to communities,10,11 this training is often limited to short sessions that center awareness over skills application.10–13 Additionally, many of these trainings are not rooted in adult pedagogical approaches that center reflection and direct skills application. Transformative learning theory and Kegan’s constructive-development theory on professional identity formation posit that critical reflection and internal, “self-authorizing” values development precedes external “meaning-making” through application.14–16
The RWJF Clinical Scholars (CS) program was designed to meet this need by providing capacity building paired with integrated, project-based, and multi-level skills development. The CS program uniquely focusing on multi-pronged, equity-focused competency development curriculum that spans the personal, interpersonal, organizational, and systems domains (Figure 1).3,13 This multilevel approach coaches leaders to internally embody and externally process equity-centered leadership rather than employing didactic instruction alone. Centering applications of skills was the justification for the program’s required Wicked Problem Impact Project (WPIP), a community-impact project that centered applied learning in-context. The 23 self-reported competencies (eg, conflict management, innovation, and organizational capacity for health equity) developed through these applications are guided by social cognitive theory, the socioecological model, and the social capital framework, which work together to emphasize individual behavior as shaped by interpersonal interactions, the environment, and society and informed the four domains (personal, interpersonal, organizational, and community-levels).7,17–19 Detailed descriptions of pedagogical theory, curricular details, and quantitative evaluations of the program can be found in other scholarship.3,20,21 This study focuses on how participants applied and integrated these competencies over time.
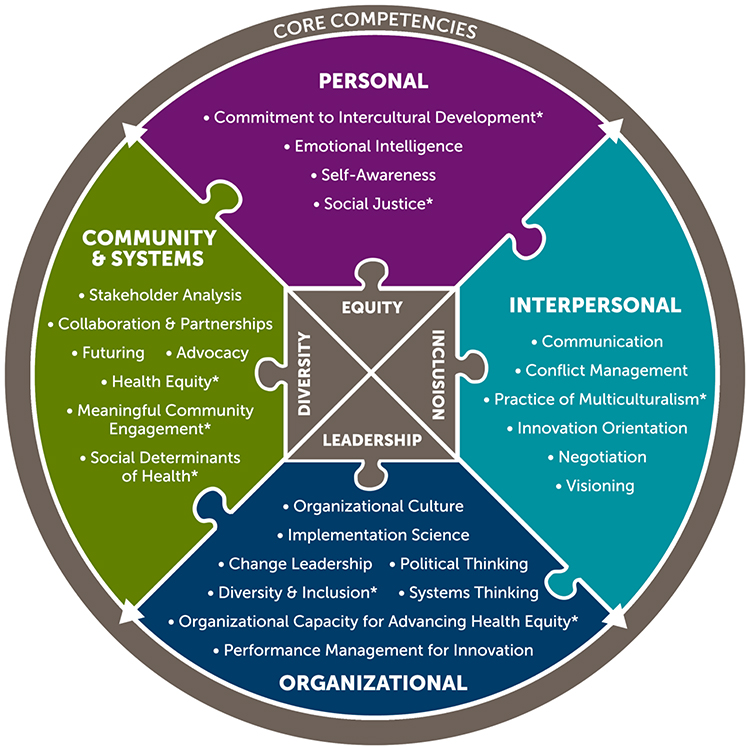 |
Figure 1 Core competencies of the Clinical Scholars program by domain. Note: “performance management for innovation” and “commitment to intercultural development” were later removed for redundancy with other competencies. They therefore do not appear in this analysis. *Competencies with explicit link to equity, diversity and inclusion. |
In summary, leadership capacity-building efforts are often assumed to bridge clinical and community spaces. However, the direct application of acquired competencies in project-based form is limited and often evaluated discretely and non-longitudinally.5,8,10 Therefore, our review of the RWJF CS program sought to document practitioner definitions of competencies, their co-occurrence, and application across multilevel domains in their community-based projects. Our inclusion of 7 years of participant reflection on the application of 23 competencies across four domains and evaluating co-occurrence of competencies as bundles enhances granularity beyond comparable evaluations. Documenting the translation of skills longitudinally and by domain provides a clear vision of how clinician training could be sequenced and evaluated to meet the complex needs of interdisciplinary community-based work.
Materials and Methods
Program Overview and Participants
In 2015, RWJF funded the University of North Carolina at Chapel Hill’s School of Medicine and Gillings School of Global Public Health to run and evaluate the CS program. The first cohort of Clinical Scholars (CS) was launched in 2016 to integrate health equity and leadership training for healthcare professionals. Between 2016 and 2023, 162 clinicians participated in five cohorts.22 Participants were mid- to late-phase healthcare professionals representing 15 different roles, including physicians, nurses and nurse practitioners, physician’s assistants, social workers, and allied health specialists such as occupational therapists, dieticians, and pharmacists.3 As described earlier, the program sought to build on the inherent leadership of health professionals through competency-based pedagogical instruction, paired with implementation of a team-based wicked problem impact project (WPIP), a community impact project. Participants’ organizations, but not the participants directly, received $35,000 per year to protect time for their project. Training was provided through a combination of seven in-person retreats, individual development plans, mentoring, leadership modules, technical assistance calls, webinars, and personal executive and team-based coaching experiences in pursuit of their community impact project, with no differences by cohort.21 The program sequence and components are described in greater depth in several articles and books.5,22 The 25 intended leadership competencies and their definitions, which guided this data collection, codebook development, and analysis are also provided in-depth in other publications (Figure 1).21 It should be noted that two of the original competencies, “commitment to intercultural development” and “performance management for innovation”, were removed in early 2017 and not part of the analysis.
Data Collection
Review of the self-reported competencies was recorded through participant submission of Online Wisdom Logs (OWLs) via Canvas Learning Management Systems, and responses were stored on a drive within a secure internal UNC server.5,23 For a minimum of six competencies, a year, self-selected by participants, activities, or general reflections were recorded in alignment with the CS competencies and in STAR format (Situation, Task, Actions, and Results).24 OWLs were required for participation but not for stipend disbursement, though participants signed a form indicating their commitment to trainings and ongoing evaluations (including OWLs) upon program acceptance. The participants submitted their OWLs to one CS competency per entry. They could submit under different competencies each time but could not log one entry under multiple competencies. For example, an individual could enter negotiating the terms of a new collaborative partnership under the interpersonal competency “negotiation” for 1 month’s entry and the implementation of that partnership under “implementation science” 2 months later. Over the course of seven years of the CS program, we collected 1561 entries across all 23 competency domains and 130 participants who completed the required assignments (n=130/162, 80%).
Analysis
The research team used a deductive, manifest (explicit) content analysis approach to document the extent and interrelationships of the self-reported competencies used by Clinical Scholars. This method is ideal for assessing the prevalence of pre-selected themes across short-answer responses and focuses on specifically stated, not latent, texts from the participants.25,26 Codes were pre-developed from extant definitions of CS competencies provided in other publications (Appendix 2).13,24 Due to the de-identified nature of the data, analysis is conducted at the log-entry level, reflecting distributions across entries, not within individuals or cohorts.
