")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Fear, Loneliness, Happiness and Mental Health in the Post-COVID-19 Period: A Cross-Cultural Study in a Sample of Japanese and Polish University Students
Authors Klinkosz W , Styk W , Iskra J , Trzepińska G
Received 28 March 2023
Accepted for publication 26 June 2023
Published 18 July 2023 Volume 2023:16 Pages 2695—2707
DOI https://doi.org/10.2147/PRBM.S414702
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Waldemar Klinkosz,1 Wojciech Styk,2 Justyna Iskra,3 Greta Trzepińska1
1Institute of Psychology, Cardinal Stefan Wyszynski University in Warsaw, Warsaw, Poland; 2Department of Psychology, Medical University of Lublin, Lublin, 20-059, Poland; 3The John Paul II Catholic University of Lublin, Lublin, Poland
Correspondence: Wojciech Styk, Email [email protected]
Background: During the COVID-19 pandemic, interpersonal relations were highly constrained due to the social distancing rules and sanitary restrictions imposed to prevent the transmission of the virus. These social changes gave rise to ever-deepening experiences of loneliness, deterioration of mental well-being, and fear of COVID-19, which affected the citizens of all the countries struggling with the pandemic.
Methods: The present paper reports the results of a study on mental health, interdependent happiness, loneliness and fear of COVID-19 in Polish and Japanese university students. A total of 180 people (83 Poles and 97 Japanese) aged 19– 41 participated in the study. The participants were surveyed using the Mental Health Continuum-Short Form to assess three dimensions of mental health; the UCLA Three-Item Loneliness Scale to measure loneliness; the Interdependent Happiness Scale based on the concept of a relational sense of community with others as associated with well-being, and the Fear of COVID-19 Scale (FCV-19S). The respondents were also asked one question about their subjectively perceived economic status.
Results: The largest cross-cultural difference in the investigated variables concerned fear of COVID-19. The Japanese university students showed higher levels of this fear. The level of fear of COVID-19 in the group of women, regardless of the culture they came from, was not associated with any other variables we analyzed. In the Japanese sample, it was negatively correlated with interdependent happiness, and in the Polish sample, fear od COVID-19 was only correlated with the Social dimension of Mental Health. Other variables that differentiated the two nationalities, though to a lesser extent, were the Social dimension of Mental Health, which was higher in the Japanese sample, and the Psychological dimension of Social Health, with higher scores in the Polish sample.
Conclusion: The power of mental resources, although it may vary among individuals, is independent of culture. Regardless of the level of fear of COVID-19 in the two cultures, the examined mental resources are positively associated with well-being and the return to normal functioning after the pandemic.
Keywords: fear of COVID-19, post-COVID-19 period, well-being, interdependent happiness, loneliness, individualism, collectivism
Introduction
During the COVID-19 pandemic, social participation changed radically due to the high transmission rate of the virus. World Health Organization data from March 2023 indicate that nearly 275 million people in Europe have contracted Covid-19. Almost 2200 people have died. Worldwide, nearly 676 million people have been infected with Covid-19 and 6.7 million have died (representing 10% of those infected).1 To limit the spread of the disease, the governments of many countries imposed severe restrictions on social contact. Lockdowns, quarantines and social distancing limited direct interactions between people. While justified, the social measures taken have not been without consequences for the well-being of those who had to adhere to them Social isolation and other changes to daily life have affected the wellbeing and the level of loneliness of those subject to the restrictions.2 Loneliness became a problem that most of the population locked up in their homes and deprived of everyday interpersonal encounters had to face. Contact with other people was restricted as everyone had to wear masks and abide by other protection measures taken to contain the virus: bans on leaving home, quarantine and social distancing. All countries introduced social contact regulations, which put a curb on social interactions to varying degrees, inhibiting the naturalness and spontaneity of interpersonal relationships. The lockdown/post-lockdown periods generated temporally and demographically distinct COVID-19 related fears patterns, with special regard to youth and elderly, two particularly vulnerable populations when faced with sudden and unexpected dramatic events.3,4 The “lockdown” measures, adopted to restrict population movements in order to help curb the novel coronavirus disease 2019 (COVID-19) pandemic, contributed to a global mental health crisis. After lifting the lockdown, a statistically significant increase in suicidal behavior and psychomotor agitation was observed, as well as a decrease in diagnoses of behavioral disorders.5,6 As research shows, the COVID-19 pandemic significantly reduced the ability to cultivate interpersonal relationships, resulting in feelings of loneliness and experiences of social isolation.7 Understanding the determinants of increased feelings of loneliness in the pandemic is important as loneliness is a significant predictor of the onset or severity of symptoms of depression and anxiety disorders.8 Labrague’s research found that the increase in loneliness was also affected university students.9 Studies conducted in the Polish population have shown similar relationships.2
An epidemic state was declared in Poland on 20 March 2020, restricting movement and the operation of commercial, service and catering premises, and imposing a quarantine order on people who may have come in contact with the virus.1 The social changes introduced at the national level, similarly to the global measures, have had an impact on people’s lives. The epidemic has had serious effects on the social and mental functioning of many individuals.10–12 Having the virus or a family member having the virus, fear for loved ones, financial problems caused by the freezing of the economy, and difficult access to medical care have all had an adverse effect on people. Confirmed cases of infection and the high mortality caused by the virus has contributed to the emergence of mental problems.10,11 The quality of life and the quality of social interactions has deteriorated. Of no small importance were also minor inconveniences and difficulties related to the pandemic, such as the obligation to wear masks, which intensified negative feelings and were responsible for the worsening of people’s mental health. The severity and duration of the restrictions had different effects on the occurrence of depression, and stress and anxiety levels. Tight restrictions were associated with the intensification of depressive symptoms, relaxed restrictions led to a high level of anxiety, while short-term restrictions were related to a high level of stress, undoubtedly having an impact on people’s well-being.13
