Back to Journals » International Journal of Women's Health » Volume 14
Fetoscopic Laser Ablation for the Selective Fetal Reduction in Twin-Twin Transfusion Syndrome Stage II–IV: The Experience of a New Fetal Medicine Center
Authors Anh ND, Hung HS ![]() , Sim NT, Ha NTT, Nguyen DL, Bac ND, Tong HV, Ville Y, Thuong PTH
, Sim NT, Ha NTT, Nguyen DL, Bac ND, Tong HV, Ville Y, Thuong PTH
Received 20 November 2021
Accepted for publication 18 March 2022
Published 14 April 2022 Volume 2022:14 Pages 555—563
DOI https://doi.org/10.2147/IJWH.S350433
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Nguyen Duy Anh,1,2 Ho Sy Hung,2 Nguyen Thi Sim,1 Nguyen Thi Thu Ha,3 Duc Lam Nguyen,2 Nguyen Duy Bac,4 Hoang Van Tong,5 Yves Ville,6 Phan Thi Huyen Thuong2,7
1Fetal Medicine Centre, Hanoi Obstetrics and Gynecology Hospital, Hanoi, Vietnam; 2Hanoi Medical University, Hanoi, Vietnam; 3Department of Assisted Reproductive and Andrology, Hanoi Obstetrics and Gynecology Hospital, Hanoi, Vietnam; 4Department of Education and Training, Vietnam Military Medical University, Hanoi, Vietnam; 5Biomedical and Pharmaceutical Applied Research Center, Vietnam Military Medical University, Hanoi, Vietnam; 6Department of Obstetrics and Fetal Medicine at Necker-Enfants-Malades Hospital at the Paris Descartes University, Paris, France; 7Department of Delivery, Hanoi Obstetrics and Gynecology Hospital, Hanoi, Vietnam
Correspondence: Phan Thi Huyen Thuong, Hanoi Medical University, Hanoi, Vietnam, Tel +84 989 330139, Email [email protected]
Objective: To evaluate the surgery outcomes of fetoscopic laser ablation (FLA) for selective umbilical cord in treating twin-twin transfusion syndrome (TTTS) with special conditions and neonatal outcomes post-operation.
Methods: A prospective study, 21 monochorionic diamniotic (MCDA) twins diagnosed with TTTS stage II–IV according to Quintero classification from 16 to 26 weeks of gestation, among that, 12 cases of TTTS stage II with selective intrauterine growth restriction (sIUGR), 6 cases of TTTS stage II with proximate cord insertions, 3 cases of TTTS stage IV underwent fetoscopic laser ablation for the selective fetal reduction at Hanoi Obstetrics and Gynecology Hospital from September 2019 to July 2021. Complications and surgical outcomes were noted. Prenatal care was carried out every 2 weeks post operation until birth. Newborn neurologic complications were assessed at birth, three months, and six months after birth using Denver II test and magnetic resonance imaging (MRI).
Results: The mean gestational age at operation was 20.30 weeks. The average operation duration was 39.52 minutes. No complications of operation, such as bleeding or infection, were recorded. The mean gestational age at birth was 34.70 ± 4.33 weeks, with a mean duration of 12.97 ± 6.87 weeks between intervention and delivery. The survival rate of newborns after the operation was 90.48%. There were two stillbirths (9.52%) within seven days after the operation. No short-term neurological complications have been reported with follow-up of the newborn to 6 months after birth.
Conclusion: Our study showed that fetoscopic laser ablation of selected fetal reduction surgery for treatment of special conditions of TTTS had no complications of operation, high neonatal survival result (90.48%), no short-term neurological complications. This should be considered for TTTS in cases of indication.
Keywords: laser ablation, selective fetal reduction, twin-twin transfusion syndrome, new fetal medicine center
Introduction
Monochorionic diamniotic (MCDA) twins are high-risk pregnancies with many complications, the most frequent of which is twin-twin transfusion syndrome (TTTS), affecting approximately 15% of MCDA twins.1,2 TTTS is associated with up to 90% neonatal mortality and neurological complications in 20% of surviving co-twin if left untreated.1–3 With the purpose of improved outcomes, various treatment modalities have been developed, including amnioreduction, septostomy, selective fetal reduction, and fetoscopic laser surgery (FLS).2,4–6 Among them, FLS coagulates the placental vascular anastomoses, prevents blood transfusion between the two fetuses, and saves both twins’ lives. It emerges as the first option in the TTTS treatment.7–9 However, in some cases, selective pregnancy reduction is the preferred choice to save the life of at least one fetus with a better prognosis, such as stage IV of TTTS, TTTS with selective intrauterine growth restriction (sIUGR), and in cases where FLS cannot be performed as proximate cord insertions.8–10 Selective fetal reduction with many techniques is used today, such as bipolar cord coagulation (BCO), radiofrequency ablation (RFA), fetoscopic laser ablation (FLA), and most recently, high energy focused ultrasound (HIFU).8,11 The two most commonly used techniques for selective fetal reduction are BCO and RFA.12–14 More recent reports have suggested that BCO is associated with an increasing risk of preterm premature rupture of membranes (PPROM) and preterm labor compared to RFA.13,15–17 However, RFA faces a decrease in the overall survival rate, and occasionally, the technique is unavailable.13,15–17 HIFU is a non-invasive treatment that has still been studied in clinical trials and has initially shown some positive results.8 To date, there has been a lack of reporting data on FLA for the selective fetal reduction in treating TTTS.8,9 Our fetal intervention center, established in 2019, has carried out the fetoscopic laser to treat TTTS, and we do not have RFA. Therefore, this study aimed to report the results of TTTS treatment using FLA for the selective fetal reduction in special cases, including surgical and neonatal outcomes after surgery.