There were seven coders total, each person coding an average of 496 entries (each entry was coded twice). Coders included two PhD-level and five masters-level students with various levels of qualitative coding experience, compensated hourly by the primary research institution. No coders for this project were involved in the CS program implementation directly and were only hired after the program was terminated, in order to mitigate investigator bias. The coders were trained on five responses during the initial coding phase. These responses were then reviewed by the primary coordinator and discussed with the coder before continuing with the remaining allocation. All entries were assigned to two coders, who independently coded the entries based on the presence of competencies (themes) and met to reconcile the codes. The calculated percent agreement was 91.33%, meaning only 8.67% of entries required reconciliation. The codes were not mutually exclusive, and there were an average of 6.78 competencies coded per entry. Percent agreement was selected over other inter-rater reliability measures due to the abundance of possible codes (n=23) with uneven prevalence (approximately 73% of entries referenced communication), non-mutually exclusive co-occurring codes (average of 6.78 per entry), and negotiated resolution (eg, consensus). These conditions violate key prevalence and independence assumptions needed to calculate kappa statistics.27,28 Coders also documented the “level”, of the targeted intervention for each project entry; (eg clinical, hospital policy, state or federal policy, or community-level interventions). Coders could mark exemplary quotes if they felt there was a need for a new code or not represented by available codes. The full data collection instrument is shown in Appendix 1.
We looked at “prevalence” of codes, or how frequently they appeared across all competency entries. Additionally, we also looked at “density” of cross-competencies or how often different competencies co-occurred within each competency entry. We added a case study on Montana, specifically, to demonstrate how these competencies were directly tailored and applied to context.
Ethics
There were no prior relationships between the coders, program staff, and program participants. IRB approval was not required because the analysis was completed on de-identified secondary data and did not involve human subjects. However, research approval was obtained for the parent project by the institutional review board at the University of North Carolina at Chapel Hill (IRB # 16–1817). This publication does not cite entries by and removes all mentions of state or location identifiers in order to preserve anonymity (excluding Montana), although we recognize that it may diminish the contextual understanding of the importance of place-based work. Montana participants consented to their identification, even with possible re-identification, as a case study for this work and other published articles. Generative AI, specifically Claude Opus 4.5, was used for editing and clarity of the manuscript, but not for primary writing or analysis.
