Back to Journals » Risk Management and Healthcare Policy » Volume 16
Forecasting Head and Neck Cancer Trends in GCC Countries: Implications for Public Health Policy and Strategy
Authors Alsharif A, Alsharif MT, Samman M ![]() , Binmadi N, Kassim S
, Binmadi N, Kassim S ![]() , Mourad S, Warnakulasuriya S
, Mourad S, Warnakulasuriya S
Received 17 October 2023
Accepted for publication 20 December 2023
Published 28 December 2023 Volume 2023:16 Pages 2943—2952
DOI https://doi.org/10.2147/RMHP.S445162
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Alla Alsharif,1,* Maha T Alsharif,2,* Meyassara Samman,3,* Nada Binmadi,2,* Saba Kassim,1,* Samah Mourad,4,* Saman Warnakulasuriya5,6,*
1Department of Preventive Dental Sciences, Taibah University Dental College & Hospital, Al-Madinah Al-Munawwarah, Saudi Arabia; 2Department of Oral Diagnostic Sciences, King Abdulaziz University, Faculty of Dentistry, Jeddah, Saudi Arabia; 3Department of Dental Public Health at King Abdulaziz University, Faculty of Dentistry, Jeddah, Saudi Arabia; 4Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Mansoura University, ElMansoura, Eldaqahlia, Egypt; 5Faculty of Dentistry, Oral & Craniofacial Sciences, King’s College London, London, UK; 6World Health Organization Collaborating Centre for Oral Cancer, London, UK
*These authors contributed equally to this work
Correspondence: Maha T Alsharif, Department of Oral Diagnostic Sciences, King Abdulaziz University, Faculty of Dentistry, P.O. Box 80209, Jeddah, 21589, Saudi Arabia, Tel +966582862000, Email [email protected]
Purpose: The data available on the incidence and mortality rates of head and neck cancer types (HNCs) in the Gulf Cooperation Council countries (GCC) have relied on global trends and covered only certain cancer sites, types or certain age groups. This study aimed to assess the incidence and mortality rates of head and neck cancer (HNCs) within the Gulf Cooperation Council (GCC) countries, providing insights into their geographic variability in 2020.
Methods: Prediction of the magnitude of the disease to 2040 was explored based on demographic projections. Estimates of incidence and mortality and the population projections were extracted from the Global Cancer Observatory (GLOBOCAN) database and the United Nations Department of Economic and Social Affairs respectively for the time frame 2020 to 2040. Additionally, we analyzed the distribution of cases and deaths by age and sex for both time periods.
Results: The analysis indicates varying patterns in HNC rates across GCC countries in 2020, with Oman and Saudi Arabia carrying the highest burden. Projections for 2040 reveal a substantial increase in new HNC cases and related deaths, particularly in Qatar, UAE, and Bahrain. Furthermore, incidence rates are predicted to rise significantly for individuals aged 50 and older, while remaining relatively stable for those under 50. With regards to sex, males generally exhibit higher rates, except in Qatar.
Conclusion: HNC burden is anticipated to rise significantly in the GCC, with variations per age, sex and geographical location. By 2040, a 2-3-fold increase in HNCs in the GCC is anticipated, emphasizing the need for focused public health strategies to address this rising health challenge.
Keywords: head and neck neoplasms, projection, globocan, cancer prevention
Introduction
The Gulf Cooperation Council (GCC) member countries include Bahrain, Oman, Kuwait, Saudi Arabia, Qatar, and the United Arab Emirates, which together are comprised of 57.4 million people.1,2 The GCC member countries tend to have similar economic, political, and sociocultural structures that shape their healthcare systems. They also share a history of healthcare practices, including traditional and modern medicine, which have further influenced the development of their healthcare systems. The healthcare outcomes of these countries are often impacted by similar environmental and psychosocial factors.
The GCC member countries are also well known for their economic prosperity, which has ultimately led to an increase in average life expectancy to more than 77 years, resulting in a rapid demographic transition.3,4 As longevity increased, chronic diseases, including cancers, became more prevalent, which suggests considerable challenges for future development.5 Head and neck cancers (HNCs) are the seventh most commonly diagnosed cancer worldwide, accounting for more than 325,000 deaths and 660,000 new cases annually.6–8 HNCs include cancers in the larynx, pharynx, lips, oral cavity, nose, and salivary glands. HNCs are the 18th most diagnosed cancer and the ≥11th most common cause of cancer deaths in the GCC countries.6
Despite the advances in treatment, the rate of survival from HNCs remains poor until recently.9 The regional differences in the incidence of HNCs are largely determined by the underlying regional populations, which are attributed to the differences in underlying risk factors and subtype distributions. The incidence of HNCs is increasing in high-income settings, with possible aetiological changes that have implications for prevention and treatment.10 Although tobacco and alcohol consumptions were once considered as the established risk factors,7,11 the risk is clearly socioeconomically mediated, and HNCs are reported among non-smoking, non-alcohol users. Furthermore, the human papillomavirus has emerged as the likely cause of oropharyngeal cancer.11,12 The increasing burden of cancer (including HNCs) is exerting tremendous economic strain, significant psychological distress, and substantial functional impairments on individuals, communities, and healthcare systems.13–15
The incidence and mortality rates of HNCs are not well studied in GCC countries. The results of the few studies published have relied on global trends or covered certain cancer sites or types.16–20 Thus, the primary focus of this study was on describing the incidence and mortality rates of HNCs at the regional level and assessing the geographic variability across GCC countries. Herein, we describe the magnitudes and distributions of the major HNC types in 2020 and end by providing an estimate of the disease in 2040 on the basis of demographic projections for GCC countries, commenting briefly on the potential public health impacts of this trend in relation to the underlying causes and prospects for future cancer control.
