Back to Journals » Journal of Pain Research » Volume 16
Frequency-Dependent Alterations in the Amplitude of Low-Frequency Fluctuations in Patients with Acute Pericoronitis: A Resting-State fMRI Study
Authors Tang X, Li B, Wang M, Gao L ![]() , He Y, Xia G
, He Y, Xia G ![]()
Received 14 November 2022
Accepted for publication 25 January 2023
Published 15 February 2023 Volume 2023:16 Pages 501—511
DOI https://doi.org/10.2147/JPR.S397523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Keith
Xin Tang,1 Bin Li,1 Mengting Wang,1 Lei Gao,2 Yulin He,1,* Guojin Xia1,*
1Department of Radiology, the First Affiliated Hospital of Nanchang University, Nanchang, People’s Republic of China; 2Department of Radiology, Zhongnan Hospital of Wuhan University, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yulin He; Guojin Xia, Department of Radiology, the First Affiliated Hospital of Nanchang University, 17 Yongwaizheng Street, Nanchang, Jiang Xi, 330006, People’s Republic of China, Tel +86 0791 8869 3802, Email [email protected]; [email protected]
Background: Acute pericoronitis (AP) is a common cause of odontogenic toothache. Pain significantly affects the structure and function of the brain, but alterations in spontaneous brain activity in patients with AP are unclear.
Purpose: To apply the amplitude of low-frequency fluctuations (ALFF) method in resting-state functional magnetic resonance imaging to investigate altered spontaneous brain activity characteristics in patients with AP in different frequency bands (typical, slow-4, and slow-5 bands) and assess their correlation with clinical scores.
Patients and Methods: Thirty-four right-handed patients with AP and 31 healthy controls (HC), matched for age, sex, education, and right-handedness, were enrolled. All subjects underwent resting-state functional magnetic resonance imaging. DPABI software was used for data preprocessing and extracting the ALFF values in different frequency bands. Subsequently, differences in ALFF values in the three bands were compared between the two groups. Correlation between ALFF values in the differential brain regions and clinical scores was assessed.
Results: In the typical band, ALFF values were higher in the left insula, left superior occipital gyrus, left inferior parietal lobule, left posterior cerebellar lobule, and right postcentral gyrus in the AP than in the HC group. In the slow-4 band, ALFF values in the left superior occipital gyrus, right superior occipital gyrus, and right middle occipital gyrus were higher, and those in the right cingulate gyrus and right superior temporal gyrus were lower in the AP than in the HC group. In the slow-5 band, the ALFF values in the left insula and left superior occipital gyrus were higher in the AP than in the HC group. The ALFF values of the typical bands in the left insula, left inferior parietal lobule, and right postcentral gyrus correlated negatively, those of the slow-4 band in the right middle occipital gyrus correlated positively, and those of the slow-5 band in the left insula correlated negatively with the visual analogue scale score in the AP group.
Conclusion: Our results suggested that the intrinsic brain activity of AP patients was abnormal and frequency-dependent. This provides new insights to explore the neurophysiological mechanisms of AP.
Keywords: acute pericoronitis, amplitude of low-frequency fluctuations, functional magnetic resonance imaging, pain, resting state
Introduction
Acute pericoronitis (AP) is a common, limited odontogenic infection.1 AP involves an inflammation of the soft tissues surrounding the third molar (wisdom tooth) when eruption is incomplete or obstructed, usually in the mandibular third molar. Toothache is the most dominant clinical symptom of AP, and the pain level can progress from a dull ache to a radiating pain.2 Toothache produced by AP is injury-receptive pain, and its conduction pathway is the trigeminal nerve‒spinal nucleus‒thalamic pathway.3 Previous studies have mostly focused on the peripheral neural mechanisms of dental pain,4,5 but less on its central neural mechanisms and cortical activity.
With increasing application of functional magnetic resonance imaging (fMRI) techniques have been applied to the study of various pain disorders, the role of the central nervous system in many pain modulation networks has gradually come to be elucidated. Recent fMRI studies on odontogenic pain have mostly focused on task-state fMRI studies in which dental pain is produced in healthy subjects by electrical stimulation,6–8 ice stimulation,9 etc., in order to observe changes in BOLD signals in the subject’s brain. The dental pain produced in the subjects by experimental stimuli was transient and qualitatively different from the spontaneous pain caused by lesions of the tooth and surrounding tissues. From the few resting-state fMRI studies that included subjects with chronic toothache,10,11 it is not clear how neuronal activity in the brain is altered in patients with AP.
Amplitude of low-frequency fluctuation (ALFF) is a resting-state fMRI analysis method that assesses the level of spontaneous activity of neurons in a specific region of the brain during a relatively short period of time, by calculating the average amplitude of the deviation of the brain’s BOLD signal from baseline.12 The simplicity and reliability of measurement and calculation make ALFF values an effective tool for studying disease characteristics, and they are widely used in brain function studies of pain-related diseases.13–15 Currently, most of the brain function studies using ALFF as a method focus on the typical frequency band, ie, 0.01‒0.08 Hz, which lacks frequency specificity. The BOLD power spectrum was divided into five different frequency ranges in the study by Zuo et al.16 The higher frequency bands, such as slow-2 (0.198‒0.25 Hz) and slow-3 (0.073‒0.198 Hz) mainly reflect the signal from the white matter of the brain and are susceptible to interference from physiological noise. The lower frequency bands, slow-5 (0.01‒0.027 Hz) and slow-4 (0.027‒0.073 Hz), on the other hand, mainly reflect the signals from gray matter, have higher retest reliability, and are less influenced by physiological noise. Several previous pain-related disorders have illustrated the frequency dependency of variations in ALFF values. For example, ALFF values in patients with postherpetic neuralgia have shown bidirectional changes in the slow-4 and slow-5 bands.17 In a study on patients with trigeminal neuralgia, it was also shown that the ALFF values in the slow-4 frequency band were significantly increased, while the default network was significantly activated in the slow-5 frequency band, in the brainstem.18
We hypothesized that there is abnormal spontaneous brain activity in patients with AP and that this would be characterized by frequency specificity. Therefore, this study sought to use the ALFF method to evaluate changes in spontaneous neuronal activity in the brain of patients with AP, in different frequency bands (the typical band, slow-4 band and slow-5 band), and to assess the correlation thereof with the clinical scores of the patients in order to improve the understanding of the central alterations caused by AP.
