Back to Journals » Clinical Interventions in Aging » Volume 18
Frailty and Adverse Outcomes After SARS-CoV-2 Infection in Elderly Patients on Maintenance Hemodialysis: A Cohort Study
Authors Yang Y, Yang H, Diao Z, Liu X, Yao L, Wang L, Shi X ![]() , Li X, Ma Q
, Li X, Ma Q ![]()
Received 6 July 2023
Accepted for publication 18 November 2023
Published 23 November 2023 Volume 2023:18 Pages 1937—1948
DOI https://doi.org/10.2147/CIA.S429226
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Yifan Yang,1,* Huayu Yang,1,* Zongli Diao,2 Xu Liu,2 Lan Yao,1 Liyan Wang,2 Xiaotian Shi,1 Xu Li,1 Qing Ma1
1Department of Geriatrics, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Nephrology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qing Ma, Department of Geriatrics, Beijing Friendship Hospital, Capital Medical University, 95, Yong-an Road, Xicheng District, Beijing, 100050, People’s Republic of China, Tel +86 10 63137641, Fax +86 10 63138730, Email [email protected]
Purpose: Frailty is an important geriatric syndrome associated with aging and adverse events, especially in patients with severe infection. To help guide prognosis for elderly patients undergoing maintenance hemodialysis (MHD) who experience acute infection, this study investigated whether baseline (pre-infection) frailty may be associated with adverse outcomes in elderly patients undergoing MHD who suffer SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) infection.
Patients and Methods: Patients (aged ≥ 60 y) receiving MHD had been assessed for overall frailty and the 5 frailty components based on the Fried Frailty Phenotype scale within 3 months prior to SARS-CoV-2 infection.
Results: There were 59 and 98 patients in the frail and non-frail groups, respectively. Three months after SARS-CoV-2 infection, 21 (13.4%) and 45 (28.7%) patients had died or were in hospital. The multivariate COX proportional risk model suggested that the all-cause mortality rate in patients judged overall frail or with low activity was significantly higher compared with that of the non-frail (P = 0.049; 0.003). The multivariate logistic regression analysis showed that hospitalization 3 months after SARS-CoV-2 infection was associated with both overall frailty and low activity (OR 2.276, 95% CI: 1.034– 5.010, P = 0.041; OR 2.809, 95% CI: 1.311– 6.020, P = 0.008, respectively).
Conclusion: Overall frailty and specifically low activity were significantly associated with all-cause mortality and hospitalization in this elderly MHD population after SARS-CoV-2 infection. Early assessment of frailty and effective interventions are recommended to improve the prognosis of patients receiving MHD who are at higher risk of acute infection.
Keywords: SARS-CoV-2, COVID-19, hemodialysis, frailty, elderly, prognosis
Introduction
In recent years hemodialysis has increasingly been used globally for the treatment of chronic kidney disease in the elderly. In China, the proportion of patients aged 65 or older on hemodialysis is as high as 28.91%,1 and the social and economic burden is correspondingly high. In addition, coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) virus has been a serious challenge to public health.2 The risk of mortality due to SARS-CoV-2 infection is higher for people with comorbidities such as chronic kidney disease.3,4
The influence of frailty within a setting of comorbidities has gained more attention over the last few decades. The prevalence of frailty in elderly patients undergoing maintenance hemodialysis (MHD) is reportedly between 35% and 72%.5–7 These studies suggest that frail patients who require MHD also experience higher rates of falls, hospitalization, and mortality.
In general, patients under MHD who suffer viral infections similar to SARS-CoV-2 are more prone to adverse events, which affect their prognosis. However, the influence of frailty, specifically, on prognosis in these patients is not known. In addition, few researchers have studied a correlation between frailty and adverse prognosis after SARS-CoV-2 infection. Results have been controversial. Tylicki et al8 found that in hospitalized patients under MHD with SARS-CoV-2 infection there was a positive association between the admission Clinical Frailty Scale score and all-cause mortality. Yet, Hendra et al9 reached the opposite conclusion.
The current cohort study investigated an association between baseline frailty status and adverse outcomes of elderly patients under MHD after SARS-CoV-2 infection.
Materials and Methods
Beijing Friendship Hospital affiliated with Capital Medical University granted ethics approval for this study (2022-P2-120-01). All the enrolled patients provided informed consent for participation in the study. Our study complies with the Declaration of Helsinki.
Study Design and Study Population
The cohort comprised elderly patients (aged ≥ 60 y) at the Blood Purification Center of Beijing Friendship Hospital affiliated with Capital Medical University, who had received MHD for at least 3 months, and who had been judged either frail or non-frail according to a baseline Fried Frailty Phenotype (FFP) scale score.10 In addition, within 3 months of the baseline assessment for frailty, all these patients experienced natural SARS-CoV-2 infection, specifically between 7 and 31 December 2022, during the COVID-19 pandemic. The diagnoses of SARS-CoV-2 infections were conducted at the outpatient or emergency department, and were based on Nucleic Acid Testing. Furthermore, only patients who provided informed consent for participation in the study were included.
