Back to Journals » Journal of Pain Research » Volume 18
Focused Extracorporeal Shock Wave Therapy for Hemiplegic Shoulder Pain: A Randomized Crossover Pilot Study in Stroke Patients
Authors Kim H, Hwang SSS, Baik H, Lim I, Choi S, Jeon H ![]() , Shin S, Kim M
, Shin S, Kim M
Received 19 June 2025
Accepted for publication 19 October 2025
Published 12 November 2025 Volume 2025:18 Pages 6073—6083
DOI https://doi.org/10.2147/JPR.S544271
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Heegoo Kim,1,2 Sean Soon Sung Hwang,1 Hongsuk Baik,1 Ikhyun Lim,1 Soyoung Choi,1 HyeongMin Jeon,1,2 Seyoung Shin,1– 3 MinYoung Kim1– 3
1Department of Rehabilitation Medicine, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Republic of Korea; 2Digital Therapeutics Research Team, CHA Future Medicine Research Institute, Seongnam, Republic of Korea; 3Rehabilitation and Regeneration Research Center, CHA University School of Medicine, Seongnam, 13496, Republic of Korea
Correspondence: MinYoung Kim, Department of Rehabilitation Medicine, CHA Bundang Medical Center, CHA University School of Medicine, 59 Yatap-ro, Bundang-gu, Seongnam, Gyeonggi-do, 13524, Republic of Korea, Tel +82 31 780 1872, Email [email protected]
Objective: Focused ESWT (F-ESWT) may be effective in relieving hemiplegic shoulder pain (HSP) in stroke patients. This study aimed to investigate the effects of F-ESWT on hemiplegic shoulder pain (HSP) and to assess potential adverse effects in stroke patients.
Design: A double-blind, randomized crossover pilot study was conducted with six stroke patients (median age 59.5) experiencing HSP (NRS ≥ 4). Participants received two conditions—real F-ESWT and sham F-ESWT— 3 days/week for 2 weeks, separated by a 10-day washout period. Sham F-ESWT was administered by tilting the probe. Pain and function were assessed using the NRS and Shoulder Pain and Disability Index before and after interventions.
Results: No adverse effects occurred. Sonography revealed calcifications and tendinosis. Significant time × condition interactions were noted for NRS and disability scores (p < 0.001). NRS scores significantly reduced after real F-ESWT (p < 0.05), with no change in the sham condition. Pain improvements were observed before and after real F-ESWT sessions (p < 0.05).
Conclusion: These results suggest that the application of F-ESWT in patients with stroke could alleviate HSP. However, further studies are required to confirm this benefit.
Keywords: hemiplegic shoulder pain, focused extracorporeal shock wave therapy, stroke, rehabilitation
Introduction
Hemiplegic shoulder pain (HSP) is a common and debilitating complication after unilateral brain injury, including stroke, with a prevalence of 34 to 84%, significantly affecting the rehabilitation process and overall quality of life.1,2 Usually, stroke-related HSP persists, affecting both the psychological and physiological status of patients, which, in turn, delays the rehabilitation process and reduces their ability to perform activities of daily living. Despite extensive research, no standalone factor has been identified as the definitive cause of HSP. Instead, a multitude of contributing factors and etiologies are known to play roles in its pathology. These conditions include rotator cuff pathology, complex regional pain syndrome, shoulder subluxation, and adhesive capsulitis.3 Current treatments, such as range of motion (ROM) exercises for the shoulder joint and transcutaneous electrical nerve stimulation, have shown limited success in providing clear pain relief. Furthermore, significant complications may arise from injection therapies, steroids, or nonsteroidal anti-inflammatory drugs, particularly in patients with underlying medical conditions.4 Therefore, there is growing interest in noninvasive alternatives that can effectively address HSP with fewer side effects and low risks.5–7
Peripheral musculoskeletal factors and central pain mechanisms such as maladaptive neuroplastic changes, central sensitization, and altered sensory processing are increasingly recognized as important contributors to persistent HSP in stroke survivors.8,9 One promising intervention is extracorporeal shock wave therapy (ESWT), which involves the use of shock waves to stimulate tissue repair and regeneration, reduce pain, and facilitate functional recovery.10–13 Based on the method of operation, ESWT can be divided into focused and radial ESWT (F-ESWT and R-ESWT, respectively), which differ in their shockwave propagation and energy characteristics. R-ESWT, which is generated using pneumatic devices, creates low-energy linear pressure waves that penetrate approximately 3 cm into the skin and cover a broader treatment area. By contrast, F-ESWT uses electromagnetic, electrohydraulic, or piezoelectric sources to produce high-pressure pulses (10–100 MPa), concentrating acoustic energy at a penetration depth of up to 12 cm.14 Among the various F-ESWT generation methods, the piezoelectric type offers distinct advantages, including precise focal targeting, consistent energy delivery, and the ability to stimulate deep tissue structures with minimal discomfort.15,16 To our knowledge, its application in stroke-related HSP has not been previously investigated, representing a novel approach in this clinical context. Additionally, F-ESWT typically involves a relatively short treatment duration and minimal recovery time, enhancing its appeal as a noninvasive therapeutic option.17 Recently, F-ESWT has been demonstrated to be superior to R-ESWT in terms of long-term pain relief in treating non-calcific rotator cuff tendinopathy, which is the most frequent lesion in HSP.18 Furthermore, a randomized, sham-controlled clinical trial of patients with lateral epicondylitis reported that F-ESWT was more effective than R-ESWT in terms of pain and functional measurements of the painful lateral elbow.19
Despite previous research findings on the effects of F-ESWT on pain relief in musculoskeletal pathologies,20–23 its application in persistent HSP is not widely known. Several studies have explored the use of ESWT in stroke-related HSP, reporting potential benefits in pain reduction and functional improvement;4,6 however, evidence specific to focused, piezoelectric F-ESWT remains limited. Considering the difficulty in managing HSP, noninvasive treatments, such as piezoelectric F-ESWT, which have shown potential for pain alleviation, require further investigation in stroke populations. Among various emerging interventions, F-ESWT has gained attention as a noninvasive modality with growing therapeutic potential. Evaluating its clinical efficacy in the management of persistent HSP may offer valuable insights and contribute to the development of safer and more effective rehabilitation strategies for stroke survivors. Despite various treatment options, the management of HSP remains challenging due to limited efficacy and potential side effects, especially among patients with comorbidities, highlighting the need for safer and more effective interventions. To address these challenges within the constraints of a pilot trial, a randomized crossover design was adopted, enabling each participant to serve as their own control and thereby reducing interindividual variability and improving statistical efficiency. Therefore, the present study aims to investigate the effects of F-ESWT on HSP alleviation and ROM improvement of the hemiplegic shoulder joints, as well as to assess potential adverse effects of the technique, in patients with stroke.
