Back to Journals » Clinical Interventions in Aging » Volume 18
Feasibility of Permanent His Bundle Pacing in the Elderly vs the Very Elderly. A Single-Center Mid-Term Follow-Up Study
Authors Pestrea C ![]() , Cicala E, Gherghina A, Ortan F, Pop D
, Cicala E, Gherghina A, Ortan F, Pop D ![]()
Received 29 March 2023
Accepted for publication 8 June 2023
Published 13 June 2023 Volume 2023:18 Pages 941—949
DOI https://doi.org/10.2147/CIA.S412808
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Catalin Pestrea,1– 3 Ecaterina Cicala,1 Alexandra Gherghina,1 Florin Ortan,1 Dana Pop2,3
1Department of Interventional Cardiology, Brasov County Clinical Emergency Hospital, Brasov, 500326, Romania; 2 5th Department of Internal Medicine, Faculty of Medicine, “Iuliu Hațieganu” University of Medicine and Pharmacy, Cluj-Napoca, 400012, Romania; 3Department of Cardiology, Clinical Rehabilitation Hospital, Cluj-Napoca, 400347, Romania
Correspondence: Catalin Pestrea, Brasov County Clinical Emergency Hospital, Brasov, 500326, Romania, Tel +40745003637, Email [email protected]
Purpose: Although feasibility studies have included older patients, specific data for His bundle pacing (HBP) in this population is scarce. The aim of this study was to evaluate the feasibility and mid-term performance of HBP in the elderly (70 to 79 years old) versus the very elderly (80 years old and above) patients with conventional indications for pacing.
Patients and Methods: About 105 patients older than 70 years of age with attempted HBP from the 1st of January 2019 to the 31st of December 2021 were reviewed. Clinical and procedural characteristics were recorded at baseline, and after a mid-term follow-up period.
Results: The procedural success rate was similar in both age groups (68.49% vs 65.62%). There was no significant difference in pacing or sensing thresholds, impedance, and fluoroscopy times. For both age intervals, patients with a baseline narrow QRS maintained a similar QRS duration after pacing, while in patients with a wide QRS, the paced QRS was significantly shorter. Baseline QRS duration, left bundle branch block morphology, and ejection fraction, were significantly associated with HBP procedural failure. The mean follow-up period was 830.34 days for the elderly and 722.76 days for the very elderly. After the follow-up period, both sensing and pacing thresholds were similar between the groups. Compared to the baseline values, there were no significant changes in both pacing and sensing parameters, irrespective of the age interval. During follow-up, no lead dislodgements were recorded. There were two cases of significant pacing threshold rise in the elderly (4%) and three cases in the very elderly group (14.2%) which were managed conservatively, without lead revision.
Conclusion: In elderly and very elderly patients, HBP is a feasible procedure associated with constant pacing and sensing parameters and with low complication rates over mid-term follow-up.
Keywords: conduction system pacing, elderly and very elderly, feasibility study, mid-term follow-up
Introduction
Cardiac pacing is a life-saving procedure performed worldwide as a routine daily practice. For decades, right ventricular pacing (RVP) has been the “gold standard” of myocardial pacing for bradyarrhythmias. Unfortunately, increasing scientific data has shown that conventional RVP is associated with a significant decline in left ventricular function as a result of electrical and mechanical dyssynchrony, a condition termed pacing-induced cardiomyopathy.1 Most studies on this topic identified the paced QRS duration and the burden of ventricular pacing as major factors in pacing-induced cardiomyopathy development.2
Consequently, several alternatives to conventional RVP have been studied and amongst them, His bundle pacing (HBP), which promotes biventricular depolarization using the specialized cardiac conduction system, emerged as the most physiological option. This procedure gained significant popularity after the development of dedicated delivery tools.3 Comparative studies have proven the superiority of HBP over RVP in terms of death and hospitalizations for heart failure.4 Also, randomized studies showed noninferiority of HBP compared to biventricular pacing in patients with heart failure and left bundle branch block (LBBB).5 The key feature of HBP, compared to any other pacing method is a very narrow QRS complex, which minimizes one of the risk factors for heart failure, as explained above.
