Back to Journals » International Journal of Women's Health » Volume 17
Flat Magnetic Stimulation for Anal Incontinence: A Prospective Study
Authors Barba M ![]() , Cola A, Re I, De Vicari D, Costa C, Frigerio M
, Cola A, Re I, De Vicari D, Costa C, Frigerio M ![]() , Da Pozzo B, Maruccia S
, Da Pozzo B, Maruccia S
Received 15 December 2024
Accepted for publication 14 April 2025
Published 21 April 2025 Volume 2025:17 Pages 1115—1122
DOI https://doi.org/10.2147/IJWH.S512439
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Marta Barba,1 Alice Cola,1 Ilaria Re,1 Desirèe De Vicari,1 Clarissa Costa,1 Matteo Frigerio,1 Benedetta Da Pozzo,1 Serena Maruccia2
1Department of Gynecology, IRCCS San Gerardo dei Tintori, University of Milano-Bicocca, Monza, 20900, Italy; 2Department of Urology, ASST Santi Paolo e Carlo, San Paolo Hospital, Milano, 20142, Italy
Correspondence: Matteo Frigerio, Email [email protected]
Introduction: Magnetic Stimulation (MS) works on neuromuscular tissue by creating a specific electromagnetic field capable of inducing an intense muscular contraction thereby deeply stimulating pelvic floor muscles and restoring neuromuscular function in a non-invasive manner. Flat MS (FMS) has a more homogeneous electromagnetic field which permits a greater recruitment of muscle fibers. With this study we aimed to evaluate the severity of symptoms and quality of life before and after treatment with Flat Magnetic Stimulation in women with anal incontinence.
Methods: This was a prospective observational study conducted from September 2023 to December 2023. At baseline and after the treatment, sexual function and the severity of anal incontinence and were evaluated through validated St. Mark’s and the Female Sexual Function Index - 19 (FSFI-19) scores respectively. The subjective improvement rate was determined through the Patient Global Impression of Improvement (PGI-I) questionnaire.
Results: We observed that there was a significant improvement in the St.Mark score both absolute and stratified according to the degree of severity, whereas there was no evidence of improvement in sexual function, accessed with the FSFI-19 score.
Conclusion: FMS represents an effective and safe non-invasive treatment for anal incontinence, resulting in patients’ QOL improvement and decrease of incontinence scores.
Keywords: magnetic stimulation, anal incontinence, pelvic floor, quality of life
Introduction
Anal incontinence (AI) is defined as the involuntary loss of solid or liquid feces or flatus.1 Globally, the median prevalence of AI is 7.7% and ranges between 2% and 20.7% depending on population,2 increasing with age and decreasing when restricting the definition to only involuntary loss of solid and liquid stool (Fecal Incontinence, FI).2,3 However, prevalence may be underestimated as many patients appear reluctant to report it to healthcare providers.4 The main risk factors for AI are bowel disturbances such as diarrhea or constipation, rectal urgency, chronic illness, and anal sphincter trauma (especially due to obstetrical injury), but neurological disorders and other pelvic floor anatomical alterations such as rectal prolapse and descending perineum syndrome can contribute to the insurgence of the condition.5 Moreover, older age, smoking, obesity, limited physical activity, and white race have been found as additional risk factors.6 The pathogenesis is multifactorial as loss of anal continence can arise due to abnormal rectal compliance, dysfunction of the anal sphincter system, altered stool consistency, or alterations in rectal sensation.5,7 In women, the role of Obstetric Anal Sphincter Injuries (OASIS) in the development of AI has been widely discussed.8–11 Symptoms have a significant negative effect on the quality of life of the patients as incontinence can lead to a loss of confidence and self-respect, with severe ramifications on social life.5 According to international guidelines, detailed clinical history and physical examination are sufficient to exclude serious underlying pathologies and direct the first line of treatment.12,13 In patients unresponsive to first line treatment other diagnostic tests such as anal manometry, endoanal and transperineal ultrasound, MRI and fluorodefecography can be employed, especially in those patients with suspected anatomical defects, whereas endoscopy and stool tests may prove useful in patients with suspected gastrointestinal underlying cause.7,14 Initial treatment is conservative: dietary adjustments, lifestyle changes, behavioral therapies, and pharmacological agents have been shown to reduce the frequency and severity of symptoms.12,13,15 Moreover, biofeedback and pelvic floor muscle training aimed at improving sensation, coordination, and strength of the