")
Back to Journals » Open Access Emergency Medicine » Volume 12
Foreign Body and Caustic Substance Ingestion in Childhood
Authors Dorterler ME , Günendi T
Received 5 December 2019
Accepted for publication 14 July 2020
Published 4 November 2020 Volume 2020:12 Pages 341—352
DOI https://doi.org/10.2147/OAEM.S241190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Mustafa Erman Dorterler, Tansel Günendi
Harran University Faculty of Medicine, Department of Pediatric Surgery, Sanliurfa, Turkey
Correspondence: Mustafa Erman Dorterler
Harran University Faculty of Medicine, Department of Pediatric Surgery, Sanlıurfa, Turkey
Tel +905053483200
Fax +90 4143444444
Email [email protected]
Abstract: Foreign body and caustic substance ingestion in childhood are common and require accurate and timely diagnosis to provide appropriate management consistent with the ingested substance/foreign body and clinical presentation as well as the associated risk status to prevent significant complications and morbidity. The aim of this paper was to present foreign body and caustic ingestion in childhood in terms of epidemiology, pathophysiology, diagnostic work-up and appropriate management and potential complications in accordance with clinical presentation and the type of ingested substance/foreign body.
Keywords: foreign body ingestion, caustic ingestion, childhood, diagnosis, treatment
Introduction
The ingestion of foreign bodies in childhood is an important cause of morbidity and mortality seen in children aged 6 months to 5 years when they have a tendency to put all objects into the mouth. It is seen more frequently in males than females and although it varies according to sociocultural characteristics, generally metal (coins, paper clips, batteries, needles) and non-metal (wooden and plastic pieces of toys) objects are swallowed and early intervention is required.1–4
Foreign body ingestion has a wide range of symptoms. In the majority of cases, gastrointestinal, respiratory and non-specific symptoms can aid to achieve diagnosis. Gastrointestinal symptoms can be vomiting, dysphagia, odynophagia, increase in saliva, changes in the daily diet resulting from loss of appetite or hematemesis that may occur in very rare cases originating from a life-threatening aorto-esophageal fistula. Respiratory symptoms may present itself as wheezing, stridor or feeling of suffocation. Non-specific symptoms may include fever, pain in the chest, neck or head. In some cases, even if the ingestion has been witnessed, symptom-free clinical presentation is also possible.
Foreign bodies may also be determined incidentally during a radiological evaluation applied for other reasons such as dysphagia, wheezing, pneumonia or asthma.1,3 While the majority of foreign bodies pass spontaneously through the gastrointestinal canal without any complication, in 10–20% of cases, the foreign body remains in anatomically narrow areas such as primarily the upper esophageal region, the pylorus, ileocecal valve and the rectosigmoid colon, resulting in indications for endoscopic removal, and surgical removal is required in <1% of cases.1–5 Following foreign body ingestion, complications may develop such as mucosal abrasion, bleeding, obstruction of the stomach outlet, esophageal or gastrointestinal perforation, mediastinitis, peritonitis, abscess and fistula formation. Therefore, although the method to be applied varies according to the time since ingestion, the localisation, the history and the physical examination, the presence of a foreign body is a strong indication for endoscopic intervention for removal (esophagoscopy, McGill forceps, Foley catheter extraction, esophageal dilation).2–4,6–9
Caustic substance ingestion is seen particularly in infants aged <3 years and more often in males. The majority of cases are accidental and it can cause acute burns in the stomach and long-term complications.10–13 Cleaning products at home (detergents, oven cleaner, drain cleaner and toilet cleaner) are the most frequently encountered caustic substances ingested by accident. These substances cause tissue damage of different severities, according to whether they are acid (damage limited to the mucosa, airway effect) or alkaline (liquefaction necrosis in the tissue, penetration and perforation of deep organ layers) the amount, concentration, physical form and duration of contact with the mucosa.14
Following caustic substance ingestion, there is a risk of perforation because of esophagus injury continuing to advance associated with tissue inflammation and vascular thrombosis, and this risk decreases significantly after 3 weeks.15,16 Strong alkali substances (NaOH, KOH) such as dry cleaning agents, ammonia and dishwasher detergent cause the most severe injuries. Some substances such as formic acid, vinegar, anti-rust compound include acids. The ingestion of large amounts of alkaline substance has the risk of gastric bleeding and perforation, while large amounts of acid ingestion can cause gastric damage and obstruction of the stomach outlet.14
In the treatment of caustic substance ingestion, sufficient clinical experience is important in addition to a multidisciplinary approach including the emergency service, surgery, anaesthesia, gastroenterology, radiology and psychiatry branches. Although rarely encountered, because of the lack of evidence-based diagnostic and treatment guidelines, there is ongoing uncertainty in clinical practice about the best treatment approach.12,17 When there is incompatibility between symptoms and findings of esophageal damage and the absence of oropharyngeal lesion or pharyngeal – esophageal symptoms, endoscopic evaluation is the gold standard for differentiating esophageal or gastric damage, grading the damage and predicting the risk of stricture. The basic treatment approach for stricture is serial dilation.12,13
The aim of this paper was to present appropriate treatment approaches and possible complications associated with the epidemiology, pathophysiology, diagnostic procedures, clinical presentation and substance characteristics of foreign body ingestion and caustic substance ingestion in childhood, and to evaluate these in the light of the relevant literature.