The issue of mental well-being has been drawing more and more attention in recent years. Well-being refers to both measurable, external factors and internal, subjective mental states, assessed on the basis of the values that a particular person deems important.14 Well-being can also be popularly understood as “happiness” and be associated with a significant predominance of positive affect over negative affect. This definition puts emphasis on the pleasant emotional sensations that a person either feels at a particular moment in life or is prone to feel in general.15 A sense of well-being is undoubtedly related to one’s satisfaction with life and the culture which one comes from. Cross-cultural studies have shown differences in life satisfaction and well-being between representatives of different nationalities and ethnic minorities.16,17 The differences in well-being between different countries correlate with average income levels in those countries. This may be due to the fact that rich countries tend to have higher social indicators, including those related to human rights, equality, life expectancy, and democracy.18
Experiences of happiness also vary from culture to culture. The concept of happiness may not only be understood differently in different cultures, but it also may be associated with completely distinct experiences or behaviors. This is important when measuring and comparing happiness across cultures. Cultural research shows, for instance, that people from the East Asian cultural sphere assess their current sense of happiness taking into account the “ups and downs” they have faced over their entire lives.19 If they are going through a more difficult period but expect the situation to improve in the near future, their sense of happiness is not affected. People from the Japanese cultural sphere are more likely to see negative experiences as inherent components of their current sense of happiness.20 Additionally, in Japanese culture, which is oriented toward interdependent happiness, being much happier than those around you is seen as inharmonious and disruptive. The concept of interdependent happiness is based on the Japanese view of happiness.21 It has less to do with one’s self-actualization and more with the feelings and experiences of the people around. For the Japanese, positive hedonistic experiences are closely related to a sense of belonging to a community and a sense of harmony with others, while in individualistic cultures, such experiences are associated with individual achievement and self-actualization.22
Prolonged, forced isolation can lead to loneliness, which can be damaging to people’s health and life satisfaction, both on an individual and social scale.23–25 Social isolation is a risk factor for a number of diseases as well as increasing mortality. The feeling of loneliness is one of the most common effects of forced isolation. Social distancing used as one of the main measures to contain the spread of coronavirus left people much more socially isolated than they had been before the pandemic.13 Feelings of social and emotional loneliness were experienced particularly strongly by women, especially those with high levels of social isolation.26 The study of Turkish adult demonstrated that COVID-19 stress predicted resilience and COVID-19 burnout. Resilience predicted COVID-19 burnout and the relationship between COVID-19 burnout and COVID-19 stress was partially mediated by resilience.27
The aim of the present study was to compare the Polish and Japanese university students after the COVID-19 pandemic in terms of fear of coronavirus, well-being, interdependent happiness and loneliness. The pandemic, as well as the resulting social changes are new phenomena that had never occurred before on such a large scale. Having found ourselves in the post-pandemic period, we wanted to learn whether people still felt the fear of COVID-19 and whether this fear was related to their interdependent happiness, sense of loneliness and mental health. We also wondered if the anxiety caused by the pandemic had different effects on the studied variables in the analyzed cultures.
Material and Methods
Mental Health
The Mental Health Continuum-Short Form is a scale designed to assess three dimensions of mental health encompassing its hedonic and eudaimonic aspects. The scale consists of 14 items, which respondents rate on a six-point scale (1 - never, 6 - every day), indicating how many times they have felt each emotion in the past month. People can be classified as doing well or doing poorly (flourishing/languishing) in terms of well-being. To be able to say that an individual is coping well (flourishing), they must respond “every day” or “almost every day” to at least seven items, one of which must come from the hedonic dimension. Individuals coping badly (languishing) report that they “never” or “once or twice” experienced at least seven of the symptoms included in the questionnaire, of which at least one must come from the hedonic dimension. The scale allows one to measure emotional, social, and psychological well-being.15 The participants in the Polish sample were surveyed using the Polish version of the test by Karaś et al.28 The Japanese participants were surveyed with the Japanese version of the test by Sakano et al.29 Reliability measured by the Cronbach’s alpha coefficient did not differ from data obtained on other samples and was, depending on the scale, 0.85 to 0.86 for the Polish sample and 0.81 to 0.85 for the Japanese sample.
Loneliness
Loneliness was measured using the UCLA Three-Item Loneliness Scale. The scale consists of three items and a simplified set of response categories, but it has good psychometric properties. Using a three-point scale, respondents indicate how often they have felt a lack of company, a sense of alienation, and isolation from others. The higher the score obtained, the stronger the sense of loneliness the respondents felt.30 The Polish translation by Czerwiński20 was used to survey the participants in the Polish sample, while the Japanese version of the test by Igarashi was used to test the Japanese respondents.21 Reliability measured by Cronbach’s alpha coefficient did not differ from data obtained on other samples and was 0.78 for the Polish sample and 0.77 for the Japanese sample.
Interdependent Happiness
The Interdependent Happiness Scale by Hitokoto and Uchida is based on the concept of a relational sense of community with others as associated with well-being. Put differently, it measures the sense of happiness derived from harmonious relationships with other people Using a five-point scale, respondents rate items representing three factors. Relationship-oriented happiness or harmony with others refers to a harmonious state of balance between the self and significant others. Quiescence refers to being in a state of low arousal serving to protect social norms. The Eastern conception of wellness is considered to be a state of low activation, best described by words such as “peaceful” or “serene”, whereas the happiness preferred in independent cultures is described as “exci- ted” or “enthusiastic”. Such quiescence is thus a significant aspect of interdependent happiness. Ordinariness describes the trait of being indistinguishable from others, of being average. Due to the strong relationship between these factors, the summed score of all the subscales of the questionnaire comprising the global index of interdependent happiness was included in the analysis of the results.31 The Japanese sample was surveyed using the original Japanese-language version of the scale, while the Polish participants completed the Polish-language version of the scale.32 Reliability measured by Cronbach’s alpha coefficient did not differ from data obtained on other samples and was 0.84 for the Polish sample and 0.85 for the Japanese sample.
