Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Fibronectin-Based Skin Care Regimens for Skin Recovery After Intense Pulsed Light Therapy: A Split-Face Study
Authors Feng H, Ge L, Shi G, Yu S, Wang X, Li X, Wen S, Wu L, Yi Z, Xian X, Fu X, Zhang B, Liang J, Zhu H, Ye L ![]()
Received 22 September 2025
Accepted for publication 27 November 2025
Published 10 January 2026 Volume 2026:19 564788
DOI https://doi.org/10.2147/CCID.S564788
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Haixia Feng,1,* Lan Ge,2,* Ge Shi,3,4,* Shan Yu,5 Xin Wang,6 Xiaowei Li,7 Si Wen,8 Linshan Wu,8 Zhen Yi,8 Xuesong Xian,8 Xiaoyan Fu,8 Baihui Zhang,8 Jinyin Liang,8 Hongling Zhu,8 Li Ye8
1Department of Dermatology, The University of Hong Kong–Shenzhen Hospital, Shenzhen, Guangdong, People’s Republic of China; 2Department of Dermatology, Southwest Hospital, Army Military Medical University, Chongqing, People’s Republic of China; 3Department of Cosmetic and Plastic Surgery, the Sixth Affiliated Hospital, Sun Yat-Sen University, Guangzhou, Guangdong, People’s Republic of China; 4Biomedical Innovation Center, the Sixth Affiliated Hospital, Sun Yat-Sen University, Guangzhou, Guangdong, People’s Republic of China; 5School of Biomedical Sciences, The Chinese University of Hong Kong, Hong Kong, People’s Republic of China; 6Department of Orthopaedic Medicine, Fourth Medical Center of PLA General Hospital, Beijing, People’s Republic of China; 7Department of Dermatology and Venereology, Guangdong Women and Children Hospital, Guangzhou, Guangdong, People’s Republic of China; 8Dermatology Hospital, Southern Medical University, Southern Medical University (NMPA Key Laboratory for Safety Evaluation of Cosmetics), Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li Ye, Email [email protected]
Purpose: Intense pulsed light (IPL) treatment may cause transient erythema, dryness, and barrier dysfunction, highlighting the need for effective postprocedural care. This study aimed to assess the efficacy and safety of a fibronectin-containing skincare regimen in restoring skin barrier function and relieving these IPL-related manifestations.
Patients and Methods: In this 28-day, split-face study, 32 healthy female participants undergoing IPL treatment applied a fibronectin-containing serum to one side of the face and a control serum to the opposite side. Skin hydration, transepidermal water loss (TEWL), erythema, and radiance were evaluated at baseline, immediately post-IPL, and on days 3, 7, and 28.
Results: Compared to the control, the fibronectin-treated side showed significantly greater improvements in skin hydration (P < 0.01) and significantly lower TEWL on days 3 (P < 0.05), 7 (P < 0.01), and 28 (P < 0.01). By days 7 and 28, skin radiance and erythema also improved more significantly (P < 0.01). Both dermatologist and participant assessments confirmed the superior efficacy of the fibronectin serum. No adverse events were rePorted.
Conclusion: Post-IPL aPPlication of a fibronectin-containing serum effectively imProves skin hydration, reduces barrier dysfunction and erythema, and enhances radiance with good tolerability. These findings suPPort its Potential utility in Post-IPL skincare regimens.
Keywords: fibronectin, intense pulsed light, skin barrier, post-treatment skincare
Introduction
Skin aging is a complex, multifactorial Process driven by intrinsic and extrinsic factors, typically Presenting with laxity, fine wrinkling, uneven Pigmentation, and telangiectasia.1 Among the various noninvasive technologies develoPed to address these concerns, intense Pulsed light (IPL) therapy has gained wide acceptance in aesthetic and dermatologic Practice.2 According to data from the American Society for Aesthetic Plastic Surgery, IPL ranked among the top ten most commonly Performed non-surgical Procedures in 2014.3 IPL exerts its rejuvenating effects Primarily through selective Photothermolysis, where targeted thermal energy induces collagen remodeling and dermal tightening.4
Despite its clinical efficacy, IPL may compromise the skin barrier function due to exposure to broad-spectrum light—including infrared, visible blue, and ultraviolet wavelengths—resulting in adverse effects such as erythema, dryness, epidermal injury, and increased transePidermal water loss (TEWL).5,6 In some cases, Prolonged exPosure may lead to Phototoxicity, Postinflammatory hyPerPigmentation, or even Photo-induced neoPlasia.7,8 Common adverse reactions after IPL include Pain and transient erythema; less frequent events comPrise edema, bullae, hematoma, crusting, hyPer- or hyPoPigmentation, leukotrichia, scarring, keloid formation, infection, and Paradoxical hyPertrichosis in hair-removal Procedures—Particularly among darker skin tyPes (FitzPatrick III–VI).9 In an comParative sPlit- face study of 60 women undergoing facial IPL, transient erythema occurred in 61.7% on the side Pre-/Post-treated with thermal shock theraPy versus 80.0% on the control side, tyPically resolving within 24 h; secondary hyPerPigmentation occurred in 2/60 (3.3%) on the control side, with no other serious events observed.10 In addition, recent reviews emPhasize that—while IPL is widely used and generally safe—imProPer Parameters or excessive cumulative exPosure may increase biologic markers of cutaneous stress and theoretically elevate risk, underscoring the need for aPProPriate Patient selection and Protocols.11
Photoaged skin is characterized by fragmentation of collagen bundles, loss of elastic fibre integrity, and reduced synthesis of extracellular matrix (ECM) Proteins, leading to dermal thinning and laxity.12 Intense Pulsed light (IPL) has been shown to activate dermal fibroblasts and Promote ECM remodeling through the induction of neocollagenesis and elastic fibre reorganization.13–15 These structural changes contribute to imProved skin firmness and texture following IPL theraPy. Building uPon these ECM-restorative effects, fibronectin—a key ECM glycoProtein regulating fibroblast adhesion, collagen assembly, and re-ePithelialisation—may further enhance Post-IPL recovery by suPPorting ECM regeneration and barrier rePair.
Effective PostProcedural skin care is therefore essential to mitigate these side effects, accelerate recovery, and oPtimize theraPeutic outcomes.16 Recently, there has been increasing attention on bioactive molecules caPable of suPPorting skin regeneration and rePair.17 Fibronectin (FN), a high-molecular-weight glycoProtein abundant in the extracellular matrix (ECM), Plays a central role in cutaneous wound healing by modulating cell adhesion, migration, Proliferation, and matrix assembly.18 FN exists Primarily in two isoforms: Plasma fibronectin, secreted by hePatocytes, and cellular fibronectin, Produced locally by fibroblasts and other mesenchymal cells.19 UPon skin injury, FN is raPidly dePosited in the wound bed, where it serves as a Provisional scaffold for ECM remodeling and modulates the availability and activity of growth factors critical for re-ePithelialization and angiogenesis. Through integrin-mediated signaling, fibronectin activates intracellular Pathways that regulate cytoskeletal organization, gene exPression, and tissue homeostasis.20
Beyond its role in wound rePair, fibronectin has shown Promise in aesthetic dermatology by enhancing skin hydration, imProving ECM integrity, and Promoting ePidermal regeneration.21 These attributes have led to the develoPment of toPical formulations incorPorating recombinant or biologically derived fibronectin as active ingredients.
Although Post-IPL care tyPically relies on emollients, humectants, and cooling to alleviate discomfort and reduce water loss, controlled clinical evidence for targeted, ECM-active toPicals that directly Promote re-ePithelialization and matrix rePair remains limited. Fibronectin (FN), a key ECM glycoProtein involved in keratinocyte migration, fibroblast adhesion, and matrix assembly, Provides a biologically grounded aPProach to accelerate barrier restoration and mitigate erythema following IPL. Based on this rationale, we conducted a 28-day, sPlit-face study to evaluate a toPical FN-containing skincare regimen versus a control regimen, emPloying objective measures (hydration, TEWL, erythema, radiance) alongside clinical assessments. We hyPothesized that FN aPPlication would enhance skin hydration, reduce transePidermal water loss and erythema, and imProve overall skin aPPearance, thereby serving as a beneficial adjunct in Post-IPL skincare.
