Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 12
Febrile Seizures: Evidence for Evolution of an Operational Strategy from an Armed Forces Referral Hospital
Authors Jain S ![]() , Santhosh A
, Santhosh A ![]()
Received 30 November 2020
Accepted for publication 10 February 2021
Published 25 March 2021 Volume 2021:12 Pages 151—159
DOI https://doi.org/10.2147/PHMT.S294729
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Video abstract of "Febrile seizures: Evolution of an operational strategy" [ID 294729].
Views: 369
Sunil Jain,1 Abhijith Santhosh2
1Department of Paediatrics, Command Hospital (Northern Command), Jammu & Kashmir, India; 2Medical Officer, Emergency Department, Command Hospital (Northern Command), Jammu & Kashmir, India
Correspondence: Sunil Jain
Professor & Head, Department of Paediatrics, Command Hospital (Northern Command), c/o 56 APO, 901131, India
Tel +91 9086068677
Email [email protected]
Purpose: Current recommendations for ‘Febrile seizures’ management include emergency first aid and treatment along with intermittent prophylaxis. Evidence of practices, efficacy, side-effects, and complications should lead to refined and rational management strategies.
Patients and Methods: Study of cases referred and treated at a tertiary level hospital, providing referral services to a large state in India. Evidence sought for the research questions identified, these were (i) immediate treatment: First aid components and practices; response to drug treatment (ii) intermittent prophylaxis: effectiveness, compliance, and side-effects (iii) complications arising due to treatment side-effects: quantifying the number of cases of CNS infections missed as a result of alterations in consciousness levels due to benzodiazepines.
Results: A total of 85 febrile seizure cases were studied. Full correct “First Aid” was provided by only 13 parents. Total 35 cases (41.18%) had seizures lasting more than 05 minutes. Emergency treatment for these included rectal diazepam in 14 cases with 57.14% success in terminating seizure, and intranasal midazolam in 21 cases with 71.43% success. The cases with persisting seizures were managed as status epilepticus treatment algorithm. Intermittent prophylaxis prevented recurrence of seizures in 90%, however side-effects were reported in 36.36%. There was no case of CNS infection missed.
Conclusion: Safe and effective management strategy should include “Health education” for correct first aid and ‘Protocols’ for timely and correct emergency treatment by parents/pre-hospital teams/emergency duty doctors. Intermittent prophylaxis is effective but refinements needed to minimize side-effects. Vigilant clinical monitoring obviates the fear that treatment may mask CNS infection.
Keywords: first aid, emergency treatment, prophylaxis, benzodiazepines, meningitis, monitoring
Plain Language Summary
The most common convulsive events are Febrile Seizures and these occur in 2–6% of the population. Emergency as well as recurrence management is important. We carried out this study for finding evidence for refinements in management of children with febrile seizures, including emergency and follow-up care.
On the basis of the evidence findings of our study and review of existing evidence, the best possible correct and comprehensive management of Febrile seizures should include (i) First aid: Stay calm; Protect the child from injury; Turn the child onto his or her side; Do not put anything in the child’s mouth; Loosen the child’s clothing, especially around the neck (ii) Emergency seizure care and/or control is always advisable. Emergency treatment is effective with proper protocols and parents/pre-hospital teams need to be aware of the correct steps for safe treatment. If the seizure lasts for longer than 5 minutes, treatment with diazepam, lorazepam, or midazolam is required. (iii) Intermittent prophylaxis for frequently recurring febrile seizures: It is effective. The benefit of such therapies is reduction, but not necessarily elimination of the risks of recurrence of febrile seizures (iv) Clinical monitoring should be done.
Introduction
The most common convulsive events are “Febrile Seizures” and these occur in 2–6% of the population.1 It is one of the most common childhood neurologic disorders.
Much attention worldwide has been that (i) treatments have no demonstrated ability to improve children’s long-term prognosis, and (ii) guiding the practitioner educate parents or caregivers about the low risks associated with simple febrile seizures (SFS).2 However, quality of life and safety are important aspects. Further recurrences should be a concern for all. Febrile seizures recur in approximately 30% of those experiencing a first episode, and this rises to 50% after two or more episodes, and to 50% if onset is at less than 1 year of age.3
Emergency correct management is important. Febrile seizures lasting more than 15 minutes are approximately 10%, and those lasting 30 minutes or longer are 5%.4 Treatment is with benzodiazepines, and phenobarbital, phenytoin, valproate, or levetiracetam may be needed in the case of febrile status epilepticus. A recent study has shown that 61% of children with prolonged febrile seizure (PFS), ie, lasting ≥15 min were medically treated by the ambulance paramedic. Only 45% of these responded to treatment.5 Another study on first aid for loss of consciousness (LOC) has found that recovery position reduces hospitalization rates. In this study, 26.6% of cases were due to febrile seizures, and this was the most common diagnosis.6 We carried out the study to assess response for this condition in our set-up.
Preventing recurrences is debatable and questionable. However, this should be of concern and receive research attention based on the following reasons (i) quality of life (ii) parental anxiety, even after counseling (iii) complications/mortality may occur. In adult patients with epilepsy, the risk of death is roughly two to three times more than expected in a matched population without epilepsy. A significant number of these patients die from accidents, status epilepticus, etc.7 The American Academy of Pediatrics (AAP) clinical practice guideline states that
In children there is a theoretical risk of a child dying during a SFS as a result of injury, aspiration, or cardiac arrhythmia. However, to the committee’s knowledge, this has never been reported.2
Children are in learning phase of life (and less experienced!) in precautions/prevention of accidents and all seizures should be concerning. Intermittent prophylaxis is recommended in cases of frequently recurring febrile seizures given during febrile illnesses.