Materials and Methods
Study Populations
This prospective study was carried out from September 2019 to July 2021 at Hanoi Obstetrics, and The Ethics Committee approved gynecology hospital, Hanoi, Vietnam, and of the Hospital and Hanoi Medical University.
Inclusion criteria were MCDA twins with TTTS gestational age from 16 to 26 weeks, diagnosed: TTTS stage IV or TTTS stage II, III with selective intrauterine growth restriction (sIUGR)18 or proximate cord insertions (the roots of the two umbilical cords are less than 2 cm).9,10
We excluded the cases of triplets with TTTS; TTTS performed FLS coagulation the placental vascular anastomoses surgery; manifestations of severe obstetrical diseases such as severe preeclampsia, HELLP syndrome, preterm labor, rupture of membranes, amniotic infection, placental abruption, or severe chronic and acute maternal illnesses with contraindications to implementation general surgery such as severe heart disease, kidney failure stage III, IV at the time of screening to select for the study.9
Procedure
All MCDA twins were followed up by sonographic examination every two weeks from 12 weeks of gestation; MCDA twins were determined according to the International Society of Ultrasound in Obstetrics and Gynecology (ISOUG) criteria.19,20 MCDA twins diagnosed with stage II–IV of TTTS according to Quintero classification21 from 16 to 26 weeks were given a study information sheet. These women were screened for eligibility by research doctors. After screening, they were provided with a full Patient Information Sheet, Consent Form and invited to a complete discussion with investigators about the study. When a patient signed informed consent, she was considered to be enrolled in the study.
Eligible women were examined pre-operation by local protocols, taken blood tests and measured cervical length (according to the Society for Maternal-Fetal Medicine – SMFM guidelines).22
Fetoscopic Laser Ablation for the Selective Fetal Reduction
Anesthesia was performed by combined general anesthesia (intravenous sedation) and local anesthesia (using Lidocaine 1%). The surgery was performed in a separate operation room for fetal surgery. Diode laser, with a 600 μ fiber, was used for cord occlusion. We used fetoscopic instruments: Image IS 4U of Karl Storz (Tuttlingen, Germany), laser instruments of Medilas D MultiBeam of Dornier, laser light guide of Dornier Medtech. Based on a previously determined position, the Seldinger technique was used to enter the polyhydramnios cavity under ultrasound guidance. Scope diameter was used in 2 sizes: 1.2 mm for the fetus under 20 weeks and 2 mm for the pregnancy over 20 weeks. Selective umbilical cord coagulation laser technique was applied to reduce pregnancy with a worse prognosis (donor fetus). The umbilical cord vessels were ablated under direct vision, and power settings from 50–60 W were required to achieve complete occlusion, depending on gestation age and cord size. The technique was considered successful when the entire umbilical cord blood vessel was occluded in the donor fetus. This was demonstrated by the loss of umbilical cord flow at the site of the ablation on Doppler ultrasound examination and the bradycardia or cardiac arrest observed on ultrasound. The amniotic fluid was subsequently drained until the maximum vertical pocket (MVP) reached the normal range (MVP 5 cm or 6 cm). Surgical characteristics such as operating duration from entering trocarts to withdrawing trocarts, anesthetic method, and amount of drained amniotic fluid were recorded.
Intra-operative and postoperative complications, including co-twin demise, bleeding in amniotic cavity, PPROM within 24 hours, maternal infection, anesthetic complications, or maternal blood loss requiring transfusion, were recorded.
Follow-Up
After surgery, pregnant women were examined and performed ultrasound at the following times: 48 hours, seven days, every two weeks until birth. Newborns were followed-up at three months and six months after birth.
The re-test of blood was performed after surgery 48 hours to determine the infection.
The study subjects were clinically examined according to the local protocol at all post-operative antenatal care visits. They measured the fetal biometric indicators, Doppler ultrasound of the umbilical artery, umbilical vein, ductus arteriosus, middle cerebral artery, and measurement of cervical length by ultrasound. No other observed or pre-existing fetal abnormalities were recorded.