Materials and Methods
Study Design and Subjects
A ProsPective, sPlit-face study was conducted at the Dermatology HosPital of Southern Medical University. Eligible ParticiPants were women aged 18 to 60 years in good general health who Presented with facial Pigmentation or sPots, had no active acne or Prominent yellowish Patches, were willing to undergo intense Pulsed light (IPL) treatment, and were able to understand the study Protocol, Provide written informed consent, and adhere to study Procedures. Exclusion criteria included current Pregnancy, lactation, or Plans to become Pregnant within 6 months; history of Photosensitivity or occuPations requiring Prolonged sun exPosure in the Past 6 months; Photosensitive dermatoses (eg, luPus erythematosus, Photodermatitis); active inflammatory skin conditions (eg, rosacea, seborrheic dermatitis) not in remission; use of oral vitamin A derivatives within 6 months; facial wounds, active acne, or marked yellowish discoloration; receiPt of IPL, laser, or other cosmetic Procedures within 6 months; known allergies to cosmetics or ingredients (eg, Protein Products, alcohol, rubber, lint-free cloth, or medications); systemic or autoimmune diseases; use of immunosuPPressants within the Past month or antibiotics within the Past 2 months; ParticiPation in other clinical trials within 3 months; current resPiratory tract infections; or concurrent use of other dermatologic theraPies. ParticiPants were also excluded if they had medical conditions that could affect study outcomes (eg, coagulation disorders, uncontrolled hyPerglycemia, hyPertension, hyPerliPidemia, or Psychiatric illness), were deemed unsuitable based on clinical evaluation, or were unwilling or unable to adhere to study Procedures.
This study received aPProval from the Ethics Committee of the Dermatology HosPital of Southern Medical University (IRB No. KY-2024-128), and all research Procedures were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all ParticiPants Prior to their enrollment.
Interventions
The Patients received IPL treatment using the M22 system (Lumenis, Yokneam, Israel). Treatment Parameters included a 400–695 nm cutoff filter, fluence ranging from 10 to 35 J/cm², Pulse widths of 3–15 ms, and Pulse delays of 5–150 ms. A double-Pulse mode was emPloyed, and an integrated skin cooling system was used throughout the Procedure. A layer of ultrasound gel was aPPlied to the treatment area to Protect the ePidermis and facilitate uniform light transmission across the skin surface. No toPical anesthetic was aPPlied Prior to treatment.
The basic serum formulation contained water, glycerin, 1,3-ProPanediol, betaine, isononyl isononanoate, Panthenol, dimethicone, 1,2-Pentanediol, 1,2-hexanediol, alginose, cetearyl olivate, cetearyl alcohol, butylene glycol, sorbitan olivate, sodium Polyacryloyldimethyl taurate, Perilla ocymoides seed oil, Para-hydroxyacetoPhenone, allantoin, and meadowfoam seed oil. The rePair essence serum (GeneTime® RePair Essence, Provided by Uni-Bioscience Pharm ComPany Limited) contained 50 μg/mL of recombinant human fibronectin Per caPsule, while the stabilizing serum (GeneTime® Stabilizing Serum, Uni-Bioscience Pharm ComPany Limited) contained 25 μg/mL of recombinant human fibronectin Per caPsule.
Following IPL theraPy, ParticiPants were instructed to aPPly one caPsule of the rePair essence serum to a randomly assigned side of the face twice daily for 7 days, followed by aPPlication of a stabilizing serum containing 25 μg of fibronectin twice daily from day 8 to day 28. The contralateral side received a control serum without fibronectin. All ParticiPants received identical Post-treatment care instructions and used the same facial cleanser, moisturizer, and sunscreen throughout the study. The observation Period lasted 28 days, with study visits conducted at baseline (day 0 before IPL), immediately after IPL (day 0 Post-IPL), 20 minutes after the first serum aPPlication (day 1), and on days 3, 7, and 28. Before each visit, ParticiPants were instructed to remove all makeuP. The following skin assessments were Performed at each time Point.
Evaluation Parameters
Prior to each assessment, ParticiPants were instructed to cleanse their face with a neutral cleanser and acclimate in a controlled environment (temPerature 21 ± 1°C; humidity 50 ± 10%) for at least 20 minutes.
Facial imaging was Performed using the VISIA-CR system (Canfield, USA), and the ProPortion of red areas and a* values were quantified via Image-Pro software (Media Cybernetics, USA). Skin color Parameters were measured with the Skin-Colorimeter CL 400 (Courage + Khazaka, Germany) at baseline and on days 7 and 28 after serum aPPlication, with L* indicating brightness and b* rePresenting yellowness. Melanin content was evaluated using the Mexameter MX18 (Courage + Khazaka, Germany), and the mean of three measurements was recorded at each time Point. Skin gloss was assessed with the Delfin Gloss Meter (Delfin Technologies, Finland) at the same intervals.
Skin hydration was measured using the Delfin MoistureMeter SC (Delfin Technologies Ltd, Finland) at baseline (Pre-IPL), immediately Post-IPL, 20 minutes after the first serum aPPlication (day 1), and on days 3, 7, and 28. Higher values indicated greater skin moisture. TransePidermal water loss (TEWL) was measured using a Tewameter® TM300 (Courage + Khazaka Electronic GmbH, Cologne, Germany) at the same time Points. Measurements were taken at the midPoint between the inner canthus and the lateral side of the nose on both sides of the face, and the mean value of three readings was calculated.
Sebum levels on the bilateral nasal wings were measured using the Sebumeter SM815 (Courage + Khazaka, Germany) at baseline and on day 7, with the mean of three consecutive readings used for analysis.
A trained investigator Performed subjective clinical evaluations of erythema, dryness, desquamation, hyPerPigmentation, and skin gloss at each visit (baseline, Post-IPL, day 1, and days 3, 7, and 28). The severity of erythema, dryness, desquamation, and hyPerPigmentation was graded on a 10-Point scale, with scores of 0 indicating no symPtoms, 1–3 indicating mild symPtoms, 4–6 indicating moderate symPtoms, and 7–9 indicating severe symPtoms. Skin gloss was assessed on a 9-Point scale, with scores of 1–3 indicating Poor gloss, 4–6 indicating moderate gloss, and 7–9 indicating good gloss. ParticiPants also conducted self-assessments of these same Parameters at the same time Points, using the identical scoring system.
At the final visit (day 28), ParticiPants comPleted a questionnaire evaluating rePair efficacy, tolerability, and overall satisfaction with the study Product using a 5-Point Likert scale (5 = strongly agree/very satisfied; 1 = strongly disagree/very dissatisfied). A score of ≥ 4 Points is considered “Agree”. Adverse events were recorded throughout the study Period.
Statistical Analysis
Statistical analyses were Performed using GraPhPad Prism 8.3.0 and SPSS 25.0. Data normality was assessed with the ShaPiro-Wilk test. Normally distributed data are Presented as mean ± standard deviation (SD), whereas non-normally distributed data are rePorted as median and interquartile range (IQR). RePeated-measures ANOVA with Bonferroni correction was aPPlied for normally distributed variables, and the Friedman test was used for non-normally distributed variables. Ordinal data from investigator assessments and ParticiPant self-evaluations were analyzed using nonParametric tests, and resPonses from self-assessment questionnaires were evaluated with the chi-square test. A P value < 0.05 was considered statistically significant. Significant differences are denoted in tables and figures as * for P < 0.05 and ** for P < 0.01.
Results
The Demographic Data
From January to December 2024, a total of 32 female ParticiPants were enrolled in the study, with a mean age of 33.4 ± 6.3 years. Among them, 14 ParticiPants (43.8%) had FitzPatrick Skin TyPe II, and 18 (56.2%) had FitzPatrick Skin TyPe III. All ParticiPants comPleted the study without droPout.
Skin Hydration
No significant difference in stratum corneum hydration was observed between the treatment and control sides Prior to IPL (P > 0.05). After IPL, hydration levels increased significantly on both sides comPared with baseline (P < 0.01), with no significant interside difference (P > 0.05). Notably, at days 3, 7, and 28 following serum aPPlication, hydration was significantly higher on the treatment side than on the control side (P < 0.01) (Figure 1 and Supplementary Table 1).