pelvic floor muscles have shown some positive results.16 In unresponsive patients, surgery can be considered: sacral neuromodulation (SNM) is indicated as the first-line surgical option, but this approach can lead to complications such as infection, implementation site pain, seroma, and hematoma formation, despite the total complications’ rate being limited;13,15,17 additionally when a sphincter defect has been clearly identified a sphincteroplasty may be undertaken although clinical effect may be transient.12,13,15,17 New approaches to AI still in clinical evaluation include autologous muscle cell therapy, magnetic sphincter augmentation, and sphincter bulking agents.18–20 Finally, if alternative therapies are not appropriate or have failed, a colostomy could allow patients to resume their normal activities, thus reducing the burden on their quality of life.21
Among the conservative therapies attempted in the management of patients with AI, magnetic stimulation (MS) has been proposed.22 MS works on neuromuscular tissue by creating a specific electromagnetic field capable of inducing intense muscular contraction thereby deeply stimulating pelvic floor muscles and restoring neuromuscular function in a non-invasive manner23–26 [Figure 1]. MS involves some advantages compared to functional electrical stimulation: endocavitary probes are not necessary, the patient is dressed and remains in a comfortable sitting position. Recent technological advances have improved magnetic stimulation equipment allowing for electromagnetic fields with a more homogenous profile: this guarantees an optimized treatment of the pelvic area because all areas can be stimulated with the same intensity thereby ensuring a more cohesive contraction of the pelvic floor and a greater recruitment of muscle fibers. Therefore FMS may be more effective than simple MS in treating neuromuscular dysfunctions.27 However, the application of both techniques to anal incontinence is still vastly unexplored, while many studies exist that study its effect on urinary incontinence.
 |
Figure 1 Magnetic stimulation works on neuromuscular tissue by creating a specific electromagnetic field which is able to optimize the effect on the entire pelvic area, in a non-invasive manner. |
To our knowledge there are currently no studies evaluating the effectiveness of FMS in the treatment of AI. Considering the impact of the AI in the quality of life of patients, it is crucial to discover treatments that are both effective and acceptable to the patient. As a consequence, with this study, we aimed to evaluate the severity of symptoms and quality of life before and after treatment with Flat Magnetic Stimulation in women with anal incontinence.
Materials and Methods
It is a prospective observational study conducted in a tertiary-level Urogynaecology department and included women with AI. Before starting the study we received the approval from the local Ethics Committee (protocol code: MAGCHAIR). Enrollement took place from September 2023 to December 2023 in the outpatients’ group of our institution.
During the period of the study, patients suffering from anal incontinence as the main pelvic floor disorder received a clinical interview. For the purpose of this study, anal incontinence was defined as the self-reported involuntary loss of solid or liquid feces or flatus.2,5
Patients were recruited among those presenting to our pelvic unit. All patients suffering from anal incontinence as the main pelvic floor disorder were evaluated by expert urogynecologists through a clinical interview which also included a pelvic exam and, if needed, an endoanal ultrasound. During the clinical interview patients who respected the criteria listed above were asked to answer, in person, a series of questionnaires to explore the impact of FI on their quality of life. At the baseline, the severity of anal incontinence was evaluated with St. Mark’s score. This is a validated questionnaire that evaluates the rate of incontinence for solid/liquid stool, incontinence for gas and alteration in lifestyle on a scale ranging from 0 (never) to 4 (daily). It also evaluates the need to wear a pad or plug, the use of constipating medication, and the lack of ability to defer defecation for 15 min with a binary option of answer yes (2/4 points) or no (0 points).28 The total score ranges from 0 (complete continence) to 24 (complete incontinence). We further subdivided the patients according to the degree of incontinence: 0–4 (mild), 5–8 (moderate), and more than 8 (severe). Patients were also asked to evaluate the sexual function through the Female Sexual Function Index - 19 (FSFI-19), a self-reported questionnaire with 19 items with 5-point Likert answer scales covering six domains of sexual function (sexual desire, lubrication, arousal, orgasm, pain, and satisfaction).29 A cut-off of 26.5 points has been proposed to differentiate patients with and without sexual disorders. An Italian version of this questionnaire is available and can be used to evaluate sexual dysfunction in very different conditions.30
