Back to Journals » Orthopedic Research and Reviews » Volume 17
First Clinical Experience with Robotic-Assisted Total Knee Arthroplasty in Indonesia: Early Results and Comparison with Global Evidence
Authors Yanuar A ![]()
Received 20 August 2025
Accepted for publication 18 December 2025
Published 22 December 2025 Volume 2025:17 Pages 593—600
DOI https://doi.org/10.2147/ORR.S561904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Andre Yanuar
Consultant Orthopaedic Surgeon Santo Borromeus Hospital, Bandung, Indonesia
Correspondence: Andre Yanuar, Santo Borromeus Hospital, Bandung, Indonesia, Email [email protected]
Objective: This study evaluated early clinical and radiographic outcomes of robotic-assisted total knee arthroplasty (RA-TKA) in Indonesia using the ROSA® Knee System, hypothesizing that outcomes would be comparable to high-income countries.
Methods: A retrospective observational study was conducted including patients undergoing primary RA-TKA between July 2024 and July 2025. Perioperative variables, radiographic alignment, postoperative mobilization, and patient satisfaction were assessed. Outcomes were compared qualitatively with published benchmarks. All procedures were performed by a single surgeon.
Results: A total of 40 patients (44 knees) were included. Median operative time was 110 minutes. Standing long-leg radiographs demonstrated mechanical alignment within ± 3° of neutral in all knees. Median time to ambulation was 6 hours (unilateral) and 19.5 hours (bilateral). No intraoperative complications occurred. Overall satisfaction was 95%. Outcomes were consistent with reports from high-income countries.
Conclusion: RA-TKA can be safely and effectively implemented within a developing healthcare system, achieving alignment accuracy, mobilization times, and satisfaction rates comparable to global benchmarks.
Keywords: robotic-assisted total knee arthroplasty, Indonesia, arthroplasty outcomes, alignment accuracy, early mobilization, patient satisfaction, developing healthcare systems
Introduction
Robotic-assisted total knee arthroplasty (RA-TKA) has gained global acceptance due to its ability to enhance alignment accuracy and reproducibility. Recent studies have demonstrated reduced complications, and shorter hospital stays with RA-TKA, reinforcing its adoption.1,2 The effectiveness of RA-TKA in improving component positioning and mechanical alignment has been demonstrated in several recent studies, supporting its growing adoption in both academic and private settings.3,4
Our institution was the first in Indonesia to acquire and implement the Robotic-Assisted Total Knee Arthroplasty (RA-TKA), becoming the pioneer of robotic-assisted joint replacement surgery in the country. TKA remains the primary surgical option for individuals with advanced-stage knee osteoarthritis where conservative treatment is no longer effective. While conventional TKA techniques have matured, challenges remain in achieving optimal alignment and component positioning.
Despite its growth in high-income countries, RA-TKA remains limited in developing healthcare systems. The present institution was the first center in Indonesia to implement the ROSA® Knee System. Considering the increasing demand for precise and reproducible TKA outcomes, evaluating the feasibility and early results of robotic systems in resource-limited settings is essential.
Hypothesis: RA-TKA performed in a developing healthcare system would achieve clinical and radiographic outcomes comparable to high-income countries.
Purpose: To evaluate early outcomes following the first year of RA-TKA implementation in Indonesia and compare them with established international evidence.
Methodology
Study Design and Setting
A retrospective observational study was conducted on patients undergoing primary RA-TKA between July 2024 and July 2025. All surgeries were performed at our institution, a secondary private hospital in Bandung, Indonesia. This study complies with the Declaration of Helsinki and received Institutional Review Board approval (Approval No. 015/KEPK/VIII/2025). Written informed consent was obtained from all participants prior to inclusion. In addition to a descriptive analysis of clinical outcomes, a qualitative comparison of our results with selected studies from high-income countries reporting RA-TKA outcomes was conducted. The purpose was to evaluate the comparability of alignment accuracy, patient satisfaction, and complication rates in our setting versus established global benchmarks. All procedures in this study were performed by a single high-volume surgeon.