Fear Related to COVID-19
The Fear of COVID-19 Scale (FCV-19S) by Ahorsu et al measures the discomfort associated with the coronavirus pandemic, including the fear of infection or death and somatic symptoms that arise at the thought of coronavirus. The respondents use a seven-point scale to evaluate the intensity to which they experience the particular emotions (fear of infection or death) and somatic symptoms (palm sweating, accelerated heartbeat) arising in them at the thought of coronavirus.33 The Polish version of the test by Pisula and Nowakowska was used to survey the Polish participants.34 The Japanese participants filled in the Japanese version of the test by Midorikawa et al.35 Reliability measured by Cronbach’s alpha coefficient did not differ from data obtained on other samples and was 0.88 for the Polish sample and 0.82 for the Japanese sample.
Subjective Social Status
In order to assess the respondents’ subjectively perceived economic status, they were asked the following question: How would you describe your family’s economic status? Responses were given on a six-point scale from “below average” to “definitely above average”.
Procedure
The data for the study was partly collected online and partly in paper-and-pencil form. The surveys were conducted in the period from March till June 2022. Once they had given their consent to participate in the study, the online participants received a direct link to the questionnaires, while the paper-and-pencil participants received printouts of the questionnaires. The content of the paper and electronic versions of the questionnaires was identical. Instructions were provided at the beginning and before each questionnaire. There was no set time limit, but the participants were informed what the estimated time needed to participate in the study was. The Japanese version of the survey was conducted entirely online. Recruitment of Japanese participants was done with the help of cooperating academics at Japanese universities. Instructions on the purpose of the study and ethical principles were provided and communicated during recruitment. In addition, in the link to the study provided, participants were informed about the purpose of the study and the possibility to opt out at any time without consequences. In the Polish version of the survey, 47 people filled in the questionnaires electronically and 36 people completed paper-and-pencil measures. The participants were also informed that participation was anonymous and voluntary, and that they could withdraw from the study at any time without any consequences.
Statistical Analyses
Statistical analyses were performed using JASP 0.16.3. The data we collected were first analyzed to determine which of them could be subjected to parametric tests. For data which could be evaluated using parametric tests, Student’s t-tests and Pearson’s r-correlation analysis were run to compare groups. For the remaining data, the Mann–Whitney test and Spearman’s rho analysis were used. The significance of differences between correlations in the samples was determined with Fisher’s Z-test using an online calculator available at www.psychometrica.de
Study Sample Characteristics
