Back to Journals » Medical Devices: Evidence and Research » Volume 19
Female Supine Urination Tech: Patent Landscape & Indicators
Authors Mesa La Guardia A ![]() , Prats Valls MT, Micó Cabedo M, Domenech Climent N, Juan Verdoy P
, Prats Valls MT, Micó Cabedo M, Domenech Climent N, Juan Verdoy P ![]() , Gual Ortí J
, Gual Ortí J ![]()
Received 25 November 2025
Accepted for publication 1 February 2026
Published 21 April 2026 Volume 2026:19 584153
DOI https://doi.org/10.2147/MDER.S584153
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mohamad Bashir
Ana Mesa La Guardia,1– 3 Maria Teresa Prats Valls,3,4 Mónica Micó Cabedo,3,4 Nuria Domenech Climent,3,5 Pablo Juan Verdoy,6 Jaume Gual Ortí7
1Department of Materials and Industrial Technologies, University of Jaume I, Castelló, Spain; 2Teaching, Training and Research Unit, Alcoy Health Department, Alcoi, Spain; 3Foundation for the Promotion of Health and Biomedical Research in the Valencia Region (FISABIO), Valencia, Spain; 4Surgery Service, General d’Ontontinyent Hospital, Ontinyent, Spain; 5Family and Community Nursing, La Bassa Health Center, Alcoy Health Department, Alcoi, Spain; 6Department of Mathematics, Universitat Jaume I, Castelló, Spain; 7Department of Industrial Systems Engineering and Design, Universitat Jaume I, Castelló, Spain
Correspondence: Ana Mesa La Guardia, Email [email protected]; [email protected]
Purpose: Female urination in the supine position is a frequent bedside need, yet common workarounds (bedpans, diapers, improvised receptacles) can be uncomfortable, increase caregiver workload, and contribute to potentially avoidable urinary catheterization. We mapped the patent landscape of non-invasive female urine-collection technologies intended for supine use and derived actionable innovation and access priorities.
Methods: We searched Espacenet (EPO), WIPO PATENTSCOPE, the USPTO database, Google Patents, and INVENES for January 2000–September 2025. Records were screened for functional relevance to female supine voiding and de-duplicated at the DOCDB family level. For each patent family we extracted priority/publication timing, jurisdictions, assignees, IPC/CPC codes, and forward citations; coded solution archetypes; and coded adoption-relevant attributes (workflow feasibility, infrastructure dependence, and single-use vs reusable design intent). A structured multi-domain appraisal (0– 2 per domain; total 0– 12) was applied to representative families to support consistent comparison.
Results: Twenty-six patent families met inclusion criteria. Innovation activity was sustained but low-intensity and uneven over time, with most filings clustered in 2010– 2020; interpretation of late years was limited by publication lag. Most inventions followed single-use/disposable pathways (≈69%). The set covered 16 IPC subclasses, although > 60% of families were concentrated in A61F 5/455. Passive external collectors showed the strongest maturity signals. Adhesive patch-type and intravaginal concepts were sporadic and heterogeneous. Suction/capillary approaches introduced stronger containment mechanisms but increased dependence on external infrastructure and proprietary consumables, limiting feasibility in home care and low-resource settings.
Conclusion: The most consistent gap lies at the intersection of ergonomics, autonomy, and reusability—female-specific supine interfaces that contain leakage without adhesives or invasive elements, operate passively or with minimal infrastructure, and enable sterilizable/reusable pathways. Priorities for R&D include usability- and risk-informed evaluation, sustainability-by-design, and access-oriented IP strategies to support diffusion beyond high-resource settings.
Keywords: female urinal, supine voiding, external urine collection device, patent landscape, usability engineering, sustainability
Introduction
Female urination in the supine position remains an unresolved, high-frequency bedside problem across acute wards, perioperative care, long-term care, and home care. When women cannot mobilize to the toilet, current workarounds (diapers, bedpans, improvised receptacles, or non-adapted urinals) can compromise dignity, increase discomfort and caregiver workload, and—importantly—push clinical teams toward urinary catheterization as a default option rather than a last resort.1–6 This review is needed now for three converging reasons: (i) the growing burden of immobility associated with ageing, frailty, neurological disease, and post-surgical recovery; (ii) intensified safety priorities to reduce avoidable catheter use and catheter-associated harms; and (iii) renewed expectations that women’s health technologies be designed for female anatomy and real-world care pathways rather than adapted from male-oriented devices.7,8
Background and Problem Statement
In routine practice, women who remain continent but cannot sit or stand still need a safe, comfortable, low-effort method to void supine. Yet traditional bedpans often require awkward positioning, lifting, and prolonged exposure to wetness or spillage, generating dissatisfaction in patients and burden in staff.1–4 Female external collection devices exist, but many perform poorly in true supine use due to sealing failures, leakage, backflow, poor fit across body habitus, or impractical workflows (eg, reliance on adhesives, complex assembly, or suction systems unavailable outside hospitals).9–11 The consequence is a persistent gap between a well-recognized clinical need and the limited availability of ergonomic, validated, female-specific solutions for supine voiding.
Clinical Decision Context: When Catheterization is Unavoidable vs Potentially Avoidable
In this context, two broad scenarios can be distinguished:
Catheterization Typically Unavoidable (Strong Clinical Indication)
- Acute urinary retention or suspected obstruction requiring decompression.
- Precise urine output monitoring that is clinically decisive in unstable/critical situations.
- Perioperative contexts where catheterization is mandated by procedure duration, anesthesia, or strict fluid balance requirements.
- Situations where external collection is unsafe or infeasible, such as severe perineal wounds/burns, uncontrolled bleeding, or repeated failure of non-invasive methods despite adequate support.
Catheterization Potentially Avoidable (Preference-Sensitive/Workflow-Driven)
- Continent but immobile women (postoperative recovery, frailty, temporary disability) who can void spontaneously if provided a feasible supine interface.
- Short-term immobility where catheterization is used for convenience, staffing constraints, or lack of suitable devices.
- Long-term care/home care contexts where low-infrastructure solutions could prevent repeated catheter cycles, improve dignity, and reduce caregiver strain.