Patients with a suspected defect of the anal sphincter system were evaluated through endoanal ultrasound (EAUS). EAUS has been proven as the most reliable method to diagnose an anatomical lesion of the muscle of anal sphincter, particularly in the case of internal sphincter’s lesions.31,32 During EAUS the proximal, middle and distal segments of the anal canal are studied, thus allowing for a complete evaluation of the whole structure of both the external (EAS) and internal anal sphincters (IAS). An intact IAS normally appears as a hypoechogenic ring in the proximal and middle anal canal, with a thickness of 2–3 mm, while the EAS presents as a hyperechoic ring surrounding the IAS in the middle anal canal and the anal mucosa distally, varying between 7–9 mm in thickness. In contrast, defects are seen as irregularities in the echogenicity or as thinning of either the IAS and the EAS, usually involving the anterior (obstetric) portion of the sphincter complex especially in the case of a previous OASIs. All 3D-EAUS were performed by an expert urogynecologist (MF) using a Flex Focus 400 (BK Medical) equipped with an anorectal 3D 2052 probe. This is a mechanical multi-frequency transducer with a built-in 3D mover to provide a 360° field of view of the anal canal. Any defect of either sphincter was reported. We considered as significant any full-thickness deficit in IAS and/or EAS greater than a 30° angle in circumferential extension and more than 50% in longitudinal extension.33,34
After proper counseling, patients were asked to choose between different pelvic floor rehabilitation techniques available in our Institution, such as pelvic floor muscle training, endoanal biofeedback and electrostimulation or magnetic stimulation, according to their preference, compliance to follow the treatment, distance from the Hospital or job’s commitments. Exclusion criteria for magnetic stimulation were pregnancy, age less than 18 years, history of neoplasia, arrhythmia, congestive heart failure, recent deep venous thrombosis, fever, acute inflammatory diseases, or fractures in the area of treatment. Moreover, women with insufficient Italian language proficiency, weight more than 160 kg, or with neurostimulators, pacemakers, defibrillators, or ferromagnetic prostheses were excluded.
Patients who choose magnetic stimulation, in the absence of exclusion criteria, were recruited. The FMS protocol was aimed to induce and optimize muscular hypertrophy. The FMS program included 8 sessions of 25 min each, spread over one month (twice a week), with Dr. Arnold (DEKA, Calenzano, Italy). Sessions 1 to 4 followed the Hypotonus/Weakness 1 protocol. Sessions 5 to 8 followed the Hypotonus/Weakness 2 protocol. They consist of a warm-up and muscle activation phase, with the aim of recovering tropism (volume) and muscle tone phase (protocol 1, 20–30Hz) and muscle strength phase (protocol 2, 40–50Hz) in a Trapezoidal shape.
Immediately at the end of the treatment, patients were asked again to score sexual function and the severity of anal incontinence with the St. Mark’s score and the FSFI-19 as previously stated. At the end of the treatment we also asked patients to complete the Patient Global Impression of Improvement (PGI-I) questionnaire.
The PGI-I questionnaire is a 7-point scale that allows a self-evaluation about how much the patient’s disease has improved or worsened compared to a baseline state collected at the beginning of the treatment. This scale rated as 1, very much improved; 2, much improved; 3, minimally improved; 4, no change; 5, minimally worse; 6, much worse; or 7, very much worse.35 An improvement compared to baseline (PGI-I score ≤ 3) was considered as a success. All questionnaires were collected and analyzed by the clinicians responsible for the first recruitment.
We used JMP software version 17 (SAS Institute, Cary, NC, USA) for the statistics. Outcomes were reported as mean ± standard deviation for continuous variables and as number (percentage) for noncontinuous variables. Pre and post-treatment comparisons were performed for objective and subjective outcomes and tested for statistical significance. Differences were tested using a paired T-test for continuous data and Chi-square test for noncontinuous data. Since there were no previous studies on FMS for AI, data on expected outcomes were not available and thus power calculation was not performed. A p-value <0.05 was considered statistically significant.