The Ingestion of Foreign Bodies in Childhood
Epidemiology
The ingestion of foreign bodies in childhood is seen especially in infants under the age of 3 years as with increasing bodily movements they often perform playing and eating activities simultaneously and have a tendency to identify objects with the mouth. These objects cannot be chewed as teeth have not yet developed, so they may be swallowed as the child has not yet developed the cognitive ability to differentiate inedible objects.15
Most foreign bodies that pass through the esophagus are spontaneously expelled from the gastrointestinal canal, while there is indication for endoscopic intervention removal in 10–20% of cases and <1% of cases require surgical removal.18–21
Although the foreign bodies swallowed show differences between countries according to nutritional habits and sociocultural characteristics, in many different populations, coins have been reported to be the most commonly swallowed foreign body followed by batteries, magnets, pieces of toys, safety pins, chicken bones, fishbones and jewellery.9,22–25
Presentation Symptoms
Symptoms on presentation show differences according to the foreign body ingested, the gastrointestinal localisation, the age of the patient, and concomitant complications.1,9,25–27 When the foreign body is lodged in the esophagus, non-specific symptoms may be seen such as a feeling of suffocation, increased saliva and impaired feeding, and symptoms such as a tendency to favour soft food and fluids because of the decreased esophagus diameter, dysphagia, odynophagia and chest pain.1,2,9 In addition, a long time after swallowing the foreign body, respiratory symptoms may emerge such as wheezing, stridor and speech disorders because of trachea pressure associated with paraesophageal soft tissue oedema directly related to the foreign body or to prolonged retention.1,2
Foreign bodies with oropharyngeal localisation are almost always asymptomatic, while coins or other foreign bodies not causing an obstruction in the stomach or small intestine generally have an asymptomatic course.1,2 Thus, a foreign body passing the distal portion of the esophagus has an asymptomatic course related to the type of foreign body, the localisation and the time since swallowing, whereas symptomatic cases can represent a wide range from gastrointestinal symptoms such as dysphagia, vomiting and increased saliva, respiratory symptoms such as cough, the feeling of suffocation and wheezing, to complications such as intestinal perforation and bleeding seen with findings such as acute abdomen, subcutaneous emphysema and hypovolemic shock.2,18,22,28
Localisation
The most common areas of localisation of foreign bodies are the stomach (60%), esophagus (20%), oropharynx (5–10%), and distal stomach (generally small intestine, 10%).1,15,22 The highest risk area in respect of requiring endoscopic intervention is the upper esophagus, which is the narrowest part of the digestive tract.9,19,25
Diagnosis
Foreign body ingestion is diagnosed primarily on the basis of witness statements and from radiological examination and endoscopic findings. Although negative findings cannot completely differentiate the diagnosis, radiography of the neck, chest and abdominal region is the most commonly performed radiological method.9,22,24 On presentation of the patient, the type and localisation of the foreign body is determined by radiological evaluation of the whole gastrointestinal system, from the pharynx to the anus.29 As there is radio-opacity with movement of 60–90% of ingested foreign bodies, it is usually possible to determine what the foreign body is and the localisation with radiological evaluation1,29 (Figure 1).
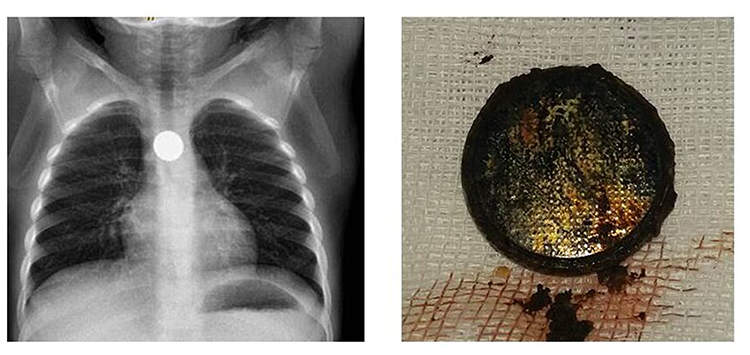 |
Figure 1 Foreign body in the oesophagus (battery).Notes: Reproduced with permission from Dörterler.7530 |
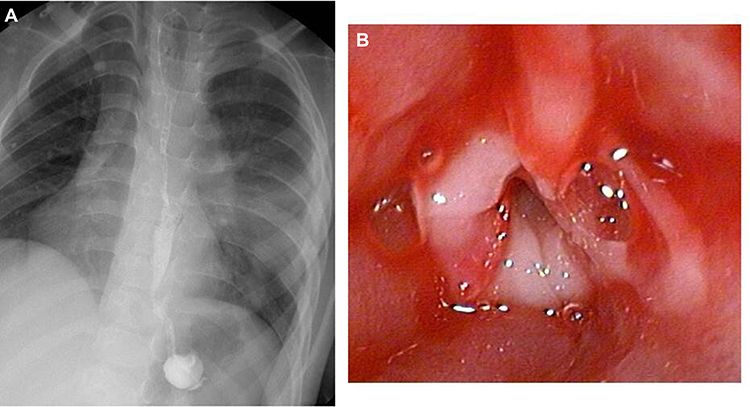 |
Figure 2 Corrosive oesophagitis: (A) radiological image (B) endoscopic image. |
Alternative diagnostic methods are accepted as 3-dimensional computed tomography (CT) for non-radio-opaque foreign bodies, and magnetic resonance imaging (MRI) for non-metallic foreign bodies.21,31,32 CT has 96% specificity and high negative predictive value in patients with negative endoscopy findings, but persistent symptoms and contrast radiography has been reported to be a less invasive alternative method than endoscopy for non-radio-opaque bodies located in the stomach.22,33
Treatment Approaches
The decision-making through available methods for the removal of foreign bodies from the gastrointestinal canal is mostly made according to the type of foreign body, localisation, the time since ingestion and the clinician’s experience.9,34
Although flexible or rigid endoscopy is the standard treatment approach for the removal of foreign bodies from the esophagus, McGill forceps, Foley catheter extraction and bougie dilation are alternative approaches to retrieve the foreign body from the esophagus.2,3,34,35 Flexible endoscopy is usually preferred for the removal of foreign bodies located in the esophagus or proximal gastrointestinal canal as it provides direct visualisation and the possibility of manipulation and the examination of potential complications in the structures of the region.