Complications of treatment also should be concerning. Benzodiazepines also have the potential of masking an evolving central nervous system (CNS) infection. A study in India on prevalence of bacterial meningitis in 6–18 months old children presenting with a first episode of seizures with fever has reported the prevalence of meningitis as (i) 2.4% in children with first febrile seizures, (ii) 0.86% in SFS, and (iii) 4.81% in complex febrile seizures (CFS).8 From US a study to find the rate of acute bacterial meningitis in children presenting with first CFS has reported 0.9% incidence.9 We need to assess do we miss diagnosis of CNS infection in cases receiving benzodiazepines. This is especially important when and where there is no routine pneumococcal vaccination program.
Our ultimate aim is to find evidence for an operational strategy, which is clientele based and patient centered for this common condition.
Patients and Methods
Aims
Evolution of comprehensive operational strategy with study for answers to the research questions identified, given in Table 1.
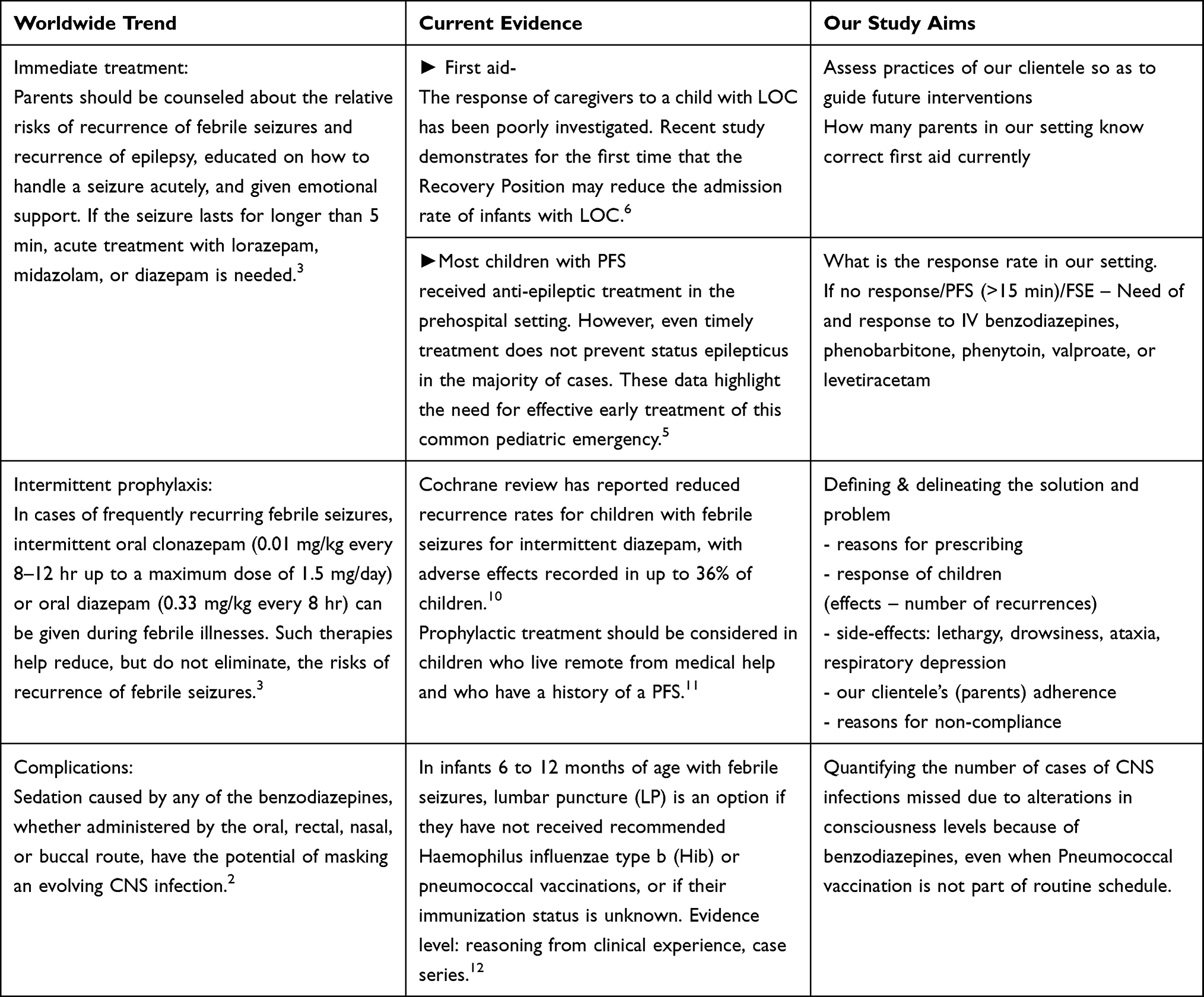 |
Table 1 Aims of the Study |
Setting
A tertiary level hospital providing referral services to a large operationally active Command area in India.
Subjects
All patients with seizures and fever in age group 06 to 60 months.
