Back to Journals » Clinical Interventions in Aging » Volume 21
Frailty Trajectories and Determinants in Older Adults After PCI: A Longitudinal Study
Authors Yao L, Wang R, Xu M, Jia W, Ma J, Li Y
Received 11 September 2025
Accepted for publication 23 December 2025
Published 8 January 2026 Volume 2026:21 567029
DOI https://doi.org/10.2147/CIA.S567029
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Li Yao,1 Rong Wang,2 Min Xu,2 Wei Jia,2 Jing Ma,2 Yanran Li2
1Department of Cardiology, The General Hospital of Ningxia Medical University, Yinchuan, People’s Republic of China; 2School of Nursing, Ningxia Medical University, Yinchuan, People’s Republic of China
Correspondence: Li Yao, Department of cardiology, The General Hospital of Ningxia Medical University, Yinchuan, 750004, People’s Republic of China, Email [email protected]
Aim: To identify distinct frailty trajectories and their determinants in older adults during the first six months after percutaneous coronary intervention (PCI), guided by the Health Ecology Model.
Design: A prospective observational design.
Methods: This study investigated the frailty status of elderly patients who underwent PCI surgery at a tertiary hospital in Ningxia, China, from November 2023 to May 2024, within six months after discharge. The Latent Growth Mixture Model was utilized to identify trajectories of frailty and classify participants based on these trajectories. Then, multivariable logistic regression analysis was employed to analyze the predictive factors of different trajectories. The reporting of this study adhered to the STROBE checklist.
Results: 218 elderly patients completed follow-up after PCI. There were three frailty trajectories among elderly people after PCI: the Low-Ascending Group (32.6%), the Middle-Alleviation Group (37.6%), and the High-Fluctuating Group (29.8%). Multivariate logistic regression analysis showed that depression, self-efficacy, occupation, NYHA class, and types of medication were influencing factors of their frailty trajectories (P< 0.05).
Conclusion: The high proportion of frailty among elderly individuals after PCI should be a cause for concern. Additionally, targeted interventions based on frailty trajectories and measures like depression screening, self-efficacy support, and polypharmacy management are needed to address frailty in elderly post-PCI patients.
Impact: This study highlights the importance of tracking the frailty status of elderly patients after PCI, providing a new perspective and theoretical basis for healthcare professionals to design personalized and targeted intervention plans to prevent or ameliorate frailty.
Patient or Public Contribution: No patient or public contribution. The study only included patients who were research participants.
Keywords: older adults, percutaneous coronary intervention, health ecology, frailty, trajectories, influencing factors
Introduction
Coronary atherosclerotic heart disease, also known as coronary heart disease (CHD), refers to heart conditions caused by the narrowing or obstruction of the coronary arteries due to atherosclerosis, leading to myocardial ischemia or necrosis. It is a common and frequently occurring disease in the cardiovascular system, resulting in various adverse outcomes and has become a severe public health issue globally. In 2017, an article published in the Lancet journal reported on the national incidence, prevalence, and years lived with disability for 328 diseases and injuries in 195 countries worldwide from 1990 to 2016.1 The study found that in 2016, there were approximately 154 million people affected by coronary heart disease, accounting for 32.7% of the global burden of cardiovascular diseases and 2.2% of the total global disease burden.1 The “China Cardiovascular Health and Disease Report 2022” indicates that there are about 11.39 million people currently suffering from coronary heart disease in China, with a prevalence rate of 27.8% among people aged 60 and above.2 Moreover, the mortality rate has been increasing year by year, posing a serious threat to the health of the elderly.
Percutaneous coronary intervention (PCI) is a minimally invasive nonsurgical treatment method used to improve blood flow in one or more segments of the coronary circulation, which can alleviate angina symptoms in patients with coronary heart disease. It has the advantages of minimal trauma, good therapeutic effects, and short hospital stays, and has become an important means of coronary blood flow reconstruction for patients with coronary heart disease.3 However, while PCI can address coronary artery stenosis and improve symptoms of myocardial ischemia, it cannot reverse or delay the progression of atherosclerosis, and patients still have the possibility of restenosis in the coronary arteries or even at the stent site after surgery.4 Studies show that in China, the readmission rate for elderly people after PCI treatment ranges from 12.02% to 15.00%.5,6 Frailty has been proven to be a strong predictive factor for patient outcomes after PCI, characterized by reduced physiological reserves, decreased functional capacity, and increased susceptibility to stressors.7,8 Research indicates that frail elderly people after PCI have a higher mortality rate and are more likely to experience adverse outcome events, such as falls and bed falls.9 Studies suggest that the degree of frailty is dynamically changing and still has a certain degree of reversibility in the early stages.10 However, investigations based on frailty trajectories in different populations indicate that the degree of frailty also varies over time.11 Currently, it is unclear how frailty changes over time in elderly people after PCI, what factors are associated with changes in their frailty trajectories, and there is a lack of comprehensive, systematic research on their physiological, psychological, and social aspects based on relevant theories. The exact impact of frailty on elderly people after PCI remains a topic of ongoing scientific exploration and discussion. Therefore, it is necessary to identify the frailty trajectories of elderly people after PCI as early as possible and to explore the influencing factors of their trajectories comprehensively under the guidance of relevant theoretical frameworks. Longitudinal studies with more comprehensive patient data can enhance our understanding of the relationship between PCI and frailty in the elderly, which can help to develop personalized intervention measures to improve the prognosis and quality of life of elderly people after PCI.