Results
Forty women were screened. After counseling, 21 female patients were enrolled. Population characteristics are shown in Table 1. None have significant (> stage I) pelvic organ prolapse nor previously underwent hysterectomy. All patients underwent 8 sessions of Flat Magnetic Stimulation according to the described protocol. Baseline and post-treatment symptoms and quality of life are reported in Table 2. Specifically, we observed that there was a significant improvement in the St.Mark score both absolute (T0: 10.3 vs T1: 6.8, p<0.0001) and stratified according to the degree of severity (p < 0.0001), whereas there was no evidence of improvement in sexual function, accessed with the FSFI score (T0: 14.1 ± 12.2; T1:16.1 ± 12.7; p 0.0545). During the treatment there were no adverse events. What’s more, according to the PGI-I score 76% of patients experienced an improvement of their condition. No side effects were reported.
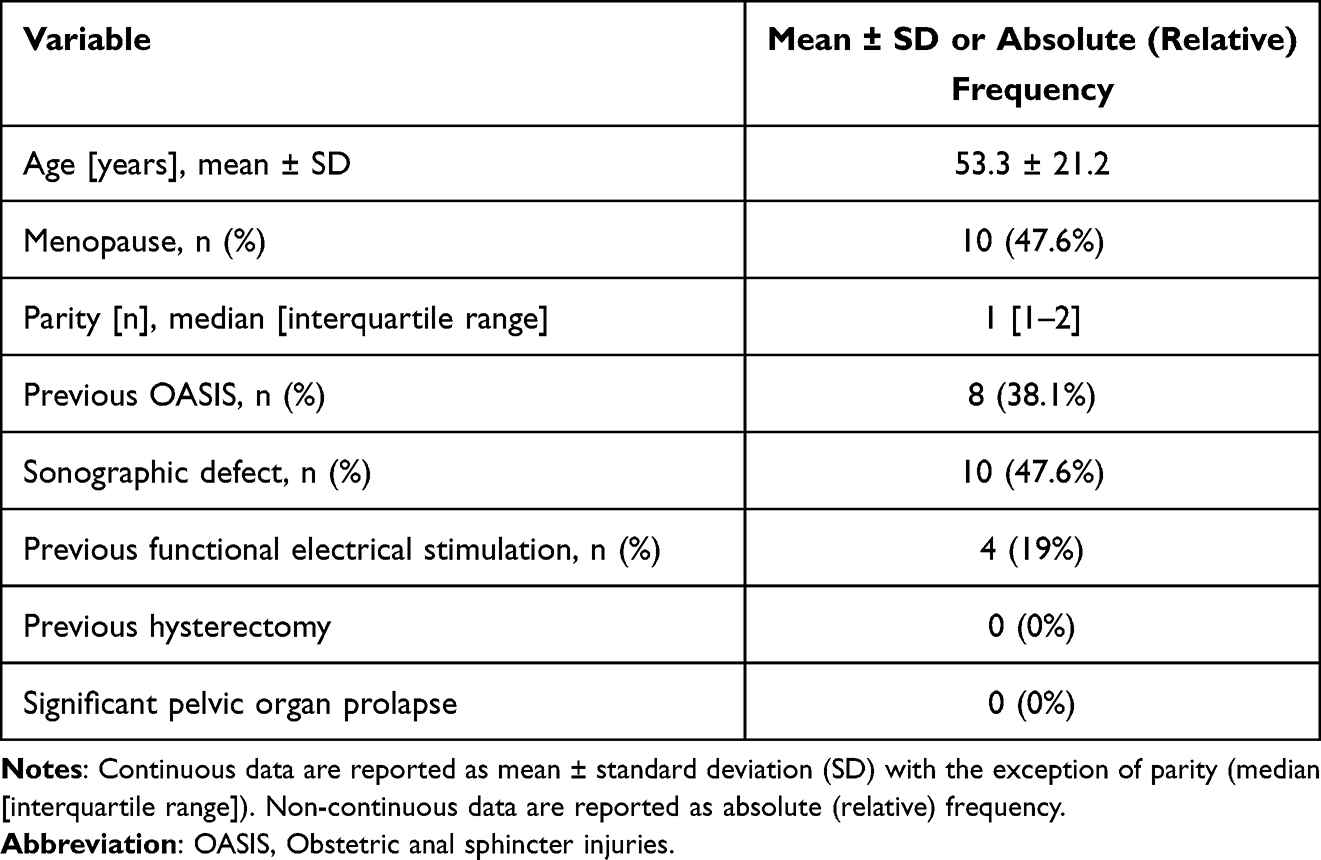 |
Table 1 Population Baseline (T0) Characteristics |
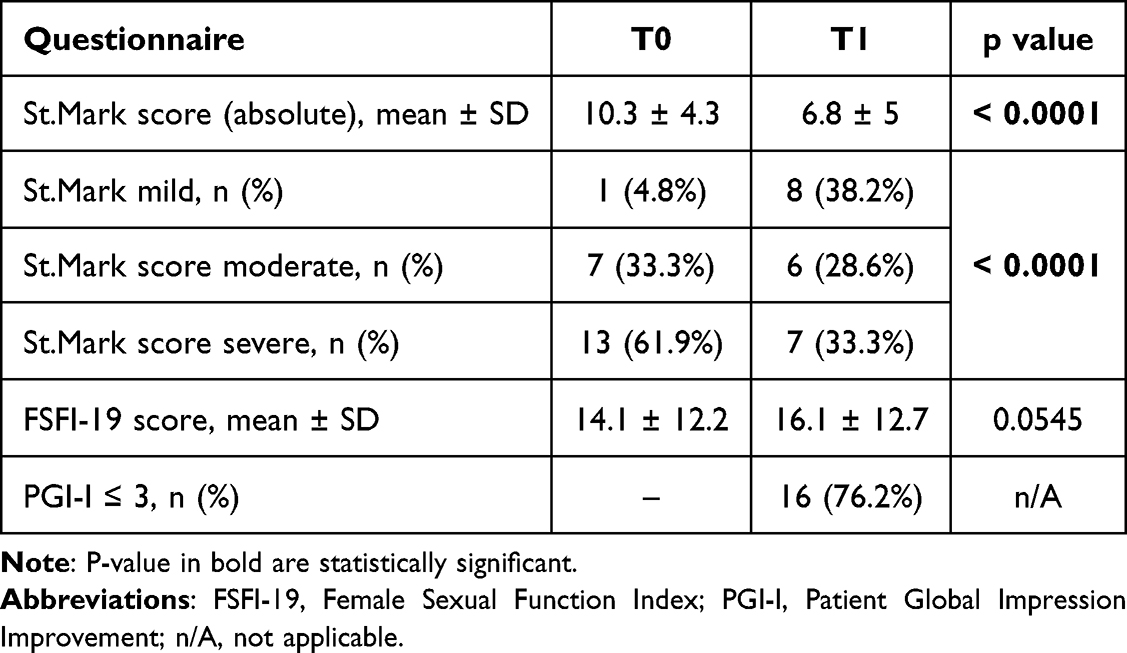 |
Table 2 Pre- (T0) and Post- (T1) Treatment Comparisons |
Discussion
Anal incontinence is a multifactorial disease.5,7 Retention of gas and feces is guaranteed by many continence processes. Anal incontinence arises from a variety of factors such as muscle competence, appropriate innervation, and the intricate working of all these structures collectively.36 As such, treatment is multifaceted ranging from lifestyle changes to surgical options.12,13,15,17 Rehabilitation can be used as a viable conservative alternative: pelvic floor muscle training and endoanal biofeedback