Back to Journals » International Journal of Women's Health » Volume 18
First-Trimester Glycated Hemoglobin (HbA1c) and Maternal Characteristics in the Prediction of Gestational Diabetes Mellitus (GDM): A Prospective Cohort Study
Authors Inthavong S ![]() , Jatavan P, Tongsong T
, Jatavan P, Tongsong T ![]()
Received 15 April 2026
Accepted for publication 28 May 2026
Published 8 June 2026 Volume 2026:18 617034
DOI https://doi.org/10.2147/IJWH.S617034
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Sathaphone Inthavong,1 Phudit Jatavan,1,2 Theera Tongsong1,2
1Department of Obstetrics and Gynecology, Chiang Mai University, Chiang Mai, Thailand; 2Fetal Center, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
Correspondence: Phudit Jatavan, Department of Obstetrics and Gynecology, Faculty of Medicine, Chiang Mai University, Chiang Mai, 50200, Thailand, Email [email protected]
Objective: To assess the predictive performance of first-trimester HbA1c, both as an individual marker and in combination with clinical risk factors, for subsequent development of GDM.
Methods: A prospective cohort study was conducted at a single tertiary center in Thailand. Singleton pregnant women between 10 and 14 weeks of gestation were consecutively recruited. Women with pregestational diabetes mellitus were excluded. Baseline clinical characteristics were systematically recorded, and blood samples were obtained for HbA1c measurement. GDM was diagnosed at 24– 28 weeks of gestation using the standard two-step approach, 100-g OGTT with NDDG thresholds. The predictive performance of HbA1c alone and in combination with clinical risk factors was evaluated using ROC curve analysis.
Results: Among 302 participants, 98 (32.5%) were diagnosed with GDM. Women who developed GDM were of more advanced maternal age and had higher pre-pregnancy BMI and body weight. They also more frequently reported a family history of diabetes mellitus and dyslipidemia. First-trimester HbA1c levels were significantly elevated in the GDM group. HbA1c alone demonstrated modest discriminatory performance (AUC=0.675). Incorporation of HbA1c into a multivariable model with maternal age and BMI improved predictive accuracy (AUC=0.726). At an probability cutoff 0.245, the combined model achieved a sensitivity of 80.6% and a specificity of 51.0%.
Conclusion: First-trimester HbA1c levels are significantly elevated among women who subsequently develop GDM. Although HbA1c alone provides modest discriminatory capacity, integrating HbA1c with maternal age and pre-pregnancy BMI substantially enhances predictive performance. These findings support the application of this straightforward combined model for early pregnancy risk stratification.
Keywords: gestational diabetes mellitus, glycated hemoglobin, HbA1c, prediction
Introduction
Gestational diabetes mellitus (GDM), defined as glucose intolerance first recognized during pregnancy,1 represents one of the most prevalent obstetric complications. GDM is associated with a spectrum of adverse maternal and perinatal outcomes, including fetal macrosomia, fetal distress, preterm birth, preeclampsia, and an increased long-term risk of type 2 diabetes mellitus and metabolic disorders in both the mother and offspring. Accordingly, early identification and timely intervention are critical to optimizing pregnancy outcomes. Although universal or risk-based screening and diagnosis are conventionally based on an oral glucose tolerance test (OGTT) performed at 24–28 weeks’ gestation,2 increasing emphasis has been placed on earlier risk stratification to enable closer surveillance and facilitate prompt diagnosis and treatment.3 In this context, numerous studies have explored first-trimester risk assessment strategies to identify women at high risk for GDM who may benefit from targeted screening at 24–28 weeks of gestation, which remains the standard approach in routine clinical practice in many settings. However, the predictive performance of existing models based solely on maternal clinical characteristics remains suboptimal, highlighting the need for more accurate and reliable predictive markers.
