Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 8
First molar health status in different craniofacial relationships
Authors Linjawi A ![]()
Received 17 March 2016
Accepted for publication 8 April 2016
Published 5 July 2016 Volume 2016:8 Pages 89—94
DOI https://doi.org/10.2147/CCIDE.S108670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Amal I Linjawi
Department of Orthodontics, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia
Objective: To investigate the association between the health status of permanent first molars and different craniofacial relationships among adolescents.
Study design: This is a retrospective study on patients’ records aged 11–15 years. Sex, skeletal relationship, vertical growth pattern, malocclusion, overjet, and overbite were assessed. The health status of permanent first molars was recorded from the orthopantomograms and intraoral photographs as “sound” and “not sound”. Chi-square, Mann–Whitney U and Kruskal–Wallis tests, and Pearson’s correlation coefficient were used to analyze and correlate the assessed variables. Significance level was set at P<0.05.
Results: A total of 210 records were evaluated; 81 were male, 68 had Class I and 91 had Class II skeletal relationships. More than half of the subjects had normal (n=67) to moderate deep bite (n=72); normal (n=91), moderately increased (n=54), to severely increased (n=50) overjet; and Class I (n=106) and Class II division 1 (n=75) malocclusion. Significant differences were found in the health status of the permanent first molars with respect to sex (P=0.034), vertical growth pattern (P=0.01), and overbite (P=0.047). Strong correlations were only found between the health status of the permanent first molars and the following variables: sex (P=0.036) and vertical growth pattern (P=0.004). Significant correlation was further found between the upper left first molar health status and sex (P=0.019) and the lower right first molar health status and the vertical growth pattern (P=0.001). No significant association was found with the anteroposterior craniofacial relationships (P>0.05).
Conclusion: Sex difference and vertical growth patterns were found to be potential predictors of the health status of the permanent first molars. No significant association was found with the anteroposterior craniofacial relationships.
Keywords: craniofacial morphology, first molars, dental caries, overbite, skeletal relationships
Introduction
The health status of the molar region is under the pressure of multiple surrounding variables, including oral hygiene, biting forces, craniofacial morphology, as well as the dental malocclusion.1–7 The permanent first molars, being the first permanent posterior teeth to erupt in the oral cavity, face high load and pressure for healthy survival until adulthood.
The correlation between dental caries on the posterior teeth and malocclusion had been investigated in the literature. Crowding was found to be strongly associated with high caries index, which was claimed to cause difficulty in brushing and maintaining good oral health,6,8,9 especially in the mandibular anterior region.2,3 In contrast, such correlation was negatively affected in the maxillary posterior region.2,3 Singh et al5 also found a strong correlation between caries and severe malocclusions among school children.Other dental problems, including posterior crossbite and mandibular overjet, were also found to be significantly associated with dental caries in the mixed dentition.10,11 However, Mtaya et al4 and Borzabadi-Farahani et al12 found that the socioeconomic status played a major role in the association between malocclusion and dental caries.
The relationship between form and function, especially in the craniofacial skeleton, might have an added effect on the health status of posterior teeth.13–16 Overbite and the biting forces on the posterior teeth were found to have a direct strong correlation.1,17 Subjects with normal vertical dimension showed twice as great mean bite force in the molar region than those with long face anterior open bite.16,18 In contrast, subjects with a short face and deep bite generated higher biting forces than those with a normal face.16,18,19 Muscle activities and the musculoskeletal relationships were also found to correlate with facial morphology and thus have an effect on the biting forces.20 For example, a square face was found to generate high biting forces by providing a higher mechanical advantage for muscles of mastication,21 while a face with a diverged mandibular plane angle showed a negative relationship with the muscle activity level.22 Tooth wear was also found to be more evident in subjects with stronger biting forces and decreased vertical skeletal relationships.7 Biting force was further found to be strongly correlated with the number of teeth in contact19,23 and age.24,25 However, other studies showed no significant correlations between biting force and the following occlusal relationships: functional occlusion, the presence of occlusal interferences,14,24 as well as the sagittal molar relationships as defined by the Angle classification.16,20 The correlation with sex showed varied results.13,14,20
From the latter findings, it was hypothesized that the permanent first molar health status might be affected by the biting forces and thus might correlate differently with different craniofacial relationships. Thus, the aim of this study was to investigate the association between the health status of the permanent first molars and different craniofacial relationships in adolescents.