Methods
Participants
The inclusion criteria for this study were confirmed unilateral stroke on neuroimaging, more than 1 month after the onset of the brain injury, HSP with a numerical rating scale (NRS) score greater than four out of 10, age over 20 years, and a Mini-Mental State Examination score of 15 or higher (indicating sufficient cognitive function to accurately report pain on the NRS). These criteria were selected based on prior literature identifying similar thresholds for stroke-related shoulder pain studies24,25 and to ensure participants could reliably report subjective pain levels. Participants were excluded if they had traumatic HSP, a high risk of bleeding due to severe coagulopathy, were pregnant, or had a pacemaker/defibrillator in the shockwave field. Additionally, individuals with a full-thickness tear of the rotator cuff, confirmed by ultrasonography before study enrollment, were excluded. Written informed consent was obtained from all participants before the experiments, in accordance with the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of the CHA Bundang Medical Center (Approval No. 2019–12-029) and registered at ClinicalTrials.gov (NCT04320108). Participant recruitment began on May 29, 2020, after obtaining ethical approval from the Institutional Review Board.
Study Design
This study was designed as a pilot exploratory study using a randomized crossover format to preliminarily assess the feasibility and potential F-ESWT on hemiplegic shoulder pain. All participants underwent six sessions of intervention as part of a sham-controlled, patient- and evaluator-blinded, crossover study design. Before the intervention, each participant was asked the standard screening questions recommended in the F-ESWT guidelines to exclude contraindications or precautions. According to the guidelines of the International Society for Medical Shockwave Treatment (ISMST),26 patients were excluded from high-energy F-ESWT if any of the following conditions were identified within the shockwave field: presence of brain tissue or central nervous system structures, vertebral bodies, skull bones, ribs, lung tissue, malignant tumors (not the tumor disease itself, but the tumor being located in the treatment field), significant coagulation disorders, a fetus (in cases of pregnancy), or implanted cardiac devices such as pacemakers or defibrillators. All contraindications were assessed through clinical evaluation and imaging prior to initiating treatment. This precaution ensured the safety and appropriateness of the therapy for all study participants. In the experimental paradigm, all participants underwent two conditions of ESWT intervention—3 days per week, for a total of six sessions within 2 weeks for each condition, separated by a 10-days washout period: 1) Condition 1: real ESWT on the hemiplegic shoulder, and 2) Condition 2: sham ESWT on the hemiplegic shoulder. After the washout period, patients who were initially allocated to Condition 1 underwent the procedures for Condition 2 and vice versa. The order of the conditions was randomly assigned to the participants. An independent research assistant randomly assigned participants to the study groups using a computer-based 1:1 randomization scheme with SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). The intervention allocation was disclosed only to the physiatrist (H.SSS) who conducted the F-ESWT on the patients. Measurements of HSP severity using the NRS and Shoulder Pain and Disability Index (SPADI), as well as ROM of the shoulder joint, were conducted before (T0) and after (T1) the six sessions of intervention by another physiatrist (B.H). Immediately after the six F-ESWT sessions (V1–V6), the severity of subjective shoulder pain was assessed using the NRS by a third physiatrist (C.S).
Adverse events were monitored by a designated clinical researcher (C.S) from study enrollment to completion, including after each intervention. Information regarding medication use was collected through a questionnaire administered to patients. The data were recorded by the researcher (C.S), who was responsible for documenting all relevant patient information throughout the study. The study design is illustrated in Figure 1.
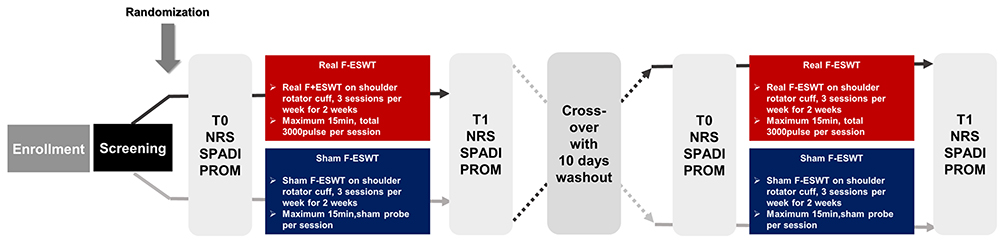 |
Figure 1 Study design. Abbreviations: T0, before 6 sessions of intervention; T1, after completing six sessions of intervention; NRS, numerical rating scale; SPADI, shoulder pain and disability index; PROM, passive range of motion; F-ESWT, focused extracorporeal shock wave therapy. |
Focused ESWT
F-ESWT was administered using the SALUS ESWT-EXPERT® device (REMED Co., Seoul, Korea). The F-ESWT device was equipped with a piezoelectric shock wave generator designed to operate by applying high-voltage electricity to induce vibrations in the piezoelectric element. These vibrations were then aligned to concentrate the generated energy at a single focal point. This focused shock wave energy was directed towards treatment target sites within the body, enabling precise energy delivery.27 A gel pad was affixed to the surface of the transducer, serving as the coupling medium to ensure optimal contact between the transducer and cushion membrane. The treatment sites were the lesser and greater tubercles of the humerus, where the subscapularis and supraspinatus of the shoulder rotator cuff are attached. In the real condition (Condition 1), participants received stimulation at a tolerable intensity level, with 3000 pulses delivered per session. The energy level was set at approximately 0.3 mJ/mm2. For sham stimulation (Condition 2), the probe was positioned at a perpendicular angle such that it did not stimulate the target site.28 While the device was activated and produced sound and slight vibrations similar to the actual treatment, no therapeutic energy was delivered to the affected area. This method mimicked the sensation of real treatment without providing any actual therapeutic effects, thereby ensuring proper blinding of the participants. Each intervention session lasted between 10 and 15 min. Special attention was given to patients aged over 60 to ensure they met safety criteria for F-ESWT, based on ISMST guidelines.