Patient Selection
Inclusion criteria consisted of primary knee osteoarthritis requiring TKA. Exclusion criteria included inflammatory arthritis, previous knee surgery, post-traumatic deformity, active or prior infection, or tumor-related pathology. A total of 40 patients (44 knees) were included.
Surgical Technique
All procedures were performed using the ROSA® Knee System. A midvastus approach was used. Bone resections were planned to achieve mechanical alignment with permissible adjustments within ±2° based on adjusted mechanical alignment principles. Femoral and tibial trackers were placed following manufacturer guidelines.
Precut balancing plans were established after assessing joint motion under manual varus and valgus stress throughout the range of motion. These data were incorporated into the ROSA® system’s balancing algorithm to aid in component alignment and gap management.Bone resections of both femur and tibia were intended to be perpendicular to their respective mechanical axes (0° varus/valgus). However, if soft tissue tension suggested excessive releases would be required, the femoral component alignment was adjusted within a 2° varus or valgus window to preserve stability with minimal soft tissue disruption according to the principle of Adjusted Mechanical Alignment (AMA).
Balancing began in flexion by modifying the femoral rotation based on real-time gap measurements. The goal was to ensure symmetrical medial and lateral joint spaces of at least 19 mm in flexion before final femoral cuts were made, irrespective of conventional anatomic references such as the epicondylar or posterior condylar axis.
In extension, the aim was to provide at least 19 mm of space in the medial compartment for valgus knees or the lateral compartment for varus knees (Figure 1). The tighter compartment was accepted at its natural state, with final releases deferred until after bone resections and residual osteophyte removal. Extension gap symmetry was reassessed using spacer blocks.
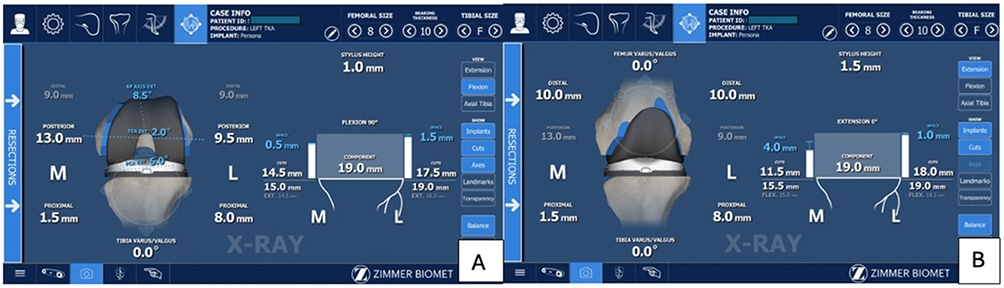 |
Figure 1 (A) The goal was to ensure symmetrical medial and lateral joint spaces of at least 19 mm in flexion before final femoral cuts were made. (B) In extension, the aim was to provide at least 19 mm of space in the lateral compartment for varus knees. |
If the medial compartment remained overly tight, a posteromedial release was performed. For lateral tightness, a fenestrated posterolateral capsular release, with or without posterior cruciate ligament (PCL) release, was performed based on sagittal plane balance and tibial lift-off evaluation. Final balancing was confirmed during trial reduction. Any required additional releases were completed before implanting the definitive prosthesis. After implantation, final gap balancing was reassessed across the entire range of motion.
Radiographic Assessment
Mechanical axis alignment was evaluated using pre- and postoperative standing long-leg radiographs. Measurements were performed by trained musculoskeletal radiologist, with postoperative alignment classified as acceptable if within ±3° of neutral mechanical axis.
Perioperative Management
All patients were managed under an Enhanced Recovery After Surgery (ERAS) protocol. Postoperative analgesia included a continuous adductor canal block and an IPACK (Infiltration between the Popliteal Artery and Capsule of the Knee) block, administered by the anesthesia team immediately following surgery.
Patients were mobilized within 6 hours postoperatively for unilateral cases, or the next day for bilateral cases, according to the institution’s physiotherapy protocol. All patients were allowed full weight bearing as tolerated and discharged once independently ambulant with walking aids.