Since more than 80% of all pacemakers are implanted in patients above 65 years of age, and up to 14% are implanted in patients older than 85 years of age, mostly in the setting of sinus node disease or atrioventricular (AV) block, there is a justified question about the benefit of HBP in the elderly.6 Conduction system disorders seen in the elderly develop mostly due to age-related degenerative changes and idiopathic fibrosis, but also secondary to comorbidities (ischemic disease, both acute and chronic, infiltrative disease, collagen vascular disease, neuromuscular disease, endocarditis, surgical or interventional trauma, adverse effects of different therapies).7 Aging leads to varying degrees of degenerative changes and calcification in the region of the central fibrous body, affecting the AV node, His bundle, as well as the proximal right or left bundle.8
Although feasibility studies have included older patients, specific data for HBP in this population is scarce. Furthermore, there is a general concern for high-pacing thresholds and for the progression of conduction disease beyond the pacing site, which may lead to a significant progressive rise in capture thresholds over time.
The aim of this study was to evaluate the feasibility and mid-term performance of permanent HBP in the elderly (70 to 79 years old) versus the very elderly (80 years old and above) patients with conventional indications for cardiac pacing (bradyarrhythmias or electrical resynchronization therapy).
Materials and Methods
Study Design
This was an analytical, retrospective study with data collected from a single center.
Patient Selection
Consecutive patients over 70 years old, who underwent an attempt at permanent HBP, either for bradycardia indications or for electrical resynchronization therapy, between the 1st of January 2019 and the 31st of December 2021 in the Cardiac Pacing Laboratory of the Brașov County Clinical Emergency Hospital in Romania, were analyzed for eligibility. Patients without a clearly identified intraprocedural His bundle electrocardiogram (HBE) were excluded. In the end, 105 patients were included in the study. According to their age, the patients were divided into two groups: the elderly group (70–79 years old) and the very elderly group (80 years old and above).
The demographic and clinical characteristics of the patients were recorded at baseline.
Pacing Procedure
The protocol used for HBP at our institution was the following: the C315 His catheter (Medtronic, Minneapolis, MN, USA) with the Select Secure 3830 lead (Medtronic, Minneapolis, MN, USA) inside were advanced at the level of the anteroseptal tricuspid annulus (Figure 1A). The HBE was identified using unipolar mapping (Figure 1B) and, at that site, pacing at different amplitudes was performed to evaluate His bundle capture. If the HBE could not be identified after a maximum of ten minutes of fluoroscopy or the His bundle capture threshold was higher than 2 Volts at 1-ms pulse duration, the HBP procedure was abandoned and other pacing options were considered.
 |
Figure 1 (A) Posteroanterior fluoroscopy image showing the final placement of a pacing lead in the right atrial appendage and a pacing lead at the level of the His bundle; (B) intraprocedural tracing during a 2:1 suprahisian AV block revealing the His bundle electrogram (*); (C) intraprocedural electrograms during His bundle capture threshold testing demonstrating the transition (marked by the black arrow), between non-selective and selective His bundle pacing. |
In patients with baseline narrow QRS complexes, selective HBP was defined as a paced QRS complex and an ST-T interval identical to the baseline morphologies and an isoelectric line between the pacing artifact and the beginning of the QRS complex. Non-selective HBP was defined as a lack of isoelectric line after the pacing artifact, with a “pseudo-delta” aspect at the beginning of the QRS complex and a transition with decremental pacing amplitude from non-selective HBP to either selective HBP or pure myocardial capture (Figure 1C).9
In patients with baseline-wide QRS complex, successful His bundle capture was considered when there was a correction of the bundle branch block or the paced QRS complex duration was lower than 130 ms.
In successful HBP cases, no ventricular backup leads were implanted.
Procedural pacing and sensing thresholds, as well as the fluoroscopy times, were recorded.
Follow-Up
The follow-up visits after the procedure were performed in the outpatient clinic at 1,3 and 6 months, and then every 6 months. Sensing and pacing thresholds, as well as late complications, were recorded during follow-up.