Rigid endoscopy is the most commonly selected method for sharp objects located in the proximal esophagus or those located in the pharynx or cricopharynx. This technique requires skill and clinical experience because of the risk of esophageal perforation and abrasion associated with the instrument.34 Endoscopy can lead to complications such as bleeding, postoperative stridor, esophageal perforation, pneumothorax and mediastinitis, and flexible endoscopy has advantages over rigid endoscopy as it is associated with a lower risk of dysphagia and complications and does not require general anaesthesia.26,34 It is possible to remove foreign bodies from oropharynx or upper esophageal localisation using McGill forceps.35
It is possible to use the Foley catheter method to remove blunt foreign objects. This method is based on inflation of the balloon end after having passed to the distal of the foreign body and then pulling back the foreign body with it while being withdrawn. Although the method has high success rates, it has the disadvantages of poor airway control, poor control of the foreign body while it is being removed, and insufficient visualisation of the esophagus.3,34,36 It has been advised that neither of these methods should be used in cases with esophagus abnormalities or when more than 24 hours has elapsed since ingestion of the foreign body.3,6
Due to the risk of obstruction, mucosal erosion, perforation and the development of fistula, localisation of the foreign body in the esophagus is an indication for removal within 24 hours of ingestion.7,23,25,29,33,34 Foreign bodies longer than 5cm or sharp foreign bodies, high-power magnets, batteries localised in the esophagus or the stomach, objects with a high lead content, and those which have been lodged in the system for more than 24 hours or an unknown period of time are indications for emergency intervention. In other cases where the foreign body can not be advanced in the canal and the patient has become symptomatic, a more conservative approach can be followed under close observation with emergency evaluation and removal of the foreign body.34
The treatment approach for removal of batteries in the esophagus is endoscopy and retrieval with magnetic probes under fluoroscopy guidance, whereas the Foley catheter and bougie dilation techniques are appropriate for coins and other regular-shaped objects and for cases with no respiratory problems and who have not previously undergone esophagus surgery.3,22,37 Lithium cells are typically 3.0 V, as compared with the 1.5 V of traditional alkaline button batteries. Ohm’s law dictates an increased damage in the mucosa with these new types of batteries. Size of button batteries change from 6 to 25 mm and those that are larger than 12 mm in diameter may become lodged in the esophagus. According to National Battery Ingestion Hotline (NBIH), batteries that are visualised in the esophagus must have an intervention within two hours. In asymptomatic patients, batteries that lie in the stomach or beyond, patient should be monitored with repeat radiographs unless an accompanying magnet is not swallowed. In such cases, stool examinations and repeat radiographs will be asked for. An accompanying magnet must be removed with no exception.39 European Society of Gastrointestinal Endoscopy (ESGE) and European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) advised the same path for esophagus batteries however they recommend to remove batteries in the stomach emergently within two hours if the child is symptomatic and/or has a known or suspected anatomical pathology in the GI tract (eg, Meckel’s diverticulum), and/or has simultaneously swallowed a magnet. If the battery lodged in the stomach is larger than 20 mm, patient should be checked by radiograph. If the battery is still in place after more than 48 hours, it should be removed. They also suggest that a single cylindrical battery in the stomach can be observed and the child monitored as an outpatient and followed by X-ray 7–14 days after ingestion if the battery is not passed in the stool.40
Foreign bodies that have passed the duodenum generally have a problem-free journey through the gastrointestinal system.29 Therefore, in the follow-up of foreign bodies that have passed the gastro-esophageal junction, the size of the object is important as to whether or not it will be able to pass the duodenum. Endoscopic removal is recommended for foreign bodies exceeding 5cm in length and 2cm in width in children as it is assumed that they will not be able to pass the pylorus and duodenum.20
Due to size, or emergencies such as an open safety pin settled in the stomach or duodenum, endoscopic removal is necessary if 4 days have not elapsed. If a longer period is waited, endoscopic removal will be more difficult as the object may penetrate the mucosa and could lead to complications such as hemopericardium or esophagus perforation.29,41 Immediate removal of alkaline batteries is recommended due to the risk of damage to the upper gastrointestinal mucosa. There are however some reports on a more conservative approach with close monitoring and it would be more appropriate to do so against potential complications in these types of cases.29
Penetrating foreign bodies such as pins which have passed into the intestines and have not changed location for 4 days are an indication for surgical intervention due to the risk of perforation. Non-penetrating foreign bodies can be followed up conservatively for a period of 6 weeks as they will not lead to complications such as peritonitis, bleeding or obstruction.29 The timing of medical intervention depends to a large extent on the type of foreign body, the time since ingestion and symptoms.
In asymptomatic cases with blunt foreign bodies, there is an opportunity for 8–16 hours of observation before intervention, but early intervention is recommended for symptomatic patients who experience airway problems or have signs of gastrointestinal obstruction or inflammation and for patients who have swallowed sharp penetrating objects such as fishbones or needles and those who have swallowed batteries.2,33,34,42–44 The majority of foreign bodies that have reached the stomach, primarily coins, are spontaneously expelled from the body within 1–2 weeks at mean 3.8 days, and there is no indication for emergency removal.33
The timing and method of removal according to the type and localisation of the foreign body are shown in Table 1. There are no standard removal methods and timing, and consensus has not been reached on a treatment approach and it can be speculated that there are limited data in literature on the success and complication rates of techniques used.2,9,34 Although the rates of complications developing associated with foreign body ingestion are low, there may be serious and life-threatening complications such as esophageal perforation, neck abscess, mediastinitis, peritonitis, and fistula.5,9,33,45,46 In this respect, early determination and correct treatment are important for foreign bodies such as organic foreign bodies, sharp and long objects and batteries that settled in the digestive tract for a long time6,10,16,45,47 (Table 1).
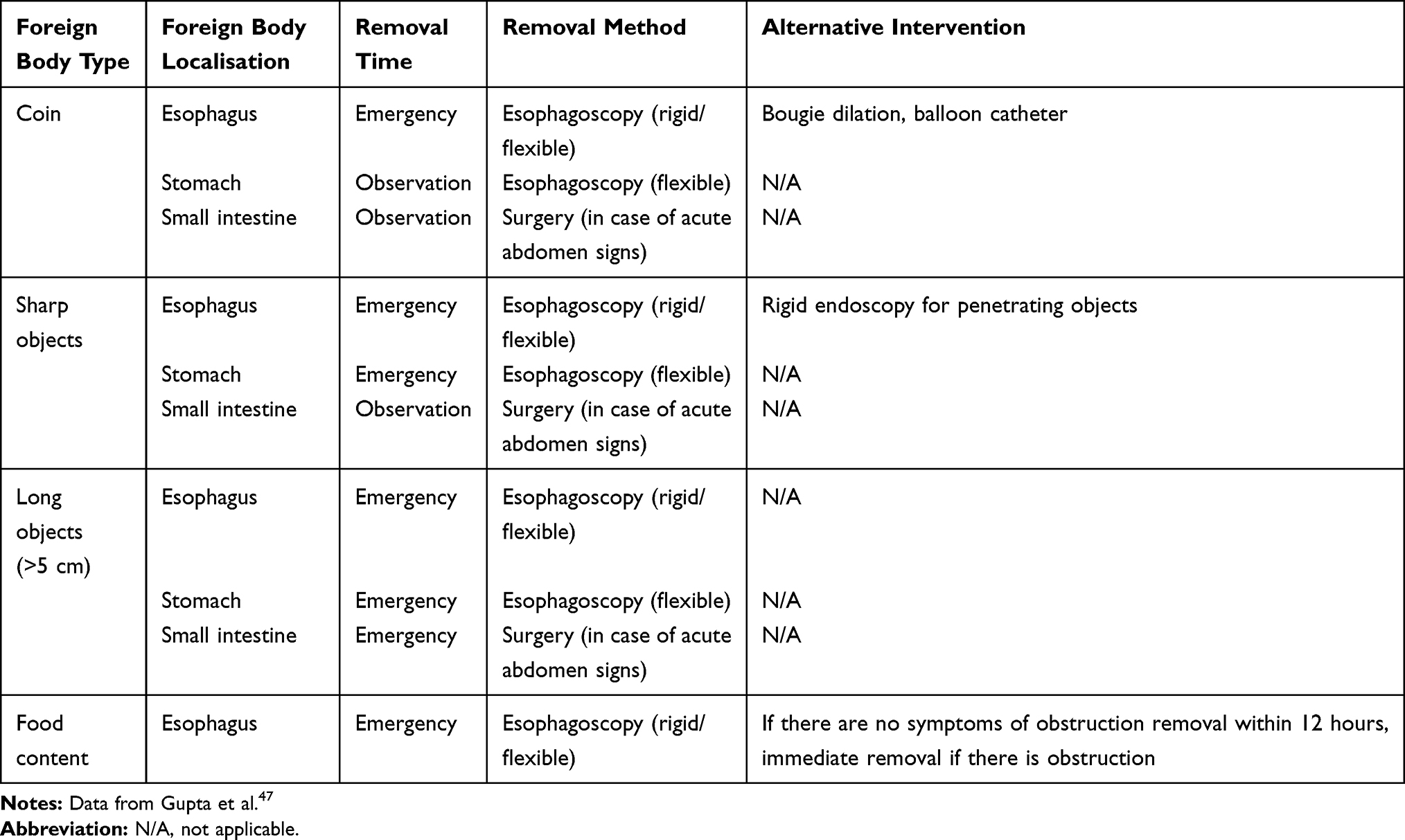 |
Table 1 Time and Method of Removal According to the Type and Localisation of the Foreign Body. |
Caustic Substance Ingestion in Childhood