Data Source and Methods
Head and Neck Cancer Prediction
Using the GLOBOCAN database (Cancer Tomorrow) of the International Agency for Research on Cancer (IARC), we retrieved predictions of the incidence and mortality rates of HNCs in GCC countries from 2020 to 2040.21 As part of the GLOBOCAN 2020 report, key results for 6 HNC types in all six GCC countries have been published along with the sources and methods used to compile the estimates (gco.iarc.fr).6,21 GLOBOCAN projections were based on constant age-specific cancer incidence throughout the years, where changes in the number of cases owing solely to population age distributions.6 Various countries use similar methods for collecting age-specific cancer incidence and mortality rates. The incidence rates of HNCs were sourced from national cancer registries for all six GCC countries, while the mortality rates were assessed by modelling national incidence estimates as incidence-to-mortality ratios using cancer registry data from neighbouring countries.6
Definition of Head and Neck Cancer
Our study adheres to the National Health Service (NHS) UK definition of HNC, NHS (UK) states that cancers can originate in over 30 specific areas within the head and neck region.22 The specific areas of the Head and Neck considered in the NHS (UK) classification are: the mouth and lips, larynx, pharynx, salivary glands, nose and sinuses, and areas at the back of the nose and mouth (nasopharynx). Those are discretely categorised according to their anatomical locations using the International Classification of Diseases Related Health Problems, 10th Revision (ICD-10).8 These include the lip, oral cavity (C00-C06), pharynx (including the oropharynx [C09–C10], hypopharynx [C12–C13], and nasopharynx [C11]), larynx (C32), and salivary glands (C07–C08).21 Paranasal sinuses and nasal cavity cancers were excluded, as they were not included in the GLOBOCAN database.
Population
Population data corresponding to the year were obtained from the United Nations (UN) website.23
Data Analysis
Future trends in the incidence and mortality rates of HNCs from 2020 to 2040 were estimated for the six GCC countries. Detailed information about the data and the methodological approach used in compiling the IARC cancer estimates can be found in detail elsewhere.24 Our study presents age-standardised incidence or mortality rates per 100,000 person-years using the 1966 Segi-Doll World standard population.25 Additionally, we present a forecast for the future burden of HNCs in 2040, utilizing demographic projections and assuming that the rates estimated at the national level in 2020 remain constant. Since cancer incidence and mortality is strongly age-dependent, we further assess the burden of HNCs by characterising age according to a binary proxy of <50 vs ≥50. The age division may have clinical relevance since it might affect cancer diagnosis, treatment choices, and prognosis. Considering that younger patients may respond differently to treatment than older patients, healthcare strategies may need to be adjusted accordingly.
Ethical Considerations
This study was based on open-access and previously anonymised data. Ethical clearance to conduct this study was obtained from the Research Ethical Committee at Taibah University College of Dentistry (TUCDREC/051233/ATAlsahrif).
Results
Current Incidence and Mortality
The estimated age standardized incidence/mortality rate (ASIR/ASMR) per 100,000 persons and cumulative risk (age 0–85) of HNCs combined are presented in Table 1. The highest burden of HNCs is observed in Oman and Saudi Arabia (ASIR 8.5 and 8.4 per 100,000 persons respectively) followed closely by UAE and Kuwait (ASIR 7.8 and 7.2 per 100,000 persons respectively) and Qatar and Bahrain (ASIR 6.7 per 100,000 persons each). The cumulative risk of developing HNCs is the highest in UAE (2.16%) and Saudi Arabia (1.99%) and the lowest in Kuwait (1.4%) and Qatar (1.32%). On sex level, the ASIR and the cumulative risk of HNCs in males are higher than in females in all GCC countries. The highest ASIR per 100,000 persons of HNCs among males are seen in Oman, Bahrain and Saudi Arabia (5.9, 5.2 and 5.1 respectively) and among females in UAE (3.7) and Saudi Arabia (3.3). The highest cumulative risk to getting HNCs among males is predicted to be in UAE (1.42%) and in Saudi Arabia among females (0.77%). With regards to mortality, the highest ASMR per 100,000 persons is observed in Oman (4.9), UAE (4.4) and Saudi Arabia (4.2). Similar to the incidence rates, the ASMR per 100,000 persons and the cumulative risk of dying from HNCs are higher in males all GCC countries except in Qatar where ASMR per 100,000 persons of females is equal to males and the cumulative risk is slightly higher among females.