Background
Previous studies have indicated that frailty trajectories are influenced by a variety of factors, such as age, gender, illiteracy, etc.12 and are also related to adverse psychological conditions, lifestyle habits, and chronic diseases.1 The Health Ecological Model posits that an individual’s health is the result of the combined effects of their personal characteristics and their living environment.13 At present, the Health Ecological Model is widely applied in the analysis of influencing factors, model construction, and intervention research.14,15 The Health Ecological Model consists of five layers, with the core being personal traits, followed outwardly by behavioral characteristics, interpersonal networks, work and living conditions, and policy environments. The factors included in the five layers interact with each other and collectively impact human health. Zeng Lin’s research16 found that the factors affecting the occurrence of frailty in community-dwelling elderly diabetic patients are multi-dimensional and complex, involving the aforementioned five levels of the Health Ecological Model. Hou et al17 conducted a longitudinal study based on the Health Ecological Model to explore factors related to cognitive frailty in middle-aged and elderly populations, indicating that attention should be focused on physiological factors (underweight, chronic diseases), psychological factors (depression), and health behaviors (alcohol consumption) in the elderly. Ding et al18 found that nutrition, comorbidities, objective support, anxiety, and economic income are health ecological factors affecting preoperative frailty in elderly gastric cancer patients. Wang Y19 conducted a search of studies applying the Health Ecological Model to the field of chronic diseases, and the results demonstrated that the Health Ecological Model can comprehensively and multi-angle analyze the influencing factors of diseases in the field of chronic disease management, providing a theoretical basis for the development of targeted and multi-dimensional intervention measures.
Therefore, based on a review of the literature and discussions within the research group, this study selects representative factors from each level of the Health Ecological Model to systematically explore the factors influencing the frailty trajectory of elderly people after PCI. The overall approach of the final model is as follows: the personal traits layer includes general demographic information (age, gender, height, weight) and disease-related data (comorbidities, types of medication, heart function classification, history of falls, history of coronary heart disease); the behavioral characteristics layer includes smoking, alcohol consumption, anxiety, depression, self-efficacy, and self-care ability; the interpersonal network layer includes social support, marital status, and living alone; the work and living conditions layer includes educational level, monthly household income, and employment status; and the policy environment layer includes medical insurance.
Summarizing the above, (1) this study, in conjunction with the “Expert Consensus on Exercise Rehabilitation after Percutaneous Coronary Intervention”,20 employs a prospective longitudinal study to investigate the frailty of elderly patients from the time of discharge after PCI to six months post-discharge; (2) based on the Health Ecological Model, it explores the factors influencing their frailty trajectories, providing a theoretical basis for the development of comprehensive nursing intervention strategies for the frailty of elderly patients following PCI.
The Study
Aim
This study aims to determine the frailty trajectories and associated factors in elderly people after PCI.
Methods
Design
This is a prospective observational design.
Participants
This study randomly recruited participants from the cardiology department, cardiac center cadre ward, and geriatrics and special needs medicine department of a tertiary hospital in Ningxia, China, from November 2023 to May 2024. The following were the inclusion criteria: 1) aged≥60 years; 2) meeting the 2020 International Society of Cardiology and World Health Organization (WHO) diagnostic criteria for coronary heart disease;21 3) capable of communicating adequately with the researchers and cooperating to complete the assessment; 4) successful implementation of PCI;22 5) patients or their families providing consent and signing an informed consent form. The following were the exclusion criteria: 1) Patients who are critically ill and at risk of life-threatening conditions at any time; 2) Patients with severe cognitive dysfunction, mental illness, or advanced-stage malignant tumors. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) was chosen as a checklist for this study.
Sample Size: When the Bayesian Information Criteria (BIC) is used as the primary indicator for model selection, the sample size should meet the requirement of N≥200.23 Considering a 10% dropout rate, at least 223 subjects needed to be included. After four rounds of follow-up, complete data were available for 218 participants, which meets the sample size requirement.
This study conducted a questionnaire survey on 241 elderly patients after PCI at discharge (T1). Follow-ups were completed by 237, 228, and 218 patients at 1 month (T2), 3 months (T3), and 6 months (T4) after discharge, respectively. The dropout rates were 1.66% (T2), 3.73% (T3), and 4.15% (T4), with an overall dropout rate of 9.54%. The main reasons for dropout were withdrawal from the study, the presence of other serious diseases, and inability to contact. Statistical analysis revealed no significant differences in the distribution of general demographic and disease-related information between the dropout and non-dropout groups. Specific details of dropout are shown in Figure 1.
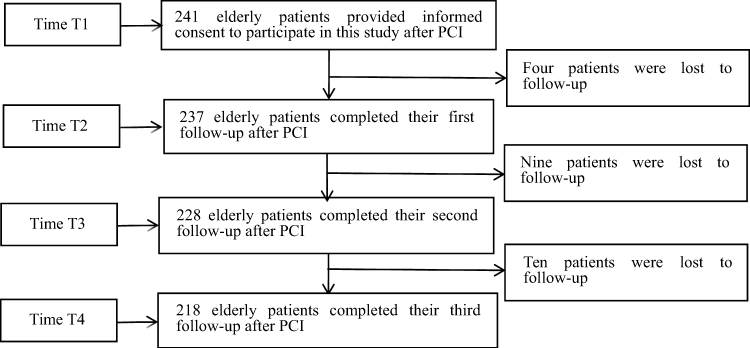 |
Figure 1 Flowchart of participant recruitment and follow-up at the four study timepoints after Percutaneous Coronary Intervention (PCI). |
Measures
Demographic Characteristics
The questionnaire includes 1) Socio-demographic variables, which collect relevant information about the characteristics of the participants, such as gender, age, marital status, level of education, employment status, personal financial situation, occupation (current job type, eg, Retired, worker, farmer), housing, and medical insurance. 2) Health-related variables, such as smoking, drinking, family history of coronary heart disease, body mass index (BMI) [BMI = weight (kg)/height (m2)] was categorized as underweight (<18.5 kg/m2), normal (18.5–25.0 kg/m2) and overweight and above (≥25.0 kg/m2), NYHA (New York Heart Association) class, history of falls within six months, and types of medication (total number of prescribed drugs at discharge, categorized as 3-<5, 5–7, or≥7). Participants were also asked if they had other chronic diseases; a list of eight diseases was provided, and if a disease was not on this list, participants could add other diseases. Multimorbidity is defined as the coexistence of two or more diseases (Johnston et al, 2019), as shown in Table 1.