Statistical Analysis
Continuous data were presented as mean ± one standard deviation and categorical data as frequencies and percentages. All study groups were assessed for the normality of data distribution. For samples with normally distributed population data, parametric tests like the t-test for independent or dependent groups were used to compare means. Otherwise, the comparison of means was performed using the Mann–Whitney U-test for independent groups or the Wilcoxon test for dependent groups. The association between continuous and dichotomous variables was assessed using binomial logistic regression. A 95% confidence interval was considered for all tests and a p < 0.05 was interpreted as statistically significant.
Statistical analysis was done using the SPSS software v 26.0 (IBM, Armonk, NY, USA).
Ethical Aspects
The study received approval from the institutional ethics committee and was conducted according to the recommendations of the Declaration of Helsinki.
Prior to the cardiac pacing procedure, all patients were informed and provided written consent.
Results
The baseline characteristics of the patients are shown in Table 1.
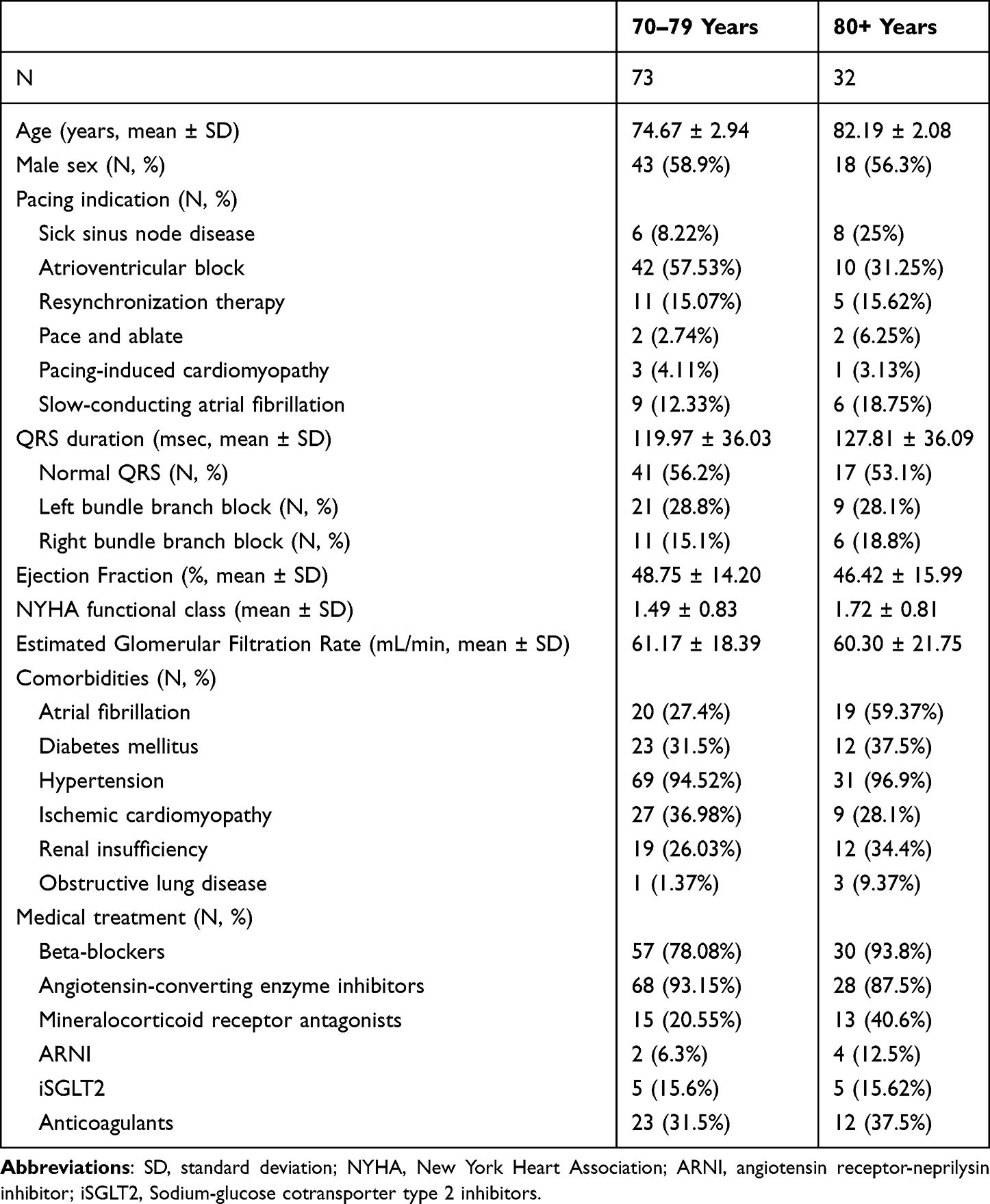 |
Table 1 Baseline Patient Characteristics |
The main indication for cardiac pacing in both groups was AV nodal dysfunction in the form of AV block, slow-conducting atrial fibrillation, and the pace-and-ablate strategy (72.6% in the elderly and 56.25% in the very elderly group). There was no significant difference between the two groups in terms of baseline QRS duration (p = 0.297), ejection fraction (p = 0.834), New York Heart Association (NYHA) functional class (p = 0.152), and estimated glomerular filtration rate (p = 0.840). There were similar percentages of LBBB and right bundle branch block (RBBB) patterns, but a higher prevalence of atrial fibrillation in the very elderly group.