Materials and Methods
Subjects
The study was approved by the Medical Research Ethics Committee of the First Affiliated Hospital of Nanchang University and in compliance with the principles of the Declaration of Helsinki. All subjects participated voluntarily and were informed of the purpose, methods, and possible risks of the study, and all signed the informed consent form.
In this experiment, 34 patients with AP (12 males and 22 females; all right-handed, aged 20‒35 years), diagnosed at the outpatient clinic of the Department of Dentistry, The First Affiliated Hospital of Nanchang University, were recruited from August 2020 to July 2021. During the same period, 31 volunteers (11 males and 20 females) matched to the AP group in terms of age, sex, education level, and handedness were recruited as healthy controls (HCs).
For the AP group, patients with toothache suffering from AP (disease duration <7 days), with no other oral and maxillofacial organic diseases, such as temporomandibular joint disorders and tumors, no history of oral and maxillofacial trauma, and who were right-handed, were included. The exclusion criteria were the presence of any of the following: a long history of chronic toothache (duration >3 months); other types of acute toothache, such as acute pulpitis or periapical periodontitis; a history of other non-dental pain, such as headache, trigeminal neuralgia, back pain, lower back pain, or muscle pain; and a history of analgesic treatment.
All subjects had to meet the following criteria: absence of a history of cardiovascular disease, such as hypertension, coronary artery disease, cerebral infarction, and cerebral hemorrhage; absence of contraindications to MRI examination, such as claustrophobia, or history of pacemaker or metal stent implantation, absence of a history of intracranial organic lesions or trauma; and absence of psychiatric disorders, such as autism, schizophrenia, depression.
Pain intensity in AP patients was assessed prior to fMRI scanning using a visual analog scale (VAS), with scores ranging from 0 to 10, indicating pain intensity ranging from no pain to unbearable pain.
MRI Acquisition
In this study, a 3.0-T Trio Tim magnetic resonance scanner (8-channel phased-array cranial coil) from Siemens (Erlangen, Germany), was used to perform cranial scans on all subjects. The subjects were scanned in a supine position with head-first entry. Subjects were instructed to close their eyes, remain calm, not to think of anything specifically, and to remain mentally alert but relaxed during the scan. A conventional MRI scan was first performed to exclude brain disease. The parameters were as follows: (1) T1-weighted imaging (T1WI): horizontal axis position, TR = 600 ms, TE = 10 ms, slice thickness = 5 mm, slice gap = 1.5 mm, field-of-view (FOV) = 240 mm × 240 mm, matrix = 256×256. (2) T2-weighted imaging (T2WI): horizontal axis position, TR = 3000 ms, TE = 122 ms, layer thickness = 5 mm, layer spacing = 1.5 mm, FOV = 240 mm × 240 mm, matrix = 256×256. High-resolution T1 thin-slice structural image sequence and parameters: acquired with sagittal 3D gradient echo T1WI (T1-weighted 3D SPGR) sequence, TR = 1900 ms, TE = 2.26 ms, slice thickness = 1 mm, slice gap = 0.5 mm, FOV = 240 mm × 240 mm, matrix = 256 × 256, flip angle = 9°. Resting-state fMRI sequence and parameters: acquired with gradient echo-echo planar imaging (GRE-EPI) sequence, TR = 2000 ms, TE = 30 ms, slice thickness = 4 mm, slice gap = 1.2 mm, FOV = 220 mm × 220 mm, matrix = 64 × 64, flip angle = 90°, 240 time points in total, 30 slices scanned continuously. The scanning area was the whole brain.
MRI Data Preprocessing
The resting fMR images were preprocessed on MATLAB 2013b (MathWorks, Natick, MA, USA) platform using DPABI software (http://rfmri.org/dpabi).19 The main steps were as follows: (1) Data format conversion. (2) Removal of the first 10 time-points. (3) Slice-timing correction, using the middle slice as the reference. (4) Head-movement correction (removal of data with head translation >2 mm and rotation >2° during the scanning process). (5) Spatial normalization (aligning images to MNI standard space). (6) Origin correction, 3 mm × 3 mm × 3 mm resampling of the normalized image. (7) Spatial smoothing (full-width at half-maximum of 6 mm × 6 mm × 6 mm). (8) De-linearization drift.
ALFF Calculation
After the above preprocessing steps, the time series of each voxel in the typical band (0.01‒0.08 Hz), slow-4 band (0.027‒0.073 Hz), and slow-5 band (0.01‒0.027 Hz) were extracted with band-pass filters, and the power spectrum was obtained by converting the time series to the frequency domain using the Fast Fourier Transform. The square root of the power spectrum was then calculated, and the square root of the average was the ALFF value for that voxel. The ALFF value for each voxel was divided by the whole-brain mean ALFF value to obtain a normalized ALFF value for subsequent statistical analysis.
Statistical Analyses
The IBM SPSS 23.0 (SPSS Inc., Chicago, IL, USA) statistical software was used for statistical analysis of the clinical data of the subjects in both groups. Sex distribution was compared by chi-square test, and age by the two-sample t-test, between the groups. Statistical significance was set at P < 0.05.
