Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Frailty and Adverse Outcomes Among Older Patients Undergoing Gastroenterological Surgery in Vietnam
Authors Than TNH, Nguyen T, Nguyen TTT ![]() , Pham T
, Pham T ![]()
Received 13 August 2021
Accepted for publication 9 September 2021
Published 24 September 2021 Volume 2021:14 Pages 2695—2703
DOI https://doi.org/10.2147/JMDH.S332986
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
The Ngoc Ha Than,1,2 Thien Nguyen,3 Tran To Tran Nguyen,1,4 Tai Pham4,5
1Department of Geriatrics, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam; 2Department of Geriatrics-Palliative Care, Ho Chi Minh City University Medical Center, Ho Chi Minh City, Vietnam; 3Department of Cardiology, 115 People’s Hospital, Ho Chi Minh City, Vietnam; 4Department of Geriatrics, Gia Dinh People’s Hospital, Ho Chi Minh City, Vietnam; 5Department of Traditional Medicine, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam
Correspondence: Tran To Tran Nguyen Tel +84 979635889
Email [email protected]; [email protected]
Purpose: With the ageing population, more older adults undergo surgery, and frailty increases the risk of postoperative complications in older patients. This study aimed to determine the association between frailty and 30-day adverse outcomes in older patients undergoing gastroenterological surgery in Vietnam.
Patients and Methods: A prospective cohort study was conducted in the Gastroenterology Department of the University Medical Center in Ho Chi Minh City. Frailty was determined using Fried’s criteria. Adverse outcomes within 30 days of gastroenterological surgery were recorded, including postoperative infections, acute respiratory failure, acute kidney injury, and death. Univariate and multivariate logistic analyses were performed to determine the association between frailty and 30-day postoperative adverse outcomes using Stata 14.0.
Results: Data of 302 elective surgical participants were collected (mean age: 69.8± 8.1 years, 53.3% female), and the prevalence of frailty was 18.5%. Frailty was an independent risk factor for 30-day adverse outcomes (odds ratio=6.56, 95% confidence interval, 2.77– 15.53, p< 0.001), which included postoperative infections, acute respiratory failure, acute kidney injury, and death. Frail participants had a significantly higher risk of postoperative infections (odds ratio=8.21, 95% confidence interval, 3.28– 20.54, p< 0.001), and exhaustion was strongly associated with postoperative adverse outcomes.
Conclusion: Frailty was a predictor of 30-day adverse outcomes in older patients undergoing gastroenterological surgery. Therefore, preoperative frailty should be screened in older patients, and frailty-associated risks should be considered during the decision-making process by physicians, patients, and their families.
Keywords: surgical risk factors, Fried’s criteria, postoperative complications, geriatrics, infections
Plain Language Summary
Ageing is a current global phenomenon, with Vietnam being the fast-ageing country in South-Eastern Asia. An increasing number of older people undergo surgical procedures and studies have shown that frailty is a predictive factor of poor outcomes in older patients undergoing surgery. Frailty is a highly common syndrome in older individuals, which is characterized by decreased function in multiple organ systems, causing the body to be vulnerable to stressors such as surgery. However, limited data are available on this relationship in older people in low-middle-income countries such as Vietnam. Therefore, we conducted this study to clarify the impact of frailty on adverse outcomes in older patients within 30 days after surgery in a teaching hospital in Vietnam. We enrolled 302 participants who underwent gastroenterological surgery and followed them up for 30 days after surgery for adverse outcomes, including infections, acute respiratory failure, acute kidney injury, and death. We found frailty to have a strong association with adverse outcomes in older Vietnamese patients undergoing surgery. Individuals with frailty had approximately 7 times higher risk of adverse outcomes and approximately 8 times higher risk infections than older patients without frailty. Therefore, surgical teams should consider older people with frailty as individuals who have a very high risk of poor outcomes after surgery, and the substantial frailty-associated risks shown in this study should be considered during the decision-making process by physicians, patients, and their families.
