Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 10 » Issue 1
Frequency and risk factors of COPD exacerbations and hospitalizations: a nationwide study in Greece (Greek Obstructive Lung Disease Epidemiology and health ecoNomics: GOLDEN study)
Authors Alexopoulos E, Malli F, Mitsiki E, Bania E, Varounis C, Gourgoulianis K
Received 29 June 2015
Accepted for publication 7 November 2015
Published 11 December 2015 Volume 2015:10(1) Pages 2665—2674
DOI https://doi.org/10.2147/COPD.S91392
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Evangelos C Alexopoulos,1 Foteini Malli,2 Eirini Mitsiki,3 Eleni G Bania,2 Christos Varounis,3 Konstantinos I Gourgoulianis1
1School of Social Sciences, Hellenic Open University, Patras, 2Respiratory Medicine Department, University of Thessaly Medical School, University Hospital of Larissa, Larissa, 3Medical Department, Novartis Hellas, Athens, Greece
Background: COPD exacerbations and hospitalizations have been associated with poor prognosis for the COPD patient.
Objective: To evaluate the frequency and risk factors of COPD exacerbations, hospitalizations, and admissions to intensive care units (ICUs) in Greece by a nationwide cross-sectional study.
Materials and methods: A nationwide observational, multicenter, cross-sectional study was conducted in the clinical practice setting of respiratory medicine physicians over a 6 month-period (October 2010 to March 2011). A total of 6,125 COPD patients were recruited by 199 respiratory physicians.
Results: Participants had a median age of 68.0 years, 71.3% were males, and 71.8% suffered from comorbidities. The median disease duration was 10.0 years. Of the patients, 45.3% were classified as having GOLD (Global initiative for chronic Obstructive Lung Disease) stage III or IV COPD. Patients with four or more comorbidities had 78.5% and threefold-higher than expected number of exacerbations and hospitalizations, respectively, as well as fivefold-higher risk of admission to the ICU compared to those with no comorbidities. Obese patients had 6.2% fewer expected exacerbations compared to those with a normal body mass index. Patients with GOLD stage IV had 74.5% and fivefold-higher expected number of exacerbations and hospitalizations, respectively, and nearly threefold-higher risk of admission to the ICU compared to stage I patients. An additional risk factor for exacerbations and hospitalizations was low compliance with treatment: 45% of patients reported forgetting to take their medication, and 81% reported a preference for a treatment with a lower dosing frequency.
Conclusion: Comorbidities, disease severity, and compliance with treatment were identified as the most notable risk factors for exacerbations, hospitalizations, and ICU admissions. The results point to the need for a multifactorial approach for the COPD patient and for the development of strategies that can increase patient compliance with treatment.
Keywords: COPD, exacerbations, hospitalizations, ICU admissions, risk factors
Introduction
COPD is a multicomponent disease characterized by lung inflammation, airflow limitation, and gradual loss of lung function. COPD is estimated to become the fifth-leading cause of years lost through early mortality or handicap (disability-adjusted life years) by 2020,1 while according to World Health Organization estimates it is predicted to become the third-leading cause of global mortality by the year 2030.2 Projected increases in the burden of COPD are attributed to a worldwide aging population (COPD incidence remains high in the elderly) and increased prevalence of COPD risk factors.3,4 COPD prevalence in Greece is estimated to be around 8.4% in those aged >35 years with a smoking history of >100 cigarettes per lifetime,5 while a study in Northern Greece estimated the prevalence to be 5.6% among those 21–80 years of age.6 It is however noted that in Greece the rate of undiagnosed COPD patients is very high.7
COPD exacerbations are defined as events of acute onset, characterized by worsening in respiratory symptoms beyond the day-to-day variations and that may warrant a change in regular medication of the COPD patient.8 They have been associated with decreases in the patients’ quality of life, increased rate of decline of lung function, increased health care-resource utilization, and socioeconomic burden.8–10 Notably, the best predictor of a subsequent exacerbation appears to be the occurrence of a previous exacerbation, with evidence pointing to a phenotype that is highly susceptible to exacerbations.11,12 Moreover, increased disease severity has been linked with an increased frequency of exacerbations12,13 and an increased risk of death following hospitalization.14 The frequency of hospitalizations due to COPD appears to be amplified by the presence of comorbid conditions.15 Hospitalizations due to COPD exacerbations16,17 and increased number of exacerbations are associated with increased mortality risk.14
The economic burden of the disease increases with increasing disease severity, but is substantially augmented by exacerbations and hospitalizations, and especially with admissions to intensive care units (ICUs).18,19 A study conducted in northern Greece has estimated that the cost per severe COPD exacerbation is €1,711 and is dependent on the severity of the disease, ranging from €1,357 for GOLD (Global initiative for chronic Obstructive Lung Disease) stage to €2,614 for GOLD stage IV.19 The observed higher cost per exacerbation in the very severe COPD stage is mainly attributed to the additional cost of ICU admissions.19
These findings underscore the importance of reducing the frequency of COPD exacerbations and hospitalizations. Moreover, identification of potential factors associated with the frequency of exacerbations and hospitalizations may assist in alleviating not only the patients’ burden but also the societal and economic burden of exacerbations and hospitalizations. In light of this, the present study aimed at collecting data from a large population in Greece with regard to the frequency of exacerbations, hospitalizations, and ICU admissions, as well as the length of hospital stay. Moreover, the study examined the factors associated with all the aforementioned measures.
