Back to Journals » Clinical Ophthalmology » Volume 19
Five-year Outcome of Aflibercept Administration with “Treat and Extend” for Neovascular Age-Related Macular Degeneration
Authors Wada I, Oshima Y ![]() , Fukuda Y
, Fukuda Y ![]() , Shiose S, Kano K, Ishikawa K, Nakao S, Kaizu Y, Hasegawa E, Kannan R, Ishibashi T, Sonoda KH
, Shiose S, Kano K, Ishikawa K, Nakao S, Kaizu Y, Hasegawa E, Kannan R, Ishibashi T, Sonoda KH
Received 14 November 2024
Accepted for publication 20 February 2025
Published 12 March 2025 Volume 2025:19 Pages 835—845
DOI https://doi.org/10.2147/OPTH.S501953
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Iori Wada,1,2 Yuji Oshima,3 Yosuke Fukuda,1 Satomi Shiose,1 Kumiko Kano,1 Keijiro Ishikawa,1 Shintaro Nakao,4 Yoshihiro Kaizu,1,5 Eiichi Hasegawa,1,2 Ram Kannan,6,7 Tatsuro Ishibashi,1 Koh-Hei Sonoda1
1Department of Ophthalmology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan; 2Department of Ophthalmology, National Hospital Organization, Kyushu Medical Center, Fukuoka, Japan; 3Section of Ophthalmology, Department of Medicine, Fukuoka Dental College, Fukuoka, Japan; 4Department of Ophthalmology, Juntendo University School of Medicine, Tokyo, Japan; 5Department of Ophthalmology, Saga University School of Medicine, Saga, Japan; 6Doheny Eye Institute, Pasadena, CA, 91103, USA; 7Stein Eye Institute, Geffen School of Medicine, University of California, Los Angeles, CA, USA
Correspondence: Yuji Oshima, Section of Ophthalmology, Department of Medicine, Fukuoka Dental College, Fukuoka, Japan, Tel +81-92-801-0411, Fax +81-92-801-0735, Email [email protected]
Purpose: This study aimed to evaluate the outcomes of aflibercept treatment using a treat-and-extend (TAE) regimen over up to 5 years in Japanese patients with neovascular age-related macular degeneration (nAMD).
Patients and Methods: This retrospective study included 126 consecutive treatment-naïve nAMD patients (126 eyes) who received at least three monthly intravitreal aflibercept (IVA) injections as a loading phase, followed by a treat-and-extend (TAE) regimen with follow-up for 5 years. Injection intervals were adjusted every 2 weeks and could be extended up to 16 weeks based on macular condition. Treatment was suspended if patients received 3 injections at 16-week intervals and the macula remained dry (defined as “monitoring”). Ophthalmic exams were conducted at each visit to assess disease activity.
Results: The mean logarithm of the minimum angle of resolution (logMAR) best corrected visual acuity (BCVA) at baseline was 0.42 ± 0.036. Following loading injections, the mean BCVA exhibited a significant improvement. Although it subsequently declined, it sustained the initial visual acuity. The average macular thickness (CMT) was significantly reduced and maintained throughout the follow-up period. The number of aflibercept injections decreased significantly from the second year and gradually decreased during the follow-up period. Intravitreal aflibercept (IVA) treatment could be discontinued in 36 (44%) cases during the follow-up period. However, 12 of these eyes (33%) experienced recurrence. Notably, significant recurrence was observed in patients who received a higher total number of aflibercept injections. Macular atrophy was significantly more likely to occur in cases with occult macular neovascularization (MNV) with subretinal hemorrhage than in cases with other forms of nAMD.
Conclusion: The long-term outcomes of IVA treatment utilizing TAE regimens for nAMD in real-world practice have demonstrated favorable results, including the maintenance of visual acuity and improvement in CMT over a 5-year period.
Keywords: long-term treatment, treatment regimen, macular atrophy
Introduction
Neovascular age-related macular degeneration (nAMD) leads to vision loss and irreversible blindness in elderly populations around the world.1,2 nAMD causes severe vision loss due to macular neovascularization (MNV) associated with retinal edema or hemorrhage. The main treatments for MNV and associated edema include laser ablation, photodynamic therapy (PDT) with verteporfin, and anti-vascular endothelial growth factor (VEGF) treatment.3,4 Currently, anti-VEGF treatment is the first choice for nAMD.
The MARINA and ANCHOR studies, the first large-scale clinical trials with anti-VEGF treatment, demonstrated that monthly ranibizumab injections were effective in improving visual acuity (VA) compared to PDT.5–7 The VIEW 1 and VIEW 2 studies with aflbercept also showed that fixed injection once every two months were effective in maintaining or improving VA. However, the SEVEN-UP STUDY demonstrated that switching to a “as needed” (pro re nata [PRN]) dosing regimen after monthly ranibizumab injections in the MARINA and ANCHOR studies resulted in eventual visual loss.8–12 Our group also reported that a reactive regimen, PRN, failed to maintain visual acuity over 5 years.13 In contrast, the treat and extend regimen (TAE) is a proactive approach in which the injection dosing interval is extended by 2 weeks if there is no recurrence of retinal fluid, resulting in better anatomical and functional stability at 12 months compared to PRN. Although the average number of injections is 1.4 higher, the number of clinical visits is reported to be lower.14 Previous reports have also demonstrated good long-term visual outcomes with TAE regimens using bevacizumab or ranibizumab for up to 8 years.15 Some long-term outcome studies in Japan have focused on nAMD patients treated with aflibercept in a TAE regimen. However, they have been limited to a follow-up period of up to 4 years.16–18 This study aims to investigate the real-world clinical outcomes of aflibercept treatment according to the TAE regimen for 5 years in Japanese patients with nAMD.
Long-term anti-VEGF treatment for nAMD is associated with atrophic macular changes, such as macular atrophy (MA), which can cause irreversibility visual loss.19–24 Previous large clinical trials have reported that MA developed in up to 41% of patients at 5 years and 98% at 7 years after the initiation of anti-VEGF treatment.8,25 In addition, various risk factors, including the size of the MNV and the presence of intraretinal fluid (IRF), retinal pigment epithelial detachment (PED), and subretinal hyperreflective material (SHRM) before anti-VEGF treatment, have been suggested as causes of MA.9,26–28 Therefore, this study also aims to elucidate the background factors contributing to MA development after long-term treatment.
