Back to Journals » Journal of Inflammation Research » Volume 19
Fire Needling Acupuncture Reduces Neutrophil Extracellular Traps (NETs) Formation and Inhibits TLR4/NF-κB/LCN2 Pathway in Psoriasis-Like Skin Lesions
Authors Wang Q ![]() , Wei J, Wang X, Yuan F, Sun J
, Wei J, Wang X, Yuan F, Sun J
Received 29 October 2025
Accepted for publication 5 March 2026
Published 20 March 2026 Volume 2026:19 569462
DOI https://doi.org/10.2147/JIR.S569462
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Anish R. Maskey
Qun Wang,* Jiangyan Wei,* Xin Wang,* Fang Yuan, Jingqing Sun
Department of Acupuncture and Moxibustion, Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing Key Laboratory of Acupuncture Neuromodulation, Beijing, 100010, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingqing Sun, Department of Acupuncture and Moxibustion, Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing Key Laboratory of Acupuncture Neuromodulation, 23 Meishuguan Back Street, Dongcheng District, Beijing, 100010, People’s Republic of China, Email [email protected]
Background: Psoriasis is a common chronic inflammatory skin disease with unclear pathogenesis and limited treatment. Fire needling acupuncture is a distinctive acupuncture technique that involves the rapid insertion of red-hot needles into skin lesions or acupoints. It has been shown to exert anti-inflammatory and immunomodulatory effects and to effectively alleviate the clinical symptoms of psoriasis. This study aims to explore the underlying mechanisms of fire needling acupuncture in the treatment of psoriasis.
Methods: Imiquimod was used to induce the psoriasis-like mouse model, and five groups were established: Control, Imiquimod (IMQ), IMQ + Methotrexate, IMQ + Fire needling acupuncture, and IMQ + Cl-amidine. Skin lesion severity and epidermal thickness were evaluated using the Psoriasis Area and Severity Index (PASI) and hematoxylin and eosin (H&E) staining. The levels of inflammatory cytokines (IL-23, IL-17, TNF-α, and IL-1β) in skin lesions were quantified by enzyme-linked immunosorbent assay (ELISA). The expression of epidermal proliferation and differentiation markers (Ki67 and K10), neutrophil surface marker (Ly6G), and neutrophil extracellular traps (NETs)-associated markers (MPO and Cit-H3) were evaluated by immunofluorescence and immunohistochemistry. In addition, the expression levels of TLR4, MyD88, NF-κB, p-NF-κB, and LCN2 in epidermis were quantified by Western blot analysis.
Results: Fire needling acupuncture significantly reduced PASI scores, epidermal thickness, and the levels of IL-23, IL-17, TNF-α, and IL-1β in psoriasis-like lesions. It also decreased Ki67 expression while increasing K10 expression in the epidermis. Moreover, the expression of Ly6G, MPO, and Cit-H3 in the lesions was reduced, and the protein levels of TLR4, MyD88, p-NF-κB, and LCN2 were downregulated in the epidermis after fire needling acupuncture treatment. Comparable effects were observed with methotrexate and Cl-amidine.
Conclusion: Fire needling acupuncture effectively improves skin lesions, suppresses abnormal keratinocyte proliferation and differentiation, and alleviates local inflammation in imiquimod-induced psoriasis-like mice. These therapeutic effects may be attributed to reduced neutrophil infiltration and NETs formation, as well as inhibition of TLR4/MyD88/NF-κB/LCN2 pathway.
Keywords: fire needling acupuncture, psoriasis, neutrophil extracellular traps, NETs, toll-like receptor 4, TLR4, nuclear factor-kappa B, NF-κB, lipocalin-2, LCN2
Introduction
Psoriasis is an immune-mediated chronic inflammatory skin disease affecting over 60 million people worldwide.1 Due to its chronic and recurrent nature, patients suffer long-term distress. This burden is further aggravated by the stigma of visible psoriatic lesions, which greatly impairs their quality of life.2 Currently, biologic therapies have achieved breakthroughs in the clinical management of psoriasis,3 but challenges such as high costs, drug resistance, adverse effects, variable individual responses, and high recurrence rates persist.4,5 Therefore, exploring new, safe, and effective treatment strategies remains a priority in psoriasis research.
Fire needling acupuncture is a specialized acupuncture technique that involves heating needles (such as filiform needles) until red-hot and rapidly inserting them into affected areas or acupoints to treat diseases.6 It has been used in China for centuries and has shown favourable efficacy in a variety of dermatological, immune, and pain conditions, including psoriasis,7 acne,8 vitiligo,9 knee osteoarthritis,10 and cancer pain.11 The most frequently reported adverse reactions are transient pain and small superficial burn marks at the needling sites, which usually heal within 1–2 weeks without permanent scarring.12,13 Evidence shows that fire needling acupuncture is both effective and safe in improving psoriasis, including alleviating skin lesions, reducing pruritus, and decreasing recurrence.7,14–16 However, its basic research remains limited, and unclear mechanisms hinder its broader application and development. Only a few studies have confirmed its regulatory effects on NF-κB pathway, macrophages, or T cells in various inflammatory disease models,17–19 demonstrating its ability to modulate immunity and reduce inflammation. Notably, fire needling acupuncture exhibits superior therapeutic effects when applied at acupoints rather than at local skin lesions,20 with Quchi (LI11) and Zusanli (ST36) being two of the most commonly used acupoints for psoriasis treatment.21 Building on these, this study further investigates the therapeutic targets of fire needling acupuncture in psoriasis.
NETosis, a representative behavior of neutrophil, is a unique form of cell death. In the process, chromatin decondenses and is released extracellularly, with various cytoplasmic enzymes and antimicrobial peptides adhering to the decondensed chromatin structure to form a web-like complex known as neutrophil extracellular traps (NETs).22 In psoriasis patients, NETs are increased in skin lesions, and the number of neutrophils undergoing NETosis in peripheral blood is significantly increased, correlating with disease severity.23 In imiquimod-induced psoriasis-like mouse models, inhibiting NETs formation with Cl-amidine or reducing peripheral blood NETs with DNase significantly improves skin lesions and reduces inflammatory mediators.24 These findings confirm the critical role of NETs in the pathogenesis of psoriasis.
One of the features of psoriasis is the elevated level of active, phosphorylated nuclear factor kappa B (NF-κB). NF-κB pathway plays a crucial role in psoriasis, as it regulates the behaviors of keratinocytes and immune cells by affecting their proliferation, differentiation, and production of cytokines.25 Toll-like receptor 4 (TLR4) is overexpressed in psoriatic lesions,26 and its downregulation reduces NF-κB pathway activation, thereby improving psoriasis-like lesions.27 Myeloid differentiation factor 88 (MyD88) is a key adaptor molecule in TLR4 signaling pathway, which is one of the major upstream pathways activating NF-κB signaling.28 Lipocalin-2 (LCN2), also known as neutrophil gelatinase-associated lipocalin, is highly expressed in psoriatic lesions, promoting neutrophil recruitment and activation.29,30 A study has shown that NETs activate keratinocytes via TLR4 in vitro, thereby triggering NF-κB signaling through TLR4/MyD88 pathway and leading to increased LCN2 expression.24 In turn, LCN2 recruits neutrophils and promotes NETs formation.31 This interaction between NETs and keratinocytes forms a positive feedback loop mediated by TLR4/MyD88/NF-κB/LCN2 pathway, amplifying and sustaining the immune-inflammatory response. Such interplay between immune cells and skin-resident cells is critical to the development and persistence of psoriasis. Therefore, this study focuses on the positive feedback loop between NETs and keratinocytes, verifying the inhibitory effects of fire needling acupuncture on NETs formation and TLR4/MyD88/NF-κB/LCN2 pathway to elucidate its mechanism in treating psoriasis.