Materials and methods
Study design
This is a retrospective study with a sample comprising pretreatment records of patients at the outpatient clinic of the Department of Orthodontics, King Abdulaziz University, Jeddah, Saudi Arabia. The study was approved by the King Abdulaziz University, Faculty of Dentistry Ethical Committee as it involved the data of patients. However, due to the restrospective nature of the study the committee deemed patient consent unnecessary.
Sample
The selection of patients’ records included the following criteria: age range from 11 to 15 years; no history of orthodontic treatment; no severe craniofacial disorders such as cleft palate; and had pretreatment intraoral photographs, orthopantomograms, and lateral cephalometric radiographs. Records of 400 randomly selected patients’ files were then screened, of which 210 files fulfilled the selection criteria.
Data collection
Lateral cephalometric radiographs of the selected cases were traced and analyzed by a trained examiner to identify the underlying anteroposterior and vertical morphologies. The anteroposterior morphologies included the anteroposterior skeletal relationship, malocclusion classification, and the overjet. The vertical morphologies included the vertical growth pattern and the overbite.
The variables assessed were then defined and categorized as follows:
- The anteroposterior skeletal relationship was defined based on ANB angle as: Class I (ANB 2–4°), Class II (ANB >4°), and Class III (ANB <2°).
- The vertical growth pattern was defined based on Frankfort-Mandibular plane angle (FMA) as; normal (FMA 23°–27°), horizontal (FMA <23°), and vertical (FMA >27°) growth patterns.
- The overbite was measured on the cephalometric radiograph to the nearest 0.5 mm and defined as: average (2–4 mm), moderate deep bite (4–6 mm), severe deep bite (>6 mm), shallow bite (0–1 mm), moderate open bite (−1 to −3 mm), and severe open bite (less than −3 mm).
- The overjet was measured on the cephalometric radiograph to the nearest 0.5 mm and defined as: normal (2–4 mm), reduced (<2–0 mm), reverse overjet (<0 mm), moderately increased (>4–6 mm), and severely increased overjet (>6 mm).
- The malocclusion was classified on the intraoral photographs according to the Angle’s classification as: Class I, Class II division 1, Class II division 2, and Class III.
The health status of the first four permanent molars (upper right, upper left, lower left, lower right) was assessed on the orthopantomograms and confirmed by the intraoral photographs. The health status of each tooth was then scored as sound (S), decayed (D), missing (M), or filled (F) tooth. The DMF (decayed, missing, filled) scores were then given a collective score as not sound (NS). Thus, each tooth was finally scored as either S or NS. The number of S and NS teeth for each case was further recorded.
Statistical analysis
Before data collection, ten cases were randomly selected and the health status of the first permanent molars was recorded twice, 2 weeks apart, to calculate the intra-examiner reliability. The kappa statistics of intra-examiner consistency was 0.80 for the first four molar categories.
Descriptive statistics and group comparison were further calculated using the Pearson chi-square test, Mann–Whitney U-test, and Kruskal–Wallis test. The Pearson’s correlation coefficient was used to correlate the assessed craniofacial components with the health status of the permanent first molars. All statistical analyses were done by the SPSS 16.0 software (SPSS Inc. Chicago, USA). The significance level was set at P<0.05.
Results
A total of 210 records were evaluated with the following findings: 81 were male subjects and 129 were female subjects. The majority of subjects had the following categories of craniofacial morphologies: Class I (n=68) and Class II (n=91) skeletal relationships; normal (n=67) to moderate deep bite (n=72); normal (n=91), moderately increased (n=54), to severely increased (n=50) overjet; and Class I (n=106) and Class II division 1 (n=75) malocclusion (Table 1).