Epidemiology and Pathophysiology
Caustic substance ingestion is encountered mostly in pre-school children, especially around the age of 3 years, and generally has a high lifelong morbidity and occasionally causes mortality. It is usually an accidental occurrence when an unsupervised child is curious about strong alkaline (pH>11.5) or acid substances or tastes and ingests the substance thinking that it is food.10,11,48,49 Risk factors have been reported to be male gender, attention-deficit hyperactivity disorder, low educational level of the parents, young parents, inadequate parental supervision and living in a rural area. In children aged over 5 years and adolescents, the ingestion of caustic substance is accepted as a generally deliberate act.11
Strong alkalis (caustic soda, sodium hydroxide, potassium hydroxide, lithium hydroxide, calcium hydroxide, trisodium phosphate, industrial detergents, oven cleaners, washing and dishwasher detergents, hair straightener) and strong acids (sulphuric acid, hydrochloric acid, nitric acid, acetic acid, citric acid, battery fluid, swimming pool and toilet cleaners, rust removers) cause burns and injury to the mouth, oropharynx, stomach, duodenum, and the airway. In addition, oxidant agents and phenols that are not strongly acid or alkaline can cause contact burns to the skin and gastrointestinal mucosa, and other toxic effects.11,15,49
Strong alkaline substances cause more severe damage than strong acid substances, as they cause saponification and liquefaction necrosis characterised by early and rapid loss of mucosal integrity, destruction of fat and protein, and permeate into deep tissue. With vascular thrombosis they also cause perforation via impairment of tissue feeding, so coagulation necrosis develops because of coagulum forming on the mucosa, limiting deep penetration and absorption.10,15,50
Although the ingestion of strong acid substances in the stomach is associated with more severe damage than the esophagus because of the potential to form pH levels which will allow deep penetration, perforation and stricture formation, the amount ingested is limited in most cases by the unpleasant taste and the stimulated gag reflex. However, when there is contact with the epiglottis, the development of oedema and chemical epiglottitis creates a risk for the requirement for emergency airway intervention.15
In case of caustic substance ingestion, the risk of stricture formation and long-term gastrointestinal morbidity has been reported to be 7–25%. Although the most commonly ingested caustic substances are oxidant substances such as peroxides or bleach, alkaline agents, primarily sodium hydroxide, are the caustic substances responsible for one-third to three-quarters of stricture formation leading to long-term gastrointestinal sequelae, and these are followed by acid agents at a rate of 2.9–15.3%.11,51,52
The mouth and pharynx are the areas most damaged in solid caustic substance ingestion, while liquid caustic substances pass quickly creating damage in the esophagus and stomach and can cause airway burns with simultaneous vapour aspiration (ammonia, formaldehyde).12,17,53
Although the amount of caustic substance ingested is the most important determinant of clinical outcome, this information can rarely be obtained.12,17,53 Toxicity control centres are important as the early contact of some caustic substances can lead to severe systemic effects such as hypocalcemia (phosphoric acid, hydrofluoric acid), hyponatremia (strong acids or alkalis), hypokalemia and acidosis.10,12
Within 4–7 days of caustic substance ingestion, there is a risk of perforation in full-layer lesions with impairment of mucosal integrity and bacterial invasion, and esophageal repair starts on the tenth day following ingestion.11,54 Some authors recommended to avoid endoscopy between the 5th–15th days after ingestion because of the reduction in stretching power. Scar retraction starts in the third week with fibroblast proliferation and scar formation may be accelerated with gastro-esophageal reflux that develops with impaired esophageal motility. Mucosal re-epithelialisation starts in this period and is generally completed in the sixth week. The process of scar formation may cause shortening in the esophagus when there is extensive involvement reaching stricture formation and the muscularis propria or deeper layers.11,12,55,56
Although seen rarely, there is a possibility that full-layer visceral perforation can result in death when the risk of sepsis and multiple organ failure cannot be prevented with early surgical intervention. In some cases, there is a risk of caustic erosion in adjacent viscera, and perforation or fistulation in the tracheobronchial tree, aorta or other vessels, the colon, small intestine, pancreas or gall bladder.11,12 Acid agents are susceptible to stomach involvement with effects delaying stomach emptying associated with scar formation and pyloric spasm, while alkaline agents may create sudden and severe damage at all levels of the gastrointestinal canal.12
Clinical Presentation
A history of substance ingestion is the most common presentation and symptoms differ according to the type, amount, and strength of the caustic substance. While crystal and solid substance forms harm the oropharynx, liquid substances tend to create damage in the esophagus.11 The most commonly seen symptoms are vomiting, increased saliva, dysphagia, oral pain, odynophagia, chest pain and abdominal pain. An increase in the number of symptoms indicates a higher possibility of the presence of a lesion and findings such as fever, chest pain and hypotension are accepted as signs of esophageal or gastric perforation.13,15 Gastric damage is more common with acid substance ingestion and may occur in the form of pyloric stenosis, stomach outlet obstruction, perforation and peritonitis. The most serious complications are hemolysis, disseminated intravascular coagulation, renal failure, peritonitis, mediastinitis and even death.15,57
Dysphagia, which occurs associated with decreased motility and increased transit time in the acute period and may last for weeks following the injury, is a symptom which may occur even in the absence of a serious damage.13,15 Airway damage after caustic substance ingestion is seen in 6–18% of cases associated with aspiration during ingestion, subsequent vomiting, oedema in the pharynx and caustic burn or volatile agents ingested with the caustic substance.11,58,59 Voice restriction, stridor and retractions indicate mucosal damage in the larynx and symptoms may develop suddenly or within several hours, especially with ingestion of the powder form of caustic substances. Flexible fiberoptic laryngoscopy performed by an experienced specialist has diagnostic value and flexible fiberoptic intubation is important in preventing the need for cricotomy or tracheotomy.15,17
One of the most controversial points in the management of caustic substance ingestion is the inconsistency between symptoms and injury severity. The presence or absence of symptoms is not reflected in the degree of damage in the digestive tract.10,15 According to some authors, two or more symptoms combined together may notify us of an esophageal injury, but it has also been reported that no single symptom or its combinations could guarantee an exact diagnosis of esophageal injury.16,47 In a series of 473 pediatric cases, esophageal lesions were determined in 61% of cases with no oral lesions.60