Using the statistical module in the DPABI toolkit, a two-sample t-test was applied to the ALFF values in the typical band, slow-4 band, and slow-5 band for the AP and HC groups, respectively, with age and sex as covariates. The statistics were then corrected for Gaussian random fields, and P < 0.001 at the voxel-level and P < 0.05 at the cluster-level were considered statistically significant. The viewer module in the DPABI toolkit was used to display the brain areas that differed between the two groups.
After extracting the ALFF values of the above-mentioned brain regions showing significant differences between the groups, using the DPABI toolkit, the correlation between the ALFF values of these brain regions and patients’ pain VAS scores was analyzed using IBM SPSS 23.0 (SPSS Inc.) statistical software. Pearson’s correlation coefficient was calculated and P < 0.05 was considered statistically significant.
Results
Demographic and Clinical Characteristics
Sixty-five subjects were included in this study. The clinical data and demographics of the subjects in both groups are shown in Table 1. There were no statistically significant differences between the AP and HC groups in terms of age and sex (P > 0.05).
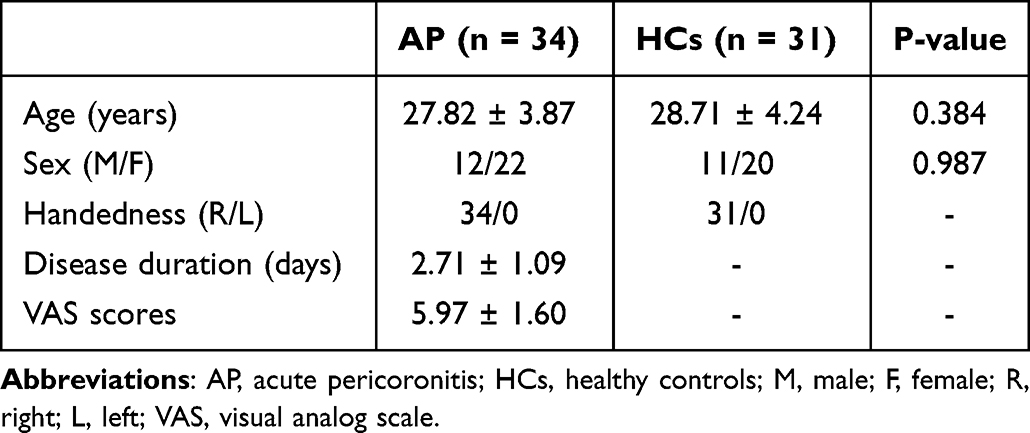 |
Table 1 Demographic and Clinical Characteristics of All Subjects |
ALFF Analysis in Different Frequency Bands
In the typical band, compared with the HC group, the brain regions with higher ALFF values in subjects in the AP group were the left superior occipital gyrus, left insula, left inferior parietal lobule, left posterior cerebellar lobe, and right postcentral gyrus (Table 2 and Figure 1). In the slow-4 band, as compared with the HC group, the brain regions with elevated ALFF values in the AP group included the left superior occipital gyrus, the right superior occipital gyrus, and the right middle occipital gyrus, while the brain regions with decreased ALFF values included the right fusiform gyrus and the right superior temporal gyrus (Table 2 and Figure 2). In the slow-5 band, the brain regions with elevated ALFF values in subjects in the AP group as compared with the HC group were the left insula and the left superior occipital gyrus (Table 2 and Figure 3).
