Back to Journals » Drug Design, Development and Therapy » Volume 11
Fentanyl-induced respiratory depression is attenuated in pregnant patients
Authors Cao X, Liu S, Sun J, Yu M, Fang Y, Ding Z
Received 26 July 2017
Accepted for publication 17 October 2017
Published 22 November 2017 Volume 2017:11 Pages 3325—3332
DOI https://doi.org/10.2147/DDDT.S147304
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qiongyu Guo
Xiaofei Cao,* Shijiang Liu,* Jie Sun, Min Yu, Yin Fang, Zhengnian Ding
Department of Anesthesiology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu Province, China
*These authors contributed equally to this work
Background: Respiratory depression is a complication of intravenous fentanyl administration. The effect of pregnancy on respiratory depression following opioid administration is unclear. This study investigated the effect of pregnancy on fentanyl-induced respiratory depression.
Patients and methods: Female patients were divided into three groups (n=20 per group): control group (non-pregnant and scheduled for laparoscopic surgery), early pregnancy group (pregnant for 45–60 days and scheduled for abortion), and postpartum group (5–7 days postpartum scheduled for complete curettage of uterine cavity). All patients received an intravenous infusion of fentanyl 2 µg/kg. Respiratory rate (RR), end-tidal pressure of carbon dioxide (PETCO2), and pulse oxygen saturation (SpO2) were recorded continuously from just before fentanyl infusion to 15 min after commencing infusion. Plasma levels of progesterone were measured.
Results: SpO2 levels in the early pregnancy and postpartum groups were significantly higher and the levels of RR and PETCO2 were significantly lower than the control group. RR and SpO2 levels were significantly decreased in all groups, whereas PETCO2 was significantly increased after fentanyl infusion. The rates of RR increase and SpO2 decrease were significantly faster in the control group than in the other groups. The lowest SpO2 after intravenous fentanyl administration was significantly positively correlated with plasma progesterone levels.
Conclusion: Pregnancy improves fentanyl-induced respiratory depression, which may be associated with the increased levels of plasma progesterone.
Keywords: fentanyl, pregnancy, respiratory depression, progesterone
Introduction
Opioids are widely used in postoperative analgesia. However, their use can cause severe adverse outcomes, such as respiratory depression. Pregnancy influences many aspects of the maternal physiological and pathological processes. Of particular interest to this study, dosages of narcotic drugs are usually less for pregnant women with hyperventilation during general anesthesia.1 However, the effect of pregnancy on respiratory depression following opioid administration is unclear. To address this question, we examined the respiratory response to intravenous fentanyl in non-pregnant, early pregnant, and postpartum females.
Patients and methods
Patient enrollment
The study was approved by the ethics and research committee of Nanjing Medical University (Nanjing, China), and informed consent was signed according to the Declaration of Helsinki. Sixty female patients aged 20–35 years weighting 47–70 kg and body mass index (BMI) 18–30 with American Society of Anesthesiologists (ASA) Grade I–II were enrolled. Exclusion criteria included allergies to opioids, history of alcohol or drug abuse, history of sedative-hypnotic and narcotic drugs, and history of sleep apnea or respiratory complications. Patients who had taken opioids or analgesics before surgery were also excluded. Twenty were non-pregnant (within 15 days before menstruation) and were scheduled for laparoscopic surgery due to infertility (control group). Twenty patients were at 45–60 days of pregnancy and were scheduled for abortion (early pregnancy group). Twenty patients were 5–7 days postpartum and were scheduled for complete curettage of uterine cavity because of placental remnants (postpartum group).
Study protocol
No premedication was given before the surgery. After entering the operation room, all patients were placed supine with inhalation of room air. Lactated Ringer solution was infused at a rate of 8 mL/kg/h. Patient’s nasal patency was confirmed. An end-tidal CO2 sampling tube was inserted 2 cm into the nasal cavity to measure end-tidal pressure of carbon dioxide (PETCO2). Respiratory rate (RR), PETCO2, and pulse oxygen saturation (SpO2) were measured continuously using a Mindray PM9000 monitor (Mindray Inc., Shenzhen, China). Thereafter, 0.1 mg/2 mL fentanyl citrate (Yichang Renfu Inc., Yichang, China) was diluted to 10 mL with normal saline and infused into the cubital vein at a rate of 1 mL/3 s with a total dose of 2 μg/kg after being completely anesthetized using only nasal breathing. The entire surgery was successful without any interruption, and the status of the patients was closely monitored. The patients remained undisturbed and breathed quietly through the nose with close monitoring. If the SpO2 was ≤80%, the patient might wake up. In that case, they were instructed to take deep breaths to increase the SpO2 level. Controlled respiration was given by breathing mask to patients in the event of severe hypoxia.