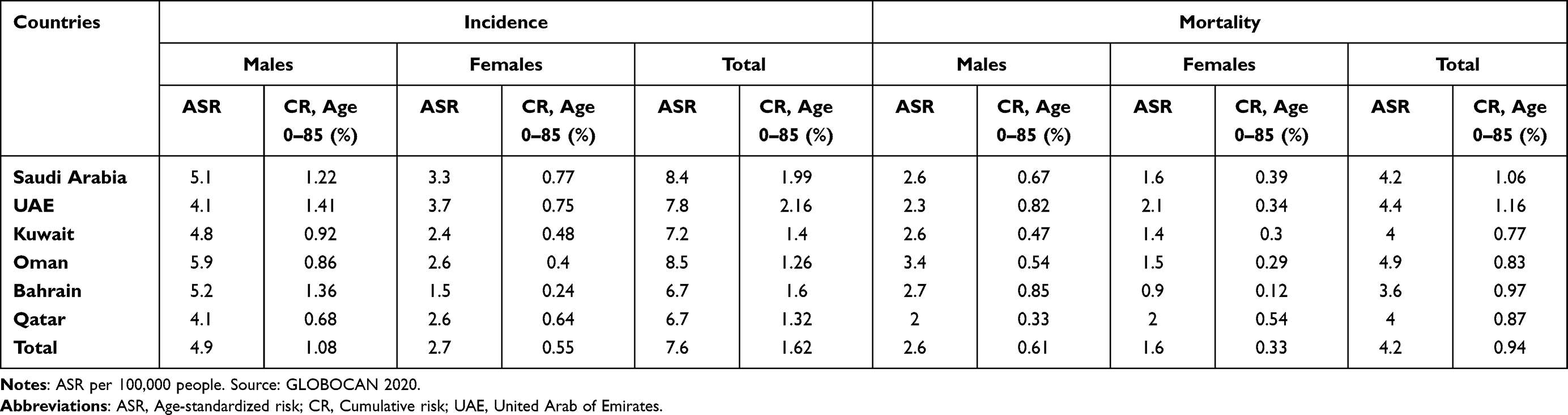 |
Table 1 Incidence and Mortality Rates (Age- Standardized Rate, Cumulative Risk) for GCC Areas and Sex for Head and Neck Cancers Combined in 2020 |
Projections of Future Incidence and Mortality
The incidence of HNCs in GCC countries was 1925 in the year 2020 and is projected to rise to 4444 by the year 2040. Meanwhile, the number of fatalities is expected to increase from 923 in 2020 to 2345 by 2040. Figure 1 illustrates the projection pattern of new HNC cases and related deaths from 2020 (baseline) to 2040 across all GCC countries. Over this time period, Qatar, UAE and Bahrain are projected to the largest increases of newly diagnosed HNC cases, with anticipated increases of +219%, +213%, and 192% respectively. In the remaining three GCC countries, the expected increases vary from +130% to + 113%. The mortality projections exhibit a similar pattern, aligning with trends observed in the incidence rates.
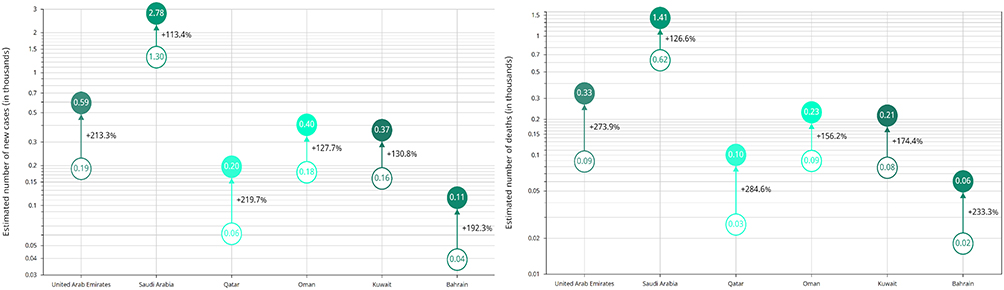 |
Figure 1 Estimated number of new cases and death cases of head and neck cancers and the percentage of change from 2020 to 2040 by country. |
Changing Profile of HNCs
The incidence of HNCs in the GCC countries for individuals below the age of 50 was 756 cases in 2020 and is projected to be 757 cases in 2040. On the other hand, the number of HNC cases for individuals aged 50 years or older is expected to rise significantly from 1169 cases in 2020 to 3688 cases in 2040. As for HNC-related deaths, in 2020, there were 285 deaths among individuals below 50 years of age, and this number is estimated to increase to 291 by 2040. For the population aged 50 years or above, the number of HNC-related deaths is anticipated to increase from 638 in 2020 to 2053 by 2040. There was a substantial change point identified in the incidence and mortality of HNCs cases from 2020 to 2040 within the older population (aged ≥ 50) across all GCC countries (Figure 2). By 2040, the projected incidence/mortality of HNC among this age group peaked approximately by 4-folds in UAE (+311%/+335%) and Qatar (+307%/+327%) followed by the reaming countries. Saudi Arabia had the lowest projected incidence and mortality with 2-folds increase (+195%/+197%). Among individuals younger than 50 years old, Oman exhibits the most significant variation in incidence projection with a remarkable increase of 46%. As for mortality projection in the same age group, Qatar stands out with a notable rise of 75%.