This distinction matters because innovation priorities differ: for scenario A, devices may play a supportive role (comfort, hygiene, monitoring adjuncts), whereas for scenario B, improved female-specific supine voiding devices can directly reduce avoidable catheter use and associated harms while improving patient experience.
Against this clinical backdrop, the present study analyses the global patent landscape of female external urination devices intended (explicitly or functionally) for supine use, focusing on how design choices, intellectual property concentration and diffusion patterns may shape what is available to clinicians and patients. Patenting strategies influence manufacturing, procurement, licensing, and ultimately access—particularly in under-served niches where markets are fragmented and evidence generation is limited.12
Scientific and Social Relevance
The lack of ergonomic, reusable, clinically workable solutions for female supine voiding represents both a care-quality gap and a women’s health innovation gap. In many settings, devices remain adaptations of male-oriented designs, often underperforming when anatomical fit, sealing mechanics, and dignity-preserving workflows are essential.7,8,13 This underperformance has downstream effects: avoidable discomfort and dependence, caregivers burden, and a higher likelihood of catheterization in preference-sensitive contexts.
The relevance is also systemic. Sex- and gender-sensitive innovation frameworks increasingly demand that design assumptions be tested against real-world female care pathways.7,8 Sustainability pressures are rising: many single-use solutions generate contaminated waste streams, in tension with circular-economy aspirations in healthcare.14 Finally, equity considerations extend beyond high-income markets: device affordability, infrastructure dependence (eg, suction, specialized consumables), and IP restrictions can amplify access gaps in low-resource settings.12,15
Rationale for a Prospective Analysis of Patents and Emerging Technologies
Patent documents provide an early, structured signal of technological intent and commercial strategy in areas where peer-reviewed clinical evidence may lag. However, patent landscapes are also intrinsically retrospective: most applications become public with a delay, and classification systems can introduce noise by capturing broader sanitary appliances that only partially overlap with true supine use. To make the analysis clinically meaningful, a patent-based approach must therefore (i) prioritize relevance to supine female voiding, (ii) interpret claims and embodiments in relation to care workflows, and (iii) translate technical patterns into actionable gaps rather than descriptive counts alone.16–20
Accordingly, this study uses patent analytics to:
- Map global innovation activity (families, jurisdictions, assignees, and IPC/CPC structure) in female supine voiding devices;
- Characterize recurring design archetypes and constraints relevant to real supine use (eg, interface geometry, sealing strategy, backflow prevention, materials and reusability, infrastructure dependence); and
- Identify actionable gaps and access-relevant IP patterns that can guide R&D and adoption strategies toward ergonomic, reusable and low-infrastructure solutions.
Primary Objective
To conduct a forward-looking patent-based analysis of female external urination devices for supine use (2000–2025) that:
- Maps the international patent landscape (families, jurisdictions, assignees, IPC/CPC, and citation-normalized indicators);
- Identifies technology and IP gaps linked to ergonomic performance, reusability, and low-resource applicability; and
- Derives innovation priorities aligned with patient dignity, caregiver workflow feasibility, sustainability, and equitable access.
Conceptual Framework
This study interprets the patent landscape for female external urination devices intended for supine use through an access-oriented framework that links (i) the clinical problem and workflow constraints, (ii) the forms of intellectual property (IP) protection used to secure device value, (iii) territorial filing strategies that signal intended markets, and (iv) adoption dynamics shaped by procurement, infrastructure and sustainability. The aim is to move beyond descriptive counts and use patent evidence to identify actionable innovation and access gaps.
Procedural and Territorial Pathways (PCT → National Phase; Exhaustion)
Intellectual property protection and access pathways matter for this niche. Many device concepts are simple (funnels, cushions, flexible interfaces) and are often protected via national patents, utility models, or PCT filings. The scope and geography of protection influence manufacturing freedom, pricing, and the feasibility of local production—especially in lower-resource regions. In addition, doctrines such as exhaustion and parallel importation affect downstream access once products are placed on the market.21–27
Patent Analytics for Innovation, Licensing and FTO
For decision-making, the patent family is treated as the operative unit because it captures the same inventive concept across jurisdictions.18–20,28 Patent analytics can then be used to infer innovation intensity and strategic intent by examining priority timing, family size and geographic spread (including PCT entries), assignee concentration, and citation-based indicators as a proxy for technological influence.18–20,28 At the same time, patent evidence must be interpreted with caution: publication lag and classification practices can limit sensitivity to the most recent or most narrowly defined developments. In this study, these signals are therefore interpreted alongside the clinical workflow requirements of true supine use.