Neonatal data including gestational age at delivery, birth method, birth weight, Apgar scores and Neonatal Intensive Care Unit (NICU) admission were collected at the time of birth.
Newborns were examined and monitored by a neonatologist at 3–6 months after birth. The mental and motor development of newborns were assessed according to the Denver II test,23 and the neonatal brain lesions were detected by Magnetic Resonance Imaging (MRI).
Statistical Analysis
Data were collected and managed using Redcap software and analyzed using the STATA 16.0 software. Qualitative variables were represented as numbers and percentages. Quantitative variables were described as mean with standard deviation and compared using the Mann–Whitney U-test. A p-value <0.05 was considered to be a statistically significant difference.
Results
During the 18 months of the study, we followed 344 participants with MCDA twins and 33 patients with TTTS who performed surgery at our fetal intervention center and neonatal follow-up up to 6 months postpartum. Twenty-one cases were successfully performed with FLA for the selective fetal reduction. However, 2 cases of fetal demises (recipient fetus) occurred within seven days after the operation, and 19 cases of post-operative pregnancy follow-up until at least six months postpartum (Figure 1).
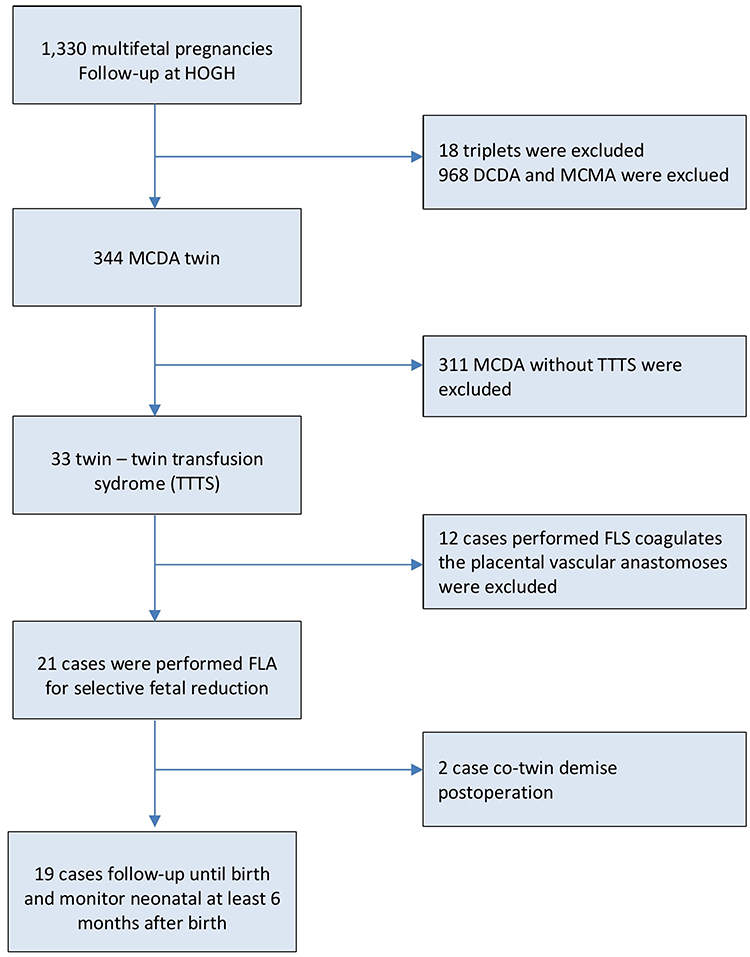 |
Figure 1 The flowchart of study groups. |
Table 1 shows general characteristics. According to Quintero classification, we have 18/21 cases of TTTS stage II (85.71%) and 3/21 cases of stage IV (14.29%). Indication for the selective fetal reduction in stage II due to TTTS with sIUGR (12 cases) and proximate cord insertions (6 cases). The average gestational age before surgery was 20.30 weeks.