Glycated hemoglobin (HbA1c) has emerged as a potential biomarker for the early prediction of GDM. As an indicator of mean glycemic exposure over the preceding 2–3 months, HbA1c offers several practical advantages, including the absence of a fasting requirement, high sample stability, and widespread availability in routine clinical practice.4 Although an HbA1c threshold ≥ 6.5% is diagnostic of overt diabetes mellitus, the clinical utility of lower first-trimester cutoffs for predicting subsequent GDM remains controversial.5–7 This uncertainty is partly attributable to physiological alterations in red blood cell turnover during pregnancy, which may influence HbA1c levels. Nevertheless, accumulating evidence indicates that women who subsequently develop GDM demonstrate significantly higher HbA1c levels as early as 8–13 weeks of gestation compared with those who maintain normal glucose tolerance. Reported predictive performance, however, has varied considerably across studies. Such heterogeneity may reflect differences in gestational age at testing, study design, and population characteristics, particularly ethnicity, which substantially influences GDM prevalence and metabolic expression. For instance, the prevalence of GDM in the Thai population has been reported to be as high as 33%,8 markedly exceeding the 8–10% observed in Caucasian populations.1 Moreover, relatively few studies have evaluated the predictive performance of first-trimester HbA1c in combination with maternal clinical characteristics.9 Some investigations have included women assessed before 10 weeks of gestation, a period during which physiological insulin resistance is not yet pronounced, potentially limiting predictive sensitivity. We therefore hypothesized that HbA1c measured at 10–14 weeks of gestation could provide a clinically useful approach for stratifying women into high- and low-risk groups for development of GDM. The objective of this study was to develop the predictive performance of first-trimester HbA1c, both as an independent biomarker and in combination with clinical risk factors, for the prediction of GDM later in pregnancy.
Materials and Methods
This prospective cohort study was conducted at the antenatal care clinic of Chiang Mai University Hospital, a tertiary referral center, between February and December 2025. The study protocol was approved by the Institutional Review Board, Faculty of Medicine, Chiang Mai University (Research Ethics Committee Panel 5; study code OBG-2567-0726). All eligible women were invited to participate and provided written informed consent prior to enrollment after receiving comprehensive information regarding the study objectives and procedures.
Participants were consecutively recruited from the antenatal clinic. The inclusion criteria were as follows: (1) singleton pregnancy confirmed by first-trimester ultrasonography; (2) maternal age 20–45 years; 3) gestational age between 10 and 14 weeks, determined by a reliable last menstrual period consistent with first-trimester crown-rump length measurement; and (4) willingness to comply with all study procedures, including blood sampling, standard two-step GDM screening, and scheduled follow-up assessments.
Exclusion criteria comprised: (1) pre-existing diabetes mellitus diagnosed prior to pregnancy; (2) HbA1c ≥ 6.5% at enrollment; (3) current use of medications known to influence glucose metabolism; and (4) loss to follow-up or failure to complete the 24–28-week GDM screening protocol.
At the enrollment visit, trained research personnel conducted standardized interviews using structured case report forms to obtain detailed demographic, obstetric, and medical history data. Collected variables included maternal age, pre-pregnancy weight and body mass index (BMI), and parity. Information regarding a first-degree family history of diabetes mellitus (DM) and history of GDM was also documented. Additionally, underlying medical disorders, including chronic hypertension and dyslipidemia, were recorded.
Laboratory Analysis
Venous blood samples for HbA1c measurement were collected from all participants at 10–14 weeks of gestation. HbA1c concentrations were determined quantitatively using the Tina-quant® Hemoglobin A1cDx Gen.3 assay on a Cobas c 503 analyzer. This test employs a Turbidimetric Inhibition Immunoassay (TINIA) applied to hemolyzed whole blood. The assay is standardized according to the Internal Federation of Clinical Chemistry (IFCC) and is transferable to the National Glycated Hemoglobin Standard Program (NGSP) units. HbA1c values were expressed as percentage (%) according to NGSP standards using the conversion equation: NGSP % = 0.915 × IFCC (mmol/mol) ± 2.15.10,11
Between 24 and 28 weeks of gestation, all participants underwent standard two-step screening for GDM. Initially, a 50-g oral glucose challenge test was performed irrespective of fasting status. A 1-hour plasma glucose level <140 mg/dL was considered normal, whereas a value ≥140 mg/dL prompted a diagnostic 100-g oral glucose tolerance test (OGTT) within one week. The OGTT, involving measuring plasma glucose levels at fasting and at 1, 2, and 3 hours after glucose ingestion. The corresponding diagnostic thresholds were ≥105 mg/dL (fasting), ≥190 mg/dL (1 hour), ≥165 mg/dL (2 hours), and ≥145 mg/dL (3 hours), following the National Diabetic Data Group criteria. GDM was diagnosed when at least two values met or exceeded these cut-off levels. If only one value was abnormal, the 100-g OGTT was repeated one month later using the same diagnostic criteria. Based on these results, participants were categorized into either the GDM or non-GDM group. Additional screening beyond 28 weeks of gestation was undertaken when clinically indicated, such as in cases of persistent glucosuria on dipstick testing or excessive gestational weight gain relative to pre-pregnancy BMI. Screening and diagnostic decisions were made by attending physicians in the antenatal clinic. Women diagnosed with GDM at any time during pregnancy were assigned to the GDM group. All participants were subsequently followed longitudinally by the research team.