Measurements
Three milliliters of blood was collected from the peripheral vein before infusion with Lactated Ringer solution. Serum was isolated for measurement of progesterone levels by microparticle chemical luminescence radioimmunoassay (Beckman Coulter Inc., Pasadena, CA, USA). RR, SpO2, and PETCO2 were recorded during a quiet period after the patients had entered the operating theater and 1–15 min after intravenous fentanyl was administered.
Statistical analyses
Data are presented as mean ± standard deviation (SD). Groups were compared using one-way analysis of variance analysis (ANOVA) followed by Tukey’s post hoc test, as appropriate with SPSS 17.0 software (SPSS Inc., Chicago, IL, USA). The correlation between two groups was analyzed. Statistical significance was set at P<0.05.
Results
Pregnancy attenuates RR decrease following fentanyl treatment
RR determined at different times in the three groups decreased following fentanyl administration, compared with their respective baseline levels (0 min) (Table 1A and Figure 1A–C). The lowest RR was observed at 6 min in the non-pregnancy group, at 7 min in the early pregnancy group and at 8 min in the postpartum group. RR gradually returned toward baseline. However, the levels at 15 min in all three groups were still significantly lower than their baseline levels.
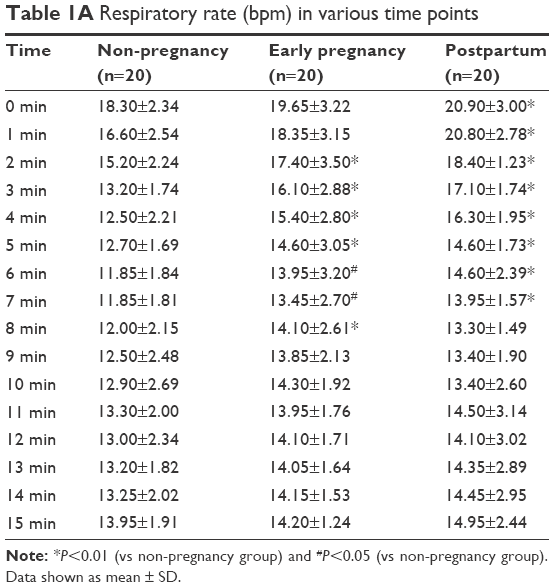 | Table 1A Respiratory rate (bpm) in various time points |
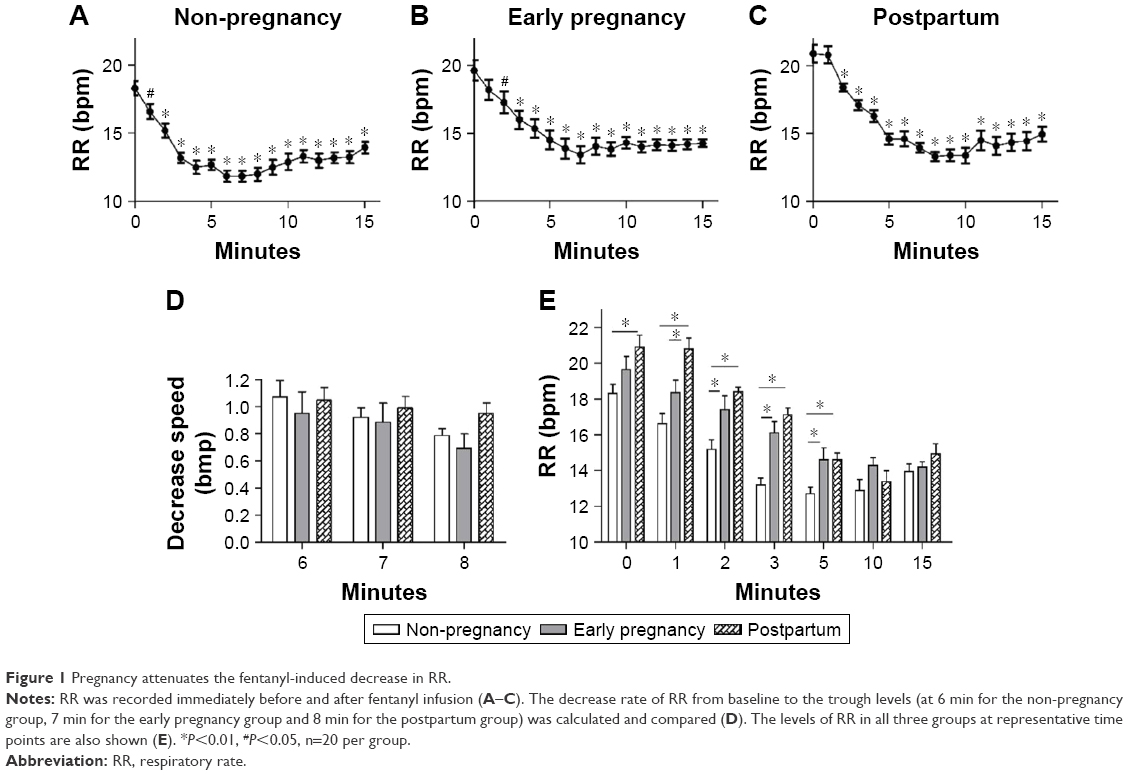 | Figure 1 Pregnancy attenuates the fentanyl-induced decrease in RR. |
The rate of decrease of RR from baseline to the trough levels was compared among three groups. The RR decrease rates at 6, 7, and 8 min following fentanyl administration showed no significant difference among the three groups (Table 1B and Figure 1D).