To connect technology signals with clinical reality, we treat the patent family—not the single filing—as the analytical unit, and we interpret citation and classification indicators as proxies of influence and breadth rather than direct measures of clinical effectiveness. This framing motivates a structured appraisal of patents in Table 1, alongside descriptive indicators (family size, jurisdictions, and forward citations) to balance novelty, feasibility, and access considerations.18–20,28
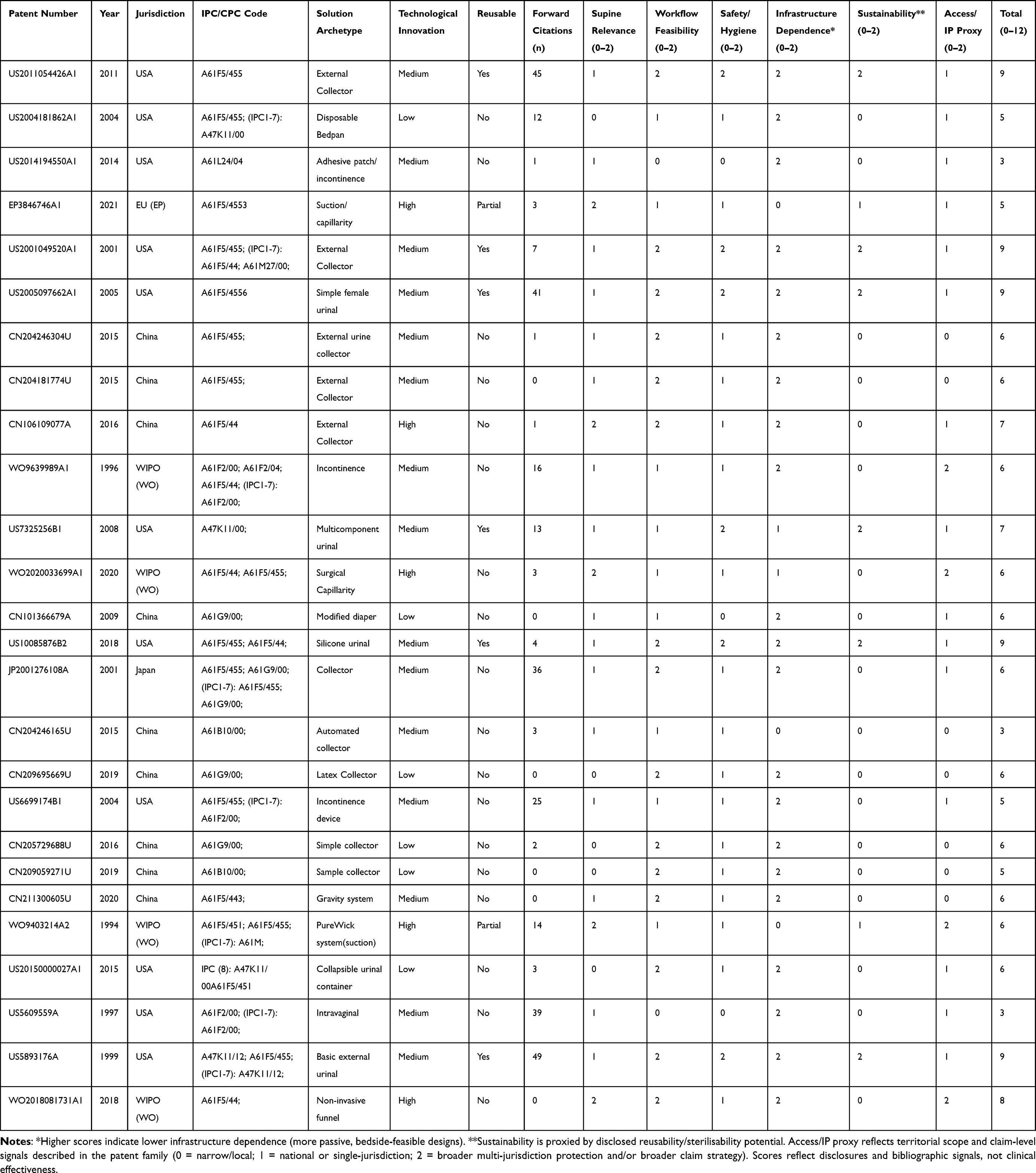 |
Table 1 Patent Set, Attributes, and Structured Appraisal Scores (0–2 per Domain; Total 0–12) |
Licensing and Access Models in Gender-Specific Device Niches
In underserved device classes, licensing strategy can either accelerate diffusion or reinforce market fragmentation. Non-exclusive licensing, field-of-use segmentation (eg, acute care vs home care), or geographically differentiated licensing can help balance incentives for investment with broad availability.20,29 Conversely, narrow exclusivity combined with proprietary consumables can create lock-in effects that constrain procurement choices and raise barriers for low-resource settings.20,29 These mechanisms are particularly relevant in gender-specific niches where demand is substantial but innovation has historically been under-prioritized.
Technology Adoption with IP Constraints (TAM/Diffusion Revisited)
Adoption is influenced by perceived usefulness, ease of use, compatibility with routines, and the observability of benefits, especially in time-pressured bedside care. We therefore interpret patent archetypes through established diffusion and acceptance constructs (eg, workflow fit and perceived burden) to anticipate where design choices are likely to succeed or fail in real-world implementation.30,31
Responsible Research and Innovation (RRI) as an Access-Oriented Lens
Finally, we position innovation priorities within responsible research and innovation (RRI) principles: inclusiveness, sustainability, and social value. For a bedside women’s health technology, this implies balancing protection and diffusion, designing for constrained infrastructures, and aligning solutions with broader sustainability and equity goals.15,32,33
Methodology
Patent Search Strategy
A reproducible, multi-database patent search was conducted to identify inventions describing female external urination devices intended (explicitly or functionally) for use in the supine position. Searches were performed in Espacenet (EPO), WIPO PATENTSCOPE, the USPTO database, Google Patents, and INVENES (OEPM, Spain), using iterative refinement of terms and classification filters to balance recall and precision.
Free-text query (example core string):
(“female urination device” OR “female urine collection” OR “external urinary device” OR “female urinal” OR “urine management” OR “bedpan” OR “urinal”) AND (“supine” OR “lying” OR “bedridden” OR “dorsal decubitus” OR “immobilized patient” OR “hospital use”)
Patent records were retrieved from Espacenet (EPO), WIPO PATENTSCOPE, INVENES (OEPM, Spain), the USPTO database, and Google Patents between January 2000 and September 2025. Search strategies combined free-text terms (eg, female urinal, external urine collector, supine urination) with IPC/CPC filters relevant to sanitary and medical urine-collection devices, followed by manual screening for functional relevance to supine use.34–36
Classification filters (IPC/CPC) were used to anchor the search in relevant sanitary and continence device classes, including:
A61F 5/44 (urinals; bedpans), A61F 5/455 (urine collection devices), A61F 5/48 (external urine collection), and related codes where female continence, interfaces, or collection systems are commonly classified. Filters were used as inclusion scaffolding rather than as a strict boundary; targeted screening outside the core codes was performed to reduce false negatives from misclassification.
Eligibility Criteria
Records were eligible if they described a device or system enabling urine collection from female anatomy in a way compatible with supine voiding (eg, interfaces designed to seal in dorsal decubitus, leakage/backflow control mechanisms, or workflows explicitly aimed at bedridden care). Patents were included regardless of assignee type (individual, SME, incumbent) and across jurisdictions. Exclusion criteria were: (i) inventions clearly limited to male anatomy; (ii) purely intraluminal catheter designs without an external female interface; (iii) toilet-seat or commode designs not intended for supine use; and (iv) records lacking sufficient technical disclosure to infer relevance to supine female voiding.