To adequately address the primary outcome, this study required a minimum sample size of 47 cases in the affected group and 118 cases in the unaffected group to detect an AUC of 0.64, compared to an AUC of 0.50 under the null hypothesis, using a one-sided test with 80% power at a 95% confidence level, assuming an affected-to-unaffected case ratio of 30:70.
Statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS), version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were presented as mean ± standard deviation (SD) or median with interquartile range (IQR), as appropriate according to data distribution. Comparisons of baseline characteristics between the GDM and non-GDM groups were performed using the Student’s t-test or Mann–Whitney U-test for continuous variables, as appropriate, and the chi-square test for categorical variables. The discriminatory ability of individual risk factors and the combined model was assessed using binary logistic regression and the area under the receiver operating characteristic curve (AUC). For the development of a novel predictive model for GDM, HbA1c and relevant clinical risk factors were initially entered into a multivariable logistic regression model, and multicollinearity was assessed using variance inflation factor diagnostics. Backward elimination, guided by the principle of parsimony, was subsequently applied to derive the most concise model by sequentially removing the variable with the highest p-value at each step, provided that model performance was not adversely affected. Model performance was compared using paired-sample receiver operating characteristic (ROC) curve analysis based on the method of DeLong et al, together with log-likelihood evaluation. Internal validation was performed using bootstrap