")
Back to Journals » Open Access Emergency Medicine » Volume 15
Frailty Identification in Prehospital Care: A Scoping Review of the Literature
Authors Alshibani A , Alharbi M , Conroy S
Received 8 March 2023
Accepted for publication 22 May 2023
Published 14 June 2023 Volume 2023:15 Pages 227—239
DOI https://doi.org/10.2147/OAEM.S409083
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Abdullah Alshibani,1– 3 Meshal Alharbi,1,2 Simon Conroy4
1Emergency Medical Services Department, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 3Department of Health Sciences, College of Life Sciences, University of Leicester, Leicester, UK; 4MRC Lifelong Health & Ageing Unit, University College London, London, UK
Correspondence: Abdullah Alshibani, Emergency Medical Services Department, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, Riyadh, 14611, Saudi Arabia, Email [email protected]
Abstract: The proportion of older adults is increasing worldwide. Frailty assessment in prehospital care was suggested to improve triage decisions and paramedics’ judgment. This study aimed to assess the scope and nature of available evidence around frailty identification in prehospital care. A systematic search of the literature was performed using MEDLINE, SCOPUS, CINHAL, and Web of Science to identify relevant articles published from January 2022 downwards. A list of indexed terms and their associated alternatives were pre-determined. Of the 71 identified and reviewed articles after removing duplicates, six articles were included in the review. Due to the heterogeneity of the included articles, the findings were described narratively. The findings of this review showed that the available evidence is limited and heterogenic. Two themes emerged from the findings of the included articles: 1) Paramedics’ Perceptions about Frailty Assessment in Prehospital Care and 2) Frailty Scores for Application in Prehospital Care. Paramedics recognised frailty assessment in pre-hospital care to be feasible and important. They highlighted the need for a simple and clear frailty score that could be used and mentioned to other healthcare professionals when handing over patients. Six frailty scores were reported to be used in prehospital care. The evidence around each frailty score is very limited. Overall, frailty assessment in prehospital care was shown to be important and feasible. Different frailty scores have been assessed for use in prehospital care. Further research investigating frailty identification in prehospital care is needed.
Keywords: aging consumers, narrative analysis, health and well-being, paramedic*, emergency, older
Introduction
The proportion of older adults is increasing worldwide. Data from the developed Western countries showed that the proportions of older adults aged 65 years and over will increase and are expected to reach a 20% of the entire population in the United States of America (USA) by 2030, 23% in the United Kingdom (UK) by 2035, and 29% in Europe by 2050.1–3 This will result in increased healthcare demands and cost as older adults are frequent healthcare users (as they are usually comorbid and are living with frailty) and, when are admitted to hospitals, they stay for prolonged periods.4–6
Compared to younger adults, older adults use ambulance services more frequently; requiring accurate triage and appropriate management plans made by paramedics that tailored to their healthcare needs.7 Current triage and management guidelines in prehospital care and are not clear about how to optimise the level of care provided to this population.8 For example, recent evidence showed that most current and developed geriatric-specific trauma triage criteria applied in prehospital care were not accurate in identifying older patients who had high injury severity and/or required trauma center care.9 This is potentially due to the fact that prehospital triage criteria and paramedics’ judgments on how to manage patients are predominantly reliant on physiological variables.10 Relying on physiological variables only when caring for older adults is inappropriate and could mislead treatment and management plans.10 The changes in anatomy and physiology with the normal process of aging, comorbidities, and medication use could greatly affect their physiological responses of older adults to acute injury/illness; possibly resulting in appropriate prehospital triage decisions and management plans for this population.10
Early frailty identification was argued to improve clinical decision-making, healthcare planning, and outcome for older patients.11,12 Frailty is theoretically defined as “a long-term condition associated with multiple diseases and ageing leading to decreased physiological reserve and poor resilience in the person who easily decompensate from minor bio-psychosocial stressors”.13 The available evidence from the literature suggested the use and integration of frailty attuned tools into prehospital care. It was shown that frailty assessment in prehospital care to be important in improving triage decisions and paramedics’ judgment and it is feasible to apply it in prehospital care. However, there was a paucity of literature around this issue in prehospital care.