Between half and two-thirds of patients are asymptomatic after caustic substance ingestion, and as inflammation and obstructive symptoms may emerge 24–48 hours later, it is important that asymptomatic patients are monitored under observation throughout this period.11,61 It must also be kept in mind that esophageal perforation can occur at any time within the first two weeks after caustic substance ingestion.11
Diagnostic Evaluation
In diagnostic evaluation and management, taking patient’s history, physical examination and resuscitation/stabilisation of patients under acute stress are very important. Upper gastrointestinal endoscopy is the basic diagnostic method in the determination of the degree of damage. According to previous reports, the absence of visible burns or pharyngeal-esophageal symptoms do not eliminate the presence of visceral lesions and in the recent years, it has been published that esophagoscopy in asymptomatic patients could be avoided.13,62,63 Published literature shows that all patients with clinically significant damage (second/third-degree) are already symptomatic in the first evaluation. In asymptomatic patients esophageal damage may not develop in the majority of children, it may not be mandatory to perform esophagoscopy to.13,47,63
European Society of Gastrointestinal Endoscopy (ESGE) and European Society of Pediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) report in their guidelines that every child who has ingested a corrosive substance should have a thorough follow-up, with endoscopy dictated by symptoms and dependent on the symptoms and signs, and that the timing should be within 24 hours. ESGE/ESPGHAN also suggest that in the case of suspected corrosive ingestion, esophagoscopy is withheld if the child is asymptomatic (no drooling of saliva/other symptoms and no mouth lesions) and that adequate follow-up is assured.64
Grading and Management
After obtaining a detailed history related to the origin, type and amount of caustic substance ingested, a sample of the caustic substance should be requested from the family to make additional analyses if available. Toxin Consultation Centre should be called for the caustic substance’s corrosive and/or toxic effects. Very first steps of the treatment begin in the Emergency Department, based on patient’s vital signs and symptoms such as hypotension, severe chest or abdominal pain.15,16,48
The use of active charcoal is not recommended as it is not effective on caustic agents. Vomiting or manoeuvres that will trigger vomiting must be prevented as it will cause renewed contact of the caustic substance within the esophagus. Although oral dilution treatment with water or milk has been found to be effective in animal models, there is no evidence for humans, and it must not be forgotten that with the ingestion of any substance, there is a risk that it could trigger vomiting, and dilution treatment must not exceed 15mL per kg of bodyweight.15
Blind insertion of a nasogastric tube is contraindicated, and the use of H2 receptor blockers, proton pump inhibitors and sucralfate has not been shown to have an effect on reducing damage. Furthermore, there is a risk that after treatment with these agents endoscopic examination will be more difficult.15,16
As there are no severe symptoms following the ingestion of low-risk substances such as bleach, observation alone is generally sufficient. If there are findings of widespread superficial ulceration in the first endoscopic evaluation after bleach ingestion, this is occasionally classified as deep tissue penetration or stricture formation.15
Stopping oral intake and the provision of intravenous hydration is very important in symptomatic patients. Chest and abdominal X-ray radiographs are fundamental in showing or eliminating the presence of free air in the mediastinum or peritoneum. In patients with airway symptoms, flexible fiberoptic laryngoscopy should be performed by an experienced clinician without leading to gagging or vomiting. Contrast esophagogram is not sufficiently sensitive in the determination of the initial level of damage in acute conditions. However, if it is to be used, a water-soluble agent should be preferred over a barium enema due to the dangerous aftermath following a possible perforation.15,63
When an esophageal lesion is visualised during an endoscopy of the posterior tracheal wall, tracheoscopy should also be performed and although the intervention is terminated in most cases following visualisation of the first circumferential lesion, it must not be forgotten that there could be more distal lesions and flexible endoscopy has the advantage of allowing visualisation of the stomach and duodenum.15,51
Grading esophageal damage is important in managing the treatment.51
In the treatment algorithm oral intake is stopped, intravenous hydration is provided and esophagoscopy is carried out within 24–48 hours in patients who present within the first 48 hours after ingestion, patients with an airway emergency which has been brought under control, patients with accompanying symptoms, and in patients with oropharyngeal lesion who ingested strong acid or alkaline substances. In patients with no symptoms, no strong acid or alkaline ingestion without oropharyngeal lesion are monitored under observation at least for 24 hours.15,52
Patients with Grade 0–1 on esophagoscopy are discharged and admitted to the follow-up program. Beyond Grade II patients, stopping oral intake is maintained in all grade groups. Intravenous antibiotics and steroid therapy are still controversial and dependant upon the clinicians referral. If a stricture develops in the follow-up, esophageal dilation is performed, otherwise water-soluble contrast esophagogram examination is performed after the 3rd week of caustic exposure. Grade II patients are managed with a feeding tube that is introduced during an esophagoscopy. Treatment for Grade III patients is managed with a feeding tube or future esophageal stents. Grade IV patients receive the same treatment modality as in Grade 3 in the early periods however they may undergo an esophageal replacement surgery in the future if long segment strictures, resistant to esophageal dilations, develop.15,52
In patients presenting after 48 hours of caustic substance ingestion, some authors do not advise endoscopy because of the instrument-related risk of perforation. A water-soluble contrast esophagogram is performed. If normal findings are seen esophagram, the esophagram is repeated after 3 weeks. If a stricture is detected, then the patient is enrolled in dilation treatment programme.15,52
Airway and hemodynamic stabilisation are essential in all cases of caustic substance ingestion. General anesthesia with airway intubation under direct visualisation with fiberoptic laryngoscope is the most appropriate option rather than a blind approach since it would reduce the risk of bleeding and additional airway damage.50 It is important to avoid over-inflation of the esophagus. Anesthesia induction is achieved with sevoflurane and neuromuscular agent in children under 2 years of age and with propofol and neuromuscular agent in children over 2 years of age. Anesthesia maintenance is achieved with 2–3% sevoflurane and oxygen-air mixture.