Patients with any of the following were excluded: severe trauma or long-term hospitalization; or malignant wasting diseases such as muscle atrophy, amputation, or advanced malignant tumor.
To investigate an association between frailty and adverse outcomes after SARS-CoV-2 infection in patients undergoing MHD, the subjects in this cohort were classified as either frail or non-frail, and compared based on various relevant parameters.
Data Collection and Procedures
Trained physicians conducted the geriatric assessments of the patients, and the data was collected from the electronic database of the hospital. The main investigators verified the final data. Baseline characteristics included demographics, medication, and medical history. The following laboratory tests were performed: blood cells, hemoglobin, albumin, uric acid, plasma electrolytes, blood lipids, urea nitrogen, serum creatinine, parathyroid hormone, and urea removal rate (URR).
Assessment of Frailty
The 5 components of the FFP were respectively included in the assessments of the patients’ frailty status:10 unintentional weight loss; slow walking speed; weakness; exhaustion; and low activity level. One point was scored for each criterion met, and ≥3 points was defined as frailty.
Specifically, weight loss was defined as unintentional if it was as much as 4.5 kg, or 5% of body weight, within the past 12 months. Walking speed was adjudged by the time required to walk 4.57 meters. Walking speed was considered slow if 6 seconds were required for men and women of heights 1.59 and 1.73 meters, respectively, or 7 seconds for men and women shorter than or equal to these heights.
Using a hand-held dynamometer, weakness was measured according to the grip strength of the patient’s dominant hand, or the hand without an arteriovenous fistula, depending on the patient’s sex and body mass index (BMI). For women with a BMI of ≤23.0, 23.1–26.0, 26.1–29, or >29.0 kg/m2, weakness was defined as a grip strength of, respectively, ≤17.0, ≤17.3, ≤18.0, and ≤21 kg. For men with a BMI of ≤24.0, 24.1–26.0, 26.1–28.0, and >28 kg/m2, weakness was considered a grip strength of ≤29.0, ≤30.0, ≤31.0, and ≤32.0 kg.
The CES-D (Center for Epidemiologic Studies Depression Scale)11 was employed to determine the presence of exhaustion. Briefly, patients were asked how often they had felt in the previous week that “everything I did was an effort” or “I could not get going.” If their answer was 3 to 4 days, or 5 to 7 days, this was accounted a sign of exhaustion.
Similarly, the low activity component of the FFP was judged based on the patient’s self-report of weekly physical activity. For women, low activity was considered an expenditure of less than 270 kcal/week, or fewer than approximately 2 hours of walking. For men, low activity was less than 383 kcal/week, or fewer than 2.5 hours of walking.
Nutritional Assessment
The assessment of nutrition was calculated based on the Geriatric Nutrition Risk Index (GNRI).12 GNRI = [14.89 × albumin, g/dL] + [41.7 × (body weight/ideal body weight)]. The ideal weight was calculated as: (height, m2) × 22. If the patient’s weight exceeded the ideal body weight, then (body weight/ideal body weight) was set to 1 (one).12
Outcome
The follow-up period ended on 31 March 2023. The main outcome was all-cause mortality at 3 months after SARS-CoV-2 infection. The secondary outcome was hospitalization.
Statistical Analysis
Categorical variables were compared using the chi-square or Fisher’s exact test, and data are reported as number (percentage). Continuous variables were compared using Student’s t-test or the Mann–Whitney U-test. Normally distributed data are reported as mean ± standard deviation, and skewed distribution data as median (interquartile range [IQR]).
Univariate and multivariable Cox proportional hazards models were used to analyze the association between frailty status and all-cause mortality. Furthermore, associations between each of the 5 frailty components of the FFP and all-cause mortality were determined, and univariate and multivariable logistic regression analyses were applied to determine the influence of overall frailty status and frailty components on the rate of hospital admissions. The univariate analysis included factors with a significance of P < 0.05. These factors, and dialysis duration, were incorporated into the multivariate study. The URR was substituted for nitrogen and serum creatinine. All statistical analyses were conducted with SPSS 26.0 software. Statistical significance was considered P < 0.05.
Results
Baseline Characteristics and Frailty Status of Patients
Among 178 patients aged 60 years or older receiving MHD in our Blood Purification Center in December 2022, 164 were confirmed by nucleic acid test to have SARS-CoV-2 infection. Among them, 21 were excluded as follows: 14 patients tested negative for SARS-CoV-2 infection; and 4, 2, and 1 due to long-term hospitalization or severe trauma, malignant tumor, and missing important data, respectively (Figure 1). Finally, 157 patients were included, 80 (51.0%) men, with a median age of 67 years (IQR 63–74 y; Table 1).
