Back to Journals » Journal of Pain Research » Volume 19
From Block to Cryoneurolysis: Ultrasound-Guided Interventions for the Infrapatellar Branch of the Saphenous Nerve in Knee Surgery: A Narrative Review
Received 15 March 2026
Accepted for publication 4 July 2026
Published 10 July 2026 Volume 2026:19 609370
DOI https://doi.org/10.2147/JPR.S609370
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Yaning Tang, Xiawei Hu
Department of Anesthesiology, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China
Correspondence: Xiawei Hu, Department of Anesthesiology, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310000, People’s Republic of China, Tel +86 19521519375, Email [email protected]
Background: The infrapatellar branch of the saphenous nerve (IPBSN) is a key contributor to perioperative pain after knee surgery. Although ultrasound-guided blocks are well established, related interventions are moving toward longer-acting methods such as cryoneurolysis.
Objective: This narrative review evaluated the role of ultrasound-guided IPBSN interventions in perioperative knee analgesia, distinguishing current nerve blocks from emerging technologies.
Methods: We conducted a narrative review of the literature on preoperative and postoperative IPBSN interventions, focusing on a qualitative synthesis of the findings.
Results: Current high-level evidence (primarily randomized controlled trials) supports targeted IPBSN blocks as an effective component of multimodal analgesia, substantially reducing acute postoperative pain. In contrast, evidence for cryoneurolysis is currently limited to case series and early feasibility studies; however, it shows promising potential for prolonged analgesia, reduced opioid consumption, and shortened hospital stays.
Conclusion: The available evidence supports ultrasound-guided IPBSN nerve blocks as a useful component of multimodal analgesia for acute postoperative pain after knee surgery, particularly when administered preoperatively. However, the evidence base for cryoneurolysis remains preliminary and is limited by small sample sizes, variable protocols, and a lack of fully powered randomized trials. Although single-injection nerve blocks represent a relatively well-established technique, cryoneurolysis should still be regarded as an emerging intervention that requires further validation. High-quality, multicenter randomized controlled trials with standardized protocols are urgently needed to clarify the comparative effectiveness, optimal timing, and patient-selection criteria for these interventions.
Keywords: anterior knee pain, nerve block, pain management, ultrasound
Introduction
The increasing volume of knee surgeries, such as total knee arthroplasty (TKA)1 and anterior cruciate ligament reconstruction (ACLR), presents a significant clinical challenge, and the incidence of revision TKA (rTKA) in the United States is projected to rise.2 Alongside arthroplasty, anterior cruciate ligament (ACL) tears remain one of the most common orthopedic injuries, and surgical management of ACL ruptures is another major contributor to postoperative anterior knee pain.3
Although substantial advances have been made in the techniques and procedures of knee arthroplasty, many patients still report limited improvement in postoperative pain and physical function.4 TKA and knee arthroscopy, such as ACLR, often cause moderate-to-severe acute postoperative pain, making them common procedures that require postoperative pain management.5 Adequate postoperative pain management is important to promote early physical rehabilitation, which aids the recovery of physical fitness and shortens the length of hospital stay.6 If not properly controlled, however, pain may progress to chronic pain.7 Most data show that the incidence of chronic pain after TKA is 10% to 34% and can persist for 3 months to 5 years.8 Adequate postoperative analgesia therefore supports Enhanced Recovery After Surgery (ERAS) and the efficacy of subsequent rehabilitation exercises.6
Siviero et al reported that current smokers and individuals with depressive symptoms often fail to achieve comparable improvements in postoperative pain and functional scores4 This difference highlights a key gap in current perioperative pain management, particularly the need for targeted analgesic strategies to reduce heightened pain sensitivity and promote early activity in these subgroups.
At the same time, current interventions cannot provide sufficient long-term pain relief and may cause side effects.9,10 A sensory peripheral nerve block can target the superficial sensory nerve without producing a motor block. Compared with femoral nerve block, it confers a lower risk of accidental falls in postoperative patients.11
The infrapatellar branch of the saphenous nerve (IPBSN) is a pure sensory nerve that innervates the skin of the anterior and medial knee.12 It is a branch of the saphenous nerve, a sensory branch of the femoral nerve, and courses beneath or around the patella to supply the anteromedial knee.13 Ultrasound visualization makes it possible to block the IPBSN and provide sensory analgesia for the knee joint without the quadriceps weakness caused by femoral nerve block.14 Cryoneurolysis treats the nerve at a temperature of −20 °C to −60 °C, leading to Wallerian degeneration. This degeneration occurs distal to the injury site and involves loss of axonal continuity and of the myelin sheath, whereas the surrounding endoneurium, perineurium, and epineurium are preserved, so that normal axonal and myelin regeneration can occur within two to four months.15 This property gives cryoneurolysis a longer duration of action for relieving postoperative knee pain.