Family Handling, de-Duplication and Chronology
We deduplicated records at the DOCDB patent family level and retained one representative member per family for descriptive reporting. Family construction and priority-country concepts followed standard patent statistics guidance.19,20
Because most patent applications are published with a delay after filing, the most recent priority years are expected to be under-represented. To mitigate interpretive bias in trend analyses, the final 18–24 months of the search horizon were treated as potentially incomplete and interpreted cautiously in time-series indicators.
Selection and Screening Process
Screening followed a staged process: (i) title/abstract screening for apparent relevance to female urination and non-invasive collection; (ii) claim-level screening of independent claims to confirm supine compatibility and identify the core inventive features; and (iii) full-text review of descriptions/figures for functional archetype coding. Screening and extraction were performed by two reviewers (blinded to assignee identity where feasible) and validated through consensus checks with the wider author team where eligibility or categorization was ambiguous.
Data Extraction and Coding
For each DOCDB family, the following variables were extracted: priority year, publication year, jurisdictions covered (including PCT entry where applicable), assignee(s) and assignee type, le.g.al status where available, IPC/CPC codes, forward citation counts, and an engineering/clinical functional typology. Functional typology captured recurring solution classes (eg, passive external collectors, bedpan-like basins, adhesive patch-type interfaces, suction-assisted systems, intravaginal solutions, and hybrid/accessory systems).
To address sustainability and infrastructure constraints relevant to adoption, devices were additionally coded for: (i) intended single-use vs reusable design; (ii) reprocessing/sterilization assumptions where described; and (iii) infrastructure dependence (eg, external suction, power, proprietary consumables).
Operationalization of Proxy Indicators
Given the small and unevenly distributed patent corpus typical of under-served niches, the analysis emphasized transparent proxy indicators rather than fitting growth models that require dense time series. Technological maturity was assessed by archetype using: (i) technological density (families per 5-year window), (ii) mean/median age (years since priority), and (iii) diversity of approaches (IPC breadth and within-archetype solution heterogeneity).
Forward citations were extracted where available and normalized by publication cohort to reduce age-related bias. We interpret citation counts as an imperfect proxy for technological influence and visibility, recognizing that citations are shaped by examination practice, jurisdiction, and field-specific norms.18,19
Technological breadth was proxied by the diversity and spread of IPC/CPC subclasses within families and across the dataset, and by diffusion indicators derived from cross-jurisdiction coverage. These measures were treated as signals of exploratory versus specialized innovation pathways rather than direct measures of clinical maturity.16,17,19
All indicators were compiled from Espacenet/Google Patents records and cross-checked across sources where bibliographic fields diverged (eg, assignee name variants, le.g.al status).
Structured Appraisal and Scoring of Key Patent Families (Table 1)
To enable transparent comparison of representative inventions, a structured multi-domain appraisal was applied to the patent families summarized in Table 1. The appraisal was designed as an interpretive tool (not a measure of clinical effectiveness) and focused on domains most relevant to real supine use and access:
- Supine clinical relevance: interface geometry/fit and leakage or backflow control in dorsal decubitus.
- Workflow feasibility: steps required for placement/removal, caregiver burden, and compatibility with ward/home routines.
- Safety and hygiene: features supporting skin integrity, contamination control and feasible reprocessing when reusable.
- Infrastructure dependence: need for external suction/power/specialized consumables vs passive operation.
- Sustainability: reusable/sterilizable design intent vs predominantly single-use disposable pathways.
- Access/IP proxy: territorial scope and claim-level signals likely to influence diffusion, design-around and supplier competition.
Each domain was rated on a 0–2 scale (0 = not addressed/poor fit; 1 = partially addressed/moderate fit; 2 = well addressed/high fit). Domain scores were summed to an overall structured appraisal score (range 0–12) used alongside descriptive indicators (year, jurisdiction, archetype, citations) to support narrative synthesis.
Risk-of-Bias and Reproducibility Controls
To improve reproducibility and reduce selection artefacts, the following controls were implemented: (i) combined free-text and classification-driven retrieval with targeted hand-searching outside core codes to reduce misclassification bias; (ii) family-level de-duplication to prevent double counting; (iii) cohort normalization of citation indicators to limit age bias; and (iv) escalation of ambiguous eligibility and coding decisions to consensus review. Machine translation was used for non-English titles/abstracts/claims, and unclear cases were rechecked against figures and independent claims.
Results
This section summarizes how design and IP patterns may affect downstream diffusion and access. We interpret broad, multi-jurisdiction protection as a potential barrier to local manufacturing, while narrower protection (or utility models) may support faster imitation but can also signal limited investment and weaker evidence generation. These trade-offs are discussed in relation to licensing, procurement, and the feasibility of low-infrastructure deployment.12,31
Technology Mapping: Year, Jurisdiction and Functional Typology
To avoid double counting across PCT (WO) publications and their national/regional counterparts, analysis was performed at the family level; where multiple publications existed, one representative publication per family was retained for document-level reporting (earliest publication authority). “WO (WIPO)” denotes PCT international publications; “EP” denotes European regional publications; and “US”, “CN” and “JP” denote national patent offices.
Chronology. Patent activity is uneven across time. Priority/publication patterns indicate sustained but low-intensity innovation, with the period 2010–2020 accounting for approximately 54% (14/26) of the families. Apparent declines in the most recent years should be interpreted cautiously because patent publication lag is expected to under-represent late priority years. Overall, the time series suggests persistent interest but limited cumulative deepening in solutions that simultaneously address supine ergonomics, reusability, and patient/caregiver autonomy (Table 1 and Figure 1).
 |
Figure 1 Heatmap of maturity proxies (density, mean age, diversity). Scale: 0–1 (min-max). Data source: Espacenet/Google Patents. |
Notably, a substantial proportion of solutions are single-use or disposable, reflecting a design pathway that prioritizes infection control and convenience but increases waste and recurrent procurement costs. This pattern warrants explicit consideration alongside circular-economy priorities and the feasibility of sterilization and reuse in different care settings.14,15
Reading Table 1 from an IP angle, the landscape combines fragmented invention with local clustering. Some families show narrow, geometry-constrained independent claims that may enable clearer design-around pathways, while others emphasise functional language or consumable-dependent elements that can increase lock-in risk and freedom-to-operate (FTO) uncertainty. Cross-classification beyond core continence codes (eg, to A61M fluid handling, A61L materials/antimicrobials, or A61G bed-related devices) also signals adjacent technical domains that may shape enforceability, licensing, and market entry.
