Back to Journals » Biologics: Targets and Therapy » Volume 20
First-Line Serplulimab versus Other Anti-PD-1/PD-L1 Antibodies Plus Chemotherapy for Esophageal Squamous Cell Carcinoma: A Systematic Review with Benefit-Risk Assessment via Matching-Adjusted Indirect Comparison
Authors Zhu Y, Qi X, Ni S, Qiu W, Chen M
Received 10 February 2026
Accepted for publication 23 February 2026
Published 28 February 2026 Volume 2026:20 602654
DOI https://doi.org/10.2147/BTT.S602654
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shein-Chung Chow
Yi Zhu, Xiao Qi, Senmiao Ni, Wenting Qiu, Mengkai Chen
Department of Biostatistics, Shanghai Henlius Biotech, Inc., Shanghai, People’s Republic of China
Correspondence: Mengkai Chen, Department of Biostatistics, Shanghai Henlius Biotech, Inc., 188 Yizhou Road, Shanghai, 200233, People’s Republic of China, Tel +86-156-5172-5532, Email [email protected]
Purpose: Blockade of the PD-L1/PD-1 pathway combined with chemotherapy has demonstrated significant survival benefits as first‑line therapy for esophageal squamous cell carcinoma (ESCC). However, comprehensive benefit-risk comparisons among approved agents remain limited. This study conducted an indirect comparison of serplulimab versus other anti-PD-1/PD-L1 antibodies plus chemotherapy in treatment-naïve ESCC patients.
Patients and Methods: A systematic review with matching-adjusted indirect comparisons (MAICs) was conducted using individual patient data (IPD) from ASTRUM-007 and aggregate data (AgD) from seven comparator trials, including CheckMate 648, ESCORT-1st, GEMSTONE-304, JUPITER-06, KEYNOTE-590, ORIENT-15, and RATIONALE-306. IPD were reweighted to match key baseline characteristics. Hazard ratios (HRs) for overall survival (OS) and progression-free survival (PFS) were estimated using the Bucher method. Subgroup analyses were further explored using Bayesian network meta-analysis.
Results: Eight Phase 3 randomized controlled trials comprising 4,702 patients were included. After adjusting for baseline imbalances, serplulimab demonstrated comparable efficacy to other PD-1/PD-L1 inhibitors. The pooled adjusted OS HR was 0.98 (95% CI, 0.87– 1.11), with numerically favorable OS versus nivolumab (HR, 0.76; 95% CI 0.47– 1.24) and comparable OS versus pembrolizumab (HR, 0.93; 95% CI, 0.71– 1.22) and camrelizumab (HR, 0.93; 95% CI, 0.70– 1.24). The pooled adjusted PFS HR was 0.91 (95% CI, 0.81– 1.02), significantly favoring serplulimab over nivolumab (HR, 0.56; 95% CI, 0.33– 0.96), with favorable trends versus pembrolizumab (HR, 0.83; 95% CI, 0.63– 1.10) and sugemalimab (HR, 0.86; 95% CI, 0.63– 1.16). Subgroup analyses suggested greater relative benefit in women and patients with locally advanced disease. Grade 3– 5 treatment-related adverse events occurred in 52.9% of serplulimab-treated patients, comparable to other PD-1/PD-L1 inhibitors (range, 47.4%-71.9%).
Conclusion: This indirect comparison provides comparative benefit-risk evidence to inform first‑line treatment selection for locally advanced or metastatic ESCC. Serplulimab plus chemotherapy demonstrated a clinically meaningful PFS benefit, comparable OS after matching, and a manageable safety profile consistent with the PD-1/PD-L1 inhibitor class.
Keywords: matching-adjusted indirect comparison, immune checkpoint inhibitor, esophageal neoplasms, benefit-risk assessment, first-line therapy
Introduction
Esophageal cancer remains a major cause of cancer-related morbidity and mortality worldwide, ranking seventh in incidence and sixth in mortality in 2020.1 Histologically, the disease is predominantly divided into esophageal squamous cell carcinoma (ESCC) and esophageal adenocarcinoma, with ESCC constituting the majority of cases at approximately 84% of all diagnoses.2 For patients with advanced or metastatic ESCC, first-line systemic therapy typically consists of platinum-based chemotherapy (cisplatin or oxaliplatin) combined with either a fluoropyrimidine or paclitaxel.3 However, clinical outcomes with these regimens remain suboptimal, with median overall survival (OS) rarely exceeding 10 months,4,5 underscoring the urgent need for more effective therapeutic strategies with acceptable safety profiles.