The broader literature investigating the use of different frailty assessment for patients with emergency care needs has supported the use of the Clinical Frailty Scale (CFS) as a method of triage in the Emergency Department (ED).12,14–16 The use of the CFS in the ED was identified recently by studies from different Western developed countries (Australia, Switzerland, UK, and the USA) to accurately predict hospital-related outcomes.12,14–16 In relation to trauma, a recent prospective study showed that the assessment of frailty for older patients with major trauma using the CFS feasible and accurate compared to the Program of Research to Integrate Services for the Maintenance of Autonomy 7, and the Trauma Specific Frailty Index.17 Another recent paper also supported the use of the CFS to assess frailty for older trauma patients in the ED as it showed that the CFS independently predicted 30-day mortality, inpatient delirium, and increased care level at discharge for this population.18 The CFS is simple and easy to use but carries an implementation burden. There is still no strong evidence so far to support its application in the prehospital care, which needs to be assessed and investigated.
This review aims to the feasibility of frailty assessment in prehospital care based on paramedics’ perspectives and list the available frailty assessment tools for use in prehospital care including the CFS and investigate the available evidence around each one of them. Up to our knowledge, this study is the first to review and discuss prehospital frailty identification. Therefore, conducting a scoping review seems appropriate to scope the feasibility of frailty assessment in prehospital care and the available frailty assessment tools for potential use in such setting.
Materials and Methods
This scoping review is conducted to assess evidence around frailty identification in prehospital care. It adhered to the Joanna Briggs Institute (JBI) guide for scoping reviews19 and followed the Preferred Reporting Items of Systematic Reviews and Meta-Analysis extension for Scoping Review (PRISMA-ScR) guidelines (see Supplement Table 1).20
Search Strategy and Selection Criteria
The search strategy of this scoping review was developed with the aim to identify any frailty score used in prehospital care. Therefore, a clear research question was developed using the Population, Intervention, Comparison, and Outcomes (PICO) format:21 What scores have been used for older adults to identify frailty in prehospital care? (P: older adults, I: any frailty score, C: n/a, and O: frailty assessment and identification).
A systematic search of the literature was performed for the following databases: MEDLINE, SCOPUS, CINHAL, and Web of Science. A list of keywords and alternatives was generated to identify all relevant articles to the review which are: (“frailty score*” OR “frailty scale*” OR “frailty instrument*” OR “frailty tool*” OR “frailty assessment” OR “frailty identification” OR “frailty screening”) AND (“prehospital” OR “pre-hospital” OR “paramedic*” OR “emergency medical service*” OR “EMS” OR “ambulance*”). The database search was performed from January 2022 downwards to identify any relevant article to the review. An example of database search is available in Supplement Table 2. In addition, the reference lists of the potentially included articles and published reviews were manually searched for possible additional articles. All identified relevant articles for either databases search or manual search of the reference lists were included for screening.
The JBI guide for scoping reviews recommends a 3-step approach for literature search. Firstly, an initial search using MEDLINE should be conducted to identify potential keywords and alternatives which was conducted in this study. The second step is conducting electronic search of the literature which was performed through MEDLINE, SCOPUS, CINHAL, and Web of Science. The third step is hand searching which was conducted through exploring and assessing the evidence from the reference lists of the included studies and other relevant reviews in urgent and emergency care settings.
Clear inclusion/exclusion criteria were determined by the reviewers prior to literature search. Published original peer-reviewed articles, pre-prints, conference proceedings, letters to the editor reporting primary data where there is an English language abstract available were included. The primary focus of the included articles must be on frailty assessment in prehospital care. Exclusion criteria included: articles that are not published in English language and articles focusing on in-hospital settings. We included articles that are only published in English language due to the difficulties in translating non-English articles which could lead to misunderstanding the findings from such articles. We are only focused on frailty assessment in prehospital care only, so any article focusing on in-hospital care was excluded. Studies that examined both in-hospital and prehospital were predetermined to be included in the review, however, none were found when the database search was conducted. No article was excluded due to its quality as quality assessment is not a priority in scoping reviews.
