Back to Journals » International Medical Case Reports Journal » Volume 13
FLACS in Congenital Iris Coloboma: A Useful Technique
Authors Balamoun AA ![]() , El Bahrawy M
, El Bahrawy M ![]()
Received 25 May 2020
Accepted for publication 5 August 2020
Published 25 August 2020 Volume 2020:13 Pages 371—378
DOI https://doi.org/10.2147/IMCRJ.S263182
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video of "FLACS in Congenital Iris Coloboma: A Useful Technique" [ID 263182].
Views: 865
Ashraf Armia Balamoun,1,2 Mohamed El Bahrawy1,2
1Al Watany Eye Hospital (WEH), Cairo, Egypt; 2Watany Research and Development Center (WRDC), Cairo, Egypt
Correspondence: Ashraf Armia Balamoun 13 El Ebour Buildings, Salah Salem Street, Heliopolis, Cairo 11371, Egypt
, Tel +20 12-2314-2814
Email [email protected]
Abstract: This paper reports the technique and outcome of femtosecond laser-assisted cataract surgery (FLACS) in an iris coloboma patient (59-year-old male patient) with bilateral grade 3 cataractous lens and a shallow anterior chamber. Best-corrected visual acuity (BCVA) was 0 on logMAR with spherical equivalent (SE) 9 D in the right eye, and BCVA of 0.3 logMAR with a SE 8.75 D in the left. FLACS was performed on the left then the right eye using the Catalys platform of Johnson & Johnson (intraocular lens implantation of AMO Tecnis 1 ZCB00). Customized parameters were constructed to create capsulotomies of 4.54.7 mm for the left and right eyes, respectively, with manual centration of the distorted pupils. On the second day of follow-up, left-eye BCVA was 0.5 with SE 1 D, and right-eye BCVA was 1 with SE − 0.75 D. At the 1-year follow-up, eyes showed stable bilateral Tecnis 1 IOL and refraction. FLACS is a safe surgical option with stable outcomes in cases of cataract with iris coloboma.
Keywords: FLACS, cataract, iris coloboma
Background
The normal structure of the iris plays an important role in a great number of physiological functions in the human eye, includes regulating the amount of light entering the eye,ensuring proper depth of focus, and regulation of total visual aberration.1 An abnormal iris-diaphragm structure can be a result of a number of pathological conditions, such as iris coloboma, aniridia, and traumatic or surgical iris defect. All of these cause a series of visual debilitating symptoms, such as photosensitivity, glare, uniocular diplopia, and decreased visual capacity.2 Patients presenting with congenital iris defects will present with other comorbidities, including lens pathologies, in the form of cataracts and lens dislocation,3,4 which are considered a great surgical challenge in the management of such cases.
Surgical management of cataract extraction and intraocular lens (IOL) implantation in cases with iris defects can vary widely, according to the extent of the defect and the stability of the lens, and this must be handled with great caution due to associated ocular malformations, such as zonular deficiency, poor pupillary dilatation, or microphthalmos. All this results increased risk of retinal detachment, associated maculopathy, or poor surgical results.5,6 The introduction of state-of-the-art femtosecond laser-assisted cataract surgery (FLACS) was debatable in terms of the value of integration of this technology into conventional cataract surgery. Still, many reports have demonstrated the relative superiority of FLACS or conventional cataract surgery in the accuracy and safety of capsule fashioning and lens-matter manipulation.7
Proper docking is a critical part of the proficiency of the FLACS procedure. Whether by applanating or nonapplanating docking systems, the nonapplanating liquid system will induce less intraocular pressure change (17.7±2.1 versus 32.4±3.4 mmHg in the applanating contact system), as well as less mean eye movement. The user-friendly interface of the FLACS system gives the surgeon good control over a number of functions, including treatment zones in both the cornea and anterior-lens capsule in respect to the pupil and limbus. Following the desired cuts, the possibility of lens fragmentation and softening is available for the surgeon.7 To the best of our knowledge, there have been no reports on utilization of FLACS in the management of challenging cataract extraction in cases of iris coloboma, and thus we report here our surgical technique in using FLACS in a colobomatous iris case.