Recent progress in immuno-oncology has substantially reshaped the therapeutic paradigm for ESCC. In particular, immune checkpoint inhibitors (ICIs) directed against the programmed cell death protein 1 (PD-1) and its ligand PD-L1 have demonstrated meaningful clinical activity across multiple malignancies, including ESCC.6 Accumulating evidence from confirmatory clinical trials has further confirmed the clinical benefit of ICI-based combination strategies. One of the preferred first-line treatments for advanced ESCC is chemoimmunotherapy, consisting of platinum-based chemotherapy administered in combination with anti-PD-1/PD-L1 agents such as pembrolizumab and nivolumab, followed by continuation of anti-PD-1/PD-L1 agents as monotherapy maintenance.7,8
Serplulimab, a recombinant humanized anti-PD-1 IgG4 monoclonal antibody (mAb), was approved by the National Medical Products Administration (NMPA) of China for the first-line treatment of adult patients with ESCC in combination with chemotherapy based on the pivotal ASTRUM-007 trial. In this phase 3 study, serplulimab plus chemotherapy significantly improved overall survival versus placebo plus chemotherapy in patients with PD-L1 positive ESCC (median OS, 15.3 months vs 11.8 months; hazard ratio [HR] 0.68 [95% confidence interval (CI): 0.53–0.87]; p = 0.0020) at a median follow-up of approximately 15 months.9
Consistent with regulatory frameworks for benefit-risk assessment, a comprehensive understanding of the relative benefit-risk profiles of available treatment options is essential for informed clinical decision-making. Despite the demonstrated efficacy of individual anti-PD-1/PD-L1 agents in the first-line treatment of ESCC, direct comparative evidence from head-to-head randomized clinical trials is lacking,7–13 precluding robust comparative benefit-risk assessments among these therapies. To address this evidence gap, we conducted a series of matching-adjusted indirect comparisons (MAICs) to evaluate the comparative efficacy and safety of serplulimab versus other anti-PD-1/PD-L1 agents plus chemotherapy in patients with ESCC. This systematic benefit-risk assessment aims to inform evidence-based treatment selection in the first-line management of advanced or metastatic ESCC.
Materials and Methods
Study Population and Established Evidence
Individual patient -level data (IPD) from the phase 3 ASTRUM-007 trial (ClinicalTrials.gov identifier: NCT03958890) served as the primary dataset for evaluating the comparative efficacy of serplulimab. In ASTRUM-007, a total of 551 eligible patients were randomized (2:1) to receive serplulimab or placebo in combination with chemotherapy. Eligible patients were aged 18–75 years with previously untreated, histologically confirmed, inoperable locally advanced or metastatic, PD-L1-positive (combined positive score [CPS] ≥1) ESCC, at least one measurable lesion per Response Evaluation Criteria in Solid Tumors (RECIST) v1.1 criteria based on central imaging review, adequate organ function, and Eastern Cooperative Oncology Group (ECOG) performance status 0–1. Additional study design details have been published previously.9
Phase 3 randomized clinical trials of seven anti-PD-1/PD-L1 antibodies were identified from the primary literature to serve as comparators. Eligible trials met the following criteria: 1) locally advanced or metastatic ESCC, 2) an anti-PD-(L)1 antibody plus platinum-based chemotherapy versus placebo plus platinum-based chemotherapy as first-line therapy. In addition, enrolled subjects were required to be aged ≥18 years, have ECOG performance status 0–1, and have received no prior systemic therapy for ESCC. Trials were further required to report OS outcomes with over 15 months of follow-up, and to have ≥50% of the protocol-specified PFS and OS events observed.
After applying the above criteria, CheckMate 648,7 ESCORT-1st,12 GEMSTONE-304,11 JUPITER-06,13 KEYNOTE-590,8 RATIONALE-306,10 and ORIENT-1514 were selected for comparison; key study characteristics and results are summarized in Table 1. Overall, eligibility criteria were broadly comparable across the included phase 3 trials.