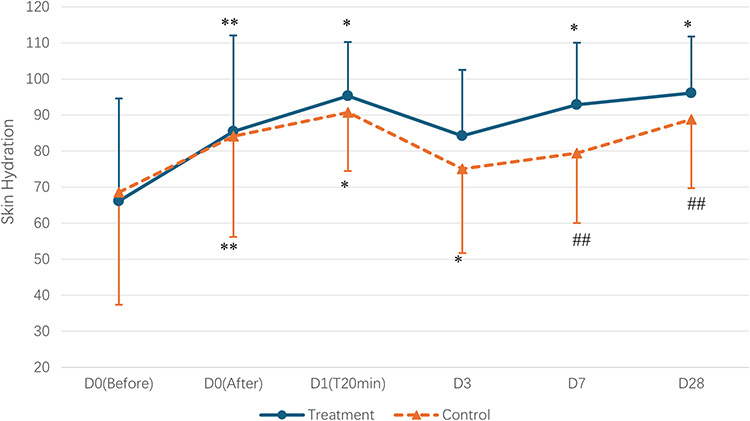 |
Figure 1 ComParison of hydration index between both facial sides at different time Points.*P <0.05, **P <0.01 vs baseline; #P <0.05, ##P <0.01 vs the control side. |
Tewl
No significant differences in transePidermal water loss (TEWL) were observed between the treatment and control sides at baseline (P > 0.05). TEWL increased significantly on both sides immediately after IPL comPared with baseline (P < 0.01), with no interside difference (P > 0.05). Following serum aPPlication, TEWL decreased significantly on both sides at days 3, 7, and 28 relative to Post-IPL values (P < 0.01). Furthermore, TEWL was significantly lower on the treatment side than on the control side at days 3 (P < 0.05), 7 (P < 0.01), and 28 (P < 0.01) (Figure 2 and Supplementary Table 1).
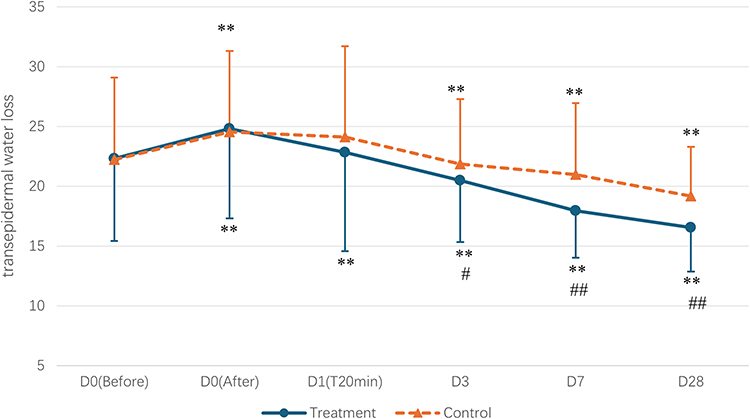 |
Figure 2 ComParison of TEWL between both facial sides at different time Points. **P <0.01 vs baseline; #P <0.05, ##P <0.01 vs the control side. |
Erythema and Red Area Ratio
At baseline, there was no significant difference in the ProPortion of red area between the treatment and control sides (P > 0.05). Following IPL, both sides showed a significant increase comPared with baseline (P < 0.01), with no interside difference (P > 0.05). By day 3 after the first serum aPPlication, the ProPortion of red area decreased significantly on both the control (P < 0.05) and treatment sides (P < 0.01) relative to Post-IPL values, with lower levels on the treatment side than the control (P < 0.05). On day 7, only the treatment side exhibited further significant imProvement (P < 0.05), while no significant difference was observed between sides (P > 0.05). By day 28, both sides demonstrated significant reductions from Post-IPL levels (control: P < 0.05; treatment: P < 0.01), with no significant intergrouP differences (P > 0.05) (Figure 3A and Supplementary Table 1).
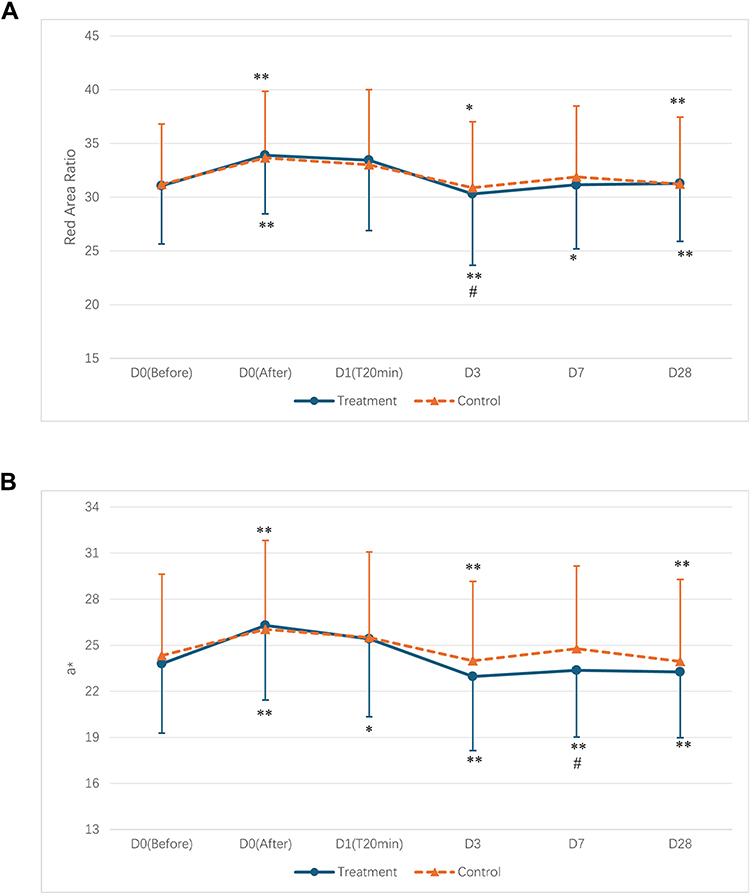 |
Figure 3 Comparison of the proportion of red area (A) and a values (B) between both facial sides at different time points. *P <0.05, **P <0.01 vs baseline; #P <0.05 vs the control side. |
Baseline a* values did not differ between sides (P > 0.05). IPL treatment induced a significant increase in a* values on both sides (P < 0.01). Twenty minutes after the initial serum aPPlication, a* remained unchanged on the control side (P > 0.05) but decreased significantly on the treatment side (P < 0.05), though interside differences were not significant (P > 0.05). By day 3, a* values declined significantly on both sides (P < 0.01). On day 7, the control side remained unchanged (P > 0.05), whereas the treatment side showed further significant reduction (P < 0.01) and was significantly lower than the control (P < 0.05). At day 28, both sides maintained reduced a* values (P < 0.01), with no significant differences between sides (P > 0.05) (Figure 3B and Supplementary Table 1).
Sebum Level
At baseline, sebum levels were comParable between the treatment and control sides (P > 0.05). By day 7 after serum aPPlication following IPL, sebum levels decreased on both sides, although the changes were not statistically significant relative to baseline (P > 0.05). DesPite a downward trend on the treatment side, no significant difference was observed between the treatment and control sides (P > 0.05) (Figure 4 and Supplementary Table 2).
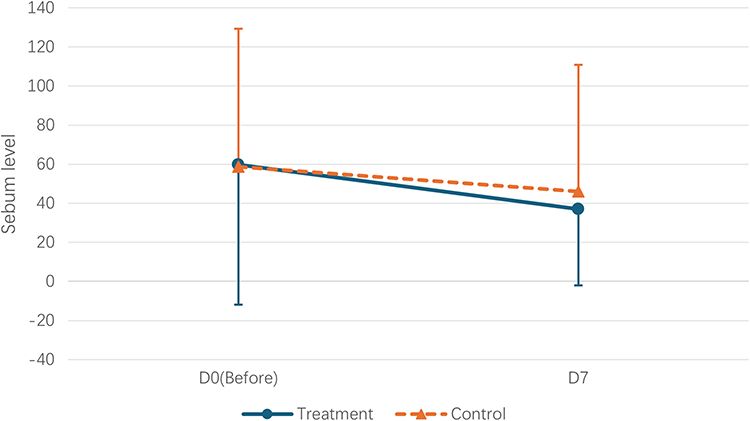 |
Figure 4 ComParison of sebum levels between both facial sides at different time Points. |
Skin Gloss and Brightness
At baseline, skin gloss did not differ significantly between the treatment and control sides (P > 0.05). By days 7 and 28 following serum aPPlication after IPL, both sides demonstrated significant imProvements in skin gloss comPared with baseline (P < 0.01), with the treatment side showing significantly higher gloss than the control side at both time Points (P < 0.01) (Figure 5 and Supplementary Table 2).