Material and Methods
This study was a retrospective, observational, open-label effectiveness study conducted through the analysis of medical records from patients who received treatment at Kyushu University Hospital in Japan.
Patient Population
This retrospective study included 126 eyes of 126 patients with nAMD was followed up for a period of 5 years subsequent to their initial aflibercept injection, including dropout cases at Kyushu University Hospital from December 2012 to March 2019. There were 88 men and 38 women, averaging 74.2 ± 8.7 years of age.
Intravitreal Treatment
This retrospective study used the medical records of nAMD patients who underwent three-monthly intravitreal administration of aflibercept (IVA) (2 mg/0.05 mL) at Kyushu University Hospital between December 2012 and September 2014. Additional injections were administered based on the “TAE” regimen during each follow-up visit. Under our institution`s TAE regimen, if retinal fluid or hemorrhage was absent upon funduscopy or optical coherence tomography (OCT) images, the inter-visit interval was extended by two weeks. Conversely, if visual acuity were declined by the anatomical changes, the inter-visit interval was shortened by two weeks. The maximum inter-visit interval was set at 16 weeks. Patients received three injections at 16-week intervals, and if the macular remained dry, treatment was suspended, and patients were diligently monitored (referred to as “monitoring”). Patients who were transferred to “monitoring” were examined every 16 weeks, and if a recurrence was observed during “monitoring”, the interval between examinations was shortened by two weeks. Informed consent was obtained from all nAMD patients. This study was approved by the Institutional Review Board at Kyushu University Hospital, and all experiments were performed in accordance with the Declaration of Helsinki for research involving human subjects.
Ophthalmologic Examinations
A comprehensive ophthalmic examination was conducted during each follow-up visit, including assessments of best corrected visual acuity (BCVA), slit-lamp biomicroscopy, dilated funduscopy, fundus photography, and spectral-domain OCT. BCVA was measured using the Landolt Chart and expressed as the logarithm of minimal angle of resolution (logMAR). Central subfield macular thickness (CMT) was measured via OCT as the average thickness of the central 1-mm thickness map measurement area. Fluorescein angiography (FA) and indocyanine green (ICGA) were performed at baseline. The eyes were classified based on the change in the logMAR VA, with a change of 0.3 or more denoted as “improved”, and the opposite as “declined”.
Characteristics
This study evaluated the association between the following characteristics and nAMD: age, sex, nAMD classification (typical nAMD: type 1 or 2 MNV, polypoidal choroidal vasculopathy (PCV), and retinal angiomatous proliferation (RAP): type 3 MNV) at baseline, medical history (diabetes mellitus and hypertension), smoking history, pretreatment (as baseline) BCVA, pretreatment CMT, and pretreatment greatest linear dimension (GLD). Information on hypertension, diabetes, and smoking history was obtained using a questionnaire by trained doctors during the initial examination on the same day of nAMD detection.
Recurrence
Based on the presence or absence of retinal fluid requiring additional anti-VEGF injections after the shift to monitoring, patients were divided into two groups: “Recurrence” and “Non-Recurrence”. The criteria for persistent retinal fluid were OCT-determined thickening of more than 50 μm at each time point following the shift to monitoring. The associations between retreatment and baseline characteristics and the total number of anti-VEGF injections, were examined.
Macular Atrophy
This study also investigated the occurrence of macular atrophy (MA) five years after treatment using fundus examination, OCT images, and fundus autofluorescence (FAF) according to the methods of previous studies.10,29 The study analyzed the characteristics of neovascular patients with MA development. These characteristics were examined by age, sex, FA classification (predominantly, minimally classic, and occult) at baseline, medical history (diabetes mellitus and hypertension), smoking history, pre- and post-treatment VA, pretreatment CMT, pretreatment GLD, pretreatment MNV, presence of IRF, PED, SHRM, subretinal drusen, subretinal hemorrhage, MA in the fellow eye at baseline, and the total number of anti-VEGF injections. MNV size in the FA image, excluding the area of subretinal hemorrhage, was measured using ImageJ 1.42 K (Version 1.51, Rasband W.S., US National Institutes of Health, Bethesda, Maryland, USA, http://imagej.nih.gov/ij/, 1997–2015) prior to anti-VEGF treatment.
Statistical Methods
All statistical analyses were performed using commercial software package (JMP pro software, version 15.0; SAS, Inc, Cary, NC). Descriptive statistics included mean, standard deviation (SD), median, range, and percentages where appropriate. Correlations between any two of the following variables were analyzed using Dunnet test, Fisher`s exact test, ANOVA test, Chi square test, multiple logistic regression analysis, and t-test: sex, age, BCVA, anamnesis, life history, CMT, GLD, changes in the BCVA and OCT parameters, and drug history. All tests of associations were considered statistically significant if p < 0.05.
Results
Baseline Characteristics
All patients with treatment-naïve nAMD received treatment with the TAE regimen at Kyushu University Hospital between December 2012 and September 2014. These 126 eyes were included in this retrospective study. The baseline characteristics of the patients are shown in Table 1. The cohort consisted of 126 eyes classified as type 1 or 2 MNV (72 eyes), PCV (49 eyes), and type 3 MNV (5 eyes). The average age of the patients was 74.1 ± 8.7 years, BCVA (logMAR) was 0.42 ± 0.036, CMT was 326.9 ± 10.8 µm, and GLD was 4037.3 ± 188.5 µm. Twenty-three (18%) patients had diabetes, and 59 (47%) had hypertension. In addition, 58 (46%) patients had a smoking history. Among the baseline characteristics analyzed by nAMD subtype, only pretreatment BCVA showed a significant difference, with type 1 or 2 MNV exhibiting significantly poorer pretreatment BCVA than the other subtypes.