Materials and methods
Study design and setting
GOLDEN was a nationwide, observational, multicenter, cross-sectional study conducted over a 6-month period (October 2010 to March 2011) in Greece. The study design has been described previously in Papaioannou et al.20 In brief, the study followed a nationwide sampling approach of respiratory medicine physicians across each of the 52 prefectures of Greece. All physicians were sampled at a single time point. In total, 218 respiratory care physicians expressed interest, and 199 (124 private practitioners and 75 hospital-based physicians) participated in the study, recruiting 6,125 patients. The pool of pulmonologists in Greece approximates 1,800. Therefore, the sample of pulmonologists that participated in the study represents approximately 11% of the total pool of the specialty. Physicians were asked to register all COPD patients consecutively visiting their office/clinic during the 6-month period.
The respiratory health care system in Greece is comprised of three levels of care: 1) primary care offered by general practitioners and private practice doctors; 2) secondary care offered by general hospitals, which includes treatment in the emergency department and inpatient care; and 3) tertiary hospitals, usually university hospitals, which provide more specialized care, such as intermediate care units and ICUs. Participating physicians were recruited from all three levels of respiratory care.
Data collected were recorded on case-report forms. Data captured included sociodemographic characteristics, smoking history, vital signs, blood gases, COPD characteristics (GOLD stage,21 disease duration, and medical treatment, including compliance), comorbidities, presence and type of respiratory failure, and exacerbation characteristics (frequency per year and hospitalizations, including duration and ICU admissions), work absenteeism and retirement due to COPD.
The study was conducted under real-life conditions of daily clinical practice and in accordance with ethical principles that have their origin in the Declaration of Helsinki (ICH-GCP guidelines) and all applicable EU and local laws and regulations. The study received approval by the ethics committees of all participating hospital sites and the Greek National Organization of Medicines.
Subjects
For enrollment in the study, patients needed to meet the following criteria: age greater than 40 years, COPD diagnosis according to the GOLD criteria,21 and available medical history. Patients were excluded from the study if they had a history of asthma or had participated in a similar study during the month preceding study enrollment. All patients were informed about the nature of the study and signed the informed consent form prior to any study-related procedures.
Definitions of study measurements
According to their smoking history, subjects were classified into three categories: never-smokers, ex-smokers, and current smokers. Ex-smokers were defined as smokers who had quit smoking for at least 12 months. Smoking history was measured by pack-years, defined as the number of cigarettes smoked per day divided by 20 and multiplied by the number of years of smoking.
Compliance with therapy was assessed via selection of one of five predefined options on the case report form according to the patient’s report, indicating the level of compliance with COPD prescribed medication: never/practically never, once/twice a month, once a week, more than once a week, and almost daily.
Pre- and postbronchodilation (ie, 30 minutes after the administration of 400 μg salbutamol with a spacer), spirometry measurements were performed in all study subjects, and forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and FEV1/FVC ratio were recorded. Postbronchodilation values were used for the evaluation of COPD severity, according to 2010 GOLD guidelines.21
Study objectives
The primary objective of the GOLDEN study was to record characteristics of COPD patients distributed across Greece in terms of disease severity and therapeutic management. Secondary objectives included the description of the burden of COPD in females vs males, as well as sex differences regarding functional characteristics, smoking habits, and frequency of exacerbations, which have been described in Papaioannou et al,20 and the estimation of the incidence of newly diagnosed COPD patients in Greece. Herein, data regarding exacerbation frequency, frequency of hospitalizations, and ICU admissions due to COPD exacerbations, as well as factors influencing the frequency of exacerbations, hospitalizations, ICU admissions, and length of hospitalizations are presented.
Statistical methods
For description of the qualitative variables, absolute (number of observations) and relative frequencies (percentages) were used. The description of the quantitative variables was based on the calculation of the median and interquartile range (IQR). Descriptive statistics were undertaken on patients with available data.
For the analysis of the number of exacerbations in the preceding year, hospitalizations (per year), days of hospitalization per exacerbation, and days of hospitalization in ICU, zero-inflated Poisson regressions were applied. The use of zero-inflated Poisson regression instead of the familiar Poisson regression is justified by the high number of zero values in our data. This choice was documented using a Vuong statistical test.22 For analysis of the factors associated with admission to the ICU, logistic regression was applied. All regression analyses were based on data from a sample size of 6,114 patients.
Results
Subject characteristics
Participating patients had a median age of 68.0 (IQR 60.0–75.0) years and a median body mass index (BMI) of 27.5 (IQR 24.9–30.6) kg/m2. The majority of the patients were male (71.3%). Regarding the patients’ smoking status, 10.2% were never-smokers, 42.0% were ex-smokers, and 47.8% were current smokers (Table 1).
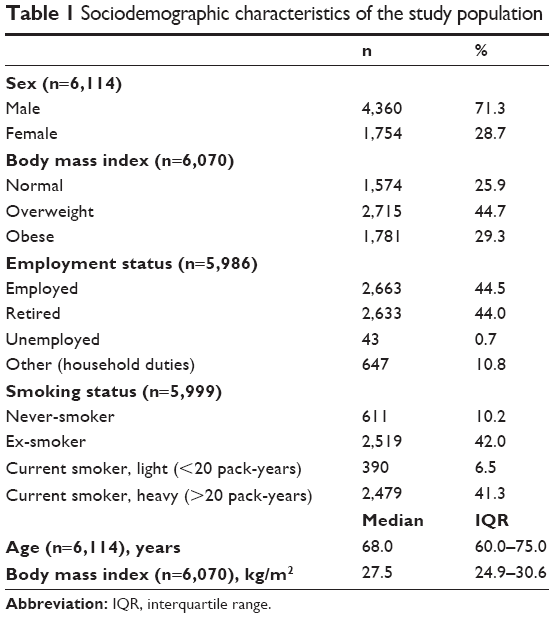 | Table 1 Sociodemographic characteristics of the study population |
More than half (54.7%) were classified as GOLD stage I or II, ie, with mild-to-moderate COPD. A total of 18.0% had been newly diagnosed. The median time since diagnosis was 10.0 (IQR 5.0–15.0) years. Most patients (71.8%) suffered from comorbid diseases, with 26.1% having one, 23.8% having two, 16.4% having three, and the remaining 15.6% having four or more comorbidities (Table 2). The most commonly reported comorbidities were hypertension (55.3%), diabetes (20.6%), heart failure (19.4%), and gastroesophageal reflux (15.3%).