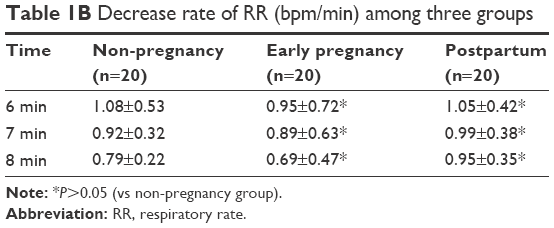 | Table 1B Decrease rate of RR (bpm/min) among three groups |
The RR levels were compared between three groups at each measured time point. Baseline RR was significantly higher in the postpartum group than in the non-pregnancy group. Importantly, the RR levels were significantly higher in the early pregnancy and postpartum groups at 1, 2, 3, and 5 min following fentanyl administration compared with time-matched non-pregnancy group measurements (Table 1A and Figure 1E).
Pregnancy attenuates PETCO2 increase following fentanyl treatment
Table 2A displays PETCO2 determined at different times in the three groups. PETCO2 levels were increased in all the three groups following fentanyl administration compared with their baseline levels (0 min) (Figure 2A–C). The PETCO2 levels then gradually returned toward the baseline. However, the levels at 15 min after fentanyl administration in all three groups were still significantly greater than each baseline level.
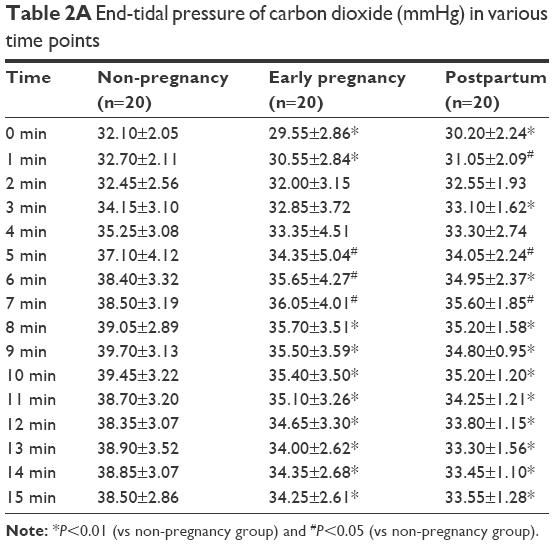 | Table 2A End-tidal pressure of carbon dioxide (mmHg) in various time points |
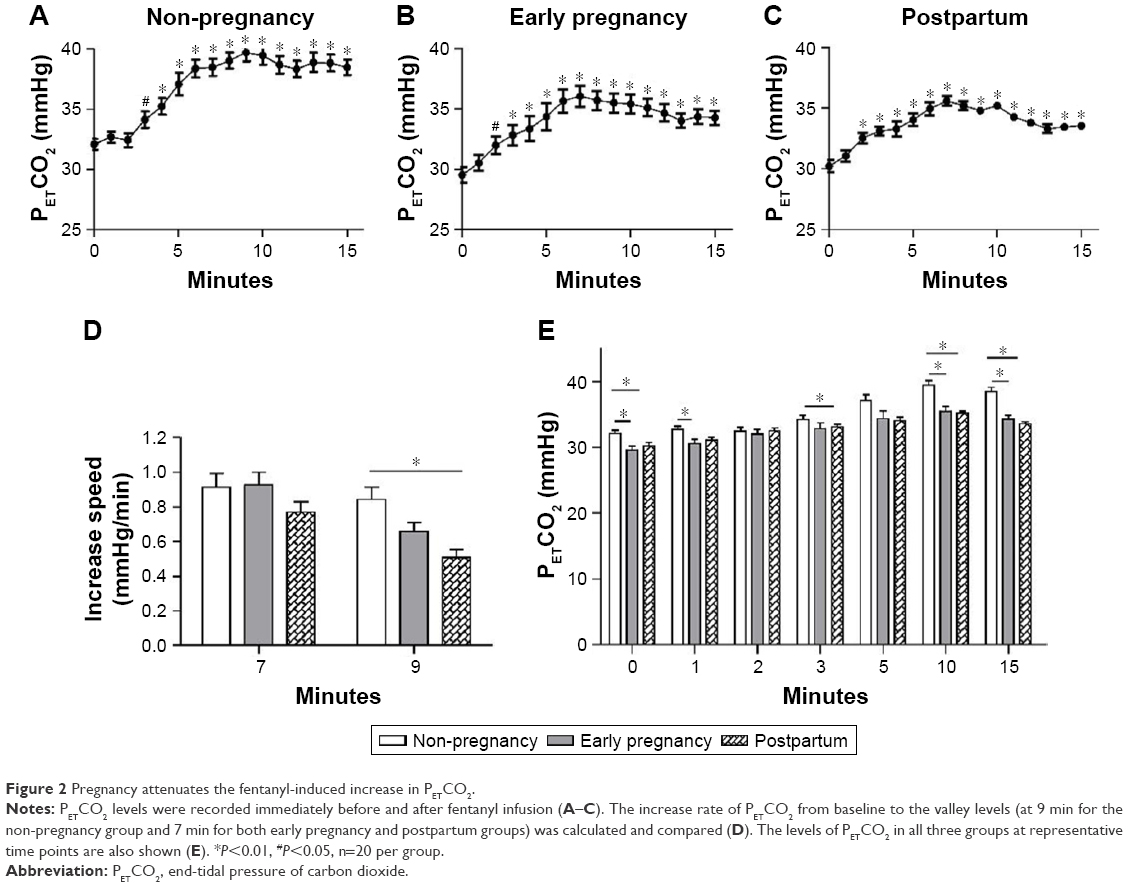 | Figure 2 Pregnancy attenuates the fentanyl-induced increase in PETCO2. |