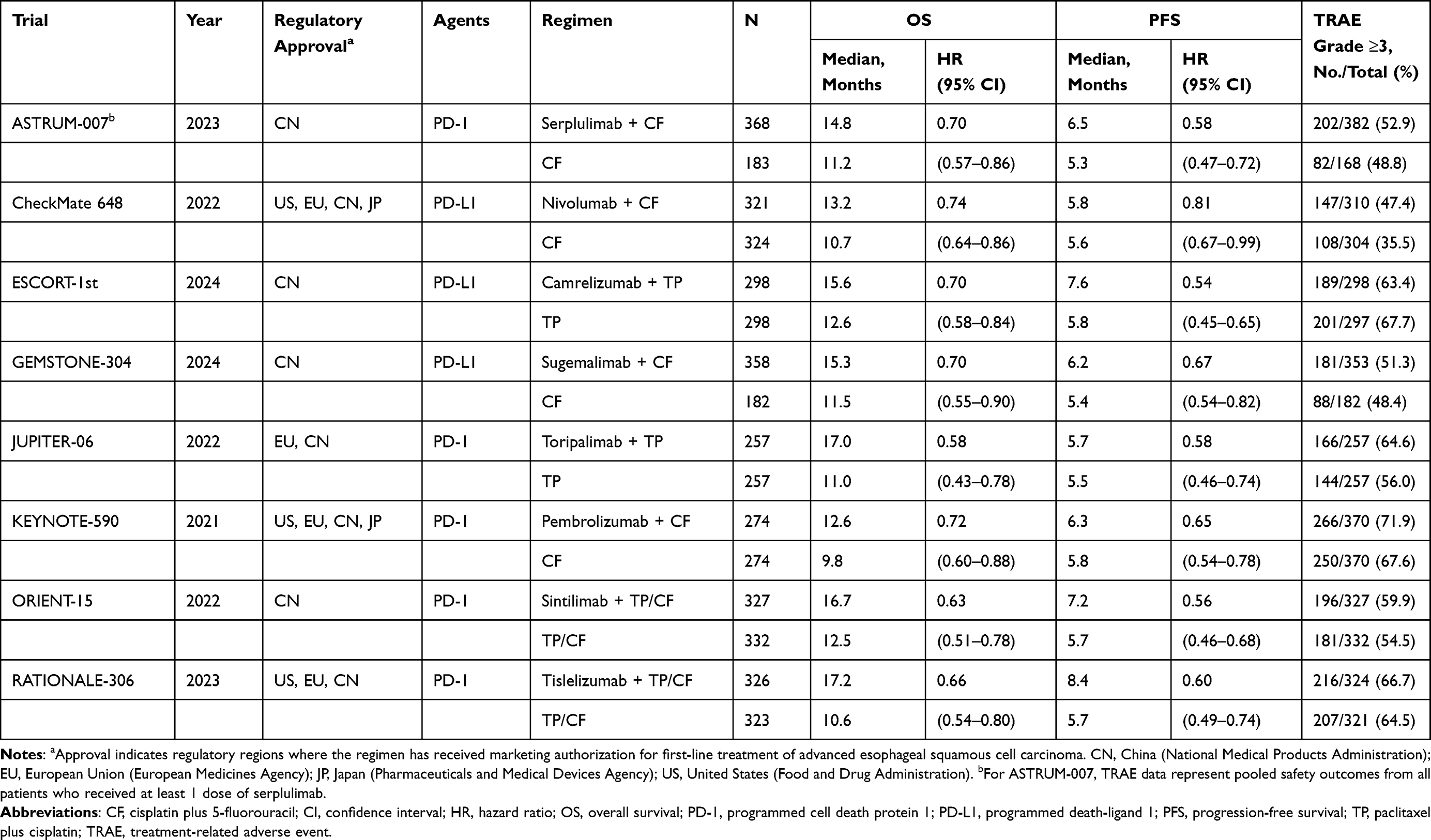 |
Table 1 Summary of Key Characteristics and Data Across Eight Studies Included in the Indirect Comparison Analysis |
Key Baseline Characteristics
Baseline characteristics with potential effect modification or prognostic value included age (<65 years vs ≥65 years), sex (male vs female), ECOG performance status (0 vs 1), smoking status (never smoker vs former/current smoker), and disease status (locally advanced or distantly metastatic). For efficacy analyses, adjustment strategies differed by trial based on data availability. In ESCORT-1st and RATIONALE-306, all prespecified baseline characteristics were adjusted. In JUPITER-06 and CheckMate 648, adjustments were made for gender, ECOG performance status, smoking status, and disease status, as the proportion of patients aged ≥65 was not reported. In GEMSTONE-304, KEYNOTE-590, and ORIENT-15, adjustments included age, sex, ECOG performance status, and disease status, as smoking status was not reported.
Outcome Measures
The efficacy outcomes evaluated were OS and PFS. OS was defined as the time from randomization to death from any cause. PFS was defined as the time from randomization to the first documented objective tumor progression according to RECIST v1.1 criteria or death from any cause, whichever occurred first. Safety was assessed based on the occurrence of treatment-related adverse events (TRAEs).
Statistical Methods
The anchored MAIC approach was applied to compare individual patient data (IPD) from ASTRUM-007 with aggregate data (AgD) derived from seven selected comparator trials.15,16 Matching weights were estimated using the Newton-Raphson optimization algorithm to balance the mean baseline characteristics of the ASTRUM-007 IPD with the published aggregate baseline characteristics from the comparator trials. Matching was performed on prespecified variables, and effective sample sizes (ESS) were calculated for both treatment arms after weighting. Indirect comparisons between the weighted ASTRUM-007 results and each of the seven comparator studies were conducted using the Bucher method.17 Baseline characteristics were summarized before and after weighting, and the anchored MAIC-adjusted HRs for OS and PFS were reported.
For subgroup analyses, because published trials did not report sufficient aggregate baseline characteristics within subgroups to support MAIC, a Bayesian network meta-analysis (NMA)18 was conducted to perform anchored unadjusted indirect comparisons across trials. The surface under the cumulative ranking curve (SUCRA) values and ranking probabilities were used to assess the relative treatment ranking among the candidate agents. All analyses were conducted using R (Version 4.5.2).