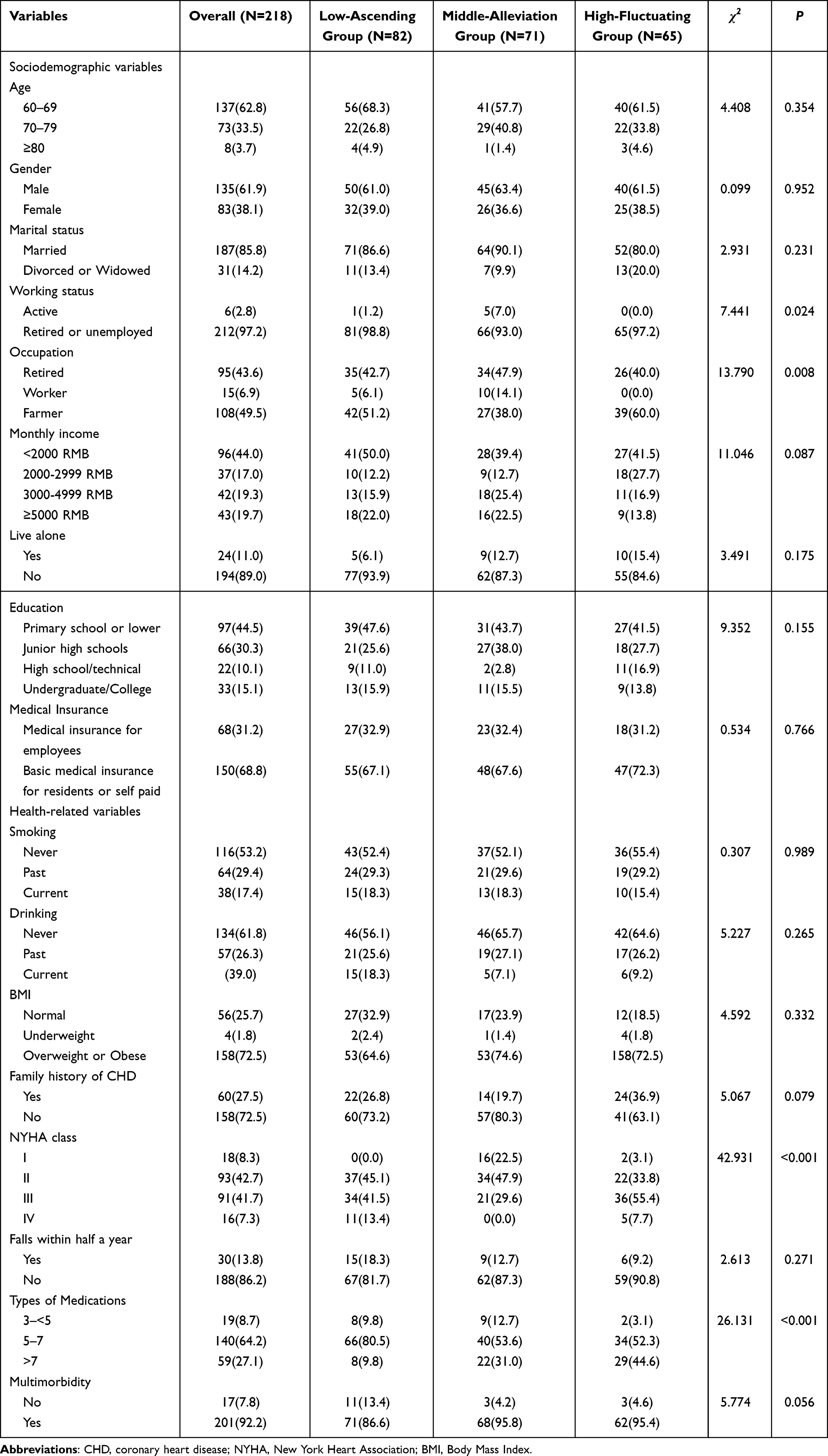 |
Table 1 Characteristics According to Frailty Trajectories at Baseline (N = 218) |
Frailty Scale
In our study, the FRAIL Scale24 was used to assess frailty status. This is a valid but brief scale that includes 5 items: fatigue, resistance, ambulation, illness, and weight loss. Additionally, this scale has previously been shown to effectively measure the degree of physical frailty in Chinese older adults, with a Cronbach’s α of 0.705.25 The total score ranges from 0 to 5, with higher scores indicating more severe frailty. A score of 3 or above indicates frailty.
Self Efficacy
The General Self-Efficacy Scale (GSES) was used to assess the patients’ self-efficacy. This scale was originally developed by German clinical and health psychologists Schwarzer et al26 in 1981 and later revised by Wang et al,27 in whose study it demonstrated excellent internal consistency with a Cronbach’s α of 0.926. The scale consists of 10 items, using a 4-point Likert scale: 1 to 4 points indicate a range from “not correct at all” to “completely correct”. The total score ranges from 10 to 40 points, with higher scores indicating better self-efficacy.
Social Support
The Social support rate scale (SSRS) was used to measure social support. This scale comprises 10 items and across three dimensions (subjective support, objective support, and support utilization), designed by Xiao.28 Items 1–5 and 8–10 are scored on a 4-point scale (1 to 4), while items 6–7 use a 2-point scale (0 to 1). The total score ranges from 12 to 66. Higher scores signify higher levels of social support. The SSRS was specifically designed for use in a Chinese context, demonstrating good validity and reliability, with a Cronbach’s α of 0.890.29
Anxiety and Depression
The Hospital Anxiety and Depression Scale (HADS) was used to assess the psychological state of the patients. This scale, developed by Zigmond et al30 in 1983, consists of 14 items, with 7 items (HADS-D) for assessing depressive symptoms and 7 items (HADS-A) for assessing anxiety symptoms. Each item is scored on a 4-point (0–3) response scale, with total scores for anxiety and depression ranging from 0 to 21. A total score greater than 8 on each subscale is considered indicative of anxiety and depression in the subjects. Both the HADS-A anxiety subscale and the HADS-D depression subscale have shown good concurrent validity, with a Cronbach’s α of 0.890.31
Self-Care Ability
The Exercise of Self-Care Agency Scale (ESCA) was used to assess the patients’ self-care abilities. This scale was designed by American scholars Kearney et al32 in 1979 based on Orem’s self-care theory. In 2000, Wang et al33 translated it into Chinese, and it has been proven to have good reliability and validity, with a Cronbach’s α of 0.77–0.80. It is the most widely used tool for measuring self-care ability in Mainland China, including 43 items across 4 dimensions: Self-Care Concept (8 items), Self-Care Responsibility (6 items), Self-Care Skills (12 items), and Health Knowledge Level (17 items). Each item is scored from 0 to 4, with a total score ranging from 0 to 172. Higher scores on the scale indicate a higher level of self-care ability: 116–172 points for high level; 58–115 points for moderate level; 0–57 points for low level.