Outcome Assessment
Perioperative variables included operative time, time to ambulation, and length of stay. Postoperative outcomes included mechanical alignment, complications, and patient satisfaction, assessed via direct structured questioning (“Are you satisfied with the result of your knee replacement surgery?”). Follow-up time ranged from 1 to 12 months postoperatively, depending on each patient’s date of surgery. Satisfaction responses were recorded as either “Satisfied” or “Not satisfied”. Given the variability in follow up timing, outcomes reflect a cross-sectional assessment of early satisfaction within the first postoperative year.
Statistical Analysis
Descriptive statistics were performed. Fisher’s exact test was used to explore associations between categorical variables and dissatisfaction. A p-value < 0.05 was considered statistically significant.
Results
A total of 40 patients (44 knees) underwent RA-TKA in this study. The demographic characteristics of the patients, including gender and age, are presented in Table 1. The median operative time was 110 minutes (IQR 100–120). The median hospital stay was 3 days (IQR 3–3) for unilateral procedures and 5 days (IQR 5–6) for bilateral procedures. The median time to ambulation was 6 hours (IQR 6–6) for unilateral cases and 19.5 hours (IQR 18.75–27.0) for bilateral cases. A postoperative mechanical alignment within 3° of neutral was achieved in 100% of knees. Overall patient satisfaction was 95%, with only two patients reported as not satisfied at final follow-up. 30 patients (75%) were female. Four patients (10%) underwent simultaneous bilateral procedures. No intraoperative or major postoperative complications were recorded. Thirty-eight patients (95%) reported being satisfied during follow-up. A correlation analysis was conducted to evaluate whether age, gender, implant type, or laterality (unilateral vs bilateral) was associated with patient dissatisfaction. Statistical testing showed no significant relationship between dissatisfaction and age (p = 1.000) and gender (p = 1.000). Whether the knees were operated sequentially or bilaterally did not influence patient satisfaction, as shown in Table 2 (p = 0.192). Likewise, the type of implant (Persona Medial Congruent, Persona Posterior Stabilized, Nexgen Cruciate Retaining, and Nexgen Posterior Stabilized) demonstrated no significant effect on patient satisfaction, as illustrated in Table 3 (p = 0.069).
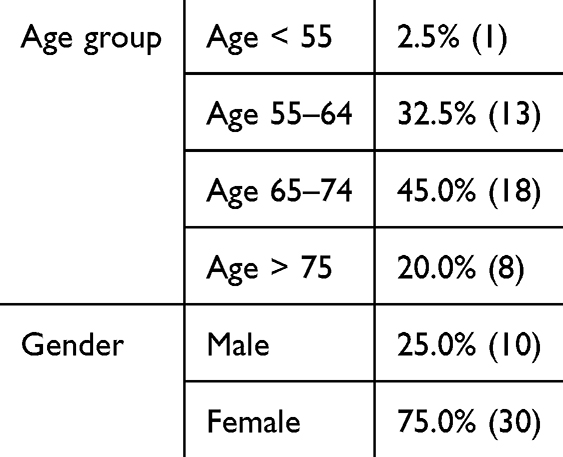 |
Table 1 Demography of Patients Included in the Study |
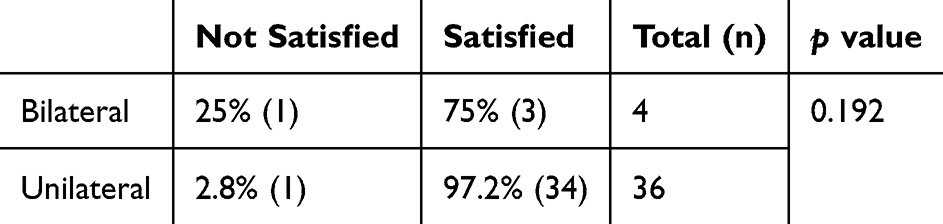 |
Table 2 Outcome of Surgery |
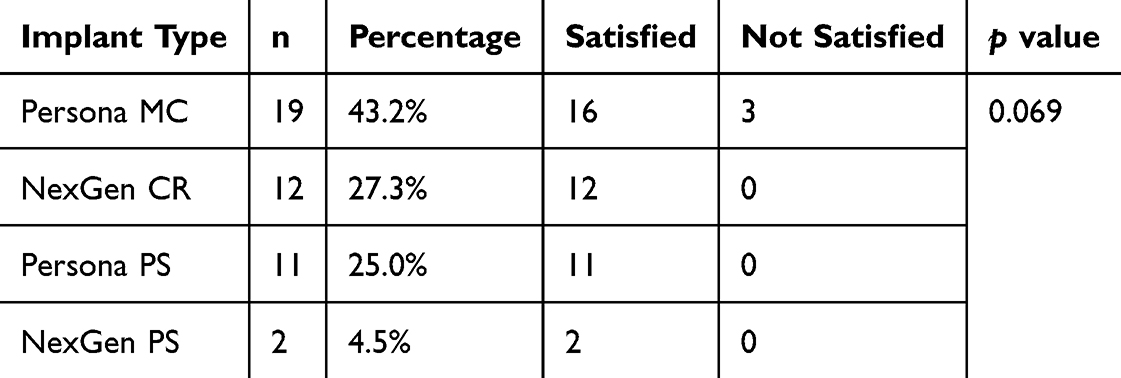 |
Table 3 Implant Type and Patient Satisfaction |
Based on the follow-up period, 15 patients (37.5%) were assessed at less than 6 months postoperatively, while 25 patients (62.5%) had follow-up durations greater than 6 months. Among patients with shorter follow-up (<6 months), 100% (15/15) reported satisfaction with the surgical outcome. In the >6 months group, 92% (23/25) were satisfied. Statistical analysis using Fisher’s Exact Test revealed no significant difference in satisfaction between the two groups (p = 0.519).
Discussion
This study represents the first reported clinical experience using the ROSA® Knee System in Indonesia. The findings demonstrate high alignment accuracy, rapid ambulation, and high patient satisfaction, consistent with RA-TKA results reported internationally.