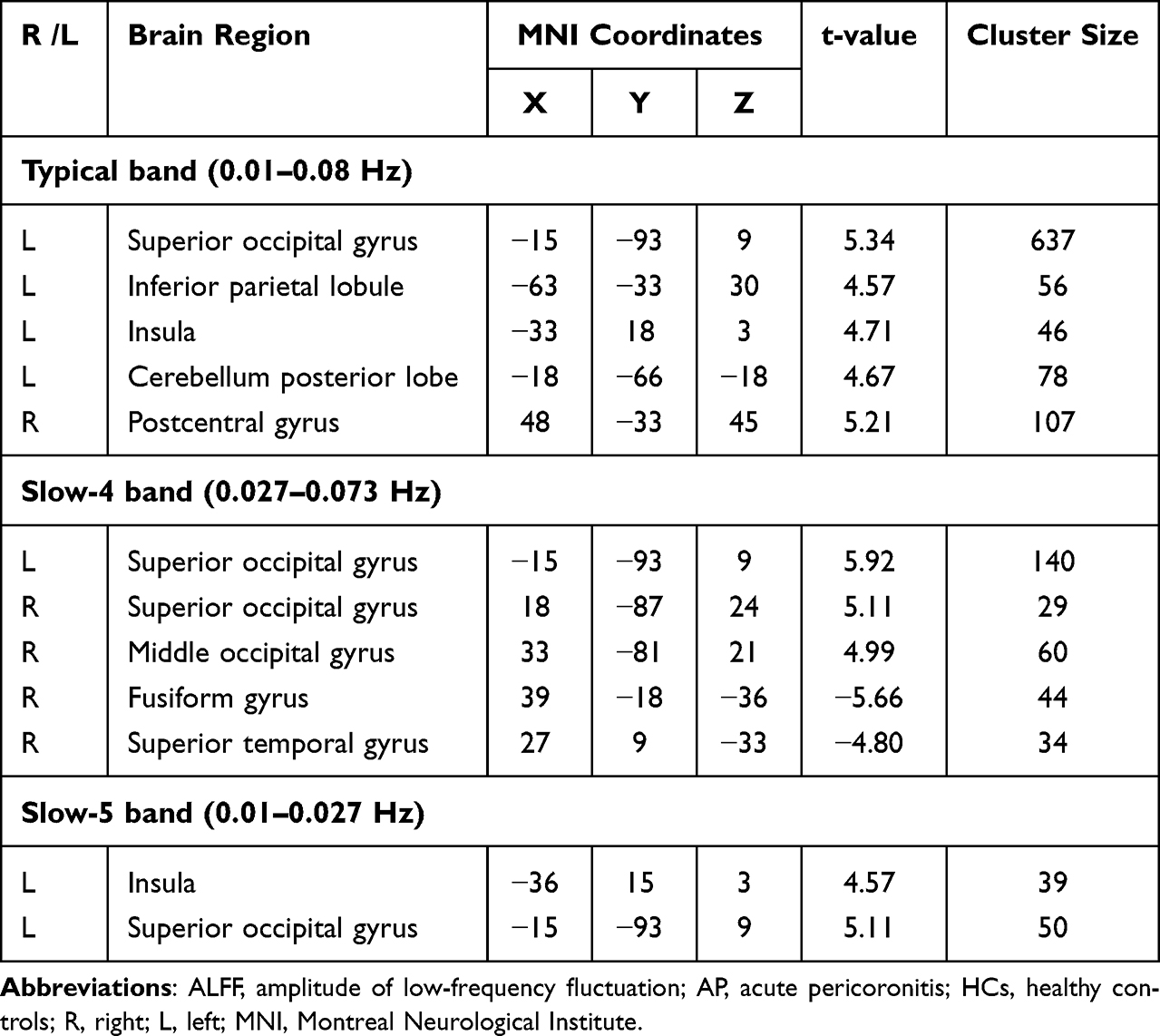 |
Table 2 The ALFF Difference in Each Frequency Band Between AP and HCs |
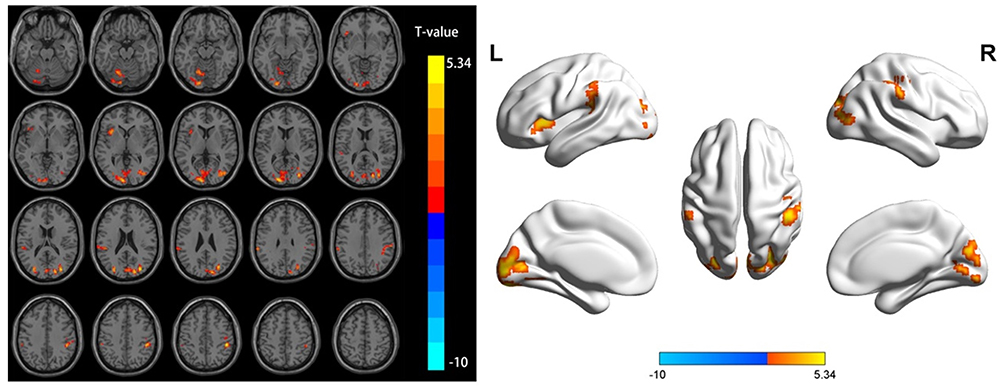 |
Figure 1 Differential brain regions of ALFF in the typical band between the AP and HC groups. Abbreviations: ALFF, amplitude of low-frequency fluctuation; AP, acute pericoronitis; HCs, healthy controls. |
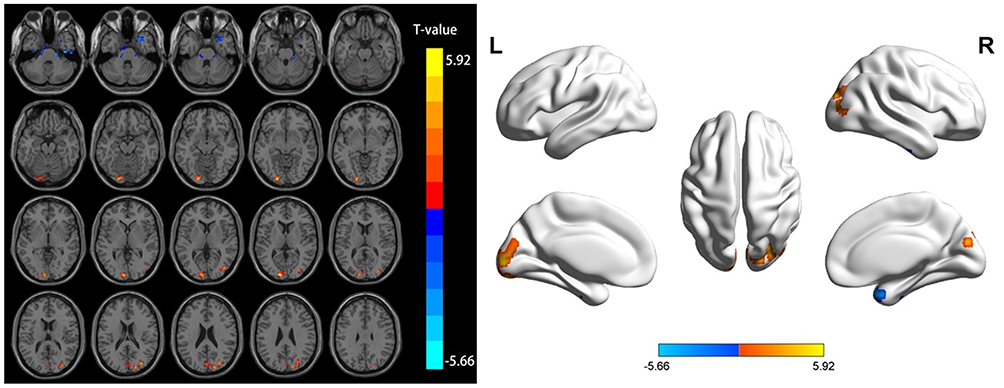 |
Figure 2 Differential brain regions of ALFF in the slow-4 band between the AP and HC groups. Abbreviations: ALFF, amplitude of low-frequency fluctuation; AP, acute pericoronitis; HCs, healthy controls. |
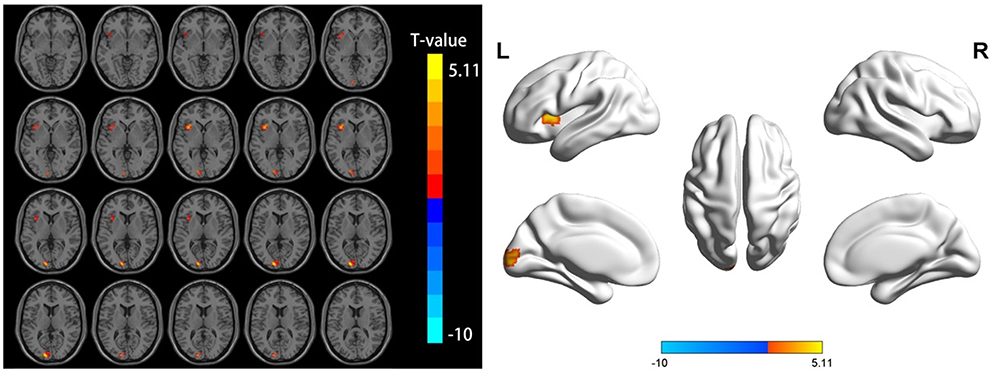 |
Figure 3 Differential brain regions of ALFF in the slow-5 band between the AP and HC groups. Abbreviations: ALFF, amplitude of low-frequency fluctuation; AP, acute pericoronitis; HCs, healthy controls. |
Correlation Analysis
The correlation between ALFF values and VAS scores in abnormally active brain regions in the typical band, slow-4 band, and slow-5 band was analyzed separately. In the typical band, ALFF values in the left insula, left inferior parietal lobule, and right postcentral gyrus of the AP group were negatively correlated with VAS scores (Table 3 and Figure 4A-C). In the slow-4 band, ALFF values in the right mid-occipital gyrus of the AP group correlated positively with VAS pain scores (Table 3 and Figure 4D). In the slow-5 band, ALFF values in the left insula of the AP group correlated negatively with VAS pain scores (Table 3 and Figure 4E). No significant correlation was seen between ALFF values and VAS scores in the remaining abnormally active brain regions in AP patients (P > 0.05).