Technological Evolution and Maturity
A coherent trajectory is visible across the corpus, but it is not a simple story of linear improvement. Early inventions often centre on disposable wedges, bedpan variants, or funnel-type collectors that attempt to manage leakage through shape alone. Later families introduce stronger “control” mechanisms—adhesives, interface sealing features, and suction/capillary approaches—to improve containment in supine use. While these additions can reduce leakage under specific conditions, they frequently trade off against workability in real care pathways: adhesives can be poorly tolerated on fragile skin or require high operator skill;9–11 suction/capillary systems can increase infrastructure dependence (power, external collection units, proprietary consumables), reducing feasibility in home care or low-resource settings.9–11 In practical terms, several solution lines improve containment but shift the burden to workflow, infrastructure, or disposability rather than resolving the ergonomics–autonomy–reusability triad.
Given the small corpus and irregular time distribution, maturity was assessed using proxy indicators rather than parametric growth models. The following proxies were computed and summarized by archetype (Figure 1):
Technological density (families per functional type).
Average age (years since priority/publication).
Diversity of approaches (heterogeneity of solution embodiments within each type).
Findings. Passive external collectors show the highest relative maturity across proxies (higher density and longer presence in the record), consistent with path-dependent refinement rather than disruptive change. Suction/capillary approaches show a smaller number of families but stronger signals of technical “control” features that may be attractive in institutional settings. In contrast, adhesive patch-type and intravaginal solutions appear more sporadic and heterogeneous, suggesting exploratory activity and barriers to routine use. Across the full set, a predominance of single-use/disposable designs (approximately 69% of families, based on disclosed use/reprocessing intent in patent documents) indicates that innovation has frequently progressed through disposable pathways, with implications for waste generation and circularity goals in healthcare (Figures 1–3).
 |
Figure 2 Schematic adapted from WO 2020033699 A1 (WIPO PATENTSCOPE).37 30 = a urinary device assembly. 31 = A female patient. 32 = overall urine aspiration system. 33 = urinary device. 34 = pelvic belt. 35 = a pump. 36 = pump suction tube. 37 = a urine reservoir. 38 = canister suction tube. |
 |
Figure 3 Comparative schematic adapted from WO 2020033699 A1 (WIPO PATENTSCOPE).37 |
Technological Influence
Forward citations and citation-normalized influence indicators suggest that earlier foundational filings accumulated visibility over time, whereas more recent patents may be underrepresented due to publication lags and examination delays. Accordingly, influence metrics were interpreted cautiously and complemented by qualitative appraisal of disclosed mechanisms and workflows.18,19
Interpretation. Influence concentration suggests that a limited number of inventive lines shape subsequent filings and may define important claim boundaries for design-around. However, citation signals should be interpreted alongside claim scope: high citation counts can reflect broad, function-oriented claims (potentially stronger barriers) or, conversely, well-known but structurally narrow solutions that are easier to design around.
Technological Breadth
Technological breadth was summarized using (i) Patent Power (mean number of distinct IPC subclasses per family) and (ii) cumulative technological expansion (unique IPC subclasses across the set). CPC was used operationally for retrieval and mapped back to IPC for comparability in reporting.
Across the 26 families, 16 unique IPC subclasses were identified. While most families remain concentrated in core continence/sanitary classes, a subset expands into adjacent domains, suggesting opportunities for cross-fertilization (eg, materials and skin-contact technologies, fluidic components, or bed-associated interfaces). Notably, more than 60% of families are single-class in A61F 5/455, indicating limited combinatorial breadth in many inventions.
Recurring Patterns and Strategic Gaps
Three robust signals emerge from the results:
Because classification-based retrieval can inflate datasets with only partially relevant sanitary appliances, we applied iterative screening and typology checks to minimize false positives. Residual noise cannot be fully eliminated and is addressed in the Limitations section.16,19
Influence Concentration
A small set of families accounts for a disproportionate share of forward citations, implying that claim boundaries from these lines may exert outsized effects on subsequent design choices. For innovators, early claim-level appraisal is essential to distinguish whether barriers are function-based (harder to design around) or structurally narrow (more straightforward design-around).
Whitespace at the Intersection of Ergonomics–Reusability–Autonomy
The corpus shows limited coverage of solutions that simultaneously deliver (i) ergonomic fit for diverse anatomy in dorsal decubitus, (ii) reusable/sterilizable pathways that reduce waste, and (iii) low-infrastructure operation (no adhesives; no external suction/power). This gap is clinically and systemically relevant because it aligns with settings where catheterization is most avoidable (continent but immobile patients) and where adoption barriers are driven by workflow and resource constraints.
Illustrative Concept [Blinded for Review]
To translate the patent-derived “whitespace” into actionable engineering requirements, an anonymised illustrative concept is outlined below. The concept is presented as a design archetype intended to address the recurring trade-offs identified in the landscape—namely leakage control in true dorsal decubitus, workflow feasibility at the bedside, and the predominance of single-use solutions—while remaining compatible with low-infrastructure settings.
The intention is not to claim clinical effectiveness at this stage, but to demonstrate how the gaps mapped in Methodology–Results can be operationalized into measurable design objectives, testable hypotheses, and an access-oriented product profile that is feasible across acute care, long-term care and home care.
Technical Rationale
Across the analyzed families, performance limitations in supine use frequently arise from (i) inadequate interface fit across anatomical variability, (ii) reliance on adhesives or insertion to achieve sealing, (iii) infrastructure dependence (eg, suction/power), and (iv) disposability as the primary pathway to reduce contamination risks. The illustrative concept therefore centers on a female-specific external interface that achieves containment through geometry and compliant materials, paired with a passive, closed collection pathway that does not require external suction.
Core Architecture
The concept comprises three modular elements: (1) a soft, anatomically contoured external interface; (2) a passive one-way fluid pathway designed to reduce backflow; and (3) a closed collection container or bag. The modules are designed for straightforward assembly/disassembly to support cleaning and reprocessing where a reusable pathway is adopted.