Procedural Characteristics
All the procedural characteristics are presented in Table 2.
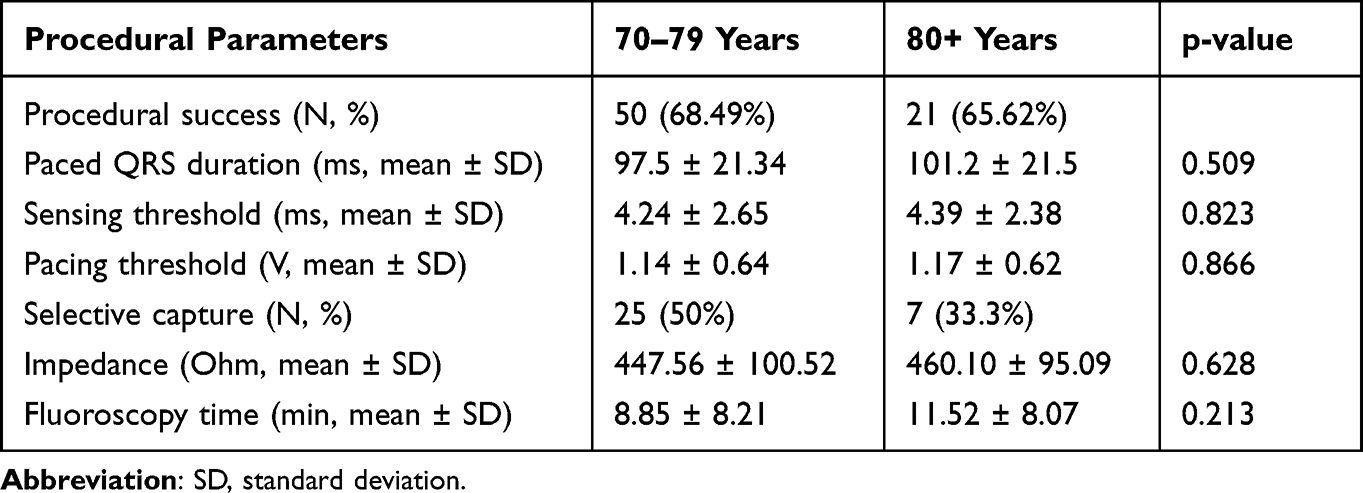 |
Table 2 Procedural Characteristics |
The procedural success rate was similar in both age groups (68.49% vs 65.62%). The reason for procedural failure was His bundle capture at unacceptably high thresholds. In successful cases, there was no significant difference in pacing threshold, sensing threshold, impedance, and fluoroscopy time. In the elderly group, selective HBP was achieved more frequently.
The paced QRS complex duration was non-statistically different between the study groups. Also, for both age intervals, patients with a baseline narrow QRS complex maintained a similar QRS duration after pacing, while in patients with a wide QRS complex, irrespective of the baseline bundle branch block morphology, the paced QRS was significantly shorter (Figure 2).