Inclusion Criteria and Definitions
Febrile seizures are seizures that occur between the age of 6 and 60 months with a temperature of ≥38°C (100.4°F), that are not the result of CNS infection or any metabolic imbalance, and that occur in the absence of a history of prior afebrile seizures.2
A simple febrile seizure (SFS) is a primary generalized, usually tonic-clonic, attack associated with fever, lasting for a maximum of 15 min, and not recurrent within a 24-hr period. A complex febrile seizure (CFS) is more prolonged (>15 min), and/or is focal, and/or recurs within 24 hr. Febrile status epilepticus (FSE) is a febrile seizure lasting longer than 30 min.3
Sample Size
Between 2% and 5% of neurologically healthy infants and children experience at least 1, usually SFS.3 Recurrence of febrile Seizures depends upon the number of risk factors, and ranges from 12% to 100%. Taking the average of this (56%), the sample size has been calculated as 79 cases of febrile seizure, at an allowable error of 20%.
Study Parameters
Clinical characteristics, Emergency treatment, and Intermittent prophylaxis, Complication monitoring.
Intermittent Prophylaxis
This was advised in cases of frequently recurring febrile seizures and included intermittent oral clonazepam (0.01 mg/kg every 8–12 hr up to a maximum dose of 1.5 mg/day) or oral diazepam (0.33 mg/kg every 8 hr) given during febrile illnesses.
Emergency Management Protocols