Data Collection
This study combines the “Expert Consensus on Post-Percutaneous Coronary Intervention Exercise Rehabilitation”, and in conjunction with the outpatient follow-up times after patient discharge, ultimately selects the survey time points as the time of patient discharge, one month after discharge, three months after discharge, and six months after discharge. On the day before the patient’s discharge, the researchers conducted a face-to-face survey and obtained two or more contact methods from the patient. During the survey, the researcher uses a unified set of instructions to explain the requirements for completing the questionnaire, ensuring that the patients fully understand the content of the survey. The questionnaires are distributed and collected on the spot, with any missing or ambiguous items in the questionnaires supplemented by verbal inquiry to ensure the completeness and reliability of the information. After the completion of the questionnaire, the next stage of the survey is scheduled with the patient. In the follow-up survey phase, surveys are conducted at one, three, and six months after discharge, using two methods: outpatient follow-up at this hospital’s cardiac rehabilitation clinic (which is basically consistent with the patient’s review time) and telephone follow-up.
Statistical Analysis
Mplus 7.4 software was used to conduct Latent Growth Mixture Modeling (LGMM) analysis to explore the frailty trajectories of elderly people after PCI. An unrestricted conditional latent class growth model was used to determine the trajectory classes and their characteristics. In the Latent Growth Mixture Modeling, both linear and quadratic growth parameters were freely estimated to allow for the identification of trajectories that could capture both steady changes and fluctuations over time. The baseline model was a 1-class model, and the number of classes in the model was increased one by one, comparing the fit indices between models. The best model was determined by combining practical significance and statistical indicators, ultimately determining the number and characteristics of frailty trajectories. Among them, the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and sample-corrected BIC (aBIC) are smaller, indicating a better model fit; when the P-values of the Vuong-Lo-Mendell-Rubin likelihood ratio test (VLMR) and the bootstrap likelihood ratio test (BLRT) for a k-class model are both significant, it indicates that the k-class model is significantly better than the (k-1)-class mo entropy reflects the precision of the latent class classification, with an entropy greater than 0.8 representing a 90% classification precision, and the higher the entropy, the more precise the classification. The parameter estimation method to be used in this study is the robust maximum likelihood estimation (RMLE), which allows for missing values in the follow-up data, assuming that the missing values are missing at random and do not affect the results.
Statistical analyses were performed using SPSS 26.0. Baseline characteristics across the identified frailty trajectories were described using frequencies and percentages [N(%)] for categorical data, and compared using the chi-square test. Continuous, normally distributed data were presented as mean (standard deviation) and compared using analysis of variance (ANOVA). Guided by the Health Ecology Model, predictor variables from its five layers were selected a priori. Subsequently, indicators that showed statistical significance in the univariate analyses were entered into a multinomial logistic regression model, with the frailty trajectory categories as the dependent variable. P<0.05 was considered statistically significant.
Ethical Considerations
The study design and procedures complied with the Declaration of Helsinki. The Ethics Committee of the General Hospital of Ningxia Medical University reviewed and approved the study (approval number: KYLL20221049). All participants gave written informed consent after being fully informed about the study’s objectives, procedures, potential risks, and benefits.
Results
Characteristics of the Study Sample
After four rounds of follow-up, the study sample included 218 participants, of which 135 (61.9%) were male and 83 (38.1%) were female. The majority of the elderly participants were in the age group of 60 to 69 years old (62.8%), identified as farmers (49.5%), not living alone (89.0%), had basic medical insurance for residents or paid for it themselves (68.8%), and were retired or unemployed (97.2%), as detailed in Table 1.
Frailty Trajectories
To determine the optimal number of frailty trajectory classes, we used latent class growth modeling (LCGM), and the fit indices (including AIC, BIC, and entropy) for different class models are presented in Appendix Table S1 and Appendix S1. The model fit indices supported a three-class solution as the optimal model (AIC = 4352.294, BIC = 4410.593; VLMR P < 0.001, BLRT P < 0.001; Entropy = 0.858). The three identified trajectories were: the Low-Ascending Group (32.6%), the Middle-Alleviation Group (37.6%), and the High-Fluctuating Group (29.8%), as shown in Figure 2. As illustrated in Figure 2, the Low-Ascending Group started from the lowest frailty scores, which then gradually increased over time. The Middle-Alleviation Group began with moderate scores and showed an alleviating trend. The High-Fluctuating Group started from the highest scores and demonstrated a fluctuating pattern throughout the follow-up period.
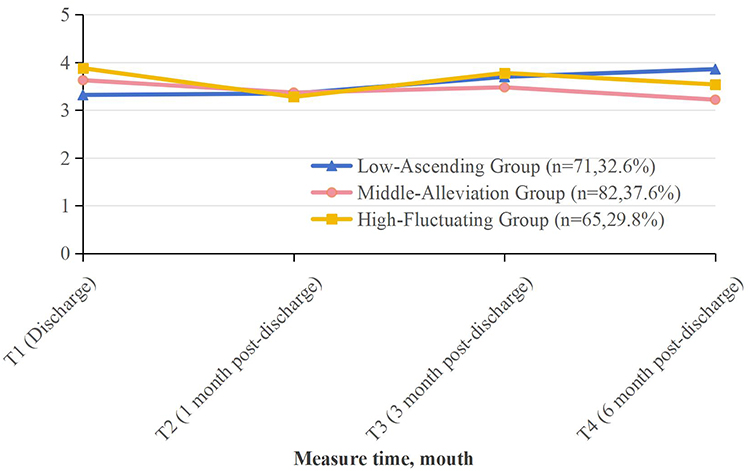 |
Figure 2 Trajectories of frailty in older adults during the six months following Percutaneous Coronary Intervention (PCI). Three distinct trajectories were identified: the Low-Ascending Group (37.6%), the Middle-Alleviation Group (32.6%), and the High-Fluctuating Group (29.8%). |
5.3. The results of the analysis on the predictive factors of frailty trajectories in elderly people after PCI.
The Results of the Univariate Analysis
Based on the chi-square test and univariate analysis of variance, the results indicate that there are statistically significant differences (P < 0.05) in anxiety, depression, social support, self-efficacy, self-care ability, working status, occupation, NYHA class, and types of medications among participants across different frailty trajectory categories. The univariate results are detailed in Table 1 and Table 2.