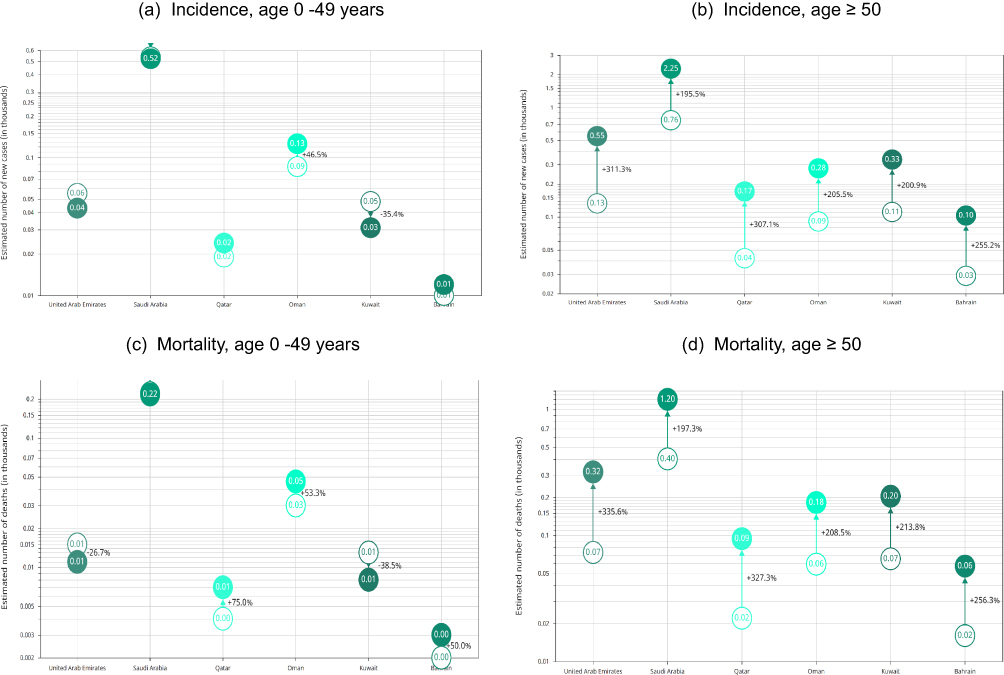 |
Figure 2 Estimated number of new cases and death cases of head and neck cancers and the percentage of change from 2020 to 2040 by country and age groups. (a) Estimated number of HNC new cases for those aged between 0 to 49 years, (b) Estimated number of HNC new cases for those aged 50 years and older, (c) Estimated number of HNC death cases for those aged between 0 to 49 years, and (d) Estimated number of HNC death cases for those aged 50 years and older. |
When considering sex, the total incidence of HNCs among males in the GCC countries was 865 cases in 2020, and this number is projected to rise significantly to 2731 cases by 2040. For females, the incidence is expected to increase from 304 cases in 2020 to 958 cases in 2040. In terms of HNC-related deaths, in 2020, there were 473 deaths among males, and this number is anticipated to increase to 1518 by 2040. For females, the number of HNC-related deaths is expected to increase from 304 in 2020 to 958 in 2040. Figure 3 illustrates the projected burden of HNCs on sex-specific level from 2020 to 2040. Surprisingly, the predicated incidence and mortality of HNCs combined is higher among females compared to males across the GCC region except in UAE and Bahrain where the projected trend is higher among males. By 2040, Qatar demonstrated the highest projected incidence/mortality of HNCs among females with estimated +417% new cases and +475% deaths followed by the remaining countries which represented between 2-3-folds increase. While among males, the projected incidence/mortality trend by 2040 are estimated to be approximately 2-folds higher in UAE, Bahrain and Qatar with percentage change of +230%/298%, +203%/264% and +198%/+250% respectively. The predicted change among males in Oman, Kuwait and Saudi Arabia are more than double by 2040.
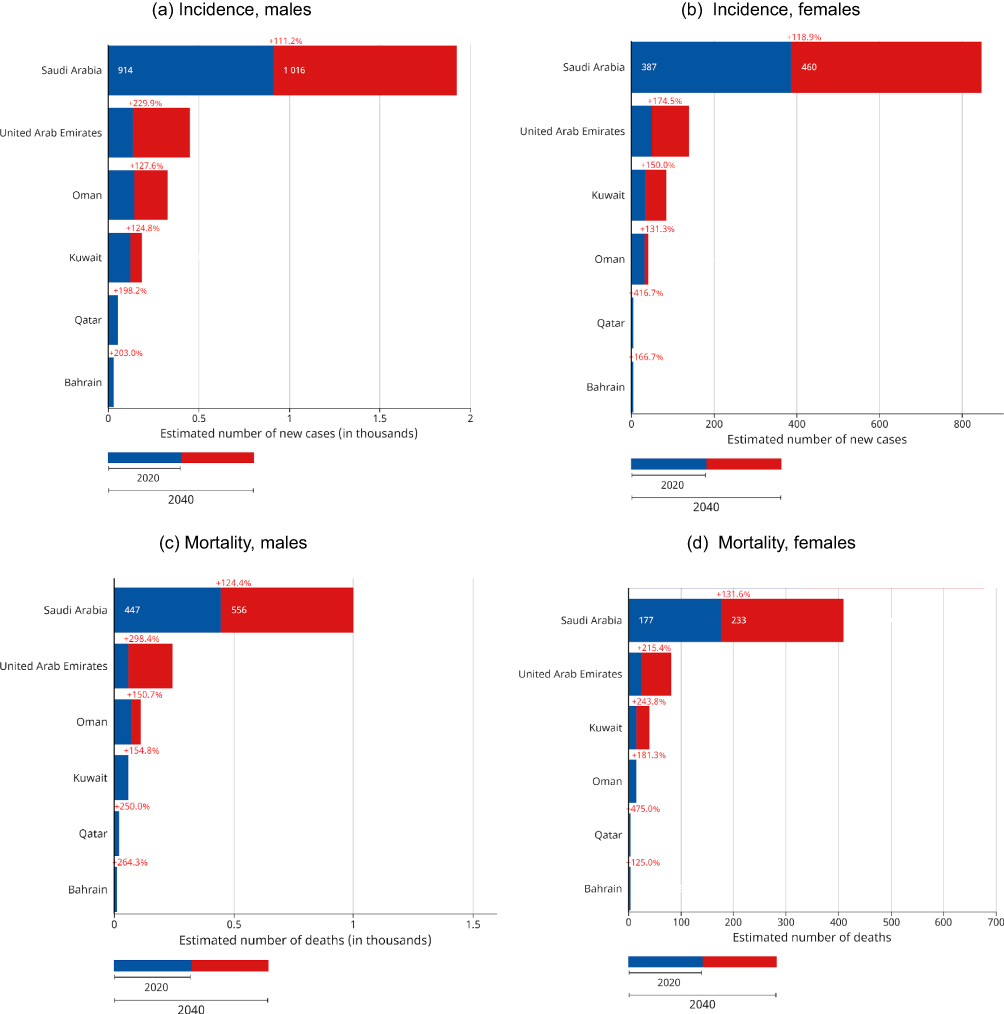 |
Figure 3 Estimated number of new cases and death cases of head and neck cancers and the percentage of change from 2020 to 2040 by country and sex. (a) Estimated number of new HNC cases among males, (b) Estimated number of new HNC cases among females, (c) Estimated number of HNC death cases among males, and (d) Estimated number of HNC death cases among females. |
Discussion
This study examined the regional incidence, mortality rate, and geographic variability of HNCs in the GCC. Oman and Saudi Arabia had the highest ASIR of HNCs, while Bahrain and Qatar had the lowest rates. The differences in the incidence rates may be partly explained by the differences in exposure to numerous risk factors, such as tobacco use26–28 and alcohol consumption,29–31 increased incidence of the human papillomavirus (HPV),32,33 and diet and familial risk34,35 Other risk factors that have a positive correlation with oral and oropharyngeal cancers, such as poor oral hygiene, genetics predispositions, and bacterial infection, are also present in the GCC.36 In two reviews involving studies from GCC countries and the Middle Eastern region, the analysis indicates a strong association between tobacco (eg cigarette, shisha and narghile) and smokeless tobacco (specifically Shamma) and oral cancer.36–38
Oman, Saudi Arabia, and Bahrain have higher cumulative incidence and mortality risk in males, while Qatar has higher mortality risk in females. This result, which aligns with that of other studies,39,40 is because the habits associated with HNCs – tobacco use and alcohol consumption – are strongly associated with males.41 Increasing trends in smoking in GCC countries have been reported in several publications,42–44 and globally, regions with high tobacco use and alcohol consumption tend to have higher HNC rates,34 primarily affecting men.45,46