These practiced were (i) If the seizure lasts for longer than 5 min, acute treatment with rectal diazepam or intranasal midazolam, followed by intravenous lorazepam if seizure not controlled. Rectal diazepam and intranasal midazolam was prescribed to families to be used at home as a rescue medication if a febrile seizure lasts longer than 5 min. (ii) For uncontrolled seizure/seizure lasting more than 15 minutes intravenous (IV) phenobarbital 15 mg/kg. Subsequent IV fosphenytoin 20 mg/kg or IV valproic acid 40 mg/kg or IV levetiracetam 60 mg/kg (iii) In cases of frequently recurring febrile seizures, intermittent oral clonazepam (0.01 mg/kg every 8–12 hr up to a maximum dose of 1.5 mg/day) or oral diazepam (0.33 mg/kg every 8 hr) was prescribed.3,13 (iv) (iv) Vigilant clinical monitoring of signs and symptoms for complications. Common symptoms monitored included that is headache, nausea, vomiting, anorexia, photophobia, restlessness, altered state of consciousness, and irritability. Common signs of CNS infection monitored included fever, neck pain and rigidity, focal neurologic deficits, seizures, obtundation, and coma. CSF examination was done in cases with clinical suspicion of CNS infection, and further testing as guided by the results.
Results
A total of 85 cases were studied. Findings of clinical characteristics studied and research questions explored are given in Tables 2–5. The ages of the children studied was 6–60 months and male to female ratio was 1.24:1, details in Table 2. Overall the time for reaching nearest medical facility/Command Hospital (Northern Command) was 10–45 minutes. Distance from home to nearest medical facility/Command Hospital (Northern Command) ranged between 02 and 35 km. Immunization complete for age against Haemophilus influenza type b (Hib) was 80% and Pneumococcal was 60%. The emergency management protocols