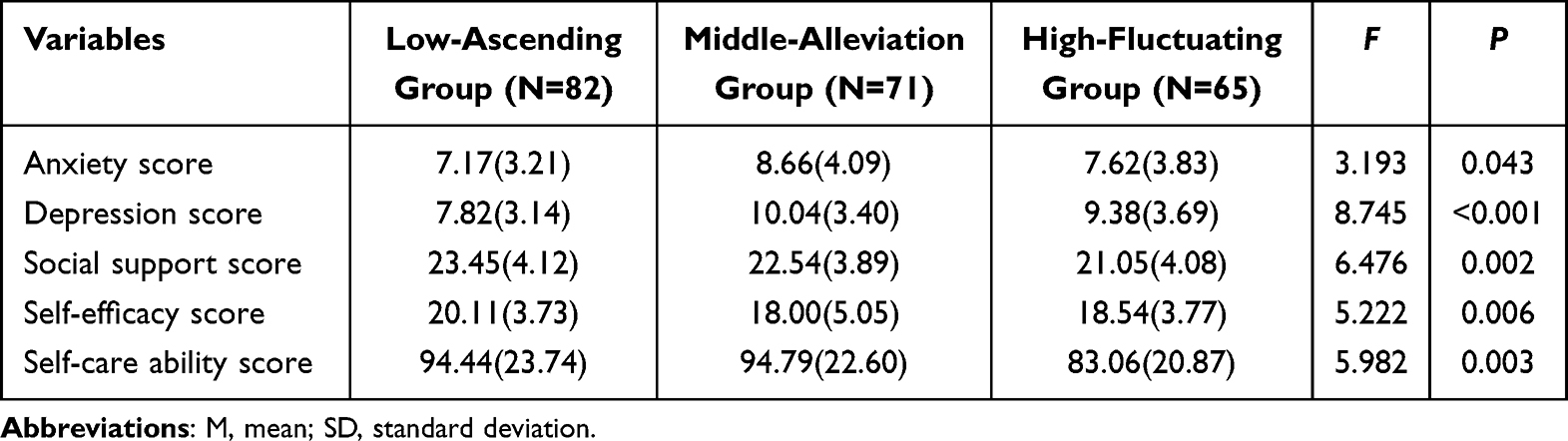 |
Table 2 Comparison of Anxiety, Depression, Social Support, Self-Efficacy, and Self-Care Ability Scores Across Different Frailty Trajectory Categories [n=218, M(SD)] |
The Results of the Multiple Logistic Regression Analysis
Using the variables that showed statistically significant differences in the univariate analysis as independent variables, and the three categories of frailty trajectories as dependent variables, a multinomial logistic regression analysis for unordered polytomous logistic regression was conducted. The regression results (Table 3) showed that factors significantly associated with frailty trajectories were depression, self-efficacy, occupation, type of medication, and NYHA class (P < 0.05). Compared to the Low-Ascending group trajectory, three risk factors were significantly associated with the middle-alleviation group trajectory: depression (OR=1.23, P=0.015), self-efficacy (OR=0.82, P=0.003), and occupation [retired and workers respectively (OR=3.05, 6.64, P=0.033, 0.032)]. Compared to the Low-Ascending group trajectory, NYHA class III (OR=5.04, P=0.003) was significantly associated with the high-fluctuating group trajectory. The type of medication was another influencing factor for the low, moderate, and high frailty group trajectories, with odds ratios for 3-<5 types of medication being 0.09 (P=0.007) and for 5–7 types of medication being 0.17 (P=0.002), and for the high-fluctuating group trajectory, the odds ratios were 0.05 for 3-<5 types of medication (P=0.003) and 0.14 for 5–7 types of medication (P<0.001).
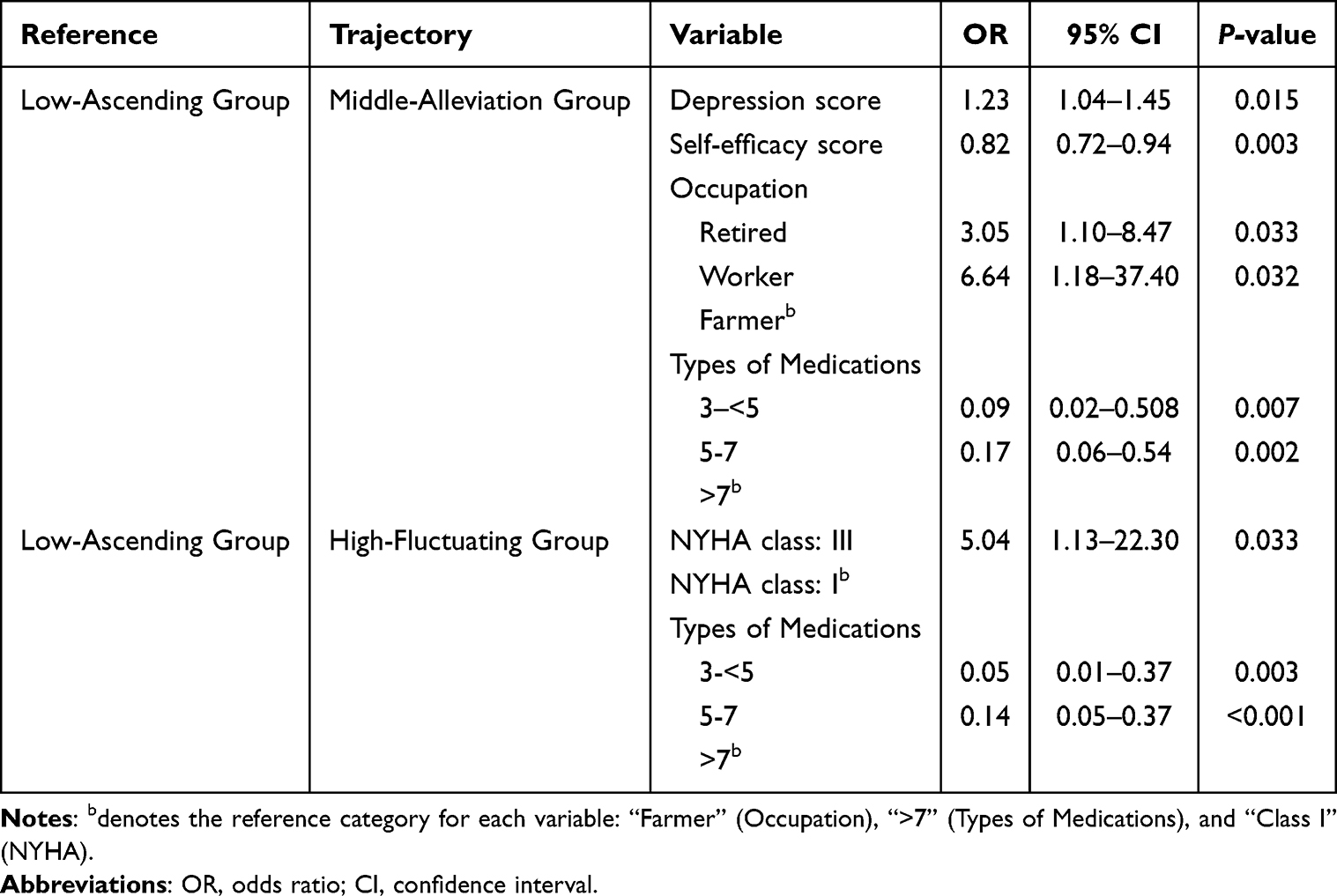 |
Table 3 Multivariate Logistic Regression Analysis of Frailty Trajectories in Elderly Patients After PCI |
Discussion
This study identified three distinct trajectories of frailty among elderly individuals aged 60 and above after PCI: the Low-Ascending Group; the Middle-Alleviation Group; and the High-Fluctuating Group. Furthermore, based on the health ecology theory model, we found that in addition to occupation, NYHA class, and types of medication from general demographic data, depression and self-efficacy also have a significant impact on the frailty trajectories of elderly individuals post-PCI, showing potential as intervention measures. The ultimate goal is to prevent or reverse frailty by early screening and timely intervention of these risk factors.
The results of this study reveal that the frailty trajectories of different subgroups of elderly individuals post-PCI exhibit varying trends and characteristics, categorized into three distinct groups: “Low-Ascending Group (32.6%)”, “Middle-Alleviation Group (37.6%)”, and “High-Fluctuating Group (29.8%)”. The “High-Fluctuating Group” consists of elderly patients with high frailty scores at discharge, which then fluctuate over time, initially decreasing, followed by an increase, and then a subsequent decrease. The “Low-Ascending Group” patients have low frailty scores at discharge, but these scores gradually increase and worsen over time post-discharge. The “Middle-Alleviation Group”, which is the largest in proportion, includes patients with moderate frailty scores at discharge, and their frailty levels follow a pattern similar to the “High-Fluctuating Group”, but with a more stable overall trend, remaining at a moderate level. These findings differ from those reported by other scholars on the frailty trajectories of the elderly. Tchalla et al34 identified four frailty trajectories among community-dwelling