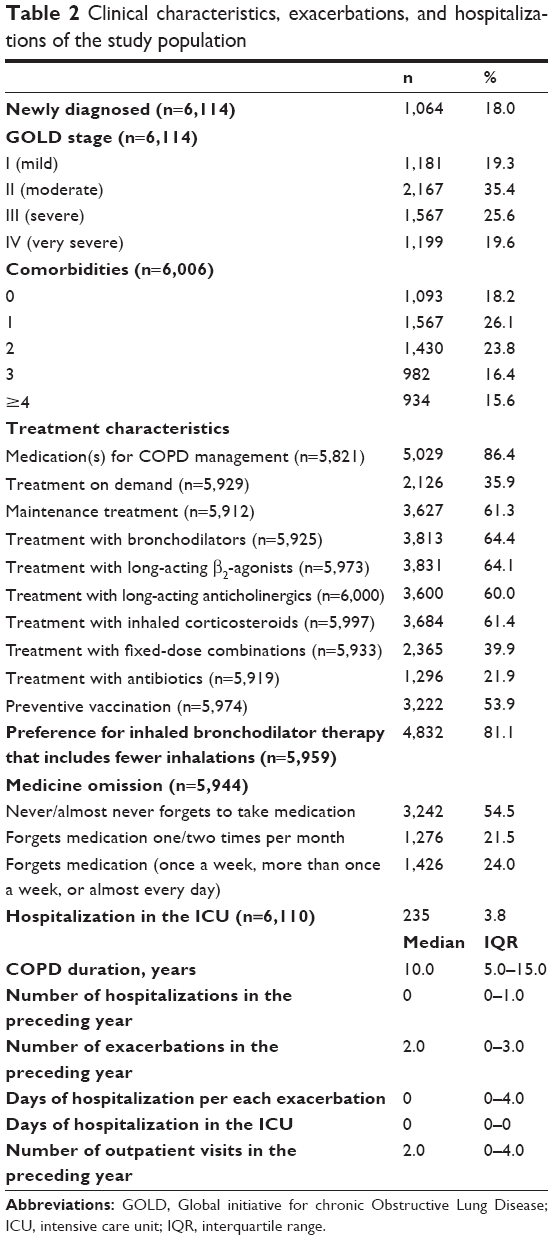 | Table 2 Clinical characteristics, exacerbations, and hospitalizations of the study population |
Of the patients recruited, 86.4% were receiving treatment for disease management. Approximately 36% reported receiving treatment on demand, 61.3% reported receiving maintenance treatment, and 2.8% did not fit either of the two groups. Approximately 60% of the total number of patients recruited were treated with a long-acting β2-agonist, a long-acting anticholinergic, or an inhaled corticosteroid alone or in combination. Antibiotics as prophylactic treatment were used by 22% of the patient population, and preventative vaccination was recorded for 54% of the study population. Approximately 45% of the patients reported forgetting to take their medication at least once a month, of which only 8% reported forgetting to take their medication once per week. Regarding the inhaled bronchodilator therapy, patients reported preference (by 81%) for a therapy with fewer daily inhalations.
In the preceding year, patients had experienced a median of two exacerbations (IQR 0–3). The IQR for hospitalizations was 0–1, while the IQR of the number of days of hospitalizations for each exacerbation was 0–4. Details on the therapeutic management are provided in Table 2.
Risk factors associated with exacerbations in the previous year
Multivariate analysis was performed to examine the factors associated with the number of exacerbations during the preceding year (Table 3). Patients aged 61–75 and ≥76 years had 13.7% (P<0.001) and 19% (P<0.001) fewer exacerbations, respectively, in the preceding year compared to those aged up to 60 years. Obese patients had 6.2% fewer exacerbations compared to those with a normal BMI (P=0.044, Table 3). Moreover, increased time since COPD diagnosis increased the number of exacerbations, as evident from higher incidence-rate ratio in both the 6–10 and ≥11 years since COPD diagnosis groups compared to those with ≤5 years since diagnosis (P<0.001 for both).