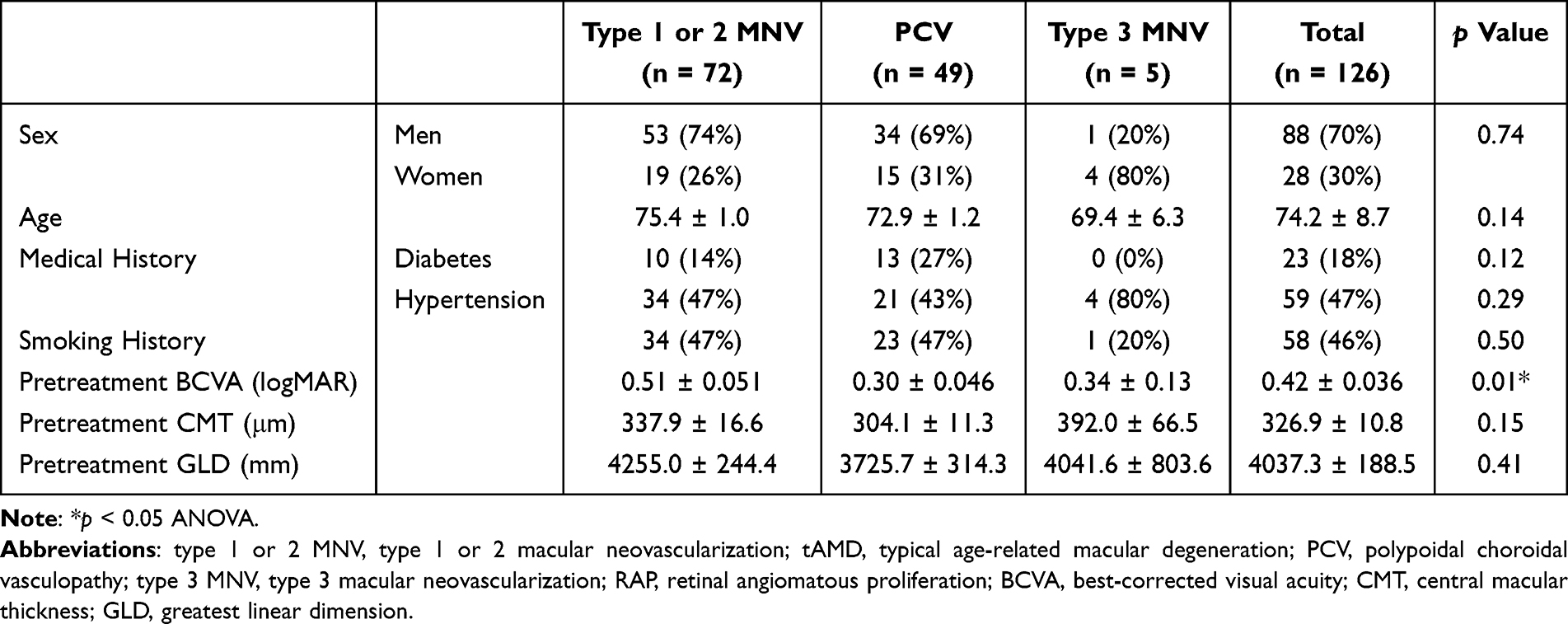 |
Table 1 Participant Characteristics at Baseline Before Treatment |
Visual Acuity Outcomes
Of the 126 patients included in the study, 63 patients were followed up for 5 years with treatment and monitoring (Supplemental Table 1). Although BCVA significantly improved in all cases of total AMD (including type 3 MNV), type 1 or 2 MNV, and PCV significantly improved until the first year after treatment, it gradually declined and returned to baseline levels (p < 0.05). The mean BCVA in all patients declined from 0.42 ± 0.036 logMAR at baseline to 0.36 ± 0.055 logMAR at 5 years without significance (Figure 1).
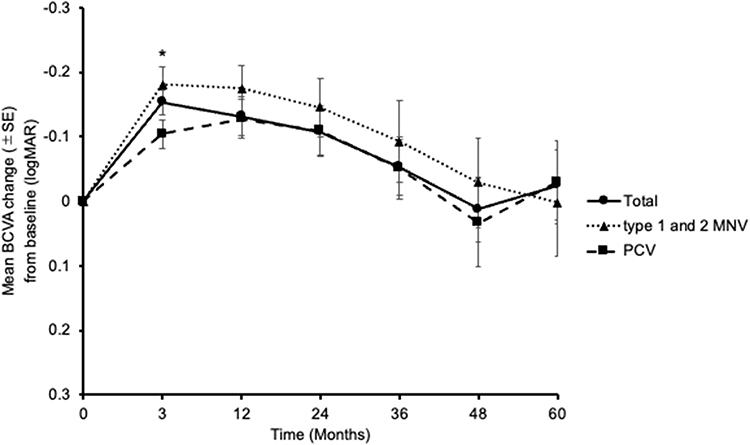 |
Figure 1 Graph showing the mean changes in best corrected visual acuity (BCVA) scores. Changes in BCVA were calculated for each patient, and the means are shown at various time points. The type of AMD included total AMD (Total), typical AMD (type 1 or 2 MNV), and PCV. All patients with AMD were observed and treated over a 5-year follow-up period. After loading injections for three months, the visual acuity in the total AMD, typical AMD, and PCV groups significantly improved, but it gradually declined by the end of year 5. *p < 0.05, Dunnett test. Abbreviations: AMD, age-related macular degeneration; PCV, polypoidal choroidal vasculopathy; PNV, pachychoroid neovasculopathy. |
When classifying the eyes based on the change in logMAR VA, 15 eyes (23.8%) showed improvement, 36 eyes (57.1%) maintained their BCVA, and 12 eyes (19.1%) experienced a decline in BCVA over the 5 -year period after the first aflibercept treatment with the TAE regiment (Figure 2). The 5-year BCVA change did not differ significantly among the three subtypes of nAMD (type 1 or 2 MNV: 0.0026 ± 0.083, PCV: −0.030 ± 0.065, type 3 MNV: 0.037 ± 0.088). These results suggest that aflibercept with the TAE regimen can maintain the initial visual acuity over a 5-year period after the start of treatment.
 |
Figure 2 Diagram showing distribution of changes in the best corrected visual acuity (BCVA) score. The diagram shows the distribution of visual acuity (VA) changes from previous time points in the total AMD (Total), typical AMD (type 1 or 2 MNV), PCV, and RAP (type 3 MNV) groups. The 5-year BCVA changes did not show significant differences between each type of AMD. Abbreviations: AMD, age-related macular degeneration; PCV, polypoidal choroidal vasculopathy; RAP, retinal angiomatous proliferation; PNV, pachychoroid neovasculopathy. |
Predictive Factors for Visual Acuity
The background characteristics were analyzed to identify predictive factors for visual acuity. The “Improve/Maintain” and “Decline” BCVA groups showed significant differences in pretreatment GLD in univariate analysis (p = 0.0097) (Table 2). Multivariable analysis identified pretreatment GLD as the only independent risk factor for better vision after 5 years of treatment (p = 0.0024) (Table 3). These findings indicate that patients with a smaller pretreatment GLD may achieve better final BCVA after 5 years of treatment.