elderly in Limoges, France, over two years: “Robust stable Trajectory (26.8%)”, “Pre-frail worsening to frailty (35.8%)”, “Frail improving to less frailty (23.3%)”, and “Frail worsening to more frailty (14.1%)”. Yang et al35 identified three frailty trajectories among Chinese elderly aged 65 and above over 16 years: “Non-frail (56.5%)”, “Moderate progression (32.1%)”, and “High progression (11.4%)”. Du et al12 identified four trajectories of physical frailty among Chinese elderly: “no-frailty (58.82%)”, “increasing frailty (17.02%)”, “worsened-frailty (12.17%)”, and “improved-frailty (11.99%)”. The differences in these frailty trajectory patterns may be attributed to the use of various frailty assessment tools, follow-up durations, frequencies, and study populations. Yang et al utilized the Frailty Index proposed by Rockwood36 to assess frailty, while Achille et al employed Fried’s37 frailty phenotype (CHS index) for measurement. Both this study and Du et al used the FRAIL Scale24 questionnaire for investigation, but this study did not observe the “no-frailty” trajectory, indicating that the frailty level among elderly post-PCI is significantly higher than that of the general elderly population. Therefore, healthcare professionals should pay close attention to the frailty changes in this population and prioritize the prevention of frailty. In summary, despite some differences in measurement tools, time points, and study outcomes, all studies have found that frailty symptoms in the elderly exhibit various trajectories of change.
Our results indicate that compared to the “Low-Ascending Group” trajectory, elderly individuals with lower self-efficacy scores and higher depression scores, particularly those whose occupation is manual labor, are more likely to fall into the “Middle-Alleviation Group”. This is similar to the findings of Wu Z,38 which demonstrated a significant association between frailty trajectories and depressive symptoms among middle-aged and older adults in China. Notably, this study also found that self-efficacy and occupation as manual labor are significantly correlated with frailty trajectories. Firstly, self-efficacy is defined as an individual’s confidence in their ability to mobilize cognitive resources, motivation, and behavior to perform important tasks, such as chronic disease management.39 Individuals with high self-efficacy are more likely to engage in positive health behaviors, such as regular exercise and a healthy diet, which can help delay the progression of frailty. In this study, elderly individuals in the “Middle-Alleviation Group” post-PCI had lower levels of self-efficacy. Secondly, occupations involving manual labor may entail more physical exertion and less decision-making control, leading to higher levels of physical fatigue and psychological stress, thereby affecting frailty trajectories. Physical labor may become more challenging with age, and a lack of control over the pace of work can increase work-related stress. Therefore, it is recommended that healthcare professionals provide guidance to elderly individuals on how to manage chronic diseases through health education programs, workshops, or individual counseling, to enhance their confidence and ability in self-managed health. For elderly individuals with manual labor occupations, healthcare professionals should pay attention to their psychological health, offering necessary psychological assessments and support to alleviate psychological stress and improve frailty trajectories.