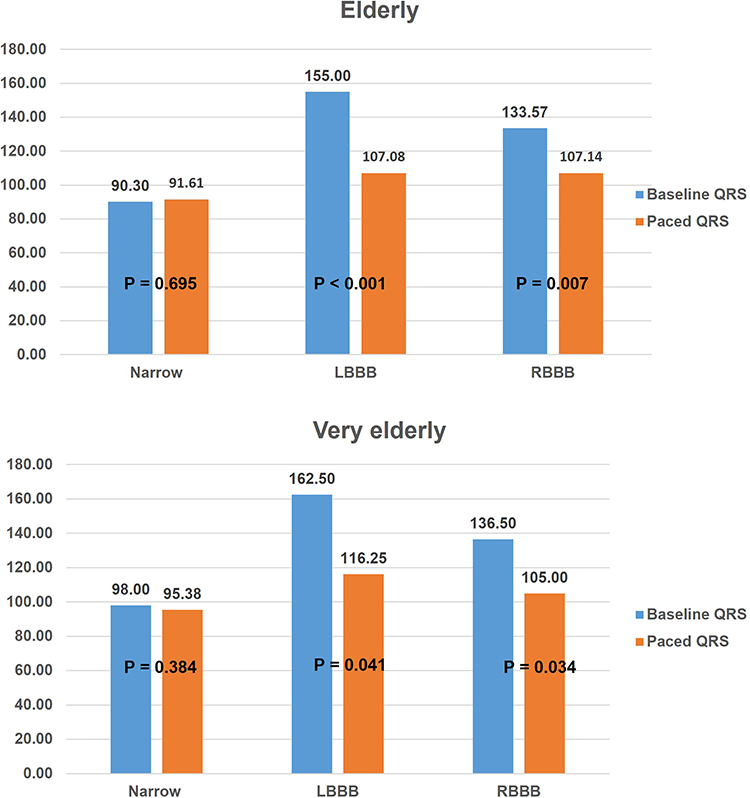 |
Figure 2 Comparison of QRS duration between baseline and postprocedural values. Abbreviations: LBBB, left bundle branch block; RBBB, right bundle branch block. |
In the next step, the association between several patient characteristics and permanent HBP outcome was evaluated using binary logistic regression. Of all the parameters studied, baseline QRS duration, LBBB morphology, and ejection fraction were significantly associated with HBP procedural failure (Table 3).
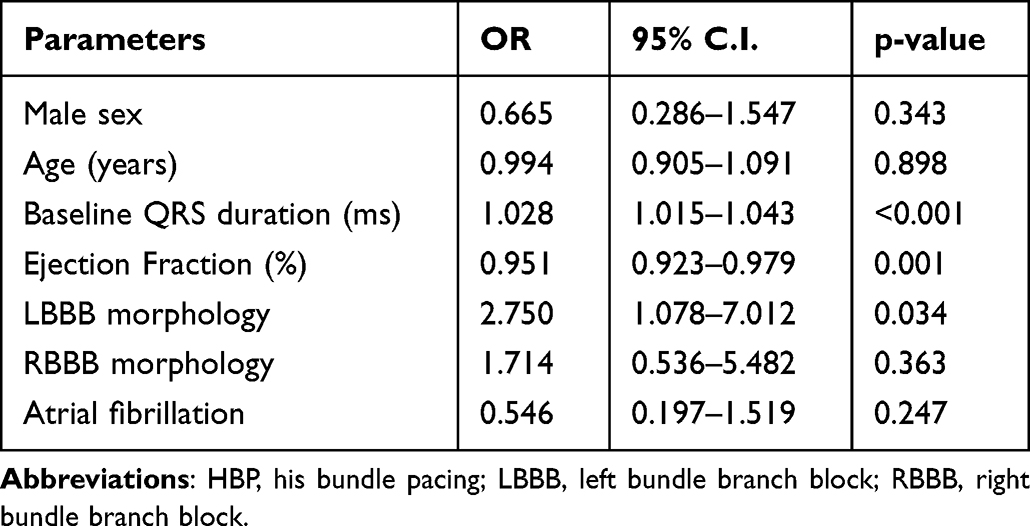 |
Table 3 Logistic Regression Analysis Between Patient Characteristics and HBP Failure |
Follow-Up
The mean follow-up period was non-statistically different for the two age groups. Six patients (12%) died in the elderly and 8 patients (38.1%) in the very elderly group during follow-up due to causes unrelated to the procedure. At the last follow-up visit, both sensing and pacing thresholds were similar between the groups (Table 4).