Materials and Methods
Experimental Animals
BALB/c mice (8 weeks old, female) were purchased from SPF (Beijing) Biotechnology Co, Ltd. The mice were maintained under specific pathogen-free conditions, with a temperature of 23 ± 1°C, relative humidity of 40–60%, a 12 h light/dark cycle, and free access to food and water. Prior to the commencement of the experiments, the mice were acclimatized for 7 days. To eliminate potential experimenter bias, the individuals conducting the experiments were blinded. All animal experiments complied with ARRIVE guidelines, were authorized by the Animal Ethics Committee of the Beijing Institute of Traditional Chinese Medicine (Approval number: BJTCM-M-2023-10-05).
Model Establishment
The dorsal hair of each mouse was shaved, and a 2 cm × 2 cm square area on the back was outlined with a skin marker for the application of imiquimod to establish the psoriasis-like mouse models. About 62.5 mg of 5% imiquimod cream (Mingxin Pharmaceutical Co, Ltd, China) was applied daily to the back for 6 consecutive days.32 Model induction was generally performed between 08:00 and 10:00. As this is an acute and short-term model, the treatment was administered concurrently with model induction in this study, consistent with common practice in previous studies.33,34
Fire Needling Acupuncture Treatment
Fire needling acupuncture was performed once daily between 14:00 and 16:00 for 6 consecutive days at bilateral Zusanli (ST36) and Quchi (LI11) acupoints using filiform needles (0.25 mm × 10 mm; Hualun Medical Appliance Co, Ltd, China). The operator held a portable alcohol lamp in one hand and the filiform needle in the other, keeping both close to the acupoint to allow rapid insertion. The needles were heated over the alcohol lamp until red-hot and then rapidly inserted into the acupoints to a depth of 0.5–1.0 mm and immediately withdrawn, and this procedure was repeated twice per treatment. Acupoint localization was based on the Animal Acupoint Atlas and T/CAAM 0002–2020 guidelines.35
Experimental Grouping
Mice were randomly and equally divided into five groups (n = 6 per group) (Figure 1): (1) Control: A dose of 62.5 mg Vaseline was applied daily to the back for 6 consecutive days; (2) Imiquimod (IMQ): 62.5 mg of 5% imiquimod cream was applied daily to the back for 6 consecutive days. (3) IMQ + Methotrexate (IMQ + MTX): Imiquimod cream was applied as in IMQ group. Methotrexate (Sine Pharmaceutical Co, Ltd, China) was dissolved in distilled water at a final concentration of 0.1 mg/mL, and 0.2 mL was administered by oral gavage daily for 6 consecutive days. (4) IMQ + Fire needling acupuncture (IMQ + FN): Imiquimod cream was applied as in IMQ group and fire needling acupuncture treatment was performed daily for 6 consecutive days. (5) IMQ + Cl-amidine (NETs inhibitor): Imiquimod cream was applied as in IMQ group. Mice were subcutaneously injected with Cl-amidine (MedChemExpress, USA) at a dose of 10 mg/kg/day for 6 consecutive days.24 In addition, the Control, IMQ, IMQ + FN, and IMQ + Cl-amidine groups were administered 0.2 mL of normal saline by oral gavage daily for 6 consecutive days.
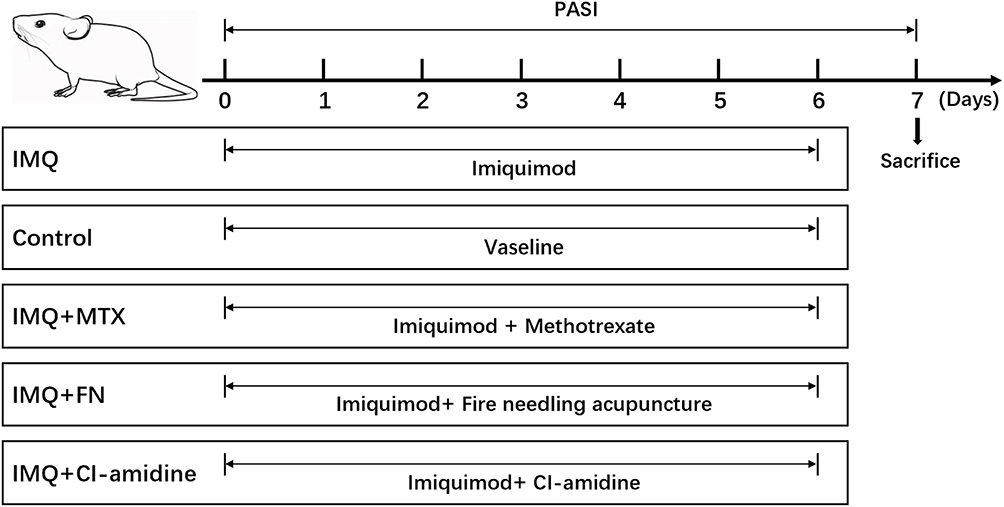 |
Figure 1 Experimental design and timeline of the study. Mice were randomly assigned to five groups (n = 6 per group): Control, Imiquimod (IMQ), IMQ + methotrexate (MTX), IMQ + fire needling acupuncture (FN), and IMQ + Cl-amidine. Psoriasis Area and Severity Index (PASI) was used to assess the severity of psoriasis-like skin lesions daily. On day 7, mice were euthanized to collect lesional skin tissues. No mice were excluded from the subsequent analyses. |
Sample Collection
On day 7, all mice were anesthetized with pentobarbital sodium and sacrificed to collect the lesional skin tissues. A portion was fixed in 4% formaldehyde, another portion was stored at −80°C, and the remaining portion was processed to isolate the epidermis for subsequent Western blot analysis.
Lesion Scoring and Histopathological Evaluation
The severity of psoriasis-like skin lesions was assessed daily from day 1 to day 7 using the Psoriasis Area and Severity Index (PASI). It consists of three components: erythema, thickness, and scales, each scored from 0 to 4, with a total score ranging from 0 to 12.36 The investigators independently scored all mouse skin lesions using PASI while blinded to group allocation.
After sample collection, the skin tissues were fixed in 4% formaldehyde, dehydrated, embedded in paraffin, sectioned and stained with hematoxylin and eosin (H&E). The histopathological changes in the skin were observed and photographed under a microscope, and epidermal thickness was measured using ImageJ software. The sections were independently and blindly evaluated by investigators.
Enzyme-Linked Immunosorbent Assay
Levels of interleukin (IL)-23, IL-17, tumor necrosis factor (TNF)-α, and IL-1β in skin lesions were quantified using Enzyme-Linked Immunosorbent Assay (ELISA) kits (Beijing Oubei Biotechnology Co, Ltd, China) following the manufacturer’s protocols. Then we used a microplate reader (Thermo Fisher Scientific, USA) to measure the absorbance at 450 nm.