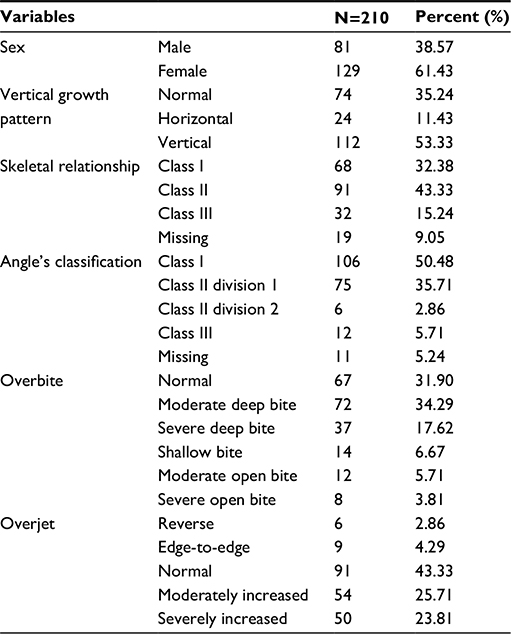 | Table 1 Sample distribution by variables |
The health status of the permanent first molars was found to differ significantly with regard to sex difference (P=0.034), vertical growth pattern (P=0.01), and overbite (P=0.047). In male subjects, 44.4% had all first molars S and only 12.3% had all first molars NS. On the other hand, in female subjects, 36.4% had all first molars S and 31.0% had all first molars NS. Others had between one and three molars as NS (Figure 1).
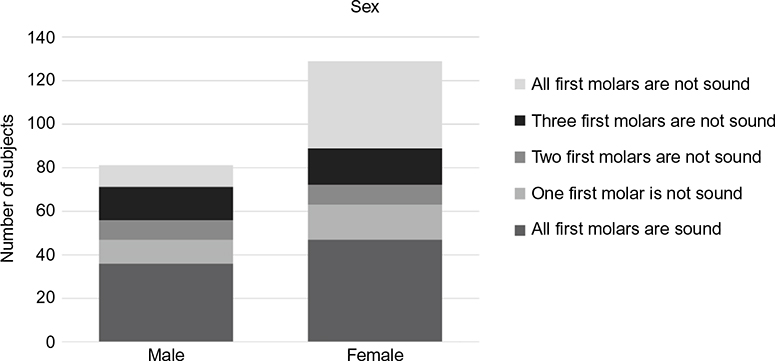 | Figure 1 Health status of the permanent first molars distributed according to sex. Note: Using a Mann-Whitney U test, a significant difference in molar health status between sex was reported (P<0.004). |
The health status of the permanent first molars was also found to differ significantly by changes in the vertical growth pattern (P=0.01). A total of 46% of the subjects with normal growth pattern had all their first molars S, while only 19% had all first molars NS. In subjects with horizontal growth pattern, 58.3% had all first molars S, while only 20.8% of those subjects had all first molars NS. In subjects with vertical growth pattern, 31.3% had all first molars S and 27.7% had all first molars NS (Figure 2).
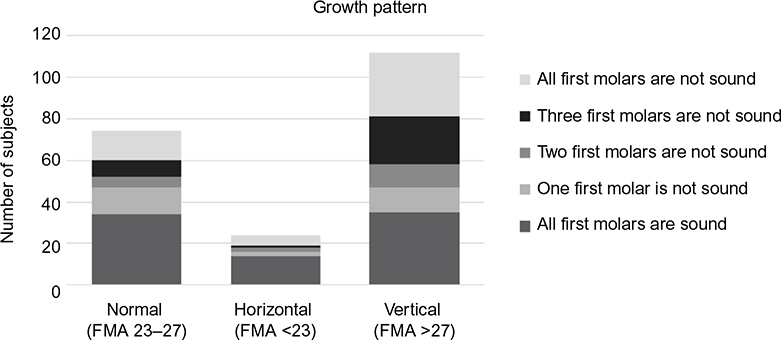 | Figure 2 Health status of the permanent first molars distributed according to vertical growth pattern. Note: Using a Kruskal-Wallis test, a significant difference in molar health status between the different growth pattern was reported (P<0.014). Abbrevation: FMA, Frankfort-Mandibular plane angle. |
The health status was also found to differ significantly by changes in overbite (P=0.047). In subjects with normal overbite, 22.4% had all first molars S and 38.8% had all first molars NS. In subjects with moderate deep bite, 29.2% had all first molars S and 37.5% had all first molars NS. In subjects with severe deep bite, only 8.1% had all first molars S and 59.5% had all first molars NS. In subjects with shallow bite, 28.6% had all first molars S and 35.7% had all first molars NS. In subjects with moderate open bite, 41.7% had all first molars S and 33.3% had all first molars NS. In subjects with severe open bite, 25.0% had all first molars S, while 75.0% of the latter group had 1–3 first molars NS, but none of the subjects had all first molars NS (Figure 3).