The participants in the study were full-time undergraduate students. The survey targeted university students in major urban centres. The aim was to recruit people who stayed in large cities during the pandemic, regardless of where they originally came from. We did not consider the student’s major or their place of origin (eg, urban or rural). A total of 180 participants (70 women and 110 men) took part in the study. In the Polish sample (n=83), 70% of the participants were women. In the Japanese sample (n=97), women represented 51.54% of the respondents. The age of the participants ranged from 19 to 41 (M = 27; SD = 5.65).
Results
Analysis of Variables in the Samples
To establish the differences between the populations studied, the mean values of the test variables were first compared. The calculated means and the statistical significance are given in Table 1. The analyses showed that the surveyed groups of Poles and Japanese differed statistically significantly in the level of perceived fear of COVID-19. In the Japanese population, this level was twice as high (M=25.14; SD=8.81) as in the Polish population (M=11.06; SD=3.96). Another variable that differentiated the two populations was the level of Mental Health as assessed on the Psychological Well-being and Social Well-being scales. Psychological well-being was higher in the Polish group (M=22.63; SD=6.39) than in the Japanese group (M=20.63; SD=6.92), whereas social well-being was higher in the Japanese group (M=16.16; SD=5.89) compared to the Polish group (M=14.31; SD=5.18). The effect size of the differences measured with Cohen’s d was the greatest for perceived fear of COVID-19 (d = 1.6), and it can be classed as large. The other differences had small effect sizes.36
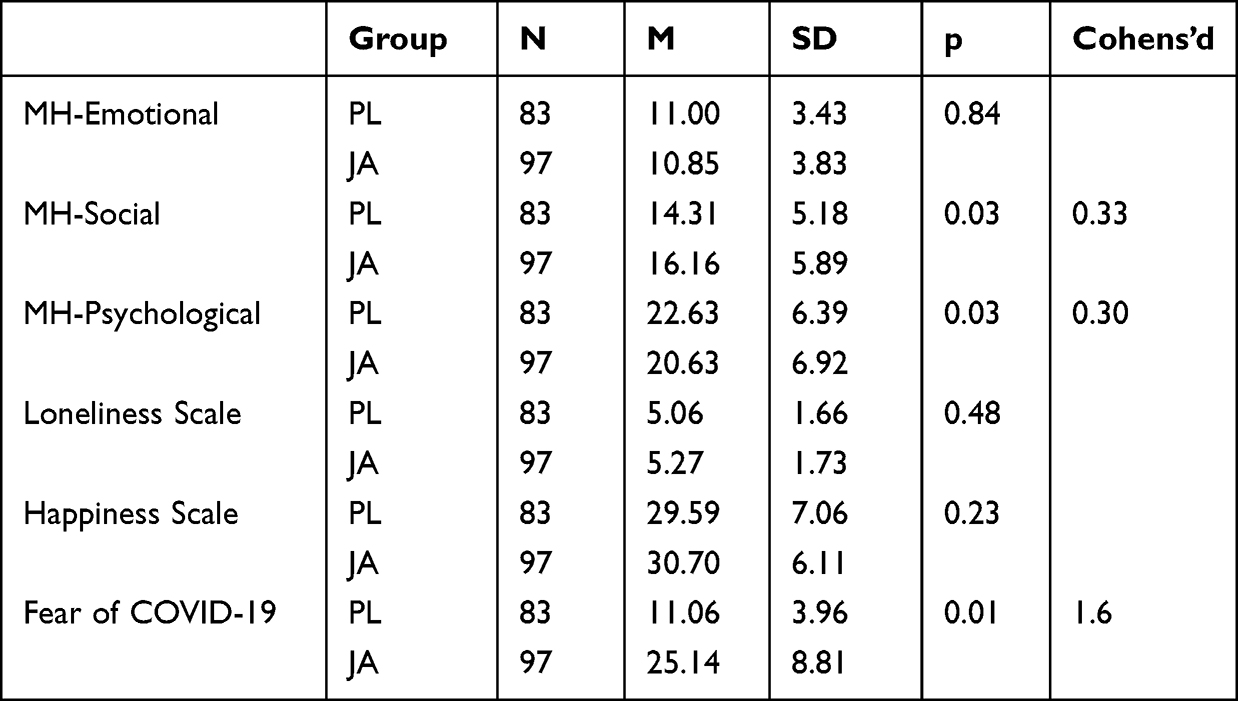 |
Table 1 Differences in the Mean Values of the Investigated Variables Between the Japanese (JA) and the Polish (PL) Samples (Student’s t-test) |
As a next step, we wanted to check whether there were gender-related differences within the study groups, of which one represented an individualistic population and the other a collectivist one. Table 2 shows the results of the analyses. In the group of Japanese participants, gender did not statistically significantly differentiate the respondents. In the group of Poles, on the other hand, the level of fear of COVID-19 was significantly higher in men (M=11.83; SD=4.10) than in women (M=9.17; SD=2.84). The effect size (rrb=0.7) of this difference measured by the rank biserial correlation was large.36
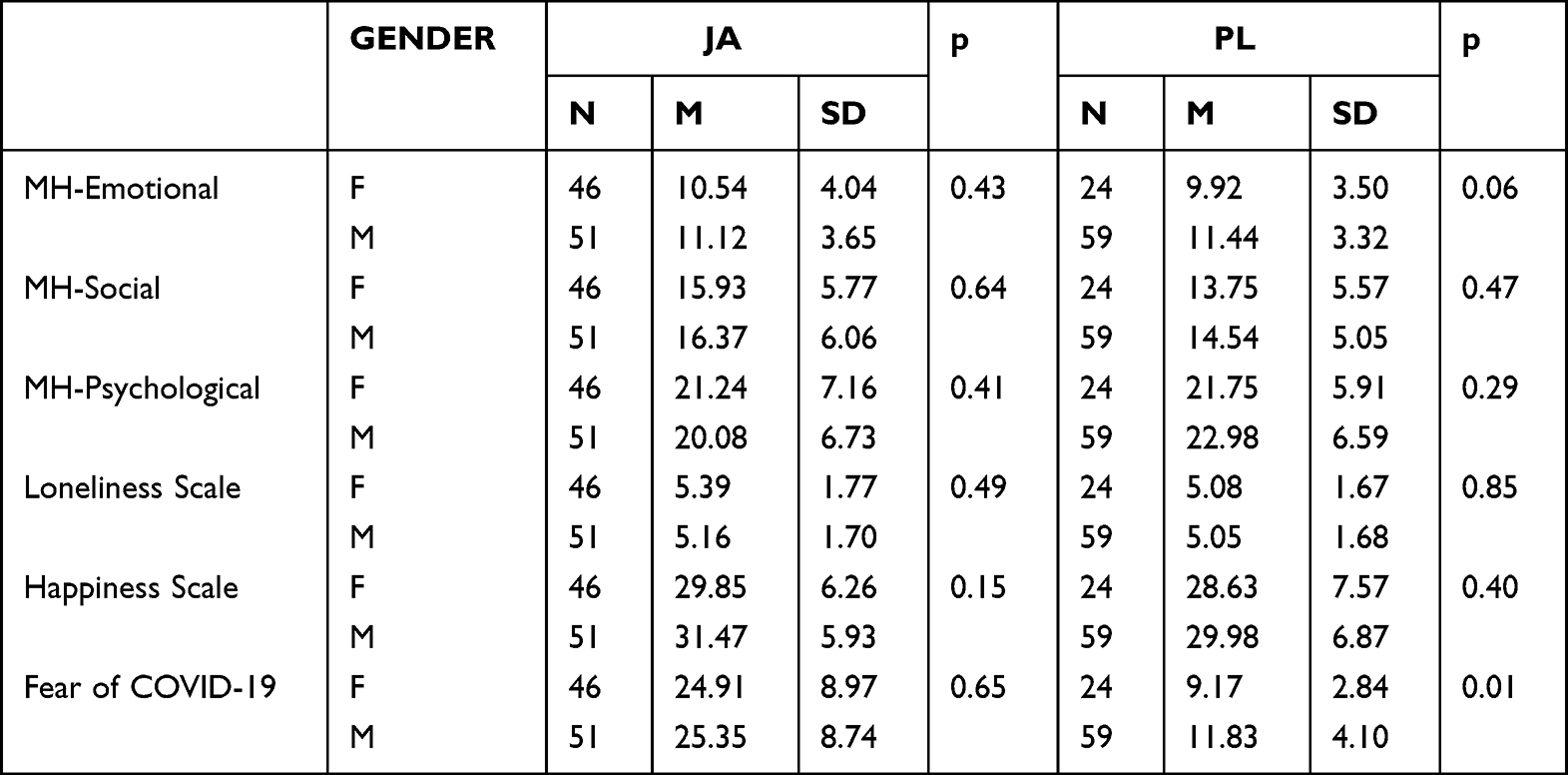 |
Table 2 Differences in the Mean Values of the Investigated Variables Between Genders in the Groups of Japanese (JA) and Polish (PL) University Students (Mann–Whitney Test) |
Correlation Analysis and Comparison by Gender in the Polish Sample
A correlation analysis was performed, controlling for gender, in the group of Poles, who represented an individualistic culture. In the group of Polish women, statistically significant, strong correlations were observed between the three dimensions of Mental Health and the Interdependent Happiness scale. The correlation results for the group of Polish women are shown in Table 3.