for seizures lasting more than 5 minutes were required in 35 (41.18%) patients, details in Table 3. Intermittent prophylaxis was prescribed in 25 (29.41%) cases. The compliance rate was 80%, with effectiveness in 90% these children. Details of side-effects (36.33%) and non-compliance (20%) are given in Table 4. Non-compliance was in 60% due to side-effect of drowsiness.
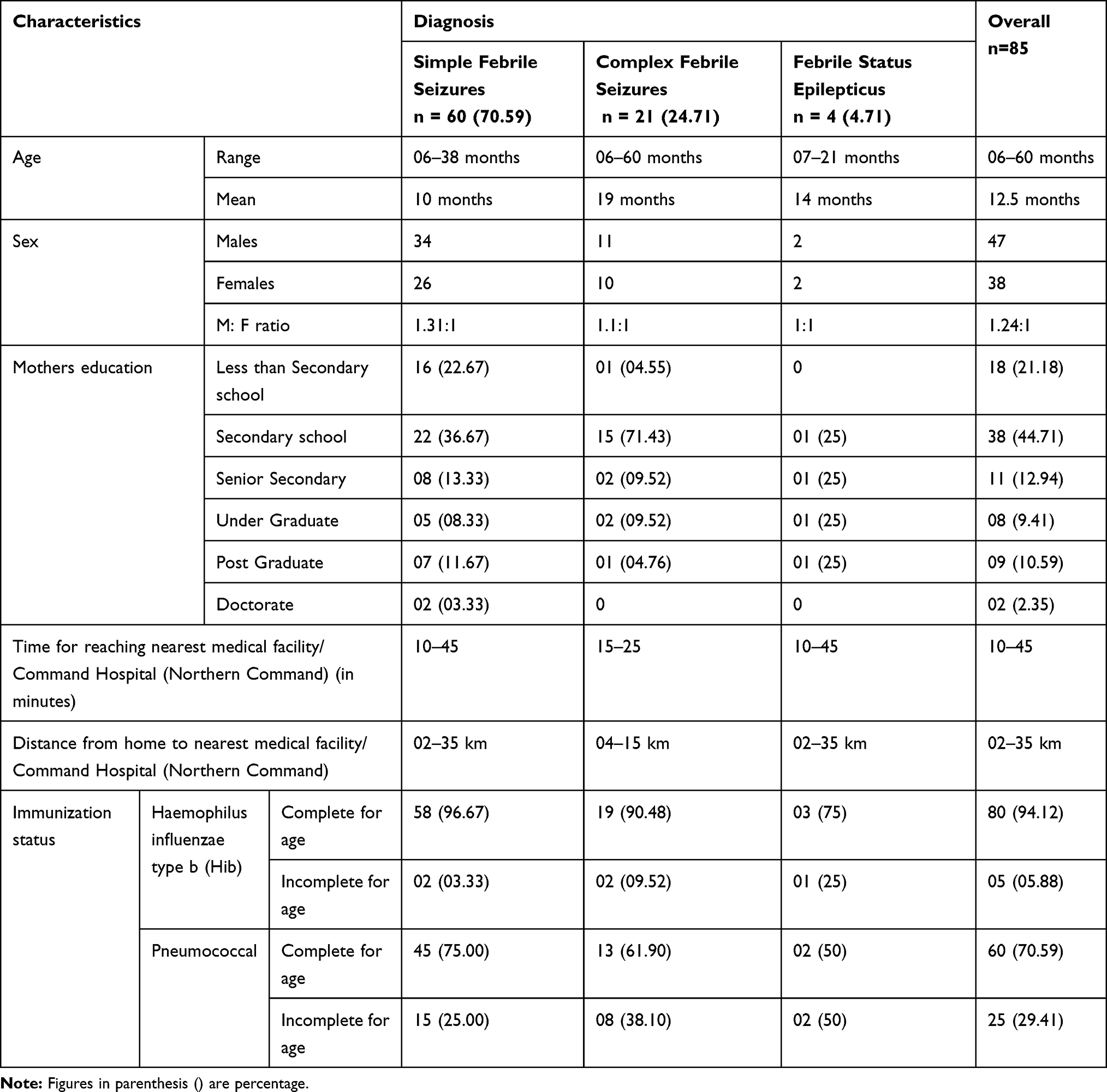 |
Table 2 Clinical Characteristics |
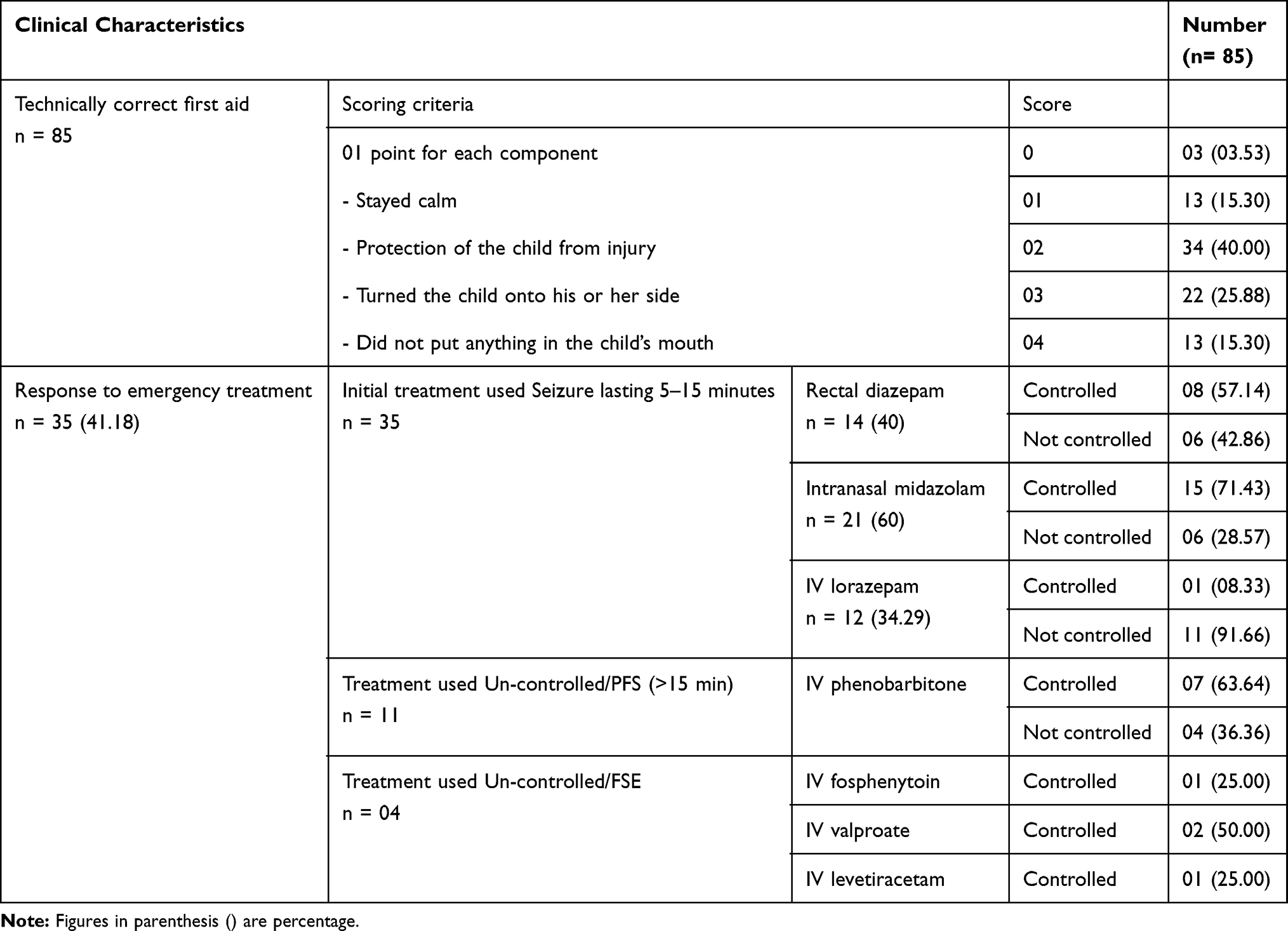 |
Table 3 Research Question Findings: Immediate Treatment |
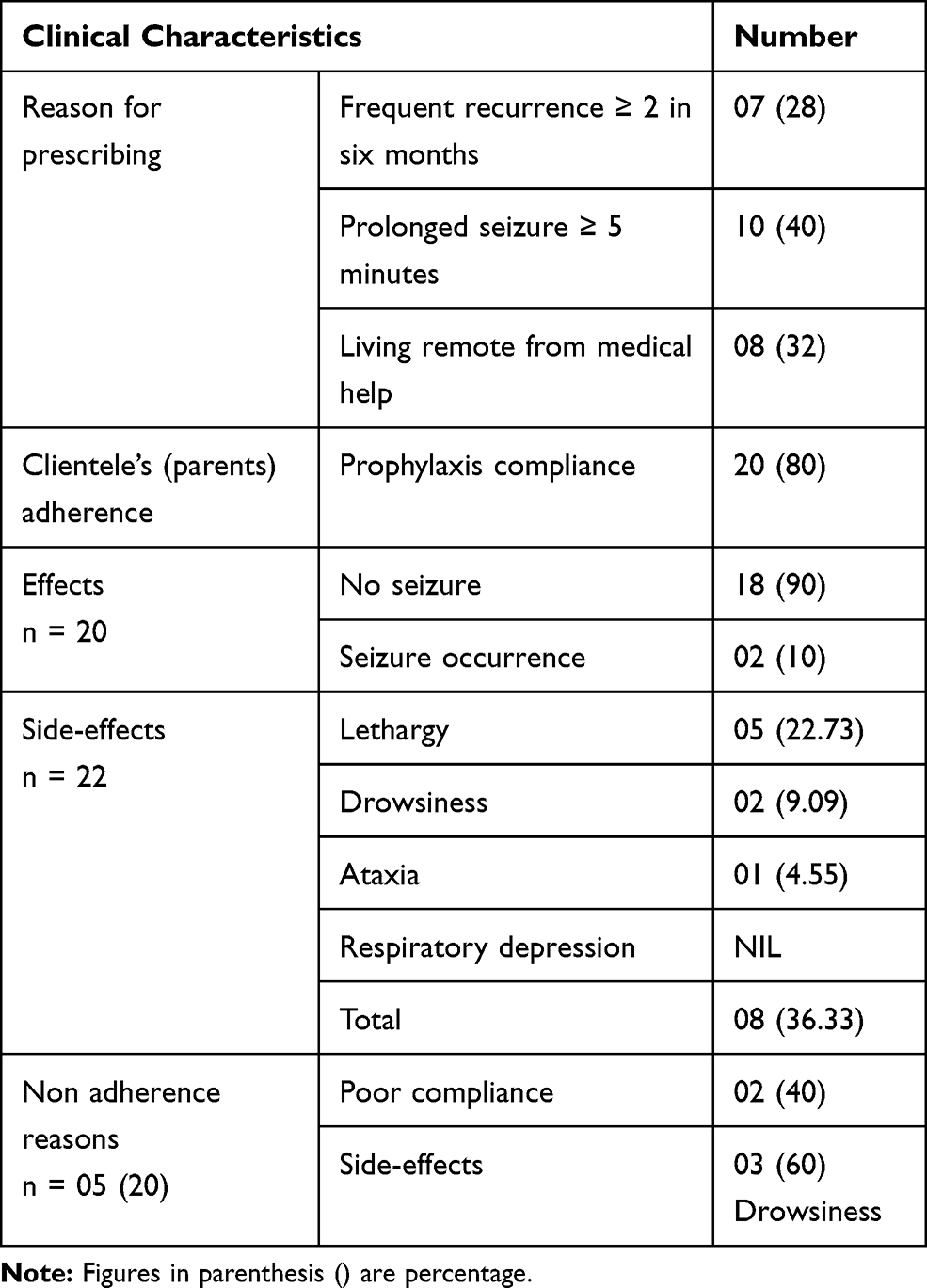 |
Table 4 Research Question Findings: Intermittent Prophylaxis n=25 |
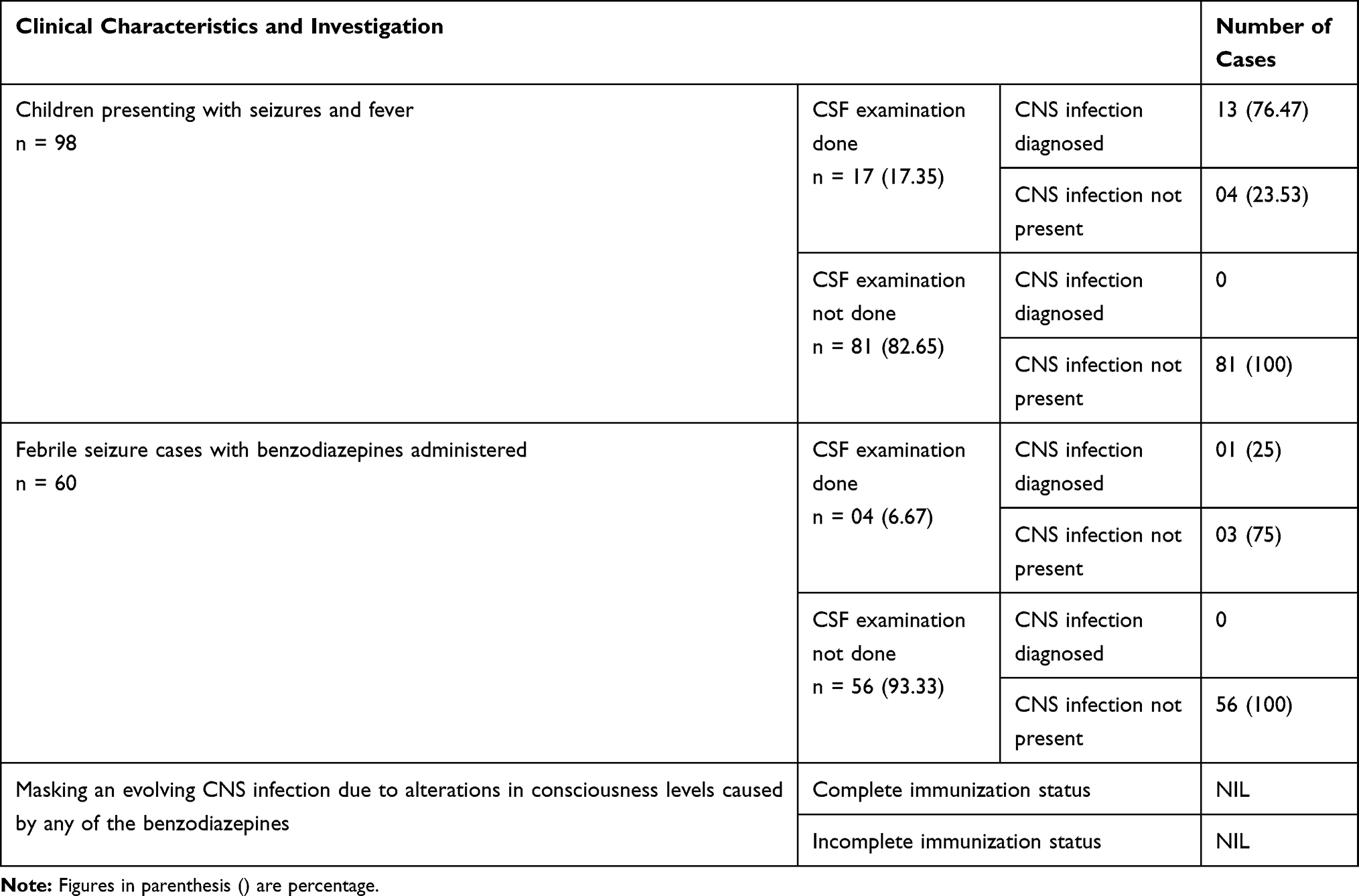 |
Table 5 Research Question Findings: Complication – CNS Infection |
The details for CNS infection complication are given in Table 5. These put in perspective are (i) 98 children presented with fever and seizures. (ii) CSF examination done in 17 with 13 (76.47%) cases showing positive results and not included in the study. (iii) Out of 85 cases included in the study 60 had benzodiazepines administered, and out of these 04 had clinical suspicion of CNS infection and had CSF examination done. Out of these 01 (25%) was diagnosed as meningitis and managed for it. Implication of this is that when clinical suspicion of CNS infection is there and CSF examination done positivity rate is 76.47% and in cases with benzodiazepines administered the results of CSF examination with clinical suspicion of CNS infection the positivity rate is only 25%. These interesting findings should guide our practice relying on clinical skills. Mortality in our study was nil.
Discussion
Common conditions require correct management by all, and parents are most often the first responders for children. Improvements desirable and possible by reviewing practices and refining strategies. Operational strategies are especially important when families are residing in distant and difficult terrains. The referral hospital where this study carried out caters to the health needs of such population.
Febrile seizures have a peak incidence between 1 and 1–1/2 years of age.14 In our study, the overall mean age of patients presenting with febrile seizures was 12.5. The mean age for SFS was 10 months, CFS was 19 months, and FSE was 14 months in our study.
Time for reaching nearest medical facility or our hospital ranged between 10 minutes to 45 minutes. Hence, the important need of parental education on correct first aid and intermittent prophylaxis if indicated, as on time medical consultation may not always be possible.
Emergency correct management prevents complications and saves lives. Correct “First Aid” components are (i) Stay calm (ii) Protect the child from injury (iii) Turn the child onto his or her side (iv) Do not put anything in the child’s mouth. Full correct “First Aid” was provided by only 13 parents (15.30%). This should also include “Loosen the child’s clothing, especially around the neck”15 especially for temperate climate residents. Health education is needed in this regard to improve this. Efforts should include mass health education campaigns for “First aid” for different emergencies including seizures, and specific educational sessions for families with history of seizures.