The rate of increase of PETCO2 from baseline to the peak levels was compared in the three groups (Table 2B). The increase rate of PETCO2 7 min following fentanyl administration was not significantly different among the three groups (Figure 2D). However, the increase rate of PETCO2 9 min following fentanyl administration was significantly attenuated by 39.5% (0.51±0.20 vs 0.84±0.32; P<0.01) in the postpartum group compared with the non-pregnancy group.
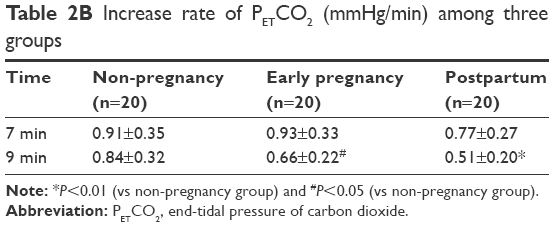 | Table 2B Increase rate of PETCO2 (mmHg/min) among three groups |
Also, we compared PETCO2 levels between three groups at each time point. PETCO2 levels at baseline were significantly lower in the early pregnancy and postpartum groups than in the non-pregnancy group. Importantly, the PETCO2 levels were significantly lower in the early pregnancy group at 1, 10 and 15 min and in the postpartum group at 3, 10 and 15 min than in the time-matched non-pregnancy group measurements (Table 1A and Figure 2E).
Pregnancy attenuates SpO2 decline following fentanyl treatment
Table 3A presents measurements of SpO2 at different times in the three groups. SpO2 levels decreased rapidly in the three groups following fentanyl administration compared with their respective baseline levels (0 min) (Figure 3A–C). The lowest level of SpO2 was observed at 8 min in the non-pregnancy group and at 7 min in both the early pregnancy and postpartum groups following fentanyl administration. SpO2 levels thereafter gradually returned toward the baseline. However, the levels at 15 min after fentanyl administration in all three groups were still significantly lower than each baseline level.