A literature search was performed in PubMed, Embase, and Web of Science without language or time restrictions, using the terms “infrapatellar branch of the saphenous nerve,” “ultrasound,” “total knee arthroplasty,” and “anterior cruciate ligament.” Randomized controlled trials, case reports, case series, and retrospective studies were included.
As this was a narrative review, we summarized the available findings narratively, rather than conducting a formal systematic review with meta-analysis. The objective of this narrative review was to comprehensively examine the relevant anatomy, mechanisms, approaches, and techniques associated with the IPBSN block and cryoneurolysis.
Anatomy
The IPBSN is the largest cutaneous branch of the saphenous nerve at the level of the knee joint. The saphenous nerve, the terminal branch of the femoral nerve, is the longest pure sensory nerve in the body; it originates from the posterior part of the lumbar plexus formed by the anterior branches of the second to fourth lumbar nerves. The saphenous nerve runs lateral to the femoral artery within the femoral triangle, enters the adductor canal, passes through the posterior margin of the adductor tendon plate at the lower end of the adductor canal, runs between the sartorius and gracilis muscles, penetrates the deep fascia, and emerges subcutaneously on the medial side of the knee joint.16,17
The IPBSN usually emerges from the main trunk of the saphenous nerve at the distal end of the adductor canal, approximately 10–15 cm proximal to the knee joint, although variations may occur at higher or lower levels. After emergence, the IPBSN runs anterolaterally and passes through the gap between the gracilis and semitendinosus muscles, accompanied by the infrapatellar branch of the descending genicular artery, with which it has a close anatomical association.18 The nerve then continues distally and distributes to the area beneath the patella and the anteromedial skin of the knee joint, and some branches may extend to the level of the tibial tuberosity19 (Figure 1).
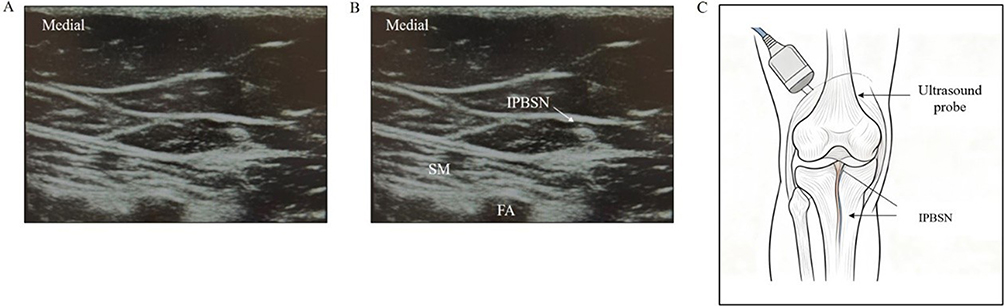 |
Figure 1 (A) Ultrasound imaging of the infrapatellar branch of the saphenous nerve; (B) Ultrasound-guided infrapatellar branch of the saphenous nerve block. The circular-like shape pointed to by the white arrow represents IPBSN; (C) clinical application pathways. Abbreviations: SM, sartorius muscle; FA, femoral artery; IPBSN, infrapatellar branch of the saphenous nerve. |
The anatomical variations of the IPBSN are substantial. They are mainly classified into four types according to how the nerve exits the gracilis muscle, of which the posterior type is the most common, accounting for approximately 62%20 (Table 1).