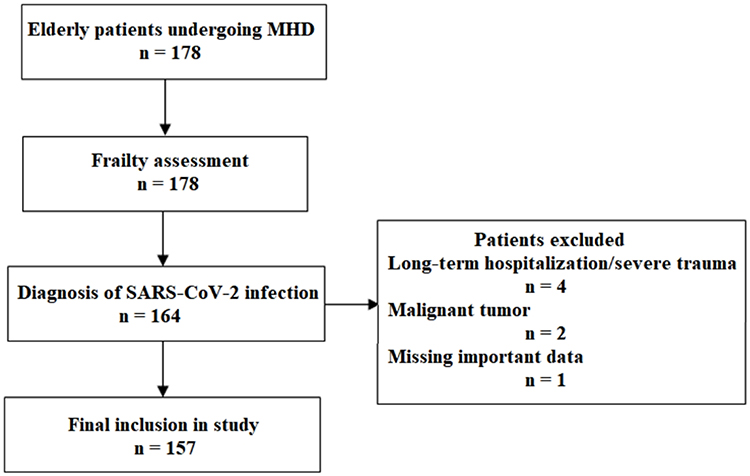 |
Figure 1 Study inclusion and exclusion flowchart. |
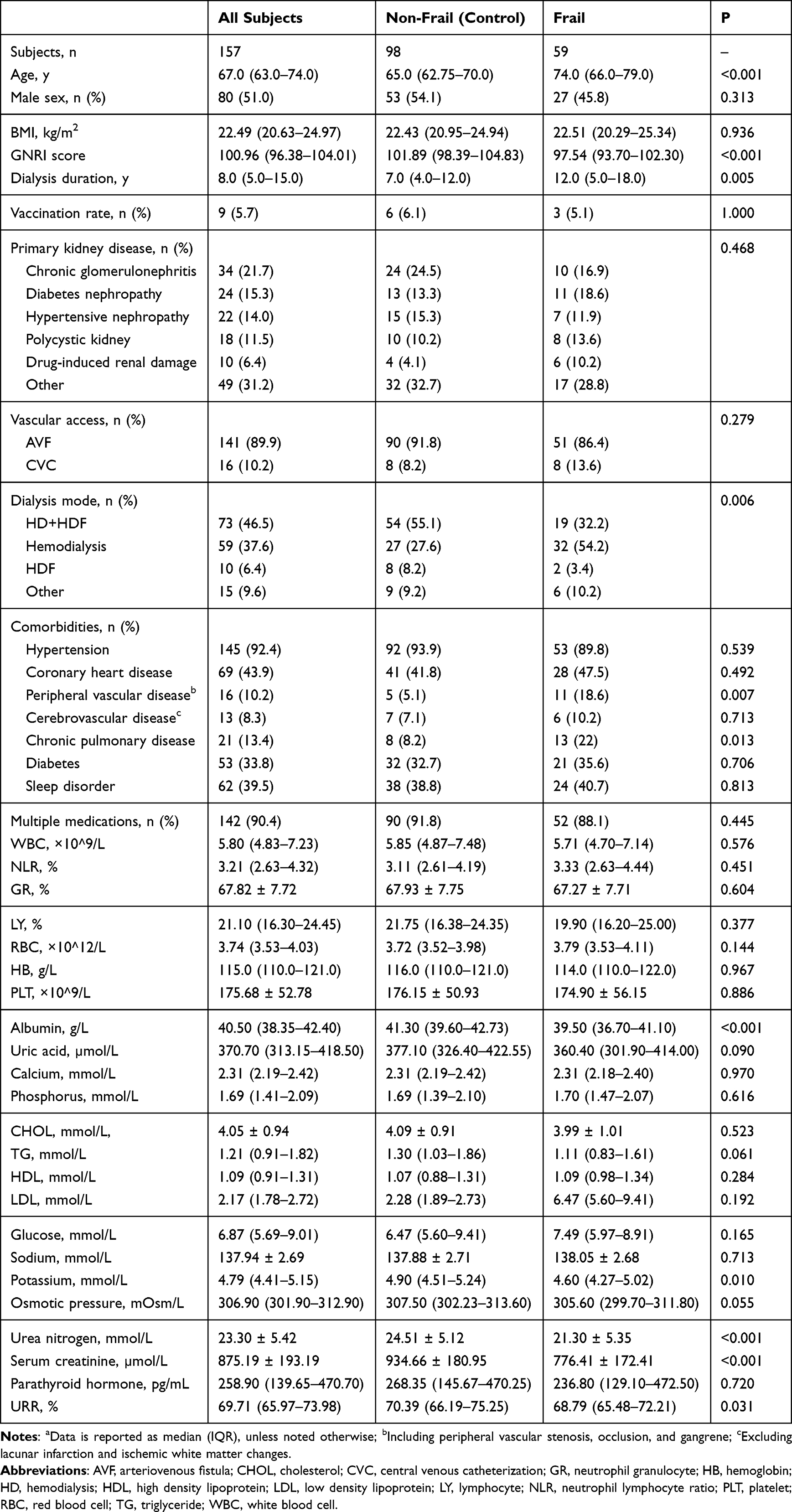 |
Table 1 Baseline Demographics and Clinical Characteristics of Elderly Patients Undergoing MHDa |
The most common etiology of end stage renal disease was chronic glomerulonephritis (21.7%), then diabetic nephropathy (15.3%) and hypertensive renal disease (14.0%; Table 1). The most frequently used dialysis access (89.9%) was arteriovenous fistula. The most common patients’ choice of dialysis mode was hemodialysis combined with hemodiafiltration (HDF; 46.5%) 3 times/week. The most common comorbidities were hypertension (92.4%), coronary heart disease (43.9%), and sleep disorders (39.5%). Only 9 (5.7%) patients received the vaccine.