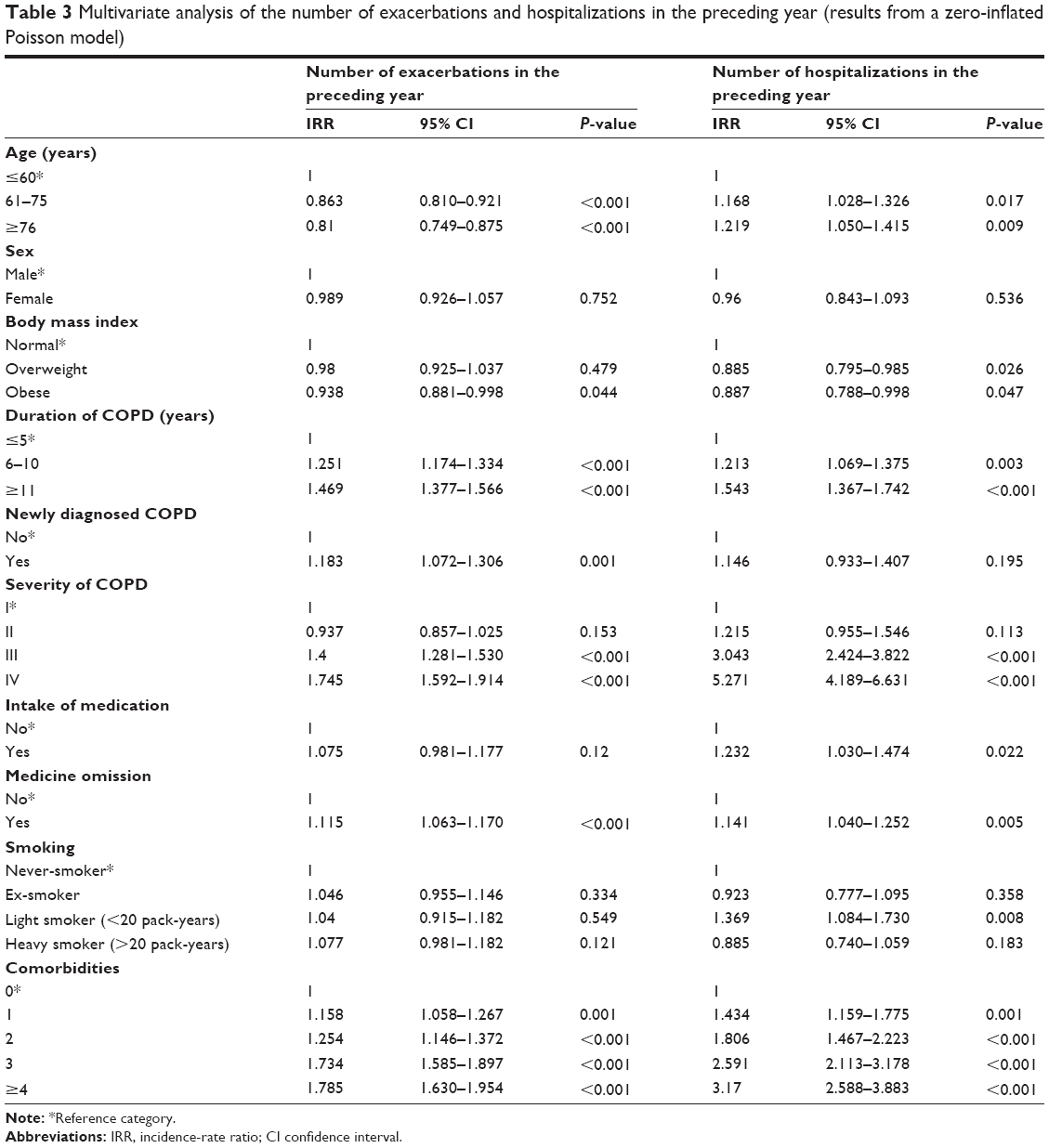 | Table 3 Multivariate analysis of the number of exacerbations and hospitalizations in the preceding year (results from a zero-inflated Poisson model) |
Notably, increased severity of COPD as defined by GOLD staging based on severity of airflow limitation was associated with an increased number of exacerbations. Specifically, compared to patients with GOLD stage I, those with GOLD stage III and IV had a greater number of exacerbations in the preceding year by 40% (P<0.001) and 74.5% (P<0.001), respectively. A similar trend was observed with increases in the number of comorbidities. Specifically, those with one, two, three, and four or more comorbidities had an increased number of exacerbations by 15.8%, 25.4%, 73.4%, and 78.5%, respectively, compared to those without comorbidities (all P<0.001). Medication omission was also positively associated with increased number of exacerbations, with those omitting their medication having 11.5% increased number of exacerbations in the preceding year compared to those who were compliant with their medication (Table 3).
Number of hospitalizations in the preceding year
According to the multivariate analysis adjusted for the covariates of the model, patients aged 61–75 years and those aged ≥76 years had 16.8% (P=0.017) and 21.9% (P=0.009), respectively, had higher expected number of hospitalizations compared to those aged up to 60 years. In addition, obese and overweight patients had an 11.5% (P=0.026) and 11.3% (P=0.047) decreased expected number of hospitalizations compared to those with a normal BMI (Table 3).
Moreover, patients with COPD duration of 6–10 years and ≥11 years had a 21.3% (P=0.003) and 54.3% (P<0.001) higher than expected number of hospitalizations per year, respectively, than those with duration up to 5 years, according to the multivariate analysis. Patients with GOLD stage III or IV had a higher expected number of hospitalizations per year (threefold [P<0.001] and 5.3-fold [P<0.001], respectively) than patients with GOLD stage I. Moreover, patients who omitted taking any medication had a 14.1% increased expected number of hospitalizations per year (P=0.005). Finally, patients with one, two, three, or four comorbidities had a 43.4% (P=0.001), 80.6% (P<0.001), 2.6-fold (P<0.001), and 3.2-fold (P<0.001) increased expected number of hospitalizations per year, respectively, than patients with no comorbidities.
Hospitalization in the intensive care unit
After the model was adjusted for the covariates, the following results were observed. Patients with a COPD diagnosis of ≥11 years had 75.5% higher odds of hospitalization in the ICU compared to patients whose disease diagnosis was up to 5 years (P=0.018). Furthermore, for patients with GOLD stage IV, the odds of hospitalization in the ICU were 2.8 times higher (P=0.002) than for patients with GOLD stage I. Additionally, for patients who omitted taking their medication, the odds of hospitalization in the ICU increased by 42.7% (P=0.043). Finally, the odds of hospitalization in the ICU were 5.5 times (P<0.001) higher in patients with four or more comorbidities than in patients with no comorbidities (Table 4).