have been used with some success in treating AI.16 Compared to electrical stimulation and biofeedback, MS is a type of passive rehabilitation that is performed passively and with no need for vaginal or anal probes, which may cause discomfort among patients: in fact, patients need to be undressed and have an endocavitary plug inserted leading to feelings of shame and discomfort and therefore to poor compliance.26
FMS is a relatively recent method that combines the benefits of electrostimulation with increased compliance. As a new application of a well-known physics principle, FMS implies that a fluctuating magnetic field will cause an electron flow within the field. The magnetic field’s precise pulsation causes tiny currents to flow through the tissue, which in turn causes the nerve axons to depolarize. This results in a nerve impulse that travels in both proximal and distal directions. The acetylcholine relapse that follows will cause the depolarization and contraction of the corresponding muscle fibers; this process of nerve fiber depolarization, which results in muscular strengthening, is essential to the effectiveness of focal muscle stimulation. The pelvic floor muscle groups’ activity is modified by the FMS clinical effect.23
Muscle strength and endurance are increased by the repetitive activation of a muscle’s activity brought on by nerve depolarization, which has a hypertrophic and hyperplastic effect on muscle tissue.24 Compared to functional electrical stimulation, less electrical current is needed to modulate the nerves because of the minor impedance of the tissues than demanded by electrical stimulation.