Based on the total FFP score, the subjects were classified as frail (59, 37.6%) or non-frail (98, 62.4%; Figure 2). The most common components of the FFP were weakness (64.3%), exhaustion (57.3%), and slow walking speed (35.7%; Figure 3).
 |
Figure 2 Prevalence of frailty in elderly hemodialysis patients according to the FFP. |
 |
Figure 3 Number and percentage of subjects within each frailty component. |
Compared with the non-frail group, the frail group was significantly older and had longer dialysis duration (Table 1). The frail group was further characterized by a higher rate of choosing HD alone (3 times/week) as the dialysis mode; lower serum potassium, albumin, GRNI score, urea nitrogen, serum creatinine, and URR; and higher prevalence of peripheral vascular disease (PVD) and chronic pulmonary disease (CPD).
Frailty and All-Cause Mortality
Among the total study population of 157 patients, at the end of the follow-up 21 (13.4%) had died, specifically 16 (10.2%) and 5 (3.2%) patients in the frail and non-frail groups, respectively (Figure 4). The univariate COX proportional risk model showed that among the FFP components, frailty (P = 0.001), low activity (P < 0.001), weakness (P = 0.047), and slow walking speed (P = 0.001) were significant risk factors for all-cause mortality (Table 2). The subsequent multivariate COX regression analysis showed that, after adjusting for age, dialysis duration, URR, GNRI, serum potassium, and history of PVD or CPD, frailty remained significantly associated with all-cause mortality (P = 0.049). Regarding an association between FFP components and all-cause mortality, after adjusting for covariates, patients with low activity had a 37.5% higher rate of all-cause mortality compared with the control (P = 0.003).
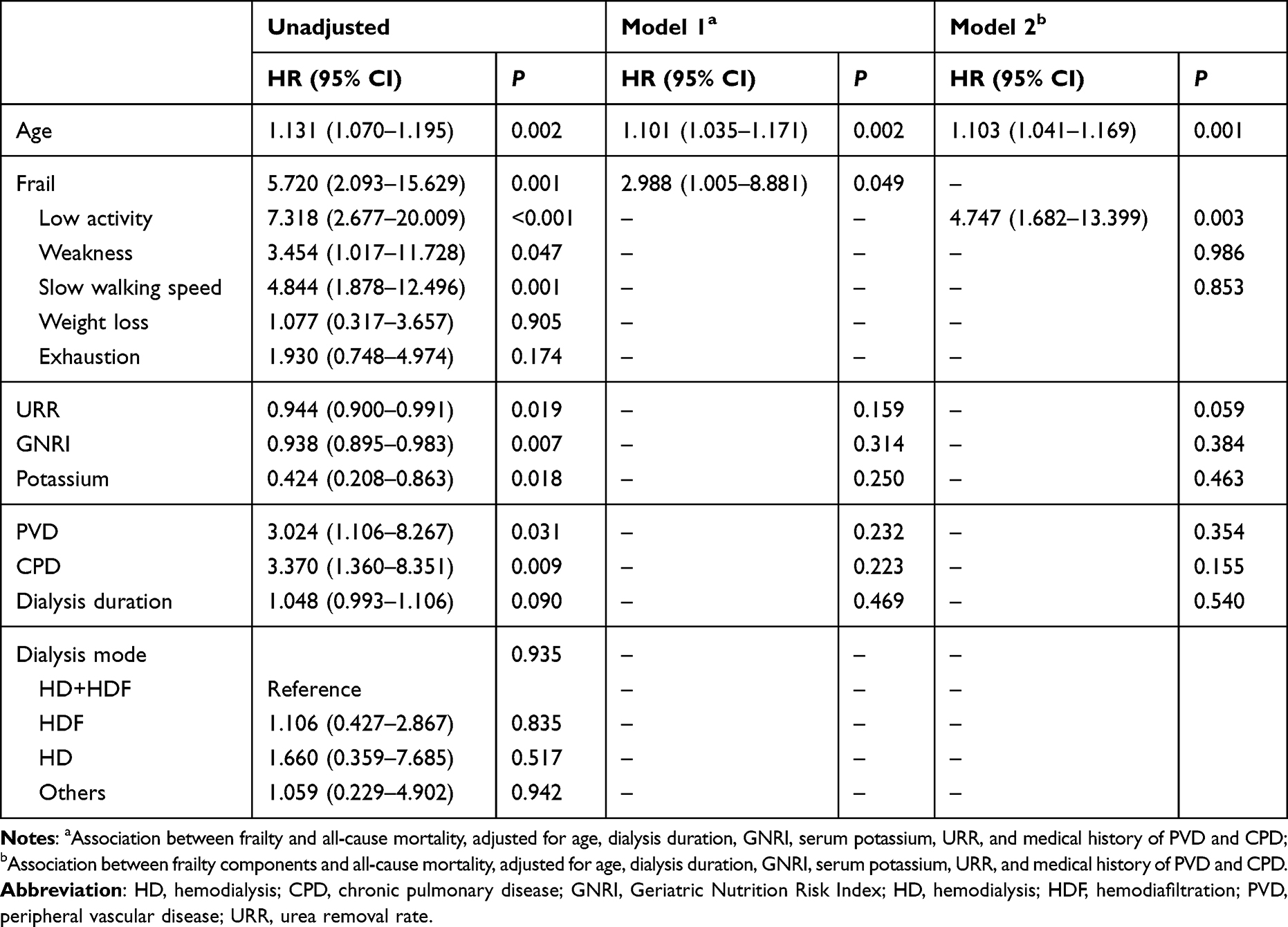 |
Table 2 Univariate and Multivariable Cox Regression Analysis of Associated Factors with All-Cause Mortality |
Frailty and Hospitalization
Forty-five (28.7%) of the patients, that is, 26 (16.6%) in the frail group and 19 (12.1%) in the non-frail group, were admitted to the hospital or visited the emergency department for 24 hours or more (Table 3; Figure 4). The univariate logistic regression analysis showed that frailty (P = 0.001) including low activity (P = 0.001), and low walking speed (P = 0.030) were risk factors for hospitalization. After adjusting for age, dialysis duration, URR, serum potassium, and history of CPD, the multivariate logistic regression analysis showed that frailty (P = 0.041) and low activity (P = 0.008) were independent risk factors for hospitalization.
 |
Figure 4 Mortality and hospitalization in the frail and non-frail groups. |
 |
Table 3 Univariate and Multivariable Logistic Regression Analyses of Associated Factors with Hospitalization |
Effect of Age on Mortality and Hospitalization
Age was an independent risk factor for 3-month all-cause mortality (P = 0.002) and hospitalization (P = 0.025).
Discussion