Sex disparity in HNC incidence and mortality was observed, with males generally having higher rates. In UAE, Qatar, and Bahrain, this trend is reversed, emphasizing the complex nature of these cancers. This raises the question of why Qatari females are affected by a notable rise in new HNC cases or mortality rates compared to females from other GCC countries. These findings could be related to its unique population structure with wide range of ethnic backgrounds, which have been associated with different health behaviours.47 Moreover, increasing HPV infections in women have been observed32,33 in Saudi Arabia and the UAE, which likely contribute to HNCs. Parallel findings are expected in other GCC countries as well. The reported data indicates a notable increase in the overall prevalence of oropharyngeal cancers in certain Gulf region countries, including Saudi Arabia and Arab Emirates, where a rise from 40% to 51% has been observed. This increase may be attributed, in part, to the rising incidence of HPV infections in these regions.36 Increased HPV infection in the GCC can be attributed to a variety of factors, including changes in sexual behavior,48 inadequate vaccination strategies, effective detection methods, and a lack of public awareness of HPV transmission.49,50 In Qatar, HNCs represent 4% of all malignant cancers, with approximately 60% of them being in advanced stages.51,52 These findings emphasise the necessity of tailored healthcare approaches and awareness campaigns to address the unique challenges posed by HNCs.
This study, in addition to depicting the magnitude and distribution of major HNC types in the GCC in 2020, offers two predictions: that, by 2040, HNCs cases could increase by approximately 2.3-fold compared to the levels in 2020, and that fatalities could rise by around 2.5-fold by 2040. These predictions indicate a concerning trend of increasing HNCs and related deaths in the coming years, with Qatar, UAE, and Bahrain expected to bear the brunt of them. Globally, the incidence and mortality rates of HNCs are on the rise, with a projected 30% rise in incidence by 2030.53 HNCs account for a significant portion of all cancers, contributing to 4.9% of incidence and 4.7% of cancer-related deaths, with the highest rates found in Southeast Asia, Western Pacific, and Pacific Asia regions.7
A key distinction in the GCC countries is the substantial shift in the HNC profiles, with an increase in cases and deaths among individuals aged 50 and above, straining the GCC’s healthcare system. However, the reverse trend is expected in Qatar, a demographic change that underscores the importance of age-specific interventions and healthcare strategies. In line with the demographic projections for GCC countries, the average population age rose from 30.2 in 2017 to 31.4 in 2021.54 This demographic shift towards an older population is expected to have implications for HNC incidence and mortality and can burden the healthcare system, particularly in terms of cancer diagnosis and treatment.
In GCC countries where HNC prognosis is poor, this study proposes a few key strategies including raising public awareness, as knowledge about HNCs is notably low.55,56 General educational campaigns as social media can help disseminate information, and dental offices can serve as educational hubs. Collaboration between medical and dental professionals is essential;57 early HNC screening in physicians’ offices, which demands excellent training and robust referral systems. Dentists can also be trained in tobacco cessation and pharmacists in HPV vaccination.58–60 HPV vaccination awareness should be heightened by following successful models, such as the UAE’s free schoolgirl vaccination programme.32 Qatar’s recent approval of the HPV vaccine and cancer screening programs are positive steps.61 Early diagnosis is vital, especially for high-risk groups, such as smokeless tobacco users.28 IARC ‘s Perspectives on oral cancer prevention could guide the policy makers to take necessary action on cancer prevention particularly on tobacco control at country levels.62 Also crucial is overcoming barriers to participate, raising awareness, and promoting screening campaigns.63,64
Implications
GLOBOCAN offers insight into cancer profiles based on country, site, age, and sex. These specifications can help ministries of health, policymakers, and healthcare organisations to formulate the necessary strategies and plans for the care and prevention for the projected increase in HNCs. The potential public health impact of this trend in relation to the underlying causes and prospects are necessary for future cancer control. Understanding the trend and variation in the incidence and mortality of HNCs can help experts from the public health, medical, allied health, nursing, community, and policy makers and cancer prevention advocacy groups to employ evidence-based decision-making in their countries.