FMS has been successfully used to treat urinary incontinence. Biondo et al analyzed 81 female patients reporting both SUI and UI. Before starting and after 3 months of follow-up, two questionnaires were administered, IIQ-7 and ICIQ-OAB. The result was a decrease in both urge and stress incontinence complaints, improving patients’ QoL without risk.24 Other two studies conducted in our center demonstrated that FMS is a safe and effective conservative option for SUI and UI management both from an objective and a subjective point of view. Moreover, we observed a substantial rhabdosphincter muscle hypertrophy, consisting of a 15.4% augmentation in muscular total volume.25
While there is currently little research on the subject, the previously outlined concepts related to urine incontinence also apply to anal incontinence. An earlier study assessed the impact of conventional magnetic stimulation on AI. This study enrolled 30 patients who underwent an FMS treatment once weekly for 8 weeks. After this period the number of solid and liquid stool leakage per week was significantly reduced (p<0.05) with a significant improvement of the Cleveland Clinic Fecal Incontinence Score (CCFIS) and fecal incontinence QOL questionnaire (FIQL) (p<0.05).22
However, the current study is the first to report the effectiveness of FMS in the treatment of AI. Our results look promising since 76% of our patients reported an improvement on quality of life after the treatment, which was particularly evident when analyzing specifically the severity of the symptoms. In fact, the St.Mark’s score was significantly reduced after treatment suggesting a quantifiable effect of FMS on the severity of AI. Moreover, the absence of side effects is particularly significant considering that AI often affects older patients who are already burdened by severe comorbidities. We did not found any improvements in sexual function. However, this may be due to the high proportion of sexually inactive women (42.8%).
Therefore our study demonstrated an objective and subjective improvement of anal incontinence and quality of life. This outcome attests to the decline in psychological distress associated with the patients’ clinical state as well as the decline in the pathology-imposed forced modifications to daily living. Therefore, because FMS is non-invasive, painless, and does not need undressing, it significantly improves patient compliance when compared to other means of pelvic floor rehabilitation, such as anal electrostimulation. Because FMS produces neural stimulation, which is capable of penetrating all types of tissue without attenuation and has a lower energy intensity than anal electrostimulation, also discomfort is expected to be significantly reduced.
Limitations
The principal limitation of the study is the small sample size, which precluded any analysis of the effect of covariates and other potential influencing factors (eg diet, physical activity). Furthermore, the long-term recurrence of symptoms following the cessation of magnetic stimulation treatment remains a key point. Long-term follow-up data following stimulation are currently unavailable, given the current study was prospective and centered on evaluating the efficacy of FMS; therefore, research on the ideal duration of stimulation, combination treatments, and randomized controlled studies with a sham-stimulation group are required.
Conclusion
FMS represents a promising non-invasive treatment for anal incontinence, resulting in patients’ QOL improvement and decrease of incontinence scores.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of ASST Monza (protocol code MAGCHAIR), date: 7th July 2022.
Author Contributions
Conceptualization, M.B.; A.C.; D.D.V.; C.C.; M.F.; formal analysis, M.B.; A.C.; D.D.V.; I.R.; C.C.; B. d.P.;S.M.; M.F.; investigation, M.B.; A.C.; D.D.V.; C.C.; M.F.; data curation, M.B.; A.C.; D.D.V.; C.C.; I.R.; B. d.P.; S.M.; M.F.; writing—original draft preparation, M.B.; A.C.; D.D.V.; C.C.; I.R.;B. d.P.; A.V.; S.M.; M.F.; writing—review and editing, M.B.; A.C.; D.D.V.; C.C.; I.R.;B. d.P.;A.V.; M.F.;S.M. project administration M.B.; A.C.; D.D.V.; C.C.; I.R.;B. d.P.; M.F. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Abrams P, Andersson KE, Birder L, et al. Members of Committees; Fourth International Consultation on Incontinence. Fourth international consultation on incontinence recommendations of the international scientific committee: evaluation and treatment of urinary incontinence, pelvic organ prolapse, and fecal incontinence. Neurourol Urodyn. 2010;29(1):213–240. doi:10.1002/nau.20870
2. Ng KS, Sivakumaran Y, Nassar N, Gladman MA. Fecal incontinence: community prevalence and associated factors--a systematic review. Dis Colon Rectum. 2015;58(12):1194–1209. doi:10.1097/DCR.0000000000000514
3. Sperber AD, Bangdiwala SI, Drossman DA, et al. Worldwide prevalence and burden of functional gastrointestinal disorders, results of Rome foundation global study. Gastroenterology. 2021;160(1):99–114. doi:10.1053/j.gastro.2020.04.014
4. Johanson JF, Lafferty J. Epidemiology of fecal incontinence: the silent affliction. Am J Gastroenterol. 1996;91(1):33–36.