Introduction
Population ageing is a current global phenomenon, and it has been fastest in South-Eastern Asian countries.1 In Vietnam, the number of people aged 60 years and above was approximately 20 million in 2019, and it is estimated that the number of older people will account for one-third of the population in 2050.2 Frailty is a highly prevalent geriatric syndrome, characterized by a decrease in physiological reserve in multiple organ systems and loss of homeostasis when facing stressors.3,4 The prevalence of frailty in the older population is 15% in the USA5 and 7.4% in Japan,6 whereas it is much higher in South-Eastern Asian countries such as Thailand (22.1%) and Vietnam (21.7%).7 Frailty affects a significant proportion of older people residing in nursing homes and hospitals (19–75.6%)8,9 and increases the risks of falls, disability, prolonged hospital stay, and mortality.3,10
In older individuals undergoing surgery, frailty is a predictive factor for adverse outcomes.11,12 A number of mechanisms possibly underline this association. Frail patients tend to be accompanied by multimorbidity;13 studies showed that surgical patients with multimorbidity had a much higher risk of death than those without multimorbidity.14 Surgery is a major physiological stress in patients with frailty who are vulnerable to stressors and have a decreased physiologic reserve.15 This implies that frail patients have a limited ability to cope with and recover from surgery, and are vulnerable to adverse outcomes.16 For example, frail patients decrease in responses to hypoxia and hypercapnia, hypovolemia, and hypoxia; thus, they are more likely to have respiratory and circulatory failure intra- and postoperation.17
Research has shown that frailty increases the risks of postoperative complications and mortality rates within 30 days, 90 days, and 1 year after surgery.11,18,19 According to a study on older patients undergoing pancreaticoduodenectomy,20 frailty predicted major complications, longer hospital stays, and surgical intensive care unit admissions. A systematic review and meta-analysis study showed that frailty significantly increased the risks of postoperative major morbidity, short-term mortality, and long-term mortality; patients with frailty had 2.5 times higher risk of postoperative morbidity and 6 times higher risk of short-term mortality than patients without frailty.21
With the ageing population increasing, more older people undergo surgical procedures.17,22 In Vietnam, to the best of our knowledge, data of older individuals undergoing surgery are unclear and no study has addressed the association between frailty and postoperative complications among older Vietnamese patients. However, a previous study found that frailty was significantly high in older hospitalized patients (35.4%).23 Understanding the association between frailty and postoperative outcomes among older patients will help geriatricians and surgeons recognize the importance of preoperative frailty screening and discuss the outcomes with patients and their families.24 In addition, it will help develop preventive strategies for frail patients undergoing surgery. Therefore, this study aimed to determine the association between frailty and adverse outcomes in older individuals within 30 days of undergoing gastroenterological surgery in Vietnam.
Materials and Methods
Study Design
This was an observational cohort study conducted in the Gastroenterology Department, including the gastrointestinal unit and the liver-biliary-pancreatic unit, at Ho Chi Minh City University Medical Center, a teaching hospital located in District 5 in Ho Chi Minh City with 1000 beds. Patients admitted to this hospital are from Ho Chi Minh City and other provinces in South and Central Vietnam. The study was conducted between February and June 2019. Participants were recruited using convenience sampling. The study was approved by the Institution Review Board of the University of Medicine and Pharmacy at Ho Chi Minh City (approval number: 434/ĐHYD-HĐĐĐ), which followed the Declaration of Helsinki.
Participants
The inclusion criteria were: elective surgery patients expected to undergo an operation in the gastrointestinal (GI) system, aged ≥60 years, able to walk 4.6 m, and able to perform handgrip measurements. Exclusion criteria included the presence of any of the following symptoms: extreme vomiting, abdominal pain, GI bleeding or unstable vital signs, or not undergoing surgery. A total of 327 eligible patients were recruited for the study. However, 25 subjects were excluded because they did not undergo surgery, and no one refused to participate in the study. The participants were evaluated within 72 hours of admission and were followed up for complications for 30 days after surgery. Written consent forms were obtained from all participants.
Procedures
Frailty Assessment
Frailty was assessed based on Fried’s criteria,3 including unintentional weight loss within the last year, exhaustion, weakness, slowness, and low physical activity. Unintentional weight loss was defined as a decrease in weight of ≥4.5 kg or ≥5% within 1 year. Patients’ subjective estimation was acceptable Exhaustion was defined as a positive answer to one of two statements from the Center for Epidemiological Study Depression scale (“I felt that everything I did require effort during the last week” and “I could not get going during the last week”). Weakness was evaluated based on handgrip strength, using the Jamar hydraulic dynamometer Model 5030J1 (JLW Instruments, Chicago, IL, USA). The average value was calculated based on three repetitions of the task with the dominant hand, and the cut-off values were stratified by sex and body mass index (BMI) (women: ≤17 kg for BMI of ≤23 kg/m2, ≤17.3 kg for BMI of 23.1–26 kg/m2, ≤18 kg for BMI of 26.1–29 kg/m2, and ≤21 kg for BMI of >29 kg/m2; men: ≤29 kg for BMI of ≤24 kg/m2, ≤30 kg for BMI of 24.1–28 kg/m2, and ≤32 kg for BMI of >28 kg/m2). Walking speed was measured over walking a distance of 4.6 m at the participant’s usual speed, and the cut-off values were stratified by sex and height (women: ≥7 s for a height of ≤159 cm and ≥6 s for a height of >159 cm; men: ≥7 for a height of ≤173 cm and ≥6 s for a height of >173 cm). Low physical activity was evaluated using the Physical Activity Scale for the Elderly (PASE),25 which was scored based on the calculation from weight and frequency values of 12 activities during the previous week, including walking outside the house, light sport, moderate sport, rigorous sport, muscle strength/endurance exercises, light housework, heavy housework, home repair, yard care, outdoor gardening, caring for another person and working for pay or as a volunteer. The cut-off values were stratified by sex (women <270 Kcals/week; men <383 Kcals/week). Subjects who met ≥3 criteria were classified as frail, and those who met 0–2 criteria were classified as non-frail (including pre-frail and robust).