Measurement of Hemiplegic Shoulder Pain and Passive Range of Motion in Hemiplegic Shoulder Joint
The primary outcome of the present study was measured using the NRS before (T0) and after the six sessions of intervention (T1). Furthermore, the NRS score for HSP was measured immediately after each intervention session (V1 to V6). The NRS is a pain severity measurement tool commonly used to assess pain intensity at a specific moment in time, using a 0–10 scale, with zero meaning “no pain” and 10 meaning “the worst pain imaginable”.29 This 11-point NRS has been recommended as a primary endpoint for pain studies by initiative groups focusing on pain assessment in clinical trials.30
The secondary outcome measure, SPADI, was assessed at two time points: before the intervention (T0) and after six sessions of the intervention (T1). The SPADI was developed to measure pain and disability associated with shoulder pathologies.31 It is a self-administered index consisting of 13 items divided into two domains: pain and disability. Each item is scored on a NRS from zero to 10, where zero represents “no pain” or “no difficulty”, and 10 represents “the worst pain imaginable” or “so difficult that assistance is required”. The pain subscale score was calculated by summing the scores of its five items, dividing by 50 (the maximum possible score for the pain subscale), and multiplying by 100 to convert it into a percentage. Similarly, the disability subscale score was calculated by summing the scores of its eight items, dividing by 80 (the maximum possible score for the disability subscale), and multiplying by 100 to yield a percentage. The total SPADI score is the sum of both subscales and ranges from zero to 130, with higher scores indicating greater pain and disability. To calculate the total percentage for the SPADI score, the total score was divided by 130 and then multiplied by 100, yielding a final percentage score on a scale of zero to 100. In the SPADI measurement, the minimal clinically important difference (MCID), used as a measure of responsiveness to an outcome tool, was suggested to be eight,32 which was calculated based on the percentage of the total score. The SPADI takes 5–10 min to complete and is the only reliable and valid region-specific measure for the shoulder.
To measure changes in the movement of the hemiplegic shoulder joint, the PROM of the hemiplegic shoulder joint was measured for flexion, extension, abduction, adduction, and internal and external rotation using a goniometer, according to standard techniques, at T0 and T1.33 The use of NRS and SPADI has been validated in multiple clinical trials for shoulder pathologies,34 and both tools are recommended in pain and functional outcome assessments for shoulder-related rehabilitation.
Statistical Analysis
To determine the statistical significance of the data, SPSS version 25 was used. Six pairs of data points at each time point, including visits, were analyzed for the measured values. First, the Wilcoxon signed-rank test was used to compare baseline measurements in both the real and sham conditions. Second, to assess the change in pain scores during the 10-days washout period in a group of three patients who received real ESWT followed by sham ESWT, the difference between the pain score immediately after real ESWT (T1 of real F-ESWT) and that before sham ESWT (T0 of sham F-ESWT) was analyzed using the Wilcoxon signed-rank test. Third, repeated-measures analysis of variance (RM-ANOVA) was conducted to confirm the time×condition interactions in the measurement variables. Fourth, the Wilcoxon signed-rank test was used to evaluate significant changes in the measurement variables before (T0) and after (T1) the six sessions of F-ESWT within each condition. Fifth, the effect of the measurement day on each condition of the NRS, measured from T0 to immediately after each intervention (V1–V6), was calculated using the Friedman test. Sixth, differences in NRS scores between T0 and V1 were compared using the Wilcoxon signed-rank test. Finally, significant differences in the NRS by condition were obtained using the Mann–Whitney U-test at T0 and each intervention, as well as differences in the percentage of the total SPADI score in each condition. For all analyses, the level of significance was set at p = 0.05.