Patient Data
A 59-year-old male patient working as a diver was referred for routine ophthalmic examination and refraction because of recent progressive decline in his visual acuity with his current prescribed glasses. He reported a number of medical conditions, including hypertension, hyperlipidemia, and ischemic heart diseases, for which he had undergone a cardiac stent procedure with a regular dose of 75 mg aspirin. Best-corrected distance visual acuity was 0 on logMAR, with a spherical equivalent (SE) of 9 D for the right eye and 0.3 on logMAR with an SE of 8.75 D in the left eye, with evident amblyopia in the left eye. On examination, he was diagnosed with bilateral cataract, with normal intraocular pressure (IOP) and normal fundus-examination results in both eyes. The patient was counseled about his condition, with the recommendation of a phacoemulsification cataract-extraction procedure in both eyes. At the same time, he was informed about the challenging nature of such a procedure in his case, because of the risk of complication and postoperative residual refractive error due to the shallow anterior chamber and the present iris defect. Knowing the potential risks, the patient decided to postpone the surgical option for some time. At his 6-months follow-up, he decided to proceed with the surgical intervention, as he was annoyed with the halos and glare caused by his cataracts, markedly affecting his work as a diver. The patient requested the best-possible available technology to be used in his surgery, and even requested that it be performed with the FLACS technique.
Our surgical team consulted the technical support and medical advisory team of the FLACS platform Catalys (Johnson and Johnson, Jacksonville, USA). Their local team and the international office confirmed that there had been no experience of a similar case, and none of the platform users worldwide reported using it in the management of such a case, meaning that the use of FLACS in this case was