Other Covariates
Participants’ comorbid conditions were collected based on medical records, and the Charlson Comorbidity Index (CCI) was also used in assessing comorbidity.26 Nutritional status was assessed using the Nutrition Risk Screening (NRS) 2002 score27 and those subjects who had a score of ≥3 were categorized as having nutritional risk. Information regarding the age, sex, weight, and height of the participants was also collected. We also collected other covariates, including surgical organ, operation procedure, operative duration, and baseline creatinine. In this study, the American Society of Anaesthesiologists (ASA) physical status classification system was used to grade the preoperative health of the surgical patients, as evaluated by anesthesiologists.
Outcome Measures
This study primarily measured adverse outcomes within 30 days after surgery, including postoperative infections, acute respiratory failure, acute kidney injury, reoperation, and death. In our study, postoperative infections comprised infections related to superficial surgical-site infection, intra-abdominal infection, pneumonia, urinary tract infection, or sepsis. These events were collected from the hospital medical records. Patients were followed up for 30 days after their surgery.
Data Analysis
Data were processed using Epidata 3.1, and statistical analyses were performed using Stata version 14 (StataCorp, College Station, TX, USA), with p <0.05 indicating statistical significance. Discrete variables were expressed as counts and percentages, and χ2 or Fisher’s exact tests were used to compare proportions. The association between frailty and adverse outcomes was determined using a logistic regression model adjusted for relevant prognostic variables. To predict the primary outcome, we used items with statistical significance from each of the univariate analyses for our predictive model. After reviewing previous studies, we used patients’ demographic data for the model.