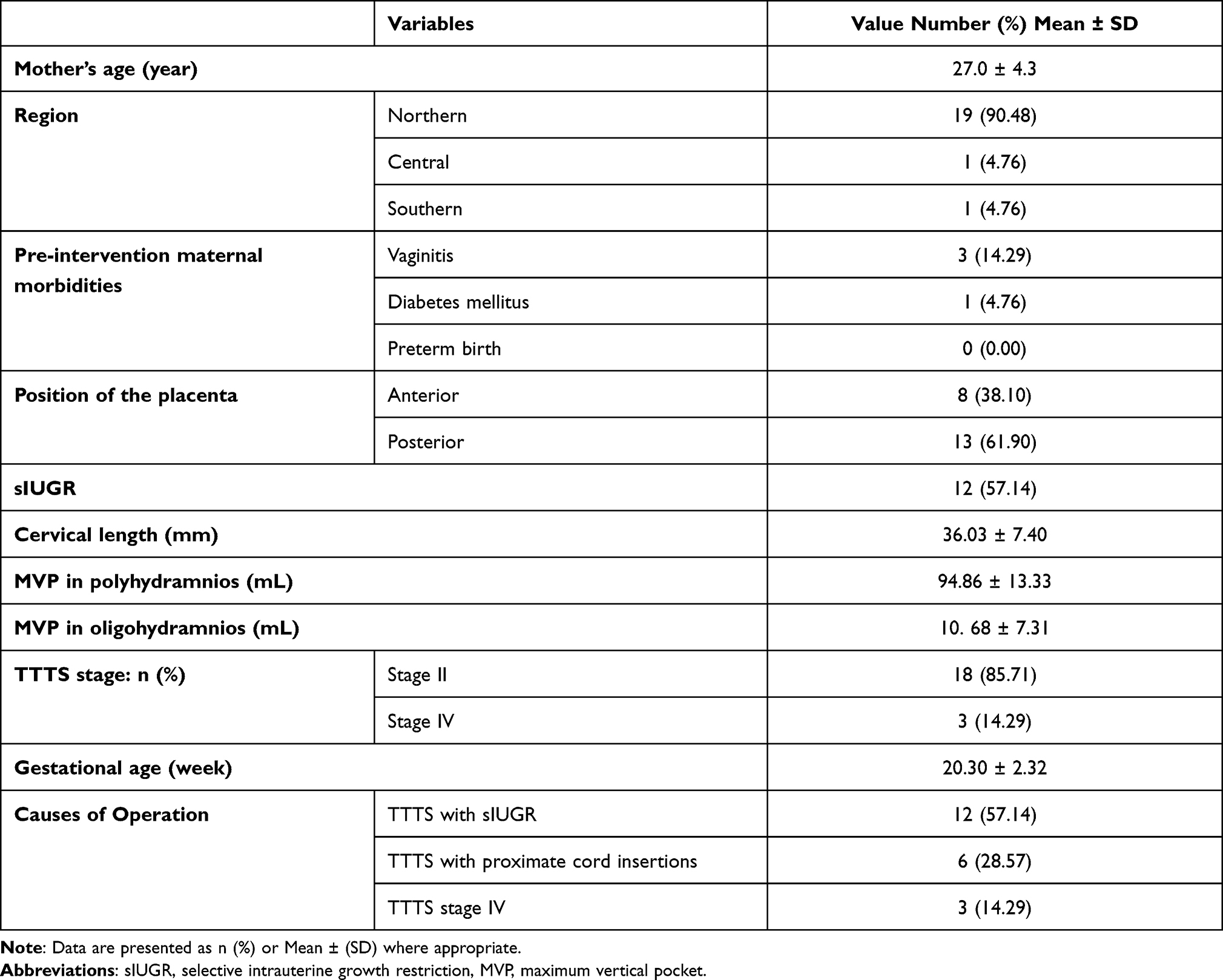 |
Table 1 General Characteristics (n = 21) |
The results of the operation are showed in Table 2. The average operation duration was 39.52 minutes; the average hospital stay was 5.42 days. We did not record any complications intra-operation and post-operation, including: co-twin demise, bleeding in the amniotic cavity, PPROM within 24 hours, maternal infection, anesthetic complications, or maternal blood loss requiring transfusion. After surgery, we recorded a decrease in cervical length at 48 hours and seven-day post-operation, but this change was not statistically significant with p < 0.05.
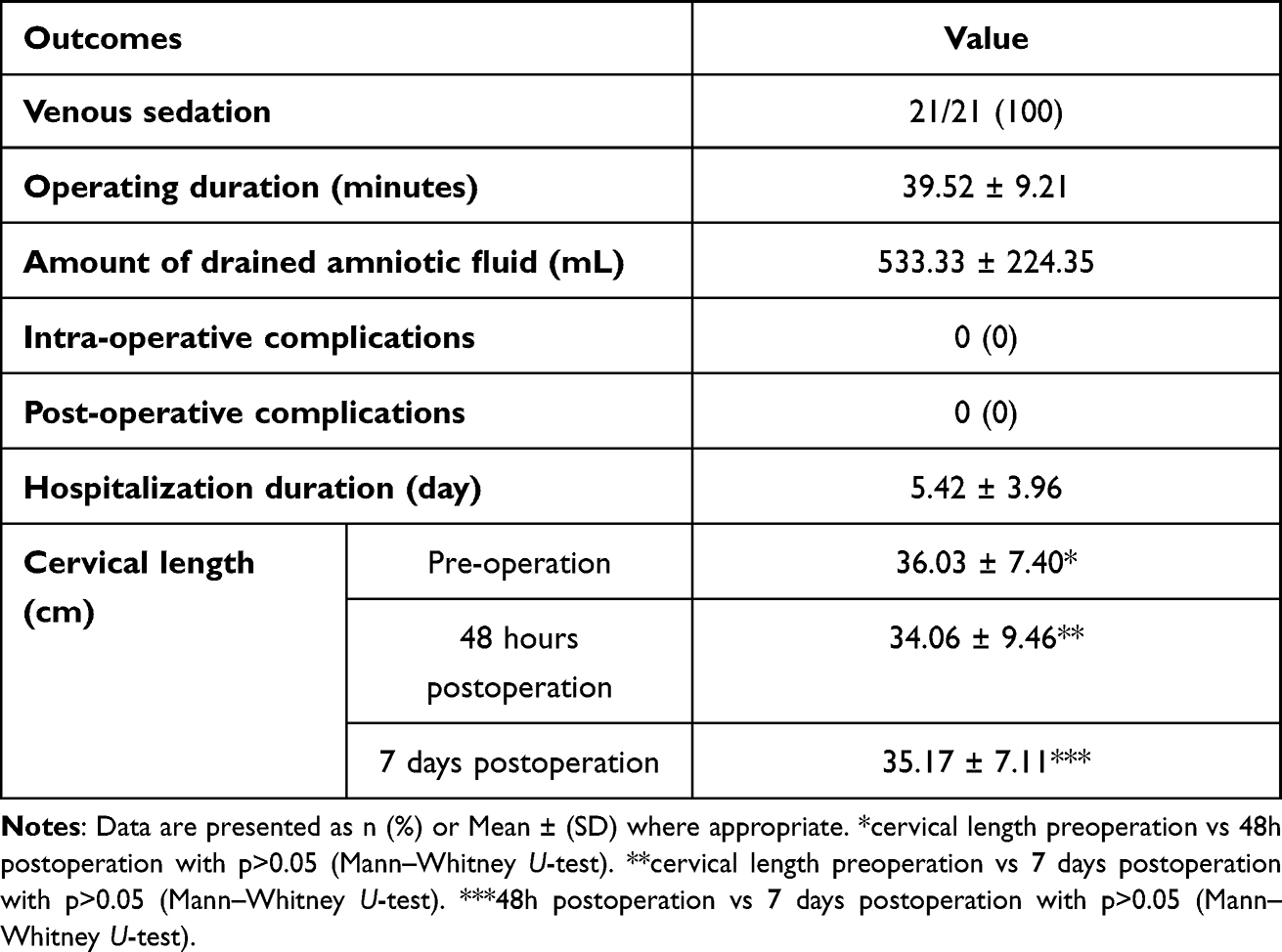 |
Table 2 Outcomes of Laser Ablation for the Selective Fetal Reduction Surgery |
The neonatal results are presented in Table 3. The mean gestational age at birth was 34.70 ± 4.33 weeks, with a mean duration of 12.97 ± 6.87 weeks between intervention and delivery. After surgery, the neonatal survival rate was 90.48%, and the average birth weight was 2281.58 ± 734.13 grams. We had 4 cases enter the NICU because of respiratory distress according to very low and extremely low birth weight. There were no postoperative maternal complications and no neurological complications when following up for at least six months postpartum.
 |
Table 3 Neonatal Results |
Discussion
Giving both fetuses a chance to live has always been the goal of TTTS treatments. However, in a few exceptional cases, survival of at least one fetus is required; otherwise, there is a risk of both fetuses’ demise. Therefore, selective fetal reduction techniques are proposed.