The results of this study show that, compared to the Low-Ascending Group trajectory, individuals with NYHA class III are more likely to enter the High-Fluctuating Group trajectory. This is inconsistent with the research findings of Gou et al40 which indicated that a higher NYHA class is significantly associated with frailty trajectories in elderly patients with chronic heart failure. The discrepancy may be due to differences in study design, population selection, sample size, and other factors between this study and theirs. Different studies have varying inclusion and exclusion criteria, leading to inconsistencies in their results. Additionally, this study found that the type of medication is another factor affecting the trajectories of the Low-Ascending Group, Middle-Alleviation Group, and High-Fluctuating Group. Patients taking more than 7 medications constituted the highest-risk group for unfavorable frailty trajectories. This is consistent with previous research.41 In the Middle-Alleviation Group and High-Fluctuating Group trajectories, the risk of frailty associated with the use of 5–7 medications is 0.17 and 0.14 times, respectively, compared to the risk associated with 3-<5 medications. Some studies have pointed out41 that polypharmacy is significantly correlated with the degree of frailty. Elderly individuals using more than five medications are more likely to exhibit frailty symptoms, possibly because polypharmacy increases the risk of drug interactions, leading to adverse reactions and negative events such as falls, thereby promoting the development of frailty. As the number of medications increases, the difficulty for elderly individuals to correctly take all their medications also increases, which may lead to decreased medication adherence,42,43 affecting treatment outcomes and thus influencing frailty trajectories. It is also possible that the use of multiple medications may bring economic burdens, affecting the quality of life and health behaviors of the elderly, and consequently influencing frailty trajectories. In conclusion, this study identified three distinct frailty trajectories and their determinants in older adults after PCI. Our findings extend beyond theoretical modeling to highlight actionable clinical targets. Specifically, the strong association of depression and low self-efficacy with unfavorable trajectories calls for the integration of routine psychological screening and self-management support into standard cardiac rehabilitation. Furthermore, the risk linked with polypharmacy underscores the critical need for proactive medication review. Such reviews, which should include direct discussions with patients, can identify opportunities for deprescribing and enhance medication adherence through personalized guidance.44
Limitations
The limitations of the study include a relatively small sample size and the use of convenience sampling, which may limit the representativeness of the sample and affect the generalizability and extrapolation of the results. Therefore, future research will require large-sample, multicenter longitudinal studies to further explore and verify the frailty trajectories of elderly people after PCI and their influencing factors.
Conclusion
This study found that there are three frailty trajectories among elderly people after PCI. Based on the Health Ecology Model, in addition to occupation, NYHA class, and types of medication, depression and self-efficacy are also significant factors affecting the frailty trajectories of elderly individuals post-PCI. This indicates that optimizing medication treatment plans for the elderly, providing psychological support, and health management guidance for diseases are crucial for preventing frailty in the elderly. The results of this study offer insights for intervention strategies for frailty symptoms in elderly individuals after PCI.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research was supported by Ningxia Natural Science Foundation of China (2023AAC03526).
Disclosure
Rong Wang is now affiliated with The 942nd Hospital of PLA Joint Logistics Support Force. The authors report no conflicts of interest in this work.
References
1. Bae S, Shimada H, Lee S, et al. Subjective cognitive decline and frailty trajectories and influencing factors in Japanese community-dwelling older adults: a longitudinal study. J Clin Med. 2023;12(18):5803. doi:10.3390/jcm12185803
2. Ma L, Wang Z, Fan J, Hu S. Interpretation of report on cardiovascular health and diseases in China 2022. Chin Gen Pract. 2023;26(34):3975–12.
3. Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 zACC/AHA/SCAI guideline for coronary artery revascularization: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(3):e4–e17. doi:10.1161/CIR.0000000000001039
4. Calderaro D, Bichuette LD, Macie PC, et al. Atualização da Diretriz de Avaliação Cardiovascular Perioperatória da Sociedade Brasileira de Cardiologia: foco em Manejo dos Pacientes com Intervenção Coronária Percutânea-2022. Arq Bras Cardiol. 2022;118(2):536–547. doi:10.36660/abc.20220039
5. Yang J, Zou S, Mao M, et al. Construction and validation of the risk prediction model for readmission among elderly patients with coronary heart disease. J Nurs PLA. 2021;38(12):20–23.
6. Li X, Wang X, Wu Y, et al. Consensus on integrated Traditional Chinese and Western Medicine for cardiac rehabilitation after percutaneous coronary intervention. Chin J Rehabil Med. 2022;37(12):1517–1528.
7. Kochar A, Peterson B, Young R, et al. Abstract 18211: does frailty matter in high risk PCI. Circulation. 2023;148(Suppl_1):A18211. doi:10.1161/circ.148.suppl_1.18211
8. Wang SS, Liu WH. Impact of frailty on outcomes of elderly patients undergoing percutaneous coronary intervention: a systematic review and meta-analysis. World J Clin Cases. 2024;12(1):107–118. doi:10.12998/wjcc.v12.i1.107
9. Yu Q, Guo D, Peng J, et al. Prevalence and adverse outcomes of frailty in older patients with acute myocardial infarction after percutaneous coronary interventions: a systematic review and meta-analysis. Clin Cardiol. 2023;46(1):5–12. doi:10.1002/clc.23929
10. Morley JE, Vellas B, Abellan Van Kan G, et al. Frailty consensus: a call to action. J Am Med Dir Assoc. 2013;14(6):392–397. doi:10.1016/j.jamda.2013.03.022
11. Howrey BT, Al Snih S, Middleton JA, Ottenbacher KJ. Trajectories of frailty and cognitive decline among older Mexican Americans. J Gerontol a Biol Sci Med Sci. 2020;75(8):1551–1557. doi:10.1093/gerona/glz295
12. Du J, Zhang M, Zeng J, et al. Frailty trajectories and determinants in Chinese older adults: a longitudinal study. Geriatr Nurs. 2024;59:131–138. doi:10.1016/j.gerinurse.2024.06.015
13. Chen Y, Shi L, Zheng X, et al. Patterns and determinants of multimorbidity in older adults: study in health-ecological perspective. Int J Environ Res Public Health. 2022;19(24):16756. doi:10.3390/ijerph192416756
14. Guo L, Zhang M, Namassevayam G, et al. Effectiveness of health management among individuals at high risk of stroke: an intervention study based on the health ecology model and self-determination theory (HEM-SDT). Heliyon. 2023;9(11):e21301. doi:10.1016/j.heliyon.2023.e21301
15. Han Y, Xing F, Huang J, Wang M. Associated factors of health-promoting lifestyle of the elderly based on the theory of social ecosystem. Aten Primaria. 2023;55(10):102679. doi:10.1016/j.aprim.2023.102679
16. Zeng L. Study on the Current Status and Risk Factors of Frailty in Community-Dwelling Older Adults with Diabetes From the Perspective of Health Ecology. Chongqing Medical University; 2024.