Results
Data were collected from 302 participants and made available to all participants at the end of the study. The mean age was 69.8 (standard deviation 8.1, range 60–92) years, and 161 (53.3%) were women; they were not significantly older than men (p=0.76).
There were 246 participants (81.5%) classified as non-frail and 56 (18.5%) as frail. In the study, 51.7% of the participants underwent laparoscopy, and the most frequent surgical indications were mechanical ileus and bleeding that required colon and/or rectal resection, which comprised 31.3% of the cases. Biliary surgery was the second most frequent procedure (25.2%).
Table 1 provides a comparison between the sample of 56 frail patients and 246 non-frail patients. The two groups of patients were similar in several factors, such as high blood pressure, BMI, and NRS score. However, the frail group had higher scores on CCI (p=0.006) and ASA classification (p<0.001).
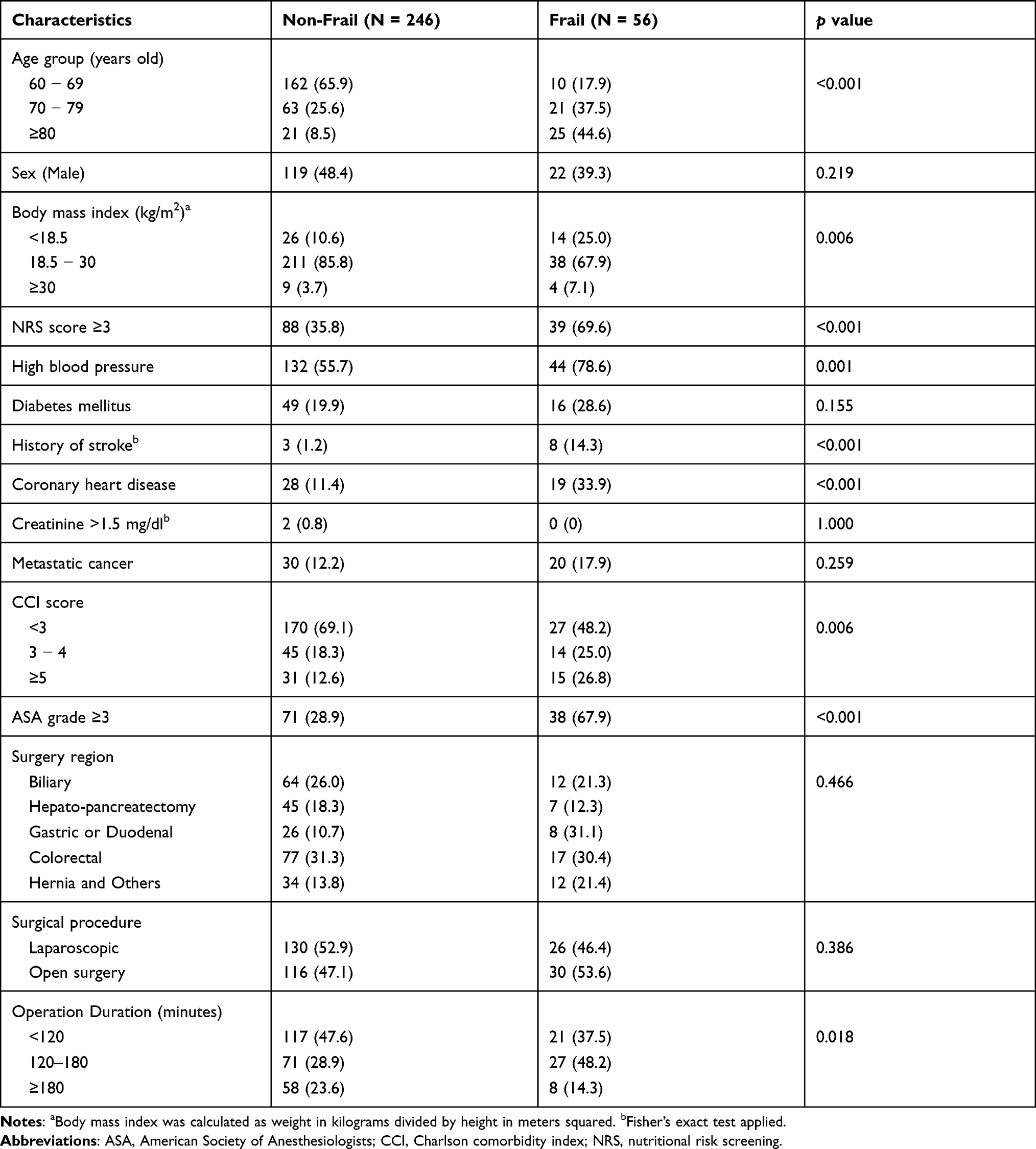 |
Table 1 General Characteristics of the Participants (n = 302) |
During the 30-day follow-up, adverse outcomes were recorded in 16.2% (49 patients) of our sample; 2.7% (8 patients) of the participants died. The most frequent complications were postoperative infections, and pneumonia was the most frequent type of infection. In our study, six patients underwent reoperation (2.0%). Table 2 shows the summary statistics for all types of complications.
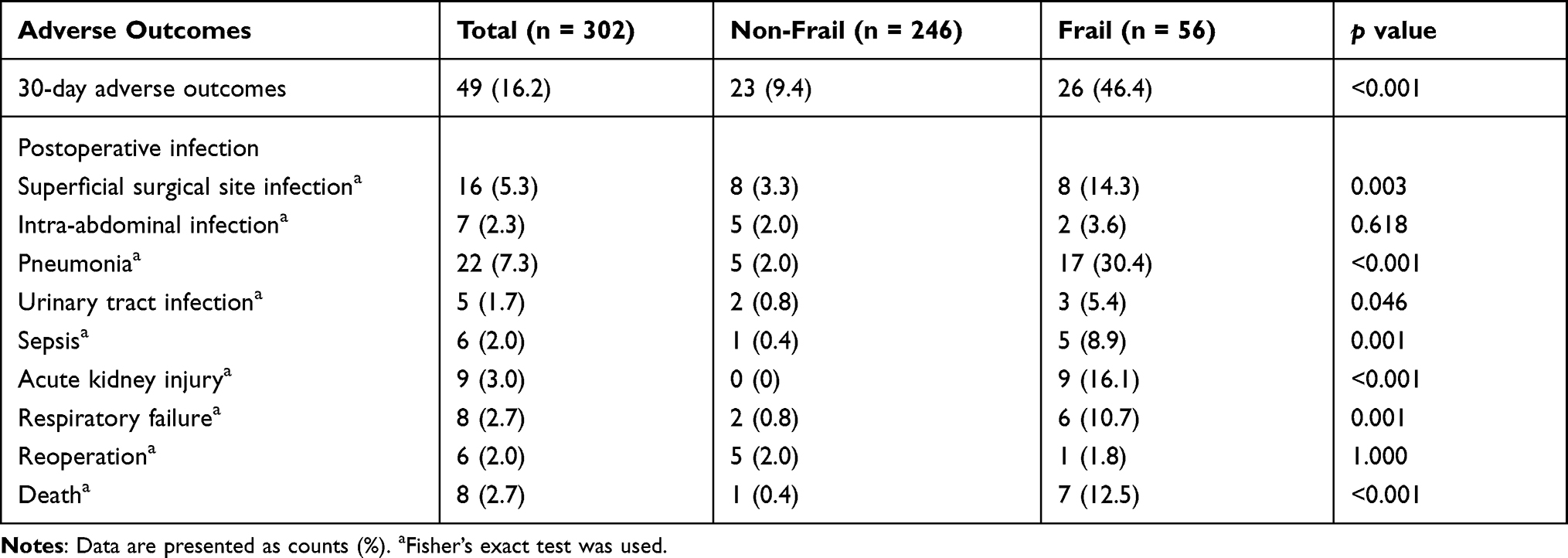 |
Table 2 Types of Adverse Outcomes of the Participants |
Univariate regression analysis showed that age, BMI, CCI score, state of metastasis, NRS score, and procedure time were predictive factors of 30-day postoperative outcomes. Detailed results of the univariate logistic regression are shown in Table 3.