The selective fetal reduction is indicated of an MCDA twin, which is either discordant for a serious anomaly, sIURG, or cases of TTTS.24,25 It improves the outcome for its co-twin.24,25 Selective fetal reduction is used to treat TTTS when one fetus is at high risk of neurological complications or fetal demises such as severe TTTS (stage IV) or TTTS with sIUGR.7–9 On the other hand, when the coagulation technique of the placental vascular anastomoses cannot be performed, as in the case of proximate cord insertions, the roots of the two umbilical cords are less than 2 cm.10,18 In this situation, cauterization of the anastomoses in the equatorial between the two fetuses may face the risk of injury and occlusion of the remaining fetal blood vessels causing stillbirth in both fetuses.10,18 Selective fetal reduction techniques must be performed with the patient’s and family’s consent.8,9 To date, selective fetal reduction protocols are not universally agreed upon and vary according to country-specific circumstances, with some countries not implementing them due to problems related to religion.7 However, the technique is always suggested in situations that risk both fetuses demise.7–9,26 Along with the development of the fetal intervention, the current trend of selective fetal reduction is towards minimally invasive or non-invasive procedures such as HIFU.8 However, HIFU is still in the process of clinical trials, and it has not been widely applied due to the difficulty of the technique.8 Currently, the three treatment methods are BCO, RFA, and FLA. Although these techniques have been compared previously, the method, which results in the best perinatal outcome is controversial.27–30 This is probably due to the relatively small case series to date, especially given the lack of data on FLA for selective fetal reduction.27–31 In addition, an important aspect influencing the chosen treatment procedure is the feasibility of the technology. RFA is not available at most fetal medicine centers. FLS for TTTS was recently performed at HOGH, the first fetal interventional surgery center in Vietnam. In specific situations, we apply FLA for selective fetal reduction.