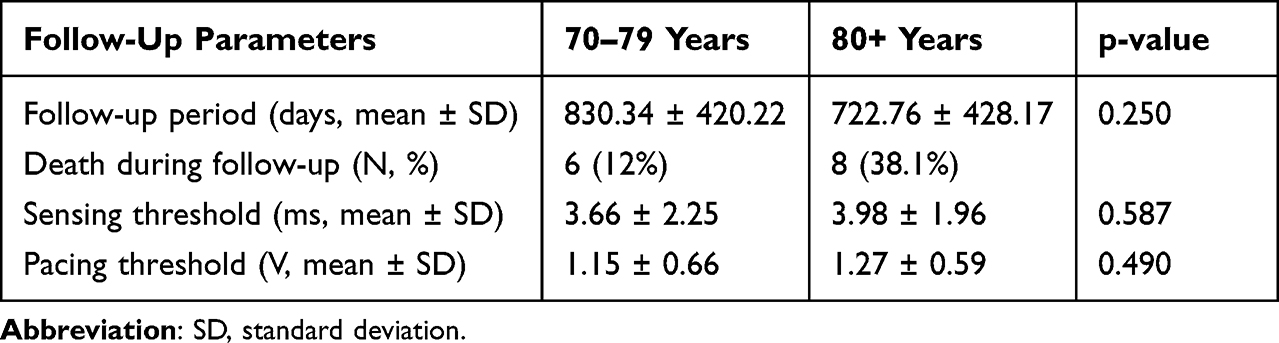 |
Table 4 Follow-Up Parameters for the Two Study Groups |
Compared to the baseline values, at the end of the follow-up period, there were no significant changes in both pacing and sensing parameters, irrespective of the age interval (Figure 3).
 |
Figure 3 Comparison of periprocedural and follow-up pacing and sensing thresholds. |
Complications
A significant postprocedural pocket hematoma was noted in three elderly patients and in two very elderly patients. All patients were under anticoagulant treatment and fortunately, all were managed conservatively. One case of large postprocedural pericardial effusion was encountered in the elderly group, which was drained percutaneous, without further recurrences.
During follow-up, no lead dislodgements were recorded. There were two cases of significant pacing threshold rise in the elderly (4%) and three cases in the very elderly group (14.2%) which were managed conservatively, without lead revision.
Discussion
The main findings of this study were that: (i) there was no statistical difference in permanent HBP procedural characteristics, and no statistical difference in follow-up parameters between the elderly and very elderly groups, and (ii) there was no difference between the baseline and follow-up parameters in the two age groups.
Previous feasibility studies for HBP showed an overall success rate of around 80%, which was reduced to 70% for patients with a wide baseline QRS complex.10 The patient characteristics in those multicenter studies were similar to the ones we reported in the present study. Over half of the patients were implanted for AV block or slowly conducted atrial fibrillation and 40% of the patients had a QRS complex larger than 120 ms. The particularities of our HBP technique were lower implemented procedural parameter cut-off values regarding both pacing thresholds and fluoroscopy times (2 V and 10 min, respectively). These aspects accounted for the better parameter values recorded in our study and probably explained in part the reduced procedural success compared to previous studies.
Non-selective HBP was more frequently achieved in the very elderly group. This was a result of a more distal placement of the lead, on the ventricular side of the His bundle, due to the concern of conduction disease progression in this age group, with a risk of His bundle capture malfunction. If this situation had occurred, the lead would act as its own backup by maintaining myocardial septal capture.
Two randomized studies evaluated the benefit of HBP compared to biventricular pacing in patients with heart failure and LBBB.5,11 In these studies, successful HBP, defined as a significant reduction in the QRS duration was achieved in 52% and 72% of patients, respectively. In our study, both baseline ejection fraction and LBBB morphology were significantly associated with procedural failure. Interestingly, although intrinsic QRS duration was significantly associated with procedural outcomes, apparently this was determined only by an LBBB morphology since baseline RBBB morphology had no impact on final procedural success. In failed procedures, LBBB may be a marker of a more distal conduction disease, which cannot be corrected by HBP. On the other hand, a lower ejection fraction is usually associated with modified cardiac anatomy, such as enlarged ventricles and atria, displacing the His bundle and thus, making it more difficult to reach and capture.