Title and Abstract Screening
The references from the database search were transferred to Covidence software for tile and abstract screening. Reviews, commentaries, and editorials were excluded at this stage. This process was performed independently by two reviewers. The two reviewers are paramedics holding a PhD degree and have published several studies including reviews. A third reviewer, who is a geriatrician and professor, was assigned in case of any disagreement between the two reviewers that was not resolved through discussions. However, disagreements between the two reviewers in this review were resolved through discussions.
Full Text Screening
Articles with available full-text were read using Covidence software. Any article mentioning any frailty scores that are applied in prehospital care were included, regardless with article objectives and study design. Full text reading was performed independently by two reviewers. Disagreements were managed through discussions between the two reviewers to achieve consensus.
Data Extraction and Analyses
Data was extracted from the included articles using Microsoft Excel to guide the collection of information from each article. A pre-defined form was, therefore, developed and applied to all included articles. The following data was extracted from each article meeting the inclusion criteria: 1) Article identification (title, journal name, journal impact factor, authors names, publication date, country, hosting institution, and study setting), 2) Methods (design, objectives, sample characteristics, and statistical analyses), 3) Main findings of the article (paramedic perspectives and applied frailty score(s) if any was reported), and 4) Article conclusions. We initially performed data collection for three articles using the pre-defined data collection form. We determined that there is no need to modify or edit the data collection form and, therefore, was applied for the remaining included articles in this review.
We anticipated that the available evidence in this review is limited and heterogenic. Therefore, the findings from the included articles in this review were described narratively and summarized using tables. Two main topics have emerged from the findings of the included studies. These topics are: 1) Paramedics’ perceptions about frailty assessment in prehospital care and 2) Frailty scores for application in prehospital care. The findings of the included studies were collected with respect to these two topics. It was then compared and contrasted with each other and reported using tables with narrative description. Tables and figures were used to illustrate the findings of this review and describe the frailty scores that could be used in prehospital care.
Results
Database search yielded 130 articles and manual search identified one additional article for potential inclusion in the review – reaching a total of 131 articles. After removing duplicates, 71 articles were included for title and abstract screening. After reading the available full-text, six articles were found relevant and, therefore, included in this review22–27 (Figure 1). The remaining three articles were excluded as they mentioned prehospital frailty assessment, but the fact is the actual assessment was performed at admission about the frailty status before current admission which is not meeting our inclusion criteria.28–30
 |
Figure 1 PRISMA flow diagram. Note: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: 10.1136/bmj.n71. Creative Commons.31 |
The included articles were published from 2014 to 2021 (Table 1). Three articles were published from the United Kingdom (UK), two from Canada, and one from Australia (Table 1). Five of the included studies were published as full text22–26 and one was a conference proceeding.27 Different study designs were applied to assess different objectives within prehospital frailty assessment (Table 1). This has resulted in applying different statistical analyses that were tailored to the study design of each article. Due to the heterogeneity of the included articles in this review, the findings were reported narratively. Two distinctive themes have emerged from the findings of the included studies in this review, which will be discussed narratively: A) Paramedics’ perceptions about frailty assessment in prehospital care and B) Applied frailty scores in prehospital care.
 |
Table 1 Characteristics of the Included Articles |
Paramedics’ Perceptions About Frailty Assessment in Prehospital Care
Frailty assessment in prehospital care was shown to be feasible and important.23,25 Paramedics recognised that frailty is a frequent condition, which has a significant impact on patients, and highlighted that paramedics should be aware about it. They also highlighted the need for a simple and clear frailty score that could be used and mentioned to other healthcare professionals when handing over patients.24 However, few paramedics were skeptical of the value of formal frailty evaluation.24
When paramedics were asked in another recent study about the circumstances where they would assess frailty, seven themes were merged.26 The most common theme was advancing age (47%).26 Other themes were related to the following: social situation (28%), type of incident including, for example, unexplained and frequent falls (23%), reduced mobility (18%), previous medical history including dementia (13%), disposition (12%), and physical situation and confusion, inability to speak, and visible frailty (11%).26
Paramedics listed potential benefits around the value of frailty assessment in prehospital care which included:
- The contributions to decisions related to possible community care, arrangements of supportive care, and requesting medication reviews.
- Providing evidence for paramedics to base their decisions on for ongoing care which could be also shared with other clinicians.