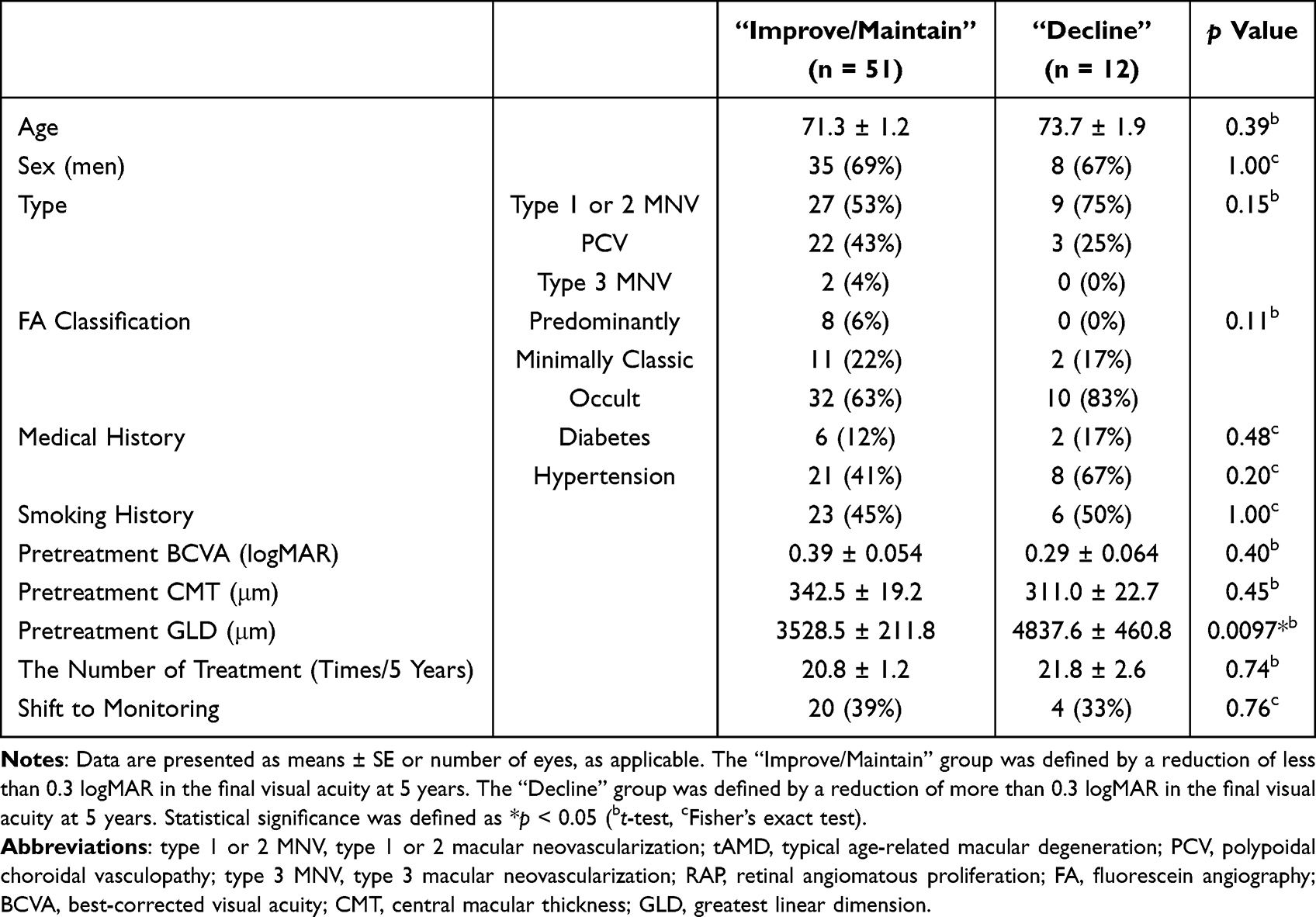 |
Table 2 Comparison Between “Improve/Maintain” and “Decline” Groups |
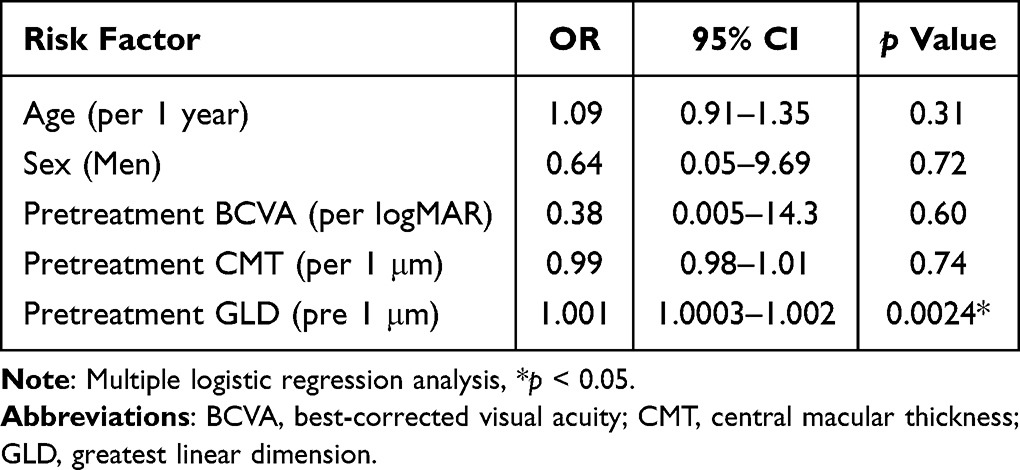 |
Table 3 Age- and Sex-Adjusted and Multivariable-Adjusted ORs of Risk Factors for Worsening Visual Acuity After 5 years |
Anatomical Outcomes
The mean CMT at baseline was 326.9 ± 10.8 μm and significantly decreased over the 5-year period following the first aflibercept treatment with the TAE regimen (235.9 ± 6.0 μm at 1 year, 224.3 ± 5.6 μm at 2 years, 225.8 ± 6.0 μm at 3 years, 232.5 ± 7.2 μm at 4 years, and 242.1 ± 18.5 μm at 5 years) (p < 0.0001) (Figure 3). These results indicate the long-term effectiveness of aflibercept with the TAE regimen in terms of anatomical outcomes.