If the seizure lasts for longer than 5 min, acute treatment with diazepam, lorazepam, or midazolam is required. Rectal diazepam is often prescribed for administration at the time of recurrence. Alternatives are buccal or intranasal midazolam.3
In recent years, efforts to improve the administration of anticonvulsant drugs through rapid non-invasive routes have become common in pre-hospital care. This is especially pertinent in pediatric practice, as IV access may be not easy.16 Findings from a study of 28 children in the pre-hospital setting showed that buccal midazolam was safe and effective. Seizures were terminated in 75% in midazolam group vs 59% in diazepam group.17 A subsequent randomized controlled trial carried out in children also reported buccal midazolam to be better than rectal diazepam.18 In our study rectal diazepam had 57.14% success, while intranasal midazolam had 71.43% success in terminating the seizure. In 12 cases in which seizures were not controlled with rectal diazepam or intranasal midazolam IV lorazepam was used. This could control seizure in only 01 case and the rest had to be administered IV Phenobarbital. Subsequent to this 04 cases were uncontrolled, and out of these in 01 case seizures controlled with IV fosphenytoin, 02 cases with IV valproate, and 01 case with IV levetiracetam (Table 3).
Evolving evidence and teaching has led to rational treatment. In 1999 MacDonald et al had commented that “overtreatment of Febrile convulsions continues”. This was the result of findings of “The National General Practice Study of Epilepsy”, a large community-based cohort study of 1195 patients carried out prospectively.19
Emergency seizure care and/or control is always advisable. Current recommendations for prophylaxis are (i) Intermittent prophylaxis for frequently recurring febrile seizures. The benefit of such therapies is reduction, but not necessarily elimination of the risks of recurrence of febrile seizures. (ii) Continuous therapy not recommended for majority of cases. The justifications for this are the side effects risks and no demonstrated long-term benefits, although the recurrence rate of febrile seizures is decreased.3 The Cochrane Systematic Review on “Prophylactic drug management for febrile seizures in children” has concluded that as recurrent febrile seizures have benign nature and anticonvulsants have high prevalence of adverse effects, parents and families should be just supported. The support should be as contact details of medical services and information on recurrence including first aid management.10
In our study, only intermittent prophylaxis was prescribed. Reasons for prescribing were medical in 68% and living remote from medical help in 32%. The effectiveness was 90%, but 36.36% had side effects (Table 4). The Cochrane Systematic review has reported that in up to 36% receiving benzodiazepine adverse effects were recorded.10 In our study non-adherence to the prescribed prophylaxis was 20%, and the reason in majority of these (60%) was drowsiness side-effect (Table 4). These findings point towards need of refinements for safe administration of this effective prophylaxis. None of our patients were placed on continuous prophylaxis.
Lower comprehension scores in children prescribed phenobarbitone have been reported. The Cochrane Systematic review results state that in general in up to 30% of children treated with phenobarbitone adverse effects are recorded.10 Hence, we recommend tapering phenobarbitone if used in emergency treatment.
A perspective of concern is sedation caused by any of the benzodiazepines, whether administered by the oral, rectal, nasal, or buccal route. This has potential of masking an evolving CNS infection. In our study out of 98 children presenting with seizures and fever, CNS infection was diagnosed in 13 cases and the rest were classified as “Febrile seizures”. Out of the 60 children with febrile seizures with benzodiazepines administered, CSF examination was done in only 04 (6.67%) cases as clinical suspicion of CNS infection was there and the rest were intensively monitored. Out of these only one case had meningitis while CSF examination in the rest three was negative. Out of the cases monitored clinically, none had CNS infection (Table 5). Thus, in our study, there was no masking of an evolving CNS infection. Clinical vigilant monitoring is all that is needed. The various symptoms and signs elucidated in Methods section are comprehensive and all need to be focused upon. A study of children between the ages of 1 months to 5 years for diagnosis of acute bacterial meningitis found that chief presentation was high fever, refusal of feeds, altered sensorium and seizures. Meningeal signs were present in only 26%.20 Viral meningitis typically presents with acute onset of fever, headache, photophobia, neck stiffness, and nausea/vomiting. Young children may present with fever and irritability without evidence of meningeal irritation.21 The clinical cues for encephalitis and encephalopathy are altered mental status (suggested by decreased or altered level of consciousness, lethargy or personality change), fever ≥38° C (100.4°F), and new onset of focal neurologic findings.22
The findings of a recent study on CFS, LP, and CNS Infections reported that rates of LP have been declining. However, it is still performed in 25% of Emergency Department visits for CFS. CNS infection was diagnosed in only 0.30% of cases. This points that the procedure could be avoided in many patients.23
Conclusion
The recommendations for evolving an effective strategy for correct and comprehensive management of febrile seizures are (i) Health education for correct first aid (ii) Emergency treatment is effective with proper protocols and parents/pre-hospital teams/emergency duty doctors need to be apprised for correct steps for safe treatment (iii) Intermittent prophylaxis is effective but refinements needed to minimize side-effects (iv) Vigilant clinical monitoring obviates the fear that treatment may mask CNS infection. Based on these evidences the current best practices are summarized as:
“Parents: No panic but proper “First aid” and
professional consultation.
Medical professionals: Confidence in clinical skills”.
Ethics
The study was conducted in accordance with the Declaration of Helsinki. The study was reviewed and approved by the ethics committee, named the “Command Hospital (Northern Command) Institutional Ethics Committee”, and informed consent of parents obtained for all cases studied.