The mean gestational age at surgery in our study was 20.30 weeks. The mean gestational age at surgery was lower than in other studies because we followed MCDA twins from 12 weeks and diagnosed TTTS early. TTTS is most frequently diagnosed in the second trimester of pregnancy. Our study’s mean procedure duration was 39.52 minutes, which was shorter when compared to the time of the RFA technique in previous studies.11 Selective pregnancy reduction surgery is interventional. The prolonged duration of the procedure raises the risk of postoperative PPROM and preterm labor.11,31,32 We did not record any surgical complications, such as bleeding in the amniotic cavity, PPROM, especially infection. Infection is one of the most common complications following a fetal intervention. Our result may explain why we perform FLA surgery in an operating room designed explicitly for fetal intervention according to international standards, the procedures performed according to the protocol, and ensure the principles of sterility. The mean duration between intervention and delivery was 12.97 ± 6.87 weeks, which helped the average gestational age at birth reach 34.70 ± 4.33 weeks. Our findings were consistent with those of Rahimi-Sharbaf et al’s study on the effectiveness of RFA in treating MCDA twin complications and were higher in the treatment of TTTS using alternative procedures such as BCO or RFA with the mean gestational age at birth was 30 weeks.31 The preterm birth rate under 34 weeks is 31.58%. Preterm birth rates are always concerned, especially since our study subjects already had an increased risk factor, which is polyhydramnios in TTTS and performing fetal intervention. Preterm birth increases the risk of neonatal mortality and neurological complications, affecting the outcome of treatment. However, our study found a considerably reduced preterm birth rate. The rate of preterm birth rate under 34 weeks in our study was much lower than previously published with LFA (64.7%) and BCO (49.5%).11,28 Our results were similar when using the RFA technique in that study.11,31 This marked difference may be explained by various potential confounders. Firstly, because of the difference in gestational age of the surgical procedure, we performed surgery in the second trimester differently from some studies performed in the third trimester, increasing the risk of premature birth following the procedure. Secondly, our study’s surgical duration was shorter, and most healthy women had no signs of threatened preterm delivery or a short cervix prior to surgery.
Neonatal survival outcomes are among the most critical outcomes of surgery. Neonatal survival rates have generally varied between 70% and 90% in selective fetal reduction studies and are around 70% lower in the treatment of TTTS.11,28,31 The neonatal survival rate with FLS is about 60–70% if both fetuses and 80–90% in at least one fetus.1,3,33 As a result, our study’s neonatal survival rate was higher than in other studies. There were two cases of co-twin demise within seven days following the operation. These two cases included: a case of TTTS stage IV and an of TTTS with sIUGR, a twin growth discordance >61%. Fetal demise is one of the most common consequences following selective fetal reduction.1,3,33 The hypothesis is that the abrupt interruption of the circulation of one fetus affects the hemodynamics of the co-twin.1,3,33 We did not find a cause of stillbirth in our study, possibly due to the limited number of study subjects. The average birth weight in our study was 2281.58 ± 734.13 grams. We had 5 cases of neonates weighing less than 1500 g, of which 4/5 entered the NICU, and 4 cases were all premature births. Preterm birth and intrauterine growth restriction are frequently encountered and worsen neonatal outcomes after surgery. Therefore, active treatment for threatening preterm birth and good intrauterine fetal growth assessment is essential for caretaking and monitoring pregnant women after surgery. Another essential neonatal outcome is the occurrence of neurological complications. Although selective fetal reduction surgery aims to save the life of the co-twin and limit neurological complications, neurological abnormalities are still reported in 11–14%.34–36 Neurological complications can result from long-term fetal cerebral ischemia or complications from preterm birth in some cases.34–36 In our study, no abnormalities were detected through assessment of brain damage by MRI and psychomotor development through Denver II test, but it may be due to our short-term follow-up, only six months after birth. This is also a limitation of the study when long-term neurological complications have not been evaluated. We will follow up with neonates up to 2 years of age to assess long-term neurologic abnormalities in the infant’s psychomotor development.
The strength of our study is that we performed the same surgical procedure at the same fetal medicine center using the same surgical standards, and the same surgeon team with considerable training in fetal medicine performs the techniques. However, our study is limited by the absence of a randomized comparison of surgical treatments for TTTS selective fetal reduction, and additionally, we lack data on long-term neonatal follow-up.
Conclusion
In summary, in our experience, FLA for Selective fetal reduction treatment of TTTS had no surgical complications and achieved a high neonatal survival rate. We suggest that FLA should be considered as the method of choice for selective fetal reduction in some cases with indications to perform the technique.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
This study was approved by the Institutional Review Board (IRB) of Hanoi Medical University (IRB No NCS25/HMU-IRB). The study was in line with the Declaration of Helsinki. Individual patient consent for inclusion in the study was obtained. Before operation, written informed consent was provided to all participants after a thorough explanation of the purpose of this study. Patients had the right to discontinue at any time during the study.