Although the use of steroids is frequently preferred in clinical practice, its use is still controversial.15,50 By using steroids, De Jong et al and Mamede et al reported success in reducing stenosis extent and number of endoscopic treatment procedures. The corticosteroids seem to reduce the formation of granulation tissue and the proliferation of fibrotic tissue.14,65,66 In their report of 473 patients, Dogan et al advised proton pump inhibitors with corticosteroids beyond Grade II lesions along with a semifluid diet.60 Long-acting glucocorticoids like dexamethasone was shown to be more effective than Prednisone to reduce the degree of stenosis.14,47,61 De Jong et al pointed out a drawback in high doses of dexamethasone usage by increasing the risk of perforation in Grade III injury.14 On the contrary, there are also reports that stress the risk of perforation in the clinical course and that corticosteroids do not reduce stricture development in Grade II injury.67,68 In Grade II lesions who show a positive effect in the reduction of stricture with a 6-week period of nasogastric tube or other stent placement, results are debatable in long term. Animal model studies have shown promising results related to collagen cross-linking inhibitors such as Vitamin E, ketotifen, N-acetylcysteine, penicillamine and B-aminopropionitrile.15 Positive results have been obtained in animal model studies with the use of topical and systemic antifibrotic agents such as pirfenidone and 5-fluorouracil and subcutaneous heparin injection.11
Complications
Stricture is the most common complication following caustic substance ingestion. Cricopharynx, arcus aorta and lower esophageal sphincter are areas of stasis and slow transit, and they are the most common areas of stricture development. Other complications are pyloric stenosis, gastric perforation, tracheoesophageal fistula formation, mediastinitis, peritonitis, pneumonia, sepsis, the development of malignancy and even death.15
The main approach following esophageal stricture formation is esophageal dilation.15 Most patients require the procedure to be repeated many times over the years which lead to problems of nutritional deficiency and decreased quality of life and sufficient long-term results are obtained only in 33–48% of patients.25,63 The application of topical mitomycin-C and/or the placement of an esophageal stent to the stricture site are other alternative treatments. However, there is a need for further studies of mitomycin-C with larger series, and there is an extremely limited amount of data related to esophageal stent placement in children.15,69,70
The primary non-surgical treatment of caustic esophageal stricture is endoscopic dilation to improve dysphagia with bougie or balloon dilators. The main purpose of therapy is providing clinically significant dilations to reduce the number of procedures to be repeated in the future.50 In cases with perforation and advanced stricture formation associated with severe lesions, the mortality risk is high; therefore, some authors suggest an early surgical resection and reconstruction of the damaged esophagus.
Replacement surgery includes isoperistaltic ileum and cecum, transverse or left colon interpositioning, but the long-term results are reported not to be satisfactory with operative complications such as malnutrition, late-stage morbidity and a rise in mortality rates up to 50% within 10 years.15,71 So far the development of safety strategies for the prevention of caustic substance ingestion is very important, with education, product labelling and legal regulations.
Persistent dysphagia in the first 3 weeks following caustic substance ingestion is a strong predictive factor for further stricture dilations in children with Grade II and Grade III lesions.11,49,51 With this negativity in mind, some authors advocate an early esophageal dilation within 10–21 days of first caustic exposure. They performed this early approach to symptomatic patients12,51,72 and suggested that it is applicable in many situations to prevent the risk of late identification of strictures associated with factors such as symptoms masking the reduction of solid food intake.11 Stricture formation varies between 2% and 63% and basically occurs in the proximal to mid-esophagus. Dilation programs ideally start in the third week following the damage. When it is delayed to more than 3 weeks there is a risk of increased fibrotic stenosis and a prolonged period required for dilation, and a delay in starting dilation treatment has been shown to increase the likelihood of esophagus replacement surgery.39 When the “age appropriate” esophageal calibration rate is reached, dilation frequency is reduced to once every 2–3 weeks or once a month, based on symptoms.11
In the majority of children who develop stricture, a dilation program is carried out once a week or every 2 weeks for 3 months, with a mean of 12 esophageal dilations.11 Gundogdu et al reported good prognostic factors following stricture dilation as; the stricture having developed associated with ingestion of a substance other than caustic soda, stricture length shorter than 5cm which have developed in the esophagus upper third, and patients’ age younger than 8 years.73
Antegrade bougie dilations under fluoroscopic guidance along with retrograde bougie dilations via a gastrostomy route are reserved for long strictures, and the perforation rate has been reported to be 0.4–17.4%.11
Esophageal carcinoma develops in 1–4% of strictures, especially in patients who underwent esophagectomy and colonic interposition. In these patients, long-term surveillance is essential since there is a risk of malignancy development.15 Previous reports have shown that the risk of development of carcinoma of the esophagus among patients with corrosive-induced esophageal strictures is more than 1000 times that of persons without strictures.74 In a recent report from Korea, Noh et al reported that the mean duration from caustic ingestion to diagnosis of cancer was estimated at 42 years.75 In their series of 15 patients, pathologic specimens revealed a squamous cell carcinoma. Ten patients had their tumor involving the stenotic portion originating from the pre-existing lye stricture, with three patients the tumor were limited to the stricture and 7 patients had their tumor extending just proximal to the stenosis site.
Conclusion
Endoscopy is the most commonly performed method for the removal of a foreign body, but as types of foreign bodies in digestive tract vary in different societies they cause a wide range of symptoms. There is a need for further extensive studies related to success and complication rates.
In cases of caustic substance ingestion, endoscopy indication criteria remain unclear as there is no correlation between symptoms and lesion severity. The determination of the treatment steps related to the stricture formation risk is based on endoscopic lesion grading. With timely and correct diagnosis of cases of foreign body and caustic substance ingestion by risk evaluation appropriate to the substance ingested and clinical presentation, it is possible to overcome serious complications and morbidities with an appropriate treatment approach.
Acknowledgments
We thank Prof. Dr. Mehmet Emin Boleken and Assistant Prof Dr. Osman Hakan Kocaman (University of Harran, Sanliurfa) for their kind support of study design/planning and data collection.
Funding
No financial funding from third parties.
Disclosure
The authors report no conflicts of interest.
References
1. Kay M, Whyllie R. Foreign body ingestions in the pediatric population and techniques of endoscopic removal. Tech Gastrointest Endosc. 2013;15:9–17.
2. Jayachandra S, Eslick GD. A systematic review of paediatric foreign body ingestion: presentation, complications, and management. Int J Pediatr Otorhinolaryngol. 2013;77:311–317.
3. Chung S, Forte V, Campisi P. A review of paediatric foreign body ingestion and management. Clin Pediatr Emerg Med. 2010;1:225–230.