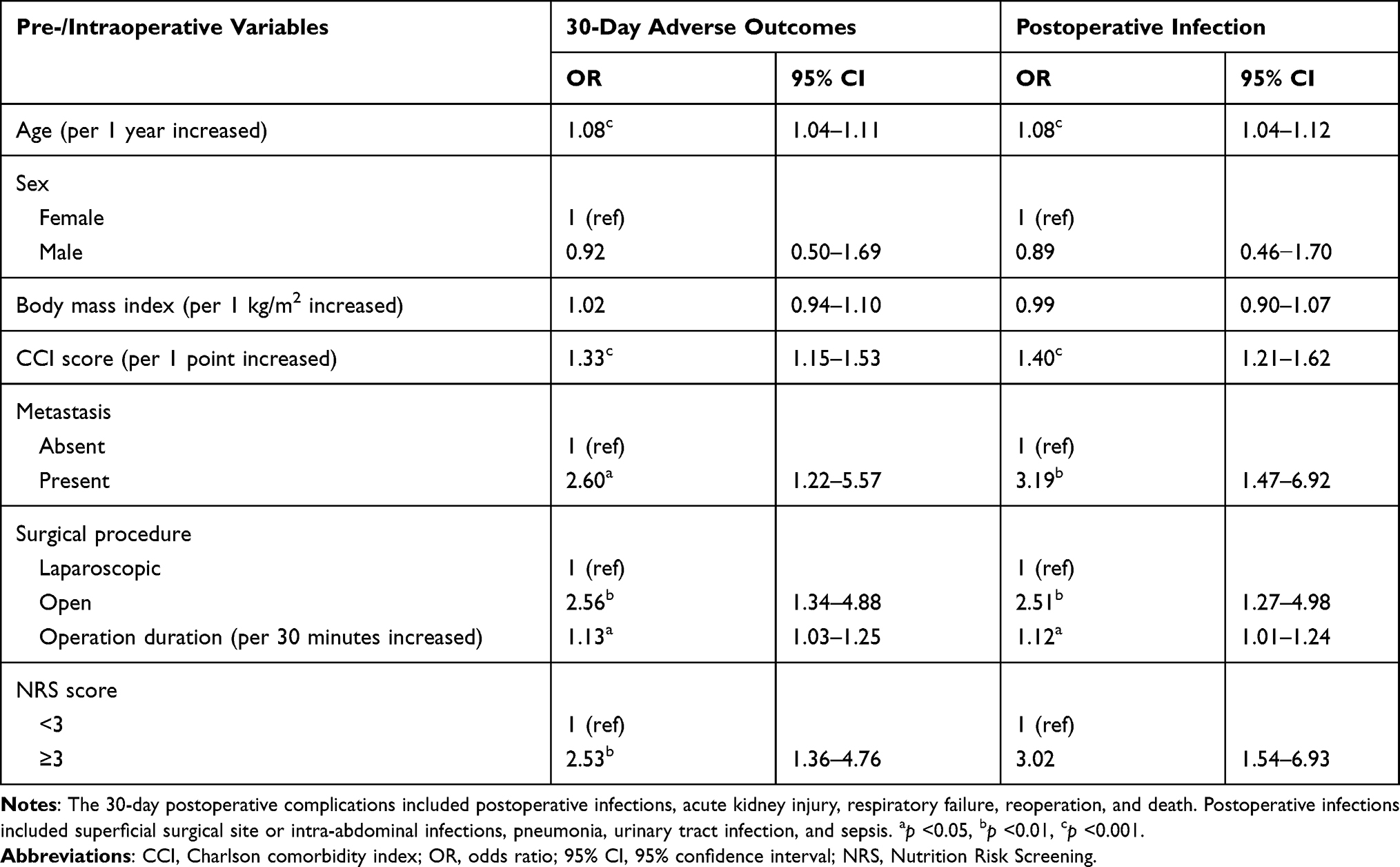 |
Table 3 Results of Univariate Logistic Regressions for Different Pre- and Intraoperative Variables of 30-Day Postoperative Complication and Postoperative Infections |
Table 4 shows the association between frailty and 30-day adverse outcomes, as revealed by multiple logistic regression analyses. The adjusted odds ratio (OR) of having an adverse outcome or postoperative infections within 30 days was 6.56 (95% confidence interval [CI]: 2.77–15.53, p<0.001) and 8.21 (95% CI: 3.28–20.54, p<0.001), respectively, in frail participants compared with those in non-frail participants. This association was found regardless of age, BMI, or surgery-related variables such as type of surgery and surgery duration.