Immunofluorescence and Immunohistochemistry
After deparaffinization, the tissue sections were immersed in 10 mM sodium citrate buffer (pH 6.0) and heated at 95°C for 10 min for antigen retrieval. Subsequently, the sections were incubated in 3% H2O2 for 30 min to quench endogenous peroxidase activity. After blocking nonspecific binding sites, the sections were incubated overnight at 4°C with primary antibodies against Ki67 (1:500; Abcam, USA), K10 (1:500; Proteintech, USA), Ly6G (1:1000; Servicebio, China), MPO (1:2000; Servicebio, China), and Cit-H3 (1:300; Novus, USA). After washing with PBS, sections stained for Ki67 and K10 were incubated with fluorescently labeled secondary antibodies at room temperature for 1 h in the dark, followed by DAPI staining. Sections stained for Ly6G, MPO, and Cit-H3 were incubated with HRP-conjugated secondary antibodies at 37°C for 30 min, washed with PBS, and visualized using DAB. Hematoxylin was used for nuclear staining. The stained sections were observed and photographed under microscopes. Positive cells were counted, and the proportion of positive areas was measured using ImageJ software. The sections were independently and blindly evaluated by investigators.
Western Blot Analysis
The epidermal tissues were minced and mixed with RIPA buffer and protease inhibitors. The mixture was homogenized and lysed for 30 min, followed by centrifugation to collect the supernatant. Protein concentration was measured using BCA assay. Protein samples were loaded onto gels for electrophoresis, followed by transfer onto polyvinylidene fluoride (PVDF) membranes. After blocking nonspecific binding sites, primary antibodies against TLR4 (1:4000; Proteintech, USA), MyD88 (1:10000; Proteintech, USA), NF-κB (1:1000; Proteintech, USA), p-NF-κB (1:1000; CST, USA), LCN2 (1:1000; Proteintech, USA), and β-actin (1:1000; Proteintech, USA) were added, and PVDF membranes were incubated overnight at 4°C. After washing with TBST, the membranes were incubated with secondary antibodies for 1 h at room temperature. Subsequently, protein bands were visualized using ECL and images were captured with a blot scanner. Band intensity was quantified using ImageJ software.
Statistical Analysis
All data were analyzed using SPSS 20.0 software and expressed as mean ± SD. One-way ANOVA was used for normally distributed data, followed by LSD post hoc test for multiple comparisons. For non-normally distributed data, the Kruskal–Wallis test was applied. Differences were considered statistically significant at P < 0.05.
Results
Fire Needling Acupuncture Improved Psoriasis-Like Lesions
Compared with Control group, all mice treated with imiquimod cream developed psoriasis-like lesions of varying severity on their backs. From day 3 to day 7, scores for erythema, thickness, scales, and PASI were significantly higher in IMQ group than in Control group and continued to increase, indicating that the imiquimod-induced psoriasis-like mouse model successfully recapitulated the clinical features of psoriasis. Fire needling acupuncture delayed the progression of the psoriasis-like lesions, with methotrexate and Cl-amidine showing a similar therapeutic effect (Figure 2C). On day 7, PASI scores in IMQ + FN, IMQ + MTX, and IMQ + Cl-amidine groups were significantly lower than those in IMQ group (Figure 2A and B). The lower PASI scores in these three groups were mainly due to reduced thickness and scales scores, while erythema scores showed a decreasing trend but without statistical significance. These results indicate that fire needling acupuncture effectively alleviated psoriasis-like lesions in imiquimod-induced mice and support the therapeutic potential of NETs inhibitor in psoriasis.
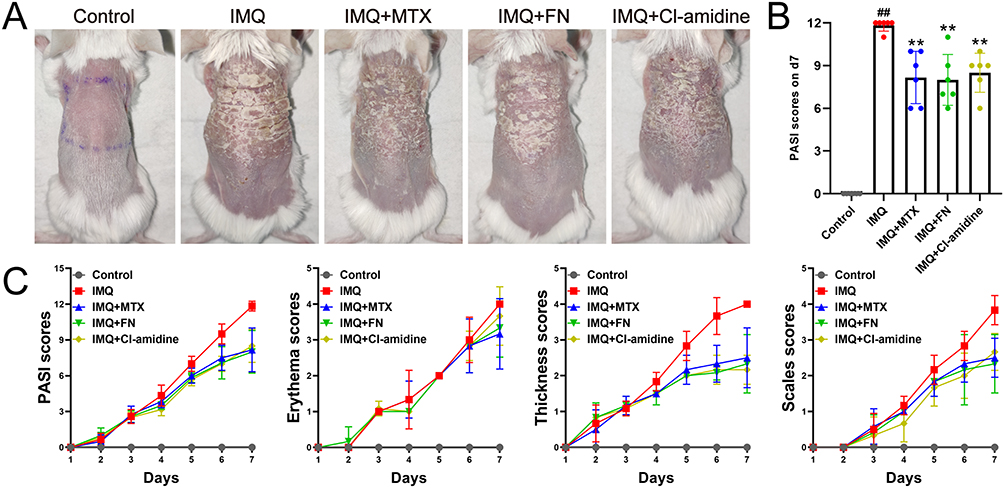 |
Figure 2 Fire needling acupuncture alleviates psoriasis-like skin lesions. (A) Representative skin lesions on the backs of mice from different groups on day 7. (B) Comparison of PASI scores on day 7 between different groups (n = 6 for each group). (C) Scores of PASI, erythema, thickness, and scales from day 1 to day 7 in different groups (n = 6 for each group). ##P < 0.01 vs Control; **P < 0.01 vs IMQ. |
Fire Needling Acupuncture Suppressed Abnormal Keratinocyte Proliferation and Differentiation in Psoriasis-Like Lesions
H&E staining revealed that, compared with Control group, IMQ group displayed marked hyperkeratosis, parakeratosis, thickening of stratum spinosum, infiltration of inflammatory cells, and proliferation of capillaries, which are pathological features of psoriasis. Fire needling acupuncture significantly reduced the thickening of stratum spinosum, and methotrexate and Cl-amidine also reduced this thickening (Figure 3A and D).