Multiple recent analyses have shown that robotic-assisted TKA improves radiologic precision, reduces complications, and may enhance patient-reported outcomes compared with conventional TKA.1,2 Our findings align with these reports, including studies demonstrating improved early function, radiographic accuracy, and survivorship in robotic cohorts.
In the broader context of RA-TKA, several platforms have gained global prominence, each with unique advantages and limitations. The ROSA® system (Zimmer Biomet) is image-based but does not require preoperative CT scans, allowing intraoperative registration and can be used also in imageless modes. In contrast, the MAKO® system (Stryker) relies on preoperative CT-based planning and haptic feedback, offering highly precise bone preparation but at the cost of higher preoperative imaging burden and longer setup time.4 The NAVIO® system (Smith & Nephew), while imageless, requires extensive intraoperative mapping and has been associated with longer learning curves.5 Other systems like VELYS™ (Depuy Synthes) and OMNIBotics® (Corin) offer unique navigation or ligament balancing tools but are less widely adopted globally.6 Each system presents trade-offs between cost, learning curve, preoperative imaging needs, and real-time intraoperative guidance. Studies have shown that while alignment accuracy is generally comparable across platforms, surgeon familiarity and institutional support play critical roles in optimizing outcomes.4,7
Among robotic systems, the MAKO® (Stryker) platform has been the most widely studied and adopted globally. It utilizes a CT-based preoperative planning protocol combined with real-time intraoperative haptic guidance. Multiple studies have reported that MAKO®-assisted TKA improves the accuracy of implant positioning and mechanical alignment compared to manual techniques. Furthermore, patients undergoing MAKO®-assisted procedures have demonstrated reduced postoperative pain, shorter hospital stays, and earlier functional recovery in several trials.8 However, drawbacks include the requirement for preoperative CT scans, increased cost, and a notable learning curve for surgical teams. When compared with imageless systems like ROSA®, clinical outcomes in terms of alignment and early patient satisfaction have been reported to be comparable in recent multicenter analyses.9
Based on the author’s experience, the learning curve associated with adopting the ROSA® Knee system was not excessively steep. The procedural flow can be aligned with the surgeon’s established habits in conventional total knee arthroplasty, minimizing disruptions during the transition to robotic assistance. Additionally, the robotization of the jigs significantly enhances intraoperative control, particularly during bone resection, offering precision without overly complicating the workflow. However, adaptation is required during specific stages of the procedure, including anatomical marker registration, preoperative planning for ligament balancing, and soft tissue assessment. These steps, while initially demanding attention to detail, become more intuitive with experience. Notably, the adaptation period was marked by operative times approaching standard procedures after approximately eight cases.