Results
Study Completion and Basic Characteristics of Participants
All procedures ensured that the participants and assessors were blinded to the condition order administered until the final visit of the sixth participant. No adverse events related to the application of F-ESWT were reported. A total of six participants (five men and one woman, median age 59.5 years [range: 54.5–67.8], and median days since stroke onset 98 days [range: 61.0–535.8]) completed the study procedures. The results of the shoulder sonogram obtained from medical record reviews are presented in Table 1. Before the intervention, there were no significant differences in the measurement variables between the conditions (Wilcoxon signed-rank test, p > 0.05).
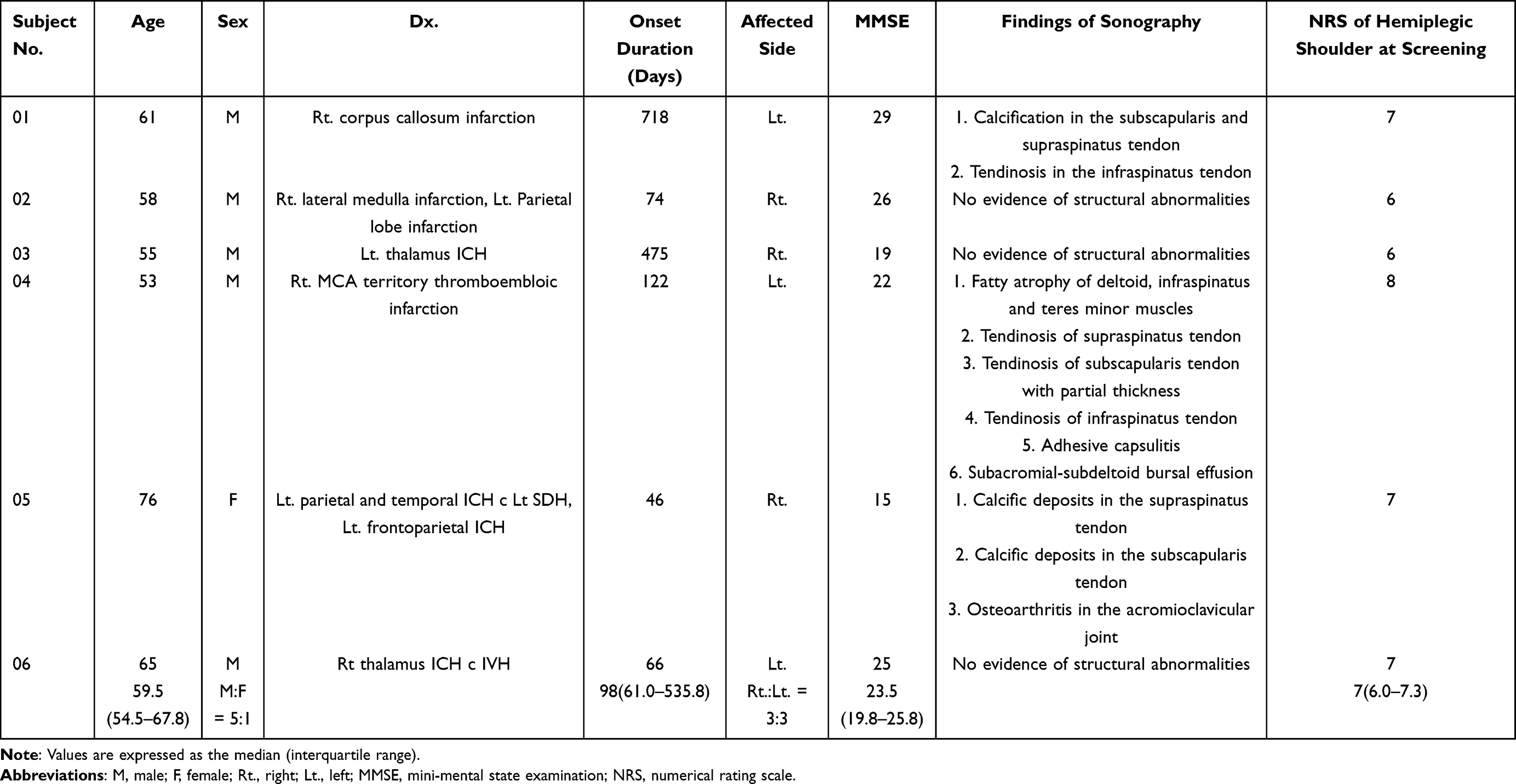 |
Table 1 Basic Characteristics of Study Participants |
Changes in the Primary Outcome
RM-ANOVA revealed a significant time × condition interaction in the NRS for HSP before (T0) and after (T1) the six interventions (F = 25.789, p < 0.001). According to the analysis of the time variables for each condition, significant changes in the NRS scores between T0 and T1 were observed only in the real F-ESWT condition (Wilcoxon signed-rank test, real F-ESWT, p = 0.027; sham F-ESWT, p = 0.327) (Figure 2A).
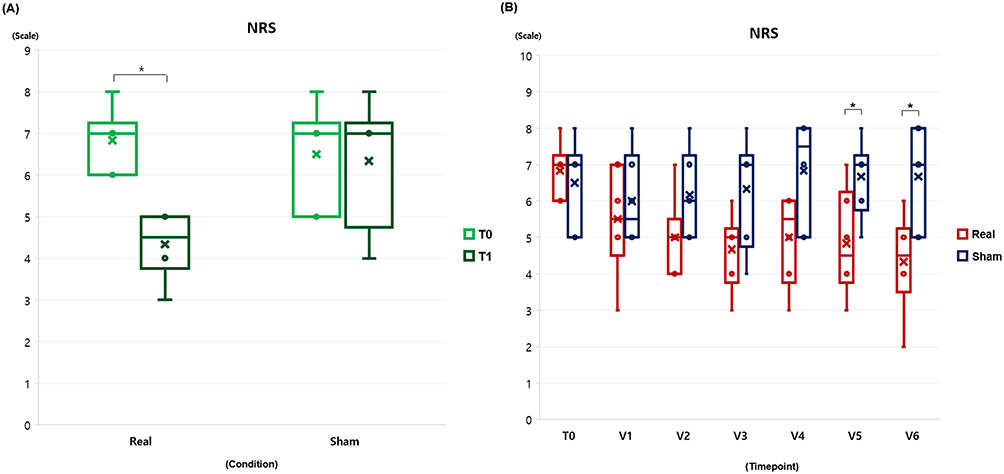 |
Figure 2 Box and whisker plots indicating changes of numerical rating scale. The central line within each box represents the median, while the upper and lower edges of the box denote the 75th and 25th percentiles, respectively, representing the interquartile range (IQR). Circles (o) indicate individual values of subjects, and crosses (x) represent average value of each graph. (A) NRS values before (T0) and after (T1) six sessions of intervention in real and sham F-ESWT conditions, (B) Changes of NRS measured immediately after every intervention in real and sham F-ESWT conditions. Black asterisks indicate statistical significance between T0 and T1 in figure (A) (Wilcoxon signed-rank test, p < 0.05). In figure (B), black asterisks indicate statistical significance between conditions (Mann–Whitney U-test, p < 0.05). Abbreviations: NRS, numerical rating scale; F-ESWT, focused extracorporeal shock wave therapy; T0, before six sessions of intervention; T1, after six sessions of intervention; V1, immediately after the first intervention; V2, immediately after the second intervention; V3, immediately after the third intervention; V4, immediately after the fourth intervention; V5, immediately after the fifth intervention; V6, immediately after the sixth intervention. |
Regarding changes in the NRS measured at T0 and immediately after each intervention, there was a significant time × condition interaction (F = 5.651, p = 0.001). Analyzing the changes in NRS measured at T0 and immediately after each intervention for each condition revealed significant effects of the time factor only in the real F-ESWT condition (Friedman test, real F-ESWT, χ2 = 20.255, p = 0.002; sham F-ESWT, χ2 = 7.750, p = 0.257). This result suggests that pain levels over time were significantly reduced when F-ESWT was applied. The comparison of NRS scores between T0 and immediately after the first intervention in the real F-ESWT condition showed a tendency toward reduction without reaching statistical significance (Wilcoxon signed-rank test, first intervention, p > 0.05). In the comparison of NRS scores immediately after each intervention by condition, the F-ESWT group demonstrated significant pain relief after the intervention. Specifically, there were statistical differences between the real and sham F-ESWT groups at V5 and V6 (Mann–Whitney U-test, p < 0.05). The results of the NRS measurements from T0 to V6 are shown in Figure 2B.
The individual NRS changes for patients in Condition 1 (real F-ESWT followed by sham F-ESWT) and Condition 2 (sham F-ESWT followed by real F-ESWT) are summarized in Tables 2 and 3, respectively. Among the three participants in Condition 1, two exhibited an increase in NRS scores following the 10-day washout period.