5. Bharucha AE, Dunivan G, Goode PS, et al. Epidemiology, pathophysiology, and classification of fecal incontinence: state of the science summary for the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) workshop. Am J Gastroenterol. 2015;110(1):127–136. doi:10.1038/ajg.2014.396
6. Ditah I, Devaki P, Luma HN, et al. Prevalence, trends, and risk factors for fecal incontinence in United States adults, 2005–2010. Clin Gastroenterol Hepatol. 2014;12(4):636–643. doi:10.1016/j.cgh.2013.07.020
7. Bharucha AE, Knowles CH, Mack I, et al. Faecal incontinence in adults. Nat Rev Dis Primers. 2022;8(1):53. doi:10.1038/s41572-022-00381-7
8. Sultan AH, Kamm MA. Faecal incontinence after childbirth. Br J Obstet Gynaecol. 1997;104(9):979–982.
9. Willis S, Faridi A, Schelzig S, et al. Childbirth and incontinence: a prospective study on anal sphincter morphology and function before and early after vaginal delivery. Langenbecks Arch Surg. 2002;387(2):101–107. doi:10.1007/s00423-002-0296-8
10. Guzmán Rojas RA, Salvesen KÅ, Volløyhaug I. Anal sphincter defects and fecal incontinence 15-24 years after first delivery: a cross-sectional study. Ultrasound Obstet Gynecol. 2018;51(5):677–683. doi:10.1002/uog.18827
11. Frigerio M, D’Alessandro G, Re I, Cola A, Vergani P, Barba M. Clinical, ultrasonographic, and functional outcomes after obstetric anal sphincter injury primary repair: a single-center experience. Int J Gynaecol Obstet. 2023;163(1):234–242. doi:10.1002/ijgo.14819
12. Bordeianou LG, Thorsen AJ, Keller DS, et al. The American society of colon and rectal surgeons clinical practice guidelines for the management of fecal incontinence. Dis Colon Rectum. 2023;66(5):647–661.
13. Assmann SL, Keszthelyi D, Kleijnen J, et al. Guideline for the diagnosis and treatment of faecal incontinence-A UEG/ESCP/ESNM/ESPCG collaboration. United Eur Gastroenterol J. 2022;10(3):251–286. doi:10.1002/ueg2.12213
14. Carrington EV, Scott SM, Bharucha A, et al; International anorectal physiology working group and the international working group for disorders of gastrointestinal motility and function. Expert consensus document: advances in the evaluation of anorectal function. Nat Rev Gastroenterol Hepatol. 2018;15(5):309–323. doi:10.1038/nrgastro.2018.27
15. Norton C, Whitehead WE, Bliss DZ, Harari D, Lang J. Conservative management of fecal incontinence in adults committee of the international consultation on incontinence management of fecal incontinence in adults. Neurourol Urodyn. 2010;29(1):199–206. doi:10.1002/nau.20803
16. Norton C, Cody JD. Biofeedback and/or sphincter exercises for the treatment of faecal incontinence in adults. Cochrane Database Syst Rev. 2012;2012(7). doi:10.1002/14651858.CD002111.pub3
17. Thaha MA, Abukar AA, Thin NN, Ramsanahie A, Knowles CH. Sacral nerve stimulation for faecal incontinence and constipation in adults. Cochrane Database Syst Rev. 2015;2015(8):CD004464. doi:10.1002/14651858.CD004464.pub3
18. Frudinger A, Gauruder-Burmester A, Graf W, et al. Skeletal muscle-derived cell implantation for the treatment of fecal incontinence: a randomized, placebo-controlled study. Clin Gastroenterol Hepatol. 2023;21(2):476–486.e8. doi:10.1016/j.cgh.2022.07.039
19. Pakravan F, Helmes C. Magnetic anal sphincter augmentation in patients with severe fecal incontinence. Dis Colon Rectum. 2015;58(1):109–114. doi:10.1097/DCR.0000000000000263
20. Ratto C, Parello A, Donisi L, et al. Novel bulking agent for faecal incontinence. Br J Surg. 2011;98(11):1644–1652. doi:10.1002/bjs.7699