off-label. The surgeon discussed with the patient that the procedure was off-label, and the patient confirmed acceptance of the nature of the procedure, as well as the possibility of the use his details for publication, through written informed consent.This investigation was approved by the Watany Research and Development Center (WRDC) ethics committee before surgery was performed.
Surgical Technique
The surgeries were planned separately, starting with the left eye, which had lower visual potential. A surgical team was set for this procedure, including an on-site technical support team from the FLACS-platform manufacturer. The first challenge started in the investigative unit during the IOL power calculation and selection, as axial length was 21.00 and 21.15 mm, while anterior-chamber depth was 2.87 and 2.79 mm for the left and right eyes consecutively (Figures 1–5). The short and shallow configurations of the eye demanded the use of IOL power of 33.5 D with residual refraction of −0.2 D for the left eye and 33.0 D with residual refraction of 0.1 D for the right eye.
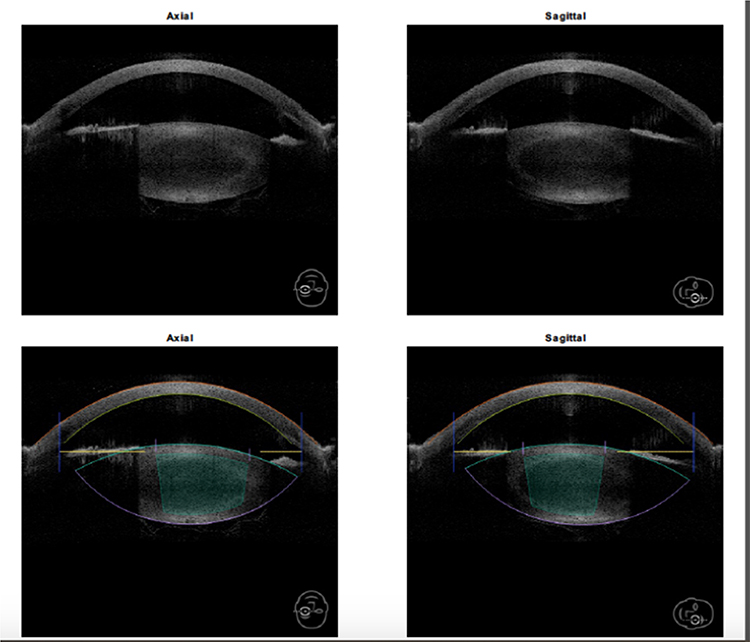 |
Figure 1 Anterior OCT of the left eye. |
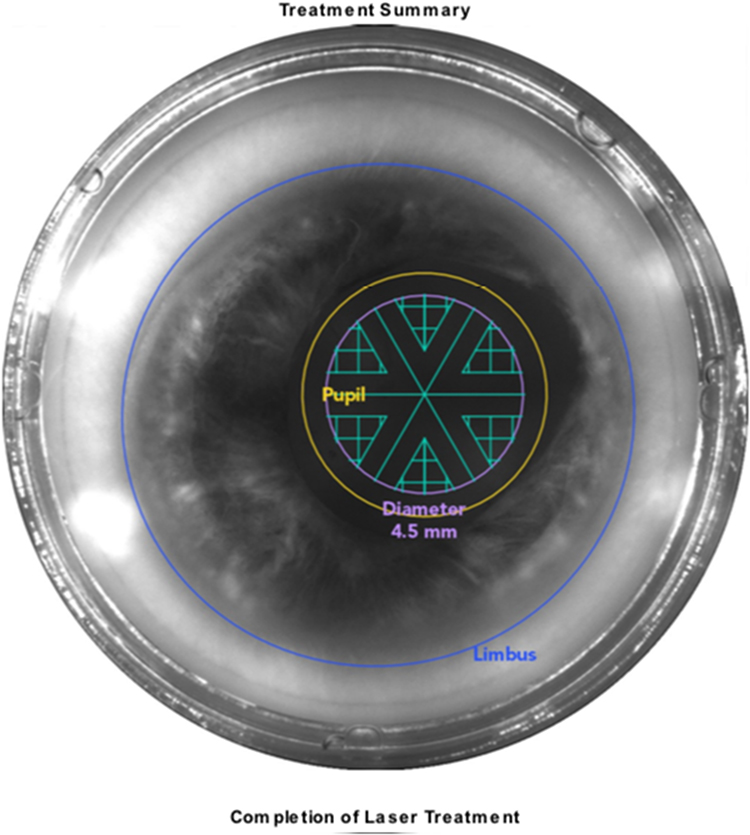 |
Figure 2 Capsulotomy and fragmentation alignment of the left eye. |
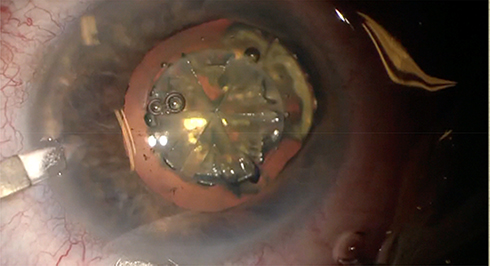 |
Figure 3 Fragmented nucleus of the left eye. |
 |
Figure 4 FLACS parameters for the left eye. |
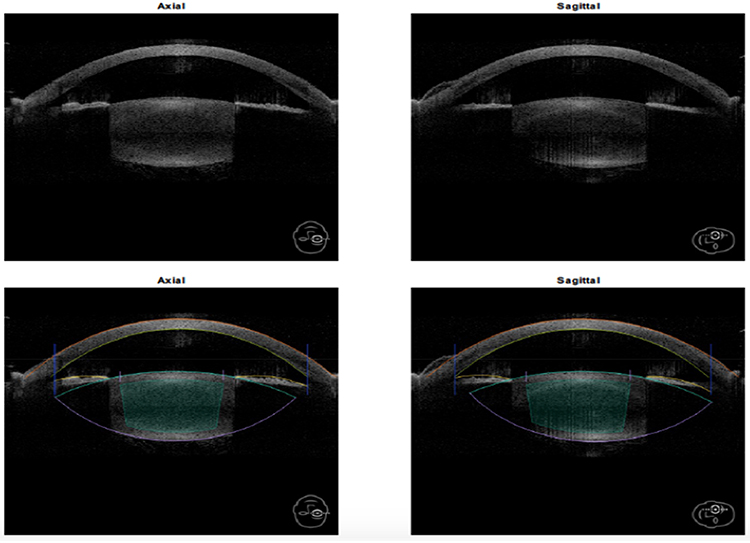 |
Figure 5 Anterior OCT of the right eye. |
Peribulbar local anesthesia was administered to enhance eye protrusion because of the micro-ophthalmic nature of the eye. This improved the docking of the femtolaser cataract platform used. Docking was done without using a speculum, and suction was ensured. When the treatment was applied, starting to create a capsulotomy of 4.8 mm, a system error stopped the treatment. It was decreased to 4.5 mm for the left eye and 4.7 mm for the right eye (Figures 2 and 6), and an error of centration was