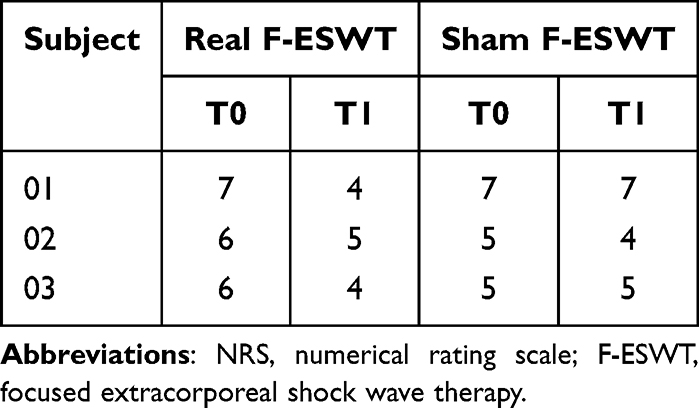 |
Table 2 Individual Value of NRS After Real F-ESWT and Before Sham F-ESWT in Three Participants Who Received Real F-ESWT Followed by Sham F-ESWT |
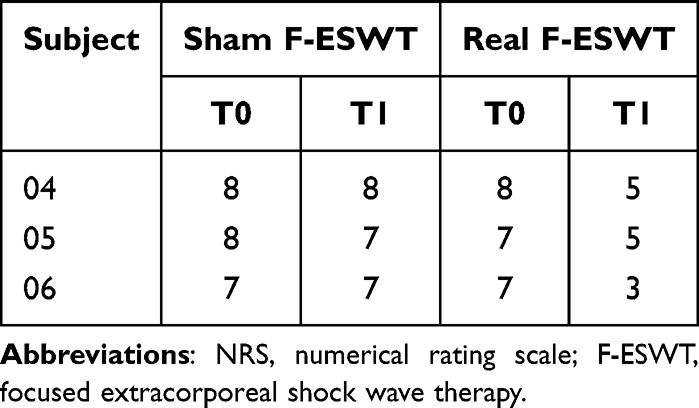 |
Table 3 Individual Value of NRS After Real F-ESWT and Before Sham F-ESWT in Three Participants Who Received Sham F-ESWT Followed by Real F-ESWT |
Changes in Secondary Outcomes
In the SPADI measurements, all subscales and the total percentages showed a significant time × condition interaction (RM-ANOVA, p < 0.05). Significant changes over time were observed in all SPADI subscales and the total percentages within the real F-ESWT condition (Wilcoxon signed-rank test, p < 0.05). However, in the sham condition, no significant changes over time were observed in any SPADI subscale or total SPADI scores (Wilcoxon signed-rank test, p > 0.05) (Figure 3).
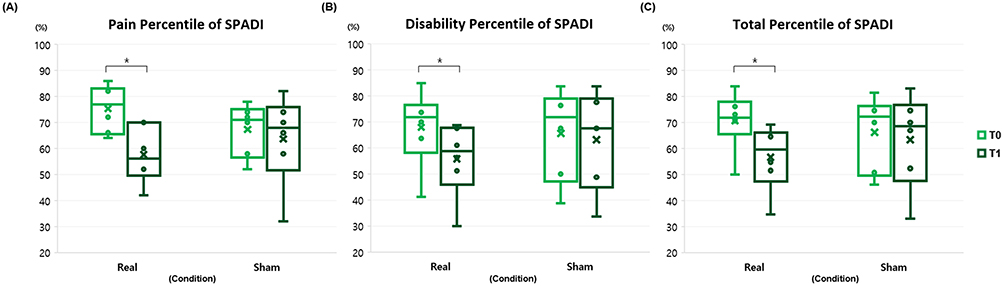 |
Figure 3 Box and whisker plots representing changes of SPADI before and after intervention. The central line within each box represents the median, while the upper and lower edges of the box denote the 75th and 25th percentiles, respectively, representing the interquartile range (IQR). Circles (o) indicate individual values of subjects, and crosses (x) represent average value of each graph. (A) Changes in pain percentile scores of SPADI before (T0) and after (T1) six sessions of intervention in real and sham F-ESWT conditions (B) Changes in disability percentile scores of SPADI before (T0) and after (T1) six sessions of intervention in real and sham F-ESWT conditions (C) Changes in total percentile scores of SPADI before (T0) and after (T1) sox sessions of intervention in real and sham F-ESWT conditions. In all figures, black asterisks indicate statistical significance between before (T0) and after (T1) six sessions of intervention in each condition (Wilcoxon signed rank test, p < 0.05). |
The individual differences in SPADI scores between T0 and T1 are shown in Table 4. In the real F-ESWT condition, five participants demonstrated a change in the total SPADI score percentile that exceeded the MCID threshold of eight points. By contrast, only one participant in the sham condition showed a change exceeding the MCID threshold. Furthermore, there were statistically significant differences in the percentages for all SPADI subscales and the total score between the real and sham F-ESWT conditions (Mann–Whitney U-test, p < 0.05). Conversely, measurements of PROM revealed no statistically significant time × condition interaction for any movements of the hemiplegic shoulder joint (RM-ANOVA, p > 0.05). Additionally, the changes in PROM values between T0 and T1 were not statistically significant in either the real or sham F-ESWT conditions (Wilcoxon signed-rank test, p > 0.05).