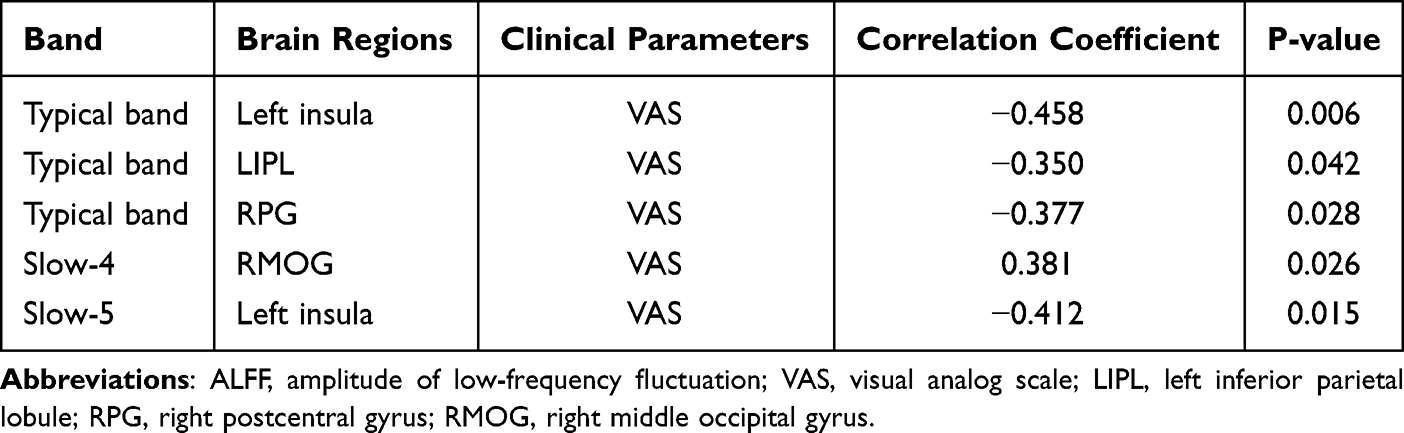 |
Table 3 Correlation Analysis Between ALFF Values and VAS Scores |
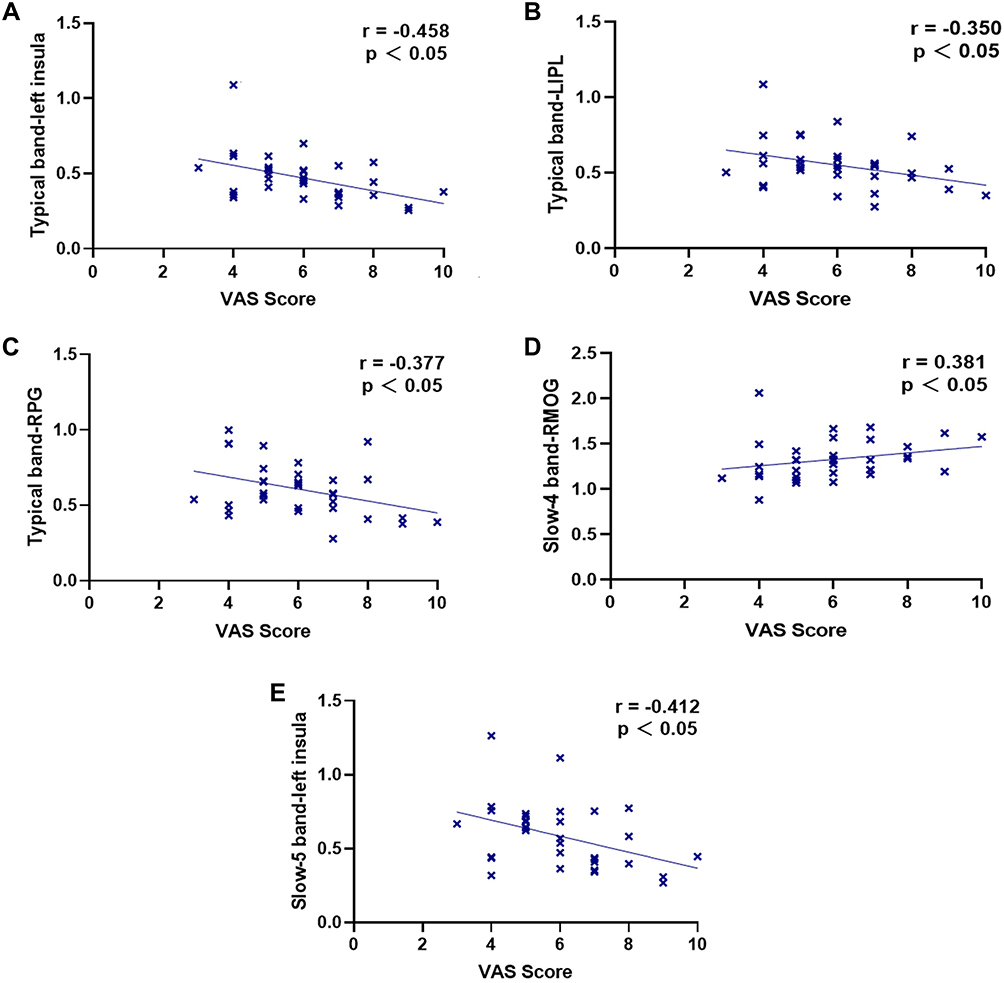 |
Figure 4 Correlation analysis between ALFF values and VAS scores in abnormally active brain regions in the AP group. (A‒C) Typical band; (D) Slow-4 band; (E) Slow-5 band. Abbreviations: ALFF, amplitude of low-frequency fluctuation; VAS, visual analog scale; LIPL, left inferior parietal lobule; RPG, right postcentral gyrus; RMOG, right middle occipital gyrus. |
Discussion
Pain is an unpleasant subjective sensation. The experience of pain signals the organism to respond to an injury. Pain is mainly composed of sensory discrimination, emotional motivation, and cognitive evaluation, and is characterized by diversity and complexity.20 As a common pain in the oral and maxillofacial region, toothache caused by AP negatively affects patients’ mood, mental health, and quality of life. Our findings suggest that dysfunction of several brain regions in the resting state exists in AP patients, and also provide some references and directions for studying the role of the central nervous system in the pathogenesis of AP dental pain.