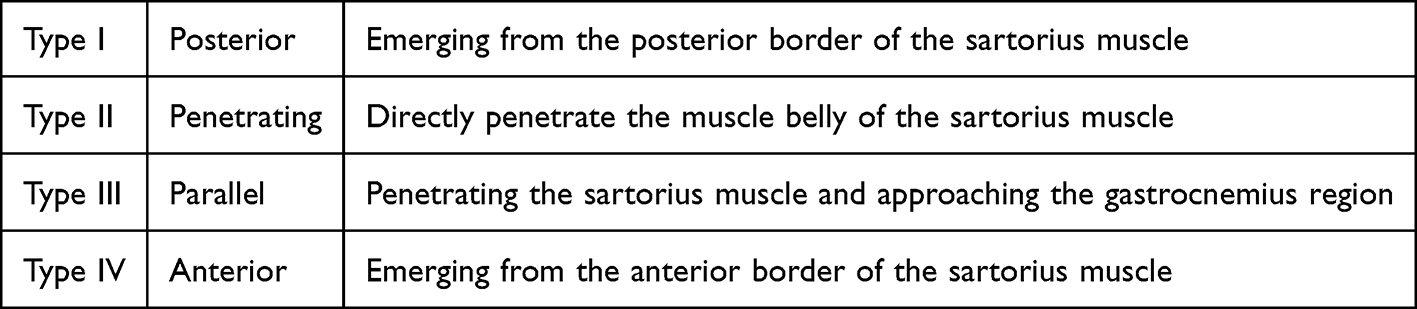 |
Table 1 IPBSN Type |
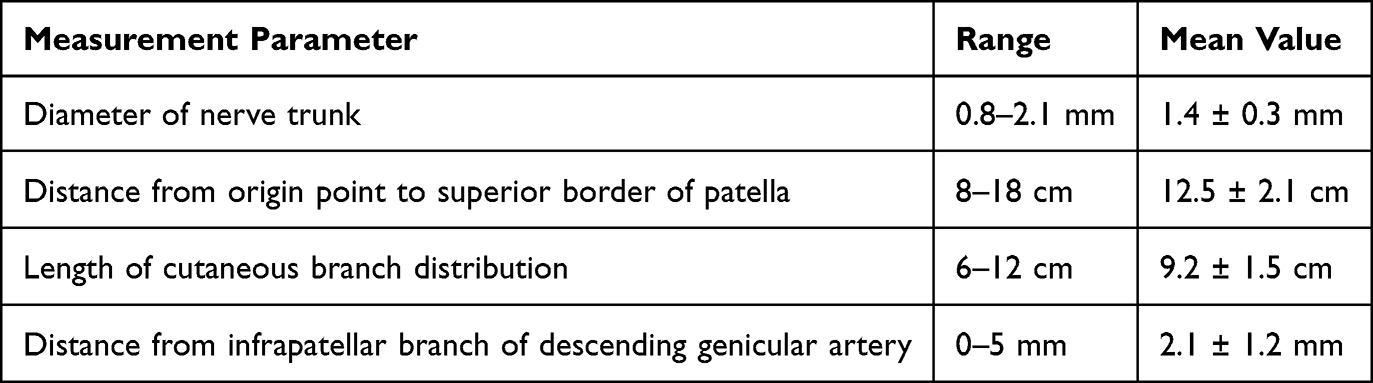
The IPBSN often shows branch variations as it passes through the gracilis muscle. A comparative study of cadaveric dissection and ultrasound found that the nerve could divide into two to three fine branches beneath the deep fascia, distributed in a fan shape. This branching pattern explains why traditional single-point block sometimes fails to achieve satisfactory results and suggests that multipoint injection or fan-shaped infiltration techniques should be adopted in clinical practice.21 A cadaveric study by Kim et al revealed that, because the nerves show higher echo contrast within muscle tissue, intramuscular variations are easier to identify with ultrasound; however, variations that emerge from the anterior and posterior margins of the sartorius muscle are more difficult to recognize because their echo pattern resembles that of the surrounding adipose tissue22,23 (Table 2)
 |
Approaches and Techniques of Ultrasound-Guided Injection
Position
A standard position was used to expose the medial side of the knee joint. The patient was placed supine with the affected limb slightly externally rotated and extended, to facilitate probe placement and needle insertion.
Approaches
In the study by Lundblad et al, the ultrasound probe was placed approximately 10–15 cm above the medial thigh muscle and above the medial joint line, perpendicular to the course of the saphenous nerve This position corresponds roughly to the upper edge of the patella (the base of the patella). The probe was moved medially until the gracilis and sartorius muscles were visible, and the saphenous nerve was identified deep within the fascia of the gracilis muscle. The saphenous nerve was first traced in the coronal plane to confirm that it lay above the femoral groove and the femoral artery, and was then traced distally until the bifurcation of the IPBSN could be identified. An out-of-plane technique was used to insert the needle tip without prior local anesthesia of the skin. Under ultrasound guidance, the needle tip was advanced adjacent to the IPBSN, and a small amount of solution was injected to verify its position; once the position was acceptable, 10 mL of the blocking agent was injected, and the solution was observed encapsulating the nerve.24 IPBSN anesthesia is defined as a nerve block occurring within an area 5 cm above the tibial tuberosity, 8 cm medial, 10 cm below, and 3 cm lateral.25
Interestingly, in 2019, Gong et al reported that in their clinical practice they did not detect the IPBSN beneath the adductor brevis muscle Given the current anatomical localization of the IPBSN, the IPBSN has no clear anatomical relationship with the adductor brevis muscle. Therefore, in their study, the ultrasound-guided IPBSN block point was located at the superficial junction between the gracilis and medial thigh muscles. The technique was applied to five adult patients undergoing patellar surgery. The patients were placed supine with the legs naturally extended. A 5–10 MHz linear probe was placed horizontally on the medial thigh, approximately 5 cm above the lateral femoral condyle, and then moved medially or laterally until the gracilis and medial thigh muscles were clearly visible. At approximately the junction of the gracilis and medial thigh muscles, an elliptical IPBSN could be found; using an in-plane needle technique under ultrasound guidance, a needle was inserted near the nerve and 5 mL of 0.33% ropivacaine was injected.26 This technique is simpler and more convenient than previously reported approaches, but further multicenter, large-sample randomized controlled trials are still needed.