Results
Of the 1561 total entries, the majority, or 41.98% (n=655), of projects from the entries focused on hospital- or institutional-level interventions such as involvement in task forces, hospital training or curricula changes, or cross-departmental collaborations; followed by projects targeting individual- or clinician-level changes (39.03%, n=609). The remaining were either community-level interventions, such as community events, engagement initiatives, and multi-institution collaborations (29.03%, n=452), or local, state, or federal policy projects (8.97%, n=140). Entries could span multiple domains (eg, not sum to 100%).
Results presented distinguish (1) prevalence of coded self-reported competencies, and (2) “density” of cross-cut competencies that function as integrative drivers of participant work across domains and contexts. “Communication” was the most prevalent, eg. most often coded, competency employed by clinicians in pursuit of equity-based community projects, appearing in the vast majority of entries (72.72%, n=1135). This was followed by “collaboration and community partnerships” (46.89%, n=732), self-awareness (46.44%, n=725), emotional intelligence (37.35%, n=583), and “improving organizational capacity for health equity” (36.32%, n=567) (Figure 2). The full prevalence of competencies across the entries is shown in Table 1.
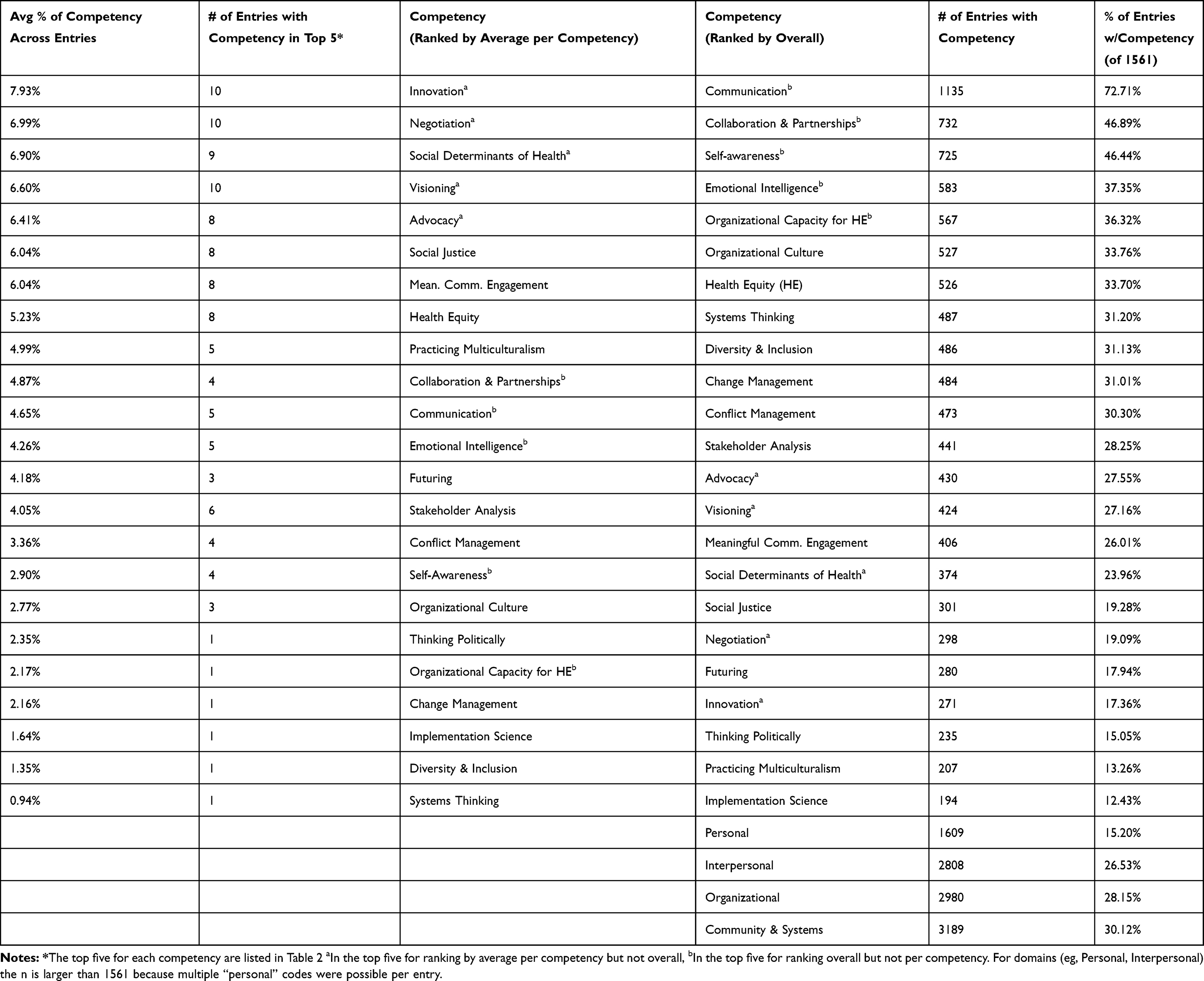 |
Table 1 Competencies Listed by Prevalence (Overall) and Density (by Average per Competency) |
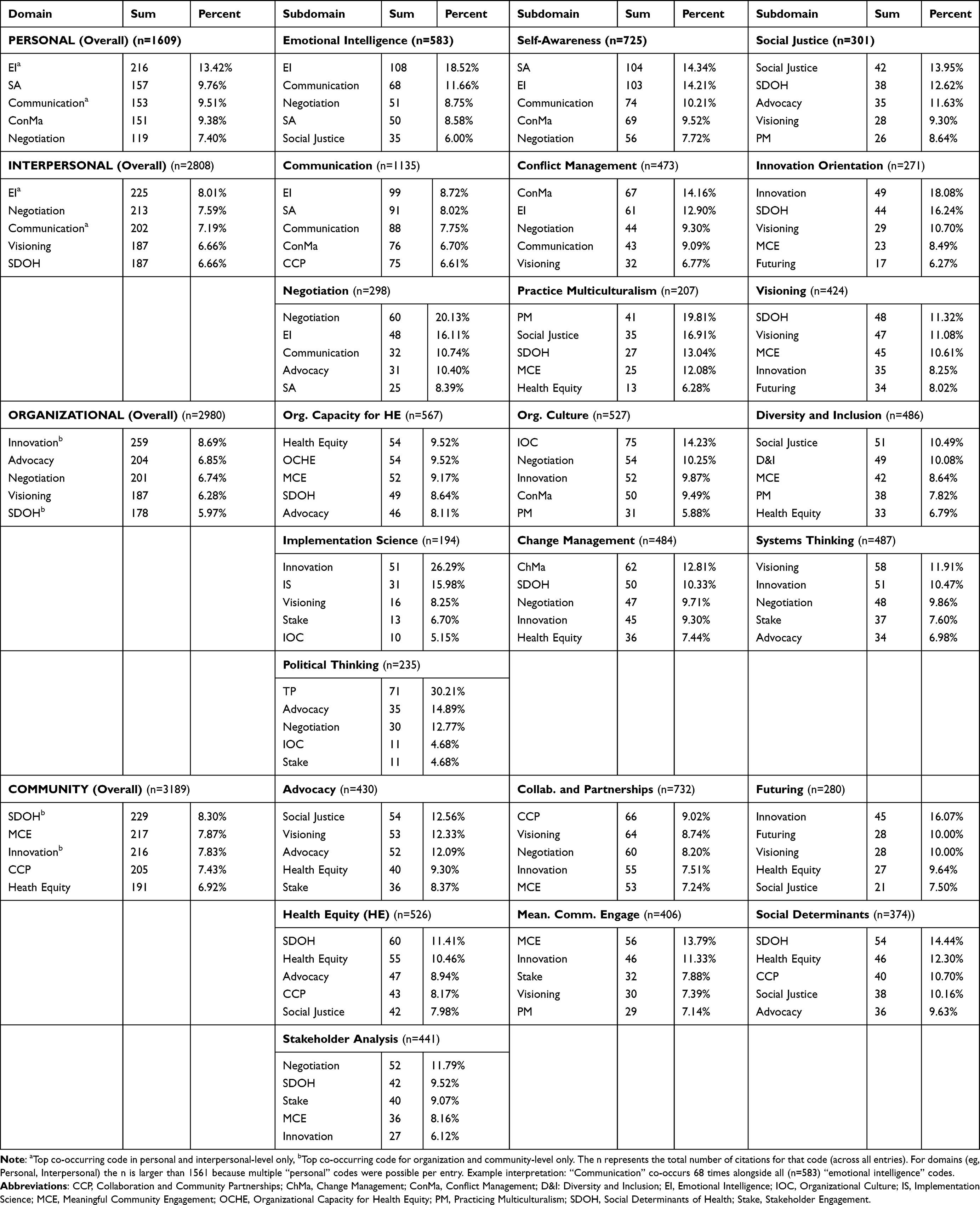 |
Table 2 Top 5 Co-Occurring Cross-Competencies (Density) by Domain and Competency |
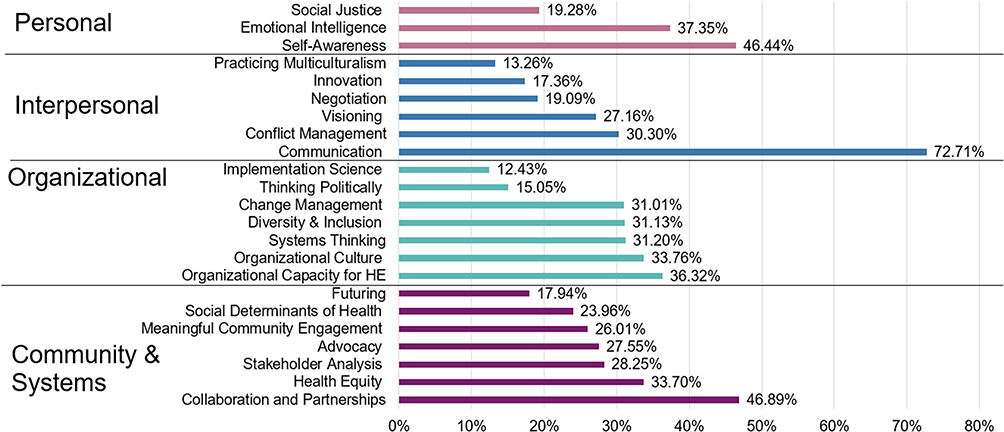 |
Figure 2 Prevalence of competencies by domain (n=1561). |
We also looked at the top co-occurring, cross-competencies that appeared within each set of competency entries (eg, “density”). For example, across all occurrences of a “communication” code (n=1135), emotional intelligence, self-awareness, conflict management, and “collaboration and community partnerships” were also coded 8.72% (n=99), 8.02% (n=91), 6.70% (n=76), and 6.61% (n=75) of the time, respectively (Table 2). Full cross-competencies for communication, as an example, are shown in Figure 3 and full co-occurring codes are listed in Table 2. Interestingly, different sets of co-occurrence were predominant in the other most prevalent competencies.