resampling with 500 replications, and calibration plots were constructed to assess agreement between predicted probabilities and observed outcomes. Diagnostic performance was further evaluated by calculating sensitivity, specificity, positive predictive value, and negative predictive value, using the probability cut-off based on fixed sensitivity of 80%. A two-sided p-value < 0.05 was considered statistically significant.
Results
During the study period, 324 women attended the antenatal care clinic and were initially enrolled, as illustrated in Figure 1. Of these, 302 met the inclusion criteria and were included in the final analysis. Ninety-eight participants (32.5%) were diagnosed with GDM at 24–28 weeks of gestation. Baseline characteristics differed significantly between women who developed GDM and those who did not (Table 1). In particular, pre-pregnancy weight and pre-pregnancy BMI were significantly higher in the GDM group. Maternal age was also significantly greater among women who developed GDM (p < 0.001). Additionally, a family history of DM and dyslipidemia were more frequently observed in the GDM group.
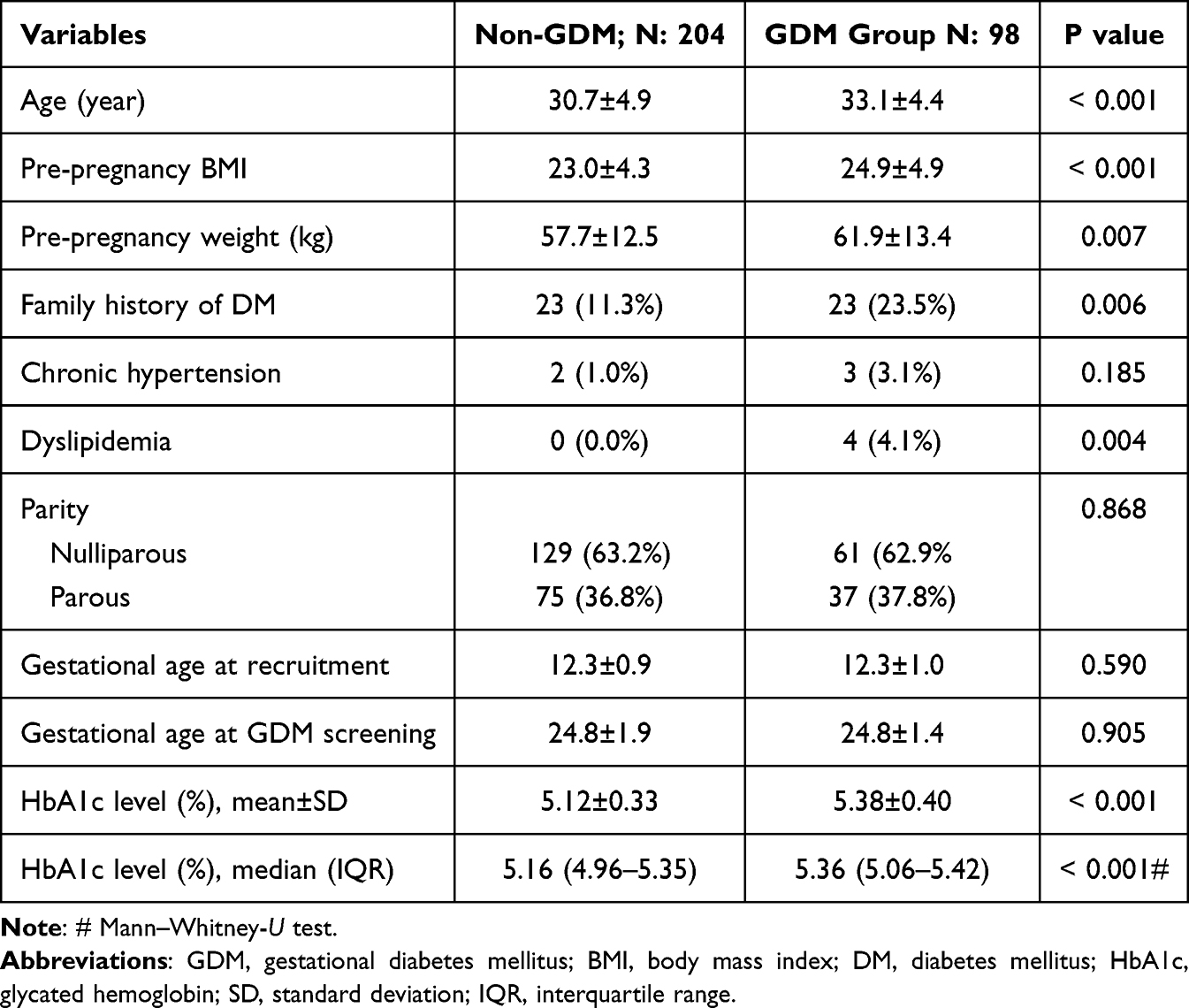 |
Table 1 Characteristics of GDM and Non-GDM Group |
 |
Figure 1 Flow chart of the study protocol. GDM: gestational diabetes mellitus. |
First-trimester HbA1c levels were significantly higher in women who subsequently developed GDM compared with those who did not, as presented in Table 1. The mean of HbA1c level in the GDM group was 5.38±0.40%, compared with 5.12±0.33% in the non-GDM group, as presented in Figure 2.
 |
Figure 2 Boxplots for comparison of the levels of Hb A1c (%) between the two groups (GDM, gestational diabetes mellitus; HbA1c, glycated hemoglobin). |