Herteleer et al proposed a selective distal IPBSN block technique based on seven lower-limb cadaveric dissections At a horizontal level above the patella, two approaches were compared: a proximal medial approach near the patella and a distal medial approach near the medial femoral condyle. For ultrasound localization, the probe was first placed on the surface of the adductor muscle at the junction of the middle and lower thirds of the thigh, where the adductor canal could be seen. The probe was then moved laterally to track the saphenous nerve and follow its bifurcation to its terminal branches, and longitudinal (proximal-to-distal or distal-to-proximal) and transverse (anterior-to-posterior or posterior-to-anterior) dynamic scans were performed to distinguish the IPBSN accurately from the saphenous nerve and the anterior branches of the femoral nerve. A 22-gauge, 50-mm needle was then advanced in-plane or out-of-plane to the target structure. The proximal approach benefits from the nerve lying within a distinct fascial compartment surrounded by low-echoic adipose tissue; however, its selectivity is relatively low, and it is prone to blocking other nearby nerves, such as the medial sural cutaneous nerve or the anterior branch of the femoral nerve. In contrast, the distal approach mitigates the effects of IPBSN branch variations and changes in position relative to the rectus femoris muscle, offering stronger selectivity but requiring advanced ultrasound skill because of the smaller size of the nerves.27
Indications and Clinical Relevance (Table 3)
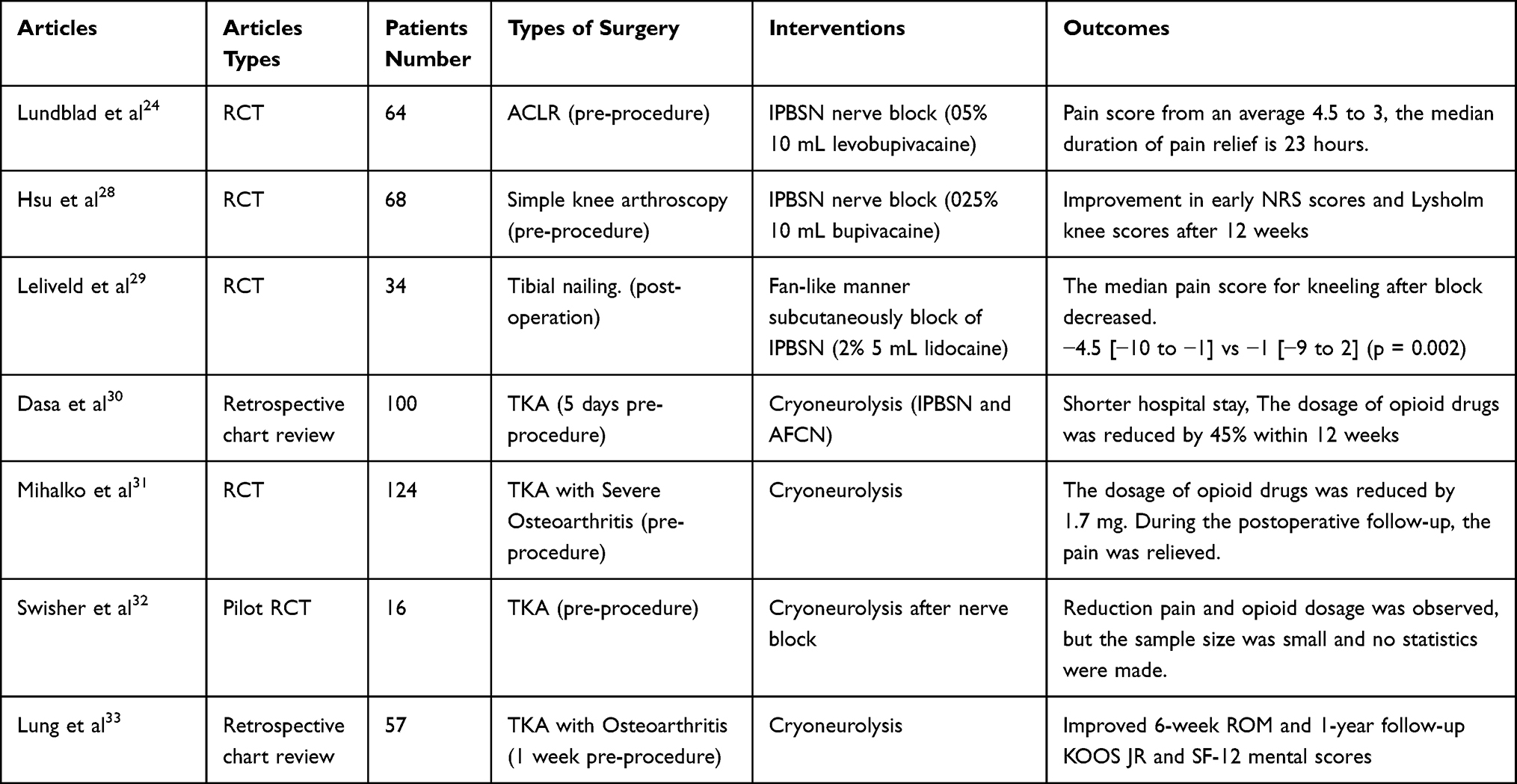 |
Table 3 Researches on IPBSN Intervention |
The clinical evidence for IPBSN interventions spans multiple study designs with varying methodological rigor. Among the included studies, prospective double-blind RCTs24,28,29 represent the highest level of evidence for IPBSN nerve block. For cryoneurolysis, one RCT31 and one pilot RCT (limited by a small sample size)32 constitute the highest available evidence, whereas retrospective chart reviews30,33 provide complementary real-world data but carry inherent selection bias. Case reports and technical descriptions26,27 illustrate procedural innovations but lack comparative controls. This hierarchy should be considered when weighing clinical recommendations: RCTs provides the most reliable evidence regarding treatment efficacy, whereas lower-level evidence primarily supports feasibility and hypothesis generation. Table 3 summarizes the key characteristics and outcomes of these studies.