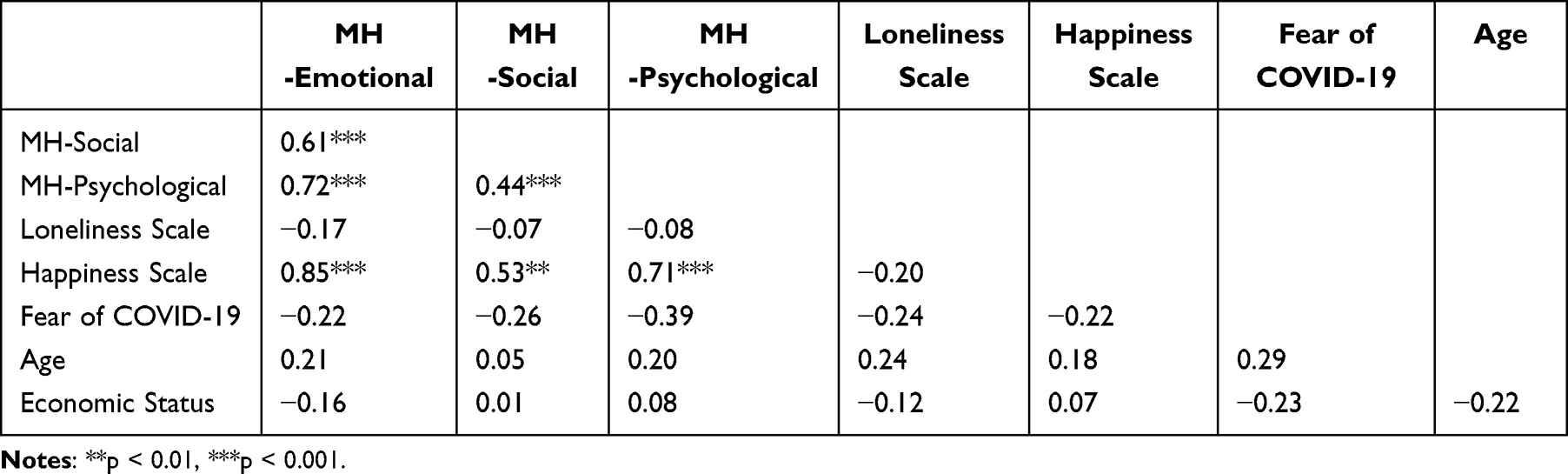 |
Table 3 Correlations Between the Test Variables in the Group of Poles: Women |
In the group of Polish men, more correlations between the variables were observed. There was a moderate to weak negative correlation between loneliness and all three dimensions of Mental Health. Interdependent happiness was also positively, moderately correlated with the three dimensions of MH. Loneliness correlated negatively with interdependent happiness. Weak relationships were also observed for economic status with the Social dimension of Mental Health and fear of COVID-19. In addition, the age of the Polish men correlated negatively with loneliness and positively with interdependent happiness. Lastly, economic status correlated with fear of COVID-19. The results of the analyses are shown in Table 4.
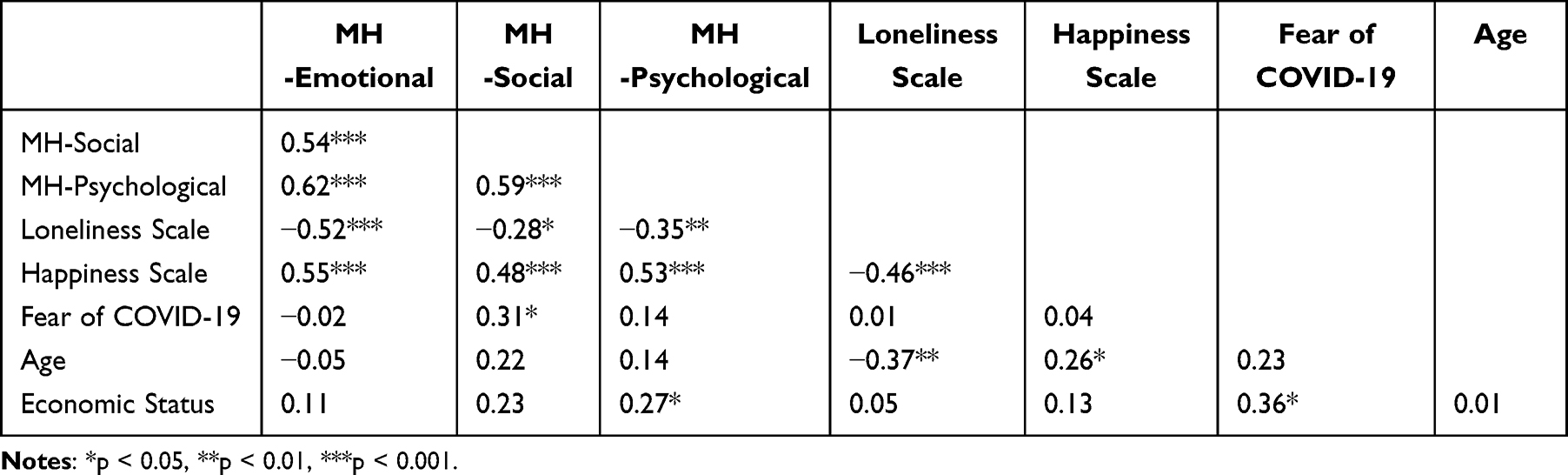 |
Table 4 Correlations of the Test Variables in the Group of Poles: Men |
The significance of the observed differences in the group of Poles was analyzed using Fisher’s Z-test. Among the statistically significant correlations, the association between the Emotional dimension of MH and interdependent happiness was much stronger in the group of women than in the group of men. The results of the comparison are shown in Table 5. In addition, we observed differences between groups in the significance of correlations, with some correlations being statistically significant in one group, but not in the other.