Differential ALFF Values Between Groups in the Typical Band
In the typical band (0.01–0.08 Hz), the AP group had higher ALFF values than those of the HC group in the left insula, left superior occipital gyrus, left inferior parietal lobule, left posterior cerebellar lobule, and right postcentral gyrus.
The postcentral gyrus belongs to the primary somatosensory cortices (S1) and its main role is to receive information about injurious stimuli from the thalamus and produce nociception.21 S1, S2, the insula, anterior cingulate cortex, thalamus, prefrontal, amygdala, and parietal regions together constitute the “pain matrix”, and each of these brain regions plays a different role in the perception and experience of pain.22 It has been shown that S1, S2, and the insula are mainly involved in primary processing of pain, including the perception of the site, nature, and intensity of pain, with S1 being activated first.23 In previous resting-state fMRI studies of patients with chronic toothache,10 ALFF values in the postcentral gyrus were shown to be significantly elevated, similar to the results of the present study, further demonstrating that toothache can raise the activity of S1. In fMRI studies of acute experimental pain, the insular cortex is the most frequently activated brain region, with multiple cognitive, emotional, and sensory properties.24 The insula is divided into anterior and posterior parts, with the anterior and posterior insula having different functions in pain perception. The anterior insula belongs to the medial pain system and is mainly related to the cognitive‒emotional aspects of pain, whereas the posterior insula belongs to the lateral pain system and is mainly related to the sensory discrimination processing of pain.25 The insula serves as a critical node in the pain matrix, is involved in encoding the intensity of painful stimuli, and leads to the generation of subjective pain. The increased ALFF values in the left insula and right postcentral gyrus of AP patients in this study demonstrated that acute dental pain activated brain regions associated with the pain matrix and facilitated the transmission of the upstream pain pathway.
The superior occipital gyrus is one of the major regions of the occipital lobe and belongs to the higher visual cortex, which is involved in the regulation of neural functions, such as memory, language, and attention, in addition to visual coding.26 In a stimulated toothache trial, researchers found that stimulated dental pain produced an increase in BOLD signals in specific areas of the cerebrum, including S1, the higher visual cortex, and supplementary motor areas.8 In the present study, we found increased ALFF values in the left superior occipital gyrus of AP patients, indicating that the visual cortex was activated in patients with AP toothache, presumably as a compensatory effect of the organism in response to the injury.
The inferior parietal lobule is part of the default mode network (DMN), which encodes incoming somatosensory information and integrates multiple sensory information, such as pain, touch, vision, and hearing.27 The DMN is a functional network, which is active in the resting state. Its main role is to integrate cognition and self-instruction and monitor the internal environment of the organism. It is not involved in the monitoring of the external environment. Thus, the function of the DMN is to ensure that the organism maintains a certain level of cognition and attention.28 Tang et al showed that the DMN network was activated in patients with acute ocular pain, mainly in the form of increased ReHo values in the precuneus and inferior parietal lobule neurons.29 We hypothesized that altered brain activity in patients with acute pain at rest causes the DMN to become dysfunctional. The elevated ALFF values in the left inferior parietal lobule of the AP patients in this study, to some extent, indicate DMN dysfunction in AP patients, which could lead to clinical symptoms of reduced attention, such as anxiety, depression, and difficulty in falling asleep.
The cerebellum is involved in processing somatosensory‒motor and cognitive‒emotional information and is anatomically and functionally linked to the cerebral cortex and limbic system.30 The cerebellum is closely linked to the “pain matrix”, receives afferent signals from peripheral injurious pathways, is involved in the processing and transmission of nociceptive and negative emotional stimuli. It is also involved in pain anticipation and injury prevention avoidance responses.31 Zhang et al showed a significant increase in cerebellar ALFF values in patients with acute low back pain, suggesting that the cerebellum may be involved in the transmission of downstream pain pathways.32 When there are abnormalities in the function of the cerebellum, the processing and encoding of emotions and nociception are impaired. The increased ALFF values in the left posterior cerebellar lobe of AP patients in this study may be due to the increased cerebellar anticipation of pain caused by the persistent pain.
Frequency-Dependent Alterations in ALFF in AP Patients
In the slow-4 band, the AP group showed significantly higher ALFF values in the left superior occipital gyrus, right superior occipital gyrus, and right middle occipital gyrus, and lower ALFF values in the right fusiform gyrus and right superior temporal gyrus. The fusiform gyrus is associated with multisensory integration and categorical recognition functions, and is an integrative area involved in perceptual retrieval procedures.33 In studies of migraine34 and trigeminal neuralgia,35 the patient group showed a reduction in cortical volume of the fusiform gyrus as compared to a control group. The above studies suggested that long-term chronic pain may cause impaired function and structure of the fusiform gyrus. The reduced ALFF values in the right fusiform gyrus of the AP patients in this study were contrary to the findings in chronic pain. We speculate that the reduced spontaneous activity of the fusiform gyrus in response to acute painful stimuli may be a short-term compensatory response of the organism to external stimuli.