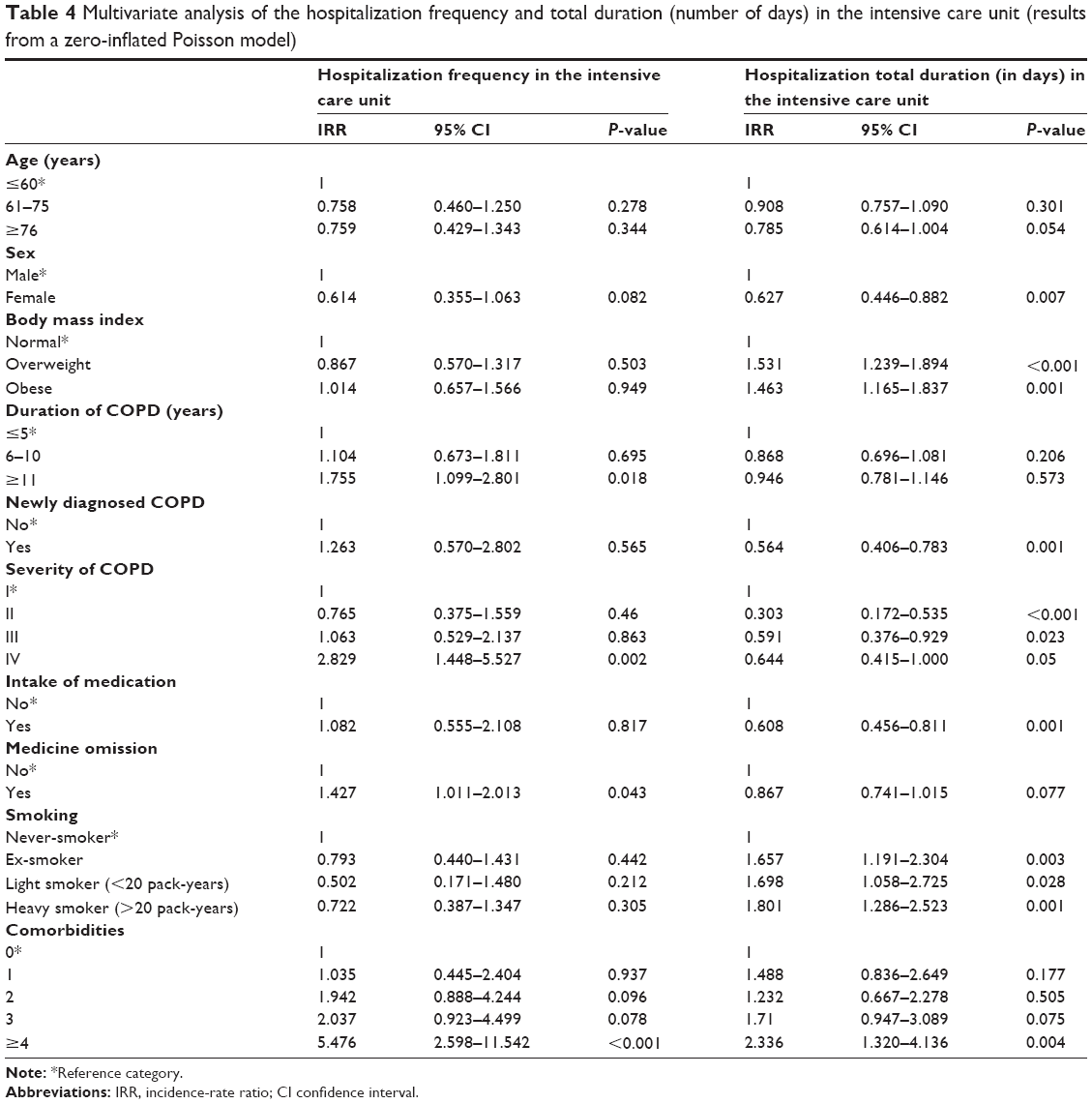 | Table 4 Multivariate analysis of the hospitalization frequency and total duration (number of days) in the intensive care unit (results from a zero-inflated Poisson model) |
Number of days of hospitalization in the intensive care unit
After we adjusted for the covariates of the model, female sex was associated with decreased expected number of days of hospitalization in the ICU by 19.4% (P=0.004) compared to males, 37.3% (P=0.007). Additionally, overweight and obese participants had increased expected number of days of hospitalization in the ICU compared to patients with normal BMI. Newly diagnosed cases had a lower expected number of days of hospitalization in the ICU by 43.6% after adjustment for covariates (P=0.001, Table 4).
According to the multivariate analysis, the expected number of days of hospitalizations in the ICU was inversely correlated with COPD-severity stage. Specifically, the expected number of days of hospitalizations in the ICU decreased by 69.7% (P<0.001), 40.8% (P=0.023), and 33.6% (P=0.05) in those with GOLD stages II, III, and IV, respectively, compared to those with GOLD stage I. In addition, current smokers had an increased expected number of days of hospitalization in the ICU, regardless of whether they were heavy or light smokers, compared to the never-smokers. Finally, patients with four or more comorbidities had an increased expected number of days of hospitalization in the ICU by 2.3-fold (P=0.004) compared to patients with no concomitant diseases (Table 4).
Number of days of hospitalization for each exacerbation
Patients aged 61–75 years had a lower expected number of days of hospitalization for each exacerbation by 7.3% (P=0.013) compared to patients aged up to 60 years. Overweight patients had a decreased expected number of days of hospitalization for each exacerbation by 6.8% (P=0.008) than patients with normal BMI. Moreover, patients with COPD duration of ≥11 years had a lower expected number of days of hospitalization for each exacerbation by 6.1% (P=0.025) than those with duration up to 5 years, after adjusting for the covariates of the model (Table 5).