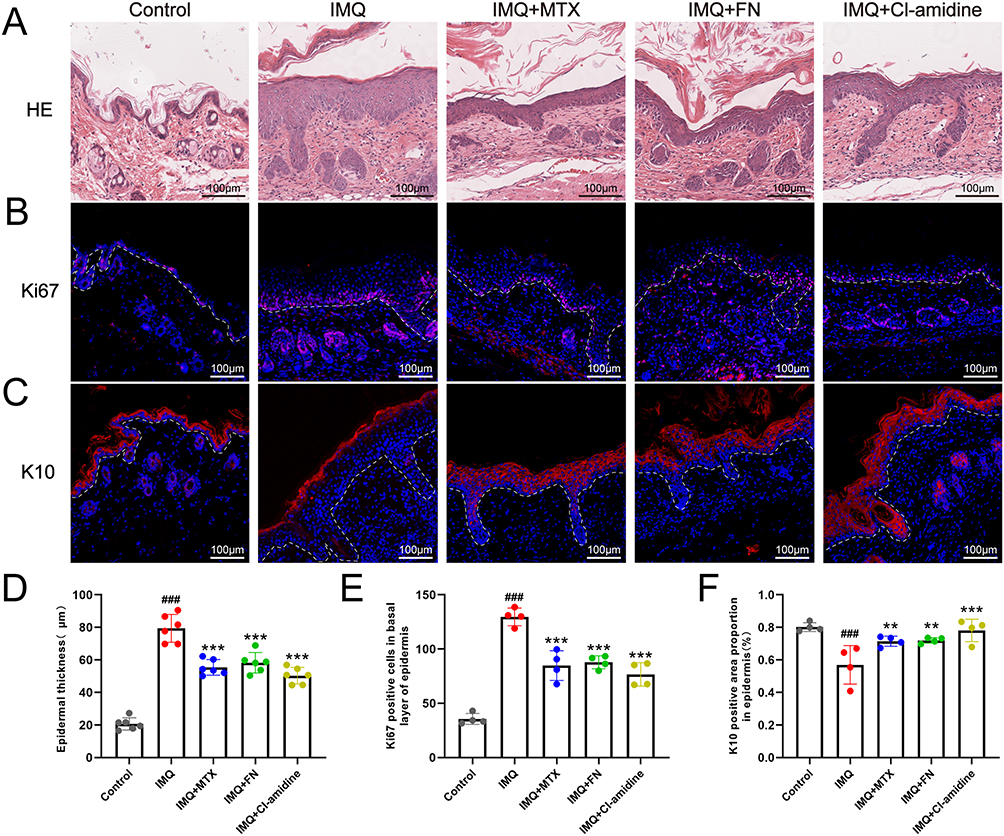 |
Figure 3 Fire needling acupuncture suppresses the abnormal proliferation and differentiation in keratinocytes. (A) H&E staining of the skin lesions. (B–C) Expression of Ki67 and K10 in skin lesions by immunofluorescence. (D) Comparison of epidermal thickness between different groups (n = 6 for each group). (E–F) Comparison of Ki67 and K10 expression in epidermis between different groups (n = 4 for each group). ###P < 0.001 vs Control; **P < 0.01, ***P < 0.001 vs IMQ. |
Psoriasis is characterized by abnormal proliferation and differentiation of keratinocytes, resulting in hyperkeratosis, parakeratosis, and thickening of stratum spinosum in epidermis.37 Ki67 and Keratin 10 (K10) are markers of cell proliferation and keratinocyte differentiation in epidermis, mainly expressed in basal layer and suprabasal layers of epidermis, respectively.38,39 Our results showed that, compared with Control group, the expression of Ki67 in basal layer was significantly increased, while the expression of K10 in suprabasal layers was significantly decreased in IMQ group. In contrast, fire needling acupuncture significantly reduced the expression of Ki67 in basal layer and increased the expression of K10 in suprabasal layers compared with IMQ group (Figure 3B, C, E and F). Furthermore, the expression of K10 in IMQ group shifted towards the upper layers of epidermis, suggesting delayed differentiation, and this shift was reversed by fire needling acupuncture (Figure 3C). Methotrexate and Cl-amidine produced effects similar to those of fire needling acupuncture. These findings suggest that fire needling acupuncture inhibited keratinocyte hyperproliferation and promoted the restoration of normal keratinocyte differentiation.
Fire Needling Acupuncture Reduced the Levels of Inflammatory Cytokines in Psoriasis-Like Lesions
Psoriatic lesions exhibit marked inflammation, with various inflammatory cytokines stimulating keratinocytes and leading to excessive proliferation and abnormal differentiation.40 We measured the levels of IL-23, IL-17, TNF-α, and IL-1β in the lesions using ELISA. The results showed that the levels of the inflammatory cytokines in IMQ group were markedly higher than in Control group. Fire needling acupuncture, methotrexate, and Cl-amidine significantly reduced the levels of these inflammatory cytokines (Figure 4). These findings suggest that fire needling acupuncture effectively alleviated local inflammation in psoriasis-like lesions and inhibition of NETs also reduced the inflammation.
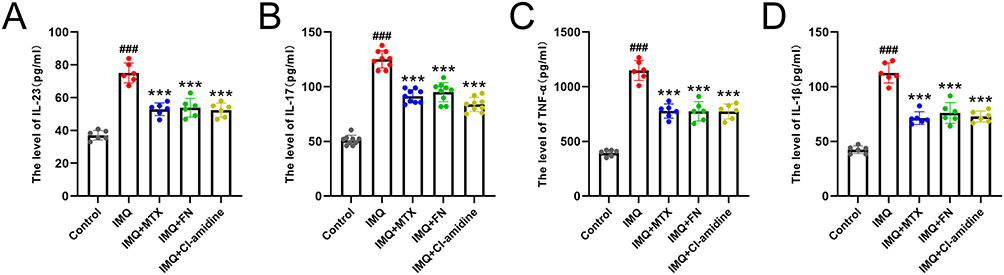 |
Figure 4 Fire needling acupuncture reduces inflammatory cytokine levels in psoriasis-like skin lesions. (A–D) Comparison of IL-23, IL-17, TNF-α, and IL-1β levels in skin lesions between different groups (n = 6 for each group). ###P < 0.001 vs Control; ***P < 0.001 vs IMQ. |
Fire Needling Acupuncture Reduced Neutrophil Infiltration and NETs Formation in Psoriasis-Like Lesions
A large number of neutrophils infiltrate psoriatic lesions and form Munro’s microabscesses in epidermis, which are regarded as pathognomonic for psoriasis.1 These neutrophils can form NETs after activation, further promoting inflammation.22,41 During NETs formation, NETs-associated markers such as myeloperoxidase (MPO) and citrullinated histone H3 (Cit-H3) are released, adhering to the web-like structure.22 We used immunohistochemistry to detect mouse neutrophil marker (Ly6G), as well as NETs-associated markers (MPO and Cit-H3) in the skin lesions. The results showed that, compared with Control group, IMQ group exhibited markedly increased numbers of Ly6G-positive and Cit-H3-positive cells, as well as elevated MPO expression in the lesions (Figure 5). Compared with IMQ group, fire needling acupuncture, methotrexate, and Cl-amidine significantly reduced the numbers of Ly6G-positive and Cit-H3-positive cells, as well as MPO expression in the lesions (Figure 5). These findings indicate that fire needling acupuncture reduced neutrophil infiltration and NETs formation. And the effects were similar to those of Cl-amidine, further confirming the inhibitory effect of fire needling acupuncture on NETs formation.