This was a cohort study of 157 patients receiving MHD who had been assessed for baseline frailty within 3 months prior to diagnosis of SARS-CoV-2 infection during the COVID-19 epidemic. To determine a prognosis for such patients, we investigated associations between the condition of frailty and outcome parameters at the 3-month follow-up after infection. The prevalence of frailty was 37.6%, and nearly one-third of the patients’ activity levels were not up to standard.
The frailty rate determined by the present study is higher than the 34.7% previously reported at our center in 2019.6 This may be due, at least partially, to the COVID-19 pandemic. A systematic review showed that the restrictions, quarantines, and lockdowns imposed during the COVID-19 pandemic greatly affected the lifestyles and physical activity of the elderly, and the rate of frailty increased.13 The elderly who live alone and socialize little were also more susceptible.14 Similarly, researchers in Spain who studied patients with MHD linked lower physical function, social function, and physical activity to the influence of the COVID-19 pandemic.15 During the COVID-19 epidemic, elderly patients receiving MHD were less physically active and thus at higher risk of frailty.
Frail patients have poor physiological reserves, low resistance to microbial attacks, and are more prone to adverse outcomes after various acute stress events.10,16 For example, frail elderly patients have a higher risk of postoperative complications, comorbidities, hospitalization, and mortality (30-day and long-term).17 In another study, frailty in elderly patients presented an independent risk of adverse events after trauma.18 A determination of frailty also has great prognostic value in a setting of acute infection. For example, frail elderly patients had a high rate of mortality or functional decline within 30 days of hospitalization for pneumonia, which was independent of pneumonia severity; a frailty assessment could inform the widely used standard of pneumonia severity (CURB-65).19,20
Relevant to the present study, acute SARS-CoV-2 infection could cause damage to multiple systems in elderly patients,21 and frail elderly patients had a higher risk of mortality after infection.22 If clinicians can improve the frailty of elderly patients, the outcome of emergency events may also improve.
The present study showed that the 3-month all-cause mortality and hospitalization rates of elderly patients under MHD after SARS-CoV-2 infection were 13.4% and 28.7%, respectively. This was lower than the 35.4% and 76.2% rates reported previously.23 Possible reasons for this discrepancy between the studies may be differences in ethnicity, age, and nutritional status of the enrolled patients, and the dialysis adequacy and the resources of the hospitals. In addition, the pathogenicity of the viral strain may have differed due to mutation. According to the Chinese Center for Disease Control and Prevention, the virus in our study was likely the Omicron variant. In addition, the dialysis access was via arteriovenous fistula (AVF) for 89.9% of the patients. Murt et al24 concluded that AVFs contributed to higher survival in MHD patients with COVID-19. This may partially explain the lower all-cause mortality rate in our study.