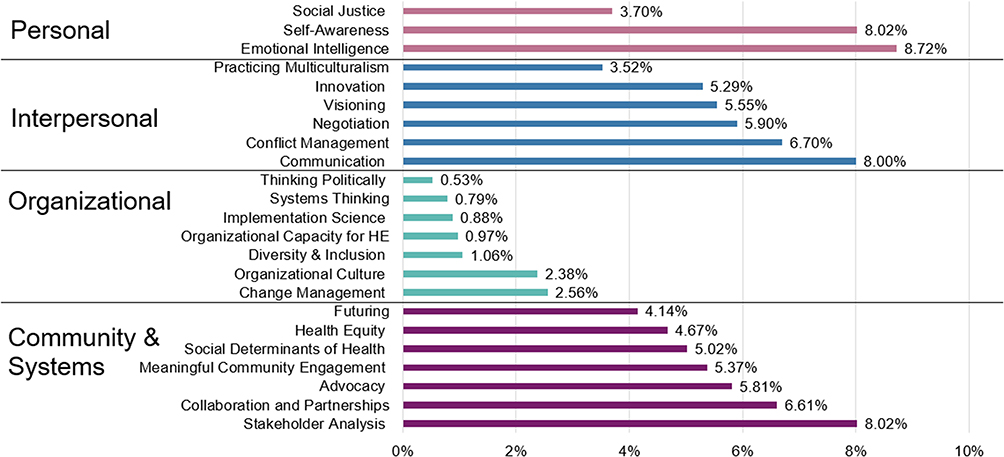 |
Figure 3 Frequency of cross-coded competencies across all “Communication” codes (n=1135). |
For example, collaboration and community partnerships codes (n=732) also employed visioning (8.74%, n=64), negotiation (8.20%, n=60), innovation (7.51%, n=55), and meaningful community-engagement (7.24%, n=53), whereas self-awareness entries co-described emotional intelligence (14.21%, n=103), communication (10.21%, n=74), conflict management (9.52%, n=69), and negotiation (7.72%, n=56) as essential to project application. In one “Communications” entry, a participant described using emotional intelligence and understanding of their specific role to communicate uncertainty and emerging conflicts from a recent hospital acquisition (conflict management). One social worker said they began with compassion stating, “it is a huge change for all of us, I continued with conviction… [and] ended with optimism that I would discuss the concerns with administration for clarification with[in] our ambulatory setting” (communication entry #50). Another collaboration and community partnership entry pivoted their innovative school-based mental health services program (innovation), given funding constraints, by negotiating with financial partners (negotiation). They reported having to “reassure the investors of the organization… while continuously cultivating the relationship with the school district through negotiation, compromise, and persistence” (collaboration and community partnerships entry #6).
In order to look at density of these codes, as compared to prevalence (eg, “communication” as most often coded, overall), we took the average of co-occurring competencies under each main competency entry, for an “average per competency.” The co-occurring competencies that had the highest average citation per competency–meaning they were highly cross-coded across more competencies–were innovation, negotiation, social determinants of health, visioning, and advocacy at 7.93%, 6.99%, 6.90%, 6.60%, and 6.41%, respectively (Table 1). Notably, these are different from the most prevalent competencies across all entries. Innovation had the highest average appearance per competency, as indicated by its presence in the top five averages for the 10 different competencies. This ranged from school-based “futuring” projects such as “initiat[ing] a Health Ambassador (HA) program that trained and brought high school students…to teach the children key topics promoting a culture of health” (futuring entry #56) to a state-wide “systems thinking” telepsychiatry program “provid[ing] behavioral health services to rural community hospitals… implemented as a pilot leveraging [State] Medicaid innovation dollars” (systems thinking entry #35).
The patterns of co-occurrence and density seem to suggest that certain competencies operate less as standalone skills and more as connective mechanisms that work in tandem to enable the translation of leadership skills into projects.
Self-reported competencies were also grouped by domain: Personal, Interpersonal, Organizational, and Community and Systems (Figure 2). These domains also had different prevalences of cross-competencies (Table 2). Examples included emotional intelligence (13.42%, n=216), self-awareness (9.76%, n=157), communication (9.51%, n=153), conflict management (9.38%, n=151), and negotiation (7.40%, n=119) highly listed under “Personal” domain entries. These seemed to overlap with certain top co-occurring competencies in the “Interpersonal” domain, the only other domains to have emotional intelligence (8.01%, n=225) and communication (7.19%, n=202) as top cross-codes. A similar trend was seen for the organizational, community, and system domains, both of which had innovation as a top cross-code at 8.69% (n=259) and 7.83% (n=216), respectively, whereas this competency did not appear in the top personal or interpersonal cross-codes.
There are several strong examples of co-occurrence of communication and emotional intelligence in personal and interpersonal domains. One healthcare provider from the South explained that their training enabled them to negotiate in an emotionally fraught situation where “despite my [hospital] administration’s resistance to applying more grants to support [partnership initiated with a local trauma and grief center]…I consistently messaged my needs to them and appealed to their visionary side,” in order to successfully continue integration of the program. Another provider from the West Coast successfully integrated emotional intelligence to reflect on the needs of their project, “I didn’t feel I represent the community most affected by this problem,” and ultimately successfully encouraged media to speak with “residents that experienced the problem first-hand…” for state-level testimony on pharmacy deserts.
Montana Pediatrics Case Study
Examining the work of Cohort 3 of the CS program (2018–2021) allows us to see how the theme of communication manifests in their chosen project. Their wicked problems involved deficits in pediatric healthcare budgets, specifically in urgent care, subspecialties, and rural health. Montana is currently ranked 38th in the United States, with only 59 board-certified pediatricians per 100,000 children, and 37 of the 56 (66%) counties do not have pediatricians. As such, providers were facing burnout exacerbated by a shrinking of the national primary care workforce.29 In 2022, Montana pediatrics launched an on-demand pediatric urgent care using a local, co-operative telemedicine model, accessible to roughly 260,000 children living in all counties across the state. The Montana CS team also initiated full-time school-based pediatric healthcare for a tribal health program. The program utilized the skills and knowledge acquired at the CS and strong partnerships with clinicians, donors, and community organizations at its founding.
The entries from Montana’s team participating in the third cohort of the CS program, comprising three pediatricians, show how different sets of competencies are manifested in a given project. An OWLs entry from Montana Pediatrics Team Member 1 addressed the challenges related to implementing new documentation for well child visits, which was vital to the program’s goal of interconnecting all participating clinic patients. However, in an era of a declining healthcare workforce and increased demands for efficiency, additional documentation is not well received by overwhelmed clinic staff and administrators. Team member 2 chose the competency, “communication”, to discuss how they had listening sessions with front desk staff at every clinic to successfully foster cooperation through validation. “The results showed nearly universal improvement in the way we documented the visits and, equally important, a wave of positive feedback that this did not feel like yet another disconnected mandate from administration.”