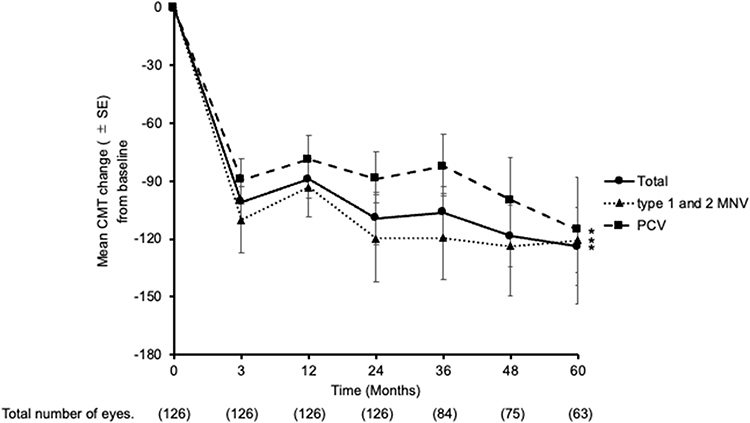 |
Figure 3 Graph showing the mean change in central macular thickness (CMT). Changes in CMT were examined for each patient by OCT, and the mean values for various time points are shown. The type of AMD included total AMD (Total), typical AMD (type 1 or 2 MNV), and PCV. One hundred twenty-seven patients with AMD were observed and treated over a 5-year follow-up period. *p < 0.05, paired t-test. Abbreviations: AMD, age-related macular degeneration; PCV, polypoidal choroidal vasculopathy; PNV, pachychoroid neovasculopathy. |
Number of Treatments
The average number of aflibercept doses in the first year was 7.4 ± 1.1. However, this number significantly decreased to 3.7 ± 1.8 after the second year and continued to decrease during the follow-up period. This trend was consistent across the different subtypes of nAMD. These findings demonstrate that aflibercept treatment with the TAE regimen can significantly reduce the number of anti-VEGF injections required for nAMD in the long term.
Disease Activity
Thirty-six of 126 eyes (29%) were shifted to follow-up without aflibercept treatment. Among these, 12 eyes (33%) (type 1 or 2 MNV: 7 eyes (44%), PCV: 5 eyes (25%)) experienced recurrence after shift to follow-up without aflibercept treatment. The mean time to re-treatment with aflibercept in cases of recurrence was 15.1 months. Analysis of recurrence by nAMD subtype did not reveal any significant differences. In addition, the background characteristics that predispose to recurrence were examined. Univariate analysis showed a significant difference only in the total number of aflibercept treatments over 5 years between the non-recurrence and recurrence groups after transitioning to follow-up without aflibercept treatment (p = 0.0005) (Table 4). However, the number of treatments was considered over the entire 5-year period, and the relapse group includes the number of treatments in which treatment was resumed after relapse, so it is thought that this is the result. These results suggest that some cases may be refractory to treatment with anti-VEGF therapy.
 |
Table 4 Comparison Between “Recurrence” and “Non-Recurrence” Groups |
Analysis for Macular Atrophy
The occurrence of MA was assessed in 53 of the 126 patients 5 years after treatment using fundus examination, OCT images, and FAF. The presence or absence of MA was assessed by three retinal experts based on fundus photography and OCT findings. Only when the three experts agreed was it determined to be MA and used in subsequent examinations. Of the 10 eyes who were followed up for 5 years, those with insufficient imaging data were excluded from this study. MA was observed in 40 images (75%) after the 5-year treatment period. MA was significantly more likely to occur in cases of minimally classic MNV compared to other nAMD subtypes (p = 0.0117), as well as in cases with worse pretreatment BCVA (p = 0.009), the presence of SHRM (p = 0.03), subretinal hemorrhage (p = 0.01), and a smaller number of total injections (p = 0.04) in the univariate analysis (Table 5). The same was examined for FA classification, but no significant differences were found. Multivariable analysis identified the presence of subretinal hemorrhage as the only independent risk factor for MA development after 5 years of treatment (Table 6). These finding emphasize the need for caution regarding the occurrence of MA after long-term treatment in patients with subretinal hemorrhage at baseline.
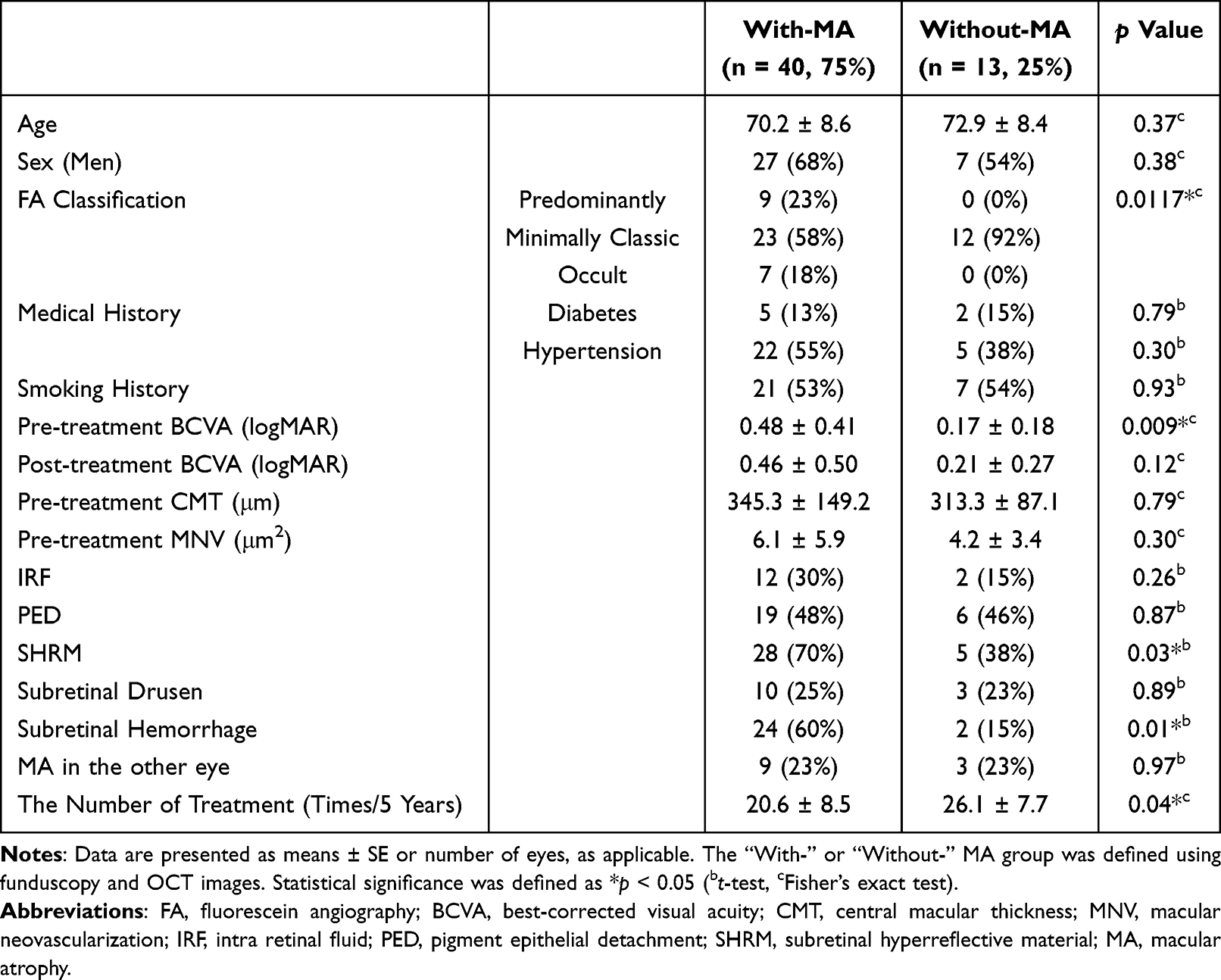 |
Table 5 Comparison Between “With-” and “Without-” Macular Atrophy Groups |
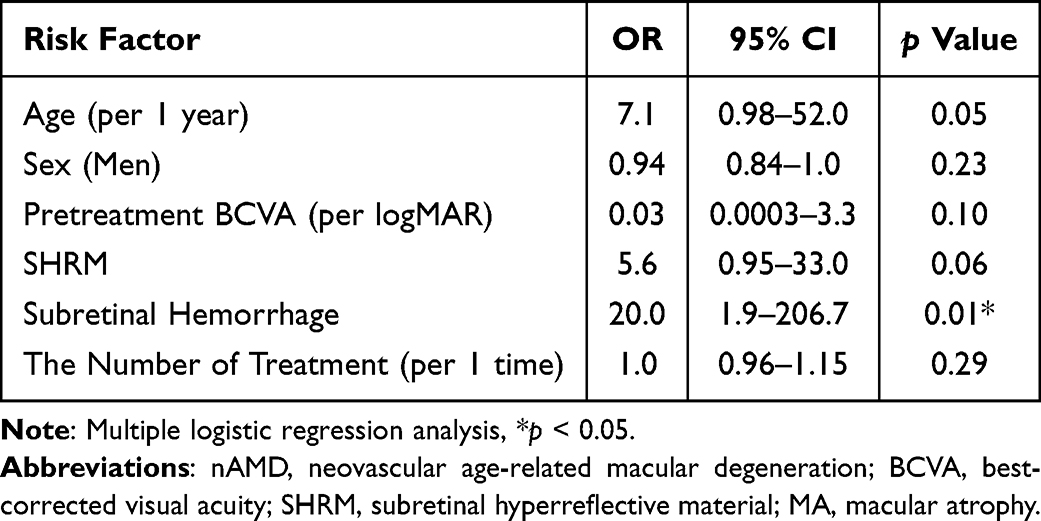 |
Table 6 Age- and Sex-Adjusted and Multivariable-Adjusted ORs of Risk Factors for MA in Eyes with nAMD |
Discussion