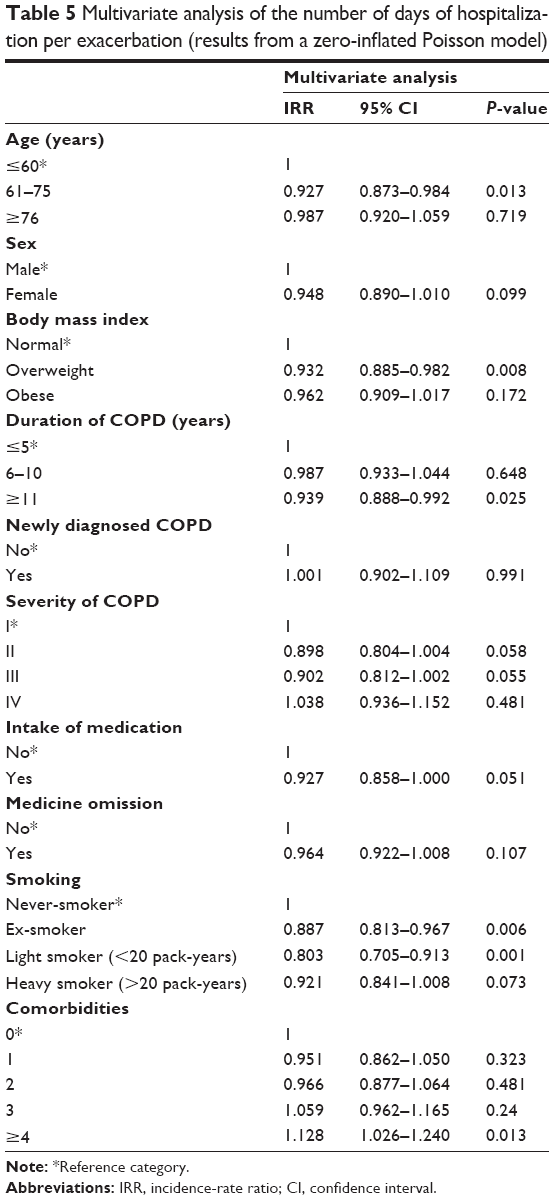 | Table 5 Multivariate analysis of the number of days of hospitalization per exacerbation (results from a zero-inflated Poisson model) |
Additionally, ex-smokers and mild smokers had a decreased expected number of days of hospitalization for each exacerbation by 11.3% (P=0.006) and 19.7% (P=0.001), respectively, than never-smokers. Patients with four or more comorbidities had an increased expected number of days of hospitalization for each exacerbation by 12.8% (P=0.013) than patients with no concomitant diseases, after adjusting for the covariates of the model (Table 5).
Discussion
The results of the present study demonstrate that disease severity (as assessed by the GOLD 2010 staging criteria)21 and presence of comorbidities are among the strongest predictors of frequencies of exacerbations, hospitalizations, and admissions to the ICU. Specifically, in regard to comorbidities, patients with three and those with four or more comorbidities had a 73.4% and 78.5% higher expected number of exacerbations, respectively, while they had a 2.6- and 3.2-fold, respectively, greater number of expected hospitalizations compared to those without any comorbid conditions. In addition, the presence of at least four comorbid conditions increased the possibility of admission to the ICU by nearly 5.5-fold compared to those with no comorbidities and doubled the expected number of days of stay in the ICU, extending the length of stay in the hospital for each exacerbation by 12.8% compared to those without any comorbidity. The impact of comorbidities on the outcomes of COPD has been extensively documented. From a practical management standpoint, there are added difficulties in the therapeutic management of the multimorbid COPD patient23 associated with increased frequency of hospitalizations, as reported in the INDACO study: the prevalence of patients with comorbidities among COPD patients being referred to pulmonology hospital units was 94.1%.24 Moreover, several studies have associated comorbidities with decreased quality of life, negative impact on the outcomes of rehabilitation and short-term prognosis following hospitalization, and increased risk of mortality.24–27 Due to comorbidities’ negative impact on the COPD patient, certain indices for their measurement have been applied. Of those, the Charlson index has been shown to be a specific indicator of mortality in patients with COPD.25 Moreover, the COTE (COPD specific cOmorbidity TEst) index was developed and proven to be applicable as a tool assessing mortality risk of the COPD patient.27
With regard to the severity of the disease, in the present study patients with GOLD stage IV compared to stage I had a higher number of expected exacerbations (by 74.5%), fivefold-higher number of expected hospitalizations, and nearly threefold-higher risk of ICU admission. Increased disease severity has been linked with an increased frequency of exacerbations12,13 and ICU admissions.19 In Geitona et al,19 the mean cost per severe COPD exacerbation in patients of northern Greece was nearly the same in patients with stage I, II, and III COPD (approximately €1,400), while it was increased by 85% in patients with stage IV disease (to approximately €2,600) as a result of increased number of ICU admissions in stage IV patients. This is especially important in light of findings indicating that a significant proportion of COPD patients in Greece experience two or more exacerbations per year and that the majority of exacerbations are moderate or severe and frequently lead to hospitalizations.28 Collectively, these findings underscore the importance of decreasing the number of exacerbations for the COPD patient, in order to alleviate the disease burden and also the economic cost of the disease. In addition, the frequent-exacerbation phenotype describing patients who are particularly susceptible to exacerbations and more likely to be readmitted to hospital needs to be taken into account in regard to strategies to manage COPD comorbidities.12 It is noteworthy that the use of inhaled corticosteroids, a therapeutic option proposed by GOLD recommendations for patients who have frequent exacerbations, was particularly high in the population recorded in the GOLDEN study, signaling that these might be patients who are possibly overtreated.