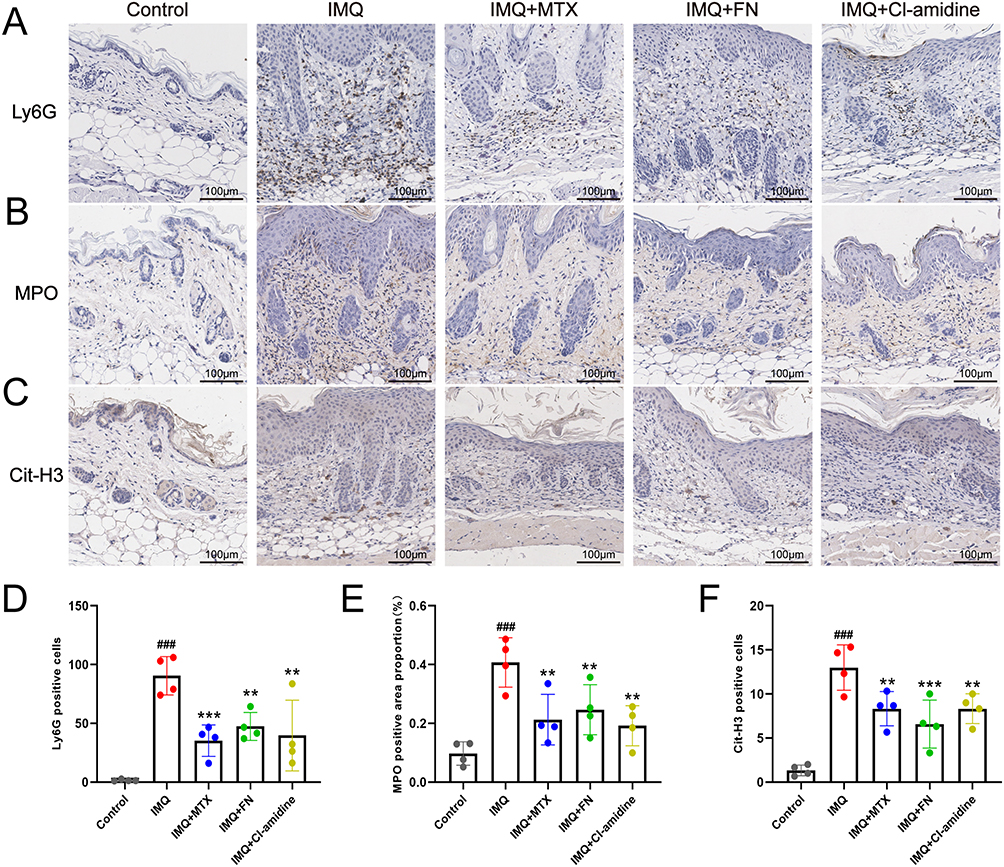 |
Figure 5 Fire needling acupuncture reduces neutrophil infiltration and NETs formation. (A–C) Expression of Ly6G, MPO, and Cit-H3 in skin lesions by immunohistochemistry. (D–F) Comparison of Ly6G, MPO, and Cit-H3 expression in skin lesions between different groups (n = 4 for each group). ###P < 0.001 vs Control; **P < 0.01, ***P < 0.001 vs IMQ. |
Fire Needling Acupuncture Inhibited TLR4/MyD88/NF-κB/LCN2 Pathway in the Epidermis of Psoriasis-Like Lesions
In vitro, NETs activate TLR4 and subsequently trigger NF-κB signaling in keratinocytes, leading to LCN2 overexpression.24 LCN2, in turn, functions as both a chemoattractant and an activator, recruiting more neutrophils and promoting further NETs formation.31 To investigate the regulatory role of fire needling acupuncture in this positive feedback loop, we performed Western blot analysis to detect key proteins involved in the pathway. The results showed that, compared with Control group, the protein levels of TLR4, MyD88, p-NF-κB and LCN2 in epidermis were significantly increased in IMQ group. In contrast, the levels of these proteins in epidermis were significantly decreased in IMQ + FN, IMQ + MTX, and IMQ + Cl-amidine groups compared with IMQ group (Figure 6). Notably, the epidermis is made almost entirely of keratinocytes,42 which can also be observed in the H&E staining results (Figure 3A). These findings suggest that fire needling acupuncture inhibited TLR4/MyD88/NF-κB/LCN2 pathway in epidermal keratinocytes, thereby reducing the recruitment of neutrophils and further NETs formation. In addition, Cl-amidine, a NETs inhibitor, inhibited TLR4/MyD88/NF-κB/LCN2 pathway in epidermal keratinocytes, verifying in vivo the interaction between NETs and keratinocytes. And fire needling acupuncture disrupted the positive feedback loop between NETs and keratinocytes.
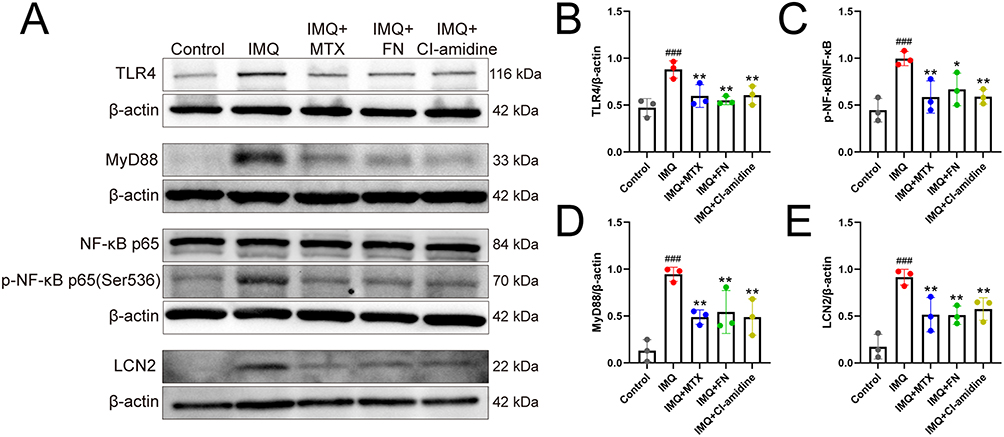 |
Figure 6 Fire needling acupuncture inhibits TLR4/MyD88/NF-κB/LCN2 pathway. (A) Representative Western blots showing TLR4, MyD88, NF-κB, p-NF-κB, and LCN2 in the epidermis of psoriasis-like skin lesions. (B–E) Comparison of TLR4, MyD88, p-NF-κB, and LCN2 protein levels between different groups (n = 3 for each group). ###P < 0.001 vs Control; *P < 0.05, **P < 0.01 vs IMQ. |
Discussion
This study, for the first time, explored the effects of fire needling acupuncture on psoriasis from the perspective of NETs and neutrophils. Results showed that fire needling acupuncture improved psoriasis-like lesions, suppressed the abnormal proliferation and differentiation of keratinocytes, and reduced local inflammatory cytokine levels. These effects of fire needling acupuncture may be associated with the inhibition of NETs formation and TLR4/MyD88/NF-κB/LCN2 pathway.
The clinical manifestations of psoriasis primarily include erythema and scaling, with histological features including abnormal keratinization, acanthosis, capillary proliferation and dilation, and inflammatory cell infiltration. The imiquimod-induced psoriasis-like mouse model exhibits similar skin lesion manifestations and histological features, which can usually be established within 5 to 7 days of induction.43 In this study, fire needling acupuncture reduced scaling and skin thickening in the mouse models, thereby lowering PASI scores. H&E staining further confirmed that fire needling acupuncture reduced the thickening of stratum spinosum.
The thickening and scaling of psoriatic lesions result from excessive keratinocyte proliferation and impaired differentiation. Therefore, we evaluated epidermal proliferation and differentiation using immunofluorescence staining for Ki67 and K10. In normal epidermis, Ki67 is sparsely expressed in the basal layer, whereas K10 is widely expressed in suprabasal layers.38,39 In contrast, psoriatic epidermis shows strong Ki67 expression in the basal layer and several suprabasal layers, while K10 expression is absent in several suprabasal layers and even in parts of the nucleated upper layers, indicating hyperproliferation and delayed differentiation.39,44 In this study, the IMQ group exhibited similar alterations in Ki67 and K10 expression, and these alterations were significantly reversed by fire needling acupuncture. These findings demonstrate that fire needling acupuncture promotes the restoration of normal epidermal proliferation and differentiation, thereby alleviating psoriasis-like skin lesions.