- Potential contribution to proactively change the way that patients with frailty are managed.24
Clinical education was argued by paramedics to help in developing more diverse vocabulary and also a structure and context to frailty assessment.24 Training in caring for older people was noted to be important as the population of older people is increasing.24 Overall, the available evidence recognised frailty assessment in prehospital care to be important, useful, and feasible but requires more education and training.
Frailty Scores for Application in Prehospital Care
Six frailty scores were reported in the included articles to be used in prehospital care which are: 1) Care Partner- Comprehensive Geriatric Assessment (CP-CGA), 2) Care Partner-derived Frailty Index based up on Comprehensive Geriatric Assessment (CP-FI-CGA), 3) Edmonton Frail Scale (EFS), 4) Groningen Frailty Index (GFI), 5) Clinical Frailty Scale (CFS), and 6) Timed-Up and Go (TUG) test (Table 1). Definition of each frailty score is available in Table 2.
 |
Table 2 Frailty Scores Used in Prehospital Care |
Care-Partner Comprehensive Geriatric Assessment (CP-CGA)
The CP-CGA was found to be feasible for use in prehospital care.23 However, several issues were reported when CP-CGA was applied in prehospital care including, for example, lacking the presence of a care partner and awareness.23 Detailed findings about the CP-CGA are available in Table 3.
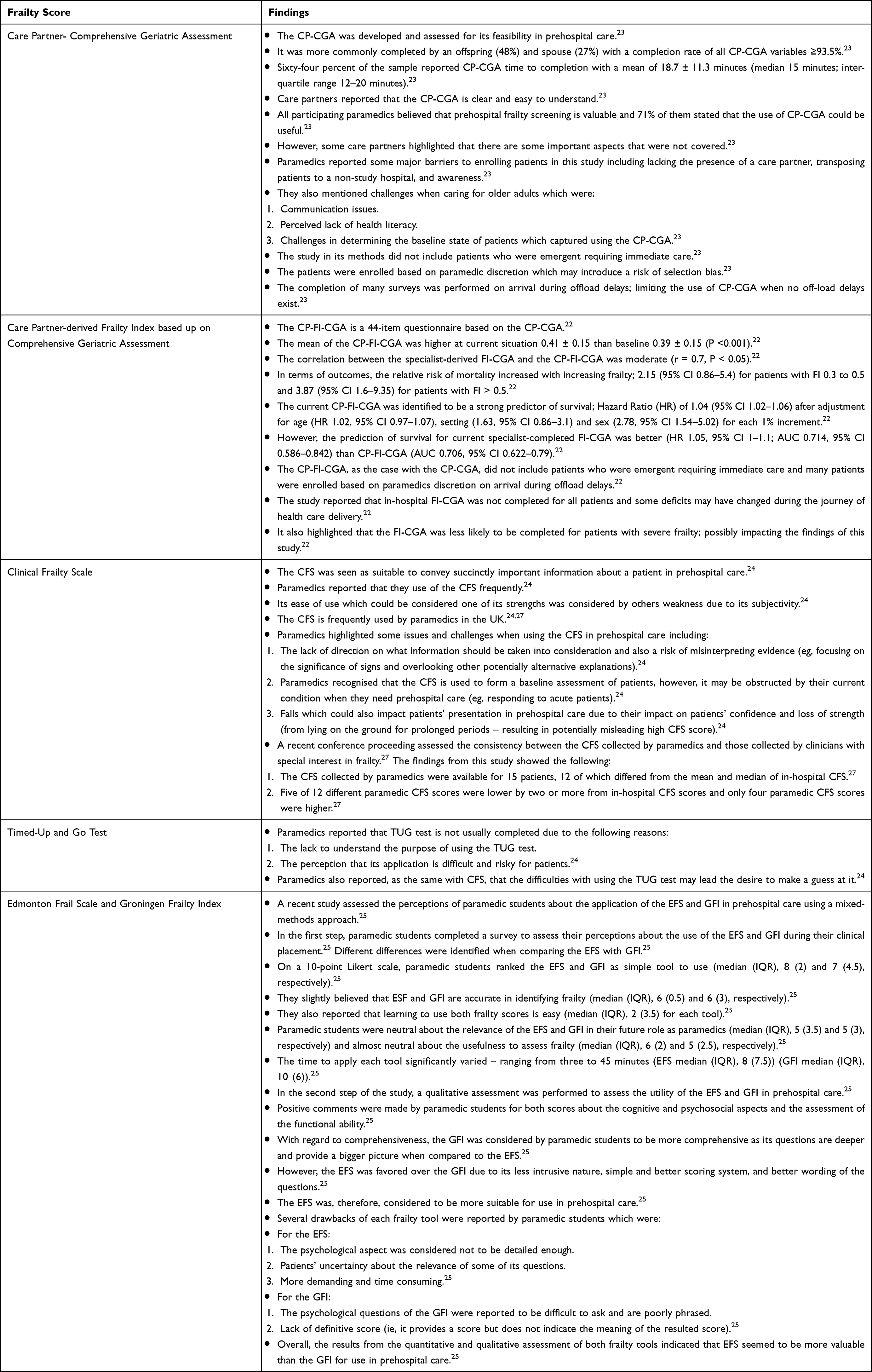 |
Table 3 Evidence Around the Use of Frailty Scores in Prehospital Care |
Care Partner-Derived Frailty Index Based Up on Comprehensive Geriatric Assessment (CP-FI-CGA)
The CP-FI-CGA was assessed for its validity for potential use in prehospital care (Table 3).22 In terms of outcomes, the relative risk of mortality increased with increasing frailty (Table 3).22 The current CP-FI-CGA was identified to be a strong predictor of survival after adjustment for age, setting, and sex for each 1% increment (Table 3).22 However, the prediction of survival for current specialist-completed FI-CGA was better than CP-FI-CGA (Table 3).22
Clinical Frailty Scale (CFS)
With regard to the CFS, paramedic considered its use to be suitable in gathering important patients’ information and they frequently use it when caring for older patients in prehospital care.24 The CFS is mainly used by paramedics in the UK.24,27 However, there were contradictory opinions among paramedics about the ease of the CFS use (Table 3).24 Furthermore, paramedics highlighted some issues and challenges when using the CFS (Table 3).24 Paramedics recognised the CFS is mainly used to broadly categorsie patients and provide a more holistic approach of patients’ assessment.24 They also highlighted that the CFS is not used for triage purposes and determining care plans, but rather serves as a guidance for identifying patients who could benefit from access to detailed assessment.24 A recent conference proceeding has assessed the consistency between the CFS collected by paramedics and that collected by clinicians with special interest in frailty (Table 3).27 It found that the CFS collected by paramedics are predominantly lower than that collected in-hospital (Table 3).27 This could be affected by the environment (mainly home) which require further investigation.27 Overall, the available evidence showed that most paramedics supported the use of the CFS, but this requires more active education and training for paramedics and further evidence about the use of the CFS in prehospital care.