17. Hou D, Sun Y, Liu Z, Sun H, Li Y, Wang R. A longitudinal study of factors associated with cognitive frailty in middle-aged and elderly population based on the health ecology model. J Affect Disord. 2024;352:410–418. doi:10.1016/j.jad.2024.02.014
18. Ding L, Miao X, Jiang X, et al. Adverse outcomes and health-ecological influencing factors of preoperative frailty among elderly patients with gastric cancer. J Cancer Res Clin Oncol. 2023;149(16):7043–7051. doi:10.1007/s00432-023-04651-z
19. Wang Y. Status and Influencing Factors of Self-Management Behavior in Patients with Coronary Heart Disease: Based on Health Ecology Model. Huzhou University; 2022.
20. Hu S, Wang L, Guo L. Interpretation of experts’ consensus for exercise rehabilitation of the Post-PCI treatment. J Shanghai Univ. 2018;24(1):9–15.
21. Juarez-Orozco LE, Saraste A, Capodanno D, et al. Impact of a decreasing pre-test probability on the performance of diagnostic tests for coronary artery disease. Eur Heart J Cardiovasc Imaging. 2019;20(11):1198–1207. doi:10.1093/ehjci/jez054
22. Yan HB. Guidelines for the Diagnosis and Treatment of Clinical Coronary Heart Disease. People’s Medical Publishing House; 2010.
23. Wang M, Deng Q, Bi X. Bayesian methods for latent variable modeling. Adv Psychol Sci. 2017;25(10):1682–1695. doi:10.3724/SP.J.1042.2017.01682
24. Morley JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging. 2012;16(7):601–608. doi:10.1007/s12603-012-0084-2
25. Dong L, Qiao X, Tian X, et al. Cross-cultural adaptation and validation of the FRAIL Scale in Chinese community-dwelling older adults. J Am Med Dir Assoc. 2018;19(1):12–17. doi:10.1016/j.jamda.2017.06.011
26. Schwarzer R, Born A, Iwawaki S. The assessment of optimistic self-beliefs: comparison of the Chinese, Indonesian, Japanese, and Korean versions of the general self-efficacy scale. Psychologia. 1997;40(1):1–13.
27. Wang C, Hu Z, Liu Y. The reliability and validity study of the general self-efficacy scale. Appl Psychol. 2001;7(1):37–40.
28. Xiao S. Theoretical basis and research applications of social support rating scale. J Clin Psychiatry. 1994;4(2):98–100.
29. Zhang Y, Ma Z, Zhou P, Yang Q. The relationship between social support and depression and the mediating effect of psychological resilience in Qinghai. Pract Prev Med. 2023;30(11):1366–1369.
30. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
31. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale: an updated literature review. J Psychosom Res. 2002;52(2):69–77. doi:10.1016/S0022-3999(01)00296-3
32. Kearney BY, Fleischer BJ. Development of an instrument to measure exercise of self-care agency. Res Nurs Health. 1979;2(1):25–34. doi:10.1002/nur.4770020105
33. Wang HH, Laffrey SC. Preliminary development and testing of instruments to measure self-care agency and social support of women in Taiwan. Kaohsiung J Med Sci. 2000;16(9):459–467.
34. Tchalla A, Cardinaud N, Gayot C, et al. Patterns, predictors, and outcomes of frailty trajectories in community-dwelling older adults: results from the FREEDOM Cohort Study. Arch Gerontol Geriatr. 2023;114:105101. doi:10.1016/j.archger.2023.105101
35. Yang X, Wang W, Zhou W, Zhang H. Effect of leisure activity on frailty trajectories among Chinese older adults: a 16-year longitudinal study. BMC Geriatr. 2024;24(1):771. doi:10.1186/s12877-024-05370-x
36. Rockwood K, Mitnitski A. Frailty in relation to the accumulation of deficits. J Gerontol a Biol Sci Med Sci. 2007;62(7):722–727. doi:10.1093/gerona/62.7.722
37. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–M156. doi:10.1093/gerona/56.3.M146
38. Wu Z. Trajectory Change and Dynamic Association of Frailty and Depression in Middle-Aged and Older Chinese People: A Study Based on CHARLS. Anhui Medical University; 2024.
39. Guo J, Dai Y, Chen Y, Chen Q, Wang X. Influencing factors of care dependence in patients with coronary heart disease after percutaneous coronary intervention—a cross‐sectional study. Nurs Open. 2023;10(2):241–251. doi:10.1002/nop2.1299
40. Gou D. Trajectory of Frailty and Its Predictors in Elderly Patients with Chronic Heart Failure: A Longitudinal Study. Zunyi Medical University; 2023.
41. Ding H, Li C, Cheng Y, et al. Trajectories of frailty in patients with chronic heart failure and their influencing factors. Nurs J. 2024;39:39–44.
42. Huang F, Yang X, Yuan L, et al. Development and validation of a predictive risk model for frailty in elderly patients with multimorbidity. Geriatr Gerontol Int. 2022;22(5):471–476. doi:10.1111/ggi.14390
43. Huang L. Current status and analysis of polypharmacy among elderly outpatients in a certain hospital. Chin J Mod Drug Appl. 2024;18(15):132–135.
44. Gualtieri L, Rigby M, Wang D, Mann E. Medication management strategies to support medication adherence: interview study with older adults. Interact J Med Res. 2024;13:e53513.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.