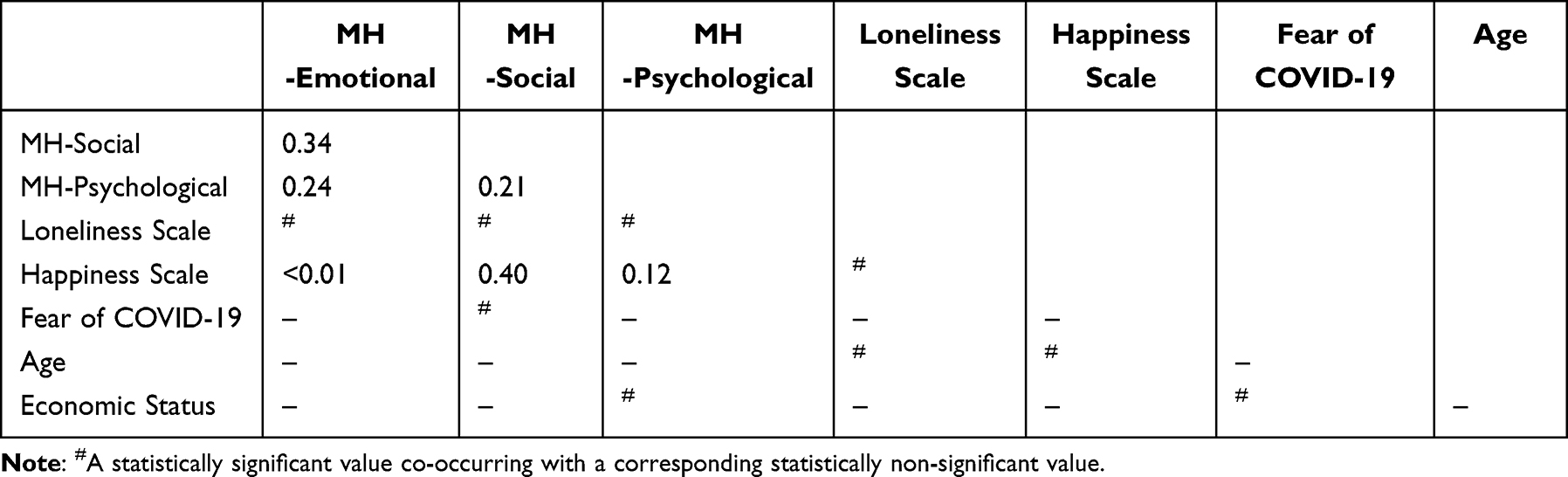 |
Table 5 The p-value of Fisher’s Z-Test for Comparing Differences Between Gender Groups in the Polish Sample |
Correlation Analysis and Comparison by Gender in the Japanese Sample
A correlation analysis was carried out, controlling for gender, in the group of Japanese participants, who represented a collectivist culture. In the group of women, statistically significant moderate correlations were observed between the three dimensions of Mental Health and the Interdependent Happiness scale. A weak negative correlation between interdependent happiness and the perceived level of loneliness was also found. The economic status of the Japanese respondents was weakly negatively correlated with their fear of COVID-19. The correlations for the group of Japanese women are shown in Table 6.
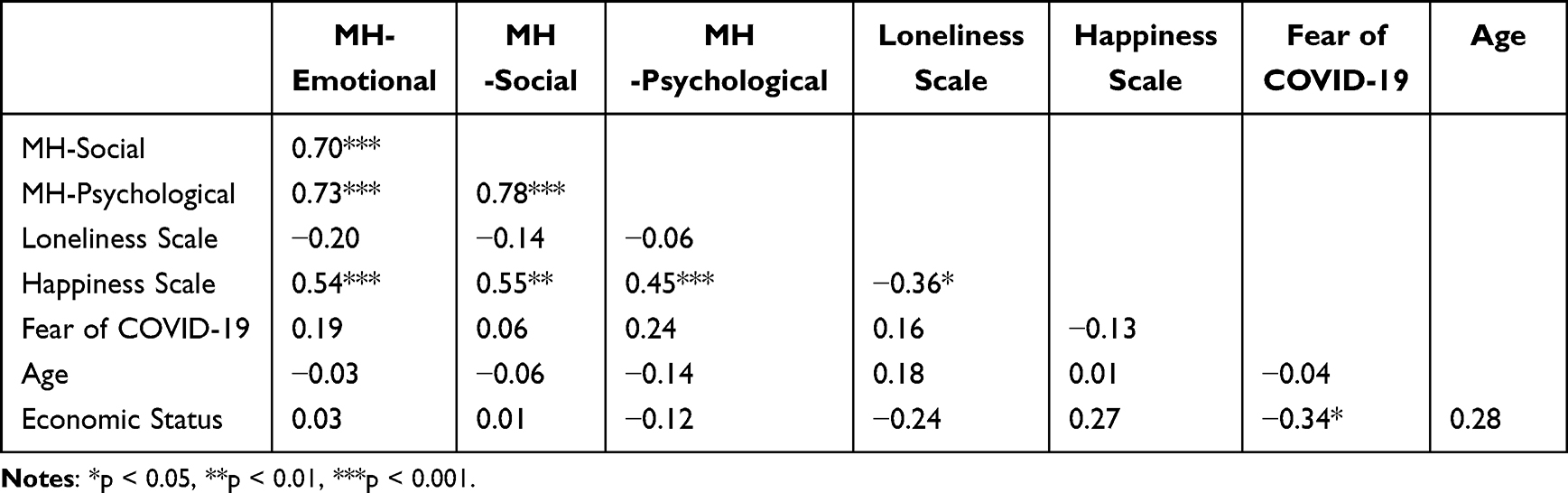 |
Table 6 Correlations Between the Test Variables in the Group of Japanese Participants: Women |
In the group of Japanese men, there were negative weak correlations between loneliness and the Psychological and Emotional dimensions of Mental Health. The level of interdependent happiness was positively, moderately associated with the three dimensions of MH and negatively with loneliness. A weak negative relationship between fear of COVID-19 and interdependent happiness was also observed. In addition, the age of the Japanese men correlated negatively with their sense of loneliness and positively with their sense of interdependent happiness. Economic status was weakly to moderately associated with most analyzed variables. The results of the analyses are shown in Table 7.