Multivariate logistic regression analysis was performed to develop a predictive model for GDM, with initial inclusion of potential risk factors, including HbA1c level, maternal age, pre-pregnancy BMI, family history of diabetes mellitus, and a history of dyslipidemia. The most parsimonious model retained only HbA1c level, maternal age, and pre-pregnancy BMI, as presented in Table 2. This model yielded an area under the receiver operating characteristic (ROC) curve of 0.726 (95% CI: 0.665 to 0.787). The area under the curve of the model incorporating HbA1c was significantly greater than that of the model without HbA1c (p = 0.035). The areas under the ROC curves for individual risk factors and for the predictive model are presented in Table 3 and Figure 3.
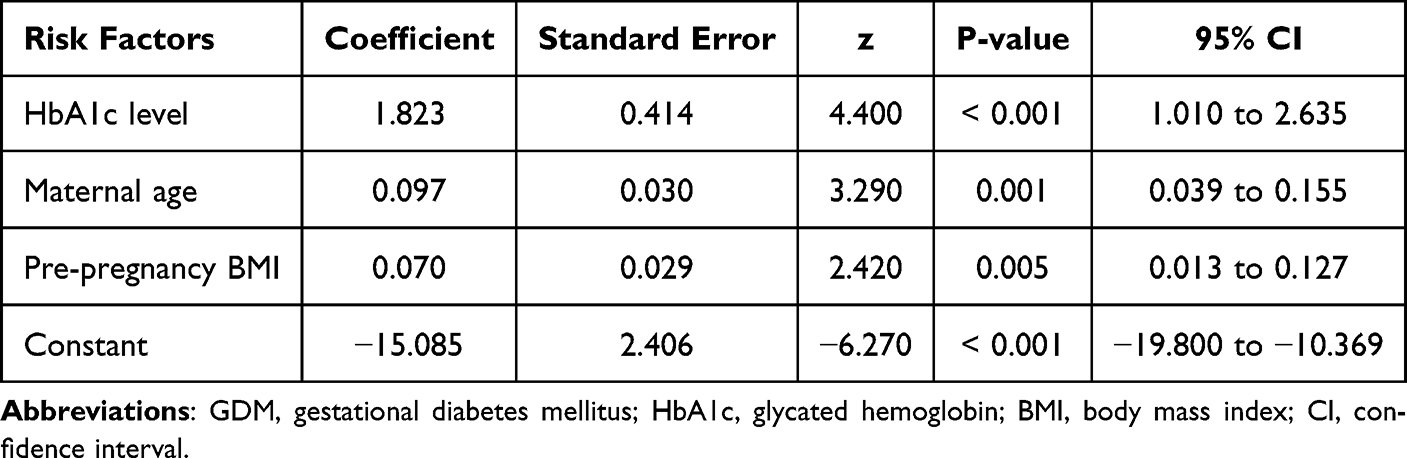 |
Table 2 Predictive Logistic Regression Parsimonious Model of First-Trimester Risk Factors for GDM |
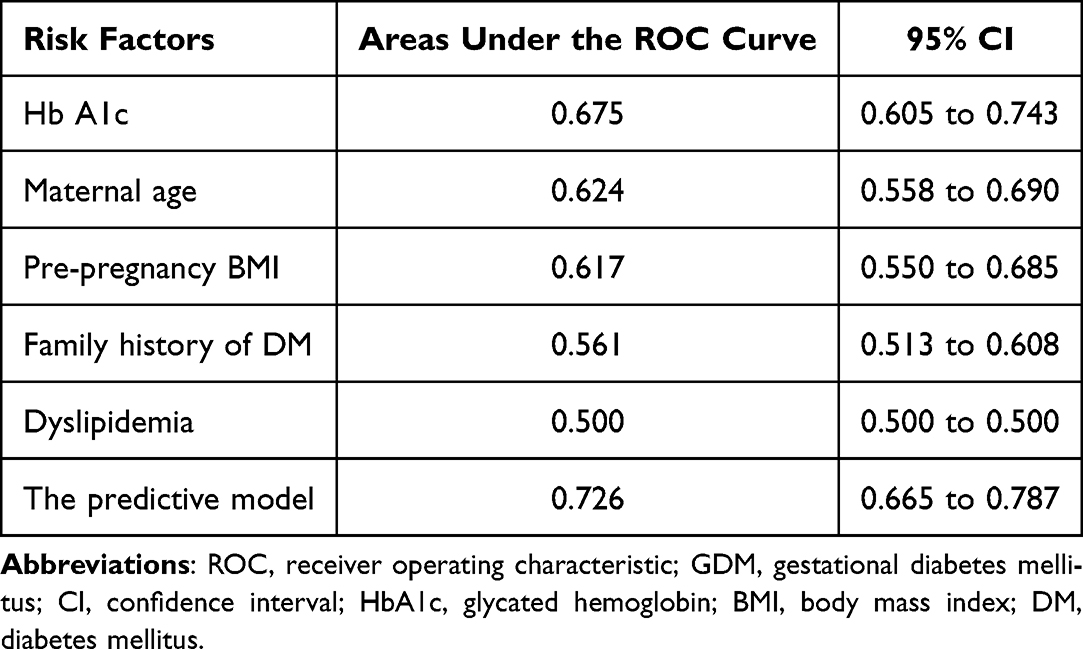 |
Table 3 Areas Under the ROC Curves of Individual First-Trimester Risk Factors and the Predictive Model for Gestational Diabetes Mellitus |
 |
Figure 3 ROC curves for individual biomarkers and combined models in predicting GDM. Abbreviations: ROC, receiver operating characteristic; GDM, gestational diabetes mellitus; BMI, body mass index; HbA1c, glycated hemoglobin. |
Internal validation of the predictive model for subsequent development of GDM, assessed using bootstrap resampling with 500 repetitions, demonstrated good calibration (slope: 0.968, AUC: 0.718, optimism: 0.008), as illustrated by the calibration plot in Figure 4. Using a probability cut-off of 0.245, the predictive model demonstrated moderate discriminative performance, with a sensitivity of 80.6% and a specificity of 51.0%, as well as high negative predictive value of 84.6%, as shown in Table 4.