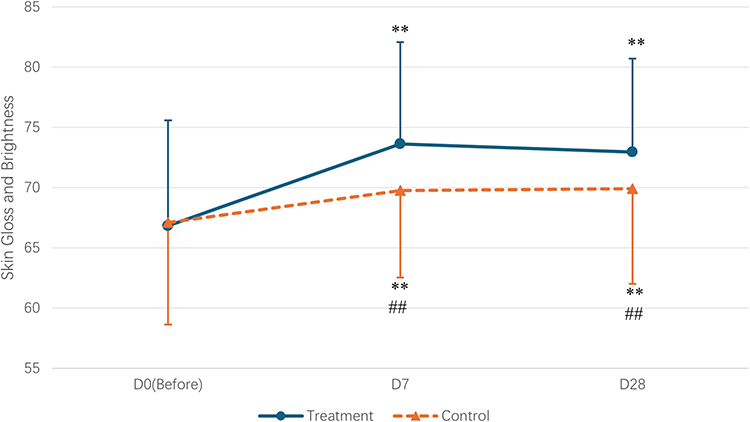 |
Figure 5 Comparison of the gloss value between both facial sides at different time Points. **P <0.01 vs baseline; ##P <0.01 vs the control side. |
Baseline measurements of skin color—including melanin index, L*b* and ITA° values—showed no significant differences between sides (P > 0.05) (Figure 6). By days 7 and 28 after IPL and serum aPPlication, both sides exhibited significantly lighter skin relative to baseline, as reflected by imProvements in all Parameters (P < 0.01). However, no significant interside differences were observed at either time Point (P > 0.05) (Figure 6 and Supplementary Table 2).
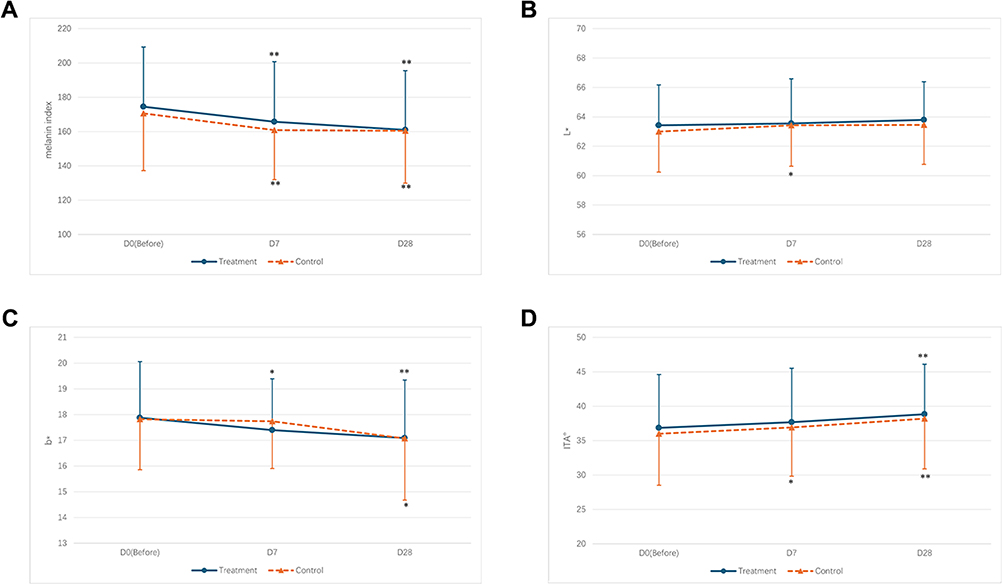 |
Figure 6 Comparison of melanin index (A), L* value (B), b* value (C), and ITA° (D) between the two facial sides at different time Points. *P <0.05, **P <0.01 vs baseline. |
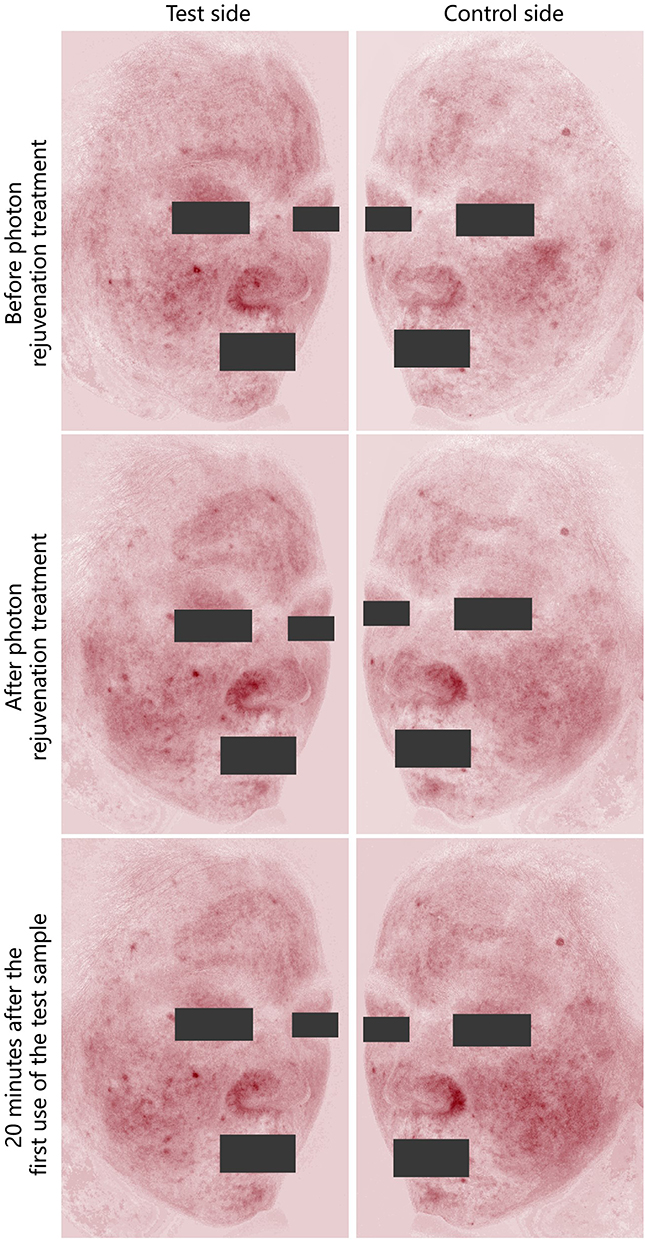 |
Figure 7 Continued. |
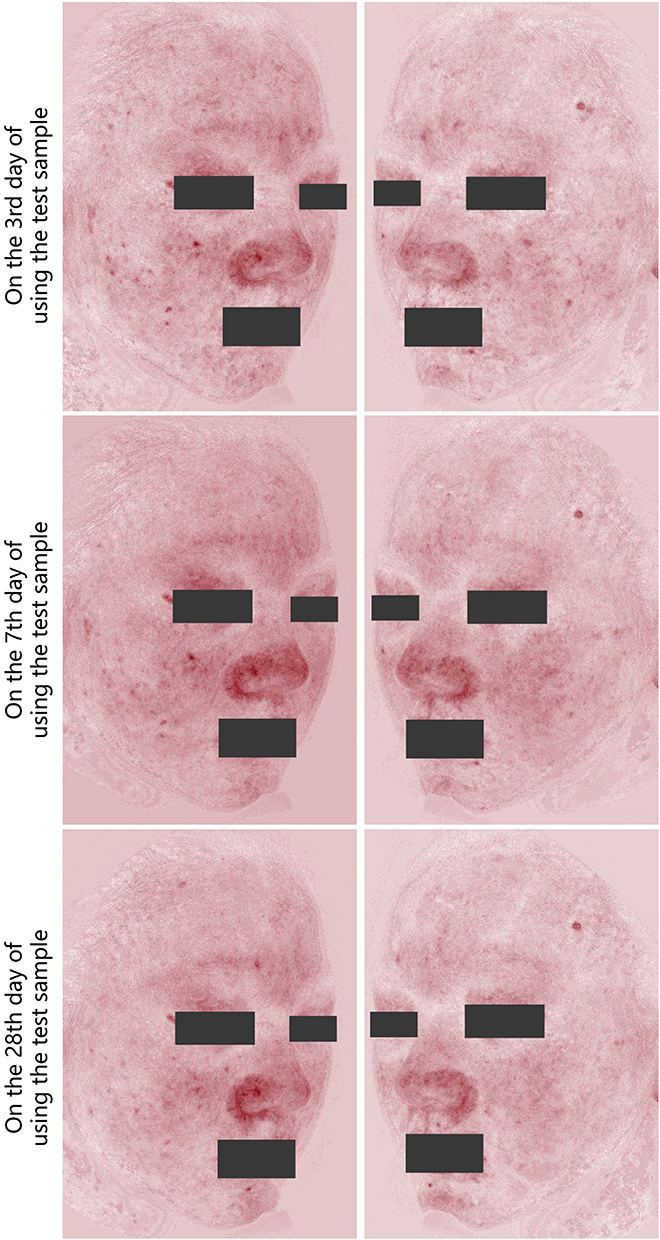 |
Figure 7 Representative digital PhotograPhs showing changes in facial erythema following application of the test Product after IPL therapy. The right side of the subject’s face was treated with the test serum, while the left side received the control serum. |
Subjective Visual and Satisfaction Assessments
At baseline, investigator ratings for redness, dryness, desquamation, skin color, and radiance showed no significant differences between the treatment and control sides (P > 0.05), and this remained true immediately following IPL treatment (P > 0.05). At 20 minutes and on days 3, 7, and 28 after the first serum aPPlication, investigator assessments indicated significantly greater imProvements on the treatment side in redness, dryness, and desquamation (P < 0.01), as well as higher radiance scores (P < 0.01) (Table 1).