Limitations
Since GLOBOCAN uses cancer registries to generate estimates, caution should be made when interpreting them, as some registries may be deficient in terms of quality or comprehensive population coverage. The scope of our study was inherently dependent on the data available in this database, which did not include specific information on paranasal sinuses, nasal cavity cancers and some detailed information on HNC types and subsites. GLOBOCAN also does not account for preventive measures or alterations in risk factors – another plausible factor for imprecision. Additionally, the GLOBOCAN data did not consider the impact of COVID-19 on cancer diagnosis.
Conclusion
Our study provides a comprehensive projection of the incidence and mortality rates of head and neck cancers in the Gulf Cooperation Council (GCC) countries from 2020 to 2040. The analyses reveal a significant projected increase in the burden of these cancers across the GCC region, with notable variations in incidence and mortality rates by country and age group. Our findings highlight the urgent need for comprehensive health policy strategies, particularly focusing on cancer prevention, early detection, and management. Furthermore, these findings have implications for resource allocation and healthcare planning. Policymakers and healthcare providers must consider these projections in their long-term planning to effectively address the growing cancer burden. The recently published Handbook on Oral Cancer Prevention provides scientific evidence on recommended interventions for control of oral cancer, which is a major cancer within the Head and Neck Region.65 Additionally, the data underscores the critical need for targeted research into region-specific risk factors such as age and gender and preventative strategies for the GCC population, to better inform future healthcare interventions.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. GCC Statistical Center (GCC-STAT). GCC statistical atlas; 2018. Available from: GCC_ATLAS_2020_V7_17_Nov_2020_2.pdf (gccstat.org).
2. Shayah MH, Sun Z. Employment in the Gulf Cooperation Council (GCC) countries – current issues and future trends.
3. Khoja T, Rawaf S, Qidwai W, Rawaf D, Nanji K, Hamad A. Health care in gulf cooperation council countries: a review of challenges and opportunities. Cureus. 2017;9(8):e1586. doi:10.7759/cureus.1586
4. The Economist: Economist Intelligence Unit. The GCC in 2020: the gulf and its people.; 2020.
5. Gupta B, Johnson NW, Kumar N. Global epidemiology of head and neck cancers: a continuing challenge. Oncology. 2016;91(1):13–23. doi:10.1159/000446117
6. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
7. Gormley M, Creaney G, Schache A, Ingarfield K, Conway DI. Reviewing the epidemiology of head and neck cancer: definitions, trends and risk factors. Br Dent J. 2022;233(9):780–786. doi:10.1038/s41415-022-5166-x
8. Johnson DE, Burtness B, Leemans CR, Lui VWY, Bauman JE, Grandis JR. Head and neck squamous cell carcinoma. Nat Rev Dis Primers. 2020;6(1):92. doi:10.1038/s41572-020-00224-3
9. Drugan C, Leary S, Mellor T, et al. Head and neck cancer in the south west of England, Hampshire, and the Isle of Wight: trends in survival 1996–2008. Br J Oral Maxillofac Surg. 2013;51(1):19–24. doi:10.1016/j.bjoms.2012.02.013
10. Thomas SJ, Penfold CM, Waylen A, Ness AR. The changing aetiology of head and neck squamous cell cancer: a tale of three cancers? Clin Otolaryngol off J ENT-UK. 2018;43(4):999–1003. doi:10.1111/coa.13144
11. Gillison ML, Chaturvedi AK, Anderson WF, Fakhry C. Epidemiology of human papillomavirus-positive head and neck squamous cell carcinoma. J Clin Oncol off J Am Soc Clin Oncol. 2015;33(29):3235–3242. doi:10.1200/JCO.2015.61.6995
12. Sturgis EM, Cinciripini PM. Trends in head and neck cancer incidence in relation to smoking prevalence: an emerging epidemic of human papillomavirus-associated cancers? Cancer. 2007;110(7):1429–1435. doi:10.1002/cncr.22963
13. Adamowicz JL, Christensen A, Howren MB, et al. Health-related quality of life in head and neck cancer survivors: evaluating the rural disadvantage. J Rural Health. 2022;38(1):54–62. doi:10.1111/jrh.12571
14. World Health Organization. Cancer. Available from: https://www.who.int/health-topics/cancer#tab=tab_1.
15. Amare N, Gintamo B, Tukeni KN, Gebremichael EH, Abera EG. The prevalence of cancer patients requiring palliative care and its associated factors at St. Paul Hospital, Addis Ababa, Ethiopia: a Cross-Sectional Study. Risk Manag Healthc Policy. 2023;16:1203–1214. doi:10.2147/RMHP.S415532
16. Cheema S, Maisonneuve P, Lowenfels AB, Abraham A, Doraiswamy S, Mamtani R. Influence of age on 2040 cancer burden in the older population of the Gulf Cooperation Council (GCC) countries: public health implications. Cancer Control. 2021;28:10732748211027158. doi:10.1177/10732748211027158
17. Aupérin A. Epidemiology of head and neck cancers: an update. Curr Opin Oncol. 2020;32(3):178–186. doi:10.1097/CCO.0000000000000629
18. Warnakulasuriya S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009;45(4–5):309–316. doi:10.1016/j.oraloncology.2008.06.002
19. Ghantous Y, Abu Elnaaj I. Global incidence and risk factors of oral cancer. Harefuah. 2017;156(10):645–649.
20. Sarode G, Maniyar N, Sarode SC, Jafer M, Patil S, Awan KH. Epidemiologic aspects of oral cancer. Dis Mon. 2020;66(12):100988. doi:10.1016/j.disamonth.2020.100988
21. International Agency for Research on Cancer. Global cancer observatory: cancer today. Available from: gco.iarc.fr/today.