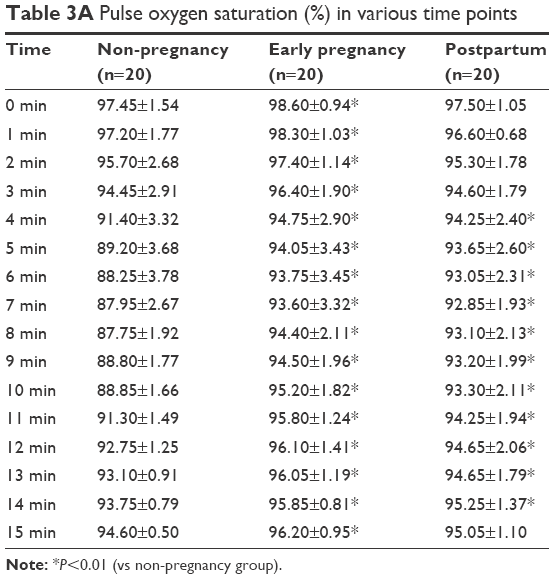 | Table 3A Pulse oxygen saturation (%) in various time points |
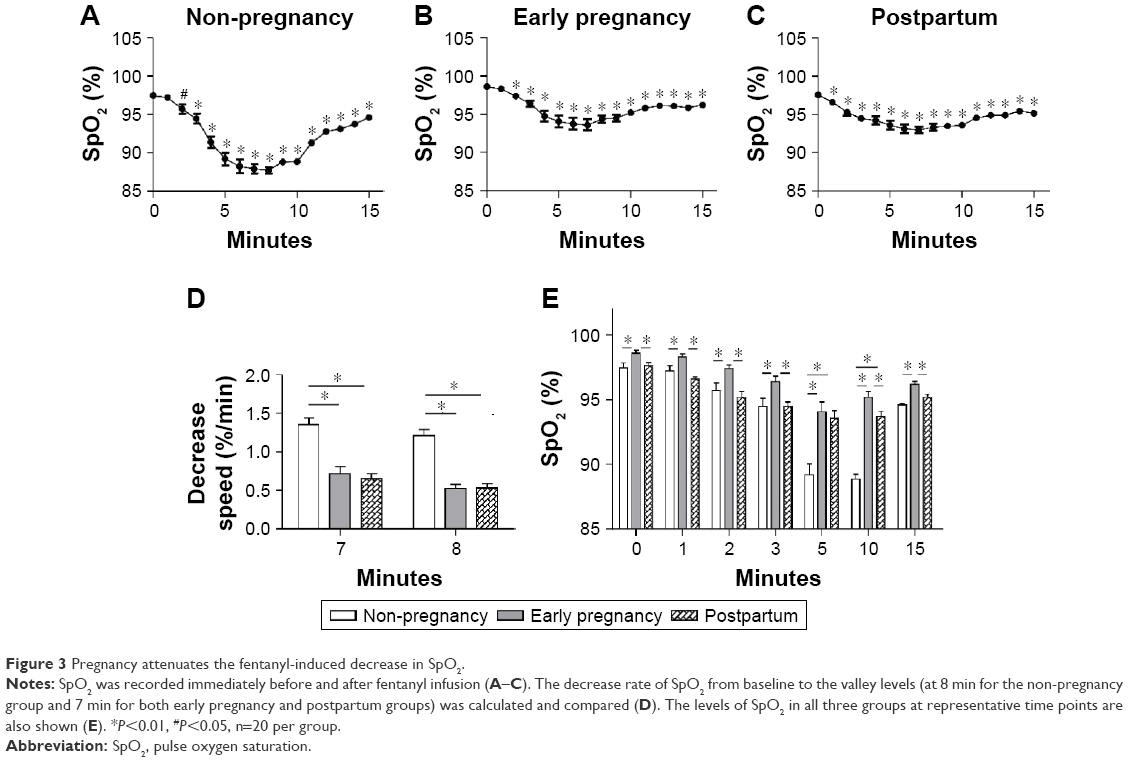 | Figure 3 Pregnancy attenuates the fentanyl-induced decrease in SpO2. |
The rate of decrease of SpO2 from baseline to the lowest levels was compared in the three groups (Table 3B). The decrease in the non-pregnancy group 7 min following fentanyl administration (1.35%/min) was significantly faster than that in the time-matched early pregnancy group (0.71%/min) and postpartum group (0.66%/min) (Figure 3D). Similar results were observed at 8 min (Table 3B and Figure 3D).