4. Dereci S, Koca T, Serdaroğlu F, Akçam M. Foreign body ingestion in children. Turk Pediatri Ars. 2015;50:234–240.
5. Gregori D, Scarinzi C, Morra B, et al. ESFBI study group. Ingested foreign bodies causing complications and requiring hospitalization in European children: results from the ESFBI study. Pediatr Int. 2010;52:26–32.
6. Louie MC, Bradin S. Foreign body ingestion and aspiration. Pediatr Rev. 2009;30:295–301.
7. Vijaysadan V, Perez M, Kuo D. Revisiting swallowed troubles: intestinal complications caused by two magnets: a case report, review and proposed revision to the algorithm for the management of foreign body ingestion. J Am Board Fam Med. 2006;19:511–516.
8. Sugawa C, Ono H, Taleb M, Lucas EC. Endoscopic management of foreign bodies in the upper gastrointestinal tract: a review. World J Gastrointest Endosc. 2014;16:475–481.
9. Altokhais TI, Al-Saleem A, Gado A, Al-Qahtani A, Al-Bassam A. Esophageal foreign bodies in children: emphasis on complicated cases. Asian J Surg. 2017;40:362–366.
10. Bonavina L, Chirica M, Skrobic O, et al. Foregut caustic injuries: results of the world society of emergency surgery consensus conference. World J Emerg Surg. 2015;10:44.
11. Arnold M, Numanoglu A. Caustic ingestion in children-a review. Semin Pediatr Surg. 2017;26:95–104.
12. Chirica M, Bonavina L, Kelly MD, Sarfati E, Cattan P. Caustic ingestion. Lancet. 2017;389:2041–2052.
13. Betalli P, Falchetti D, Giuliani S, et al. Caustic ingestion italian study group. Caustic ingestion in children: is endoscopy always indicated? The results of an Italian multicenter observational study. Gastrointest Endosc. 2008;68:434–439.
14. de Jong AL, Macdonald R, Ein S, Forte V, Turner A. Corrosive esophagitis in children: a 30-year review. Int J Pediatr Otorhinolaryngol. 2001;57:203–211.
15. Schoem SR, Rosbe KW, Bearelly S. Aerodigestive foreign bodies and caustic ingestions. In: Flint PW, Bruce H, Haughey K, et al., editors. Cummings Otolaryngology - Head and Neck Surgery E-Book. Elsevier Saunders; 2015:3195–3199.
16. Lupa M, Magne J, Guarisco JL, Amedee R. Update on the diagnosis and treatment of caustic ingestion. Ochsner J. 2009;9(2):54–59.
17. Contini S, Scarpignato C. Caustic injury of the upper gastrointestinal tract: a comprehensive review. World J Gastroenterol. 2013;19:3918–3930.
18. Dray X, Cattan P. Foreign bodies and caustic lesions. Best Pract Res Clin Gastroenterol. 2013;27:679–689.
19. Zhang S, Cui Y, Gong X. Endoscopic management of foreign bodies in the upper gastrointestinal tract in South China: a retrospective study of 561 cases. Dig Dis Sci. 2010;55:1305–1312.
20. Yalcin S, Karnak I, Ciftci A. Foreign body ingestion in children: an analysis of pediatric surgical practice. Pediatr Surg Int. 2007;23:755–761.
21. Eisen GM, Baron TH, Dominitz JA, et al. Guideline for the management of ingested foreign bodies. Gastrointest Endosc. 2002;55:802–806.
22. Arana A, Hauser B, Hachimi-Idrissi S. Management of ingested foreign bodies in childhood and review of the literature. Eur J Pediatr. 2001;160:468–472.
23. Shivakumar AM, Naik AS, Prashanth KB, Yogesh BS, Hongal GF. Foreign body in upper digestive tract. Indian J Pediatr. 2004;71:689–693.
24. Orji FT, Akpeh JO, Okolugbo NE. Management of esophageal foreign bodies: experience in a developing country. World J Surg. 2012;36:1083–1088.
25. Little DC, Shah SR, St Peter SD, et al. Esophageal foreign bodies in the pediatric population: our first 500 cases. J Pediatr Surg. 2006;41:914–918.
26. Gmeiner D, von Rahden BH, Meco C, Hutter J, Oberascher G, Stein HJ. Flexible versus rigid endoscopy for treatment of foreign body impaction in the esophagus. Surg Endosc. 2007;21:2026–2029.
27. Rodriguez H, Passali GC, Gregori D. Management of foreign bodies in the airway and oesophagus. Int J Pediatr Otorhinolaryngol. 2012;76:84–91.
28. Uyemura MC. Foreign body ingestion in children. Am Fam Physician. 2005;72:287–291.
29. Tiryaki HT, Akbıyık F, Senel E, Mambet E, Livanelioğlu Z, Atayurt HF. Foreıgn body ıngestıon ın chıldhood. Turk J Pediatr Dis. 2010;4:94–99.
30. Dörterler ME. Clinical Profile and Outcome of Esophageal Button Battery Ingestion in Children: An 8-Year Retrospective Case Series. Emerg Med Int. 2019;2019:3752645. doi:10.1155/2019/3752645
31. Kazam JK, Coll D, Maltz C. Computed tomography scan for the diagnosis of esophageal foreign body. Am J Emerg Med. 2005;23:897–898.
32. Muensterer OJ, Joppich I. Identification and topographic localization of metallic foreign bodies by metal detector. J Pediatr Surg. 2004;39:1245–1248.
33. Lin CH, Chen AC, Tsai JD, Wei SH, Hsueh KC, Lin WC. Endoscopic removal of foreign bodies in children. Kaohsiung J Med Sci. 2007;23:447–452.
34. Srivastava G. Foreign bodies in the oropharynx, gastointestinal tract, ear, and nose. Clin Pediatr Emerg Med. 2010;11:81–94.
35. Cetinkursun S, Sayan A, Demirbag S, Surer I, Ozdemir T, Arikan A. Safe removal of upper esophageal coins by using Magill forceps: two centers’ experience. Clin Pediatr. 2006;45:71–73.
36. Dahshan AH, Kevin Donovan G. Bougienage versus endoscopy for esophageal coin removal in children. J Clin Gastroenterol. 2007;41:454–456.
37. Litovitz T, Whitaker N, Clark L. Preventing battery ingestions: an analysis of 8648 cases. Pediatrics. 2010;125:1178–1183.
38. Katzka DA. Caustic injury to the esophagus. Curr Treat Options Gastroenterol. 2001;4:59–66.
39. Tiryaki T, Livanelioglu Z, Atayurt H. Early bougienage for relief of stricture formation following caustic esophageal burns. Pediatr Surg Int. 2005;2:78–80.