22. NHS. Head and neck cancer; 2021. Available from: https://www.nhs.uk/conditions/head-and-neck-cancer/.
23. United Nations Statistics Division. Standard country or area codes for statistical use (M49). Available from: https://unstats.un.org/unsd/methodology/m49/.
24. Ferlay J, Colombet M, Soerjomataram I, et al. Cancer statistics for the year 2020: an overview. Int J Cancer. 2021;149(4):778–789. doi:10.1002/ijc.33588
25. Doll R, Payne P, Waterhouse J. Cancer Incidence in Five Continents: A Technical Report. Berlin: Springer-Verlag; 1966.
26. Al-Jaber A, Al-Nasser L, El-Metwally A. Epidemiology of oral cancer in Arab countries. Saudi Med J. 2016;37(3):249–255. doi:10.15537/smj.2016.3.11388
27. Alsanosy RM. Smokeless tobacco (shammah) in Saudi Arabia: a review of its pattern of use, prevalence, and potential role in oral cancer. Asian Pac J Cancer Prev. 2014;15(16):6477–6483. doi:10.7314/apjcp.2014.15.16.6477
28. Allard WF, DeVol EB, Te OB. Smokeless tobacco (shamma) and oral cancer in Saudi Arabia. Oral Epidemiol. 1999;27(6):398–405. doi:10.1111/j.1600-0528.1999.tb02038.x
29. Sankaranarayanan R, Ramadas K, Thara S, et al. Long term effect of visual screening on oral cancer incidence and mortality in a randomized trial in Kerala, India. Oral Oncol. 2013;49(4):314–321. doi:10.1016/j.oraloncology.2012.11.004
30. Kowalski LP, Franco EL, Torloni H, et al. Lateness of diagnosis of oral and oropharyngeal carcinoma: factors related to the tumour, the patient and health professionals. Eur J Cancer B Oral Oncol. 1994;30B(3):167–173. doi:10.1016/0964-1955(94)90086-8
31. Alqahtani AS, Alqhtani NR, Gufran K, et al. Analysis of trends in demographic distribution of dental workforce in the Kingdom of Saudi Arabia. J Healthc Eng. 2022;2022:1–12. doi:10.1155/2022/5321628
32. Ortashi O, Raheel H, Shalal M. Acceptability of human papilloma virus vaccination among women in the United Arab Emirates. Asian Pac J Cancer Prev. 2014;15(5):2007–2011. doi:10.7314/apjcp.2014.15.5.2007
33. Al-Ahdal MN, Al-Arnous WK, Bohol MF, et al. Human papillomaviruses in cervical specimens of women residing in Riyadh, Saudi Arabia: a hospital-based study. J Infect Dev Ctries. 2014;8(3):320–325. doi:10.3855/jidc.4220
34. Abdul-Hamid G, Saeed NM, Al-Kahiry W, Shukry S. Pattern of head and neck cancer in Yemen. Gulf J Oncolog. 2010;7:21–24.
35. Decker J, Goldstein JC. Risk factors in head and neck cancer. N Engl J Med. 1982;306(19):1151–1155. doi:10.1056/NEJM198205133061905
36. Alqahtani WS, Almufareh NA, Al-Johani HA, et al. Oral and oropharyngeal cancers and possible risk factors across Gulf Cooperation Council countries: a systematic review. World J Oncol. 2020;11(4):173–181. doi:10.14740/wjon1283
37. Quadri MFA, Tadakamadla SK, John T. Smokeless tobacco and oral cancer in the middle east and North Africa: a systematic review and meta-analysis. Tob Induc Dis. 2019;17:56. doi:10.18332/tid/110259
38. Maziak W. The waterpipe: an emerging global risk for cancer. Cancer Epidemiol. 2013;37(1):1–4. doi:10.1016/j.canep.2012.10.013
39. Gilyoma JM, Rambau PF, Masalu N, Kayange NM, Chalya PL. Head and neck cancers: a clinico-pathological profile and management challenges in a resource-limited setting. BMC Res Notes. 2015;8(1):772. doi:10.1186/s13104-015-1773-9
40. da Lilly-Tariah OB, Somefun AO, Adeyemo WL. Current evidence on the burden of head and neck cancers in Nigeria. Head Neck Oncol. 2009;1(1):14. doi:10.1186/1758-3284-1-14
41. Otoh EC, Johnson NW, Mandong BM, Danfillo IS. Primary head and neck cancers in Jos, Nigeria: a re-visit. West Afr J Med. 2006;25(2):92–100. doi:10.4314/wajm.v25i2.28256
42. Al Makadma AS. Adolescent health and health care in the Arab Gulf countries: today’s needs and tomorrow’s challenges. Int J Pediatr Adolesc Med. 2017;4(1):1–8. doi:10.1016/j.ijpam.2016.12.006
43. Awan KH, Hussain QA, Khan S, et al. Accomplishments and challenges in tobacco control endeavors - report from the Gulf Cooperation Council countries. Saudi Dent J. 2018;30(1):13–18. doi:10.1016/j.sdentj.2017.08.003
44. Ahmed A, Alwadey A, Areabi H. Validation of Arabic questionnaire on impact of gulf council countries cigarette package warning labels. J Int Oral Health. 2016;8(3):313