Among other important factors associated with increased number of exacerbations and hospitalizations, including ICU admissions, in the present study, was treatment compliance, with patients who omitted their medication expected to have an increased frequency of both exacerbations and hospitalizations (including to the ICU). In the present study, nearly 45% of patients reported forgetting their medication at a frequency greater than or equal to once or twice a month, in alignment with various studies suggesting that the rate of medication adherence in COPD is approximately 50%.29 Adherence in COPD is commonly influenced by such factors as patient age, cost of the drug, comorbidities, and dosing frequency.29,30 It is worth mentioning that in the present study, more than 80% of the patients noted their preference for an inhaled bronchodilator with fewer inhalations. An additional factor that needs to be taken into account is the high incidence of comorbidities in our study population (71.8% had at least one comorbid condition), which likely increased the number of medications a patient received and negatively impacted medication compliance. Additionally, the number of hospitalizations appeared to be negatively associated with age. This is possibly signifying that as recorded in this study group, older patients might have fewer exacerbations that however might be more severe (due to the longer duration of COPD or the presence of more comorbidities), leading to more hospitalizations.
Concerning treatment management of the COPD patient, it should be noted that our patient population had a median of 10 years of diagnosis, while about 18.0% were newly diagnosed (indicating that they were not receiving any COPD medications at the time of the study visit). Most were receiving maintenance treatment, as expected by a patient population with a long duration of the disease. Notably, antibiotics as prophylactic treatment were used by merely 22% of the patient population, despite the fact that the use of antibiotics has been directly associated with decreased frequency of exacerbations.31
Another interesting association is that obese and overweight patients had a lower expected number of exacerbations and hospitalizations compared to those of normal weight, although they had an increased duration of hospitalization in the ICU. Previous studies have in fact demonstrated an association of higher BMI with a lower mortality risk compared to normal BMI.32,33 Moreover, the elderly had a lower than expected number of exacerbations, but a higher number of hospitalizations; older age has been described previously as a risk factor for hospitalization.14,34
Certain limitations of the study should be noted. In accordance with its observational design, our study may have been subject to patient-selection bias. In the present study, this limitation mainly stems from the fact that the study was conducted between October and March, thus encompassing all the winter months. Seasonal variations regarding COPD exacerbations, with a higher frequency observed during the winter season, might have introduced bias in the results obtained.35 In addition, patients with mild COPD are more likely to be seen and treated by general practitioners. It is thus likely that patients with less severe disease are underrepresented in our study population, which was solely recruited by respiratory medicine physicians.
Moreover, comorbidities were recorded from patients’ medical history and their personal medical files, which contain information on diagnostic examinations as well as on all prescribed medications. Therefore, in some patients this may have led to an underdiagnosis of comorbid conditions. On the other hand, it should be noted that data extraction from medical files provides more robust and unbiased data compared to data that would be collected through patient interview, which is subject to recall bias. In addition, the study involved a large sample size, limiting the influence of potential confounding factors on the study results. Additional strengths of the study include the fact that all levels of respiratory health care in Greece were represented, as well as that patients were recruited from all geographical regions of Greece, reflecting variations in societal and environmental factors as well as physician practices.
Conclusion
The GOLDEN study underscores the fact that the frequency of exacerbations and hospitalizations increases with disease severity and with a higher number of comorbidities. Moreover, compliance with treatment appears to be a significant factor in reducing the occurrence of exacerbations. In light of the impact of the Greek socioeconomic crisis on the health care system, as well as the high prevalence of COPD in our country, it is imperative that strategies are identified to improve COPD outcomes, decrease costs, and increase compliance with treatment. The results overall indicate the need for multifactorial management of the COPD patient, as well as for the identification of interventions that will decrease disease exacerbations and hospitalizations. Finally, our outcomes indicate the need to educate the COPD patient on early identification of symptoms, as well as on identification, reporting, and management of COPD exacerbations.
Author contributions
EM, EGB, ECA, and KIG were involved in the study conception and design, FM, EM, and EGB collected the data, ECA undertook the statistical analysis of the data, FM, EM, and CV prepared the manuscript, and all authors read and approved the final paper. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
Eirini Mitsiki and Christos Varounis are employees of Novartis Hellas. Eleni G Bania has worked for Novartis Hellas. Evangelos C Alexopoulos held a contract with Novartis Hellas for study design and statistical analysis. Konstantinos I Gourgoulianis has received investigator’s fees for the GOLDEN study from Novartis Hellas. The study was funded by Novartis Hellas. The authors report no further conflicts of interest in this work.