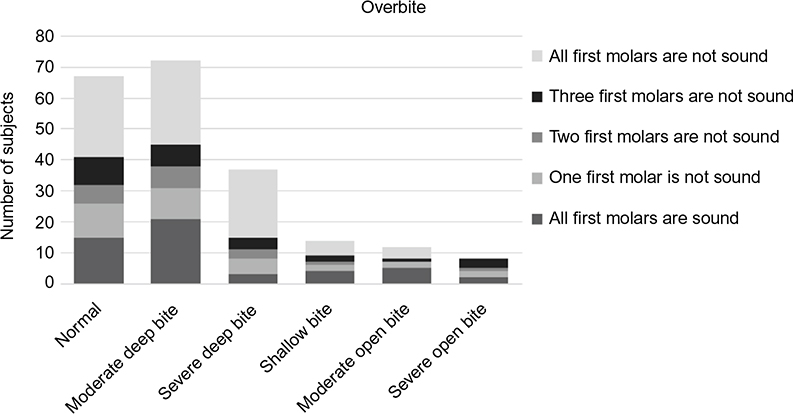 | Figure 3 Health status of the permanent first molars distributed according to overbite. Note: Using a Kruskal-Wallis test, a significant difference in molar health status between the different overbite was reported (P<0.047). |
In contrast to the latter findings, no significant association was found between the health status of the permanent first molars and the following anteroposterior variables: skeletal relationship (P=0.503), malocclusion classification (P=0.849), and overjet (P=0.536).
The Pearson’s correlation coefficient revealed that the sex (P=0.036) and vertical growth pattern (P=0.004) had a significant impact on the first molar health status (Table 2).
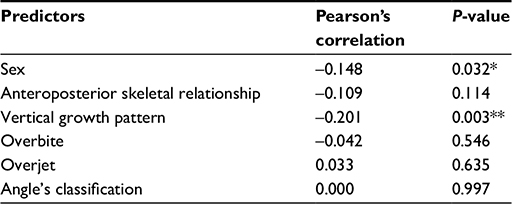 | Table 2 Results of the Pearson correlation coefficient analysis based on “health status of permanent first molars” Notes: Significant using the Pearson’s correlation test at *P<0.05, **P<0.01. |
Data were further analyzed for significant association between the health status of each category of permanent first molars and the different craniofacial components assessed. Results showed a significant association between the health status of the upper left first molar and sex (P=0.019). Seventy-four percent of the male subjects had the upper left first molar recorded as S, while female subjects had equal percentages of upper left first molar recorded as S and NS. Results also showed a significant association between the health status of the lower right first molar and the vertical growth pattern (P=0.001). In total, 70.8% of the horizontal growers and 64.8% of the normal growers had their lower right first molars recorded as S, while almost 60% of the vertical growers had their lower right first molars recorded as NS.
Discussion
The health status of the permanent first molars seems to be affected by multiple factors. They are the first permanent teeth to erupt in the oral cavity and act as the first vertical, anteroposterior, and transverse stop for the permanent occlusion. Understanding the skeletal, functional, and dental components that affect the health status of the permanent first molars is thus a crucial step when planning for preserving them.