It is a known fact that HBP is the technique associated with the narrowest-paced QRS complex, superior to both left bundle branch pacing and biventricular pacing.12 The explanation for this phenomenon is the concomitant activation of both ventricles through the specialized conduction system. Existing data has shown that, in a significant percentage of patients, HBP can correct both LBBB and RBBB morphologies due to the capture and activation of fibers beyond the site of the bundle branch block.13 The findings of our study supported these observations. Patients with a baseline narrow QRS complex maintained the same QRS duration, while patients with wide baseline QRS (irrespective of the morphology) had a significantly lower QRS in both age groups.
One of the concerns regarding permanent HBP is the possible increase in capture threshold over time. Previous studies reported an increase in the pacing threshold to higher than 2.5 V in up to 27% of the patients and loss of His bundle capture in 7.6% of the patients.14 One of the few existing data on HBP feasibility in octogenarians and nonagenarians yielded threshold rises at 6-month follow-up occurring in 7% of the patients.15 In our study, both pacing and sensing thresholds were stable over time. There were no lead dislodgments recorded. Only 4% of the patients in the elderly group and 14.2% of the patients in the very elderly group had a threshold rise above 2.5 V, but none of them led to the interruption of HBP as the matter was resolved by device reprogramming. We believe that the lower incidence of threshold rise in our study was explained by the initial excellent pacing thresholds, which suggested adequate fixation of the lead in the conduction system, a very important endpoint since we did not use any ventricular backup leads. Furthermore, especially in patients over 80 years of age, a higher pacing amplitude leading to faster battery depletion is of less concern than in younger patients since it may anyway possibly exceed their life expectancy. There were five cases in total of postprocedural pocket hematomas in anticoagulated patients, with no infections occurring during follow-up. This complication was expected since older age is associated with a higher risk of bleeding and due to the fact that we usually performed the procedures under uninterrupted vitamin K antagonist treatment with an International Normalized Ratio value of 2 to 2.5, or with the withdrawal of direct oral anticoagulants for 24 hours prior to the procedure and resumption the day after. All cases were managed successfully with local compressive bandages.
To our knowledge, this is the only study that reported the mid-term performance of His bundle leads specifically in the elderly population. An important limitation of long follow-ups in studies involving old patients is the significantly reduced life expectancy in these age groups, especially over 80 years. Also, a limitation of this study was the retrospective nature of data collection from a single center, which limits the strength of the evidence. We included only patients with an identified His bundle electrogram. In a prospective setting, probably with the preferential use of, the now available, deflectable delivery catheters and a more flexible procedural technique, the localization of the His bundle and consequently the success rates could be different.
The key point of this study evaluating elderly and very elderly patients is that, once His bundle capture is achieved with low pacing thresholds, the risk of future complications that would lead to HBP interruption is low, at least in the medium term. This alleviates the need for a backup ventricular pacing lead, which increases the procedural costs and risk. Given the higher percentage of comorbidities in this group and the structural modifications of the heart associated with aging, conventional RVP could accelerate the decline in left ventricular function, making physiological pacing an attractive and feasible option in these patients.
Conclusions
In elderly and very elderly patients, HBP is a feasible procedure associated with constant pacing and sensing parameters, as well as with low complication rates over a mid-term follow-up.
Data Sharing Statement
The datasets are available upon reasonable request to the corresponding author.
Ethical Statement
The study was approved by the Ethics Board of the Brasov County Emergency Clinical Hospital (Number 30/21.02.2022) and the Ethics Board of the “Iuliu Hațieganu” University of Medicine and Pharmacy in Cluj-Napoca (Number AVZ34/14.02.2022). The study respected all the ethical principles of the Seventh Revision of the Helsinki Declaration from 2013.
Consent for Publication
Informed consent was signed by all patients involved in the study prior to the cardiac pacing procedure.
Funding
This research received no external funding.
Disclosure
Catalin Pestrea has received speaker and proctorship fees from Medtronic. The authors report no other conflicts of interest in this work.