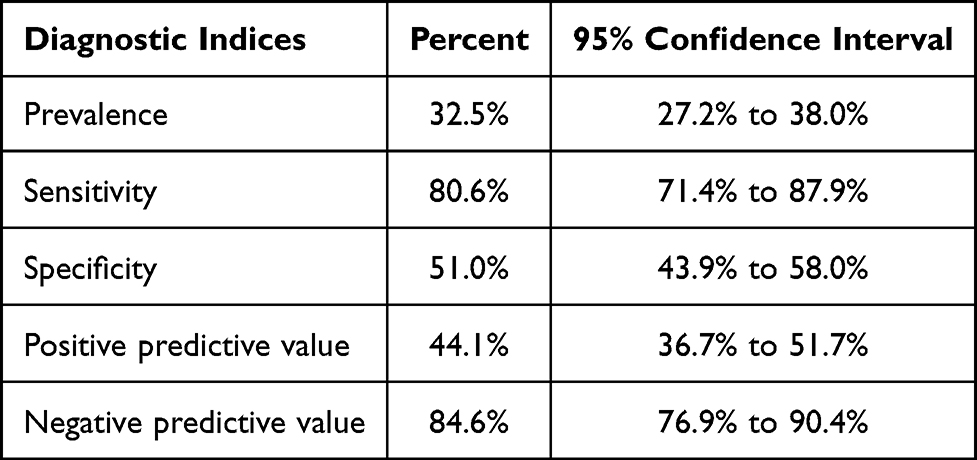 |
Table 4 Diagnostic Performance of the Predictive Model to Predict the Development of GDM in Late Pregnancy (a Probability Cut-off of 0.245) |
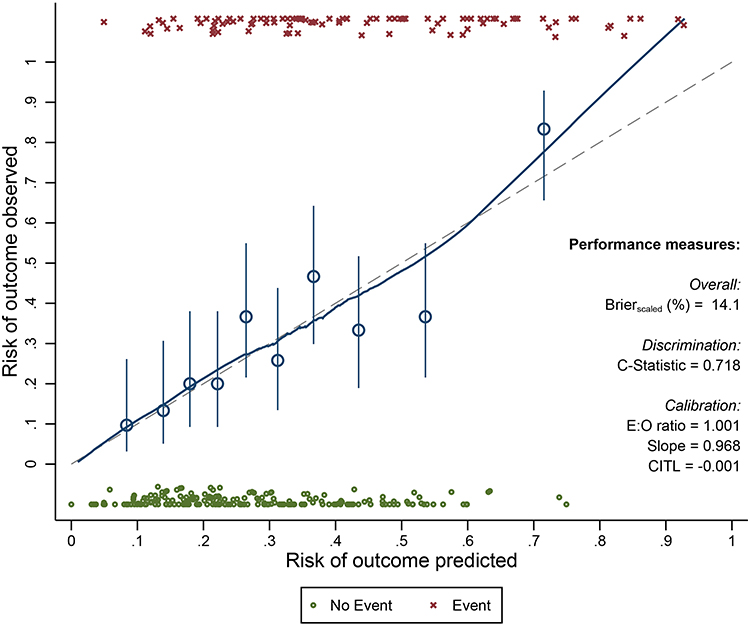 |
Figure 4 Calibration plot of the predictive model in predicting subsequent gestational diabetes mellitus. |
Discussion
Insights gained from this study are as follows: 1) First trimester HbA1c had modest performance in predicting GDM. 2) The combination of HbA1c levels and clinical characteristics could substantially improve the performance in predicting GDM.
First-trimester HbA1c levels were significantly higher among women who subsequently developed GDM compared with those who did not (5.38% vs. 5.12%, p < 0.001), consistent with findings from previous studies conducted in diverse populations.6,7,9,12,13 Comparable mean HbA1c values between GDM and non-GDM groups have been reported in Chinese (5.23% vs. 5.06%),7 Turkish (5.31% vs. 5.01%),13 Asian Indian (5.04% vs. 4.90%),6 and Swiss cohorts (5.26% vs. 5.10%).9 Despite the statistically significant difference observed, the discriminatory performance of HbA1c alone in our cohort was modest (AUC = 0.675). This performance was slightly superior to that reported in Asian Indian, Swiss, and Chinese populations (AUC range, 0.563–0.62),6,9,14 yet lower than the substantially higher accuracy described in Turkish and Iranian cohorts (AUC approximately 0.84).15,16 Such variability may be attributable to ethnic differences in baseline HbA1c distributions, as well as heterogeneity in diagnostic or inclusion criteria and study methodologies across populations. For example, some studies did not exclude cases with HbA1c levels greater than 6.5%,7,16 whereas others,15 including our study, applied this exclusion criterion. This may have narrowed the discriminatory range of HbA1c values and consequently contributed to the lower AUC observed.
Although HbA1c demonstrates statistical significance, it generally lacks adequate sensitivity to serve as a standalone screening or diagnostic test for GDM.7,14 While the application of higher HbA1c thresholds, such as values exceeding 5.9%, may improve specificity, sensitivity remains suboptimal, thereby increasing the likelihood of missed diagnoses when HbA1c is used in isolation.6,7 In contrast to most previous studies, our study evaluated HbA1c in combination with established clinical risk factors. This integrated approach significantly enhanced screening performance compared with HbA1c alone. From a practical standpoint, incorporating readily available clinical characteristics into risk assessment represents a pragmatic and cost-effective strategy, as these variables can be obtained without additional procedures, resources, or financial burden.