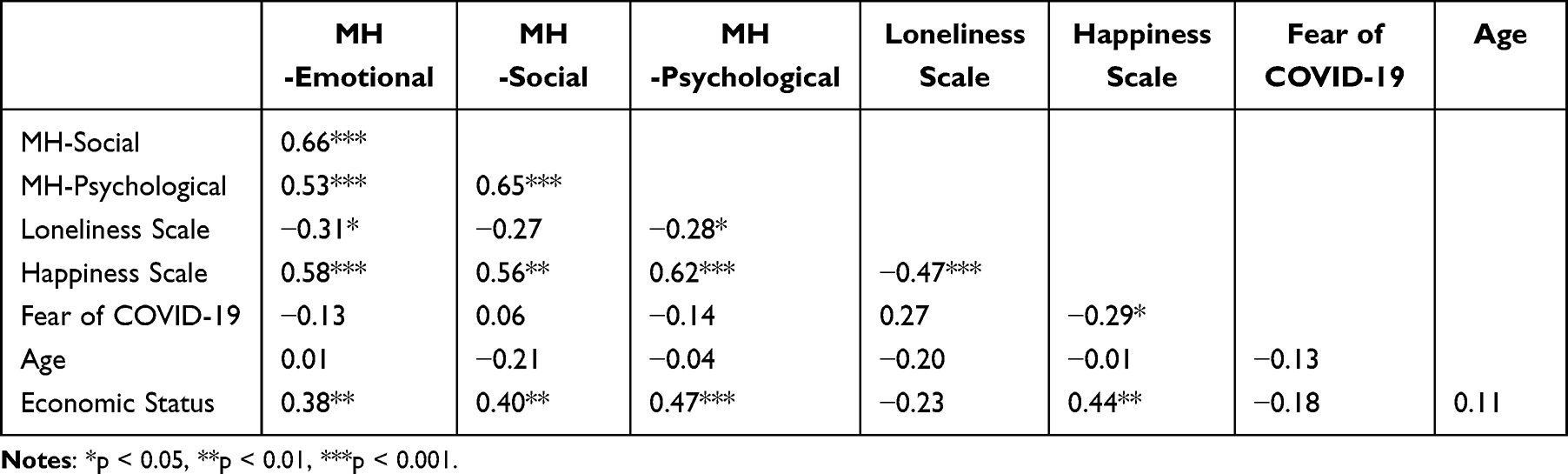 |
Table 7 Correlations Between the Test Variables in the Group of Japanese Participants: Men |
In order to determine the significance of the observed differences in the Japanese sample, we performed an analysis using Fisher’s Z-test. Among the statistically significant correlations, the association between the Emotional and Psychological dimensions of MH was much stronger in the group of Japanese women than in Japanese men. The results of the comparison are shown in Table 8. In addition, we observed differences between groups in the significance of correlations, with some correlations being statistically significant in one group, but not in the other.
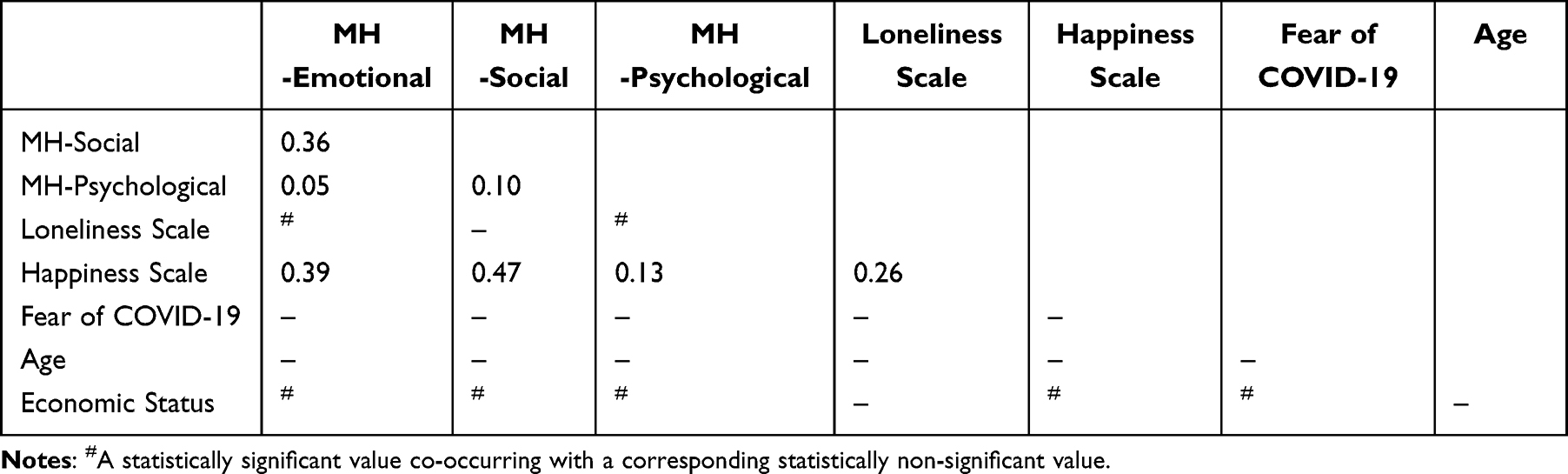 |
Table 8 The p-value for Fisher’s Z-Test Comparing Gender Groups in the Japanese Sample |
Comparison of the Polish and Japanese Participants’ Scores
In order to check whether the variables related to mental well-being differed, after the period of forced isolation caused by the COVID-19 pandemic, between populations representing different cultures, the survey data were compared using Fisher’s Z-test. Separate comparisons were made for men and women. In the group of women, the only differences between the Polish and Japanese participants concerned the relationship of the Psychological and Emotional dimensions of Mental Health with interdependent happiness. In the group of Polish women, this relationship was significantly stronger than in the group of Japanese women. Also, the relationship of economic status with loneliness and fear of COVID-19 was different in these culturally distinct groups. In the group of Polish women, economic status was not statistically significantly related to the variables in question. In the group of Japanese women, it was negatively correlated with loneliness and fear of COVID-19. The results of this analysis are shown in Table 9.