40. Kramer RE, Lerner DG, Lin T, et al. Management of ingested foreign bodies in children: a clinical report of the NASPGHAN endoscopy committee. J Pediatr Gastroenterol Nutr. 2015;60(4):562–574.
41. Gün F, Salman T, Abbasoglu L, Celik R, Celik A. Safety-pin ingestion in children: a cultural fact. Pediatr Surg Int. 2003;19:482–484.
42. Paul SP, Wilkinson R. Foreign body ingestion in children. Nurs Times. 2012;108:25.
43. George AT, Motiwale S. Magnets, children and the bowel: a dangerous attraction? World J Gastroenterol. 2012;18:5324–5328.
44. Waltzman ML, Baskin M, Whpij D, Mooney D, Jones D, Fleisher G. A randomized clinical trial of the management of esophageal coins in children. Pediatrics. 2005;116:614–619.
45. Kamath P, Bhojwani KM, Prasannaraj T, Abhijith K. Foreign bodies in the aerodigestive tract e a clinical study of cases in the coastal belt of South India. Am J Otolaryngol. 2006;27:373–377.
46. Olives JP. Ingested foreign bodies. J Pediatr Gastroenterol Nutr. 2000;31:188.
47. Gupta SK, Croffie JM, Fitzgerald JF. Is esophagogastroduodenoscopy necessary in all caustic ingestions? J Pediatr Gastroenterol Nutr. 2001;32:50–53.
48. Rafeey M, Ghojazadeh M, Mehdizadeh A, Hazrati H, Vahedi L. Intercontinental comparison of caustic ingestion in children. Korean J Pediatr. 2015;58:491–500.
49. Karaman I, Koc O, Karaman A, et al. Evaluation of 968 children with corrosive substance ingestion. Indian J Crit Care Med. 2015;19::714–718.
50. Maa DL, Timbol ABG, Tuazon DJS. Management of esophageal caustic injury. World J Gastrointest Pharmacol Ther. 2017;8:90–98.
51. Zargar SA, Kochhar R, Mehta S, Mehta SK. The role of fiberoptic endoscopy in the management of corrosive ingestions and modified endoscopic classification of burns. Gastrointest Endosc. 1991;37:165–169.
52. Elshabrawi M, A-Kader HH. Caustic ingestion in children. Expert Rev Gastroenterol Hepatol. 2011;5:637–645.
53. Hugh TB, Kelly MD. Corrosive ingestion and the surgeon. J Am Coll Surg. 1999;189:508–522.
54. Osman M, Russell J, Shukla D, Moghadamfalahi M, Granger DN. Responses of the murine esophageal microcirculation to acute exposure to alkali, acid, or hypochlorite. J Pediatr Surg. 2008;43:1672–1678.
55. Mattos GM, Lopes DD, Mamede RC, Ricz H, Mello-Filho FV, Neto JB. Effects of time of contact and concentration of caustic agent on generation of injuries. Laryngoscope. 2006;116:456–460.
56. Chirica M, Resche-Rigon M, Pariente B, et al. Computed tomography evaluation of high-grade esophageal necrosis after corrosive ingestion to avoid unnecessary esophagectomy. Surg Endosc. 2015;29:1452–1461.
57. Salzman M, O’Malley RN. Updates on the evaluation and management of caustic exposures. Emerg Med Clin North Am. 2007;25:459–476.
58. Riffat F, Cheng A. Pediatric caustic ingestion: 50 consecutive cases and a review of the literature. Dis Esophagus. 2009;22::89–94.
59. Turner A, Robinson P. Respiratory and gastrointestinal complications of caustic ingestion in children. Emerg Med J. 2005;22:359–361.
60. Dogan Y, Erkan T, Cokugras FC, Kutlu T. Caustic gastroesophageal lesions in childhood: an analysis of 473 cases. Clin Pediatr. 2006;45:435–438.
61. Lamireau T, Rebouissoux L, Denis D, Lancelin F, Vergnes P, Fayon M. Accidental causticingestioninchildren: isendoscopyalwaysmandatory? J Pediatr Gastroenterol Nutr. 2001;33:81–84.
62. Arevalo-Silva C. Ingestion of caustic substances: a 15-year experience. Laryngoscope. 2006;116:1422–1426.
63. Kay M, Wyllie R. Caustic ingestions and the role of endoscopy. J Pediatr Gastroenterol Nutr. 2001;32:8–10.
64. Thomson M, Tringali A, Dumonceau JM, et al. Paediatric gastrointestinal endoscopy: European society for paediatric gastroenterology hepatology and nutrition and European society of gastrointestinal endoscopy guidelines. J Pediatr Gastroenterol Nutr. 2017;64(1):133–153. doi:10.1097/MPG.0000000000001408
65. Mamede RCM. Treatment of caustic ingestion: an analysis of 239 cases. Dis Esophagus. 2002;15:210–213.
66. Baskin D, Urganci N, Alkim C, et al. A standardised protocol for the acute management of corrosive ingestion in children. Pediatr Surg Int. 2004;20(11–12):824–828.
67. Anderson KD, Rouse TM, Randolph JG. A controlled trial of corticosteroids in children with corrosive injury of the esophagus. N Engl J Med. 1990;323:637–640.
68. Fulton JA, Hoffman RS. Steroids in second degree caustic burns of the esophagus: a systematic pooled analysis of fifty years of human data: 1956–2006. Clin Toxicol. 2007;45:402–408.
69. Rosseneu S, Afzal N, Yerushalmi B, et al. Topical application of mitomycin-C in oesophageal strictures. J Pediatr Gastroenterol Nutr. 2007;44:336–341.
70. Best C, Sudel B, Foker JE, Krosch TC, Dietz C, Khan KM. Esophageal stenting in children: indications, application, effectiveness, and complications. Gastrointest Endosc. 2009;70:1248–1253.
71. Chirica M, Resche-Rigon M, Bongrand NM, et al. Surgery for caustic injuries of the upper gastrointestinal tract. Ann Surg. 2012;256:994–1001.
72. Bicakci U, Tander B, Deveci G, Rizalar R, Ariturk E, Bernay F. Minimally invasive management of children with caustic ingestion: less pain for patients. Pediatr Surg Int. 2010;26:251–255.
73. Gundogdu HZ, Tanyel FC, Buyukpamukcu N, Hicsonmez A. Conservative treatment of caustic esophageal strictures in children. J Pediatr Surg. 1992;27:767–770.
74. Appelqvist P, Salmo M. Lye corrosion carcinoma of the esophagus: a review of 63 cases. Cancer. 1980;45(10):2655–2658.
75. Noh SY, Kim HJ, Lee HJ, et al. Corrosive-induced carcinoma of esophagus: esophagographic and CT findings. Am J Roentgenol. 2017;208:1237–1243. doi:10.2214/AJR.16.17138
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.