 |
Table 4 Odds Ratios Comparing Frail and Non-Frail Patients on 30-Day Postoperative Complications and Postoperative Infections by Multivariable Logistic Regressions |
Table 5 presents the association of five components of Fried’s criteria and 30-day postoperative adverse outcomes. The results showed that the exhaustion criterion had the most impact on 30-day postoperative adverse outcomes (OR= 22.43, 95% CI: 6.07–82.90, p<0.001) and postoperative infections (OR=24.92, 95% CI: 6.67–93.19, p<0.001) whereas the weakness criterion had the least impact.
 |
Table 5 The Association of Five Components of Fried’s Criteria and 30-Day Postoperative Adverse Outcomes and Postoperative Infections by Multivariable Logistic Regressions |
Discussion
This study addressed the association between frailty and 30-day adverse outcomes in older Vietnamese patients undergoing gastroenterological surgery. The results showed that 18.5% of older patients undergoing surgery met frailty, and the rate of 30-day adverse outcomes in individuals with frailty was 5 times higher than that in individuals without frailty. We found that frailty had a significant association with postoperative adverse outcomes; older patients with frailty had approximately 7 times higher risk of 30-day postoperative complications and approximately 8 times higher risk of postoperative infection than older patients without frailty. Moreover, the mortality rate in the frail group was significantly higher than that in the non-frail group (7% vs 0.4%, p<0.001). The data indicated frailty was a predictive risk factor for 30-day adverse outcomes among older Vietnamese patients undergoing gastroenterological surgery.
These results are in line with those of previously reported studies.28–30 In a study of colorectal cancer resection, Tan et al found that frailty significantly increased the risk of major adverse outcomes (OR=4.08; 95% CI, 1.93–11.63),19 and similar results were observed by Myrick et al, who showed that frailty was associated with a higher risk of 30-day mortality in older postoperative patients.31 This can be explained by the decreased functional reserve across multiple physiological systems and an increased vulnerability to poor resolution of homeostasis when coping with surgery. As surgery is an essential stressor, it puts frail patients at a high risk of postoperative adverse outcomes such as postoperative infection, acute respiratory failure, and acute kidney injury.3 Moreover, frail individuals tend to have multimorbidity.13,32 In our study, a higher rate of comorbidity was observed in frail patients, of whom 26.8% had a high CCI score, compared with 12.6% in non-frail patients (p=0.006). This contributed to higher rates of poor outcomes in frail individuals. Similarly, according to a study on patients undergoing emergent cholecystectomy,33 frailty was independently associated with mortality, which coincides with our study. In another study in China, Binru et al reported that frailty was an independent risk factor for postoperative complications in older Chinese patients undergoing major thoracic and abdominal surgery (OR= 16.59, 95% CI: 4.56–60.40, p< 0.001).34 This result is relatively higher than the finding of our study. It may be due to the differences in the study populations. The participants in Binru’s study underwent major thoracic and abdominal surgery, whereas those in our study merely underwent abdominal surgery. Major thoracic surgery is a high-risk procedure, thus the probability of postoperative complications was higher.35 Furthermore, the prevalence of frailty in Binru’s study was also higher than the result of our study (26.1% vs 18.5%).
An interesting finding of our study is that in the five components of Fried criteria, exhaustion had the highest impact on 30-day postoperative adverse outcomes, and weakness (handgrip strength) had the least impact. This can be because exhaustion was evaluated based on patients’ self-reports, and as it is a subjective criterion, it may be more sensitive than other objective criteria in frailty.3 Meanwhile, in a study on cardiac surgery, Chung et al found that handgrip strength was a predictive factor of postoperative complications in patients with heart failure,36 and another study reported that walking speed was a predictor of postoperative morbidities in older patients undergoing gastrectomy.37 However, the authors only chose one component and did not compare other components in Fried’s criteria.
Our findings suggest that gastroenterological surgery may be considered high risk for frail people, and frailty was a predictive risk factor for 30-day adverse outcomes, including postoperative infections, acute respiratory failure, acute kidney injury, and death. Therefore, older patients considering gastroenterological surgery should be screened for frailty. Regardless of the surgical indication, the substantial frailty-associated risks shown here should be considered during the decision-making process shared by physicians, patients, and their families. Furthermore, preventive strategies need to be well-prepared to ensure perioperative safety for frail patients in clinical practice in a fast-ageing country such as Vietnam.
Strengths and Limitations
In our study, frailty was assessed using Fried’s criteria, which is considered a reference standard in frailty diagnosis. To the best of our knowledge, this is the first study to evaluate the association of frailty and postoperative complications in older patients in Vietnam, adding a clearer understanding of the impact of frailty on postoperative adverse outcomes in a South-Eastern Asian country. However, this study has several limitations. First, information regarding adverse outcomes was collected based on medical records, and there is a possibility that the diagnoses were not consistent among physicians. Second, this is a single-center study and the patient enrollment was performed by convenience sampling; thus, our results may not be nationally representative. Furthermore, older patients requiring emergency surgery were not recruited in our study, and there is a possibility that we underestimated the effect of frailty on poor outcomes.