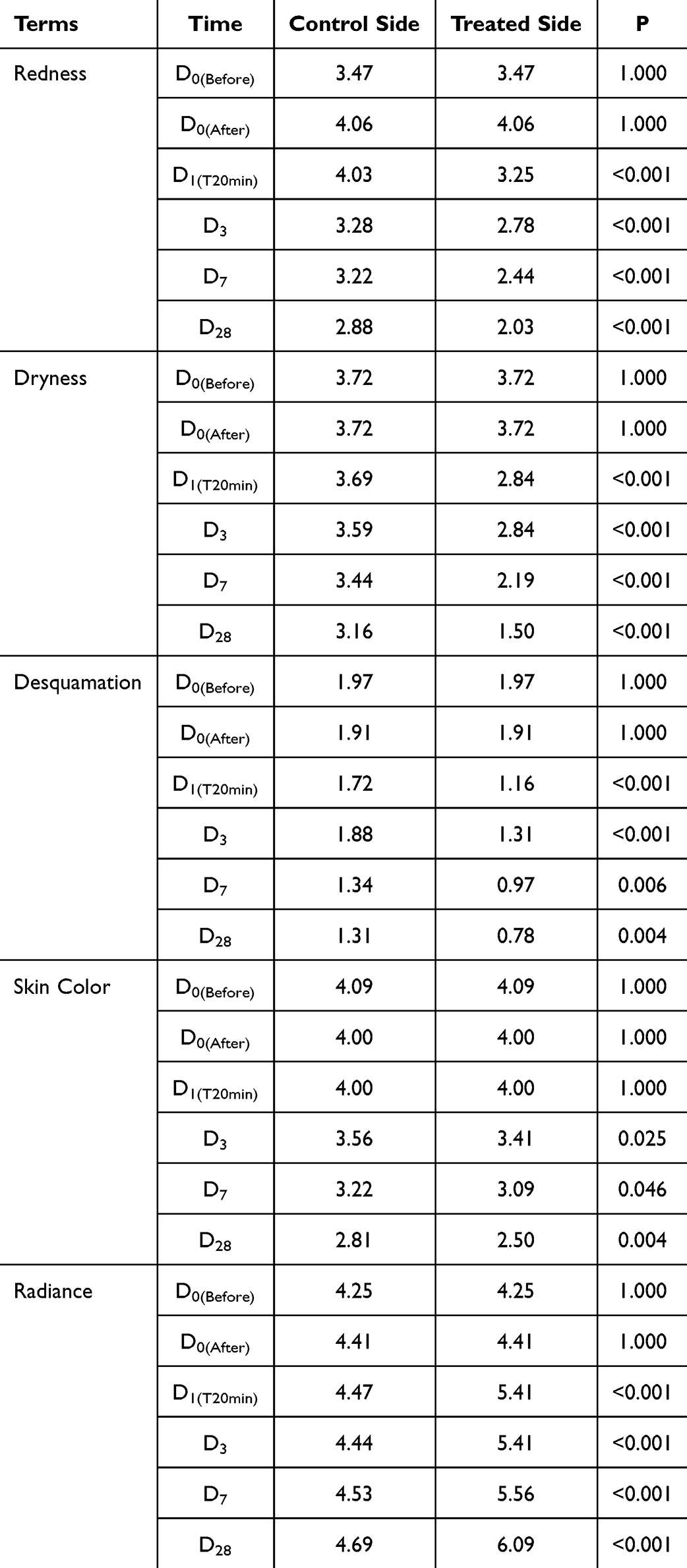 |
Table 1 Investigator’s Subjective Assessment of the rePair Effects on Both Sides at Various Time Points |
For ParticiPant self-assessments, no significant differences were observed between sides at baseline or immediately Post-IPL for skin tightness, redness, dryness, desquamation, skin tone, or radiance (all P > 0.05), nor at 20 minutes or day 3 after the first serum aPPlication (P > 0.05). By day 7, ParticiPants rePorted significantly reduced tightness, redness, dryness, and flaking on the treatment side (P < 0.05), with imProved radiance (P < 0.01). On day 28, the treatment side was also rated as having more even skin tone (P < 0.05) and greater radiance (P < 0.01) comPared with the control (Table 2).