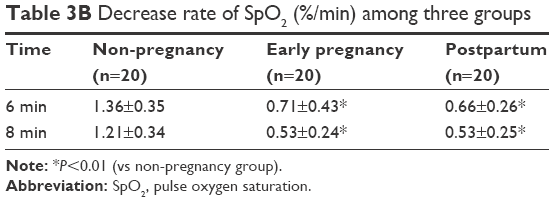 | Table 3B Decrease rate of SpO2 (%/min) among three groups |
We also compared SpO2 levels in the three groups at each measured time point. SpO2 levels were significantly higher in the early pregnancy group compared to the other groups at almost all the time points following fentanyl administration (Table 3A and Figure 3E). The postpartum group showed significantly higher SpO2 levels at 5 and 10 min compared with the time-matched non-pregnancy group measurements (5 min: 93.65%±2.60% vs 89.20%±3.68%; 10 min: 93.30%±2.11% vs 88.85%±1.66%) (Table 3A and Figure 3E).
Lowest SpO2 levels correlate positively with plasma progesterone levels following fentanyl treatment
Progesterone is an essential hormone to maintain pregnancy and functions in regulating the respiratory response.1,2 Thus, we examined the relationship between progesterone levels in plasma and the lowest SpO2 levels in the three groups following fentanyl treatment (Table 4). As shown in Figure 4A, progesterone levels were 96.01±0.68 nmol/L in the early pregnancy group and 8.26±0.45 nmol/L in the postpartum group, which were significantly higher than that in the non-pregnancy control group (2.45±0.61 nmol/L). Similarly, the lowest SpO2 levels in early pregnancy and postpartum groups were significantly higher than the non-pregnancy control group (Figure 4B).
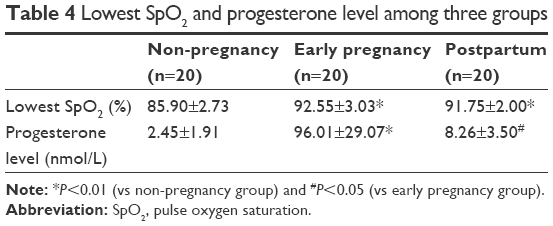 | Table 4 Lowest SpO2 and progesterone level among three groups |
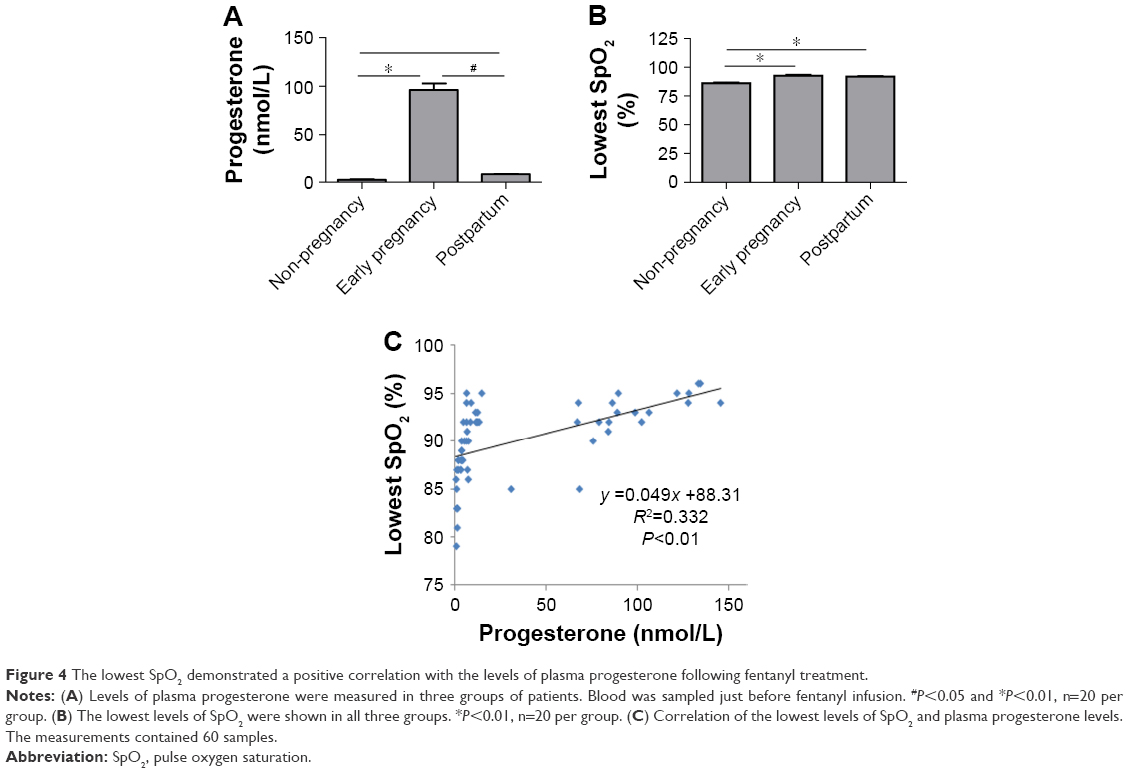 | Figure 4 The lowest SpO2 demonstrated a positive correlation with the levels of plasma progesterone following fentanyl treatment. |
To determine whether progesterone content affects SpO2 following fentanyl administration, we analyzed the correlation between plasma progesterone contents and the lowest SpO2 levels in all patients of three groups. As shown in Figure 4C, the lowest SpO2 levels after intravenous fentanyl showed a positive correlation with plasma progesterone levels (y =0.049x +88.31, R2=0.332, P<0.01).