Results
Study Characteristics and Baseline Demographics
Eight pivotal phase 3 randomized controlled trials (RCTs) involving 4,702 patients were included in this comparative analysis. All trials enrolled patients with previously untreated, unresectable, locally advanced, recurrent, or metastatic ESCC. In the experimental arms, first-line PD-1/PD-L1 inhibitors were administered in combination with platinum-based doublet chemotherapy (paclitaxel-cisplatin or cisplatin-5-fluorouracil) and compared against the corresponding chemotherapy alone. Study characteristics and efficacy endpoint results are summarized in Table 1. ASTRUM‑007 (serplulimab plus cisplatin-5-fluorouracil) served as the index trial for all indirect comparisons.
Across trials, baseline characteristics were generally balanced. Male patients accounted for 78.8%-87.7% in treatment arms and 84.8%-88.3% in control arms. ECOG performance status 1 was reported in 53.3%-79.1% of patients in the treatment arms. Most patients had metastatic disease at baseline. Among trials reporting age group, approximately 30%-50% of participants were aged ≥65 years. Former or current smoking was reported in the five trials that provided smoking status. Key baseline characteristics are presented in Table 2.
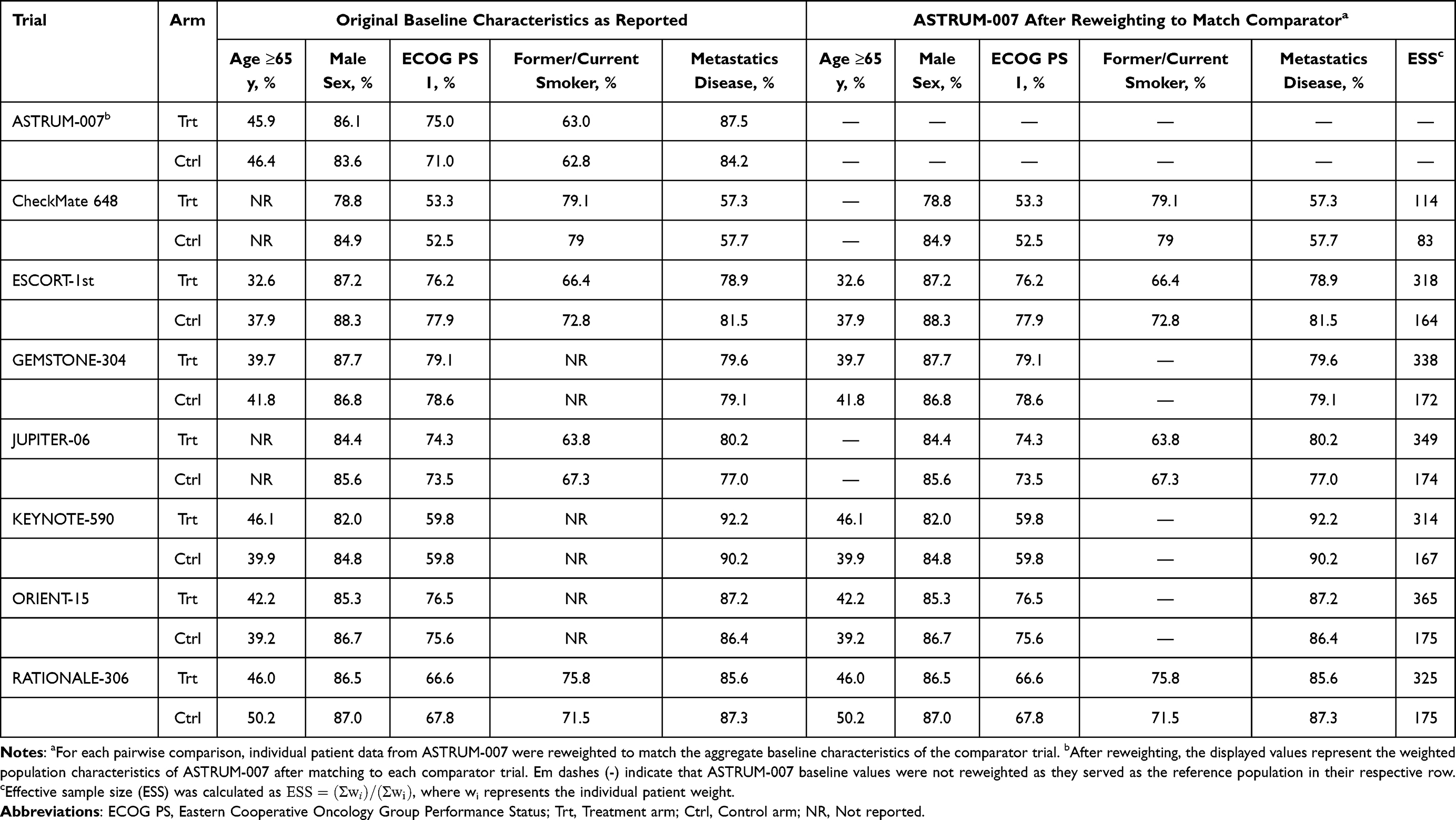 |
Table 2 Baseline Characteristics Before and After Reweighting ASTRUM-007 to Match Each Comparator Study |
Population-Adjusted Comparative Efficacy via Anchored MAIC
To adjust for cross-trial heterogeneity, anchored MAIC was conducted for each comparison. After weighting, the ESS for the ASTRUM‑007 serplulimab and chemotherapy arms ranged from 114 to 365 and 83 to 175, respectively, suggesting acceptable statistical precision and overlap between the reweighted populations (Table 2). The weighted baseline characteristics of ASTRUM‑007 were well balanced with those of each comparator trial.