Perioperative Nerve Block in Knee Surgery
IPBSN interventions can provide postoperative patients with treatment options that alleviate perioperative pain with fewer side effects. An RCT by Lundblad et al included 64 patients who underwent arthroscopy-assisted anterior cruciate ligament repair, all of whom received multimodal analgesia; the authors found that pain scores decreased and sleep improved in the 31 patients who received an ultrasound-guided IPBSN nerve block within 16–24 hours after surgery.24 Hsu et al studied 68 patients who underwent simple knee arthroscopy (meniscectomy, meniscal repair, or synovial debridement) and found that patients who received an IPBSN nerve block had lower early NRS pain scores and improved Lysholm knee scores at 12 weeks, with no significant reduction in quadriceps strength.28 Leliveld et al, considering that tibial fixation might damage the IPBSN and cause knee pain, conducted an RCT in 34 patients who had undergone tibial nailing, using 5 mL of 2% lidocaine for subcutaneous fan-shaped block of the IPBSN, and found that pain in the kneeling position was significantly relieved29 Although these findings are encouraging, the sample sizes across these RCTs were relatively modest (34 to 68 patients), most assessed only short-term outcomes (24 hours to 12 weeks postoperatively), and all trials were single-center, which may limit external validity.
Perioperative Cryoneurolysis in Knee Surgery
Postoperative TKA is often accompanied by severe and persistent pain, so a peripheral nerve block based on local anesthesia is commonly used to achieve postoperative analgesia. Cryoneurolysis uses low temperature to achieve a reversible sensory (and motor) block, and its duration of action can extend to weeks or even months, which is more consistent with the duration of common pain after TKA. Several clinical studies have investigated IPBSN cryoablation as a potential option for post-TKA pain management.30–33 However, the evidence base for cryoneurolysis remains less robust than that for nerve blocks. The existing literature is characterized by heterogeneous protocols (varying timing, duration, and target temperatures), and only one fully powered RCT31 has been published to date. The pilot RCT by Swisher et al32 included only 16 patients and did not reach statistical significance for its primary endpoints, underscoring the need for larger, adequately powered confirmatory trials.
Collectively, the available studies suggest that IPBSN-targeted interventions may improve pain relief and reduce opioid consumption, providing a useful adjunct for perioperative pain management in knee surgery. Nevertheless, the strength of this conclusion is tempered by the methodological limitations and heterogeneity of the evidence discussed above.
Contraindications
No contraindications are clearly defined or universally agreed upon. Relative contraindications include, but are not limited to, IPBSN anatomical variation, local infection or inflammation, abnormal coagulation, a previous history of knee nerve injury or surgery, prior radiotherapy, inability of the patient to cooperate, local sensory loss or chronic skin ulceration, extremely short life expectancy or end-stage disease, severe knee deformity, and severe obesity (BMI > 35).
Complications
Nerve Block
The most common complication of nerve block is nerve injury. Because the IPBSN is a pure sensory nerve, such injury causes only numbness or reduced sensation in the subpatellar skin, without any motor or functional impairment. Other potential complications include puncture injury to small blood vessels, skin infection, short-term numbness, and local anesthetic allergy.
Cryoneurolysis
To date, no complications associated with cryoneurolysis have been reported. Local bruising is the most common finding (without clinical impact), and no persistent numbness or other neurological effects were observed during follow-up.