Our results support that RA- TKA with ROSA® can deliver high alignment accuracy and early functional recovery. These findings are consistent with recent meta analysis by Klincke et al, which demonstrated superior radiologic outcomes but comparable early clinical outcomes for RA-TKA compared with covnetional TKA.10
The use of midvastus approach, adjusted mechanical alignment combined with ERAS protocols including regional anesthesia allowed for early ambulation and short hospital stay. The adjusted mechanical alignment technique helped avoid extensive soft tissue releases and may have contributed to the high satisfaction rates. This aligns with findings from Selvanathan et al, who advocate for individualized satisfaction metrics rather than relying on broad scoring systems.
Similar to our findings, a recent retrospective study from Switzerland comparing ROSA®-assisted TKA with conventional techniques (n ≈ 55 per group) demonstrated comparable radiographic alignment accuracy—including coronal and sagittal planes—but noted significantly higher Oxford Knee Scores (OKS) at 6 months in the ROSA® group, despite slightly longer operative times and blood loss.3 In a dual-robot comparison from Japan, involving 48 ROSA® versus 40 NAVIO® cases, both systems achieved excellent early radiographic accuracy and similar clinical outcomes at 1 year. Notably, ROSA® showed slightly better symptom scores on the Knee Society Score, underscoring its functional advantages.11
A recent systematic review of four ROSA®-assisted TKA studies reported consistent improvements in early (<1 year) functional outcomes compared to traditional TKA, despite heterogeneity in protocols and alignment strategies.12
Meanwhile, an ongoing RCT in the Netherlands compares ROSA®-based inverse kinematic alignment to conventional alignment strategies, highlighting the technology’s ability to personalize surgical plans.13
These international data resonate with our early results showing high technical precision (100% within ±3°), quick recovery, and high satisfaction. The slightly longer operative times observed in our study are comparable to global ROSA® benchmarks (The median operative time was 110 minutes). Importantly, while various alignment strategies—like inverse kinematic alignment—are under investigation abroad, our use of adjusted mechanical alignment appears to deliver equally robust early outcomes.
Our reported satisfaction rate of 95% and excellent alignment (mean Hip Knee Ankle angle of 0.2°) reflects the reproducibility of robotic precision. For instance, Selvanathan et al in Australia reported a 95% overall satisfaction and 93% outcome satisfaction at one year post-ROSA® Assisted TKA among 175 patients.14 In contrast to the findings of Selvanathan et al, who reported a greater tendency for patient dissatisfaction among those undergoing bilateral TKA simultaneously our study did not demonstrate a statistically significant difference in satisfaction levels between unilateral and bilateral TKA groups (p = 0.192). This suggests that, under standardized surgical protocols and multidisciplinary team preparation, bilateral procedures can achieve outcomes comparable to unilateral cases. These findings support the feasibility and reliability of bilateral robotic-assisted TKA when performed with consistent technique and perioperative care.
Additionally, comparative studies between robotics system (ROSA® vs NAVIO®) showed equivalent early functional outcomes and component placement accuracy at one year.11 These consistencies across diverse setting reinforce the conclusion that, with adequate resources and multidisciplinary expertise, RA- TKA in Indonesia can deliver outcomes comparable to established international standards.
The implant brands used in this study were Persona and NexGen (Zimmer Biomet), with selection based on patient preference. The choice between Posterior-Stabilized (PS), Cruciate-Retaining (CR), or Medial Congruent (MC) designs was determined by the condition of the Posterior Cruciate Ligament (PCL) and the need to achieve optimal knee joint balancing. No statistically significant association was observed between implant type and patient satisfaction. While all cases of dissatisfaction occurred among patients who received the Persona MC implant, statistical analysis using Fisher’s Exact Test yielded a p-value of 0.069, indicating a non-significant trend. Although medial congruent (MC) designs—such as the Persona MC implant—are often associated in the literature with higher rates of patient satisfaction and improved postoperative function, our study found that all cases of dissatisfaction occurred in patients implanted with Persona MC.