The current study showed a significant association between the health status of the permanent first molars and the vertical growth pattern. The more horizontal the growth, the more was the number of sound and healthy first molars recorded. Similar positive findings were reported when correlating the molar biting force with the vertical growth pattern.16,18–20
The current study also showed a negative correlation between the health status of the permanent first molars and overbite. The more increase in overbite, the less was the number of sound and healthy first molars recorded. On the contrary, the relationship between the molar biting force and the overbite showed positive correlations in multiple studies.1,16–20,23,26
No correlation between the anteroposterior craniofacial morphology and the health status of the permanent first molars was reported in this study, as well as with the biting force as reported in other studies.16,18
The biting force and sex in most studies showed a strong correlation, as males exhibit stronger molar biting force than females.13,14,16,20 The current findings also showed that sex difference had a significant impact on the health status of the first molars.
In comparison to findings related to the biting forces, the health status of the permanent first molars showed similar direct association with the vertical craniofacial dimensions, including vertical growth pattern and overbite; as well as with sex difference. Thus, a direct correlation between the biting force and the health status of the permanent first molars can be investigated in further research.
Limitations
Multiple studies reported a significant association between dental caries and crowding.6 Others found a significant correlation between the number of teeth in contact and the molar biting force.16–20,23,26 Alabdullah et al27 also reported a positive correlation between the molar biting force and the axial inclination of upper and lower incisors. They found that the higher the number of proclined incisors, the more the molar biting force.27 Transverse craniofacial relationships and crossbite also had a reported association with the biting force.10,11 However, such factors, which might have a contributing effect on the health status of the permanent first molars, were not assessed in the current study. Other variables, such as the oral hygiene status, were also not evaluated. Further research is required to assess all the factors together for better conclusion. A direct assessment of the correlation between the biting force and the health status of the permanent first molars is also needed.
Conclusion
The health status of the permanent first molars was strongly affected by sex difference and vertical growth pattern. No significant association was found with the anteroposterior craniofacial relationships.
Disclosure
The author reports no other conflicts of interest in this work.
References
Feldens CA, Dos Santos Dullius AI, Kramer PF, Scapini A, Busato AL, Vargas-Ferreira F. Impact of malocclusion and dentofacial anomalies on the prevalence and severity of dental caries among adolescents. Angle Orthod. 2015;85(6):1027–1034. | ||
Hafez HS, Shaarawy SM, Al-Sakiti AA, Mostafa YA. Dental crowding as a caries risk factor: a systematic review. Am J Orthod Dentofacial Orthop. 2012;142(4):443–450. | ||
Long H, Lai W. No reliable evidence for the association between dental crowding and caries. Evid Based Dent. 2013;14(1):12. | ||
Mtaya M, Brudvik P, Astrom AN. Prevalence of malocclusion and its relationship with socio-demographic factors, dental caries, and oral hygiene in 12- to 14-year-old Tanzanian schoolchildren. Eur J Orthod. 2009;31(5):467–476. | ||
Singh A, Purohit B, Sequeira P, Acharya S, Bhat M. Malocclusion and orthodontic treatment need measured by the dental aesthetic index and its association with dental caries in Indian schoolchildren. Community Dent Health. 2011;28(4):313–316. | ||