Overall Survival
In the adjusted anchored MAIC analysis for OS, serplulimab demonstrated comparable efficacy to other first-line PD-1/PD-L1-based regimens, with a numerical survival advantage versus nivolumab (Figure 1A). Compared with nivolumab (CheckMate 648), serplulimab was associated with a 24% lower risk of death (adjusted HR, 0.76; 95% CI, 0.47–1.24), although the confidence interval crossed unity. Serplulimab demonstrated OS outcomes similar to those with camrelizumab (adjusted HR, 0.93; 95% CI, 0.70–1.24), pembrolizumab (adjusted HR, 0.93; 95% CI, 0.71–1.22), and sugemalimab (adjusted HR, 0.95; 95% CI, 0.69–1.31). Comparisons with sintilimab and toripalimab yielded point estimates close to 1.0 with overlapping confidence intervals, suggesting no meaningful difference in long-term survival. Overall, the pooled estimate was 0.98 (95% CI, 0.87–1.11) with no detectable heterogeneity (I2=0.0%), supporting robust cross-trial consistency.
 |
Figure 1 Adjusted Hazard Ratios for Efficacy Outcomes in Matching-Adjusted Indirect Comparison. Abbreviations: CI, confidence interval; ESS, effective sample sizes; HR, hazard ratio. Notes: Hazard ratios (HRs) and 95% CIs for overall survival (A) and progression-free survival (B). Individual patient data from ASTRUM-007 were reweighted to match aggregate baseline characteristics of comparator trials. HRs less than 1.0 favour serplulimab plus chemotherapy. |
Progression-Free Survival
In the anchored MAIC for PFS, serplulimab showed a favorable efficacy profile across the comparator landscape (Figure 1B). Serplulimab significantly reduced the risk of progression or death versus nivolumab (adjusted HR, 0.56; 95% CI, 0.33–0.96), corresponding to a 44% relative risk reduction in the weighted population. Point estimates also favored serplulimab versus pembrolizumab (adjusted HR, 0.83; 95% CI, 0.63–1.10), sugemalimab (adjusted HR, 0.86; 95% CI, 0.63–1.16), and tislelizumab (adjusted HR, 0.91; 95% CI, 0.67–1.23). Comparisons with toripalimab (adjusted HR, 0.97; 95% CI, 0.70–1.34) and sintilimab (adjusted HR, 1.01; 95% CI, 0.75–1.35) yielded near‑unity estimates with overlapping confidence intervals. Overall, the pooled HR was 0.91 (95% CI, 0.81–1.02) with no heterogeneity (I2=0.0%), supporting consistent PFS benefit across trials.
Efficacy Profiles in Key Subgroups via Bayesian Network Meta-Analysis
An NMA was conducted to compare treatments within prespecified clinically relevant subgroups, with ranking summarized using SUCRA.
Overall Survival by Subgroups
Serplulimab demonstrated generally consistent OS benefit versus chemotherapy across subgroups (Figures 2 and 3). In both age strata (<65 and ≥65 years), serplulimab (HR, ~0.70 vs chemotherapy; SUCRA, ~0.555 and 0.495) showed clinically meaningful benefit comparable to leading PD-1-based regimens.