Author Contributions
All authors made substantial contributions to conceptualization and design, data acquisition, data analysis and interpretation, took part in drafting of the initial manuscript and revising it critically, gave final approval for the version to be published, agreed to submit to the current journal, and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Akkermans J, Peeters SH, Klumper FJ, Lopriore E, Middeldorp JM, Oepkes D. Twenty-five years of fetoscopic laser coagulation in twin-twin transfusion syndrome: a systematic review. Fetal Diagn Ther. 2015;38(4):241–253. doi:10.1159/000437053
2. Glennon CL, Shemer SA, Palma-Dias R, Umstad MP. The history of treatment of twin-to-twin transfusion syndrome. Twin Res Hum Genet. 2016;19(3):168–174. doi:10.1017/thg.2016.27
3. Sago H, Ishii K, Sugibayashi R, Ozawa K, Sumie M, Wada S. Fetoscopic laser photocoagulation for twin-twin transfusion syndrome. J Obstet Gynaecol Res. 2018;44(5):831–839. doi:10.1111/jog.13600
4. Schatz F. Die Gef, sseverbindungen der Placentarkreisl, ufe eineiiger Zwillinge, ihre Entwicklung und ihre Folgen. Arch Gynaecol. 1886;27:1–72.
5. Ville Y, Hecher K, Ogg D, Warren R, Nicolaides K. Successful outcome after Nd: YAG laser separation of chorioangiopagus-twins under sonoendoscopic control. Ultrasound Obstet Gynecol. 1992;2(6):429–431. doi:10.1046/j.1469-0705.1992.02060429.x
6. Ville Y, Hecher K, Gagnon A, Sebire N, Hyett J, Nicolaides K. Endoscopic laser coagulation in the management of severe twin-to-twin transfusion syndrome. Br J Obstet Gynaecol. 1998;105(4):446–453. doi:10.1111/j.1471-0528.1998.tb10132.x
7. Akkermans J, Peeters SH, Middeldorp JM, et al. A worldwide survey of laser surgery for twin-twin transfusion syndrome. Ultrasound Obstet Gynecol. 2015;45(2):168–174. doi:10.1002/uog.14670
8. Bamberg C, Hecher K. Update on twin-to-twin transfusion syndrome. Best Pract Res Clin Obstet Gynaecol. 2019;58:55–65. doi:10.1016/j.bpobgyn.2018.12.011
9. Viral MP, Stirnemann J, Colmant C, Ville Y. Current practice and protocols: endoscopic laser therapy for twin-twin transfusion syndrome. Matern-Fetal Med. 2020;2:1.
10. Khalil A, Lewi L, Asma Khalil EL, Lewi L, Lopriore E, eds. Twin and Higher- Order Pregnancies. Springer; 2021.
11. Shinar S, Agrawal S, El-Chaar D, et al. Selective fetal reduction in complicated monochorionic twin pregnancies: a comparison of techniques. Prenat Diagn. 2021;41(1):52–60. doi:10.1002/pd.5830
12. Lanna MM, Rustico MA, Dell’Avanzo M, et al. Bipolar cord coagulation for selective feticide in complicated monochorionic twin pregnancies: 118 consecutive cases at a single center. Ultrasound Obstet Gynecol. 2012;39(4):407–413. doi:10.1002/uog.11073
13. Bebbington MW, Danzer E, Moldenhauer J, Khalek N, Johnson MP. Radiofrequency abla- tion vs bipolar umbilical cord coagulation in the management of complicated monochorionic pregnancies. Ultrasound Obstet Gynecol. 2012;40:319–324. doi:10.1002/uog.11122
14. Kumar S, Paramasivam G, Zhang E, et al. Perinatal- and procedure-related outcomes following radiofrequency ablation in mono- chorionic pregnancy. Am J Obstet Gynecol. 2014;210(5):e1–6. doi:10.1016/j.ajog.2013.12.009
15. Paramasivam G, Wimalasundera R, Wiechec M, Zhang E, Saeed F, Kumar S. Radiofrequency ablation for selective reduction in complex monochorionic pregnancies. BJOG. 2010;117(10):1294–1298. doi:10.1111/j.1471-0528.2010.02624.x
16. Lee H, Wagner AJ, Sy E, et al. Efficacy of radiofrequency ablation for twin-reversed arterial perfusion sequence. Am J Obstet Gynecol. 2007;196(5):
17. Nobili E, Paramasivam G, Kumar S. Outcome following selective fetal reduction in monochorionic and dichorionic twin pregnancies discordant for structural, chromosomal and genetic disorders. Aust N Z J Obstet Gynaecol. 2013;53(2):319–324. doi:10.1111/ajo.12071
18. Townsend R, Khalil A. Ultrasound screening for complications in twin pregnancy. Semin Fetal Neonatal Med. 2018;23(2):133–141. doi:10.1016/j.siny.2017.11.008