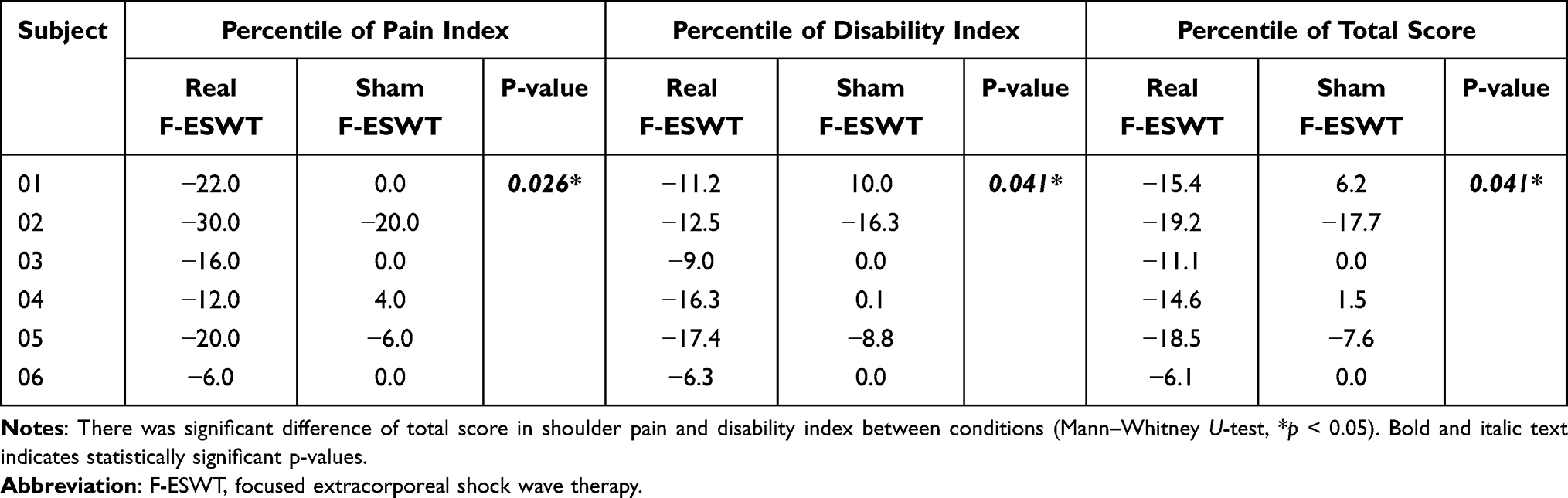 |
Table 4 Individual Value of Differences in Shoulder Pain and Disability Index |
Discussion
In this crossover pilot study, we explored the potential effects of F-ESWT with piezoelectric waves on pain relief in the hemiplegic shoulder joints of patients with stroke. Our preliminary findings were significant time × condition interactions in the NRS and SPADI scores between T0 and T1, revealing the effects of real F-ESWT on HSP. Furthermore, a significant time × condition interaction was observed in the changes in NRS scores measured at T0 and after each intervention. Additionally, significant reductions in NRS scores were observed only in the real F-ESWT group, whereas the sham condition showed no statistically significant improvement, according to the results of the Friedman test. Based on the T0 and T1 results, a significant reduction in HSP was observed only in the real F-ESWT condition. Notably, five participants in the real F-ESWT group exceeded the MCID in SPADI scores, with statistical analysis confirming significant differences compared with the sham group. However, there were no significant changes in PROM measures, and neither group showed notable changes in hemiplegic shoulder joint movements. These results provide compelling evidence that F-ESWT is effective in alleviating shoulder pain and improving shoulder function in this population, as demonstrated by the significant improvements in both NRS and SPADI scores.
Since the successful treatment of kidney stones with extracorporeal shock waves in 1980,35 ESWT has gradually expanded from lithotripsy to chronic pain treatment. Regarding the analgesic mechanism of ESWT, Chen et al36 speculated that this effect involves the promotion of neurotransmitter release, such as β-endorphins, which contribute to relieving pain. ESWT is generally classified into R-ESWT and F-ESWT, with studies reporting that differences in their mechanisms of action result in varying effects on pain alleviation. R-ESWT is effective for surface muscle and broad pain relief, making it suitable for superficial tissue tension or widespread muscle stiffness; however, it may be limited in addressing deep-seated instability.37 Conversely, F-ESWT is known to reach deeper tissues more effectively than R-ESWT, potentially providing better outcomes for deep joint issues, shoulder subluxation, or capsulitis by promoting tissue recovery and reducing inflammation in specific targeted areas.38 Because of its mechanism of action, other clinical trials have revealed that F-ESWT yields superior long-term pain reduction and functional improvement over R-ESWT in treating non-calcific rotator cuff tendinopathy.18 A previous meta-analysis demonstrated the effectiveness of F-ESWT for pain relief, functional restoration, and deposit resorption in calcifying shoulder conditions.39 Recently, clinical trials have been conducted to evaluate the effects of piezoelectric F-ESWT on calcific tendinitis of the rotator cuff, given its advantages of precise focal control, minimal pain and discomfort, uniform energy distribution, and low risk of side effects.40
To the best of our knowledge, this is the first clinical randomized crossover pilot study to suggest the effects of F-ESWT with piezoelectric waves on stroke-induced HSP. Our NRS and SPADI results indicate that F-ESWT using piezoelectric waves is effective in addressing stroke-induced HSP. Furthermore, the SPADI results suggest that the application of F-ESWT to hemiplegic shoulders is effective not only for pain relief but also for functional improvement. These findings suggest that the F-ESWT intervention method used in this study, which enables the delivery of piezoelectric waves to deep tissues, is beneficial for alleviating HSP, a condition often primarily caused by calcification and tendinopathies following stroke. In the shoulder sonography findings described in Table 1, the majority of patients participating in our study presented with calcific deposits and tendinosis in the rotator cuff muscles, which are well-established indications for F-ESWT based on previous studies showing its effectiveness. Additionally, the use of piezoelectric wave-based F-ESWT enabled more precise targeting and effectively stimulated deeper tissue areas to alleviate HSP in our study population. However, among the participants assigned to Condition 1 (real F-ESWT followed by sham F-ESWT), two exhibited a tendency for NRS and SPADI scores to increase at T0 of sham F-ESWT compared to T1 of real F-ESWT. This result suggests that these participants had a relatively long stroke onset duration of over 1 year, indicating that their stroke-induced HSP had become chronic. These findings indicate that the number of intervention sessions in this study may have been insufficient to sustain chronic HSP relief. Furthermore, the absence of significant changes in PROM measurements across both conditions demonstrates that the primary benefit of F-ESWT lies in pain alleviation and functional improvement rather than joint mobility. This may be because of the mechanisms of action of F-ESWT, which likely include soft tissue healing41 and pain modulation induced by the long-lasting degeneration of free nerve endings42 rather than structural changes in joint movement.