Design Objectives and Performance Targets
Key objectives are organized into clinically meaningful domains:
- Anatomical fit in dorsal decubitus: accommodate a range of vulvar morphology and body habitus without insertion or skin adhesives; maintain position with minimal manual holding.
- Leakage and backflow control: provide a stable seal under typical supine conditions and reduce rewetting through passive one-way features (valve or geometry-driven anti-backflow).
- Comfort and skin integrity: minimize pressure points and shear; use compliant materials; avoid prolonged moisture exposure and minimize contact area where feasible.
- Workflow feasibility: enable placement and removal in a small number of steps; support use by a single caregiver; allow patient participation where mobility permits; minimize bedding disturbance.
- Low infrastructure dependence: function without external suction, power, or proprietary consoles; rely on gravity and passive flow control.
- Hygiene and reprocessing: minimize crevices; enable disassembly; ensure materials and joints tolerate common cleaning and disinfection procedures; clearly define a reprocessing pathway if reusable.
- Sustainability: prioritize reusable/sterilizable materials and components where feasible; when single-use components are required, confine them to the lowest-mass elements and consider recyclable or bio-based options where compatible with infection control.
Materials and Reusability Strategy
To align with circular-economy goals in healthcare, the baseline pathway assumes a reusable patient-interface made from biocompatible materials (eg, medical-grade silicone or thermoplastic elastomers) selected for skin tolerance, flexibility, and resistance to common cleaning/disinfection agents. Reusability is treated as a design constraint from the outset: joints are simplified; surfaces are smoothed; and disassembly is enabled so that the interface and fluid path can be cleaned effectively. Where sterilization is required by the intended use environment, materials and assemblies should be qualified for the relevant reprocessing method used locally (eg, high-level disinfection, low-temperature sterilization, or other validated pathways).
Usability and Safety Engineering
Because bedside adoption is strongly mediated by ease of use and caregiver burden, the concept is framed for usability engineering: critical tasks include correct positioning, seal verification, spill prevention during removal, and safe disposal or handling of collected urine. These tasks can be translated into formative usability tests and scenario-based simulations (eg, varying body habitus, limited caregiver time, restricted patient mobility). Risk management priorities include leakage leading to maceration, cross-contamination during handling, pressure-related discomfort, and improper reprocessing when a reusable pathway is adopted.21–24
Access and Global Applicability
The concept intentionally avoids dependencies that can limit diffusion outside highly resourced hospitals. Passive operation (no suction, no power), minimal consumables, and compatibility with standard collection containers support use in home care and long-term care as well as in lower-resource settings. An access-oriented design profile also anticipates procurement constraints by minimizing proprietary lock-ins and by enabling manufacturing routes that can be scaled without specialized components.
Optional Extensions
If future development priorities include monitoring or assisted autonomy, a sensor-ready architecture can be explored as an optional module (eg, non-invasive fill-level detection in the container or simple usage logging). Such functions should remain modular so they do not compromise the baseline low-infrastructure pathway.
Strategic Framing
From an innovation standpoint, the concept targets the recurring gap where existing filings tend to trade leakage control for either adhesives/insertion, infrastructure dependence, or disposability. A clinically relevant contribution would be demonstrated by showing that an external, non-adhesive, passive system can achieve acceptable containment in dorsal decubitus while remaining workable for caregivers and compatible with reuse pathways. The structured appraisal introduced in Structured Appraisal and Scoring of Key Patent Families (Table 1) can be used to position the concept against representative patent families in Table 1 and to justify the novelty and practical relevance of its design choices.
Discussion
Overview of the Contribution
This study maps a small but clinically consequential patent landscape for female external urination devices intended for supine use, and translates bibliographic and claim-level patterns into actionable gaps. The findings indicate sustained interest over time but fragmented innovation, with repeated rediscovery of similar interface geometries and limited convergence on solutions that are simultaneously workable at the bedside, low-infrastructure, and compatible with reusable pathways (Table 1 and Figures 1–3).
In scenario B contexts, where catheterization is often preference- or workflow-driven, better female-specific supine devices have the potential to reduce avoidable catheter use and catheter-associated harms while improving patient experience.5,6,11
This prioritization aligns with contemporary stewardship guidance that emphasizes minimizing catheter use and duration, and with emerging evidence that external female collection systems can reduce indwelling catheter exposure in appropriate populations.5,6,11
Trade-Offs Visible in Existing Inventions
Across families and archetypes, leakage control in supine use is commonly pursued by adding “control” layers—adhesives, insertion, suction, or proprietary fluid-handling components. These strategies can improve containment under selected conditions, but frequently introduce new barriers to routine use: skin intolerance and operator dependence with adhesives; acceptability barriers with insertion; and feasibility limitations in home care or resource-constrained settings when suction/power or proprietary consumables are required.
Whitespace: Ergonomics–Autonomy–Reusability
The most consistent gap lies at the intersection of (i) ergonomic fit across anatomical variability in dorsal decubitus, (ii) passive or low-infrastructure operation that supports patient/caregiver autonomy, and (iii) reusable or sterilizable pathways that reduce waste. While individual patents address one or two of these dimensions, the portfolio provides limited evidence of mature, integrated solutions that reconcile all three in a clinically workable product profile.
Sustainability Implications and Circularity
A predominance of single-use or disposable pathways (approximately 69% of the identified families) suggests that innovation has often advanced by shifting contamination risk management into disposability. This approach may simplify short-term workflow but increases contaminated waste and can conflict with circular-economy and sustainability aspirations in healthcare systems. A pragmatic research direction is therefore to develop reusable, biocompatible, reprocess able interfaces with clearly defined cleaning/disinfection pathways and to confine single-use components—when needed—to the lowest-mass elements.
Global Accessibility Beyond EU/US Markets
Territorial filing patterns and device dependencies have direct implications for global accessibility. Designs requiring powered suction, specialized consumables, or proprietary consoles are less likely to diffuse into long-term care and home care, and are often impractical in low-resource settings. Conversely, passive, low-infrastructure interfaces compatible with standard collection containers can support broader adoption across regions. Interpreting the landscape through an access lens highlights that the clinical need is global, but the feasible solution space varies sharply with infrastructure and procurement constraints.