Limitations and Future Directions
IPBSN-targeted interventions represent one component of a comprehensive analgesic strategy that should also include systemic pharmacotherapy (acetaminophen, NSAIDs, and gabapentinoids), local infiltration analgesia (LIA), and other regional anesthesia techniques such as adductor canal block (ACB) and femoral nerve block (FNB). Although ACB preserves quadriceps strength better than FNB,11 the IPBSN block offers the theoretical advantage of even more selective sensory blockade without any motor involvement, given that the IPBSN is a purely cutaneous nerve. However, direct comparative studies between IPBSN block and ACB are currently lacking, representing an important gap in the literature.
The choice of regional anesthetic technique must also consider patient-specific factors, the surgical approach, and the expected duration of postoperative pain. In a prospective study of 155 patients undergoing percutaneous hallux valgus surgery, Biz et al34 compared ultrasound-guided sciatic–femoral nerve block with ankle block and found that both techniques were safe and effective in reducing postoperative pain, with no significant difference in the incidence of chronic pain syndrome (CPS) at 6-month follow-up (7.1% and 8.4%, respectively). Importantly, that study showed that several regional anesthesia options can achieve satisfactory analgesia and that factors such as ASA classification, BMI, and pre-existing low back pain may influence patient-reported outcomes more than the choice of block technique itself. Extrapolating to knee surgery, these findings suggest that IPBSN interventions should not be viewed in isolation but rather as part of a tailored, multimodal approach in which the incremental benefit of adding an IPBSN block to existing analgesic regimens requires further verification.
Several issues in the current evidence warrant further consideration. First, the available RCTs of IPBSN nerve block, although methodologically sound, have relatively small sample sizes and narrow inclusion criteria, which may limit generalizability to broader surgical populations. Second, the literature on cryoneurolysis, though promising, remains preliminary: the absence of large, multicenter RCTs, the heterogeneity of freeze protocols (timing, duration, and number of cycles), and the lack of standardized outcome measures hinder meaningful cross-study comparison. Third, conflicting evidence exists regarding the magnitude of analgesic benefit; although most studies report positive outcomes, some RCTs have not demonstrated statistically significant reductions in opioid consumption, suggesting that the effect size may be modest and influenced by patient selection and concomitant analgesic regimens. Fourth, the long-term safety profile of cryoneurolysis, particularly regarding nerve regeneration and the potential for neuroma formation, remains incompletely characterized beyond the 6- to 12-month follow-up reported in current studies.
From a clinical perspective, integrating IPBSN interventions into ERAS pathways appears promising, but several questions remain unresolved. The optimal timing of cryoneurolysis (preoperative versus postoperative), the ideal patient population (eg, those with high opioid tolerance or chronic pain), and the cost-effectiveness of these interventions compared with conventional approaches have not been rigorously established. Future research should prioritize head-to-head comparisons with established regional techniques, standardization of procedural protocols, and longer-term follow-up to fully characterize the risk–benefit profile of IPBSN-targeted therapies.
This review has several limitations. As it is a narrative rather than a systematic review, the literature search did not adhere to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. In addition, the included studies used no unified standards or follow-up time points for pain assessment and outcome reporting, which limits cross-study comparability. The evidence for cryoneurolysis is drawn from a small number of studies with heterogeneous protocols, and long-term outcomes beyond one year remain largely unexplored. Further validation through multicenter, large-sample, blinded randomized controlled trials with standardized protocols is needed to establish the optimal role of IPBSN interventions in perioperative knee analgesia.
Conclusions
In summary, the current evidence on IPBSN interventions in knee surgery is characterized by high variability in study design, procedural protocols, outcome measures, and follow-up duration. Ultrasound-guided IPBSN nerve block, supported by several small-to-moderate-sized randomized controlled trials,24,28,29 can be considered a relatively established technique for acute postoperative analgesia as part of a multimodal regimen. In contrast, cryoneurolysis—though promising in terms of prolonged pain relief and opioid-sparing effects30–33—remains an emerging intervention supported predominantly by pilot data and retrospective studies, with only one fully powered randomized controlled trial published to date. The existing evidence is heterogeneous, and some randomized controlled trials have not demonstrated consistent benefits, underscoring the need for further verification through standardized protocols and large-sample studies.
Preoperative and postoperative applications must be distinguished. Preoperative IPBSN intervention is based primarily on the concept of preventive analgesia, aiming to block nociceptive signals before surgical incision and reduce central sensitization; this approach is supported by several RCTs of nerve block24,28 and by emerging cryoneurolysis data.31,32 Postoperative intervention, by contrast, is used to treat chronic neuropathic pain (persisting ≥ 3 months) attributed to iatrogenic IPBSN injury during surgery; after etiological confirmation by diagnostic block, cryoablation or neurectomy may be considered for targeted denervation. Both strategies have been reported as safe, with only transient hypoesthesia or local ecchymosis as the main adverse events; however, rigorous long-term safety data, particularly for cryoneurolysis, remain limited.