In another entry under the communication competency, Montana Pediatrics Team Member 2 discussed the necessary collaboration between herself and a technology innovator who was working on their web-based communication and electronic medical record (EMR) platform. Sensing that the individual needed more information on tribal decision-making hierarchies and differences between communities in Montana for the web-based system to be culturally relevant, Team member 2 had the requisite discussions. This entry highlights the importance of other CS competencies, such as multiculturalism, diversity and inclusion, health equity, advocacy, and social determinants of health. “As a result, we were able to learn and respect the cultures of tribal populations in our state and work mindfully to engage diverse tribal leadership in our project as consumers, resulting in a more culturally competent healthcare delivery model.”3
Among the Montana Pediatrics team members’ entries (n=40, 282 codes applied), “communication” was also the most frequently occurring competency (9.57%, n=27). Interestingly, the next most frequent competencies were “collaboration and partnerships” (7.45%, n=21), “organizational culture” (6.03%, n=17), “self-awareness” (5.67%, n=16), and “meaningful community engagement” (5.32%, n=15), mirroring the top five highest frequency competencies (excluding organizational culture and meaningful community engagement) (Figure 4). This demonstrates that acquired skills of cultural competency, community engagement, and collaboration are needed to successfully incorporate 142 more providers with the technological support needed to serve such a widespread population of hundreds of thousands of children. As described by Team Members 2 and 3, the CS program equipped these physicians with applied skills otherwise lacking in clinical contexts, “creating a system by which our… team [could] grow a collaborative clinical community” to expand after-hours and virtual teamwork. These connections fostered through enhanced communication and equity skills of the CS program were “… the most integral and necessary partnerships we had to build” to “truly solidify Montana Pediatrics into the web of care” options.3
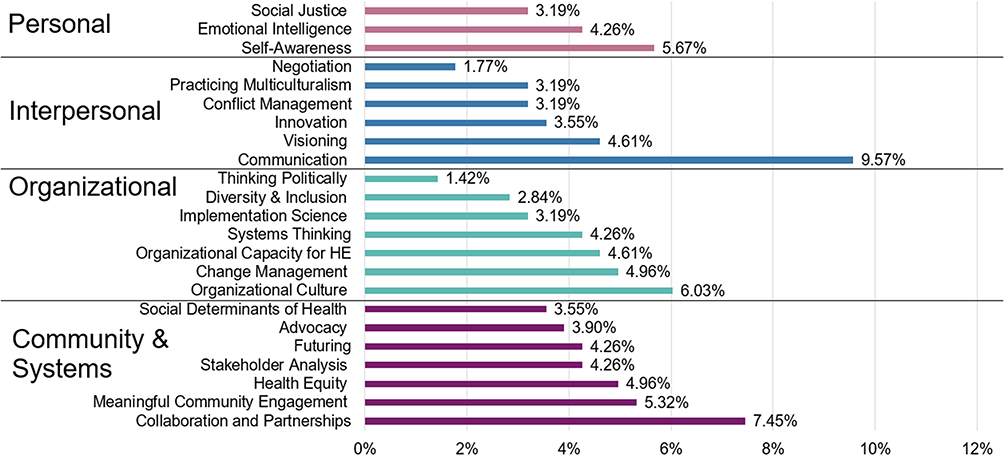 |
Figure 4 Montana prevalence of competencies by domain (n=282). Note: Competency order aligns with Figure 2 on overall prevalence, for ready comparison. |
Discussion
Our review of the CS program sought to document how clinicians operationalize and implement equity-based competencies as a result of targeted capacity building efforts, often assumed to bridge clinician-to-advocate gaps. Our study is further innovative in that it tracks entries over multiple time points and sorts them into dimensional constructs. Therefore, the narratives were able to highlight the process of various initiatives; not just the “what”, but the “how”, rarely documented temporally and in full.
Findings
Communication was the most prevalent competency, found in 72.7% of the 1561 entries, and was highly cross-coded with several competencies spanning the personal, interpersonal, and community and systems domains (emotional intelligence, self-awareness, negotiation, collaboration, and community partnerships). The high prevalence of “communication” across all entries seems to indicate its status as a competency that underpins successful implementation of other competencies. It also highly co-occurred in personal and interpersonal domain entries (Table 2). This reveals the importance of mastering interiority as a foundation for successful communication in interpersonal and community settings and its mechanistic role in translating projects at these levels. The prevalence of reported competencies (communication, partnerships, emotional intelligence, and self-awareness) reflects relational groundwork but does not capture the requisite integrative skills required to enact change across settings.
The density of co-occurring codes (eg, differing percentages of codes occurring within selected competency entries) seems to indicate different bundling of competencies needed for different project foci. For example, innovation, negotiation, social determinants of health, and visioning had the highest average co-occurring competencies per competency entry (Table 1). Each has a connotation of changing the status quo. The domain-level variation in and differences between sets of prevalence and density of competencies indicates adaptability to the context employed by clinicians for each project description. Capacity-building efforts would benefit by targeting the integrative, multi-dimensional, and discrete mastery of subjects not covered in clinical training. Furthermore, domain-level variation (personal, interpersonal, organizational, community, and systems) in the prevalence of competencies (Table 2) may indicate a progression of the skills needed to scale systems leadership. Indeed, the pedagogy of the CS leadership and health equity curriculum was designed to develop a progression of skills, from more basic to adaptive, through sophisticated leadership skill sets.3 Capacity-building efforts should target the natural progression of competency development needed for each stage. By acknowledging communication and innovation as integral parts of equity-based leadership competency at each level, change efforts may become more successful.