Timed-Up and Go Test
One of the key points when considering patient management safely at home is mobility. The TUG test is one tool that is applied in prehospital care for such purpose.24 However, paramedics working in the UK reported that they do not usually complete the assessment due to several challenges (Table 3).24
Edmonton Frail Scale and Groningen Frailty Index
A recent study assessed the perceptions of paramedic students about the application of the EFS and GFI in prehospital care using a mixed-methods approach (Table 3).25 Both tools were considered to be easy to learn and use (Table 3).25 However, both tools were slightly believed by the participants to be accurate in identifying frailty and were ranked almost neutral with regard to its usefulness to assess frailty (Table 3).25 Several positive comments and drawback of each frailty score were reported by the participants (Table 3).25 Overall, the EFS was favored over the GFI and considered to be appropriate for use in prehospital care.25
Discussion
This is the first review, up to our knowledge, focusing on frailty identification in prehospital care. The findings of this review showed that the available evidence is limited and heterogenic. Paramedics recognised that frailty assessment is important and feasible and paramedics should be aware about it. However, few paramedics were skeptical about the value of formal frailty evaluation. Different frailty scores were assessed for use in prehospital care. The CP-CGA and CP-FI-CGA were shown to be feasible and valid for use in prehospital care. However, both scores are entirely dependent on the presence of knowledgeable care partners and require longer periods to be completed; adversely affecting their applicability in prehospital care. The CFS was reported to used more frequently in prehospital care in the UK but was criticised for its subjectivity and its possibility to mislead the actual baseline frailty especially for patients who have had fallen. With regard to the TUG test, paramedics highlighted that they do not understand the purpose of applying it in prehospital care and also reported difficulties for its application in such setting. The use of the EFS and GFI was considered by paramedic students in Australia to be feasible for use in prehospital care. The GFI was thought to be more comprehensive, but the EFS was determined to more suitable for use in prehospital care when compared to each other. Overall, frailty identification in prehospital care was shown to be important and feasible and several frailty scores could be used by paramedics to assess frailty in prehospital care.