Discussion
Postoperative pain is a fundamental issue in clinics. Of all the contemporary analgesics, opioids are the most potent analgesic drugs. However, the side effect of respiratory depression induced by opioids is a concern for anesthesiologists and limits the use of opioids in the postoperative analgesia.2 The present data demonstrate that the intravenous fentanyl-induced respiratory depression is improved in early pregnancy and postpartum patients compared with non-pregnant patients, with improvement being positively correlated with plasma progesterone level.
Opioid-induced respiratory depression following postoperative analgesia is related to various factors, including the type of the drug, dosage, rate of infusion, type of surgery and patient age and gender. This respiratory depression has rarely been found in the setting of obstetric analgesia.3 The mechanism for this phenomenon is still unclear. Presently, we observed the changes in the respiratory parameters after intravenous fentanyl use in patients with different pregnancy status to investigate the effect of pregnancy on respiratory response to intravenous fentanyl. The early pregnancy group comprised women with high level of progesterone because of pregnancy, the postpartum group included women with a medium level of progesterone due to placental remnants and the control group included women who were not pregnant with a low level of progesterone.
Intravenous injection of fentanyl 2 μg/kg at a rate of 1 mL every 3 s was reported to be a good model to observe the effect of fentanyl on ventilatory response.4 In this study, we observed that, after intravenous infusion of 2 μg/kg fentanyl, patients of the early pregnancy group and postpartum group had less respiratory depression, compared with those in the non-pregnancy control group. Only one patient in the control group had a temporary hypoxemia with the SpO2 marginally <80% (79%). The patient recovered after being reminded to take a deep breath.
There was no significant difference in the baseline PETCO2 level between the early pregnancy group and the postpartum group. However, the baseline level of the PETCO2 in the control patients was significantly higher than that in early pregnancy and postpartum patients. Following fentanyl infusion, the values of PETCO2 increased rapidly in all the three groups of patients. However, the increased rate was significantly more rapid in the control group. Moreover, PETCO2 values at 1, 3, 10, and 15 min following fentanyl infusion were significantly increased in control patients. The data suggest that pregnancy attenuates the fentanyl-induced increase in PETCO2.
The levels of SpO2 were decreased immediately after fentanyl infusion, with a significantly slower subsequent rate of decrease in the early pregnancy and postpartum groups than that in the control group. Interestingly, there was a significantly higher level of SpO2 in the early pregnancy group both at baseline and after fentanyl administration. The data suggest an effect of pregnancy on SpO2 decrease in fentanyl-treated patients. After the intravenous fentanyl injection, hyperventilation during pregnancy may at least partially alleviate the respiratory depressive effects of opioids. Jensen et al1 reported that the pregnancy-induced hyperventilation and the accompanied hypocapnia were the result of pregnancy-induced changes of the respiratory function, acid–base balance, metabolism, and cerebral blood flow. Of note, progesterone increases the alveolar ventilation of the women in pregnancy and luteal phase5 and has been successfully used in the treatment of sleep apnea syndrome.6 Comparison of women at 20 weeks post-partum demonstrated that women in the third trimester of pregnancy had lower progesterone, estradiol, and intravenous CO2 levels, but the change of the CO2 was not related to the levels of progesterone and estradiol,1,7 which is consistent with our study. But, we found the lowest SpO2 of all patients after the fentanyl injection was significantly correlated with their progesterone levels.