 |
Figure 2 League Tables of Treatment Comparisons from Bayesian Network Meta-Analysis. Abbreviations: CF, cisplatin plus 5-fluorouracil; TP, paclitaxel plus cisplatin. Notes: Pairwise comparisons from Bayesian network meta-analysis, column treatments are compared with row treatments. Hazard ratios (HRs) with 95% credible intervals for overall survival (A, upper triangle) and progression-free survival (A, lower triangle), HR <1.0 indicates an efficacy benefit. Risk ratios for grade ≥3 treatment-related adverse events (B). Column treatments are compared with row treatments. RR < 1 indicates better tolerance. |
 |
Figure 3 Treatment Rankings for Efficacy and Safety Outcomes. Abbreviations: ECOG, Eastern Cooperative Oncology Group; OS, overall survival; PFS, progression‑free survival; TRAE, treatment‑related adverse event. Notes: Bayesian ranking profiles from the first to the last on improving the OS or PFS of the immunotherapies in the total population and the efficacy profiles of subgroups, or from the most likely to cause TRAEs and TRAEs of grades ≥3. The first rank shows the highest probabilities for improving OS or prolonging PFS or being the most likely to cause the AEs of grades ≥3. The last rank is on the contrary. |
Serplulimab showed greater efficacy in female patients and those with locally advanced disease. Among women, serplulimab (HR, 0.62; 95% CI, 0.45–0.87; SUCRA, 0.631) was ranked among the top regimens, with numerically better OS than sugemalimab and pembrolizumab and markedly better outcomes than nivolumab. In locally advanced disease, serplulimab was ranked first (alongside tislelizumab) and was associated with a marked reduction in mortality versus chemotherapy (HR, 0.47; 95% CI, 0.34–0.65; SUCRA, 0.730). In metastatic disease, serplulimab (HR, 0.75; 95% CI, 0.63–0.88) showed comparable benefit with the other PD-1/PD-L1 inhibitors. Subgroup-specific HRs and SUCRA values for OS are provided in Supplementary Table 1.
Progression-Free Survival by Subgroups
Serplulimab was consistently ranked among the most effective regimens for PFS across prespecified subgroups (Figures 2 and 3). In patients aged ≥65 years, serplulimab (HR, 0.54; 95% CI, 0.42–0.69; SUCRA, 0.613) showed a robust PFS benefit versus chemotherapy, with efficacy comparable to other leading PD-1 inhibitors.
Consistent with the OS findings, serplulimab conferred the greatest PFS benefit in women (HR, 0.36; 95% CI, 0.24–0.54; SUCRA, 0.790), where it ranked first among all evaluable regimens. According to disease status, serplulimab was associated with reduced progression risk in both locally advanced (HR, 0.68; 95% CI, 0.50–0.93) and metastatic disease (HR, 0.56; 95% CI, 0.46–0.68). Subgroup-specific HRs and SUCRA values for PFS are provided in Supplementary Table 2.
Safety Outcomes
Safety was evaluated using an NMA of TRAEs versus chemotherapy (Figure 3; Supplementary Table 3). Serplulimab showed a safety profile consistent with that for other PD-1 inhibitors. For all-grade TRAEs, serplulimab had no meaningful increase versus chemotherapy (risk ratio [RR], 1.01; 95% CI, 0.94–1.09; SUCRA, 0.497) and was comparable to pembrolizumab (SUCRA, 0.491), indicating no excess low-grade toxicity burden.
For grade 3–5 TRAEs, serplulimab showed an acceptable severe-toxicity profile (RR, 1.09; 95% CI, 0.73–1.63; SUCRA, 0.470) and was numerically more favorable than nivolumab (RR, 1.34; SUCRA, 0.153). Overall, the clinical benefits of serplulimab were not accompanied by a disproportionate increase in severe TRAEs.
Discussion
While immunotherapy plus chemotherapy is now established as the standard first-line treatment for locally advanced or metastatic ESCC, the optimal choice among available chemoimmunotherapy regimens remains unclear. In this study, we performed indirect comparison analyses of serplulimab versus seven other anti-PD-1/PD-L1 agents combined with chemotherapy in the first-line setting for ESCC. After matching, serplulimab plus chemotherapy was associated with a clinically meaningful improvement in PFS and OS outcomes comparable to those of other first-line PD-1/PD-L1 inhibitor-based regimens, while demonstrating a safety profile consistent with that for other PD-1 inhibitors. These findings suggest a favorable benefit-risk profile for serplulimab-based chemoimmunotherapy in this setting.
One important consideration in trial design for this indirect comparison is the heterogeneity in chemotherapy backbones across these trials. Cisplatin plus 5-fluorouracil is a commonly used first-line chemotherapy backbone for advanced ESCC. However, this regimen was adopted only in GEMSTONE-304, KEYNOTE-590, and CheckMate 648, whereas the other studies primarily employed paclitaxel plus cisplatin or allowed multiple chemotherapy options. Moreover, even among the three trials using cisplatin plus 5-fluorouracil, differences in dosing schedules were evident, with variations in per-cycle dose intensity and treatment duration. These discrepancies in chemotherapy regimens and administration schedules may have contributed to cross-trial heterogeneity. Nevertheless, existing retrospective analyses have suggested that there are no substantial differences in efficacy or safety outcomes between the two regimens.19 Another potential source of heterogeneity is that the ASTRUM-007 trial enrolled only patients from China, which may raise concerns regarding the generalizability of the findings. However, available evidence suggests that race is unlikely to be a major effect modifier, as clinically relevant differences in survival outcomes between Asian and non-Asian populations were not observed in CheckMate 648 or RATIONALE-306. In addition, ASTRUM-007 included only patients with PD-L1-positive ESCC (CPS ≥1). Importantly, PD-L1 expression level does not appear to be a key effect modifier in this setting, as comparable survival benefits across PD-L1 subgroups have been reported in JUPITER-06.