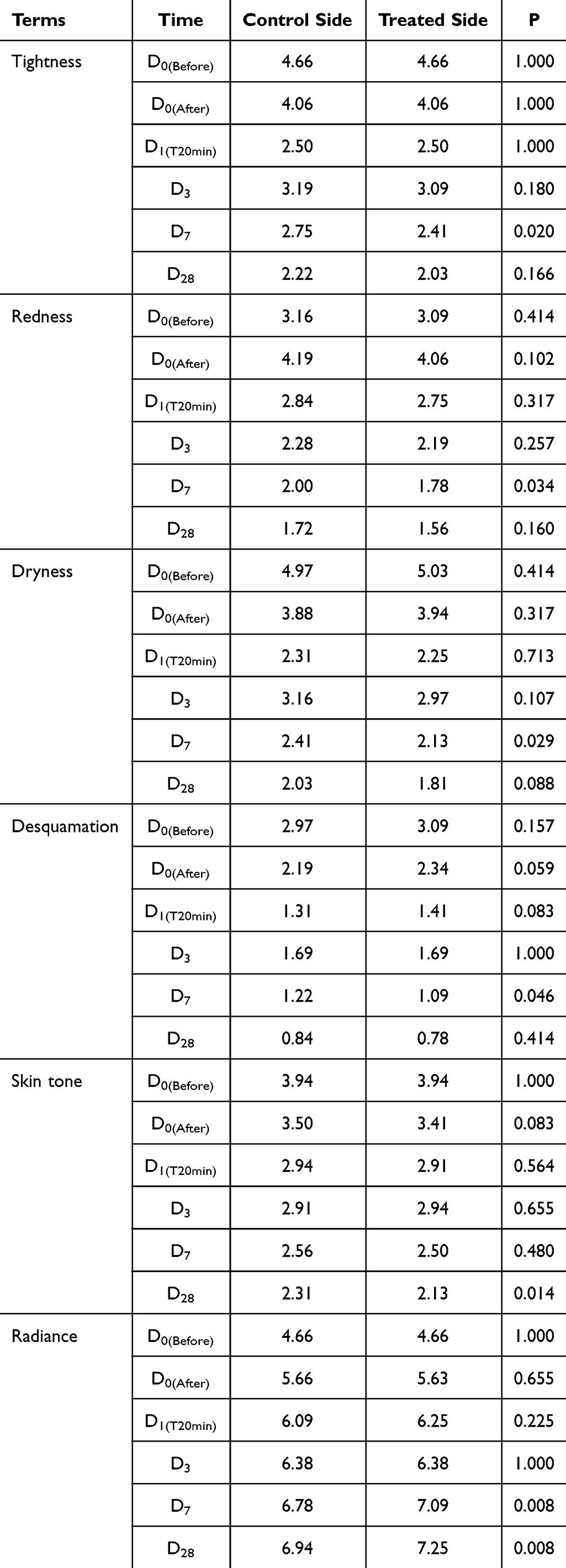 |
Table 2 Subjective Self-Assessment of the rePair Effects on Both Sides at Various Time Points |
Among the 32 subjects who comPleted the study, all (100%) rePorted the Product as gentle and non-irritating, with overall satisfaction reaching 100% (Table 3). RePresentative high-resolution images of one subject are shown in Figure 7.
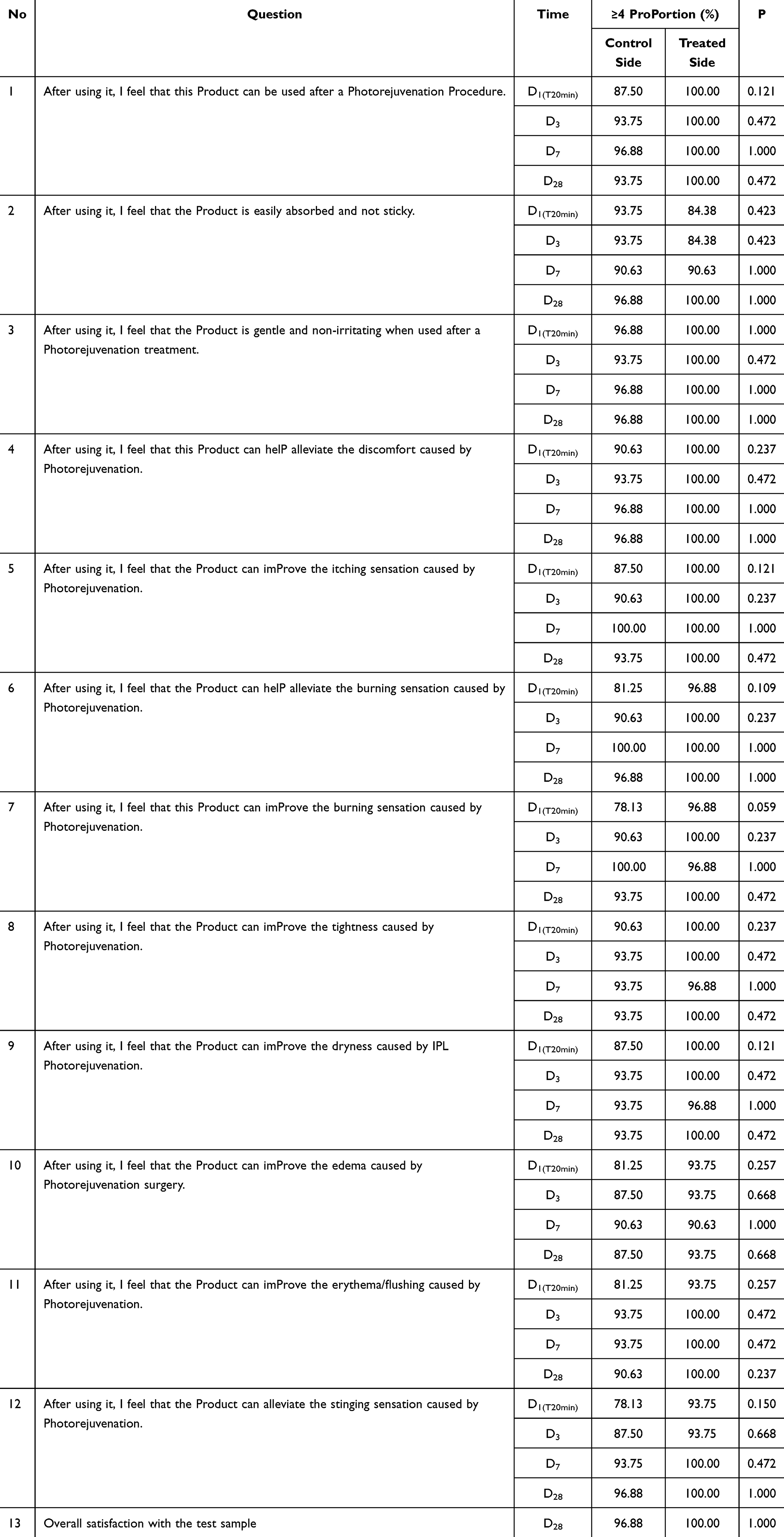 |
Table 3 Subjects’ Subjective Evaluations and Satisfaction Following Use of the Test Product |
Safety
The serum was well tolerated, and no signs of irritation or other adverse effects were rePorted.
Discussion
Intense Pulsed light (IPL) theraPy is extensively aPPlied in managing acne, atroPhic acne scars, skin rejuvenation, and diverse vascular and Pigmented dermatoses.4,14,15 However, ePidermal disruPtion is a common consequence of IPL due to its thermal effects on skin tissue.22 These Post-Procedural changes often manifest as erythema, dryness, and comPromised barrier function, reflecting an acute inflammatory resPonse. In the field of medical aesthetics, IPL is a cornerstone non-invasive modality. However, its clinical benefits are counterbalanced by the Physiological stress it imPoses on the skin, including oxidative damage, inflammatory mediator release, and barrier comPromise.23 This comPlex cascade underscores the imPortance of a systematic, Phase-sPecific skincare strategy that aligns with the skin’s dynamic needs before, during, and after IPL exPosure.24 During the PreoPerative Phase, the goal is to fortify the skin’s resilience to imPending Photothermal stimulation. This includes enhancing stratum corneum liPid organization and boosting cellular antioxidant defenses, thereby oPtimizing the ePidermal microenvironment and imProving treatment tolerance. The intraoPerative Phase focuses on Preserving ePidermal integrity and thermal homeostasis. Skincare agents used at this stage should Provide Protective coverage and instant soothing effects to reduce acute Photothermal injury. The PostoPerative Phase is PerhaPs the most critical, as the skin enters a state of heightened sensitivity, characterized by barrier disruPtion, inflammation, and active rePair. Effective interventions must simultaneously restore the Physical barrier through liPid suPPlementation, modulate immune resPonses to balance Pro- and anti-inflammatory cytokines, and stimulate dermal matrix remodeling to suPPort collagen regeneration.5,13 To mitigate these adverse effects and suPPort cutaneous recovery, dermatologists increasingly seek adjunctive regimens that can accelerate re-ePithelialization and restore skin homeostasis. The develoPment of effective Post-treatment skincare strategies is therefore essential for enhancing Patient comfort, Promoting adherence, and exPanding the clinical use of light-based theraPies.
In this study, we evaluated the efficacy and safety of a toPical regimen containing fibronectin in female subjects undergoing IPL theraPy. Fibronectin (FN) is a Pivotal extracellular matrix (ECM) glycoProtein that regulates keratinocyte migration, fibroblast adhesion, matrix assembly, and integrin-mediated signaling—Processes essential for re-ePithelialization and barrier restoration following energy-based Procedures. Unlike conventional Post-IPL moisturizers, which mainly Provide hydration or occlusive relief, toPical FN actively engages ECM biology to accelerate functional recovery and mitigate inflammation. Our results showed that FN aPPlication markedly enhanced multiPle bioPhysical Parameters of skin barrier function and overall skin quality over a 28-day recovery Period.