As this review was focused on frailty identification and frailty scores used in prehospital care, it only included articles relevant to its focus. However, there are other articles, which were not included in this review, that assessed the use of other assessment tools in prehospital care which are not focused on assessing frailty itself but are relevant to older people living with frailty.8 These assessment tools are:
- The 4-item Elders at Risk of Independence Loss (PERIL) rule.
- The Identifying Seniors at Risk (ISAR) tool.
- Computerized Clinical Decision Support (CCDS) for patient who have fallen.8
The 4-item PERIL rule was shown to perform better than paramedic judgment and have the ability to set different thresholds that meet the needs prehospital care.8 The ISAR had similar performance to the 4-item PERIL rule, but the 4-item PERIL rule was reported to be simpler and had better adherence.8 The use of the CCDS by paramedics was shown to be safe and effective in referring patients to community fall services, and possibly is cost-effective.8
Frailty assessment has been increasingly applied in emergency and urgent care setting for the purpose of early identification of frailty to guide care and clinical decision-making. The CFS, for example, has been embedded increasingly in many Emergency Departments (EDs).12,14,16,32,33 The assessment of the CFS at ED triage was seen in recent literature to predict adverse outcomes.12 Our findings showed that the CFS is frequently used by paramedics in the UK. However, the use of the CFS have not been fully assessed and investigated for application and benefits when applied in prehospital care.
There are also other frailty assessment tools and other tools relevant to patients living with frailty that were used in emergency and urgent care settings.11,34 These tools are: 1) ISAR tool, 2) Vulnerable Elders Survey (VES-13), 3) Barthel Index, 4) Life Space Assessment (LSA), 5) Emergency Geriatric Screening tool (EGS), 6) Mini-Mental State Exam (MMSE), 7) Falls risk, 8) the 6-item Activities-specific Balance Confidence (ABC-6), 9) Geriatric Depression Scale (GDS-5), 10) Lawton Activities of Daily Living (ADL) scale, 11) Deficit Accumulation Index (DAI), and 12) Study of Osteoporotic Fracture frailty index (SOF).11,34 However, these tools have never been investigated for use in prehospital care except for ISAR.8
This review is the first to investigate frailty identification in prehospital care. However, the review has some limitations. The limited available evidence along with the heterogeneity of the included articles could impact the value of the findings of this review. The search strategy was limited to articles that were published in English only, which could obscure the findings from other non-English articles.
The review has several recommendations for practice and research. Paramedics should be aware about the value of frailty assessment and the available frailty scores that could be used in prehospital care. Education and training for the assessment and management of older people living with frailty is needed for prehospital care providers. Further research is also needed to assess the application of different frailty scores in prehospital care and determine appropriate frailty scores for use in such setting.
Conclusion
Frailty assessment in prehospital care is important and feasible. The importance of frailty assessment in prehospital care lies within its role in the contributions to decisions related to possible community care, arrangements of supportive care, and requesting medication reviews. It also included providing evidence for paramedics to base their decisions on for ongoing care which could be also shared with other clinicians, and potential contribution to proactively change the way that patients with frailty are managed in prehospital care. Thus, formal frailty assessment could guide decisions of paramedics and affect their behaviour, for example, providing proactive care. However, the evidence into this limited and heterogenic. Paramedics had different perceptions about the usefulness of frailty assessment in prehospital care and reported potential benefits of frailty assessment in such setting. Different frailty scores have been assessed for use in prehospital care; all of which seem feasible and could be implemented in prehospital care. Further education and training for prehospital care providers in caring for older people living with frailty is needed. Further research is also needed to investigate frailty identification in prehospital care.