MAIC is an established approach that integrates IPD from one RCT with aggregated data from comparator trials, enabling adjustment for cross-trial differences in key population characteristics through matching and weighting. By statistically accounting for observed heterogeneity, this method facilitates clinically meaningful comparative effectiveness assessments when head-to-head randomized studies are not available. In this analysis, age, sex, ECOG performance status, smoking status, and disease status were selected for adjustment. The rationale for identifying these variables as prognostic factors and potential effect modifiers is as follows. Age is a well-established prognostic factor in oncology, as it is associated with greater comorbidity burden and reduced treatment tolerance, and it is routinely incorporated as a stratification factor in clinical trials. Sex is considered a potential effect modifier in chemoimmunotherapy, as clinically meaningful differences in survival outcomes between male and female patients were observed in the CheckMate-648 and JUPITER-06 trials. ECOG performance status is a recognized prognostic factor in oncology immunotherapy, with significant associations with treatment tolerability, immune competence, and survival outcomes.20 Furthermore, smoking may impair T cell-mediated immune responses, supporting its potential impact on immunotherapy outcomes in ESCC.21 In addition, distant metastatic disease may attenuate immunotherapy efficacy through mechanisms such as T-cell exhaustion and systemic immune suppression.22,23
Nevertheless, several key limitations have to be considered. First, extensive adjustment for multiple potential effect modifiers and prognostic factors can substantially reduce the ESS, which may in turn increase the uncertainty and variability of relative treatment effect estimates. Second, as with any indirect comparison of nonrandomized treatment groups, residual confounding may persist if relevant characteristics are unmeasured or unreported across trials.24 Although known differences were addressed through MAIC, this analysis relied on aggregated baseline information from the seven comparator trials; consequently, unmeasured, inconsistently defined, or unreported variables may have influenced the comparative results. Third, OS is influenced by local medical practices and subsequent treatments, and while MAIC adjusts for population characteristics, confounding related to post-progression therapy and other unobserved factors may remain.
Conclusion
This analysis provides comparative evidence to inform decision-making regarding the optimal first-line chemoimmunotherapy regimen for patients with locally advanced or metastatic ESCC. After adjusting for baseline differences, serplulimab in combination with chemotherapy demonstrated PFS and OS comparable to other first-line PD-1/PD-L1 inhibitor-based regimens and a safety profile consistent with that for other PD-1 inhibitors. Collectively, these findings support a favorable benefit-risk profile for serplulimab-based chemoimmunotherapy in this patient population.
Abbreviations
AgD, aggregate data; CI, confidence interval; CPS, combined positive score; ECOG, Eastern Cooperative Oncology Group; ESCC, esophageal squamous cell carcinoma; ESS, effective sample sizes; HR, hazard ratio; ICIs, immune checkpoint inhibitors; IPD, individual patient data; MAIC, matching‑adjusted indirect comparison; NMA, Bayesian network meta‑analysis; OS, overall survival; PD‑1/PD‑L1, programmed cell death‑1/programmed death‑ligand 1; PFS, progression‑free survival; RCT, randomized controlled trial; RECIST v1.1, Response Evaluation Criteria in Solid Tumors version 1.1; SUCRA, surface under the cumulative ranking curve; TRAE, treatment‑related adverse event.
Data Sharing Statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics Approval and Informed Consent
The ASTRUM-007 trial was approved by institutional review boards and conducted per the Declaration of Helsinki. All patients provided informed consent. This secondary analysis used de-identified data with sponsor permission; no additional ethics approval was required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Shanghai Henlius Biotech, Inc., the manufacturer of serplulimab and sponsor of the ASTRUM-007 trial. The sponsor participated in study design, data analysis, and manuscript preparation.
Disclosure
All authors are employees of Shanghai Henlius Biotech, Inc. The authors report no other conflicts of interest in this work.
References
1. Arnold M, Ferlay J, van Berge Henegouwen MI, Soerjomataram I. Global burden of oesophageal and gastric cancer by histology and subsite in 2018. Gut. 2020;69(9):1564–12. doi:10.1136/gutjnl-2020-321600
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Obermannová R, Alsina M, Cervantes A, et al. Oesophageal cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(10):992–1004. doi:10.1016/j.annonc.2022.07.003
4. Moehler M, Maderer A, Thuss-Patience PC, et al. Cisplatin and 5-fluorouracil with or without epidermal growth factor receptor inhibition panitumumab for patients with non-resectable, advanced or metastatic oesophageal squamous cell cancer: a prospective, open-label, randomised Phase III AIO/EORTC trial (POWER). Ann Oncol. 2020;31(2):228–235. doi:10.1016/j.annonc.2019.10.018
5. Hiramoto S, Kato K, Shoji H, et al. A retrospective analysis of 5-fluorouracil plus cisplatin as first-line chemotherapy in the recent treatment strategy for patients with metastatic or recurrent esophageal squamous cell carcinoma. Int J Clin Oncol. 2018;23(3):466–472. doi:10.1007/s10147-018-1239-x
6. Deboever N, Jones CM, Yamashita K, Ajani JA, Hofstetter WL. Advances in diagnosis and management of cancer of the esophagus. BMJ. 2024;385:e074962.