Conclusion
This study found that frailty was an independent risk factor for 30-day adverse outcomes in older patients undergoing gastroenterological surgery in Vietnam. The rate of postoperative infections was approximately 8 times greater in frail patients, and the rate of 30-day adverse outcomes was approximately 7 times higher. Exhaustion was the most significant associated factor with 30-day adverse outcomes compared with other components in Fried’s criteria. Therefore, frailty should be assessed before surgery in older patients to prevent poor postoperative outcomes. Furthermore, surgeons, anesthesiologists, and other physicians may wish to consider strategies to optimize outcomes for frail patients.
Abbreviations
ASA, American Society of Anesthesiologists; BMI, Body mass index; CCI, Charlson comorbidity index; CI, confidence interval; GI, gastrointestinal; NRS, Nutrition risk screening; OR, odds ratio.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon a reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Institution’s Reviewed Board (IRB) of the University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam (approval number: 434/ĐHYD-HĐĐĐ), according to the Declaration of Helsinki.
Consent for Publication
Written informed consent for publication of their details was obtained from the study participants.
Acknowledgments
We would like to thank the participants who joined the study. We also deeply appreciate the support of the authorities of Ho Chi Minh City University Medical Center during the study period.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This study did not receive any funding.
Disclosure
All of the contributing authors declare that they have no conflict of interest. We do not have any financial or non-financial competing interests.
References
1. United Nations- Department of Economic and Social Affairs. World Population Ageing 2019. New York: United Nations; 2019.
2. Help Age Network in Asia Pacific. Ageing population in Vietnam. Vietnam agewatch report card; 2018. Available from: https://ageingasia.org/ageing-population-vietnam/.
3. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol. 2001;56A(3):M146–M156.
4. Bandeen-Roche K, Xue QL, Ferrucci L, et al. Phenotype of frailty: characterization in the women’s health and aging studies. J Gerontol Series A. 2006;61(3):262–266. doi:10.1093/gerona/61.3.262
5. Bandeen-Roche K, Seplaki CL, Huang J, et al. Frailty in older adults: a nationally representative profile in the United States. J Gerontol Series A. 2015;70(11):1427–1434. doi:10.1093/gerona/glv133
6. Kojima G, Iliffe S, Taniguchi Y, Shimada H, Rakugi H, Walters K. Prevalence of frailty in Japan: a systematic review and meta-analysis. J Epidemiol. 2017;27(8):347–353. doi:10.1016/j.je.2016.09.008
7. Nguyen AT, Nguyen LH, Nguyen TX, et al. Frailty prevalence and association with health-related quality of life impairment among rural community-dwelling older adults in Vietnam. Int J Environ Res Public Health. 2019;16(20):3869. doi:10.3390/ijerph16203869
8. Kojima G. Prevalence of frailty in nursing homes: a systematic review and meta-analysis. J Am Med Dir Assoc. 2015;16(11):940–945. doi:10.1016/j.jamda.2015.06.025
9. Richards SJG, D’Souza J, Pascoe R, Falloon M, Frizelle FA. Prevalence of frailty in a tertiary hospital: a point prevalence observational study. PLoS One. 2019;14(7):e0219083–e0219083. doi:10.1371/journal.pone.0219083
10. Nguyen TN, Cumming RG, Hilmer SN. The impact of frailty on mortality, length of stay and re-hospitalisation in older patients with atrial fibrillation. Heart Lung Circ. 2016;25(6):551–557. doi:10.1016/j.hlc.2015.12.002
11. Lin HS, Watts JN, Peel NM, Hubbard RE. Frailty and post-operative outcomes in older surgical patients: a systematic review. BMC Geriatr. 2016;16(1):157. doi:10.1186/s12877-016-0329-8
12. Sadiq F, Kronzer VL, Wildes TS. Frailty phenotypes and relations with surgical outcomes: a latent class analysis. Anesth Analg. 2018;127(4):1017–1027. doi:10.1213/ANE.0000000000003695
13. Vetrano DL, Palmer K, Marengoni A, et al. Frailty and multimorbidity: a systematic review and meta-analysis. J Gerontol Series A. 2019;74(5):659–666. doi:10.1093/gerona/gly110
14. Silber JH, Reiter JG, Rosenbaum PR, et al. Defining multimorbidity in older surgical patients. Med Care. 2018;56(8):701–710. doi:10.1097/MLR.0000000000000947
15. McIsaac DI, Taljaard M, Bryson GL, et al. Frailty as a predictor of death or new disability after surgery: a prospective cohort study. Ann Surg. 2020;271(2):283–289. doi:10.1097/SLA.0000000000002967