The present study showed that the baseline frailty of elderly patients under MHD was significantly associated with all-cause mortality and hospitalization 3 months after SARS-CoV-2 infection. This is consistent with previous findings in adult patients undergoing dialysis. Bouwmans et al25 reported that baseline frailty was an independent risk factor for 3-month mortality in hospital, and in the intensive care unit. Hilbrands et al26 found that baseline frailty was associated with 28-day mortality. However, in another retrospective study,9 frailty was not associated with poor prognosis in adult patients under MHD care. These differences may be due to study population, frailty assessment tools, and follow-up time. Previous studies have assessed frailty based on the Clinical Frailty Scale, which is easy to use in the clinic but relies on the subjective judgment of the clinicians.27 In the present research the FFP was applied to objectively reflect the patient’s functional status.10 A correlation between frailty and adverse prognosis after acute viral infection in elderly patients under MHD needs further exploration in multi-center and large sample studies.
When analyzing the individual components of frailty in our patients 3 months after SARS-CoV-2 infection, we found a significant association between the score for the low activity component of the FFP and poor outcomes. Suzuki et al28 showed that baseline low activity status and gradual decrease in activity levels were significantly associated with a higher risk of all-cause mortality and cardiovascular events in patients under MHD. Another study showed that in patients with advanced chronic kidney disease, higher levels of physical activity could reduce the risk of mortality.29 Furthermore, multiple reviews regarding patients on dialysis have reported that physical activity could improve physical functions (grip strength and walking speed), fatigue and pain, depression, and quality of life.30–33 Therefore, we believe that physical activity can improve frailty, at least partially. Although the best pattern of activity is uncertain, we should still encourage patients to engage in appropriate physical activity based on a comprehensive consideration of their general situation.30
The univariate analysis of the present study suggested that after SARS-CoV-2 infection low grip strength and low walking speed were associated with all-cause mortality, and low walking speed was also associated with hospitalization. Grip strength and walking speed can reflect muscle strength and performance34 and are included in the diagnostic criteria for sarcopenia. Some researchers have proposed that these components were more prognostic than sarcopenia in patients under MHD.35,36 Johansen et al37 reported that, in patients under MHD, all 5 components of the FFP were associated with all-cause mortality, and joint evaluation was the best approach. We conclude that geriatricians need to pay attention to all components of the FFP, and actively take interventive measures to improve each patient’s prognosis.
The present study also found that age was an independent risk factor for adverse outcomes of elderly patients under MHD after SARS-CoV-2 infection. This result is consistent with previous research.8,9,23,38 Aging tends to develop into a chronic low-grade pro-inflammatory state, which is an important risk factor for morbidity, physical and cognitive disability, frailty, and death.39 Yet frailty, as an alternative indicator of biological age, may be more predictive than actual age.40
The present research is limited by its small sample size and data from a single medical center. However, our results regarding the association between baseline frailty and adverse outcomes in patients under MHD after acute events warrant verification by larger studies and multiple centers.
Conclusion
Frailty in patients aged 60 years or more and undergoing MHD should be assessed as a baseline measure, including the components of frailty. Low physical activity is an especially important prognostic factor for 3-month all-cause mortality and hospitalization in the event of an acute infection. Nephrologists and geriatric physicians should be cognizant of the high incidence and implications of frailty in elderly patients under MHD care. Early assessment, active intervention, and optimized management may improve patients’ ability to cope and survive acute physical insults.
Data Sharing Statement
To protect the confidentiality of the participants, these data are not publicly available. The data supporting the results of this study may be provided by appropriate request of the corresponding author.
Acknowledgments
The authors thank all the patients, researchers, and staff who were involved in this study. We thank Medjaden Inc. for assisting in the preparation of this manuscript.
Author Contributions
All the authors contributed significantly to this work whether by conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the final published version; agreed on the journal to which the article was submitted; and are accountable for all aspects of the work.