still there. Adjustment was done by moving the capsulotomy manually on the screen to align it in an area away from the undilated part of the iris coloboma. The treatment was restarted, and this time the machine completed a fine paracentral capsulorhexis. In the management of the nucleus, a six-quadrant division with softening was applied in the left eye, while six-quadrants division only was applied in the right eye, being less hard (Figures 3 and 7). After completion of all the steps of the femtosecond laser treatment (Figures 4 and 8), the patient was moved to the surgical room to continue the cataract-extraction procedure. Sterilization was done with betadine 5% for the skin and the eyelids, including the lashes, with protection of the cornea with an ocular viscoelastic device (OVD). A noncompressing special eye speculum was used so as not to produce any positive pressure or wildly open the eyelids. Two paracentesis openings (1.2 mm) were created using a diamond blade, and a 2.2 mm clear corneal tunnel wound was also created using a diamond keratome (Video 1). A double OVD coat was used to protect the cornea, and a highly cohesive OVD (Helon GV) was used to maintain the shallow anterior chamber (3.1 mm) in both eyes. Removal of the capsule was done by a capsulorhexis forceps (Rumex, India), followed by a careful hydrodissection with a gentle press on the nucleus to get the air bubbles trapped within the small capsulorhexis. Quadrant removal was done using a low flow rate and low vacuum to maintain the shallow anterior chamber using a Centurion phacoemulsification device (Alcon, Fort Worth, TX, USA). The irrigation aspiration was a challenge to remove the sticky cortex through the narrow capsulorhexis. Finally, intraocular implantation of a Tecnis 1 aspheric IOL (Johnson and Johnson, Jacksonville, USA) was performed, followed by removal of the OVD and hydration of the wounds (Video 1). The left and right eyes were operated on successively, with 1 week in between.