45. Sanghvi LD, Rao DN, Joshi S. Epidemiology of head and neck cancers. Semin Surg Oncol. 1989;5(5):305–309. doi:10.1002/ssu.2980050503
46. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA Cancer J Clin. 2006;56(2):106–130. doi:10.3322/canjclin.56.2.106
47. Bulatao RA, Anderson NBE; National Research Council (US) Panel on Race, Ethnicity, and Health in Later Life. Understanding Racial and Ethnic Differences in Health in Late Life: A Research Agenda. Washington (DC): National Academies Press (US).; 2004. doi:10.17226/11036
48. Alsubaie ASR. Exploring sexual behaviour and associated factors among adolescents in Saudi Arabia: a call to end ignorance. J Epidemiol Glob Health. 2019;9(1):76–80. doi:10.2991/jegh.k.181210.001
49. Husain Y, Alalwan A, Al-Musawi Z, Abdulla G, Hasan K, Jassim G. Knowledge towards human papilloma virus (HPV) infection and attitude towards its vaccine in the Kingdom of Bahrain: cross-sectional study. BMJ Open. 2019;9(9):e031017. doi:10.1136/bmjopen-2019-031017
50. Okunade KS, John-olabode SO. An overview of HPV screening tests to improve access to cervical cancer screening amongst underserved populations: from development to implementation. Risk Manag Healthc Policy. 2022;September:1823–1830.
51. Jboor DH, Al-Darwish MS, Nur U. Oral cancer knowledge, attitude, and practice of dentists in the state of Qatar. Dent J. 2019;7(2):43. doi:10.3390/dj7020043
52. Ministry of development planning and statistics. Sukkan Newsletter. Available from: https://www.mdps.gov.qa/en/statistics/StatisticalReleases/Population/Population/2017/Sukkan_38_En_Dec_2017.pdf.
53. Thomas GR, Gross JH, Stubbs VC. Head and neck squamous cell carcinoma. Genomic Precis Med Oncol Third Ed. 2022;6(1):297–318. doi:10.1016/B978-0-12-800684-9.00018-6
54. Khan HTA, Hussein S, Deane J. Nexus between demographic change and elderly care need in the Gulf Cooperation Council (GCC) countries: some policy implications. Ageing Int. 2017;42(4):466–487. doi:10.1007/s12126-017-9303-9
55. Alqaryan S, Aldrees T, Almatrafi S, Alharbi A, Alhumaid H. Awareness of head and neck cancers in Saudi Arabia. Saudi Med J. 2020;41(4):400–405. doi:10.15537/smj.2020.4.24990
56. Joseph BK, Ali MA, Sundaram DB. Awareness of mouth cancer among adult dental patients attending the Kuwait University dental school clinic. J Cancer Educ. 2016. doi:10.1007/s13187-016-1110-6
57. Kerr AR, Changrani JG, Gany FM, Cruz GD. An academic dental center grapples with oral cancer disparities: current collaboration and future opportunities. J Dent Educ. 2006;68(5):531–541. doi:10.1002/j.0022-0337.2004.68.5.tb03771.x
58. Almaghlouth AK, Bohamad AH, Alabbad RY, Alghanim JH, Alqattan DJ, Alkhalaf RA. Acceptance, awareness, and knowledge of human papillomavirus vaccine in Eastern Province, Saudi Arabia. Cureus. 2022;14(11):e31809. doi:10.7759/cureus.31809
59. Alsous MM, Ali AA, Al Azzam SI, et al. Knowledge and awareness about human papillomavirus infection and its vaccination among women in Arab communities. Sci Rep. 2021:1–8. doi:10.1038/s41598-020-80834-9
60. Husain Y, Alalwan A, Musawi ZA, Abdulla G, Hasan K, Jassim G. Knowledge towards human papilloma virus (HPV) infection and attitude towards its vaccine in the Kingdom of Bahrain: cross-sectional study. BMJ Open. 2019;9:e031017. doi:10.1136/bmjopen-2019-031017
61. Ministry of Public Health. Qatar cancer plan 2023–2026; 2023. Available from: https://qcic.moph.gov.qa/nas/documents/QCP-English.pdf?csrt=4850885234744798392.
62. Bouvard V, Nethan ST. Spe ci a l R e p or t IARC perspective on oral cancer prevention. N Engl J Med . 2022;387(21):1999–2005. doi:10.1056/NEJMsr2210097
63. Theisen C. In different cultures, cancer screening presents challenges. J Natl Cancer Inst. 2004;96(1):10–12. doi:10.1093/jnci/96.1.10
64. Venchiarutti RL, Pho L, Palme CE, Young JM, Clark JR. A qualitative exploration of the facilitators and barriers to early diagnosis and treatment of head and neck cancer: perceptions of patients and carers. Eur J Cancer Care. 2022;May:1–13. doi:10.1111/ecc.13718
65. International Agency on Research for Cancer. IARC handbooks of cancer prevention volume 19. Available from: https://publications.iarc.fr/Book-And-Report-Series/Iarc-Handbooks-Of-Cancer-Prevention/Oral-Cancer-Prevention-2023.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.