Attenuated respiratory depression observed in the women during 45–60 days of gestation and 5–7 days postpartum is possibly related to the pregnancy-induced decrease of the response to opioids. The locus coeruleus (LC) principally regulates the body dependence on opioids. Morphine and enkephalin can inhibit the discharge of LC. In animals with morphine tolerance, LC discharge is also tolerated.8 Compared with the non-pregnant rats, rats at the end of pregnancy reportedly display increased endogenous enkephalin and μ-receptor in the nucleus tractus solitarius, resulting in release of presynaptic norepinephrine, inhibition of corticotrophin-releasing hormone, and activity of the hypothalamic–pituitary–adrenal axis.9 This series of reactions may be related to the metabolism of progesterone to allopregnanolone, which can induce the expression of enkephalin-A mRNA in the nucleus tractus solitarius (NTS) of non-pregnant or late-pregnant rats.10 Thus, it is possible that the pregnancy-induced increase in endogenous opioids like enkephalin can inhibit the function of the nucleus and cause the increase of the opioid receptors or even result in tolerance, which leads to less potency of the exogenous opioids and less opioid-induced respiratory depression. This may be related to the progesterone level. The reduced anesthetic requirements for women in the luteal phase11 may be interpreted as the above reasons, but the exact mechanism remains to be clarified further.
There are some limitations of the study. First, the sample size is not large. This could limit the power of the statistical analysis. Multicenter clinical trials should be done to confirm the correlation found presently. Second, we did not monitor arterial carbon dioxide concentrations to assess respiratory depression. Instead, we used RR and PETCO2 levels, because they could be monitored in real-time and their dynamic change could be easily measured. As well, the PETCO2 could indirectly reflect arterial carbon dioxide concentrations. Third, we did not recruit late pregnancy patients because fentanyl is rarely used in this setting. Instead, we chose the patients with placental remnants scheduled for complete curettage. Although many of the physiological changes of pregnancy would have changed at this stage, these patients could still have relatively high levels of progesterone. More studies recruiting different trimesters of pregnant patients with proper sample size and more accurate monitoring indicators should be carried out.
Conclusion
Pregnancy can attenuate the respiratory depression induced by intravenous fentanyl injection, which may be related to increased progesterone level.
Acknowledgment
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
Jensen D, Duffin J, Lam YM, et al. Physiological mechanisms of hyperventilation during human pregnancy. Respir Physiol Neurobiol. 2008;161(1):76–86. | ||
Roozekrans M, van der Schrier R, Okkerse P, Hay J, McLeod JF, Dahan A. Two studies on reversal of opioid-induced respiratory depression by BK-channel blocker GAL021 in human volunteers. Anesthesiology. 2014;121(3):459–468. | ||
Carvalho B. Respiratory depression after neuraxial opioids in the obstetric setting. Anesth Analg. 2008;107(3):956–961. | ||
Dahan A, Roozekrans M, van der Schrier R, Smith T, Aarts L. Primum non nocere or how to resolve drug-induced respiratory depression. Anesthesiology. 2013;118(6):1261–1263. | ||
Kimura H, Tatsumi K, Kunitomo F, et al. Obese patients with sleep apnea syndrome treated by progesterone. Tohoku J Exp Med. 1988;156(suppl):151–157. | ||
Andersen ML, Bittencourt LR, Antunes IB, Tufik S. Effects of progesterone on sleep: a possible pharmacological treatment for sleep-breathing disorders. Curr Med Chem. 2006;13(29):3575–3582. | ||
Jensen D, Webb KA, Davies GA, O’Donnell DE. Mechanisms of activity-related breathlessness in healthy human pregnancy. Eur J Appl Physiol. 2009;106(2):253–265. | ||
Guajardo HM, Snyder K, Ho A, Valentino RJ. Sex differences in μ-opioid receptor regulation of the rat locus coeruleus and their cognitive consequences. Neuropsychopharmacology. 2017;42(6):1295–1304. | ||
Brunton PJ, Russell JA. Attenuated hypothalamo-pituitary-adrenal axis responses to immune challenge during pregnancy: the neurosteroid opioid connection. J Physiol. 2008;586(2):369–375. | ||
Brunton PJ, Meddle SL, Ma S, Ochedalski T, Douglas AJ, Russell JA. Endogenous opioids and attenuated hypothalamic-pituitary-adrenal axis responses to immune challenge in pregnant rats. J Neurosci. 2005;25(21):5117–5126. | ||
Erden V, Yangin Z, Erkalp K, Delatioğlu H, Bahçeci F, Seyhan A. Increased progesterone production during the luteal phase of menstruation may decrease anesthetic requirement. Anesth Analg. 2005;101(4):1007–1011. table of contents. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.