Baskaradoss JK, Geevarghese A, Roger C, Thaliath A. Prevalence of malocclusion and its relationship with caries among school children aged 11–15 years in southern India. Korean J Orthod. 2013;43(1):35–41. | ||
Kiliaridis S, Johansson A, Haraldson T, Omar R, Carlsson GE. Craniofacial morphology, occlusal traits, and bite force in persons with advanced occlusal tooth wear. Am J Orthod Dentofacial Orthop. 1995;107(3):286–292. | ||
Vellappally S, Gardens SJ, Al Kheraif AA, et al. The prevalence of malocclusion and its association with dental caries among 12–18-year-old disabled adolescents. BMC Oral Health. 2014;14:123. | ||
Gaikwad SS, Gheware A, Kamatagi L, Pasumarthy S, Pawar V, Fatangare M. Dental caries and its relationship to malocclusion in permanent dentition among 12–15 year old school going children. J Int Oral Health. 2014;6(5):27–30. | ||
Stahl F, Grabowski R. Malocclusion and caries prevalence: is there a connection in the primary and mixed dentitions? Clin Oral Investig. 2004;8(2):86–90. | ||
Castelo PM, Gaviao MB, Pereira LJ, Bonjardim LR. Masticatory muscle thickness, bite force, and occlusal contacts in young children with unilateral posterior crossbite. Eur J Orthod. 2007;29(2):149–156. | ||
Borzabadi-Farahani A, Eslamipour F, Asgari I. Association between orthodontic treatment need and caries experience. Acta Odontol Scand. 2011;69(1):2–11. | ||
Abu Alhaija ES, Al Zo’ubi IA, Al Rousan ME, Hammad MM. Maximum occlusal bite forces in Jordanian individuals with different dentofacial vertical skeletal patterns. Eur J Orthod. 2010;32(1):71–77. | ||
Koc D, Dogan A, Bek B. Effect of gender, facial dimensions, body mass index and type of functional occlusion on bite force. J Appl Oral Sci. 2011;19(3):274–279. | ||
Park JC, Shin HS, Cha JY, Park JT. A three-dimensional finite element analysis of the relationship between masticatory performance and skeletal malocclusion. J Periodontal Implant Sci. 2015;45(1):8–13. | ||
Sathyanarayana HP, Premkumar S, Manjula WS. Assessment of maximum voluntary bite force in adults with normal occlusion and different types of malocclusions. J Contemp Dent Pract. 2012;13(4):534–538. | ||
Iwasaki H, Fujita S, Yoshida H, Inaba R, Iwata H. 岩崎, 秀., 節. 藤田, 英. 吉田, 良. 井奈波 and 弘. 岩田 (1995). “咬合力と顎顔面形態との関係.” 日本衛生学雑誌 [Relationships between biting force and the morphology of the maxilloface]. Nihon Eiseigaku Zasshi. 1995;50(2):683–692. Japanese. | ||
Proffit WR, Fields HW, Nixon WL. Occlusal forces in normal- and long-face adults. J Dent Res. 1983;62(5):566–570. | ||
Sonnesen L, Bakke M. Molar bite force in relation to occlusion, craniofacial dimensions, and head posture in pre-orthodontic children. Eur J Orthod. 2005;27(1):58–63. | ||
Singh S, Sandhu N, Kashyap R. A study of bite force and various variables in children segregated by Angle’s classification. Int J Clin Pediatr Dent. 2012;5(2):118–123. | ||
Bonakdarchian M, Askari N, Askari M. Effect of face form on maximal molar bite force with natural dentition. Arch Oral Biol. 2009;54(3):201–204. | ||
Garcia-Morales P, Buschang PH, Throckmorton GS, English JD. Maximum bite force, muscle efficiency and mechanical advantage in children with vertical growth patterns. Eur J Orthod. 2003;25(3):265–272. | ||
Sonnesen L, Bakke M, Solow B. Bite force in pre-orthodontic children with unilateral crossbite. Eur J Orthod. 2001;23(6):741–749. | ||
Takaki P, Vieira M, Bommarito S. Maximum bite force analysis in different age groups. Int Arch Otorhinolaryngol. 2014;18(3):272–276. | ||
Varga S, Spalj S, Lapter Varga M, Anic Milosevic S, Mestrovic S, Slaj M. Maximum voluntary molar bite force in subjects with normal occlusion. Eur J Orthod. 2011;33(4):427–433. | ||
Roldan SI, Restrepo LG, Isaza JF, Velez LG, Buschang PH. Are maximum bite forces of subjects 7 to 17 years of age related to malocclusion? Angle Orthod. 2016;86(3):456–461. | ||
Alabdullah MM, Saltaji H, Abou-Hamed H, Youssef M. The relationship between molar bite force and incisor inclination: a prospective cross-sectional study. Int Orthod. 2014;12(4):494–504. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.