Notably, HbA1c appears to be more appropriately applied as a tool for early risk stratification rather than as a replacement for the OGTT.17 The proposed simplified model was able to identify approximately 80% of women who subsequently developed GDM within the Thai population. However, the false-positive rate was relatively high, which may increase the clinical workload associated with GDM screening, particularly in settings where universal screening is not routinely implemented. Importantly, elevated first-trimester HbA1c levels have been associated with adverse pregnancy outcomes, including fetal macrosomia, independent of a formal GDM diagnosis. This observation suggests that the clinical relevance of HbA1c may extend beyond the prediction of glucose intolerance alone, potentially reflecting broader metabolic risk during pregnancy.5,18,19
In clinical practice, where HbA1c is routinely used to exclude overt diabetes mellitus at the first visit, this model may help raise clinicians’ awareness and facilitate stratification of women into low- and high-risk groups for the subsequent development of GDM. However, for this purpose, HbA1c should be used in conjunction with clinical risk factors rather than used as a standalone predictor.
Research Implication
Although HbA1c may be useful for risk stratification in the first trimester, its predictive performance remains suboptimal. Therefore, additional biomarkers or clinical predictors that could enhance the diagnostic accuracy of HbA1c for early GDM screening warrant further investigation.
Strengths and Limitations
This study has several notable strengths. Its prospective design and consecutive recruitment strategy enhance methodological rigor and minimize selection bias. Additionally, the relatively adequate sample size and the homogeneity of the study population contribute to the internal validity and reliability of the findings, which was confirmed by the calibration plots. Nevertheless, certain limitations should be acknowledged. The sample size may have been insufficient to adequately evaluate less prevalent risk factors, such as dyslipidemia or a family history of DM, thereby limiting the statistical power to detect incremental benefits when incorporating these variables into the predictive model. Furthermore, the single-center design and exclusive inclusion of a Thai population may restrict the generalizability of the findings. Finally, other subtle conditions that may have confounded HbA1c levels, such as hemoglobinopathies and iron deficiency, were not evaluated in the present study.
Conclusions
First-trimester HbA1c levels are significantly elevated among women who subsequently develop GDM. Although HbA1c alone provides modest discriminatory capacity, integrating HbA1c with maternal age and pre-pregnancy BMI substantially enhances predictive performance. These findings support the application of this straightforward combined model for early pregnancy risk stratification, facilitating the identification of women at increased risk and enabling closer surveillance and timely intervention. Nonetheless, its predictive performance remains suboptimal. Therefore, further investigation into additional clinical predictors or novel biomarkers with stronger predictive capability is warranted to enhance the diagnostic accuracy of HbA1c for early screening of GDM.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by Research Ethics Committee 5, Faculty of Medicine, Chiang Mai University (Research Ethics Committee Panel 5; Research ID: OBG-2567-0726; date of approval: 06 January 2025).
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author (TT) upon reasonable request.
Informed Consent Statement
Written informed consent was obtained from all participants.