Considering the collective findings from previous and present studies examining the effects of F-ESWT on shoulder pain relief, it can be inferred that F-ESWT is a promising therapeutic option for patients with various shoulder conditions. While our findings are encouraging, it is important to interpret them cautiously due to the limitations inherent in pilot research. First, the small sample size limits the generalizability of the results, and further large-scale studies are required to validate the efficacy of F-ESWT in hemiplegic shoulder pain. Second, although participants were required to be over 20 years of age and present with moderate to severe shoulder pain (NRS ≥4), no upper age limit or minimum SPADI score was set as part of the inclusion criteria. This may have introduced variability in the functional status of participants. Third, while traumatic shoulder injuries and full-thickness rotator cuff tear confirmed by ultrasonography were excluded at the time of subject recruitment and thus not part of the study cohort, other common shoulder pathologies such as calcific tendinitis, adhesive capsulitis, and tendinosis were included in enrollment criteria. These conditions, which are frequent findings in stroke patients with shoulder pain, were included to better reflect the practical clinical needs associated with managing this complication. Fourth, clinical assessment of active shoulder joint movements was not sufficiently conducted, which may have limited the understanding of functional improvement beyond pain relief. Fifth, no active follow-up measures were taken during the 10-day washout period, which restricts interpretation of potential carryover effects between interventions. Lastly, because the study focused on short-term outcomes without long-term follow-up or active control conditions, the sustained efficacy and safety profile of repeated F-ESWT treatments remain unclear. Future studies should address these limitations by incorporating stricter inclusion and exclusion criteria, structured follow-up protocols, imaging-based diagnostics, and extended longitudinal designs to better evaluate the clinical utility of F-ESWT.
Conclusion
This pilot study offers preliminary evidence suggesting that piezoelectric F-ESWT may be a promising non-invasive intervention for managing hemiplegic shoulder pain in stroke patients. Improvements in both pain and functional outcomes, as reflected in the NRS and SPADI scores, support the potential utility of this approach. Further large-scale, longitudinal studies are required to establish the clinical efficacy, safety, and optimal application parameters of F-ESWT in this patient population.
Institutional Review Board Statement
This study was conducted in accordance with the guidelines of the Declaration of Helsinki and was reviewed and approved by Institutional Review Board of the Bundang CHA Medical Center.
Data Sharing Statement
The authors do not intend to share individual deidentified participant data or other study documents because the study’s ethical approval and participant consent did not include provisions for data sharing.
Informed Consent Statement
The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Acknowledgment
The ESWT instrument used in this study was afforded by REMED Ltd. (Republic of Korea).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Korea Planning & Evaluation Institution of Industrial Technology, funded by the Ministry of Trade, Industry, and Energy (grant number: RS-2025-08762968) and Ministry of Health and Welfare (grant number: RS-2023-00262005) of the Republic of Korea.
Disclosure
The authors have no potential conflicts of interest to disclose for this work.
References
1. Adey-Wakeling Z, Arima H, Crotty M, et al. Incidence and associations of hemiplegic shoulder pain poststroke: prospective population-based study. Arch Phys Med Rehabil. 2015;96(2):241–247.e1. doi:10.1016/j.apmr.2014.09.007
2. Adey-Wakeling Z, Liu E, Crotty M, et al. Hemiplegic shoulder pain reduces quality of life after acute stroke: a prospective population-based study. American J Physical Med Rehabil. 2016;95(10):758–763. doi:10.1097/PHM.0000000000000496
3. Yoon TS, Kim DH, Park JW, et al. Causes of the hemiplegic shoulder pain. J Korean Acad Rehabil Med. 2010;34(2):158–162.
4. Kim SH, Ha KW, Kim YH, et al. Effect of radial extracorporeal shock wave therapy on hemiplegic shoulder pain syndrome. Ann Rehabil Med. 2016;40(3):509–519. doi:10.5535/arm.2016.40.3.509
5. Abdelhakim EE, Darwish MH, Ahmed SM, Elsherif AA. Hemiplegic shoulder pain: causes and physical therapy management. Egyptian J Physical Ther. 2025;21(1). doi:10.21608/ejpt.2025.360724.1209
6. Zhang T, Zhang C. Extracorporeal shock wave therapy for shoulder pain after stroke: a systematic review and meta-analysis. Clin Rehabil. 2023;37(6):774–790. doi:10.1177/02692155231152134
7. de Sire A, Moggio L, Demeco A, et al. Efficacy of rehabilitative techniques in reducing hemiplegic shoulder pain in stroke: systematic review and meta-analysis. Ann Phys Rehabil Med. 2022;65(5):101602. doi:10.1016/j.rehab.2021.101602
8. Benlidayi IC, Basaran S. Hemiplegic shoulder pain: a common clinical consequence of stroke. Pract Neurol. 2014;14(2):88–91. doi:10.1136/practneurol-2013-000606
9. Wilson RD, Chae J. Hemiplegic shoulder pain. Physical Med Rehabil Clin. 2015;26(4):641–655. doi:10.1016/j.pmr.2015.06.007
10. Lee J-H, Kim E-J. A comprehensive review of the effects of extracorporeal shock wave therapy on stroke patients: balance, pain, spasticity. Medicina. 2023;59(5):857. doi:10.3390/medicina59050857
11. Zelle BA, Gollwitzer H, Zlowodzki M, Bühren V. Extracorporeal shock wave therapy: current evidence. J Orthop Trauma. 2010;24(Supplement 1):S66–S70. doi:10.1097/BOT.0b013e3181cad510
12. Zhang X, Ma Y. Global trends in research on extracorporeal shock wave therapy (ESWT) from 2000 to 2021. BMC Musculoskeletal Disord. 2023;24(1):312. doi:10.1186/s12891-023-06407-9
13. Chung B, Preston Wiley J. Extracorporeal shockwave therapy: a review. Sports Med. 2002;32(13):851–865. doi:10.2165/00007256-200232130-00004
14. Dymarek R, Halski T, Ptaszkowski K, Slupska L, Rosinczuk J, Taradaj J. Extracorporeal shock wave therapy as an adjunct wound treatment: a systematic review of the literature. Ostomy Wound Manag. 2014;60(7):26–39.