Predictably, most initiatives (41.98%, n=655) occurred at the hospital or clinical levels. This suggests that clinicians are still innovating community projects through a clinical origin, rather than initiating projects from the community. However, this was a core tenet of the CS program, and indeed, community-based research paradigms center communities as partners rather than “to be learned from”, “trained on”, or “taught”.30 The program believed it was important for clinicians to develop their internal and organizations’ skills prior to engaging in radical community work. Thus, interactions were at maximal capacity and in a way that honored community expertise.3,31 Further, only ~50% of CS program participants were MDs, an intentional decision by the RWJF.32 The prevalence of clinical-level projects, alongside narrative descriptions, suggests that the developed competencies may enable non-MD clinicians to leverage power and expand sphere of influence in settings where hierarchical structures have otherwise been a barrier to collaboration and integration.33–35 Interdisciplinary care in clinical contexts where team members feel respected and empowered is known to increase quality of patient care, reduce length of stay, and reduce burnout.36–38 Other community-engagement programs seeking to improve engagement in ways that do not exacerbate community distrust in medical institutions should ground competency development in these community-based, non-hierarchical, and co-developed community-based participatory theories and approaches.31 Conversely, the low percentage of local- and state-level policy projects (<10%) may indicate that additional curricula are needed to equip clinicians with skills for advocacy and change at these levels. It may also simply reflect clinicians focusing on “small p” institutional policy arenas they were most familiar with or felt were within their sphere of influence. However, policy curricula efforts should not create redundancy or amplify the efforts of policy institutes emerging across the country, although these mostly center on advocacy, political framing, and communication rather than overt leadership.39–42
Alignment
The results reveal the importance of communication and innovation as bridging factors in implementing projects to achieve health equity in community-academic partnerships and provide a roadmap for multidimensional targets of capacity building.43 Clinicians at academic medical centers have long indicated interest in community partnerships, but report not having training or protected time to do so.44 Further, true sustainable community change involves complex and slow change over time.45 The CS program uniquely provides the infrastructure paired with protected time and funding to make sustainable change. The cross-dimensionality and bundling of the competencies seems to indicate that providing these elements might meet the complexity needed to implement long-term, sustainable projects.11,44,46
The differences between top competencies at the personal or interpersonal versus community and systems levels are reflected in the public health leadership and adult pedagogical, professional identity literature.14–16 Grimm et al (2018) discussed the differences between developing “leaders” as compared to “leadership” skills, by highlighting the need for certain internal improvements that precede applied competencies developed through community engagement and involvement.47 A similar Maternal and Child Health leadership program noted the importance of evaluating skills development along “core” and “community/institutional” domains, mirroring the importance of mastering self-competencies that precede community outreach.48,49 Finally, the iterative, longitudinal nature of the responses and the program’s commitment to creating sustainable leadership aligns with literature on healthcare professional identity formation as a continuing process shaped by leadership reflection and practice rather than competencies alone.14–16,50 Indeed, the RWJF CS curricula are a didactic then applied pedagogical approach to meet this need, indicating internal consistency with CS program goals.3,20,22
This internal consistency is also supported by the results of this qualitative evaluation, which align with quantitative evaluations of the CS program. A 2024 evaluation of the first two cohorts (2016 and 2017) evaluated the most significant improvements in reported self-efficacy for community and systems domains for program participants,32 which aligns with its appearance as the most cited in number of competencies within that domain (n=3189). In our evaluation, social determinants of health (SDOH) were among the highest cross-coded competency, appearing in the top 5 for interpersonal, organizational, and community-level domains. Correspondingly, a quantitative evaluation of all program cohorts (2016–2020) in 2024 reported SDOH to have the highest change in average self-efficacy across competencies, increasing by 1.33 points from baseline to endline (to 6.21 out of 7).3 The alignment of increased self-efficacy in reported competencies and frequency of their implementation supports the program’s aim to develop practitioners through applied, learning-by-doing approaches that are seminal to adult learning.51
Lastly, the leadership development competencies from this project align with the priority areas of several major healthcare organizations. For example, the Josiah Macy Jr. Foundation specifically references interprofessional education and expanded clinical education beyond direct provision to address health equity concerns more directly.52 Both the National Academies of Medicine and American Medical Association (AMA) specifically mention leadership development in their priority areas to address the aging workforce and burnout for nurses and primary care physicians.53,54 Therefore, applied leadership training programs that specifically cultivate the cited competencies are urgently needed.
Limitations
Despite adding to the literature on which competencies are self-employed by practitioners in pursuit of equity-based projects, the evaluation has notable limitations. First, the RWJF program was designed to address domestic clinical leadership gaps related to healthcare access and therefore limits generalizability of findings to other international healthcare settings and leadership programs. The OWLs logs were de-identified and, therefore, we were unable to assess demographics for individual entries. This limits our ability to investigate differences in competency applications across role, setting, and other contexts that may have resulted in unmeasured heterogeneity in documented perspectives and introduce interpretive bias in our findings. Also, entries were not linked to the outcome data, which has no comparator group. Therefore, the qualitative applications of each competency described may not inherently mean “successful” project implementation, although documentation exists through other published books, manuscripts, and reports on CS and at their website.3,22,32,55 Inherent in deductive approaches, the coding categorizations were pre-defined and therefore may be too restrictive, overlooking emergent or novel themes that may arise in the data, also limiting ability to assess saturation with a predefined sample size.56 This may have also increased the risk of confirmation bias, as coders may have fit responses into codes that require more alignment or nuance. Also, the entries were self-reported and therefore subject to social desirability bias and recall bias. The self-selection could lead to over- or under-representation of competencies if participants wanted to portray their work positively or misremember the details due to time delay of entries. These limit our understanding of the leadership competencies required by healthcare professionals to develop applied projects. Future studies should link these qualitative responses with a self-evaluative tool, outcome data, or track longitudinal changes over time to truly evaluate the competencies that may play a key role in successful implementation. Comparison of results against a control group or across cohorts would strengthen our understanding of the impact of contextual factors. However, other publications on the CS program have evaluated both participant experience with the programmatic components (internal validity) and quantitative evaluation of the competencies along key predictors of adult learning: self-efficacy and confidence.5,32
Conclusion
This review of the self-reported competency entries from the Robert Wood Johnson Foundation Clinical Scholars (CS) program demonstrates that equipping clinicians with the opportunity to self-define and apply competencies may reduce critical learning gaps. Providing clinicians with protected time and resources allows for critical reflection of how they conceptualize and apply their learned competencies outside of single didactic efforts. The prevalence and bundling of competencies such as communication, collaboration, self-awareness, and innovation underscore the relational foundations needed to change the health equity status quo. Different sets of competencies that cluster across versus within domains illustrate the need for context-responsive, staged training progression, and diverse sets of tools to truly address the complexity of health equity paradigms.
Abbreviations
CS – Clinical Scholars; OWLs – Online Wisdom Logs; RWJF – Robert Wood Johnson Foundation; STAR format – Situation, Task, Action, Results format; WPIP – Wicked Problem Impact Project.
Data Sharing Statement
De-identified data (coding responses) are available upon reasonable request. For privacy concerns, we cannot provide the OWLs logs and responses.
Ethics Approval and Informed Consent
Since the data was de-identified and retroactive, there was no IRB approval required. However, consent for participation and data usage for the original CS program evaluation was obtained from the IRB at the University of North Carolina at Chapel Hill (IRB # 16-1817). Participants consented to information and data usage as part of program participation at program onset.
Consent for Publication
Participants consented to information and data usage as part of program participation at program onset.
Acknowledgments
The authors would like to thank the team of coders required for the sheer volume of qualitative analysis required for this study, including Lauren Enochs, Melissa Luna De La Garza, Martina Spain, Elikem Togo, and Toni Howell. We’d also like to thank Clinical Scholars team members, Rachel Berthiaume, Melissa Green, Katherine Donnald, Katherine Brandert, Giselle Corbie, Guarav Dave, and Michelle Abel-Shoup.