Several key questions remain unresolved. The effect of IPBSN intervention varies considerably with the timing of the procedure, technical specifications, and patient selection, and these techniques should not be regarded as a replacement for systemic multimodal pharmacotherapy. Well-designed, multicenter, blinded randomized controlled trials with adequate sample sizes, standardized freeze protocols (for cryoneurolysis), and uniform outcome measures are urgently needed to establish evidence-based recommendations. Future research should prioritize head-to-head comparisons between IPBSN interventions and established regional techniques, long-term functional and safety outcomes beyond one year, and cost-effectiveness analyses to define the optimal role of these interventions in individualized enhanced recovery pathways.
Funding
The review was funded by the National Natural Science Foundation of China (Grant nos. 82402555).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stubnya BG, Schulz M, Váncsa S, et al. Global trends in joint arthroplasty: a systematic review and future projections. J Clin Med. 2025;14(22):8214. doi:10.3390/jcm14228214
2. Schwartz AM, Farley KX, Guild GN, et al. Projections and epidemiology of revision Hip and knee arthroplasty in the United States to 2030. J Arthroplasty. 2020;35(6S):S79–8. doi:10.1016/j.arth.2020.02.030
3. Biz C, Cigolotti A, Zonta F, et al. ACL reconstruction using a bone patellar tendon bone (BPTB) allograft or a hamstring tendon autograft (GST): a single-center comparative study. Acta Biomed. 2019;90(12–S):109–117. doi:10.23750/abm.v90i12-S.8973
4. Siviero P, Marseglia A, Biz C, et al. Quality of life outcomes in patients undergoing knee replacement surgery: longitudinal findings from the QPro-Gin study. BMC Musculoskelet Disord. 2020;21(1):436. doi:10.1186/s12891-020-03456-2
5. Gerbershagen HJ, Aduckathil S, van Wijck AJ, et al. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology. 2013;118(4):934–944. doi:10.1097/ALN.0b013e31828866b3
6. Li Y, Wulamu W, Yushan N, et al. Effects of adding morphine to periarticular infiltration analgesia combined with single-dose epidural morphine in total knee arthroplasty: a randomized controlled study. Orthop Surg. 2023;15(4):1021–1027. doi:10.1111/os.13637
7. Althaus A, Arránz Becker O, Neugebauer E. Distinguishing between pain intensity and pain resolution: using acute post-surgical pain trajectories to predict chronic post-surgical pain. Eur J Pain. 2014;18(4):513–521. doi:10.1002/j.1532-2149.2013.00385.x
8. Beswick AD, Wylde V, Gooberman-Hill R, et al. What proportion of patients report long-term pain after total Hip or knee replacement for osteoarthritis? A systematic review of prospective studies in unselected patients. BMJ Open. 2012;2(1):e000435. doi:10.1136/bmjopen-2011-000435
9. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain—United States, 2016. JAMA. 2016;315(15):1624–1645. doi:10.1001/jama.2016.1464
10. Li L, Zeng Z, Zhang H, et al. Different prevalence of neuropathic pain and risk factors in patients with knee osteoarthritis at stages of outpatient, awaiting, and after total knee arthroplasty. Orthop Surg. 2022;14(11):2871–2877. doi:10.1111/os.13491
11. Kim DH, Lin Y, Goytizolo EA, et al. Adductor canal block versus femoral nerve block for total knee arthroplasty: a prospective, randomized, controlled trial. Anesthesiology. 2014;120(3):540–550. doi:10.1097/ALN.0000000000000119
12. Tran J, Peng PWH, Lam K, et al. Anatomical study of the innervation of anterior knee joint capsule: implication for image-guided intervention. Reg Anesth Pain Med. 2018;43(4):407–414. doi:10.1097/AAP.0000000000000778
13. Bademkiran F, Obay B, Aydogdu I, et al. Sensory conduction study of the infrapatellar branch of the saphenous nerve. Muscle Nerve. 2007;35(2):224–227. doi:10.1002/mus.20682
14. Horner G, Dellon AL. Innervation of the human knee joint and implications for surgery. Clin Orthop Relat Res. 1994;(301):221–226.