IP Structure, Diffusion, and Freedom-to-Operate (FTO)
The landscape shows influence concentration in a limited subset of families and a broader set of locally filed inventions with narrower scope. For innovators and health systems, this implies two parallel priorities: (i) early claim-level appraisal to anticipate FTO constraints and viable design-around options, and (ii) access-oriented licensing strategies (eg, non-exclusive or geographically differentiated licensing) that can support diffusion in gender-specific device niches without reinforcing lock-in through proprietary consumables.
Methodological Interpretation: Publication Lag and Classification Noise
Patent analytics provide structured signals of technological intent, but they are inherently retrospective: most applications are published with a delay after filing, and late priority years are therefore under-represented. In addition, IPC/CPC systems can introduce noise by capturing broader sanitary appliances that only partially overlap with true supine use. The staged screening used here (title/abstract → independent claims → full text/figures) reduces, but does not eliminate, these artefacts. Consequently, the results should be read as a map of disclosed innovation and IP strategy rather than a complete inventory of ongoing private R&D.
Implications for R&D and Evaluation
The findings point to concrete priorities for next-generation solutions: female-specific interfaces that seal without adhesives or insertion; passive or low-infrastructure operation that can work in home care and long-term care; materials that are biocompatible, sterilizable and reuse-oriented; and modular architectures that can later incorporate optional monitoring (eg, fill-level sensing) without compromising the baseline pathway. Future studies should pair engineering development with usability engineering and risk management, using scenario-based simulation and formative testing to validate placement workflow, leakage/backflow performance, skin integrity, and safe handling/reprocessing.
Limitations and Future Research Directions
Patent-Data Scope and Publication Lag
Patent landscapes map disclosed inventions and IP strategies rather than the full universe of ongoing R&D. Because most applications are published with a delay after filing, late priority years are under-represented; recent trends should therefore be interpreted cautiously.
Classification and Retrieval Noise
IPC/CPC systems can capture broader sanitary appliances that only partially overlap with true supine female voiding, and relevant inventions may also be filed under adjacent classes. Although staged screening (title/abstract, independent claims, full text/figures) and family-level de-duplication reduce misclassification bias and double counting, residual noise and missed records remain possible.
Inference Limits From Bibliographic Indicators
Proxy indicators such as forward citations, family size, and IPC breadth provide interpretable signals but do not measure clinical effectiveness or market adoption. Citation counts are influenced by age and jurisdictional practices; normalization reduces but does not eliminate this bias.
Generalization to Clinical Practice
Patent disclosures can be incomplete regarding usability, failure modes, and reprocessing feasibility. Therefore, conclusions about workflow feasibility, patient comfort, and sustainability should be treated as hypotheses to be tested in empirical studies rather than definitive performance claims.
Conclusions
This patent-based landscape analysis indicates that innovation in female external urination devices intended for supine use has been sustained but fragmented, with repeated reinvention of similar interface geometries and limited convergence on solutions that are simultaneously reliable in dorsal decubitus, feasible for real care workflows, and scalable across settings. The record shows that containment improvements are often pursued via adhesives, insertion, suction or disposable pathways—approaches that can reduce leakage but frequently introduce new barriers related to skin tolerance, acceptability, infrastructure dependence, or waste generation.
The most consistent gap lies at the intersection of ergonomics, autonomy and reusability: clinically viable solutions remain scarce that (i) accommodate anatomical variability without adhesives or invasive interfaces, (ii) operate passively or with minimal infrastructure to support home care and long-term care, and (iii) enable reusable or sterilizable pathways compatible with infection control. Given that avoidable catheterization is most common in continent but immobile patients, progress in this design space has the potential to improve dignity and comfort while reducing caregiver burden and catheter-associated harms.
Future development and evaluation should prioritize female-specific interfaces made from biocompatible materials that tolerate cleaning, high-level disinfection or sterilization; passive or low-infrastructure designs that do not require external suction; and modular architectures that can incorporate underserved functions such as integrated sensing (eg, fill-level or leakage detection) without compromising baseline simplicity. Finally, access-oriented strategies—including early freedom-to-operate assessment and licensing models that avoid proprietary lock-in—are important to support diffusion beyond EU/US markets and into settings where affordability and infrastructure constraints are decisive.
Code Availability
Not applicable. No custom code or software was developed for this study.
Data Sharing Statement
Patent records analyzed in this study are publicly available from Espacenet (EPO), WIPO PATENTSCOPE, INVENES (OEPM), the USPTO database and Google Patents. The derived dataset (search strings, screening decisions, and coded variables used for analysis) is available from the corresponding author on reasonable request.
Ethics Approval
Not applicable. This study did not involve human participants or animals.
Acknowledgments
The authors thank Universitat Jaume I, FISABIO, and the collaborating health departments for the support received. This research was funded by UJI.>LAB Impuls 2024, a public funding program of Universitat Jaume I aimed at promoting applied research and innovation. Parts of this article are available online in a preprint on SSRN: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5362955.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Universitat Jaume I (UJI) through the LABS Impuls 2024 programme. The funder had no role in the study design; data collection, analysis, or interpretation; manuscript preparation; or the decision to submit the manuscript for publication.
Disclosure
Ana Mesa La Guardia, Maria Teresa Prats Valls, Mónica Micó Cabedo and Jaume Ortí report a patent P202330948 issued. The authors report no other conflicts of interest in this work.
References
1. Benton JG, Brown BB, Rusk HA. Energy expended by patients on bedpans. JAMA. 1950;144(17):1443–17.
2. Cailleteau A, Brillac D, Debat N, et al. Bedpan manipulation: patient comfort and staff constraints, which levers can be used for improvement? PLoS One. 2024;19(7):e0306773. doi:10.1371/journal.pone.0306773
3. Garg A, Owen B. Reducing back stress to nursing personnel: an ergonomic intervention in a nursing home. Ergonomics. 1992;35(11):1353–1375. doi:10.1080/00140139208967398
4. Fader M, Pett Ersson L, Dean G, Brooks R, Cottenden A. The selection of female urinals: the contribution of one continence clinic. Br J Nurs. 1999;8(14):918–925. doi:10.12968/bjon.1999.8.14.6540
5. Centers for Disease Control and Prevention. Summary of recommendations: catheter-associated urinary tract infections (CAUTI). Centers for Disease Control and Prevention website. 2024. Available from: https://www.cdc.gov/infection-control/hcp/cauti/summary-of-recommendations.html.