Funding
Capital Health Research and Development of Special Fund (2022-2-2028).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang L, Zhao MH, Zuo L, et al. China Kidney Disease Network (CK-NET) 2015 Annual Data Report. Kidney Int Suppl. 2019;9(1):e1–e81. doi:10.1016/j.kisu.2018.11.001
2. Wu F, Zhao S, Yu B, et al. A new coronavirus associated with human respiratory disease in China. Nature. 2020;579(7798):265–269. doi:10.1038/s41586-020-2008-3
3. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
4. Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. 2020;369:m1966. doi:10.1136/bmj.m1966
5. Guo Y, Tian R, Ye P, Luo Y. Frailty in older patients undergoing hemodialysis and its association with all-cause mortality: a prospective cohort study. Clin Interv Aging. 2022;17:265–275. doi:10.2147/CIA.S357582
6. Li Y, Zhang D, Ma Q, Diao Z, Liu S, Shi X. The impact of frailty on prognosis in elderly hemodialysis patients: a prospective cohort study. Clin Interv Aging. 2021;16:1659–1667. doi:10.2147/CIA.S329665
7. Soldati A, Poggi MM, Azzolino D, Vettoretti S, Cesari M. Frailty index and adverse outcomes in older patients in haemodialysis. Arch Gerontol Geriatr. 2022;101:104673. doi:10.1016/j.archger.2022.104673
8. Tylicki L, Puchalska-Reglińska E, Tylicki P, et al. Predictors of mortality in hemodialyzed patients after sars-cov-2 infection. J Clin Med. 2022;11(2):285. doi:10.3390/jcm11020285
9. Hendra H, Vajgel G, Antonelou M, et al. Identifying prognostic risk factors for poor outcome following COVID-19 disease among in-centre haemodialysis patients: role of inflammation and frailty. J Nephrol. 2021;34(2):315–323. doi:10.1007/s40620-020-00960-5
10. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–156. doi:10.1093/gerona/56.3.M146
11. Orme JG, Reis J, Herz EJ. Factorial and discriminant validity of the center for epidemiological studies depression (CES-D) scale. J Clin Psychol. 1986;42(1):28–33. doi:10.1002/1097-4679(198601)42:1<28::AID-JCLP2270420104>3.0.CO;2-T
12. Bouillanne O, Morineau G, Dupont C, et al. Geriatric Nutritional Risk Index: a new index for evaluating at-risk elderly medical patients. Am J Clin Nutr. 2005;82(4):777–783. doi:10.1093/ajcn/82.4.777
13. Oliveira MR, Sudati IP, Konzen VM, et al. Covid-19 and the impact on the physical activity level of elderly people: a systematic review. Exp Gerontol. 2022;159:111675. doi:10.1016/j.exger.2021.111675
14. Yamada M, Kimura Y, Ishiyama D, et al. The influence of the covid-19 pandemic on physical activity and new incidence of frailty among initially non-frail older adults in japan: a follow-up online survey. J Nutr Health Aging. 2021;25(6):751–756. doi:10.1007/s12603-021-1634-2
15. Segura-Ortí E, Martínez-Olmos FJ, Ródenas-Pascual Á, et al. Impact of COVID-19 pandemic on health-related quality of life and physical activity of patients in hemodialysis. Healthcare (Basel). 2022;10(11). doi:10.3390/healthcare10112217
16. Dent E, Morley JE, Cruz-Jentoft AJ, et al. Physical frailty: ICFSR international clinical practice guidelines for identification and management. J Nutr Health Aging. 2019;23(9):771–787. doi:10.1007/s12603-019-1273-z
17. Ko FC. Preoperative frailty evaluation: a promising risk-stratification tool in older adults undergoing general surgery. Clin Ther. 2019;41(3):387–399. doi:10.1016/j.clinthera.2019.01.014
18. Zhao F, Tang B, Hu C, Wang B, Wang Y, Zhang L. The impact of frailty on posttraumatic outcomes in older trauma patients: a systematic review and meta-analysis. J Trauma Acute Care Surg. 2020;88(4):546–554. doi:10.1097/TA.0000000000002583
19. Park CM, Kim W, Rhim HC, et al. Frailty and hospitalization-associated disability after pneumonia: a prospective cohort study. BMC Geriatr. 2021;21(1):111. doi:10.1186/s12877-021-02049-5
20. Park CM, Kim W, Lee ES, et al. Comparison of frailty index to pneumonia severity measures in older patients with pneumonia. J Am Med Dir Assoc. 2022;23(1):165–169. doi:10.1016/j.jamda.2021.08.044
21. Anaya JM, Rojas M, Salinas ML, et al. Post-COVID syndrome. A case series and comprehensive review. Autoimmun Rev. 2021;20(11):102947. doi:10.1016/j.autrev.2021.102947
22. Saragih ID, Advani S, Saragih IS, Suarilah I, Susanto I, Lin CJ. Frailty as a mortality predictor in older adults with COVID-19: a systematic review and meta-analysis of cohort studies. Geriatr Nurs. 2021;42(5):983–992. doi:10.1016/j.gerinurse.2021.06.003
23. Vergara A, Molina-van den Bosch M, Toapanta N, et al. The impact of age on mortality in chronic haemodialysis population with COVID-19. J Clin Med. 2021;10(14):3022. doi:10.3390/jcm10143022