16. Gilbertson EA, Bailey TR, Kraiss LW, et al. Long-term impact of vascular surgery stress on frail older patients. Ann Vasc Surg. 2021;70:9–19. doi:10.1016/j.avsg.2020.06.048
17. Yang R, Wolfson M, Lewis MC. Unique aspects of the elderly surgical population: an anesthesiologist’s perspective. Geriatr Orthop Surg Rehabil. 2011;2(2):56–64. doi:10.1177/2151458510394606
18. Chen CL, Chen CM, Wang CY, et al. Frailty is associated with an increased risk of major adverse outcomes in elderly patients following surgical treatment of hip fracture. Sci Rep. 2019;9(1):19135. doi:10.1038/s41598-019-55459-2
19. Tan KY, Kawamura YJ, Tokomitsu A, Tang T. Assessment for frailty is useful for predicting morbidity in elderly patients undergoing colorectal cancer resection whose comorbidities are already optimized. Am J Surg. 2012;204(2):139–143. doi:10.1016/j.amjsurg.2011.08.012
20. Dale W, Hemmerich J, Kamm A, et al. Geriatric assessment improves prediction of surgical outcomes in older adults undergoing pancreaticoduodenectomy: a prospective cohort study. Ann Surg. 2014;259(5):960–965. doi:10.1097/SLA.0000000000000226
21. Sandini M, Pinotti E, Persico I, Picone D, Bellelli G, Gianotti L. Systematic review and meta-analysis of frailty as a predictor of morbidity and mortality after major abdominal surgery. BJS Open. 2017;1(5):128–137. doi:10.1002/bjs5.22
22. Neuman MD, Bosk CL. The redefinition of aging in American surgery. Milbank Q. 2013;91(2):288–315. doi:10.1111/milq.12014
23. Vu HTT, Nguyen TX, Nguyen TN. Prevalence of frailty and its associated factors in older hospitalised patients in Vietnam. BMC Geriatr. 2017;17(1):216. doi:10.1186/s12877-017-0609-y
24. Shah R, Attwood K, Arya S, et al. Association of frailty with failure to rescue after low-risk and high-risk inpatient surgery. JAMA Surg. 2018;153(5):e180214. doi:10.1001/jamasurg.2018.0214
25. Washburn RA, Smith KW, Jette AM, Janney CA. The Physical Activity Scale for the Elderly (PASE): development and evaluation. J Clin Epidemiol. 1993;46(2):153–162. doi:10.1016/0895-4356(93)90053-4
26. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
27. Kondrup J, Rasmussen HH, Hamberg O, Stanga Z. Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials. Clin Nutr. 2003;22(3):321–336. doi:10.1016/S0261-5614(02)00214-5
28. Mrdutt MM, Papaconstantinou HT, Robinson BD, Bird ET, Isbell CL. Preoperative frailty and surgical outcomes across diverse surgical subspecialties in a large health care system. J Am Coll Surg. 2019;228(4):482–490. doi:10.1016/j.jamcollsurg.2018.12.036
29. Rothenberg KA, Stern JR, George EL, Trickey AW, Morris AM, Hall DE. Association of frailty and postoperative complications with unplanned readmissions after elective outpatient surgery. JAMA Netw Open. 2019;2(5):e194330. doi:10.1001/jamanetworkopen.2019.4330
30. Ko FC. Preoperative frailty evaluation: a promising risk-stratification tool in older adults undergoing general surgery. Clin Ther. 2019;41(3):387–399. doi:10.1016/j.clinthera.2019.01.014
31. Shinall MC, Arya S, Youk A. Association of preoperative patient frailty and operative stress with postoperative mortality. JAMA Surg. 2020;155(1):e194620–e194620. doi:10.1001/jamasurg.2019.4620
32. Villacampa-Fernández P, Navarro-Pardo E, Tarín JJ, Cano A. Frailty and multimorbidity: two related yet different concepts. Maturitas. 2017;95:31–35. doi:10.1016/j.maturitas.2016.10.008
33. Lorenzon L, Costa G, Massa G, Frezza B, Stella F, Balducci G. The impact of frailty syndrome and risk scores on emergency cholecystectomy patients. Surg Today. 2017;47(1):74–83. doi:10.1007/s00595-016-1361-1
34. Han B, Li Q, Chen X. Frailty and postoperative complications in older Chinese adults undergoing major thoracic and abdominal surgery. Clin Interv Aging. 2019;14:947–957. doi:10.2147/CIA.S201062
35. Irons JF, Martinez G. Complex, high-risk thoracic surgery—does risk always outweigh the benefit or can we manage it safely? Video Assist Thorac Surg. 2017;2(9):63. doi:10.21037/vats.2017.09.03
36. Chung CJ, Wu C, Jones M, et al. Reduced handgrip strength as a marker of frailty predicts clinical outcomes in patients with heart failure undergoing ventricular assist device placement. J Card Fail. 2014;20(5):310–315. doi:10.1016/j.cardfail.2014.02.008
37. Chandoo A, Chi CH, Ji W, et al. Gait speed predicts post-operative medical complications in elderly gastric cancer patients undergoing gastrectomy. ANZ J Surg. 2018;88(7–8):723–726. doi:10.1111/ans.14325
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.