References
1. Kiehl EL, Makki T, Kumar R, et al. Incidence and predictors of right ventricular pacing-induced cardiomyopathy in patients with complete atrioventricular block and preserved left ventricular systolic function. Heart Rhythm. 2016;13(12):2272–2278. doi:10.1016/j.hrthm.2016.09.027
2. Khurshid S, Liang JJ, Owens A, et al. Longer paced QRS duration is associated with increased prevalence of right ventricular pacing-induced cardiomyopathy. J Cardiovasc Electrophysiol. 2016;27(10):1174–1179. doi:10.1111/jce.13045
3. Zanon F, Ellenbogen KA, Dandamudi G, et al. Permanent His-bundle pacing: a systematic literature review and meta-analysis. Europace. 2018;20(11):1819–1826. doi:10.1093/europace/euy058
4. Abdelrahman M, Subzposh FA, Beer D, et al. Clinical outcomes of his bundle pacing compared to right ventricular pacing. J Am Coll Cardiol. 2018;71(20):2319–2330. doi:10.1016/j.jacc.2018.02.048
5. Upadhyay GA, Vijayaraman P, Nayak HM, et al. On-treatment comparison between corrective His bundle pacing and biventricular pacing for cardiac resynchronization: a secondary analysis of the His-SYNC Pilot Trial. Heart Rhythm. 2019;16(12):1797–1807. doi:10.1016/j.hrthm.2019.05.009
6. DePaula RS, Antelmi I, Vincenzi MA, et al. Cardiac arrhythmias and atrioventricular block in a cohort of asymptomatic individuals without heart disease. Cardiology. 2007;108(2):111–116. doi:10.1159/000095950
7. Chow GV, Marine JE, Fleg JL. Epidemiology of arrhythmias and conduction disorders in older adults. Clin Geriatr Med. 2012;28(4):539–553. doi:10.1016/j.cger.2012.07.003
8. Lim WY, Prabhu S, Schilling RJ. Implantable cardiac electronic devices in the elderly population. Arrhythm Electrophysiol Rev. 2019;8(2):143–146. doi:10.15420/aer.2019.3.4
9. Vijayaraman P, Dandamudi G, Zanon F, et al. Permanent his bundle pacing: recommendations from a multicenter his bundle pacing collaborative working group for standardization of definitions, implant measurements, and follow-up. Heart Rhythm. 2018;15(3):460–468. doi:10.1016/j.hrthm.2017.10.039
10. Keene D, Arnold AD, Jastrzębski M, et al. His bundle pacing, learning curve, procedure characteristics, safety, and feasibility: insights from a large international observational study. J Cardiovasc Electrophysiol. 2019;30(10):1984–1993. doi:10.1111/jce.14064
11. Vinther M, Risum N, Svendsen JH, Møgelvang R, Philbert BT. A randomized trial of his pacing versus biventricular pacing in symptomatic HF patients with left bundle branch block (his-alternative). JACC Clin Electrophysiol. 2021;7(11):1422–1432. doi:10.1016/j.jacep.2021.04.003
12. Tokavanich N, Prasitlumkum N, Mongkonsritragoon W, et al. A network meta-analysis and systematic review of change in QRS duration after left bundle branch pacing, His bundle pacing, biventricular pacing, or right ventricular pacing in patients requiring permanent pacemaker. Sci Rep. 2021;11(1):12200. doi:10.1038/s41598-021-91610-8
13. Sharma PS, Naperkowski A, Bauch TD, et al. Permanent his bundle pacing for cardiac resynchronization therapy in patients with heart failure and right bundle branch block. Circ Arrhythm Electrophysiol. 2018;11(9):e006613. doi:10.1161/CIRCEP.118.006613
14. Zanon F, Abdelrahman M, Marcantoni L, et al. Long term performance and safety of His bundle pacing: a multicenter experience. J Cardiovasc Electrophysiol. 2019;30(9):1594–1601. doi:10.1111/jce.14063
15. Saini A, Khan MZ, Saini H, et al. Abstract 15012: his bundle pacing in the elderly - acute success, feasibility and safety in the octogenarian and nonagenarian population. Circulation. 2018;138:A15012.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.