Psoriasis is characterized by persistent inflammation in skin lesions. Multiple inflammatory cytokines stimulate keratinocytes, which is a major cause of abnormal epidermal proliferation and differentiation.40 IL-17, as a key effector cytokine,45 works together with IL-23 through IL-23/Th17 axis to play a central role in the pathogenesis of psoriasis.46 TNF-α not only promotes dendritic cells to release IL-23 but also acts synergistically with IL-17 to stimulate keratinocytes to produce inflammatory cytokines.47,48 IL-1β can induce the differentiation of Th17 cells and γδT cells, thereby enhancing IL-17 production.49 In this study, fire needling acupuncture significantly reduced the levels of IL-23, IL-17, TNF-α, and IL-1β in skin lesions, alleviating skin inflammation and promoting the restoration of normal functions in keratinocytes.
NETs and neutrophils amplify the inflammatory response during the onset and progression of psoriasis. As the “first-line” cells in acute inflammation, neutrophils are rapidly recruited to the skin in the early stage of psoriasis and can form NETs under stimulation by pathogens and cytokines, thereby promoting inflammation.22,41 During NETs formation, large amounts of IL-17 are released,50 along with abundant antimicrobial peptide–DNA/RNA complexes.51 Among these, LL37–DNA complexes stimulate plasmacytoid dendritic cells (pDCs) to produce type I interferon (IFN), promoting T cell activation and differentiation, thereby initiating Th1-, Th17-, and Th22-related inflammatory pathways.52 LL37–RNA complexes, on the other hand, recruit and activate neutrophils, thereby promoting further NETs formation and creating a self-amplifying inflammatory loop that drives psoriasis progression.53 In this study, Cl-amidine (NETs inhibitor) reduced NETs formation, thereby suppressing inflammation and improving psoriasis-like lesions. Meanwhile, fire needling acupuncture significantly reduced neutrophil infiltration and the expression of NETs-associated markers (MPO and Cit-H3) in skin lesions, and these effects were comparable to those of Cl-amidine. These findings indicate that fire needling acupuncture may alleviate inflammation by reducing neutrophil infiltration and NETs formation, thereby improving psoriasis-like skin lesions.
LCN2 is a protein stored in specific granules of neutrophils.54 It acts both as a chemoattractant to promote neutrophil infiltration and as an activator to enhance neutrophil activation in skin lesions, thereby facilitating further LCN2 secretion and continuous NETs formation.31 In this study, fire needling acupuncture reduced LCN2 protein level and neutrophil infiltration in skin lesions, attenuating NETs formation and the amplification of inflammation. In addition to neutrophils, keratinocytes are another important source of LCN2.55 In vitro, NETs can activate keratinocytes by TLR4, promoting LCN2 overexpression via TLR4/MyD88/NF-κB pathway.24 Thus, NETs and keratinocytes establish a positive feedback loop mediated by TLR4/MyD88/NF-κB/LCN2 pathway, amplifying and sustaining the immune-inflammatory response. In this study, Cl-amidine inhibited TLR4/MyD88/NF-κB/LCN2 pathway in epidermal keratinocytes, verifying in vivo the interaction between NETs and keratinocytes. Fire needling acupuncture also inhibited TLR4/MyD88/NF-κB/LCN2 pathway in epidermal keratinocytes, thereby reducing the recruitment of neutrophils and further NETs formation. Consequently, the positive feedback loop between NETs and keratinocytes was disrupted (Figure 7). This is likely a key mechanism underlying the anti-inflammatory effects of fire needling acupuncture and the improvement of psoriasis-like skin lesions.
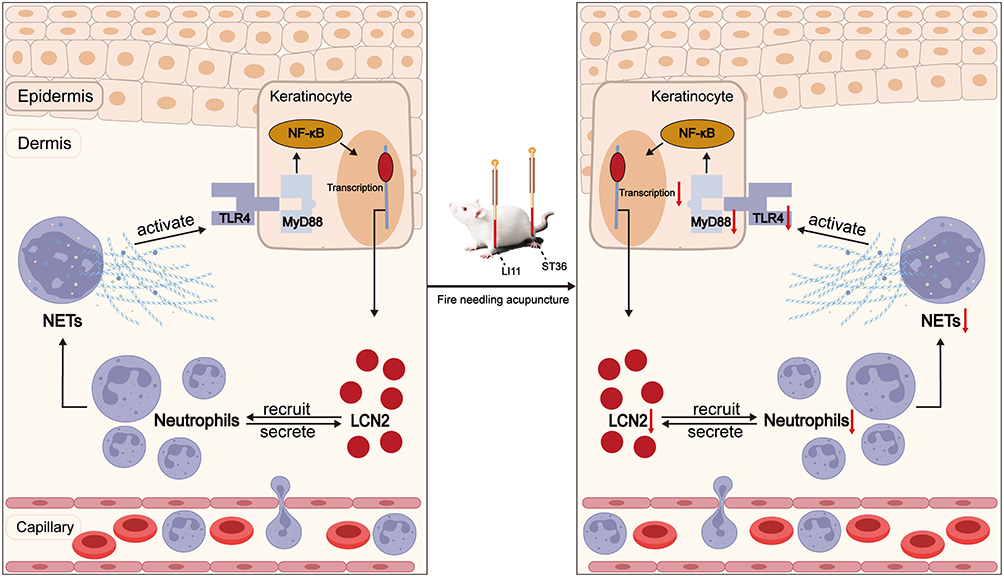 |
Figure 7 Fire needling acupuncture reduces NETs formation and inhibits TLR4/MyD88/NF-κB/LCN2 pathway in psoriasis (the red arrows indicate inhibition). |
This study has several limitations. First, the temperature of the fire needle and its contact time with skin could not be accurately measured. In addition, although we propose that NETs and TLR4/MyD88/NF-κB/LCN2 pathway may be key mechanisms by which fire needling acupuncture ameliorates psoriasis-like skin lesions, we did not experimentally validate a specific causal pathway. Future studies are needed to clarify these causal relationships and to develop the standardization of fire needling acupuncture parameters.
Conclusion
Fire needling acupuncture effectively improves skin lesions, suppresses abnormal keratinocyte proliferation and differentiation, and alleviates local inflammation in imiquimod-induced psoriasis-like mice. These effects may result from its ability to reduce neutrophil infiltration and NETs formation and to inhibit TLR4/MyD88/NF-κB/LCN2 pathway.
Data Sharing Statement
Data sets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We sincerely thank Hohhot Hospital of Traditional Chinese Medicine and Mongolian Medicine, as well as Chief Physician Durina, for supporting this study. We would like to thank Songtao Kuang and Jingwen Zhao from Beijing University of Chinese Medicine, and Yuxin Hong from Beijing Institute of Traditional Chinese Medicine, for their technical assistance.