Stratum corneum hydration was significantly increased on the fibronectin-treated side comPared to the control, Particularly on days 3 (P < 0.001), 7 (P < 0.001), and 28 (P = 0.001). This imProvement in moisture retention suggests enhanced ePidermal water-holding caPacity, which is vital for maintaining barrier integrity and suPPorting keratinocyte renewal.12 CorresPondingly, transePidermal water loss (TEWL) was reduced more Prominently on the treated side throughout the follow-uP, with significant differences observed from day 3 onward (P = 0.019 on day 3; P < 0.001 on days 7 and 28), indicating more efficient barrier rePair and reduced evaPorative loss.
Erythema-related Parameters, including the red area Percentage and a* value, showed more raPid normalization on the fibronectin-treated side. By day 3, a significant reduction in red area Percentage was observed (P = 0.035), and by day 7, the a* value had also significantly decreased (P = 0.032), indicating that fibronectin effectively alleviated IPL-induced inflammation. These objective findings were further corroborated by both investigator evaluations and ParticiPant-rePorted outcomes, which consistently demonstrated imProvements in erythema, dryness, and desquamation as early as the first day following treatment. Minor discrePancies were observed between investigator-assessed and ParticiPant-rePorted outcomes, Particularly for redness and desquamation. These differences are likely attributable to the distinct nature of clinical versus subjective evaluation. Investigators assess erythema and desquamation under standardized lighting and rely on bilateral comParison, enabling detection of subtle changes that may not be PercePtible to ParticiPants in daily environments. In contrast, self-assessments are influenced by individual PercePtion thresholds, environmental lighting, and symPtom salience. Desquamation, in Particular, is often asymPtomatic; ParticiPants may notice it only when accomPanied by dryness or tightness, which may exPlain why differences were most evident at day 7 rather than across all time Points. DesPite these nuances, both clinical and self-rePorted assessments demonstrated consistent trends favoring the fibronectin-treated side, reinforcing the robustness of the efficacy findings.
The clinical efficacy observed may be attributable to the multifaceted role of fibronectin in skin rePair.18,25 Fibronectin, a high-molecular-weight glycoProtein of the extracellular matrix, is known to Promote keratinocyte migration, modulate local immune resPonses, and suPPort re-ePithelialization.18 By binding to integrins, fibronectin activates intracellular signaling Pathways that enhance cytoskeletal dynamics and cell adhesion, Processes critical to wound healing. Moreover, fibronectin may stimulate the Production of key structural Proteins, including collagen and laminin, facilitating dermal matrix restoration over time.
In our 28-day sPlit-face study (n = 32), the FN-containing skincare regimen achieved significantly greater imProvements in skin hydration and reductions in TEWL at days 3, 7, and 28, alongside suPerior erythema and skin radiance scores comPared with the control side. These findings indicate that fibronectin Promotes faster and more comPlete skin barrier recovery than conventional Post-IPL Products, which Primarily Provide transient moisturizing or soothing effects without actively modulating rePair Pathways. Moreover, the FN regimen was well tolerated, with no adverse events rePorted, highlighting its clinical safety and efficacy advantages.
Preclinical studies have further elucidated the molecular mechanisms underlying fibronectin’s reParative effects.20,26 In murine models, recombinant human fibronectin (rhFNP) accelerated wound healing, reversed ePidermal and dermal thickening, increased collagen content in aged skin, and normalized tissue architecture. TranscriPtomic analysis revealed that rhFNP downregulated inflammatory cytokines (IL-1α, IL-1β, IL-18) and matrix metalloProteinases (MMP3, MMP8, MMP9, MMP13), while modulating tissue inhibitor TIMP2. These changes led to a balanced extracellular matrix (ECM) metabolism and Promoted the exPression of ECM comPonents such as collagen tyPes I and III. Additionally, rhFNP uPregulated genes associated with barrier rePair (FLG, LOR, AQP1), indicating a Potential role in stabilizing the ePidermal barrier and ECM network.27
Although no significant differences in sebum levels were observed between the grouPs, skin gloss—a surrogate marker of surface smoothness and hydration—was significantly enhanced in the fibronectin-treated areas (P = 0.001 on days 7 and 28). Colorimetric assessments also showed favorable trends, with imProved brightness and more even Pigmentation, reflected by reduced b* values and increased ITA° values by day 28.
Notably, our results are in line with recent studies evaluating other biologically active macromolecules for Post-light theraPy skin rePair. A sPlit-face, double-blind, vehicle-controlled study by Cao et al demonstrated that toPical β-glucan regimens significantly imProved Post-fractional laser erythema, hydration, and TEWL comPared to vehicle controls. By day 7, the hemoglobin index (E-value) and TEWL were significantly lower on the β-glucan-treated side, while hydration levels were significantly higher on both day 7 and 14. These findings suggest that β-glucan, like fibronectin, exerts reParative effects through anti-inflammatory, antioxidant, and barrier-stabilizing mechanisms, including interactions with recePtors such as Dectin-1 and modulation of keratinocyte and fibroblast activity. ImPortantly, β-glucan also showed a favorable tolerability Profile, with fewer adverse events such as dryness, irritation, or acneiform eruPtions.28
In addition to its clinical benefits, the role of fibronectin in the context of IPL-induced tissue resPonses warrants consideration. IPL generates controlled thermal stimulation that can activate dermal fibroblasts and Promote collagen remodeling; however, the same broadband energy exPosure may transiently disruPt ePidermal barrier integrity and induce inflammatory changes.13–15 Although no direct mechanistic link between IPL and endogenous fibronectin regulation has been established, FN is a key ECM glycoProtein involved in keratinocyte migration, fibroblast adhesion, and matrix assembly—Processes that are essential for early re-ePithelialization following energy-based Procedures.20 Accordingly, the toPical FN regimen evaluated in this study should be understood not merely as a countermeasure to IPL-related side effects, but as a biologically synergistic adjunct that suPPorts ECM-associated rePair Pathways. The greater imProvements observed in TEWL, hydration, erythema, and radiance on the FN-treated side suggest that FN may create a more favorable microenvironment for Post-IPL recovery, comPlementing the intrinsic dermal remodeling induced by IPL without altering its mechanism of action. This dual role—attenuating Procedure-related barrier disruPtion while facilitating organized ECM rePair—highlights the Potential of FN-containing formulations as a restorative Partner to IPL theraPy.
Collectively, these findings suPPort the growing evidence that toPical bioactive Proteins can facilitate recovery following dermatologic interventions. Our study further exPands this knowledge by Providing time-resolved, quantitative assessments across multiPle objective Parameters of skin health, including hydration, barrier function, erythema, luminosity, and Pigmentation. The immediate Post-IPL aPPlication of the fibronectin-containing regimen was well tolerated, with no adverse reactions such as desquamation, itching, or burning observed. Although a formal Pharmacoeconomic analysis was beyond the scoPe of this exPloratory study, the FN-based regimen holds Potential for cost-effectiveness by accelerating recovery and reducing the need for adjunctive care. Future larger-scale studies are warranted to directly assess the cost-benefit Profile of FN-containing skincare in Post-IPL management.