15. Biel E, Aroke EN, Maye J, et al. The applications of cryoneurolysis for acute and chronic pain management. Pain Pract. 2023;23(2):204–215. doi:10.1111/papr.13182
16. Standring S, ed.. Gray’s Anatomy: The Anatomical Basis of Clinical Practice.
17. Peng MS, Clendenen SR, Shi GG, et al. Infrapatellar branch of saphenous nerve: from anatomy, sonoanatomy, to its clinical implications. Reg Anesth Pain Med. 2026;51(4):465–472. doi:10.1136/rapm-2025-106383
18. Saranteas T, Anagnostis G, Paraskeuopoulos T, et al. Anatomy and clinical implications of the ultrasound-guided subsartorial saphenous nerve block. Reg Anesth Pain Med. 2011;36(4):399–402. doi:10.1097/AAP.0b013e318220f172
19. Kalthur SG, Sumalatha S, Nair N, et al. Anatomic study of infrapatellar branch of saphenous nerve in male cadavers. Ir J Med Sci. 2015;184(1):201–206. doi:10.1007/s11845-014-1087-2
20. Arthornthurasook A, Gaew-Im K. Study of the infrapatellar nerve. Am J Sports Med. 1988;16(1):57–59. doi:10.1177/036354658801600110
21. Riegler G, Jengojan S, Mayer JA, et al. Ultrasound anatomic demonstration of the infrapatellar nerve branches. Arthroscopy. 2018;34(10):2874–2883. doi:10.1016/j.arthro.2018.05.043
22. Kim J, Kim SH, Moon HK, et al. Validation of ultrasound-guided approximation of infrapatellar branch of the saphenous nerve: a cadaveric study. Anesth Analg. 2024;139(1):247–249. doi:10.1213/ANE.0000000000006882
23. Li Q, Aierken A, Qin J, et al. Targeting the infrapatellar branch of the saphenous nerve for pain relief in patients with acute or chronic knee pain: a systematic review of randomized controlled trials and cohort studies. Orthop Surg. 2025;17(4):981–989. doi:10.1111/os.14349
24. Lundblad M, Forssblad M, Eksborg S, et al. Ultrasound-guided infrapatellar nerve block for anterior cruciate ligament repair: a prospective, randomised, double-blind, placebo-controlled clinical trial. Eur J Anaesthesiol. 2011;28(7):511–518. doi:10.1097/EJA.0b013e32834515ba
25. Lundblad M, Kapral S, Marhofer P, et al. Ultrasound-guided infrapatellar nerve block in human volunteers: description of a novel technique. Br J Anaesth. 2006;97(5):710–714. doi:10.1093/bja/ael241
26. Gong W, Wang A, Fan K. A simple and novel ultrasound-guided approach for infrapatellar branch of the saphenous nerve block. J Clin Anesth. 2019;57:22–23. doi:10.1016/j.jclinane.2019.02.027
27. Herteleer M, Roussel N, Deroubaix L, et al. Selective distal block of the infrapatellar branch of the saphenous nerve: anatomical and ultrasonographic insights. Surg Radiol Anat. 2025;47(1):87. doi:10.1007/s00276-025-03598-9
28. Hsu LP, Oh S, Nuber GW, et al. Nerve block of the infrapatellar branch of the saphenous nerve in knee arthroscopy: a prospective, double-blinded, randomized, placebo-controlled trial. J Bone Joint Surg Am. 2013;95(16):1465–1472. doi:10.2106/JBJS.L.01534
29. Leliveld MS, Kamphuis SJM, Verhofstad MHJ. An infrapatellar nerve block reduces knee pain in patients with chronic anterior knee pain after tibial nailing: a randomized, placebo-controlled trial in 34 patients. Acta Orthop. 2019;90(4):377–382. doi:10.1080/17453674.2019.1613808
30. Dasa V, Lensing G, Parsons M, et al. Percutaneous freezing of sensory nerves prior to total knee arthroplasty. Knee. 2016;23(3):523–528. doi:10.1016/j.knee.2016.01.011
31. Mihalko WM, Kerkhof AL, Ford MC, et al. Cryoneurolysis before total knee arthroplasty in patients with severe osteoarthritis for reduction of postoperative pain and opioid use in a single-center randomized controlled trial. J Arthroplasty. 2021;36(5):1590–1598. doi:10.1016/j.arth.2020.11.013
32. Swisher MW, Ball ST, Gonzales FB, et al. A randomized controlled pilot study using ultrasound-guided percutaneous cryoneurolysis of the infrapatellar branch of the saphenous nerve for analgesia following total knee arthroplasty. Pain Ther. 2022;11(4):1299–1307. doi:10.1007/s40122-022-00427-4
33. Lung BE, Karasavvidis T, Sharma AK, et al. Cryoneurolysis is a safe, effective modality to improve rehabilitation after total knee arthroplasty. Life. 2022;12(9):1344. doi:10.3390/life12091344
34. Biz C, de Iudicibus G, Belluzzi E, et al. Prevalence of chronic pain syndrome in patients who have undergone hallux valgus percutaneous surgery: a comparison of sciatic-femoral and ankle regional ultrasound-guided nerve blocks. BMC Musculoskelet Disord. 2021;22(1):1043. doi:10.1186/s12891-021-04911-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.