The temporal lobe is involved in the perception of emotions and is capable of secondary processing of pain. It has been shown that the lateral temporal lobe has an emotion-regulation function, while the medial temporal lobe is involved in pain perception and its regulation.36 The reduced ALFF values of the right superior temporal gyrus in AP patients in this study suggested impaired superior temporal gyrus function, and may be related to the generation of negativistic emotions in AP patients. In contrast, a significant increase in spontaneous activity in the occipital lobe was generally consistent with the typical frequency band results, indicating that the visual cortex was activated in AP patients. We hypothesized that patients experience and endure constant pain during pericoronitis attacks. This process generates various negative emotions and leads to difficulty sleeping, or even to insomnia. Thus, the brain remains awake and active, so that the visual cortex is significantly activated.
In the slow-5 band, the AP group had significantly higher ALFF values in the left insula and left supraoccipital gyrus, consistent with the results in the typical band. In a frequency banding study, we found partially bidirectional changes in ALFF values in the AP group, with increased spontaneous activity in the insula in the slow-5 band and decreased spontaneous activity in the fusiform gyrus and superior temporal gyrus in the slow-4 band, which may be more sensitive for detecting changes in brain activity in AP patients. In this study, more ALFF-abnormal brain regions were noted based on the slow-4 band than based on the slow-5 band. In a study of schizophrenia,37 extensive abnormal ALFF alterations were shown in the slow-4 band, with reduced ALFF values in the left precuneus and lingual gyrus and increased ALFF values in the left para-hippocampal gyrus. Another study of children with ADHD also showed that the slow-4 band provided additional diagnostic information.38 Therefore, we can speculate that the slow-4 band has better band-specificity, although this concept requires further study.
Correlation analysis showed that ALFF values of the left insula, left inferior parietal lobule and right postcentral gyrus in the AP group were negatively correlated with VAS scores in the typical band; in the slow-5 band, ALFF values of the left insula in the AP group were negatively correlated with VAS scores. The insula and postcentral gyrus belonged to the pain matrix and the inferior parietal lobule belonged to the DMN, and we hypothesized that continuous severe injurious stimulation might attenuate the response of the pain matrix and DMN to peripheral stimuli. In contrast, in the slow-4 band, ALFF values in the right middle occipital gyrus of the AP group were positively correlated with VAS scores, and occipital cortex is involved in visual processing and sensory integration. Therefore, we hypothesized that an increase in pain intensity played a dominant role in the activation of occipital cortex. In the clinical situation we found that persistent pain leads to anxiety, irritability, insomnia and even depression, which further corroborates that pain stimulates the visual cortex.
Limitation
Some limitations still remained in this study, which should be addressed in future studies. First, the sample size was small and should be expanded in future to improve the accuracy of the experimental results. Second, the current study was a cross-sectional study. In future, longitudinal changes in brain function in AP patients, during the acute episode versus after wisdom teeth removal, should be studied.
Conclusion
The present study showed that AP patients have functional abnormalities in several brain regions in the resting state, mainly involving different dimensions of pain processing, such as nociceptive discrimination, cognition, emotion, and visual processing. This suggests that AP patients may have central dysfunction and functional reorganization. In our frequency-dependent study, the various frequency bands showed differences in the brain regions that were abnormally active in AP patients, suggesting frequency-dependent spontaneous brain activity in AP patients, and providing new insights into the neurophysiological mechanisms of AP, which can form the basis for further exploration.
Acknowledgments
This study was supported by the Science and Technology Department Project of Jiangxi Province (Grant No.20202BBGL73122), and Postgraduate Innovation Special Fund Project of Jiangxi Province (Grant No. YC2020-S136).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Singh P, Nath P, Bindra S, Rao S, Reddy K. The predictivity of mandibular third molar position as a risk indicator for pericoronitis: a prospective study. Natl J Maxillofac Surg. 2018;9(2):215–221.
2. Miranda-Rius J, Brunet-Llobet L, Lahor-Soler E. The periodontium as a potential cause of orofacial pain: a comprehensive review. Open Dent J. 2018;12:520–528.
3. Coimbra F, Coimbra A. Dental noxious input reaches the subnucleus caudalis of the trigeminal complex in the rat, as shown by c-fos expression upon thermal or mechanical stimulation. Neurosci Lett. 1994;173:201–204.
4. Kato J, Svensson C. Role of extracellular damage-associated molecular pattern molecules (DAMPs) as mediators of persistent pain. Prog Mol Biol Transl Sci. 2015;131:251–279.
5. Shibukawa Y, Sato M, Kimura M, et al. Odontoblasts as sensory receptors: transient receptor potential channels, pannexin-1, and ionotropic ATP receptors mediate intercellular odontoblast-neuron signal transduction. Pflugers Arch. 2015;467(4):843–863.
6. Ettlin D, Brügger M, Keller T, et al. Interindividual differences in the perception of dental stimulation and related brain activity. Eur J Oral Sci. 2009;117(1):27–33.
7. Brügger M, Ettlin D, Meier M, et al. Taking Sides with Pain - Lateralization aspects Related to Cerebral Processing of Dental Pain. Front Hum Neurosci. 2011;5:12.
8. Brügger M, Lutz K, Brönnimann B, et al. Tracing toothache intensity in the brain. J Dent Res. 2012;91(2):156–160.
9. Upadhyay J, Granitzka J, Bauermann T, et al. Detection of central circuits implicated in the formation of novel pain memories. J Pain Res. 2016;9:671–681.