7. Doki Y, Ajani JA, Kato K, et al. Nivolumab combination therapy in advanced esophageal squamous-cell carcinoma. N Engl J Med. 2022;386(5):449–462. doi:10.1056/NEJMoa2111380
8. Sun J-M, Shen L, Shah MA, et al. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): a randomised, placebo-controlled, phase 3 study. Lancet. 2021;398(10302):759–771. doi:10.1016/S0140-6736(21)01234-4
9. Song Y, Zhang B, Xin D, et al. First-line serplulimab or placebo plus chemotherapy in PD-L1-positive esophageal squamous cell carcinoma: a randomized, double-blind phase 3 trial. Nat Med. 2023;29(2):473–482. doi:10.1038/s41591-022-02179-2
10. Xu J, Kato K, Raymond E, et al. Tislelizumab plus chemotherapy versus placebo plus chemotherapy as first-line treatment for advanced or metastatic oesophageal squamous cell carcinoma (RATIONALE-306): a global, randomised, placebo-controlled, phase 3 study. Lancet Oncol. 2023;24(5):483–495. doi:10.1016/S1470-2045(23)00108-0
11. Li J, Chen Z, Bai Y, et al. First-line sugemalimab with chemotherapy for advanced esophageal squamous cell carcinoma: a randomized phase 3 study. Nat Med. 2024;30(3):740–748. doi:10.1038/s41591-024-02797-y
12. Luo H, Lu J, Bai Y, et al. Effect of camrelizumab vs placebo added to chemotherapy on survival and progression-free survival in patients with advanced or metastatic esophageal squamous cell carcinoma: the ESCORT-1st randomized clinical trial. JAMA. 2021;326(10):916–925. doi:10.1001/jama.2021.12836
13. Wang Z-X, Cui C, Yao J, et al. Toripalimab plus chemotherapy in treatment-naïve, advanced esophageal squamous cell carcinoma (Jupiter-06): a multi-center phase 3 trial. Cancer Cell. 2022;40(3):277–288.e3. doi:10.1016/j.ccell.2022.02.007
14. Lu Z, Wang J, Shu Y, et al. Sintilimab versus placebo in combination with chemotherapy as first line treatment for locally advanced or metastatic oesophageal squamous cell carcinoma (ORIENT-15): multicentre, randomised, double blind, phase 3 trial. BMJ. 2022;377:e068714. doi:10.1136/bmj-2021-068714
15. Signorovitch JE, Sikirica V, Erder MH, et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health. 2012;15(6):940–947. doi:10.1016/j.jval.2012.05.004
16. Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. Methods for population-adjusted indirect comparisons in health technology appraisal. Med Decis Making. 2018;38(2):200–211. doi:10.1177/0272989X17725740
17. Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J Clin Epidemiol. 1997;50(6):683–691. doi:10.1016/S0895-4356(97)00049-8
18. Shim SR, Kim S-J, Lee J, Rücker G. Network meta-analysis: application and practice using R software. Epidemiol Health. 2019;41:e2019013. doi:10.4178/epih.e2019013
19. Liu Y, Ren Z, Yuan L, et al. Paclitaxel plus cisplatin vs. 5-fluorouracil plus cisplatin as first-line treatment for patients with advanced squamous cell esophageal cancer. Am J Cancer Res. 2016;6(10):2345–2350.
20. Gao L, Tang L, Peng J, Hu Z, Yang J, Liu B. PD-1 inhibitor combined with chemotherapy for first-line treatment of esophageal squamous cell carcinoma patients with distant metastasis: a real-world retrospective study. Front Immunol. 2024;15:1353445. doi:10.3389/fimmu.2024.1353445
21. Wang G, Pan C, Cao K, et al. Impacts of cigarette smoking on the tumor immune microenvironment in esophageal squamous cell carcinoma. J Cancer. 2022;13(2):413–425. doi:10.7150/jca.65400
22. Yu J, Green MD, Li S, et al. Liver metastasis restrains immunotherapy efficacy via macrophage-mediated T cell elimination. Nat Med. 2021;27(1):152–164. doi:10.1038/s41591-020-1131-x
23. Jiang C, Zhang Z-H, Li J-X. Consideration on immunotherapy of liver metastases of malignant tumors. World J Gastrointest Surg. 2024;16(8):2374–2381. doi:10.4240/wjgs.v16.i8.2374
24. Signorovitch JE, Wu EQ, Yu AP, et al. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with Adalimumab or etanercept. Pharmacoeconomics. 2010;28(10):935–945. doi:10.2165/11538370-000000000-00000
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.