21. Ivatury SJ, Wilson LR, Paquette IM. Surgical treatment alternatives to sacral neuromodulation for fecal incontinence: injectables, sphincter repair, and colostomy. Clin Colon Rectal Surg. 2021;34(1):40–48. doi:10.1055/s-0040-1714285
22. Brusciano L, Gambardella C, Gualtieri G, et al. Effects of extracorporeal magnetic stimulation in fecal incontinence. Open Med. 2020;15(1):57–64. doi:10.1515/med-2020-0009
23. Sun K, Zhang D, Wu G, et al. Efficacy of magnetic stimulation for female stress urinary incontinence: a meta-analysis. Ther Adv Urol. 2021;13:17562872211032485. doi:10.1177/17562872211032485
24. Biondo A, Gonzalez Isaza P, Fusco I. Efficacy of top flat magnetic stimulation technology for female stress and urge urinary incontinence: a clinical evaluation. World J Nephrol Urol. 2022;11(1):18–23. doi:10.14740/wjnu432
25. Barba M, Cola A, Rezzan G, et al. Flat magnetic stimulation for urge urinary incontinence. Medicina. 2023;59(11):1999. doi:10.3390/medicina59111999
26. Takahashi S, Kitamura T. Overactive bladder: magnetic versus electrical stimulation. Curr Opin Obstet Gynecol. 2003;15(5):429–433. doi:10.1097/00001703-200310000-00012
27. Frigerio M, Barba M, Cola A, et al. Flat magnetic stimulation for stress urinary incontinence: a prospective comparison study. Bioengineering. 2023;10(3):295. doi:10.3390/bioengineering10030295
28. Roos AM, Sultan AH, Thakar RS. Mark’s incontinence score for assessment of anal incontinence following obstetric anal sphincter injuries (OASIS). Int Urogynecol J Pelvic Floor Dysfunct. 2009;20(4):407–410. doi:10.1007/s00192-008-0784-7
29. Neijenhuijs KI, Hooghiemstra N, Holtmaat K, et al. The Female Sexual Function Index (FSFI)-a systematic review of measurement properties. J Sex Med. 2019;16(5):640–660. doi:10.1016/j.jsxm.2019.03.001
30. Filocamo MT, Serati M, Li Marzi V, et al. The Female Sexual Function Index (FSFI): linguistic validation of the Italian version. J Sex Med. 2014;11(2):447–453. doi:10.1111/jsm.12389
31. Nielsen MB, Hauge C, Pedersen JF, Christiansen J. Endosonographic evaluation of patients with anal incontinence: findings and influence on surgical management. AJR Am J Roentgenol. 1993;160(4):771–775. doi:10.2214/ajr.160.4.8456663
32. Sultan AH, Kamm MA, Talbot IC, Nicholls RJ, Bartram CI. Anal endosonography for identifying external sphincter defects confirmed histologically. Br J Surg. 1994;81(3):463–465. doi:10.1002/bjs.1800810349
33. Roos AM, Thakar R, Sultan AH. Outcome of primary repair of obstetric anal sphincter injuries (OASIS): does the grade of tear matter? Ultrasound Obstet Gynecol. 2010;36(3):368–374. doi:10.1002/uog.7512
34. Starck M, Bohe M, Valentin L. Results of endosonographic imaging of the anal sphincter 2-7 days after primary repair of third- or fourth-degree obstetric sphincter tears. Ultrasound Obstet Gynecol. 2003;22(6):609–615. doi:10.1002/uog.920
35. Srikrishna S, Robinson D, Cardozo L. Validation of the Patient Global Impression of Improvement (PGI-I) for urogenital prolapse. Int Urogynecol J. 2010;21(5):523–528. doi:10.1007/s00192-009-1069-5
36. Heitmann PT, Vollebregt PF, Knowles CH, Lunniss PJ, Dinning PG, Scott SM. Understanding the physiology of human defaecation and disorders of continence and evacuation. Nat Rev Gastroenterol Hepatol. 2021;18(11):751–769. doi:10.1038/s41575-021-00487-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.