Author Contributions
LC contributed to formal analysis, investigation, methodology, project administration, supervision, validation, visualization, and writing–original draft. WR contributed to formal analysis, validation, visualization, and writing–original draft. GA contributed to formal analysis, validation, and writing–original draft. GC contributed to conceptualization, data curation, funding acquisition, project administration, resources, supervision, validation, and writing–review and editing. CF contributed to conceptualization, data curation, funding acquisition, project administration, resources, supervision, validation, and writing–review and editing.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was partially supported by a National Research Service Award Pre-Doctoral Traineeship from the Agency for Healthcare Research and Quality (AHRQ) sponsored by The Cecil G. Sheps Center for Health Services Research, The University of North Carolina at Chapel Hill, Grant No. T32-HS000032 and a NRSA Post-doctoral traineeship from the AHRQ for Emory University Center for Health Services Research, Grant No. T32-HS029585. The Clinical Scholars program was supported by a generous grant from the Robert Wood Johnson Foundation. The funders played no role in the study design, analysis, data interpretation, or writing, and the results of this paper do not reflect on the funder.
Disclosure
Ruben Fernandez, JD, served as a faculty member and an executive coach in the Clinical Scholars program and is a co-author on It-Factor Leadership: Become a Better Leader in 13 Steps, a core text used in the program; he is a creator and author of the Online Leadership Library housed at WeTrainLeaders.com, a core distance education resource used in the program, and is the spouse of Dr Claudia Fernandez, a co-author for this study. Mr. Fernandez and Dr. Fernandez were frequent collaborators for the program, but not the evaluation, as authorized by RWJF. The authors report no other conflicts of interest in this work.
References
1. The Commonwealth Fund. Mirror, mirror 2024: a portrait of the failing US. Health Syst. 2024. doi:10.26099/ta0g-zp66
2. National Academies of Sciences, Engineering, and Medicine (NASEM). Integrating Social Care Into the Delivery of Health Care: Moving Upstream to Improve the Nation’s Health. Washington (DC): National Academies Press; 2019.
3. Fernandez CSP, Corbie G, Green MA, et al. Successful, sustainable and scalable: how clinical scholars leveraged community-based system-level outcomes to address health disparities nationwide. In: From Clinical Practice to Public Health Applications - the Successful, Sustainable and Scalable Outcomes of the Clinical Scholars Program. London:IntechOpen;2025. doi:10.5772/intechopen.115583
4. Jack L. Advancing health equity, eliminating health disparities, and improving population health. Prev Chronic Dis. 2021;18. doi:10.5888/pcd18.210264
5. Corbie G, Brandert K, Noble CC, et al. Advancing health equity through equity-centered leadership development with interprofessional healthcare teams. J Gen Intern Med. 2022;37(16):4120–16. doi:10.1007/s11606-022-07529-x
6. Fernandez CS, Corbie-Smith G. Leading Community Based Changes in the Culture of Health in the US: Experiences in Developing the Team and Impacting the Community. Norderstedt (Germany): BoD–Books on Demand; 2021.
7. Corbie G, Brandert K, Fernandez CS, Noble CC. Leadership development to advance health equity: an equity-centered leadership framework. Acad Med. 2022;97(12):1746–1752. doi:10.1097/ACM.0000000000004851
8. Sadowski B, Cantrell S, Barelski A, O’Malley PG, Hartzell JD. Leadership training in graduate medical education: a systematic review. J Grad Med Educ. 2018;10(2):134–148. doi:10.4300/JGME-D-17-00194.1
9. Angood PB, Falcone CM. Preparing physician leaders for the future. Physical Leadershi J. 2023;10(4). doi:10.55834/wp.3106435376
10. Gard LA, Peterson J, Miller C, et al. Social determinants of health training in US primary care residency programs: a scoping review. Acad Med. 2019;94(1):135–143. doi:10.1097/ACM.0000000000002491
11. Chung B, Norris K, Mangione C, et al. Faculty participation in and needs around community engagement within a large multi-institutional clinical and translational science awardee. Clin Transl Sci. 2015;8(5):506–512. doi:10.1111/cts.12314
12. Upshaw V, Rice D, Cipriani K, Fernandez CSP. Equity, diversity, and inclusion in public health practice. In: Novick Morrow’s Public Health Adm Princ Popul Based Management.
13. Brandert K, Corbie-Smith G, Berthiaume R, Green M, Fernandez CS. Clinical scholars: making equity, diversity and inclusion learning an integral part of leadership development. In: Leading Community Based Changes in the Culture of Health in the US-Experiences in Developing the Team and Impacting the Community. London: IntechOpen; 2021. doi:10.5772/intechopen.98450
14. Jones A. Transformative learning in clinical education: using theory to inform practice. In: Nestel D, Reedy G, McKenna L, Gough S editors. Clinical Education for the Health Professions. Springer Nature Singapore; 2023:463–479. doi:10.1007/978-981-15-3344-0_33
15. Lewin LO, McManamon A, Stein MT, Chen DT. Minding the form that transforms: using Kegan’s model of adult development to understand personal and professional identity formation in medicine. Acad Med. 2019;94(9):1299–1304. doi:10.1097/ACM.0000000000002741
16. Maile E, McKimm J, Till A. Exploring medical leader identity and its formation. Leadersh Health Serv. 2019;32(4):584–599. doi:10.1108/LHS-12-2018-0066
17. Bandura A. Social cognitive theory in cultural context. Appl Psychol. 2002;51(2):269–290. doi:10.1111/1464-0597.00092
18. McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Q. 1988;15(4):351–377. doi:10.1177/109019818801500401
19. Putnam RD. Bowling alone: america’s declining social capital. In: Crothers L, Lockhart C editors. Culture and Politics. Palgrave Macmillan US; 2000:223–234. doi:10.1007/978-1-349-62397-6_12
20. Dave G, Noble C, Chandler C, Corbie-Smith G, Fernandez CS. Clinical scholars: using program evaluation to inform leadership development. In: Leading Community Based Changes in the Culture of Health in the US-Experiences in Developing the Team and Impacting the Community. IntechOpen; 2021. doi10.5772/intechopen.98451
21. Fernandez CSP, Noble CC, Chandler C, et al. Equity-centered leadership training found to be both relevant and impactful by interprofessional teams of health-care clinicians: recommendations for workforce-development efforts to update leadership training. Consult Psychol J. 2024;76(1):42–69. doi:10.1037/cpb0000239
22. Fernandez CS, Corbie-Smith G, Green M, Brandert K, Noble C, Dave G. Clinical scholars: effective approaches to leadership development. In: Leading Community Based Changes in the Culture of Health in the US-Experiences in Developing the Team and Impacting the Community. IntechOpen; 2021.