Acknowledgments
Thankful to all the infants, children, and their parents for participation in the study. Thankful to all the emergency health staff of Command Hospital (Northern Command) and MI Rooms/Field Hospitals referring the patients.
Disclosure
The authors report no financial interest or any other conflict of interest in this work.
References
1. Camfield P, Camfield C. Febrile seizures and genetic epilepsy with febrile seizures plus (GEFS+). Epileptic Disorders. 2015;17(2):124–133. doi:10.1684/epd.2015.0737
2. AAP Steering. Committee on Quality Improvement and management, subcommittee on febrile seizures. Febrile seizures: clinical practice guideline for the long-term management of the child with simple febrile seizures. Pediatrics. 2008;121(6):1281–1286. doi:10.1542/peds.2008-0939
3. Mikati MA, Tchapyjnikov D. Febrile Seizures. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, editors. Nelson Textbook of Pediatrics.
4. Berg AT, Shinnar S. Complex febrile seizures. Epilepsia. 1996;37(2):126–133. doi:10.1111/j.1528-1157.1996.tb00003.x
5. Bassan H, Barzilay M, Shinnar S, Shorer Z, Matoth I, Gross-Tsur V. Prolonged febrile seizures, clinical characteristics, and acute management. Epilepsia. 2013;54(6):1092–1098. doi:10.1111/epi.12164
6. Julliand S, Desmarest M, Gonzalez L, et al. Recovery position significantly associated with a reduced admission rate of children with loss of consciousness. Arch Dis Child. 2016;101(6):521–526. doi:10.1136/archdischild-2015-308857
7. Lowenstein DH. Seizures and Epilepsy. In: Jameson JL, Fauci AS, Kasper DL, Hauser SL, Longo D, Loscalzo J, editors. Harrison’s Principles of Internal Medicine.
8. Batra P, Gupta S, Gomber S, Saha A. Predictors of meningitis in children presenting with first febrile seizures. Pediatr Neurol. 2011;44(1):35–39. doi:10.1016/j.pediatrneurol.2010.07.005
9. Kimia A, Ben-Joseph EP, Rudloe T, et al. Yield of lumbar puncture among children who present with their first complex febrile seizure. Pediatrics. 2010;126(1):62–69. doi:10.1542/peds.2009-2741
10. Offringa M, Newton R, Cozijnsen MA, Nevitt SJ. Prophylactic drug management for febrile seizures in children. Cochrane Database Sys Rev. 2017;Issue 2:CD003031.
11. Farrell K, Goldman RD. The management of febrile seizures. BC Med J. 2011;53(6):268–273.
12. AAP. Subcommittee on febrile seizures. Febrile seizures: guideline for the neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics. 2011;127(2):389. doi:10.1542/peds.2010-3318
13. Mikati MA, Tchapyjnikov D. Status Epilepticus. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, editors. Nelson Textbook of Pediatrics.
14. Leung AKC, Hon KL, Leung TNH. Febrile seizures: an overview. Drugs in Context. 2018;7:212536. doi:10.7573/dic.212536
15. Capovilla G, Mastrangelo M, Romeo A, Vigevano F. Recommendations for the management of “febrile seizures”: ad Hoc Task Force of LICE Guidelines Commission. Epilepsia. 2009;50(Suppl 1):2–6. doi:10.1111/j.1528-1167.2008.01963.x
16. Silverman EC, Sporer KA, Lemieux JM, et al. Prehospital care for the adult and pediatric seizure patient: current evidence-based recommendations. West J Emerg Med. 2017;18(3):419–436. doi:10.5811/westjem.2016.12.32066
17. Scott RC, Besag FM, Neville BG. Buccal midazolam and rectal diazepam for treatment of prolonged seizures in childhood and adolescence: a randomised trial. Lancet. 1999;353(9153):623–626. doi:10.1016/S0140-6736(98)06425-3
18. McIntyre J, Robertson S, Norris E, et al. Safety and efficacy of buccal midazolam versus rectal diazepam for emergency treatment of seizures in children: a randomised controlled trial. Lancet. 2005;366(9481):205–210. doi:10.1016/S0140-6736(05)66909-7
19. MacDonald BK, Johnson AL, Sander JW, Shorvon SD. Febrile convulsions in 220 children–neurological sequelae at 12 years follow-up. Eur Neurol. 1999;41(4):179–186. doi:10.1159/000008048
20. Chinchankar N, Mane M, Bhave S, et al. Diagnosis and outcome of acute bacterial meningitis in early childhood. Indian Pediatr. 2002;39(10):914–921.
21. Cantu RM, Das M, Viral Meningitis J. StatPearls [Internet]. Available from. Treasure Island (FL): StatPearls Publishing;2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545217/.
22. Venkatesan A, Tunkel AR, Bloch KC, et al. International Encephalitis Consortium. Case definitions, diagnostic algorithms, and priorities in encephalitis: consensus statement of the international encephalitis consortium. Clin Infect Dis. 2013;57(8):1114–1128. doi:10.1093/cid/cit458
23. Lee J, Delaroche AM, Janke AT, Kannikeswaran N, Levy PD. Complex febrile seizures, lumbar puncture, and central nervous system infections: a national perspective. Acad Emerg Med. 2018;25(11):1242–1250. doi:10.1111/acem.13441
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.