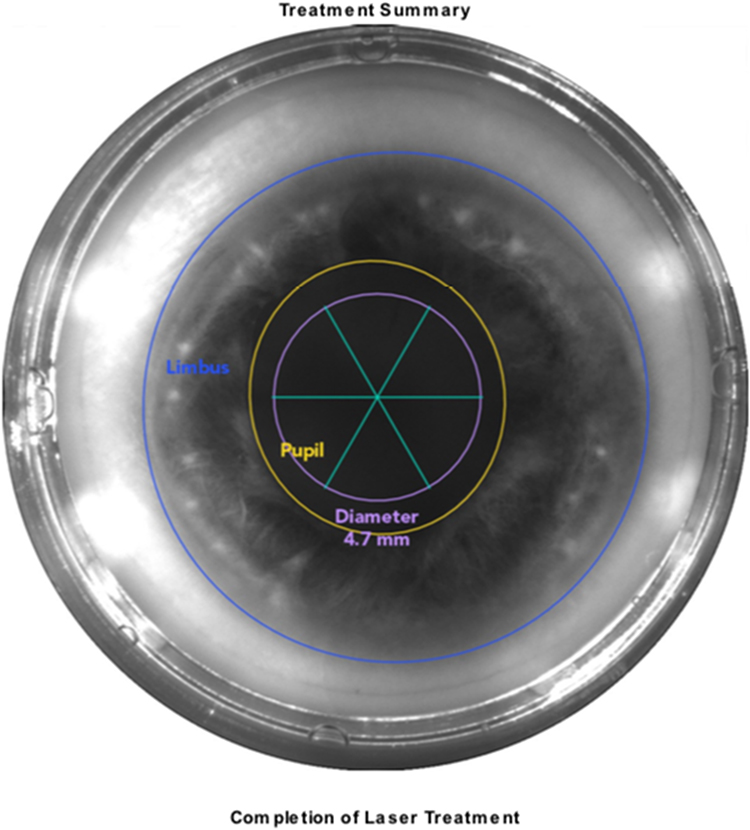 |
Figure 6 Capsulotomy and fragmentation alignment for the right eye. |
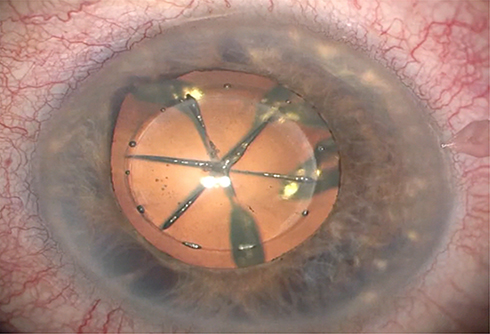 |
Figure 7 Fragmented nucleus, right eye. |
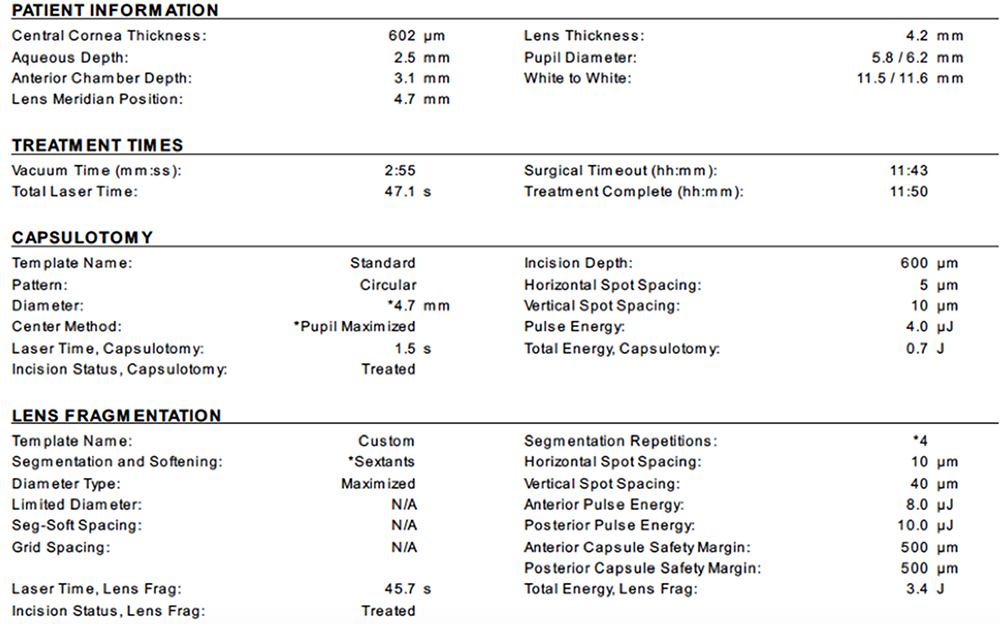 |
Figure 8 FLACS parameters for right eye. |
Results
At the first postoperative follow-up of the left eye, showed best corrected visual acuity (BCVA) of 0.3 on a logMAR chart using a refraction of – 0.75/–0.75 with an axis of 60°. The eye was quiet, with a formed anterior chamber, posterior chamber IOL in place, IOP 18 mmHg, and normal retinal view. For the right eye, the first postoperative follow-up showed BCVA of 0 on the logMAR chart with −0.5/–0.75 C and an axis of 55°. The eye was also quiet, with formed anterior chamber, posterior chamber, IOL in place, IOP 18 mmHg, and normal retinal view (Figures 9 and 10). The patient was followed up 1 year after the surgery. BCVA for the right eye was −0.75 SE with vision reaching 1, and for the left eye with −1.75 SE and axis of 75°, it was 0.6 (Figures 11 and 12).