This retrospective study demonstrates the long-term efficacy of IVA treatment with the TAE regimen for nAMD in Japanese patients, preserving baseline visual acuity. Our previous study with ranibizumab using the PRN regimen also showed initial improvement in visual acuity by the end of the first year, but a gradual decline below baseline levels at 5 years, irrespective of nAMD subtype13 Comparisons with major trials are challenging due to differences in baseline characteristics, visual acuity measurements, and retreatment criteria. Tsunekawa et al reported a 4-year outcome of aflibercept treatment for nAMD in Japanese patients using the TAE regimen, with 6.7% of eyes experiencing a decline in visual acuity by more than 0.3 logMAR.18 In our study, 10 out of 42 eyes (23.8%) demonstrated a visual acuity decline of 0.3 logMAR or greater. This may be attributed to an increase in the number of patients with worse visual acuity over time, as those with unchanged visual acuity dropped out, resulting in a relatively higher proportion of patients with worse visual acuity.
Various factors have been considered to explain vision loss, including AMD subtype, number of injections, residual exudate, MA and fibrosis.30,31 In this study, a multivariate analysis was conducted to identify independent risk factors for post-treatment visual acuity in this study. Comparing the groups with visual acuity improvement and stable/worsening, only baseline GLD emerged as an independent risk factor for visual acuity after 5 years of treatment. In other words, these findings suggest that a smaller GLD at baseline is crucial for maintaining good visual acuity after 5 years of treatment.
In our study, 36 eyes (29%) successfully transitioned to follow-up visits without anti-VEGF treatment over 5 years, with recurrence observed in 12 (33%) of these eyes. These results are similar to previous report.32 Univariate analysis revealed a significantly higher frequency of aflibercept administration in the recurrence group. One possible cause of recurrence may be the elongation of the MNV. In a previous study using an AMD mouse model, we demonstrated regression of vascular endothelial cells in the MNV after IVA, whereas the vascular sleeve, which acts as a scaffold for new blood vessels, remained intact.33 This residual sleeve could contribute to treatment resistance to aflibercept administration and may require new treatment strategies upon on recurrence, such as additional PDT known as rescue-PDT, as we have previously reported.34
Furthermore, 40 eyes (75%) in our study developed MA over the 5-year period, a rate higher than that reported in previous studies using the TAE regimen.35,36 This MA development could be attributed to the lower average number of doses per year in our study compared to previous reports. On the other hand, opposing views exist. Martin et al using 2-year data from the CATT study, reported a higher risk of developing MA in eyes treated monthly.9 Further studies are needed to elucidate the impact of anti-VEGF therapy on the retina and retinal pigment epithelium (RPE) cells. Subretinal hemorrhage not only causes direct damage to RPE cells and photoreceptor due to iron content but also hamper the diffusion of bioactive substances between the retina and RPE cells and induces mechanical damage through fibrin contraction during the repair process.37–41
The retrospective nature of this study has some limitations. During the 5-years study period, 48.8% of the patients dropped out, and anatomic changes were evaluated only through funduscopy and OCT images. Further evaluation using FAF or OCT angiography is necessary. Safety was not the primary focus of this study, as there were no untreated patients, patients exclusively treated with other companies’ products, or comparison groups for different aflibercept regiments. Nonetheless, this study provides valuable real-world long-term outcome data on visual acuity and anatomic findings in Japanese nAMD patients.