23. Instructure, Inc. Canvas. [Internet]. Salt Lake City (UT): Instructure, Inc; 2025. Available from: https://www.instructure.com.
24. Tross SA, Maurer TJ. The effect of coaching interviewees on subsequent interview performance in structured experience-based interviews. J Occup Organ Psychol. 2008;81(4):589–605. doi:10.1348/096317907X248653
25. Lawrence W. Social Research Methods-Qualitative and Quantitative Approaches. British Library Cataloguing-in-Publication Data; 2014.
26. Corbin J, Strauss A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. Sage publications; 2014.
27. McHugh ML. Interrater reliability: the kappa statistic. Biochem Medica. 2012;22(3):276–282. doi:10.11613/BM.2012.031
28. Geijer M, Båth M, Wessman C. Some common statistical methods for assessing rater agreement in radiological studies. Acta Radiol. 2025;66(6):675–683. doi:10.1177/02841851251319666
29. Bodnar C. Telemedicine and Pediatrics–Building a Technology-Based Collaborative in Montana. In: From Clinical Practice to Public Health Applications-The Successful, Sustainable and Scalable Outcomes of the Clinical Scholars Program. IntechOpen; 2025.
30. Collins SE, Clifasefi SL, Stanton J, et al. Community-based participatory research (CBPR): towards equitable involvement of community in psychology research. Am Psychol. 2018;73(7):884–898. doi:10.1037/amp0000167
31. Minkler M, Wallerstein N. Community-Based Participatory Research for Health: From Process to Outcomes.
32. Henry E, Chandler C, Laux J, et al. Evaluating leadership development competencies of clinicians to build health equity in America. J Contin Educ Health Prof. 2024;44(2):90. doi:10.1097/CEH.0000000000000526
33. Tajeu GS, Halanych J, Juarez L, et al. Exploring the association of healthcare worker race and occupation with implicit and explicit racial bias. J Natl Med Assoc. 2018;110(5):464–472. doi:10.1016/j.jnma.2017.12.001
34. Bransby DP, Mayo AT, Cronin MA, Park K, Yuan CT. A systematic review of respect between acute care nurses and physicians. Health Care Manage Rev. 2023;48(3):237–248. doi:10.1097/HMR.0000000000000370
35. Nembhard IM, Edmondson AC. Making it safe: the effects of leader inclusiveness and professional status on psychological safety and improvement efforts in health care teams. J Organ Behav. 2006;27(7):941–966. doi:10.1002/job.413
36. Gittell JH. Organizing work to support relational co-ordination. Int J Hum Resour Manag. 2000;11(3):517–539. doi:10.1080/095851900339747
37. Ramarajan L, Barsade SG, Burack OR. The influence of organizational respect on emotional exhaustion in the human services. J Posit Psychol. 2008;3(1):4–18. doi:10.1080/17439760701750980
38. Cronin MA, Bezrukova K, Weingart LR, Tinsley CH. Subgroups within a team: the role of cognitive and affective integration. J Organ Behav. 2011;32(6):831–849. doi:10.1002/job.707
39. Brandeis Leadership Institute. The physicians foundation. Available from: https://physiciansfoundation.org/brandeis-leadership-institute/.
40. NYU Wagner Graduate School of Public Service. Health policy for clinicians [Internet]. New York (NY): New York University; 2025. Available from: https://wagner.nyu.edu/education/certificates-non-degree-programs/health-policy-clinicians.
41. Residency Fellowship in Health Policy (RFHP). Available from: https://socialmission.org/training-programs/rfhp/.
42. American Medical Association. Training Physicians in the art of the public forum. AMA Ed Hub. Available from: https://edhub.ama-assn.org/ama-education/interactive/18574875.
43. Merrill KG, Dougherty A, Battalio SL, et al. Implementing capacity-building initiatives addressing health equity through community–academic partnerships: a qualitative study. Transl Behav Med. 2025;15(1):ibaf017. doi:10.1093/tbm/ibaf017
44. Wilkinson J, Goff M, Rusoja E, Hanson C, Swanson RC. The application of systems thinking concepts, methods, and tools to global health practices: an analysis of case studies. J Eval Clin Pract. 2018;24(3):607–618. doi:10.1111/jep.12842
45. Fernandez CSP, Taylor MM, Dave G, et al. Accelerating diversity, equity, and inclusion goals: a qualitative assessment from the lens of scientists at the 2020 clinical translational science awards annual meeting. J Clin Transl Sci. 2023;7(1):e35. doi:10.1017/cts.2022.516
46. Stamm L, Shirin A, Jenkins A, Fung C. Building capacity and trust through community engagement: lessons learned from a research in health equite symposium. J Prim Care Community Health. 2025;16:21501319251370612. doi:10.1177/21501319251370612
47. Grimm B, Tibbits M, Maloney S, Johansson P, Siahpush M. Suggestions for strengthening the public health leadership development model. Pedagogy Health Promot. 2018;4(2):88–94. doi:10.1177/2373379917721721
48. Fernandez CSP, Noble CC, Garman L. A qualitative analysis of Maternal and Child Health Public Health Leadership Institute (MCH PHLI) leaders: assessing the application of leadership skills at the “others” and “wider community” levels of the MCH leadership competencies 4.0. Matern Child Health J. 2021;25(9):1437–1446. doi:10.1007/s10995-021-03134-2
49. Fernandez CSP, Noble CC, Jensen E, Steffen D. Moving the needle: a retrospective pre- and post-analysis of improving perceived abilities across 20 leadership skills. Matern Child Health J. 2015;19(2):343–352. doi:10.1007/s10995-014-1573-1
50. Cornett M, Palermo C, Ash S. Professional identity research in the health professions—a scoping review. Adv Health Sci Educ. 2023;28(2):589–642. doi:10.1007/s10459-022-10171-1
51. Merriam SB. Adult learning theory. In: Contemporary Theories of Learning; Learning Theory in Their Own Words.
52. Irby D. Improving Environments for Learning in the Health Professions. Josiah, Macy Jr. Foundation; 2018.
53. American Medical Association (AMA). Focus on these 6 areas to boost physician well-being. 2025. Available from: https://www.amaassn.org/practice-management/physician-health/focus-these-6-areas-boost-physician-well-being.
54. National Academies of Sciences. Engineering, and Medicine: the Nursing Workforce. In: The Future of Nursing 2020-2030: Charting a Path to Achieve Health Equity. National Academies Press (US); 2021.
55. Diekmann G. Home. Clinical Scholars National Leadership Institute [Internet]. Available from: https://clinicalscholarsnli.org.
56. Leese J, Li LC, Nimmon L, Townsend AF, Backman C. Moving beyond “until saturation was reached”: critically examining how saturation is used and reported in qualitative research. Arthritis Care Res. 2021;73(8):1225–1227. doi:10.1002/acr.24600
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.