Abbreviations
USA, United States of America; UK, United Kingdom; CFS, Clinical Frailty Scale; JBIv Joanna Briggs Institute; PRISMA-ScR, Preferred Reporting Items of Systematic Reviews and Meta-Analysis extension for Scoping Review; PICO, Population, Intervention, Comparison, and Outcomes; CP-CGA, Care Partner- Comprehensive Geriatric Assessment; CP-FI-CGA, Care Partner-derived Frailty Index based up on Comprehensive Geriatric Assessment; EFS, Edmonton Frail Scale; GFI, Groningen Frailty Index; TUG, Timed-Up and Go; 4-item PERIL, The 4-item Elders at Risk of Independence Loss; ISAR, The Identifying Seniors at Risk; CCDS, Computerized Clinical Decision Support; ED, Emergency Department.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research is funded by King Abdullah International Medical Research Center. The role of this funding is to cover publication fees for open access.
Disclosure
The Authors declare that there is no conflicts of interest.
References
1. Centers for Disease Control and Prevention. The State of Aging and Health in America 2013. Atlanta, GA: Centers for Disease Control and Prevention, US Dept of Health and Human Services; 2013.
2. European Commission. The Ageing Europe - Looking at the Lives of Older People in the EU. The Publications Office of the European Union; 2020.
3. Office for National Statistics. Population Ageing in the UK and Its Constituent Countries and the European Union. Office for National Statistics; 2012.
4. Bonne S, Schuerer DJ. Trauma in the older adult: epidemiology and evolving geriatric trauma principles. Clin Geriatr Med. 2013;29(1):137–150. doi:10.1016/j.cger.2012.10.008
5. Newell MA, Rotondo MF, Toschlog EA, et al. The elderly trauma patient: an investment for the future? J Trauma Acute Care Surg. 2009;67(2):337–340. doi:10.1097/TA.0b013e3181add08b
6. Staudenmayer KL, Hsia RY, Mann NC, Spain DA, Newgard CD. Triage of elderly trauma patients: a population-based perspective. J Am Coll Surg. 2013;217(4):569–576. doi:10.1016/j.jamcollsurg.2013.06.017
7. Goldstein J, Jensen JL, Carter AJ, Travers AH, Rockwood K. The epidemiology of prehospital emergency responses for older adults in a provincial EMS system. Can J Emerg Med. 2015;17(5):491–496. doi:10.1017/cem.2015.20
8. Alshibani A, Banerjee J, Lecky F, Coats TJ, Alharbi M, Conroy S. New horizons in understanding appropriate prehospital identification and trauma triage for older adults. Open Access Emerg Med. 2021;13:117–135. doi:10.2147/OAEM.S297850
9. Alshibani A, Alharbi M, Conroy S. Under-triage of older trauma patients in prehospital care: a systematic review. Eur Geriatr Med. 2021;12(5):903–919. doi:10.1007/s41999-021-00512-5
10. Alshibani A, Singler B, Conroy S. Towards improving prehospital triage for older trauma patients. Z Gerontol Geriatr. 2021;54(2):125–129. doi:10.1007/s00391-021-01844-4
11. Elliott A, Hull L, Conroy SP. Frailty identification in the emergency department—a systematic review focussing on feasibility. Age Ageing. 2017;46(3):509–513. doi:10.1093/ageing/afx019
12. Elliott A, Taub N, Banerjee J, et al. Does the clinical frailty scale at triage predict outcomes from emergency care for older people? Ann Emerg Med. 2021;77(6):620–627. doi:10.1016/j.annemergmed.2020.09.006
13. Xue Q-L. The frailty syndrome: definition and natural history. Clin Geriatr Med. 2011;27(1):1–15. doi:10.1016/j.cger.2010.08.009
14. Kaeppeli T, Rueegg M, Dreher-Hummel T, et al. Validation of the clinical frailty scale for prediction of thirty-day mortality in the emergency department. Ann Emerg Med. 2020;76(3):291–300. doi:10.1016/j.annemergmed.2020.03.028
15. Lewis ET, Dent E, Alkhouri H, et al. Which frailty scale for patients admitted via emergency department? A cohort study. Arch Gerontol Geriatr. 2019;80:104–114. doi:10.1016/j.archger.2018.11.002