Author Contributions
Conceptualization: Qun Wang, Xin Wang, Jingqing Sun. Formal analysis: Qun Wang, Jiangyan Wei, Xin Wang. Funding acquisition: Fang Yuan, Jingqing Sun. Investigation: Qun Wang, Jiangyan Wei. Project administration: Xin Wang. Resources: Xin Wang, Fang Yuan, Jingqing Sun. Supervision: Xin Wang, Jingqing Sun. Validation: Qun Wang, Jiangyan Wei, Xin Wang, Fang Yuan. Visualization: Qun Wang. Writing – original draft: Qun Wang, Jiangyan Wei, Fang Yuan. Writing – review and editing: Xin Wang, Fang Yuan, Jingqing Sun. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Technical Cooperation Agreement between Beijing Hospital of Traditional Chinese Medicine, Capital Medical University and Hohhot Hospital of Traditional Chinese Medicine and Mongolian Medicine; The National Natural Science Foundation of China (No 82205246); Hospital-level Research Project of Beijing Hospital of Traditional Chinese Medicine, Capital Medical University (No LYYB202225).
Disclosure
The authors declare that there are no conflicts of interest.
References
1. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. 2021;397(10281):1301–13. doi:10.1016/S0140-6736(20)32549-6
2. Singh S, Taylor C, Kornmehl H, Armstrong AW. Psoriasis and suicidality: a systematic review and meta-analysis. J Am Acad Dermatol. 2017;77(3):425–440.e2. doi:10.1016/j.jaad.2017.05.019
3. Armstrong AW, Blauvelt A, Callis Duffin K, et al. Psoriasis. Nat Rev Dis Primers. 2025;11(1):45. doi:10.1038/s41572-025-00630-5
4. Tian D, Lai Y. The relapse of psoriasis: mechanisms and mysteries. JID Innov. 2022;2(3):100116. doi:10.1016/j.xjidi.2022.100116
5. Lee HJ, Kim M. Challenges and future trends in the treatment of psoriasis. Int J Mol Sci. 2023;24(17):13313. doi:10.3390/ijms241713313
6. Zhang J, Lin P, Guo C, et al. Effects and safety of fire needle adjuvant chemical peels therapy in acne vulgaris: a systematic review and meta-analysis. J Dermatolog Treat. 2023;34(1):2240455. doi:10.1080/09546634.2023.2240455
7. Liu L, Sun XY, Zhao YD, et al. Efficacy and safety of fire needle therapy for plaque psoriasis: a randomized, single-blind, multicenter clinical trial. QJM. 2025. doi:10.1093/qjmed/hcaf275
8. Xing M, Yan X, Sun X, et al. Fire needle therapy for moderate-severe acne: a PRISMA systematic review and meta-analysis of randomized controlled trials. Complement Ther Med. 2019;44:253–260. doi:10.1016/j.ctim.2019.04.009
9. Luo Y, Qian W, Dai T, et al. A new therapy for vitiligo using fire needles: a systematic review of evidence from 3618 subjects. Evid Based Complement Alternat Med. 2020;2020:8492097. doi:10.1155/2020/8492097
10. Xin S, Liu J, Yang Z, Li C. Comparative effectiveness of moxibustion and acupuncture for the management of osteoarthritis knee: a systematic review and meta-analysis. Heliyon. 2023;9(7):e17805. doi:10.1016/j.heliyon.2023.e17805
11. Zhang Q, Yuan Y, Zhang M, et al. Efficacy and safety of acupuncture-point stimulation combined with opioids for the treatment of moderate to severe cancer pain: a network meta-analysis of randomized controlled trials. Front Oncol. 2023;13:1166580. doi:10.3389/fonc.2023.1166580
12. Su YQ, Liu ZY, Wei G, Zhang CM. Topical halometasone cream combined with fire needle pre-treatment for treatment of primary cutaneous amyloidosis: two case reports. World J Clin Cases. 2022;10(20):7147–7152. doi:10.12998/wjcc.v10.i20.7147
13. Li M, Zhu X, Cao Z, Du L, Wei J, Zhang C. Fire needle combined topical mupirocin for the treatment of simple skin abscesses in pediatric patients: a case series. Infect Drug Resist. 2023;16:3683–3692. doi:10.2147/IDR.S416917
14. Long Q, Yang C, Li Y. Fire needle reduced the clinical symptoms of psoriasis vulgaris. Asian J Surg. 2024;47(12):5253–5254. doi:10.1016/j.asjsur.2024.05.305
15. Liu L, Sun X, Lu Y, et al. Fire needle therapy for the treatment of psoriasis: a quantitative evidence synthesis. J Altern Complement Med. 2021;27(1):24–37. doi:10.1089/acm.2019.0409
16. Xu J, Zhou Q, Xie F, Cao Y, Yang X, Tao M. Effect of fire needle combined with traditional Chinese medicine on psoriasis: a systematic review and meta-analysis. Medicine. 2024;103(7):e35832. doi:10.1097/MD.0000000000035832
17. Chen H, Zhou GX, He XJ, Guo F, Chen JM, Qian X. Efficacy of fire needle on acute gouty arthritis induced by monosodium urate in rat. J Tradit Chin Med. 2021;41(4):564–570. doi:10.19852/j.cnki.jtcm.2021.03.008
18. Wei J, Yang X, Ge X, et al. Therapeutic effects of fire needling acupuncture on pain relief and cartilage protection in MIA-induced knee osteoarthritis rats: the role of macrophage polarization in synovium and angiogenesis in subchondral bone. J Inflamm Res. 2025;18:7459–7475. doi:10.2147/JIR.S518829
19. Shi Y, Chen D, Wang Y, et al. Filiform fire needling therapy relieves T cells-mediated melanocyte apoptosis and dysfunction by inhibiting JAK/STAT3 pathway via Mfsd4a in vitiligo. Chin Med. 2025;20(1):117. doi:10.1186/s13020-025-01172-4
20. Feng F, Wang Y, Zhao JX, et al. Effect of fire needling on imiquimod induced psoriasis-like lesion and STAT3 pathway in mice. Zhongguo Zhen Jiu. 2022;42(5):541–548. doi:10.13703/j.0255-2930.20211112-k0005
21. Zhang Y, Meng Y, Du C. Analysis of the rules of acupuncture treatment for psoriasis. West J Tradit Chin Med. 2024;37(06):47–51.