24. Murt A, Yadigar S, Yalin SF, et al. Arteriovenous fistula as the vascular access contributes to better survival of hemodialysis patients with COVID-19 infection. J Vasc Access. 2023;24(1):22–26. doi:10.1177/11297298211021253
25. Bouwmans P, Brandts L, Hilbrands LB, et al. The clinical frailty scale as a triage tool for ICU admission of dialysis patients with COVID-19: an ERACODA analysis. Nephrol Dial Transplant. 2022;37(11):2264–2274. doi:10.1093/ndt/gfac246
26. Hilbrands LB, Duivenvoorden R, Vart P, et al. COVID-19-related mortality in kidney transplant and dialysis patients: results of the ERACODA collaboration. Nephrol Dial Transplant. 2020;35(11):1973–1983. doi:10.1093/ndt/gfaa261
27. Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. Cmaj. 2005;173(5):489–495. doi:10.1503/cmaj.050051
28. Suzuki Y, Matsuzawa R, Hoshi K, et al. Physical activity and its trajectory over time and clinical outcomes in hemodialysis patients. Int Urol Nephrol. 2022;54(8):2065–2074. doi:10.1007/s11255-021-03098-w
29. Rampersad C, Brar R, Connelly K, et al. Association of physical activity and poor health outcomes in patients with advanced CKD. Am J Kidney Dis. 2021;78(3):391–398. doi:10.1053/j.ajkd.2020.12.018
30. Bernier-Jean A, Beruni NA, Bondonno NP, et al. Exercise training for adults undergoing maintenance dialysis. Cochrane Database Syst Rev. 2022;1(1):Cd014653. doi:10.1002/14651858.CD014653
31. Hargrove N, El Tobgy N, Zhou O, et al. Effect of aerobic exercise on dialysis-related symptoms in individuals undergoing maintenance hemodialysis: a systematic review and meta-analysis of clinical trials. Clin J Am Soc Nephrol. 2021;16(4):560–574. doi:10.2215/CJN.15080920
32. Bakaloudi DR, Siargkas A, Poulia KA, Dounousi E, Chourdakis M. The effect of exercise on nutritional status and body composition in hemodialysis: a systematic review. Nutrients. 2020;12(10):3071. doi:10.3390/nu12103071
33. Clarkson MJ, Bennett PN, Fraser SF, Warmington SA. Exercise interventions for improving objective physical function in patients with end-stage kidney disease on dialysis: a systematic review and meta-analysis. Am J Physiol Renal Physiol. 2019;316(5):F856–f872. doi:10.1152/ajprenal.00317.2018
34. Chen LK, Woo J, Assantachai P, et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(3):300–307.e302. doi:10.1016/j.jamda.2019.12.012
35. Kittiskulnam P, Chertow GM, Carrero JJ, Delgado C, Kaysen GA, Johansen KL. Sarcopenia and its individual criteria are associated, in part, with mortality among patients on hemodialysis. Kidney Int. 2017;92(1):238–247. doi:10.1016/j.kint.2017.01.024
36. Giglio J, Kamimura MA, Lamarca F, Rodrigues J, Santin F, Avesani CM. Association of sarcopenia with nutritional parameters, quality of life, hospitalization, and mortality rates of elderly patients on hemodialysis. J Ren Nutr. 2018;28(3):197–207. doi:10.1053/j.jrn.2017.12.003
37. Johansen KL, Delgado C, Kaysen GA, et al. Frailty among patients receiving hemodialysis: evolution of components and associations with mortality. J Gerontol a Biol Sci Med Sci. 2019;74(3):380–386. doi:10.1093/gerona/gly206
38. Hsu CM, Weiner DE, Aweh G, et al. COVID-19 among us dialysis patients: risk factors and outcomes from a national dialysis provider. Am J Kidney Dis. 2021;77(5):748–756.e741. doi:10.1053/j.ajkd.2021.01.003
39. Bektas A, Schurman SH, Sen R, Ferrucci L. Aging, inflammation and the environment. Exp Gerontol. 2018;105:10–18. doi:10.1016/j.exger.2017.12.015
40. Polidori MC, Sies H, Ferrucci L, Benzing T. COVID-19 mortality as a fingerprint of biological age. Ageing Res Rev. 2021;67:101308. doi:10.1016/j.arr.2021.101308
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
A Pilot Study of 0.4% Povidone-Iodine Nasal Spray to Eradicate SARS-CoV-2 in the Nasopharynx
Sirijatuphat R, Leelarasamee A, Puangpet T, Thitithanyanont A
Infection and Drug Resistance 2022, 15:7529-7536
Published Date: 21 December 2022
Distinct Features of Vascular Diseases in COVID-19
Ceasovschih A, Sorodoc V, Shor A, Haliga RE, Roth L, Lionte C, Onofrei Aursulesei V, Sirbu O, Culis N, Shapieva A, Tahir Khokhar MA, Statescu C, Sascau RA, Coman AE, Stoica A, Grigorescu ED, Banach M, Thomopoulos C, Sorodoc L
Journal of Inflammation Research 2023, 16:2783-2800
Published Date: 6 July 2023
Elevated High Sensitivity Cardiac Troponin T is Nonlinearly Associated with Poor Prognosis in Aging COVID-19 Patients: A Retrospective Study
Jin X, Yang H, Ma W, Yuan Y, Li T
Infection and Drug Resistance 2023, 16:5155-5163
Published Date: 9 August 2023
Prognosis of Older Adult Patients Suffering from Atrial Fibrillation and Hypokalemia
Wang XD, Wang Y, Liu J, Yao JW, Zhang J, Zhang YN
Clinical Interventions in Aging 2023, 18:1363-1371
Published Date: 17 August 2023