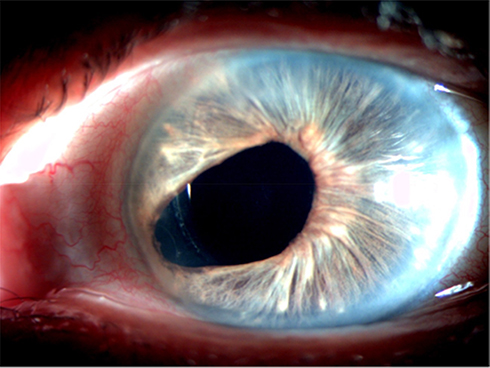 |
Figure 9 First follow-up, left eye. |
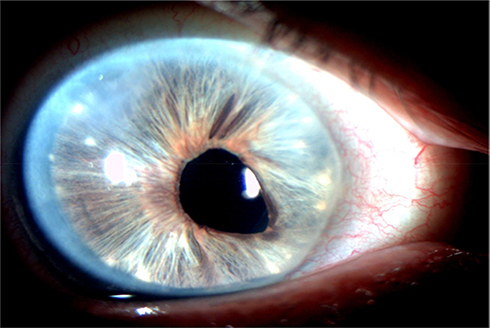 |
Figure 10 First follow-up, right eye. |
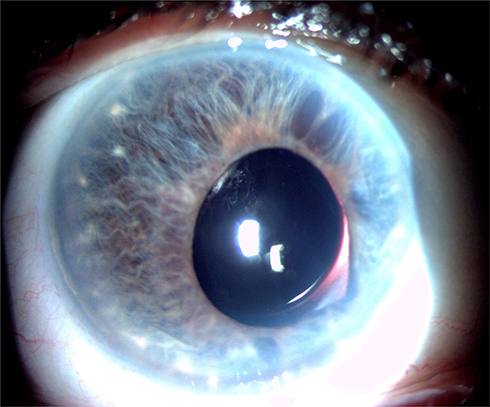 |
Figure 11 One year follow-up, left eye. |
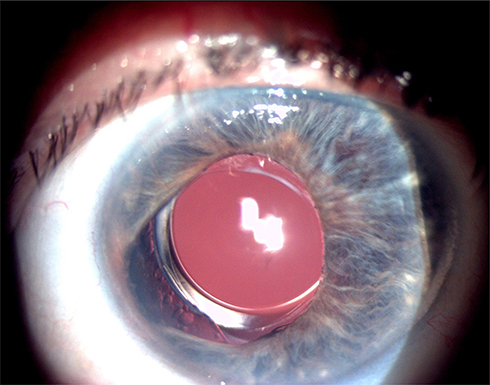 |
Figure 12 One year follow-up, right eye. |
Discussion
FLACS can provide better precision and predictability over manual phacoemulsification,8 especially in challenging cases with a shallow anterior chamber, subluxated cataracts, or an iris coloboma with a narrow pupil in a microphthalmic eye, as in our case.9 On the other hand, it requires more time and costs more. Also, it may induce miosis and a weaker capsulorhexis compared to manual capsulorhexis.10,11 The minimally invasive nature of FLACS induces less interruption to the internal structure of the eye, while minimizing surgeon-driven complications, giving more confidence to the surgeon and facilitating the learning curve for the cataract-extraction procedure.12 The clinical judgment of the surgeon and the ability to convert to manual capsulorhexis is a rather critical part in FLACS practice, especially in challenging cases, such as this case of iris coloboma. Further refinements in technology may be needed to give it distinct advantages over manual phacoemulsification and to make it the norm in cataract surgery.