In conclusion, aflibercept monotherapy using the TAE regimen-maintained baseline visual acuity and reduced CMT for 5 years in Japanese patients with nAMD. A smaller GLD was independently associated with better visual acuity.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 helsinki Declaration and its later amendments or comparable ethical standards.
Consent to Participate
Informed consent was obtained from all participants included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
JSPS KAKENHI Grant (#Kiban C 21K09677 [to Y.O.]). The organization had no role in the design or conduct of this research.
Disclosure
K.S. has received research grants from Santen Pharmaceutical Co., Ltd. S.N. reports personal fees from Bayer, Boehringer Ingelheim, Chugai Pharmaceutical, HOYA, Kowa, Machida, Mitsubishi Tanabe, Nipro, Novartis, Novo Nordisk Pharma, Santen, Senju, Wakamoto, and Riverfield, outside the submitted work. All other authors have no conflicts of interest to declare for this study.
References
1. Gheorghe A, Mahdi L, Musat O. Age-Related Macular Degeneration. Rom J Ophthalmol. 2015;59(2):74–77.
2. Francis PJ, Klein ML. Update on the role of genetics in the onset of age-related macular degeneration. Clin Ophthalmol. 2011;5:1127–1133. doi:10.2147/OPTH.S11627
3. Macular Photocoagulation Study Group. Laser photocoagulation of subfoveal neovascular lesions in age-related macular degeneration. Results of a randomized clinical trial. Arch Ophthalmol. 1991;109(9):1220–1231. doi:10.1001/archopht.1991.01080090044025
4. Treatment of age-related macular degeneration with photodynamic therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: one-year results of 2 randomized clinical trials--TAP report. Arch Ophthalmol. 1999;117(10):1329–1345.
5. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
6. Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1432–1444. doi:10.1056/NEJMoa062655
7. Singer MA, Awh CC, Sadda S, et al. HORIZON: an open-label extension trial of ranibizumab for choroidal neovascularization secondary to age-related macular degeneration. Ophthalmology. 2012;119(6):1175–1183. doi:10.1016/j.ophtha.2011.12.016
8. Rofagha S, Bhisitkul RB, Boyer DS, et al. Seven-year outcomes in ranibizumab-treated patients in ANCHOR, MARINA, and HORIZON: a multicenter cohort study (SEVEN-UP). Ophthalmology. 2013;120(11):2292–2299. doi:10.1016/j.ophtha.2013.03.046
9. Comparison of Age-related Macular Degeneration Treatments Trials Research G, Martin DF, Maguire MG, Fine SL, et al. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. 2012;119(7):1388–1398. doi:10.1016/j.ophtha.2012.03.053.
10. Comparison of Age-related Macular Degeneration Treatments Trials Research G, Maguire MG, Martin DF, Ying G-S, et al. Five-Year Outcomes with Anti-Vascular Endothelial Growth Factor Treatment of Neovascular Age-Related Macular Degeneration: the Comparison of Age-Related Macular Degeneration Treatments Trials. Ophthalmology. 2016;123(8):1751–1761. doi:10.1016/j.ophtha.2016.03.045.
11. Boulanger-Scemama E, Sayag D, Ha Chau Tran T, et al. Ranibizumab and exudative age-related macular degeneration: 5-year multicentric functional and anatomical results in real-life practice. J Fr Ophtalmol. 2016;39(8):668–674. doi:10.1016/j.jfo.2016.06.001
12. Heimes B, Lommatzsch A, Zeimer M, et al. Long-term visual course after anti-VEGF therapy for exudative AMD in clinical practice evaluation of the German reinjection scheme. Graefes Arch Clin Exp Ophthalmol. 2011;249(5):639–644. doi:10.1007/s00417-010-1524-5
13. Wada I, Oshima Y, Shiose S, et al. Five-year treatment outcomes following intravitreal ranibizumab injections for neovascular age-related macular degeneration in Japanese patients. Graefes Arch Clin Exp Ophthalmol. 2019;257(7):1411–1418. doi:10.1007/s00417-019-04361-8
14. Okada M, Kandasamy R, Chong EW, et al. The Treat-and-Extend Injection Regimen Versus Alternate Dosing Strategies in Age-related Macular Degeneration: a Systematic Review and Meta-analysis. Am J Ophthalmol. 2018;192:184–197. doi:10.1016/j.ajo.2018.05.026
15. Jaki Mekjavic P, Zaletel Benda P. Outcome of 5-Year Treatment of Neovascular Age-Related Macular Degeneration With Intravitreal Anti-VEGF Using ”Treat and Extend. Regimen Front Med. 2018;5:125.