For instance, a cohort of 327 knees using various bearing types including MC, CR, and PS showed that MC knees were associated with significantly higher rates of “very satisfied” outcomes and fewer dissatisfied patients compared to CR designs (92.6% vs 81.5%, p = 0.04).15 Similarly, systematic review data have consistently reported good survivorship and comparable or better clinical outcomes with MC implants in short- to mid-term follow-up cohorts.16 In contrast, our clinical series—despite achieving excellent alignment and early mobilization—showed that all dissatisfied knees were associated with Persona MC. These findings suggest that in our setting, the expected benefits of MC bearing design may not directly translate to patient satisfaction, possibly due to factors such as surgical execution variables, soft-tissue balancing nuances, or patient expectation mismatches. Larger-scale, prospective studies would be valuable to further investigate this unexpected deviation.
In this study, patient satisfaction was assessed through a direct question regarding their perceived outcome rather than through standardized scoring system. This pragmatic approach reflect the real-word clinical setting in which time and resource limitations made comprehensive patient-reported outcome measures (PROMs) less feasible. In addition, there is currently no universally accepted gold standard for measuring PROMs in total knee arthroplasty. Various PROMs such as KOOS (Knee injury and Osteoarthritis Outcome Score), WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index), and Oxford Knee Score exist, yet they each have limitations in terms of complexity, cultural adaptation, and sensitivity to individual satisfaction. Moreover, direct satisfaction queries may better capture patient-centered impressions, which are not always reflected in formal scores.
One of the methodological considerations in this study was the variability in the postoperative follow-up period, which ranged from 1 to 12 months. While this heterogeneity might raise concerns about consistency in patient-reported outcomes, our analysis revealed no significant difference in satisfaction levels between patients assessed at less than 6 months and those with longer follow-up durations (p = 0.519). This suggests that patient-perceived satisfaction following robotic-assisted TKA may stabilize early in the postoperative period and remain consistent over time. Similar findings have been reported in previous studies, where improvements in pain, mobility, and functional outcomes tend to plateau within the first 3 to 6 months after surgery. Therefore, although longer follow-up is ideal for assessing durability and long-term outcomes, the early postoperative period may be sufficient to evaluate primary endpoints related to patient satisfaction in TKA.
Limitations
This study has several limitations;
First, the retrospective design and relatively small sample size limit the generalizability of our findings. The absence of a control group (eg, conventional TKA) prevents direct comparison of outcomes.
Second, patient satisfaction was assessed using a single binary question, which may not capture nuanced perceptions of postoperative recovery or function. While this approach has precedent in the literature, incorporating validated scoring systems such as the Oxford Knee Score or the Knee Society Score in future studies would provide more comprehensive outcome assessment.
Third, follow-up duration was limited to early outcomes (up to 12 months), and long-term implant performance and survivorship remain unknown.
Fourth, postoperative outcomes were assessed at varying time points, with some patients followed for only one month and others up to twelve months. This heterogeneity may influence satisfaction responses and limits the ability to draw time-specific conclusions.
Lastly, the study was conducted at a single private institution, which may not reflect practices or outcomes in other settings within Indonesia or comparable developing healthcare systems.