15. Iuamoto LR, Hsing WT. Penetration depth and tissue interaction of focused extracorporeal shock waves: an in-vitro investigation. Cureus. 2025;17(3). doi:10.7759/cureus.80205
16. Ramon S, Gleitz M, Hernandez L, Romero LD. Update on the efficacy of extracorporeal shockwave treatment for myofascial pain syndrome and fibromyalgia. Int J Surg. 2015;24:201–206. doi:10.1016/j.ijsu.2015.08.083
17. Ogden JA, Tóth-Kischkat A, Schultheiss R. Principles of shock wave therapy. Clin Orthopaedics Related Res. 2001;387:8–17. doi:10.1097/00003086-200106000-00003
18. Li C, Li Z, Shi L, Wang P, Gao F, Sun W. Effectiveness of focused shockwave therapy versus radial shockwave therapy for noncalcific rotator cuff tendinopathies: a randomized clinical trial. Biomed Res Int. 2021;2021(1):6687094. doi:10.1155/2021/6687094
19. Kaplan S, Sah V, Ozkan S, Adanas C, Delen V. Comparative effects of focused and radial extracorporeal shock wave therapies on lateral epicondylitis: a randomised sham-controlled trial. Methodology. 2020.
20. Abo Al-Khair MA, El Khouly RM, Khodair SA, Al Sattar Elsergany MA, Hussein MI, Eldin Mowafy ME. Focused, radial and combined shock wave therapy in treatment of calcific shoulder tendinopathy. Physic Sports Med. 2021;49(4):480–487. doi:10.1080/00913847.2020.1856633
21. Pellegrino R, Di Iorio A, Filoni S, et al. Radial or focal extracorporeal shock wave therapy in lateral elbow tendinopathy: a real-life retrospective study. Int J Environ Res Public Health. 2023;20(5):4371. doi:10.3390/ijerph20054371
22. Tognolo L, Giordani F, Carlo B, et al. Myofascial points treatment with focused extracorporeal shock wave therapy (f-ESWT) for plantar fasciitis: an open label randomized clinical trial. Eur J Phys Rehabil Med. 2022;58(1):85. doi:10.23736/S1973-9087.21.06814-3
23. Shafshak T, Amer MA. Focused extracorporeal shockwave therapy for youth sports-related apophyseal injuries: case series. J Orthopaedic Surg Res. 2023;18(1):616. doi:10.1186/s13018-023-04065-0
24. Wynne CF, Ling SM, Remsburg R. Comparison of pain assessment instruments in cognitively intact and cognitively impaired nursing home residents. Geriatric Nurs. 2000;21(1):20–23. doi:10.1067/mgn.2000.105793
25. Gandolfi M, Donisi V, Battista S, et al. Health-related quality of life and psychological features in post-stroke patients with chronic pain: a cross-sectional study in the neuro-rehabilitation context of care. Int J Environ Res Public Health. 2021;18(6):3089. doi:10.3390/ijerph18063089
26. Eid J. Consensus statement on ESWT indications and contraindications. Int Soc Med Shockwave Treat. 2016;1–4.
27. Maier M, Tischer T, Gerdesmeyer L. ESWT in orthopedics. Therapeutic Energy Application Urol. 2005;144–153.
28. Speed C, Nichols D, Richards C, et al. Extracorporeal shock wave therapy for lateral epicondylitis—a double blind randomized controlled trial. J Orthop Res. 2002;20(5):895–898. doi:10.1016/S0736-0266(02)00013-X
29. Holdgate A, Asha S, Craig J, Thompson J. Comparison of a verbal numeric rating scale with the visual analogue scale for the measurement of acute pain. Emergency Med. 2003;15(5‐6):441–446. doi:10.1046/j.1442-2026.2003.00499.x
30. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. pain. 2005;113(1):9–19. doi:10.1016/j.pain.2004.09.012
31. Breckenridge JD, McAuley JH. Shoulder pain and disability index (SPADI). J Physiother. 2011;57(3):197. doi:10.1016/S1836-9553(11)70045-5
32. Paul A, Lewis M, Shadforth M, Croft P, Van Der Windt D, Hay E. A comparison of four shoulder-specific questionnaires in primary care. Ann Rheumatic Dis. 2004;63(10):1293–1299. doi:10.1136/ard.2003.012088
33. Clarkson HM. Musculoskeletal Assessment: Joint Range of Motion and Manual Muscle Strength. Lippincott Williams & Wilkins; 2000.
34. Anwer S, Alghadir AH, Al-Eisa ES, Iqbal ZA. The relationships between shoulder pain, rangeof motion, and disability in patients with shoulder dysfunction. J Back Musculoskeletal Rehabil. 2018;31(1):163–167. doi:10.3233/BMR-169762
35. Chaussy C, Brendel W, Schmiedt E. Extracorporeally induced destruction of kidney stones by shock waves. Lancet. 1980;316(8207):1265–1268. doi:10.1016/S0140-6736(80)92335-1
36. Chen YJ, Kuo YR, Yang KD, Wang CJ, Huang HC, Wang FS. Shock wave application enhances pertussis toxin protein‐sensitive bone formation of segmental femoral defect in rats. J Bone Miner Res. 2003;18(12):2169–2179. doi:10.1359/jbmr.2003.18.12.2169
37. Furia JP, Rompe J-D, Maffulli N, Cacchio A, Schmitz C. Radial extracorporeal shock wave therapy is effective and safe in chronic distal biceps tendinopathy. Clin J Sport Med. 2017;27(5):430–437. doi:10.1097/JSM.0000000000000399
38. Poenaru D, Sandulescu MI, Cinteza D. Biological effects of extracorporeal shockwave therapy in tendons: a systematic review. Biomed Rep. 2022;18(2):15. doi:10.3892/br.2022.1597
39. Vavken P, Holinka J, Rompe JD, Dorotka R. Focused extracorporeal shock wave therapy in calcifying tendinitis of the shoulder: a meta-analysis. Sports Health. 2009;1(2):137–144. doi:10.1177/1941738108331197
40. Moya D, Gómez D, Serrano DV, Domínguez PB, Lazzarini ID, Gómez G. Treatment protocol for rotator cuff calcific tendinitis using a single-crystal piezoelectric focused shock wave source. JoVE. 2022;(190):e64426.
41. Zhang D, Kearney CJ, Cheriyan T, Schmid TM, Spector M. Extracorporeal shockwave-induced expression of lubricin in tendons and septa. Cell Tissue Res. 2011;346(2):255–262. doi:10.1007/s00441-011-1258-7
42. Takahashi N, Ohtori S, Saisu T, Moriya H, Wada Y. Second application of low-energy shock waves has a cumulative effect on free nerve endings. Clin Orthopaedics Related Res. 2006;443:315–319. doi:10.1097/01.blo.0000188064.56091.a7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.