16. Sakamoto S, Takahashi H, Inoue Y, et al. Intravitreal aflibercept for exudative age-related macular degeneration with good visual acuity: 2-year results of a prospective study. Clin Ophthalmol. 2018;12:1137–1147. doi:10.2147/OPTH.S160961
17. Itagaki K, Sekiryu T, Kasai A, et al. Three-year outcome of aflibercept treatment for Japanese patients with neovascular age-related macular degeneration. BMC Ophthalmol. 2020;20(1):276. doi:10.1186/s12886-020-01542-6
18. Tsunekawa Y, Kataoka K, Asai K, et al. Four-year outcome of aflibercept administration using a treat-and-extend regimen in eyes with recurrent neovascular age-related macular degeneration. Jpn J Ophthalmol. 2021;65(1):69–76. doi:10.1007/s10384-020-00783-8
19. Maguire P, Vine AK. Geographic atrophy of the retinal pigment epithelium. Am J Ophthalmol. 1986;102(5):621–625. doi:10.1016/0002-9394(86)90535-0
20. Holz FG, Wolfensberger TJ, Piguet B, et al. Bilateral macular drusen in age-related macular degeneration. Prognosis and risk factors. Ophthalmology. 1994;101(9):1522–1528. doi:10.1016/S0161-6420(94)31139-0
21. Sunness JS, Gonzalez-Baron J, Applegate CA, et al. Enlargement of atrophy and visual acuity loss in the geographic atrophy form of age-related macular degeneration. Ophthalmology. 1999;106(9):1768–1779. doi:10.1016/S0161-6420(99)90340-8
22. Grunwald JE, Pistilli M, Ying GS, et al. Growth of geographic atrophy in the comparison of age-related macular degeneration treatments trials. Ophthalmology. 2015;122(4):809–816. doi:10.1016/j.ophtha.2014.11.007
23. Grunwald JE, Pistilli M, Daniel E, et al. Incidence and Growth of Geographic Atrophy during 5 Years of Comparison of Age-Related Macular Degeneration Treatments Trials. Ophthalmology. 2017;124(1):97–104. doi:10.1016/j.ophtha.2016.09.012
24. Holz FG, Strauss EC, Schmitz-Valckenberg S, van Lookeren Campagne M. Geographic atrophy: clinical features and potential therapeutic approaches. Ophthalmology. 2014;121(5):1079–1091. doi:10.1016/j.ophtha.2013.11.023
25. Sharma S, Toth CA, Daniel E, et al. Macular Morphology and Visual Acuity in the Second Year of the Comparison of Age-Related Macular Degeneration Treatments Trials. Ophthalmology. 2016;123(4):865–875. doi:10.1016/j.ophtha.2015.12.002
26. Busbee BG, Ho AC, Brown DM, et al. Twelve-month efficacy and safety of 0.5 mg or 2.0 mg ranibizumab in patients with subfoveal neovascular age-related macular degeneration. Ophthalmology. 2013;120(5):1046–1056. doi:10.1016/j.ophtha.2012.10.014
27. Ho AC, Busbee BG, Regillo CD, et al. Twenty-four-month efficacy and safety of 0.5 mg or 2.0 mg ranibizumab in patients with subfoveal neovascular age-related macular degeneration. Ophthalmology. 2014;121(11):2181–2192. doi:10.1016/j.ophtha.2014.05.009
28. Gillies MC, Hunyor AP, Arnold JJ, et al. Macular Atrophy in Neovascular Age-Related Macular Degeneration: a Randomized Clinical Trial Comparing Ranibizumab and Aflibercept (RIVAL Study). Ophthalmology. 2020;127(2):198–210. doi:10.1016/j.ophtha.2019.08.023
29. Takahashi A, Ooto S, Yamashiro K, et al. Photoreceptor Damage and Reduction of Retinal Sensitivity Surrounding Geographic Atrophy in Age-Related Macular Degeneration. Am J Ophthalmol. 2016;168:260–268. doi:10.1016/j.ajo.2016.06.006
30. Takahashi Y, Koizumi H, Hasegawa T, et al. Comparison of subfoveal choroidal structures in typical neovascular age-related macular degeneration and polypoidal choroidal vasculopathy. Jpn J Ophthalmol. 2018;62(5):576–583. doi:10.1007/s10384-018-0615-4
31. Ogasawara M, Koizumi H, Yamamoto A, et al. Prognostic factors after aflibercept therapy for typical age-related macular degeneration and polypoidal choroidal vasculopathy. Jpn J Ophthalmol. 2018;62(5):584–591. doi:10.1007/s10384-018-0605-6
32. Adrean SD, Chaili S, Grant S, Pirouz A. Recurrence Rate of Choroidal Neovascularization in Neovascular Age-Related Macular Degeneration Managed with a Treat-Extend-Stop Protocol. Ophthalmol Retina. 2018;2(3):225–230. doi:10.1016/j.oret.2017.07.009
33. Wada I, Nakao S, Fukuda Y, et al. Persistence of vascular empty sleeves in choroidal neovascularization after VEGF therapy in both animal models and humans. Graefes Arch Clin Exp Ophthalmol. 2023;261:2189–2197.
34. Wada I, Shiose S, Ishikawa K, et al. One-year efficacy of ”rescue photodynamic therapy” for patients with typical age-related macular degeneration, polypoidal choroidal vasculopathy, and pachychoroid neovasculopathy refractory to anti-vascular endothelial growth factor therapy. Graefes Arch Clin Exp Ophthalmol. 2022;260(6):2029–2036. doi:10.1007/s00417-022-05553-5
35. Abdelfattah NS, Zhang H, Boyer DS, Sadda SR. Progression of Macular Atrophy in Patients with Neovascular Age-Related Macular Degeneration Undergoing Antivascular Endothelial Growth Factor Therapy. Retina. 2016;36(10):1843–1850. doi:10.1097/IAE.0000000000001059
36. Spooner KL, Fraser-Bell S, Cozzi M, et al. Macular Atrophy Incidence and Progression in Eyes with Neovascular Age-Related Macular Degeneration Treated with Vascular Endothelial Growth Factor Inhibitors Using a Treat-and-Extend or a Pro Re Nata Regimen: four-Year Results of the MANEX Study. Ophthalmology. 2020;127(12):1663–1673. doi:10.1016/j.ophtha.2020.06.019
37. Lewis H, Resnick SC, Flannery JG, Straatsma BR. Tissue plasminogen activator treatment of experimental subretinal hemorrhage. Am J Ophthalmol. 1991;111(2):197–204. doi:10.1016/S0002-9394(14)72259-7
38. Toth CA, Morse LS, Hjelmeland LM, Landers III MB. Fibrin directs early retinal damage after experimental subretinal hemorrhage. Arch Ophthalmol. 1991;109(5):723–729. doi:10.1001/archopht.1991.01080050139046
39. Avery RL, Fekrat S, Hawkins BS, Bressler NM. Natural history of subfoveal subretinal hemorrhage in age-related macular degeneration. Retina. 1996;16(3):183–189. doi:10.1097/00006982-199616030-00001
40. Sawa M, Ober MD, Freund KB, Spaide RF. Fundus autofluorescence in patients with pseudoxanthoma elasticum. Ophthalmology. 2006;113(5):814–20e2. doi:10.1016/j.ophtha.2006.01.037
41. Notomi S, Hisatomi T, Murakami Y, et al. Dynamic increase in extracellular ATP accelerates photoreceptor cell apoptosis via ligation of P2RX7 in subretinal hemorrhage. PLoS One. 2013;8(1):e53338. doi:10.1371/journal.pone.0053338
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.