Conclusion
Technology is a tool to help surgeons and offer better safety to patients. Manual modification of the settings of a machine according to the surgical judgment of the operator (if done carefully and with close supervision) can be an important tool to stretch the indications and use of such a technology as FLACS and overcome the restrictions of the machine’s original settings.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Eagle RC. Congenital, developmental, and degenerative disorders of the iris and ciliary body. In: Principles and Practice of Ophthalmology. Clinical Practice. Albert DM, Jacobiec FA, editors.
2. Beekhuis WH, Drost NH, van der Velden Samderubun EM. A new treatment for photophobia in posttraumatic aniridia: a case report. Cornea. 1998;17:338–341. doi:10.1097/00003226-199805000-00017
3. Palacz O, Lubiński W, Barnyk K. Implantation of posterior chamber lenses with trans-scleral fixation. Klin Oczna. 1999;101:433–436.
4. Kim JH, Kang MH, Kang SM, Song BJ. A modified iris repair technique and capsular tension ring insertion in a patient with coloboma with cataracts. Korean J Ophthalmol. 2006;20:246–249. doi:10.3341/kjo.2006.20.4.246
5. Migneco MK. Contact lens management of aniseikonia and photophobia induced by trauma. Eye Contact Lens. 2005;31:252–253. doi:10.1097/01.ICL.0000161704.09733.72
6. Cionni RJ, Karatza EC, Osher RH, Shah M. Surgical technique for congenital iris coloboma repair. J Cataract Refract Surg. 2006;32:1913–1916. doi:10.1016/j.jcrs.2006.08.017
7. Talamo JH, Gooding P, Angeley D, et al. Optical patient interface in femtosecond laser-assisted cataract surgery: contact corneal applanation versus liquid immersion. J Cataract Refract Surg. 2013;39:501–510. doi:10.1016/j.jcrs.2013.01.021
8. Ang RET, Quinto MMS, Cruz EM, Rivera MCR, Martinez GHA. Comparison of clinical outcomes between femtosecond laser-assisted versus conventional phacoemulsification. Eye Vis. 2018;5:8. doi:10.1186/s40662-018-0102-5
9. Vasavada VA, Vasavada S, Vasavada AR, Vasavada V, Srivastava S. Comparative evaluation of femtosecond laser-assisted cataract surgery and conventional phacoemulsification in eyes with a shallow anterior chamber. J Cataract Refract Surg. 2019;45(5):547–552. doi:10.1016/j.jcrs.2018.11.037
10. Quiñones A, Gleitsmann K, Freeman M, et al. Benefits and harms of femtosecond laser assisted cataract surgery: a systematic review [internet]. Washington (DC): Department of Veterans Affairs (US); 2013 Dec. EXECUTIVE SUMMARY. Available from: https://www.ncbi.nlm.nih.gov/books/NBK185095/.
11. Spalton D. Capsulorhexis strength with FLACS surgery. Invest Ophthalmol Vis Sci. 2016;57(6):2850. doi:10.1167/iovs.16-19629
12. Zhu Y, Chen X, Chen P, et al. Lens capsule-related complications of femtosecond laser-assisted capsulotomy versus manual capsulorhexis for white cataracts. J Cataract Refract Surg. 2019;45(3):337–342. doi:10.1016/j.jcrs.2018.10.037
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.