Acknowledgments
We would like to express our gratitude to MFM team who helped us in patient recruitment and collecting data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Faculty of Medicine, Chiang Mai University Research Fund (Grant Number: 091/2568). The funder had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. American Diabetes Association Professional Practice Committee. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S17–10. doi:10.2337/dc22-S002
2. Metzger BE, Gabbe SG, Persson B, et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(3):676–682. doi:10.2337/dc10-0719
3. Simmons D, Immanuel J, Hague WM, et al. Treatment of gestational diabetes mellitus diagnosed early in pregnancy. N Engl J Med. 2023;388(23):2132–2144. doi:10.1056/NEJMoa2214956
4. Bonora E, Tuomilehto J. The pros and cons of diagnosing diabetes with A1C. Diabetes Care. 2011;34 Suppl 2(Suppl 2):S184–190. doi:10.2337/dc11-s216
5. Hughes RC, Moore MP, Gullam JE, Mohamed K, Rowan J. An early pregnancy HbA1c ≥5.9% (41 mmol/mol) is optimal for detecting diabetes and identifies women at increased risk of adverse pregnancy outcomes. Diabetes Care. 2014;37(11):2953–2959. doi:10.2337/dc14-1312
6. Punnose J, Malhotra RK, Sukhija K, Mathew A, Sharma A, Choudhary N. Glycated haemoglobin in the first trimester: a predictor of gestational diabetes mellitus in pregnant Asian Indian women. Diabet Res Clin Pract. 2020;159:107953. doi:10.1016/j.diabres.2019.107953
7. Sun J, Chai S, Zhao X, et al. Predictive value of first-trimester glycosylated hemoglobin levels in gestational diabetes mellitus: a Chinese population cohort study. J Diabetes Res. 2021;2021:5537110. doi:10.1155/2021/5537110
8. Phoblap N, Jatavan P, Tongsong T. Comparison of universal screening for gestational diabetes mellitus between one-step and two-step method among Thai pregnant women: a randomized control trial. J Diabetes Investig. 2025;16(4):728–734. doi:10.1111/jdi.14370
9. Amylidi-Mohr S, Lang C, Mosimann B, et al. First-trimester glycosylated hemoglobin (HbA1c) and maternal characteristics in the prediction of gestational diabetes: an observational cohort study. Acta Obstet Gynecol Scand. 2023;102(3):294–300. doi:10.1111/aogs.14495
10. Goodall I. HbA1c standardisation destination--global IFCC Standardisation. How, why, where and when--a tortuous pathway from kit manufacturers, via inter-laboratory lyophilized and whole blood comparisons to designated national comparison schemes. Clin Biochem Rev. 2005;26(1):5–19.
11. Seino Y, Nanjo K, Tajima N, et al. Report of the committee on the classification and diagnostic criteria of diabetes mellitus. J Diabetes Investig. 2010;1(5):212–228. doi:10.1111/j.2040-1124.2010.00074.x
12. Arbib N, Shmueli A, Salman L, Krispin E, Toledano Y, Hadar E. First trimester glycosylated hemoglobin as a predictor of gestational diabetes mellitus. Int J Gynaecol Obstet. 2019;145(2):158–163. doi:10.1002/ijgo.12794
13. Kansu-Celik H, Ozgu-Erdinc AS, Kisa B, Eldem S, Hancerliogullari N, Engin-Ustun Y. Maternal serum glycosylated hemoglobin and fasting plasma glucose predicts gestational diabetes at the first trimester in Turkish women with a low-risk pregnancy and its relationship with fetal birth weight; a retrospective cohort study. J Matern Fetal Neonatal Med. 2021;34(12):1970–1977. doi:10.1080/14767058.2019.1651837
14. Wu K, Cheng Y, Li T, et al. The utility of HbA1c combined with haematocrit for early screening of gestational diabetes mellitus. Diabetol Metab Syndr. 2018;10(1):14. doi:10.1186/s13098-018-0314-9
15. Çetin C, Güngör ND, Yavuz M. First trimester glycosylated hemoglobin for gestational diabetes mellitus screening. Taiwan J Obstet Gynecol. 2021;60(5):899–902. doi:10.1016/j.tjog.2021.08.002
16. Valadan M, Bahramnezhad Z, Golshahi F, Feizabad E. The role of first-trimester HbA1c in the early detection of gestational diabetes. BMC Pregnancy Childbirth. 2022;22(1):71. doi:10.1186/s12884-021-04330-2
17. Benaiges D, Flores-Le Roux JA, Marcelo I, et al. Is first-trimester HbA1c useful in the diagnosis of gestational diabetes? Diabet Res Clin Pract. 2017;133:85–91. doi:10.1016/j.diabres.2017.08.019
18. Bhavadharini B, Mahalakshmi MM, Deepa M, et al. Elevated glycated hemoglobin predicts macrosomia among Asian Indian pregnant women (WINGS-9). Indian J Endocrinol Metab. 2017;21(1):184–189. doi:10.4103/2230-8210.196003
19. Mañé L, Flores-Le Roux JA, Benaiges D, et al. Role of first-trimester HbA1c as a predictor of adverse obstetric outcomes in a multiethnic cohort. J Clin Endocrinol Metab. 2017;102(2):390–397. doi:10.1210/jc.2016-2581
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Serum D-Dimer, Glycated Serum Protein, and HbA1c Levels in Predicting Macrosomia in Gestational Diabetes Mellitus
Quan Y, Wang Y
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2913-2921
Published Date: 15 August 2025
Predictive Value of Serum Pentraxin 3 and Galectin-3 in Early Pregnancy for Gestational Diabetes Mellitus in Chinese Women
Su Q, Yang J, Yang J, Zhang H, Fan Y
International Journal of Women's Health 2026, 18:612304
Published Date: 14 July 2026