16. Serina P, Lo AX, Kocherginsky M, et al. The clinical frailty scale and health services use for older adults in the emergency department. J Am Geriatr Soc. 2021;69(3):837–839. doi:10.1111/jgs.16937
17. Jarman H, Crouch R, Baxter M, et al. Feasibility and accuracy of ED frailty identification in older trauma patients: a prospective multi-centre study. Scand J Trauma Resusc Emerg Med. 2021;29(1):1–9. doi:10.1186/s13049-021-00868-4
18. Rickard F, Ibitoye S, Deakin H, et al. The clinical frailty scale predicts adverse outcome in older people admitted to a UK major trauma centre. Age Ageing. 2021;50(3):891–897. doi:10.1093/ageing/afaa180
19. Peters MD, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020;18(10):2119–2126. doi:10.11124/JBIES-20-00167
20. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
21. Elkins MY. Using PICO and the brief report to answer clinical questions. Nursing2010. 2010;40(4):59–60. doi:10.1097/01.NURSE.0000369871.07714.39
22. Goldstein J, Hubbard RE, Moorhouse P, Andrew MK, Mitnitski A, Rockwood K. The validation of a care partner-derived frailty index based upon comprehensive geriatric assessment (CP-FI-CGA) in emergency medical services and geriatric ambulatory care. Age Ageing. 2015;44(2):327–330. doi:10.1093/ageing/afu161
23. Goldstein J, Travers A, Hubbard R, Moorhouse P, Andrew MK, Rockwood K. Assessment of older adults by emergency medical services: methodology and feasibility of a care partner Comprehensive Geriatric Assessment (CP-CGA). Can J Emerg Med. 2014;16(5):370–383.
24. Green J, Kirby K, Hope S. Ambulance clinicians’ perceptions, assessment and management of frailty: thematic analysis of focus groups. Br Paramed J. 2018;3(3):23–33. doi:10.29045/14784726.2018.12.3.3.23
25. Harris W, Lucas PV, Eyles H, Parker L. Paramedic assessment of frailty: an exploratory study of perceptions of frailty assessment tools. Ir J Paramed. 2018;3(1):1–10. doi:10.32378/ijp.v3i1.80
26. Jadzinski P, Pocock H, Lofthouse-Jones C, et al. Improving recording and reporting of dementia and frailty via electronic patient record by ambulance staff in a single service (IDEAS). Br Paramed J. 2021;6(3):31–40. doi:10.29045/14784726.2021.12.6.3.31
27. Robson G, Lane S, Hines L, Ibude A, Sinclair A, Godden T. Electronic recording of clinical frailty scale scores for all acute hospital admissions age over 75: is the electronic score consistent with scores performed by frailty specialists, foundation doctors and paramedics?
28. Goldfarb M, Afilalo J, Chan A, Herscovici R, Cercek B. Early mobility in frail and non-frail older adults admitted to the cardiovascular intensive care unit. J Crit Care. 2018;47:9–14. doi:10.1016/j.jcrc.2018.05.013
29. Hope AA, Enilari OM, Chuang E, Nair R, Gong MN. Prehospital frailty and screening criteria for palliative care services in critically ill older adults: an observational cohort study. J Palliat Med. 2021;24(2):252–256. doi:10.1089/jpm.2019.0678
30. Hope AA, Munoz M, Hsieh S, Gong MN. Surrogates’ and researchers’ assessments of prehospital frailty in critically ill older adults. Am J Crit Care. 2019;28(2):117–123. doi:10.4037/ajcc2019285
31. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: 10.1136/bmj.n71
32. Shrier W, Dewar C, Parrella P, Hunt D, Hodgson LE. Agreement and predictive value of the Rockwood clinical frailty scale at emergency department triage. Emerg Med J. 2021;38(12):868–873. doi:10.1136/emermed-2019-208633
33. Wallis S, Wall J, Biram R, Romero-Ortuno R. Association of the clinical frailty scale with hospital outcomes. QJM. 2015;108(12):943–949. doi:10.1093/qjmed/hcv066
34. Jørgensen R, Brabrand M. Screening of the frail patient in the emergency department: a systematic review. Eur J Intern Med. 2017;45:71–73. doi:10.1016/j.ejim.2017.09.036
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.