References
Raherison C, Girodet PO. Epidemiology of COPD. Eur Respir Rev. 2009;18(114):213–221. | ||
World Health Organization. What is COPD? Available from: http://www.who.int/respiratory/copd/en. Accessed May 14, 2014. | ||
Lopez AD, Shibuya K, Rao C, et al. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J. 2006;27(2):397–412. | ||
Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. | ||
Tzanakis N, Anagnostopoulou U, Filaditaki V, Christaki P, Siafakas N. Prevalence of COPD in Greece. Chest. 2004;125(3):892–900. | ||
Sichletidis L, Tsiotsios I, Gavriilidis A, et al. Prevalence of chronic obstructive pulmonary disease and rhinitis in northern Greece. Respiration. 2005;72(3):270–277. | ||
Minas M, Hatzoglou C, Karetsi E, et al. COPD prevalence and the differences between newly and previously diagnosed COPD patients in a spirometry program. Prim Care Respir J. 2010;19(4):363–370. | ||
GOLD (Global initiative for chronic Obstructive Lung Disease). Global Strategy for the Diagnosis, Management, and Prevention of COPD. 2013. Available from: http://www.goldcopd.org/uploads/users/files/GOLD_Report_2013_Feb20.pdf. Accessed November 10, 2015. | ||
Halpin DM, Decramer M, Celli B, Kesten S, Liu D, Tashkin DP. Exacerbation frequency and course of COPD. Int J Chron Obstruct Pulmon Dis. 2012;7:653–661. | ||
Pasquale MK, Sun SX, Song F, Hartnett HJ, Stemkowski SA. Impact of exacerbations on health care cost and resource utilization in chronic obstructive pulmonary disease patients with chronic bronchitis from a predominantly Medicare population. Int J Chron Obstruct Pulmon Dis. 2012;7:757–764. | ||
Wedzicha JA, Seemungal TA. COPD exacerbations: defining their cause and prevention. Lancet. 2007;370(9589):786–796. | ||
Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363;(12):1128–1138. | ||
Perera WR, Hurst JR, Wilkinson TM, et al. Inflammatory changes, recovery and recurrence at COPD exacerbation. Eur Respir J. 2007;29(3):527–534. | ||
Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. | ||
Holguin F, Folch E, Redd SC, Mannino DM. Comorbidity and mortality in COPD-related hospitalizations in the United States, 1979–2001. Chest. 2005;(128):2005–2011. | ||
Anzueto A, Sehti S, Martinez FJ. Exacerbations of chronic pulmonary disease. Proc Am Thorac Soc. 2007;(4):554–564. | ||
Groenewegen KH, Schols AM, Wouters E. Mortality and mortality-related factors after hospitalization for acute exacerbation of COPD. Chest. 2003;124(2):459–467. | ||
Jansson SA, Andersson F, Borg S, Ericsson A, Jönsson E, Lundbäck B. Costs of COPD in Sweden according to disease severity. Chest. 2002;122(6):1994–2002. | ||
Geitona M, Hatzikou M, Steiropoulos P, Alexopoulos EC, Bouros D. The cost of COPD exacerbations: a university-based study in Greece. Respir Med. 2011;105(3):402–409. | ||
Papaioannou AI, Bania E, Alexopoulos EC, Mitsiki E, Malli F, Gourgoulianis KI. Sex discrepancies in COPD patients and burden of the disease in females: a nationwide study in Greece (Greek Obstructive Lung Disease Epidemiology and health ecoNomics: GOLDEN study). Int J Chron Obstruct Pulmon Dis. 2014;9:203–213. | ||
GOLD (Global initiative for chronic Obstructive Lung Disease). Global Strategy for the Diagnosis, Management, and Prevention of COPD. 2010. Available from: http://www.goldcopd.org/uploads/users/files/GOLDReport_April112011.pdf. Accessed November 10, 2015. | ||
Cheung YB. Zero-inflated models for regression analysis of count data: a study of growth and development. Stat Med. 2002;21(10):1461–1469. | ||
Tsiligianni IG, Kosmas E, Van der Molen T, Tzanakis N. Managing comorbidity in COPD: a difficult task. Curr Drug Targets. 2013;14(2):158–176. | ||
Fumagalli G, Fabiani F, Forte S, et al. INDACO project: a pilot study on incidence of comorbidities in COPD patients referred to pneumology units. Multidiscip Respir Med. 2013;8(1):28–36. | ||
Almagro P, Cabrera FJ, Diez J, et al. Comorbidities and short-term prognosis in patients hospitalized for acute exacerbation of COPD: the EPOC en Servicios de Medicina Interna (ESMI) study. Chest. 2012;142(5):1126–1133. | ||
Crisafulli E, Cost S, Luppi F, et al. Role of comorbidities in a cohort of patients with COPD undergoing pulmonary rehabilitation. Thorax. 2008;63(6):487–492. | ||
Divo M, Cote C, de Torres JP, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(2):155–161. | ||
Stafyla E, Kerenidi T, Gourgoulianis KI. Chronic obstructive pulmonary disease exacerbation frequency and severity. Int J Chron Obstruct Pulmon Dis. 2013;8:533–535. | ||
Bryant J, McDonald VM, Boyes A, Fisher RS, Paul C, Melville J. Improving medication adherence in chronic obstructive pulmonary disease: a systematic review. Respir Res. 2013;14(1):109. | ||
Cramer JA, Bradley-Kennedy C, Scalera A. Treatment persistence and compliance with medications for chronic obstructive pulmonary disease. Can Respir J. 2007;14(1):25–29. | ||
Herath SC, Poole P. Prophylactic antibiotic therapy for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2013;11:CD009764. | ||
Cao C, Wang R, Wang J, Bunjhoo H, Xu Y, Xiong W. Body mass index and mortality in chronic obstructive pulmonary disease: a meta-analysis. PLoS One. 2012;7(8):e43892. | ||
Lainscak M, von Haehling S, Doehner W, et al. Body mass index and prognosis in patients hospitalized with acute exacerbation of chronic obstructive pulmonary disease. J Cachexia Sarcopenia Muscle. 2011;2(2):81–86. | ||
Gadoury MA, Schwartzman K, Rouleau M, et al. Self-management reduces both short- and long-term hospitalization of COPD. Eur Respir J. 2005;26(5):853–857. | ||
Rabe KF, Fabbri LM, Vogelmeier C, et al. Seasonal distribution of COPD exacerbations in the Prevention of Exacerbations with Tiotropium in COPD trial. Chest. 2013;143(3):711–719. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.