19. Townsend R, Khalil A. Ultrasound surveillance in twin pregnancy: an update for practitioners. Ultrasound. 2018;26(4):193–205. doi:10.1177/1742271X18794013
20. No GT. Management of monochorionic twin pregnancy: Green-top Guideline No. 51. BJOG. 2017;124(1):e1–e45. doi:10.1111/1471-0528.14188
21. Quintero RA, Morales WJ, Allen MH, Bornick PW, Johnson PK, Kruger M. Staging of twin-twin transfusion syndrome. J Perinatol. 1999;19(8 Pt 1):550–555. doi:10.1038/sj.jp.7200292
22. Jennifer McIntosh HF, Berghella V, Manuck T; Society for Maternal-Fetal Medicine (SMFM). The role of routine cervical length screening in selected high- and low-risk women for preterm birth prevention. Am J Obstet Gynecol. 2016;215(3):B2–7. doi:10.1016/j.ajog.2016.04.027
23. Glascoe FP, Byrne KE, Ashford LG, Johnson KL, Chang B, Strickland B. Accuracy of the Denver-II in developmental screening. Pediatrics. 1992;89(6):1221–1225. doi:10.1542/peds.89.6.1221
24. Ong SSC ZJ, Khan KS, Kilby MD. Prognosis for the co-twin following single- twin death: a systematic review. BJOG. 2006;113(9):992–998. doi:10.1111/j.1471-0528.2006.01027.x
25. Gratacós E, Martinez JM. A systematic approach to the differential diagnosis and management of the complications of monochorionic twin pregnancies. Fetal Diagn Ther. 2012;32:145–155. doi:10.1159/000342751
26. Van Der Veeken L, Couck I, Van Der Merwe J, et al. Laser for twin-to-twin transfusion syndrome: a guide for endoscopic surgeons. Facts Views Vis Obgyn. 2019;11(3):197–205.
27. Roman A, Papanna R, Johnson A, et al. Selective reduction in complicated monochorionic pregnancies: radiofrequency ablation vs. bipolar cord coagulation. Ultrasound Obstet Gynecol. 2010;36(1):37–41. doi:10.1002/uog.7567
28. Abdel-Sattar M, Chon AH, Llanes A, Korst LM, Ouzounian JG, Chmait RH. Comparison of umbilical cord occlusion methods: radiofrequency ablation versus laser photocoagulation. Prenat Diagn. 2018;38(2):110–116. doi:10.1002/pd.5196
29. Yinon Y, Ashwal E, Weisz B, Chayen B, Schiff E, Lipitz S. Selective reduction in complicated monochorionic twins: prediction of obstetric outcome and comparison of techniques. Ultrasound Obstet Gynecol. 2015;46(6):670–677. doi:10.1002/uog.14879
30. Bebbington M. Selective reduction in multiple gestations. Best Pract Res Clin Obstet Gynaecol. 2014;28(2):239–247. doi:10.1016/j.bpobgyn.2013.12.007
31. Rahimi-Sharbaf F, Ghaemi M, Nassr AA, Shamshirsaz AA, Shirazi M. Radiofrequency ablation for selective fetal reduction in complicated Monochorionic twins; comparing the outcomes according to the indications. BMC Pregnancy Childbirth. 2021;21(1):189. doi:10.1186/s12884-021-03656-1
32. Gaerty K, Greer RM, Kumar S. Systematic review and metaanalysis of perinatal outcomes after radiofrequency ablation and bipolar cord occlusion in monochorionic pregnancies. Am J Obstet Gynecol. 2015;213(5):637–643. doi:10.1016/j.ajog.2015.04.035
33. Hoffman M, Habli M, Donepudi R, et al. Perinatal outcomes of single fetal survivor after fetal intervention for complicated monochorionic twins. Prenat Diagn. 2018;38(7):511–516. doi:10.1002/pd.5278
34. Salomon LJ, Örtqvist L, Aegerter P, et al. Long-term developmental follow-up of infants who participated in a randomized clinical trial of amniocentesis vs laser photocoagulation for the treatment of twin-to-twin transfusion syndrome. Am J Obstet Gynecol. 2010;203(5):444e1–7. doi:10.1016/j.ajog.2010.08.054
35. Korsakissok M, Groussolles M, Dicky O, et al. Mortality, morbidity and 2-years neurodevelopmental prognosis of twin to twin trans- fusion syndrome after fetoscopic laser therapy: a prospective, 58 patients cohort study. J Gynecol Obstet Hum Reprod. 2018;47(10):555–560. doi:10.1016/j.jogoh.2018.04.003
36. Chmait RH, Chon AH, Schrager,SM, et al. Neonatal cerebral lesions predict 2-year neurodevelopmental impairment in children treated with laser surgery for twin-twin transfusion syndrome. J Matern-Fetal Neonatal Med. 2019;32(1):80–84. doi:10.1080/14767058.2017.1371694
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.