Conclusion
RA-TKA using the ROSA® Knee System can be safely implemented in a developing healthcare environment, producing alignment accuracy, early mobilization, and satisfaction rates comparable to international benchmarks. These results support broader adoption of robotic arthroplasty where resources and training allow. Larger controlled studies with long-term outcomes are warranted.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Maman D, Laver L, Becker R, Mahamid A, Berkovich Y. Robotic‐assisted total knee arthroplasty reduces postoperative complications and length of stay without increased cost compared to navigation‐guided techniques: a national analysis. Knee Surg Sports Traumatol Arthrosc. 2025;33(1):336–342. doi:10.1002/ksa.12348
2. Maman D, Laver L, Becker R, et al. Trends and epidemiology in robotic‐assisted total knee arthroplasty: reduced complications and shorter hospital stays. Knee Surg Sports Traumatol Arthrosc. 2024;32(12):3281–3288. doi:10.1002/ksa.12353
3. Hax J, Leuthard L, Baumann G, Preiss S, Stadelmann VA, Worlicek M. Comparable results in total knee arthroplasty using the ROSA knee system versus the conventional technique: a retrospective propensity‐matched cohort study. Knee Surg Sports Traumatol Arthrosc. 2024;32(12):3239–3251. doi:10.1002/ksa.12330
4. Kayani B, Konan S, Tahmassebi J, Pietrzak JRT, Haddad FS. Robotic-arm assisted total knee arthroplasty is associated with improved early functional recovery and reduced time to hospital discharge compared with conventional jig-based total knee arthroplasty. Bone Joint J. 2018;100-B(7):930–937. doi:10.1302/0301-620X.100B7.BJJ-2017-1449.R1
5. Batailler C, Swan J, Marinier ES, Servien E, Lustig S. New technologies in knee arthroplasty: current concepts. J Clin Med. 2020;10(1):47. doi:10.3390/jcm10010047
6. Sodhi N, Khlopas A, Piuzzi N, et al. The learning curve associated with robotic total knee arthroplasty. J Knee Surg. 2018;31(01):017–021. doi:10.1055/s-0037-1608809
7. Clement ND, MacDonald D, Simpson AHRW. The minimal clinically important difference in the oxford knee score and short form 12 score after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2014;22(8):1933–1939. doi:10.1007/s00167-013-2776-5
8. Mart J-PS, Goh EL. The current state of robotics in total knee arthroplasty. EFORT Open Rev. 2021;6(4):270–279. doi:10.1302/2058-5241.6.200052
9. Rajgor HD, Mayne A, Munasinghe C, et al. Mako versus ROSA: comparing surgical accuracy in robotic total knee arthroplasty. J Robot Surg. 2024;18(1):33. doi:10.1007/s11701-023-01786-6
10. Klincke V, Huyghe R, Vermue H, Martens M, Victor J. Robot‐assisted total knee arthroplasty demonstrates superior radiological but comparable clinical outcomes compared to conventional techniques: a meta‐analysis of prospective studies. Knee Surg Sports Traumatol Arthrosc. 2025. doi:10.1002/ksa.70007
11. Hasegawa M, Tone S, Naito Y, Sudo A. Comparison of accuracy and early outcomes in robotic total knee arthroplasty using NAVIO and ROSA. Sci Rep. 2024;14(1):3192. doi:10.1038/s41598-024-53789-4
12. Demirtas Y, Emet A, Ayik G, Cakmak G, Aksahin E, Celebi L. A novel robot-assisted knee arthroplasty system (ROSA) and 1-year outcome: a single center experience. Medicine. 2023;102(42):e35710. doi:10.1097/MD.0000000000035710
13. Eijking HM, Dorling IM, van Haaren EH, et al. Image-based robotic (ROSA® knee system) total knee arthroplasty with inverse kinematic alignment compared to conventional total knee arthroplasty. J Orthop Surg Res. 2025;20(1):47. doi:10.1186/s13018-024-05427-y
14. Selvanathan N, Ayeni FE, Sorial R. Is 80% satisfaction still the expectation in modern TKA mechanically aligned with robot assist? We think not. J Robot Surg. 2024;18(1):137. doi:10.1007/s11701-024-01888-9
15. Frye BM, Patton C, Kinney JA, Murphy TR, Klein AE, Dietz MJ. A medial congruent polyethylene offers satisfactory early outcomes and patient satisfaction in total knee arthroplasty. Arthroplast Today. 2021;7:243–249.e0. doi:10.1016/j.artd.2020.11.003
16. Romano F, Rossi R, Cottino U, Bruzzone M, Pirato F, Rosso F. Medial CONGRUENT AND MEDIAL PIVOT INSERTS IN TOTAL KNEE ARTHROPLASTY: A SCOPING REVIEw. Medicina. 2025;61(5):844. doi:10.3390/medicina61050844
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.