10. Yang J, Li B, Yu Q, et al. Altered intrinsic brain activity in patients with toothaches using the amplitude of low-frequency fluctuations: a resting-state fMRI study. Neuropsychiatr Dis Treat. 2019;15:283–291.
11. Wu S, Zhang M, Shu H, et al. Changes in functional connectivity of specific cerebral regions in patients with toothache: a resting-state functional magnetic resonance imaging study. Dis Markers. 2020;2020:6683161.
12. Zang Y, He Y, Zhu C, et al. Altered baseline brain activity in children with ADHD revealed by resting-state functional MRI. Brain Dev. 2007;29(2):83–91.
13. Xue T, Yuan K, Cheng P, et al. Alterations of regional spontaneous neuronal activity and corresponding brain circuit changes during resting state in migraine without aura. NMR Biomed. 2013;26(9):1051–1058.
14. Pan Z, Li H, Bao J, et al. Altered intrinsic brain activities in patients with acute eye pain using amplitude of low-frequency fluctuation: a resting-state fMRI study. Neuropsychiatr Dis Treat. 2018;14:251–257.
15. Ma X, Li S, Tian J, et al. Altered brain spontaneous activity and connectivity network in irritable bowel syndrome patients: a resting-state fMRI study. Clin Neurophysiol. 2015;126(6):1190–1197.
16. Zuo X, Di Martino A, Kelly C, et al. The oscillating brain: complex and reliable. NeuroImage. 2010;49(2):1432–1445.
17. Gu L, Hong S, Jiang J, et al. Bidirectional alterations in ALFF across slow-5 and slow-4 frequencies in the brains of postherpetic neuralgia patients. J Pain Res. 2019;12:39–47.
18. Zhang Y, Mao Z, Pan L, et al. Frequency-specific alterations in cortical rhythms and functional connectivity in trigeminal neuralgia. Brain Imaging Behav. 2019;13(6):1497–1509.
19. Yan C, Wang X, Zuo X, Zang Y. DPABI: data Processing & Analysis for (Resting-State) Brain Imaging. Neuroinformatics. 2016;14(3):339–351.
20. Seifert F, Maihöfner C. Functional and structural imaging of pain-induced neuroplasticity. Curr Opin Anaesthesiol. 2011;24(5):515–523.
21. Bingel U, Lorenz J, Glauche V, et al. Somatotopic organization of human somatosensory cortices for pain: a single trial fMRI study. NeuroImage. 2004;23(1):224–232.
22. Mouraux A, Diukova A, Lee M, Wise R, Iannetti G. A multisensory investigation of the functional significance of the “pain matrix”. NeuroImage. 2011;54(3):2237–2249.
23. Kakigi R, Inui K, Tran D, et al. Human brain processing and central mechanisms of pain as observed by electro- and magneto-encephalography. J Chin Med Assoc. 2004;67(8):377–386.
24. Apkarian AV, Bushnell MC, Treede RD, Zubieta JK. Human brain mechanisms of pain perception and regulation in health and disease. Eur J Pain. 2005;9(4):463–484.
25. Wiech K, Jbabdi S, Lin C, Andersson J, Tracey I. Differential structural and resting state connectivity between insular subdivisions and other pain-related brain regions. Pain. 2014;155(10):2047–2055.
26. Chen B, Fan G, Liu H, Wang S. Changes in anatomical and functional connectivity of Parkinson’s disease patients according to cognitive status. Eur J Radiol. 2015;84(7):1318–1324.
27. Caspers S, Geyer S, Schleicher A, Mohlberg H, Amunts K, Zilles K. The human inferior parietal cortex: cytoarchitectonic parcellation and interindividual variability. NeuroImage. 2006;33(2):430–448.
28. Raichle M, Snyder A. A default mode of brain function: a brief history of an evolving idea. NeuroImage. 2007;37(4):1083–1090.
29. Tang L, Li H, Huang X, et al. Assessment of synchronous neural activities revealed by regional homogeneity in individuals with acute eye pain: a resting-state functional magnetic resonance imaging study. J Pain Res. 2018;11:843–850.
30. Stoodley C. The cerebellum and cognition: evidence from functional imaging studies. Cerebellum. 2012;11(2):352–365.
31. Garcia-Larrea L, Peyron R. Pain matrices and neuropathic pain matrices: a review. Pain. 2013:2;S29–S43.
32. Zhang S, Wu W, Yang J, Wang C. Abnormal spontaneous brain activity in acute low-back pain revealed by resting-state functional MRI. Am J Phys Med Rehabil. 2017;96(4):253–259.
33. Ter Minassian A, Ricalens E, Humbert S, Duc F, Aubé C, Beydon L. Dissociating anticipation from perception: acute pain activates default mode network. Hum Brain Mapp. 2013;34(9):2228–2243.
34. Schwedt T, Chong C, Chiang C, Baxter L, Schlaggar B, Dodick D. Enhanced pain-induced activity of pain-processing regions in a case-control study of episodic migraine. Cephalalgia. 2014;34(12):947–958.
35. Parise M, Kubo T, Doring T, Tukamoto G, Vincent M, Gasparetto E. Cuneus and fusiform cortices thickness is reduced in trigeminal neuralgia. J Headache Pain. 2014;15:17.
36. Ploner M, Lee M, Wiech K, Bingel U, Tracey I. Flexible cerebral connectivity patterns subserve contextual modulations of pain. Cerebral Cortex. 2011;21(3):719–726.
37. Hoptman M, Zuo X, Butler P, et al. Amplitude of low-frequency oscillations in schizophrenia: a resting state fMRI study. Schizophr Res. 2010;117(1):13–20.
38. Di Martino A, Ghaffari M, Curchack J, et al. Decomposing intra-subject variability in children with attention-deficit/hyperactivity disorder. Biol Psychiatry. 2008;64(7):607–614.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.