6. National Institute for Health and Care Excellence (NICE). Infection pssrevention and control. Quality standard QS61: quality statement 4: urinary catheters. 2014. Available from: https://www.nice.org.uk/guidance/qs61/chapter/Quality-statement-4-Urinary-catheters.
7. European Commission. Directorate-General for Research and Innovation. Gendered Innovations 2: How Inclusive Analysis Contributes to Research and Innovation. Publications Office of the European Union; 2020.
8. Abelson B, Sun D, Que L, et al. Sex differences in lower urinary tract biology and physiology. Biol Sex Differ. 2018;9:45. doi:10.1186/s13293-018-0204-8
9. Beeson T, Graham J, Vowell V, et al. Effectiveness and acceptability of a female external urine diversion device as an alternative to indwelling catheter use in acute care. J Wound Ostomy Continence Nurs. 2023;50(1):38–44. doi:10.1097/WON.0000000000000923
10. McRae AD, Thomas B, Parsons D, et al. Evaluation of external female urinary catheters: a retrospective analysis of efficacy and clinical outcomes. Continence. 2023;7:100750. doi:10.1016/j.cont.2023.100750
11. Pryor N, Wang J, Young J, et al. Clinical outcomes of female external urine wicking devices as alternatives to indwelling catheters: a systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2024;45(9):1121–1129. doi:10.1017/ice.2024.73
12. Organisation for Economic Co-operation and Development (OECD). Intellectual property and emerging technologies: IP-based approaches to technology transfers and licensing. OECD; 2020.
13. Cooper C, Powell P. Patient-centred design of medical technologies: a review of processes and outcomes. Health Technols. 2024;14:225–235. doi:10.1007/s12553-024-00818-0
14. European Commission. A new circular economy action plan: for a cleaner and more competitive Europe. COM(2020) 98 final. 2020. Available from: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:52020DC0098.
15. United Nations. Transforming our world: the 2030 agenda for sustainable development. 2015. Available from: https://documents.un.org/doc/undoc/gen/n15/291/89/pdf/n1529189.pdf.
16. Daim TU, Rueda G, Martin H, Gerdsri P. Forecasting emerging technologies: use of bibliometrics and patent analysis. Technol Forecast Soc Change. 2006;73(8):981–1012. doi:10.1016/j.techfore.2006.04.004
17. Lee JY, Lee SJ, Yoon B. Patent-based technology network analysis for identifying the technological trajectory and convergence. Res Policy. 2021;50(4):104215. doi:10.1016/j.respol.2021.104215
18. Jaffe AB, de Rassenfosse G. Patent citation data in social science research: overview and best practices. J Assoc Inf Sci Technol. 2017;68(6):1360–1374. doi:10.1002/asi.23731
19. Organisation for Economic Co-operation and Development (OECD). OECD Patent Statistics Manual. OECD Publishing; 2009.
20. de Rassenfosse G, Dernis H, Guellec D, Picci L, van Pottelsberghe de la Potterie B. The worldwide count of priority patents: a new indicator of inventive activity. arXiv. 2014. Available from: https://arxiv.org/abs/1309.5338.
21. European Parliament and Council of the European Union. Regulation (EU) 2017/745 of the European parliament and of the council of 5 April 2017 on medical devices. Off J Eur Union. 2017;L117:1–175.
22. International Electrotechnical Commission (IEC). Medical devices—Part 1: application of usability engineering to medical devices. IEC 62366-1:2015+A1:2020. Geneva, Switzerland: IEC; 2020.
23. International Organization for Standardization (ISO). Medical devices—application of risk management to medical devices. ISO 14971:2019. Geneva, Switzerland: ISO; 2019.
24. International Organization for Standardization (ISO). Biological evaluation of medical devices—Part 1: evaluation and testing within a risk management process. ISO 10993-1:2018. Geneva, Switzerland: ISO; 2018.
25. World Intellectual Property Organization (WIPO). PCT applicant’s guide. WIPO website. Available from: https://www.wipo.int/pct/en/guide/.
26. World Trade Organization (WTO). Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS). WTO website. 1994. Available from: https://www.wto.org/english/docs_e/legal_e/27-trips.pdf.
27. World Trade Organization (WTO). TRIPS and public health: exhaustion and parallel importation. WTO website. Available from: https://www.wto.org/english/tratop_e/trips_e/public_health_e.htm.
28. United States Patent and Trademark Office (USPTO). Manual of Patent Examining Procedure (MPEP). USPTO website. Available from: https://www.uspto.gov/web/offices/pac/mpep/index.html.
29. European Patent Office (EPO). Guidelines for examination. EPO website. 2024. Available from: https://www.epo.org/en/legal/guidelines-epc.
30. Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989;13(3):319–340. doi:10.2307/249008
31. Rogers EM. Diffusion of Innovations.
32. European Commission. Transforming institutions to foster responsible research. Research and Innovation website. Available from: https://research-and-innovation.ec.europa.eu/projects/success-stories/all/transforming-institutions-foster-responsible-research_en.
33. High-Level Expert Group on Artificial Intelligence. Ethics guidelines for trustworthy AI. Publications Office of the European Union; 2019. Available from: https://op.europa.eu/en/publication-detail/-/publication/d3988569-0434-11ea-8c1f-01aa75ed71a1.
34. European Patent Office (EPO). Espacenet: resource book/help and search guidance. EPO website. Available from: https://worldwide.espacenet.com/help?locale=en_EP.
35. World Intellectual Property Organization (WIPO). PATENTSCOPE user’s guide/search guidance. WIPO website. Available from: https://www.wipo.int/patentscope/en/users_guide.html.
36. Oficina Española de Patentes y Marcas (OEPM). INVENES database (patent search interface). OEPM website. Available from: https://consultas2.oepm.es/InvenesWeb/faces/busquedaInternet.jsp.
37. GodinezS, NoskowiczDS, DickinsonS, CovodeB; inventors; Medline Industries, Inc. assignee. Female external urinary device and assembly. International patent asspplication WO 2020033699 A1. 2020.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.