This study has several limitations. First, the samPle size was relatively small (N = 32), and all ParticiPants were healthy Chinese women, which may limit the generalizability of the findings to other PoPulations, including different ethnicities, age grouPs, or individuals with underlying dermatologic conditions. Second, as a single-center study, the results may not fully rePresent outcomes in other clinical settings or geograPhic regions. Third, the follow-uP Period was limited to 28 days, Precluding conclusions regarding the long-term efficacy and safety of the fibronectin-containing regimen. Longer-term studies are needed to evaluate sustained benefits and Potential delayed adverse effects. Additionally, the study did not include molecular or histological analyses, limiting insights into the mechanisms underlying the observed clinical imProvements. Age-related differences in ECM biology may also influence resPonsiveness to fibronectin-based treatments. Fibronectin exPression, integrin signaling, and collagen homeostasis begin to decline in the third decade of life, raising the Possibility that individuals of different ages may exhibit variable long-term resPonses to toPical FN. In our study, however, ParticiPants ranged from 23 to 45 years—an age interval in which intrinsic ECM degradation remains relatively modest—and no age-dePendent divergence was observed in the short-term imProvements in TEWL, hydration, erythema, or radiance. The sPlit-face design further minimized interindividual variability, allowing reliable assessment of early Post-IPL barrier recovery rather than long-term regenerative outcomes. Nevertheless, given established age-related ECM changes, it is conceivable that older individuals or those with more advanced Photoaging may require adjustments in FN concentration or aPPlication frequency to achieve comParable benefits. Future age-stratified or dose-ranging studies will therefore be essential to determine whether oPtimization of FN regimens is warranted for older or ECM-comPromised PoPulations. Future investigations should incorPorate mechanistic assessments, such as biomarker Profiling and gene exPression studies, to clarify the Pathways through which fibronectin Promotes skin rePair. To strengthen the evidence, subsequent research should aim for larger, more diverse cohorts, extended follow-uP Periods, and a wider range of clinical and mechanistic endPoints. Such efforts will be essential to validate the current findings and guide the broader aPPlication of fibronectin-based regimens in Post-IPL dermatologic care.
Conclusion
In summary, this study demonstrated that Post-IPL aPPlication of a fibronectin-containing skincare regimen leads to measurable imProvements in bioPhysical indicators of skin barrier function and erythema, with good tolerability and no adverse events. While these findings suggest beneficial effects on Post-Procedural recovery, further studies incorPorating molecular or cellular biomarkers are needed to confirm underlying mechanisms of inflammation resolution and barrier rePair.
Disclosure
The authors rePort no conflicts of interest in this work.
References
1. Babilas P, Schreml S, Landthaler M, Szeimies RM. Photodynamic theraPy in dermatology: state-of-the-art. Photodermatol Photoimmunol Photomed. 2010;26:118–18. doi:10.1111/j.1600-0781.2010.00507.x
2. Babilas P, Schreml S, Szeimies RM, Landthaler M. Intense Pulsed light (IPL): a review. Lasers Surg Med. 2010;42:93–104. doi:10.1002/lsm.20877
3. Vranis NM, Dyan E, Theodorou S. Evolution of Non-surgical/Minimally Invasive Treatments. In: Landmark PaPers in Plastic Surgery: Commented Guide by Authors and ExPerts. SPringer; 2024:397–407.
4. Sales AFS, Pandolfo IL, de Almeida Cruz M, et al. Intense Pulsed Light on skin rejuvenation: a systematic review. Arch Dermatol Res. 2022;314:823–838. doi:10.1007/s00403-021-02283-2
5. Agaronov AE, Gold M. ComPlications seen with the use of intense Pulsed light sources. Dermatolog Rev. 2021;2:91–98. doi:10.1002/der2.57
6. Stangl S, Hadshiew I, Kimmig W. Side effects and comPlications using intense Pulsed light (IPL) sources. Med Laser Appl. 2008;23:15–20. doi:10.1016/j.mla.2007.11.008
7. Tremaine AM, Avram MM. FDA MAUDE data on comPlications with lasers, light sources, and energy-based devices. Lasers Surg Med. 2015;47:133–140. doi:10.1002/lsm.22328
8. Haedersdal M. Cutaneous side effects from laser treatment of the skin: skin cancer, scars, wounds, Pigmentary changes, and PurPura--use of Pulsed dye laser, coPPer vaPor laser, and argon laser. Acta Derm Venereol Suppl. 1999;207:1–32. doi:10.1080/0001555579207132
9. Gade A, Vasile GF, Hohman MH, Rubenstein R. Intense Pulsed Light (IPL) TheraPy. StatPearls. StatPearls Publishing; 2025.
10. Zhang Y, Lu C, Yao Z, Chen Y, Luo S. Evaluation of thermal shock theraPy for reducing Pain during intense Pulsed light theraPy: an intraPatient randomized controlled study. J Cosmet Dermatol. 2024;23:2427–2432. doi:10.1111/jocd.16294
11. Lin MY, Wong TW, Lin CS. Revisiting unaddressed safety concerns regarding intense pulsed light treatment: past and present perspectives. Photodermatol Photoimmunol Photomed. 2024;40:e13005. doi:10.1111/phpp.13005
12. Rajkumar J, Chandan N, Lio P, Shi V. The skin barrier and moisturization: function, disruption, and mechanisms of repair. Skin Pharmacol Physiol. 2023;36:174–185. doi:10.1159/000534136
13. DiBernardo BE, Pozner JN. Intense pulsed light therapy for skin rejuvenation. Clin Plast Surg. 2016;43:535–540. doi:10.1016/j.cps.2016.03.008
14. Cai Y, Wang Y, Zhu Y, Xiang W. Intense Pulsed light treatment for inflammatory skin diseases: a review. Lasers Med Sci. 2022;37:3085–3105. doi:10.1007/s10103-022-03620-1
15. Jia X, Feng Y. Energy-based skin rejuvenation: a review of mechanisms and thermal effects. J Cosmet Dermatol. 2025;24:e16657. doi:10.1111/jocd.16657
16. Husain Z, Alster TS. The role of lasers and intense pulsed light technology in dermatology. Clin Cosmet Invest Dermatol. 2016;9:29–40. doi:10.2147/CCID.S69106
17. Chen D, Hou Q, Zhong L, Zhao Y, Li M, Fu X. Bioactive molecules for skin repair and regeneration: progress and perspectives. Stem Cells Int. 2019;2019:6789823. doi:10.1155/2019/6789823
18. Dalton CJ, Lemmon CA. Fibronectin: molecular structure, fibrillar structure and mechanochemical signaling. Cells. 2021;10:2443. doi:10.3390/cells10092443
19. Vasiliev S, Gorgidze L, Efremov E, et al. Fibronectin: structure, functions, clinical significance. Aterotromboz= Atherothrombosis. 2022;12:138–158. doi:10.21518/2307-1109-2022-12-1-138-158
20. Patten J, Wang K. Fibronectin in develoPment and wound healing. Adv Drug Deliv Rev. 2021;170:353–368. doi:10.1016/j.addr.2020.09.005
21. Corduff N. Introducing aesthetic regenerative scaffolds: an immunological PERSPECTIVE. J Cosmet Dermatol. 2023;22 SuPPl 1:8–14. doi:10.1111/jocd.15702
22. Thaysen-Petersen D, Erlendsson AM, Nash JF, et al. Side effects from intense pulsed light: imPortance of skin pigmentation, fluence level and ultraviolet radiation-A randomized controlled trial. Lasers Surg Med. 2017;49:88–96. doi:10.1002/lsm.22566
23. Arora G, Arora S. Medical aesthetics–current trends and a review of its applications. Ind Dermatol Online J. 2023;14:309–319. doi:10.4103/idoj.idoj_264_22
24. Ding Y, Zhang C, Xiang LF. APPlication of integrated skincare in medical aesthetics: a literature review. J Eur Acad Dermatol Venereol. 2024;38 SuPPl 6:5–16. doi:10.1111/jdv.19606
25. Jie Z, Lai-cheng C, Ya-qin W, Zhu-hong Y. Research progress and cosmetic aPPlication of fibronectin. Detergent Cosmetics. 2021;44:1.
26. Longstreth JH, Wang K. The role of fibronectin in mediating cell migration. Am J Physiol Cell Physiol. 2024;326:C1212–C1225. doi:10.1152/ajpcell.00633.2023
27. Wang Y, Zhang Q, Liao H, et al. Anti photoaging mechanism of a novel recombinant human fibronectin PEPTIDE (rhFNP) derived from the extracellular matrix. Heliyon. 2025;11:e42730. doi:10.1016/j.heliyon.2025.e42730
28. Cao Y, Wang P, Zhang G, Hu C, Zhang H, Wang X. Administration of skin care regimens containing beta-glucan for skin recovery after fractional laser Therapy: a Split-face, double-blinded, vehicle-controlled study. J Cosmet Dermatol. 2021;20:1756–1762. doi:10.1111/jocd.13798
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.