22. Czerwińska J, Owczarczyk-Saczonek A. The role of the neutrophilic network in the pathogenesis of psoriasis. Int J Mol Sci. 2022;23(3):1840. doi:10.3390/ijms23031840
23. SC-S H, Yu H-S, Yen F-L, Lin C-L, Chen G-S, Lan -C-CE. Neutrophil extracellular trap formation is increased in psoriasis and induces human β-defensin-2 production in epidermal keratinocytes. Sci Rep. 2016;6:31119. doi:10.1038/srep31119
24. Shao S, Fang H, Dang E, et al. Neutrophil extracellular traps promote inflammatory responses in psoriasis via activating epidermal TLR4/IL-36R crosstalk. Front Immunol. 2019;10:746. doi:10.3389/fimmu.2019.00746
25. Guo J, Zhang H, Lin W, Lu L, Su J, Chen X. Signaling pathways and targeted therapies for psoriasis. Signal Transduct Target Ther. 2023;8(1):437. doi:10.1038/s41392-023-01655-6
26. Kumar V. Going, Toll-like receptors in skin inflammation and inflammatory diseases. EXCLI J. 2021;20:52–79. doi:10.17179/excli2020-3114
27. Tang H, Guo Z, Tang X, et al. MST1 modulates Th17 activation in psoriasis via regulating TLR4-NF-κB pathway. Hum Cell. 2021;34(1):28–36. doi:10.1007/s13577-020-00423-w
28. Wang Y, Sadike D, Huang B, et al. Regulatory T cells alleviate myelin loss and cognitive dysfunction by regulating neuroinflammation and microglial pyroptosis via TLR4/MyD88/NF-κB pathway in LPC-induced demyelination. J Neuroinflammation. 2023;20(1):41. doi:10.1186/s12974-023-02721-0
29. Kamata M, Tada Y, Tatsuta A, et al. Serum lipocalin-2 levels are increased in patients with psoriasis. Clin Exp Dermatol. 2012;37(3):296–299. doi:10.1111/j.1365-2230.2011.04265.x
30. El-Hadidi H, Samir N, Shaker OG, Otb S. Estimation of tissue and serum lipocalin-2 in psoriasis vulgaris and its relation to metabolic syndrome. Arch Dermatol Res. 2014;306(3):239–245. doi:10.1007/s00403-013-1414-x
31. Shao S, Cao T, Jin L, et al. Increased lipocalin-2 contributes to the pathogenesis of psoriasis by modulating neutrophil chemotaxis and cytokine secretion. J Invest Dermatol. 2016;136(7):1418–1428. doi:10.1016/j.jid.2016.03.002
32. Van Der Fits L, Mourits S, Voerman JSA, et al. Imiquimod-induced psoriasis-like skin inflammation in mice is mediated via the IL-23/IL-17 axis. J Immunol. 2009;182(9):5836–5845. doi:10.4049/jimmunol.0802999
33. Alsabbagh MM. Imiquimod-induced psoriasis model: induction protocols, model characterization and factors adversely affecting the model. Acta Biochim Pol. 2023;70(4):729–733. doi:10.18388/abp.2020_6426
34. Sun X, Liu L, Wang J, et al. Targeting STING in dendritic cells alleviates psoriatic inflammation by suppressing IL-17A production. Cell Mol Immunol. 2024;21(7):738–751. doi:10.1038/s41423-024-01160-y
35. Moxibustion, China Institute of Acupuncture. Name and location of commonly used acupoints in laboratory animals Part 3: mice. Acupuncture Res. 2021;46(5):445–446.
36. Yang W, He R, Qu H, et al. FXYD3 enhances IL-17A signaling to promote psoriasis by competitively binding TRAF3 in keratinocytes. Cell Mol Immunol. 2023;20(3):292–304. doi:10.1038/s41423-023-00973-7
37. Zhou X, Chen Y, Cui L, Shi Y, Guo C. Advances in the pathogenesis of psoriasis: from keratinocyte perspective. Cell Death Dis. 2022;13(1):81. doi:10.1038/s41419-022-04523-3
38. Zhang X, Yin M, Zhang L. Keratin 6, 16 and 17—critical barrier alarmin molecules in skin wounds and psoriasis. Cells. 2019;8(8):807. doi:10.3390/cells8080807
39. Ando M, Kawashima T, Kobayashi H, Ohkawara A. Immunohistological detection of proliferating cells in normal and psoriatic epidermis using Ki-67 monoclonal antibody. J Dermatol Sci. 1990;1(6):441–446. doi:10.1016/0923-1811(90)90014-5
40. Rendon A, Schäkel K. Psoriasis pathogenesis and treatment. Int J Mol Sci. 2019;20(6):1475. doi:10.3390/ijms20061475
41. Rodriguez-Rosales YA, Langereis JD, Gorris MAJ, et al. Immunomodulatory aged neutrophils are augmented in blood and skin of psoriasis patients. J Allergy Clin Immunol. 2021;148(4):1030–1040. doi:10.1016/j.jaci.2021.02.041
42. De Jongh GJ, Zeeuwen PL, Kucharekova M, et al. High expression levels of keratinocyte antimicrobial proteins in psoriasis compared with atopic dermatitis. J Invest Dermatol. 2005;125(6):1163–1173. doi:10.1111/j.0022-202X.2005.23935.x
43. Hawkes JE, Gudjonsson JE, Ward NL. The snowballing literature on imiquimod-induced skin inflammation in mice: a critical appraisal. J Invest Dermatol. 2017;137(3):546–549. doi:10.1016/j.jid.2016.10.024
44. Bernerd F, Magnaldo T, Darmon M. Delayed onset of epidermal differentiation in psoriasis. J Invest Dermatol. 1992;98(6):902–910. doi:10.1111/1523-1747.ep12460344
45. Blauvelt A, Chiricozzi A. The immunologic role of IL-17 in psoriasis and psoriatic arthritis pathogenesis. Clin Rev Allergy Immunol. 2018;55(3):379–390. doi:10.1007/s12016-018-8702-3
46. Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323(19):1945–1960. doi:10.1001/jama.2020.4006
47. Zaba LC, Cardinale I, Gilleaudeau P, et al. Amelioration of epidermal hyperplasia by TNF inhibition is associated with reduced Th17 responses. J Exp Med. 2007;204(13):3183–3194. doi:10.1084/jem.20071094
48. Chiricozzi A, Guttman-Yassky E, Suárez-Fariñas M, et al. Integrative responses to IL-17 and TNF-α in human keratinocytes account for key inflammatory pathogenic circuits in psoriasis. J Invest Dermatol. 2011;131(3):677–687. doi:10.1038/jid.2010.340
49. Cai Y, Xue F, Quan C, et al. A critical role of the IL-1β–IL-1R signaling pathway in skin inflammation and psoriasis pathogenesis. J Invest Dermatol. 2019;139(1):146–156. doi:10.1016/j.jid.2018.07.025
50. Lin AM, Rubin CJ, Khandpur R, et al. Mast cells and neutrophils release IL-17 through extracellular trap formation in psoriasis. J Immunol. 2011;187(1):490–500. doi:10.4049/jimmunol.1100123
51. Martín Monreal MT, Kvist-Hansen A, Massarenti L, et al. Characterization of circulating extracellular traps and immune responses to citrullinated LL37 in psoriasis. Front Immunol. 2023;14:1247592. doi:10.3389/fimmu.2023.1247592
52. Lande R, Gregorio J, Facchinetti V, et al. Plasmacytoid dendritic cells sense self-DNA coupled with antimicrobial peptide. Nature. 2007;449(7162):564–569. doi:10.1038/nature06116
53. Herster F, Bittner Z, Archer NK, et al. Neutrophil extracellular trap-associated RNA and LL37 enable self-amplifying inflammation in psoriasis. Nat Commun. 2020;11(1):105. doi:10.1038/s41467-019-13756-4
54. Kjeldsen L, Bainton DF, Sengeløv H, Borregaard N. Identification of neutrophil gelatinase-associated lipocalin as a novel matrix protein of specific granules in human neutrophils. Blood. 1994;83(3):799–807. doi:10.1182/blood.V83.3.799.799
55. Ren K, Peng X, Duan X, et al. Synergistic effects of LCN2 and TWEAK on the progression of psoriasis. Cell Mol Immunol. 2025;22(7):760–775. doi:10.1038/s41423-025-01292-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.