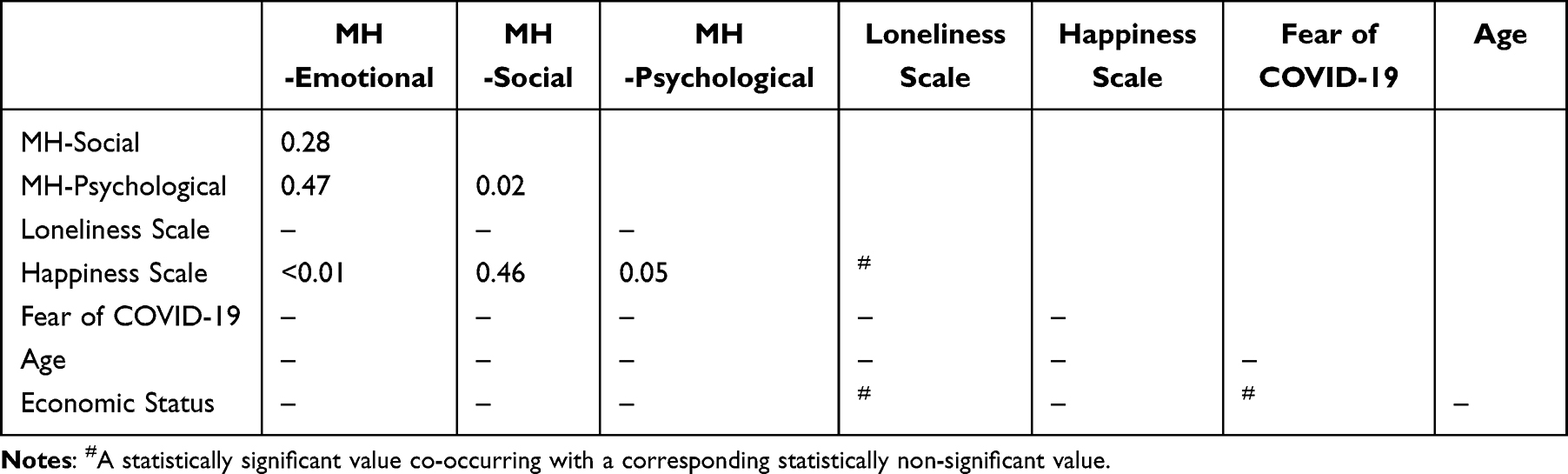 |
Table 9 The p-value for Fisher’s Z-Test Comparing Differences Between Japanese and Polish Women |
The groups of men from the two distinct cultures did not differ statistically significantly in the variables analyzed with Fisher’s Z-test. However, numerous differences were observed between these groups in the statistical significance (vs non-significance) of relationships. The main differences of this type concerned the relationship between economic status and the remaining test variables. In the Japanese group, economic status correlated moderately positively with the Emotional and Social aspects of Mental Health and with interdependent happiness but negatively with loneliness. In the group of Poles, no such correlations were observed. The results of this analysis are shown in Table 10.
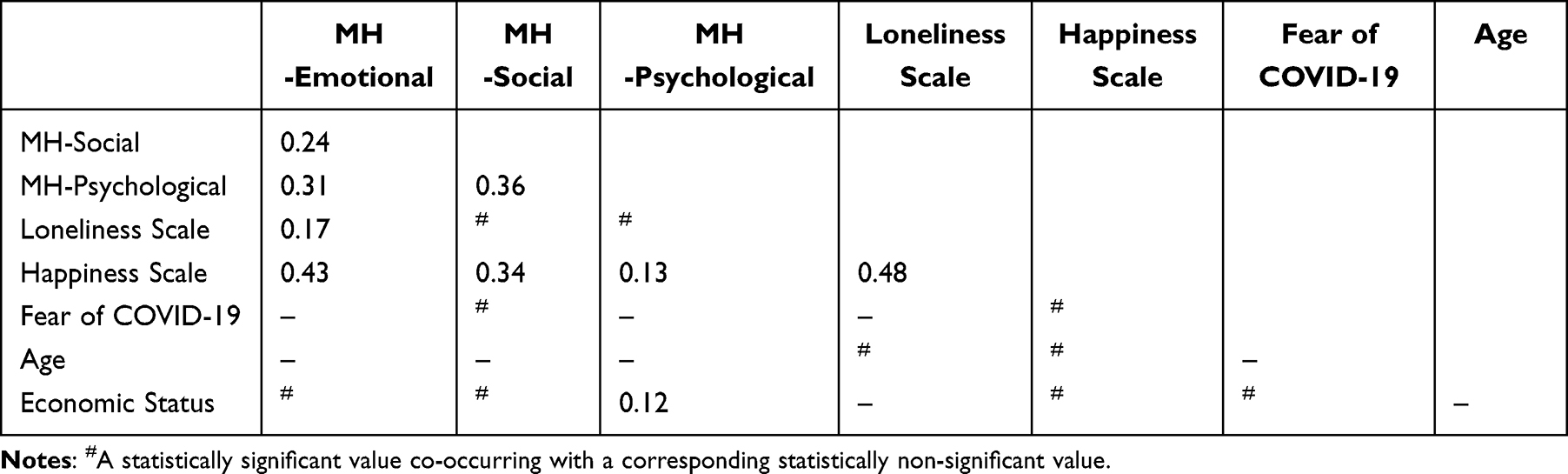 |
Table 10 The p-value for Fisher’s Z-Test Comparing Differences Between Japanese and Polish Men |
Discussion
The COVID-19 pandemic hit some countries harder than others. Research suggests that cultural differences between countries may be as important to understanding the phenomenon as demographic or economic factors.37 One of the methods of capturing cultural differences are Hofstede’s Cultural Dimensions. One dimension that describes different cultures is Individualism vs Collectivism. It describes the degree of interdependence a society maintains among its members and refers to whether people’s self-image is defined in terms of “me” or “us”. In individualistic societies, people take care of themselves and their immediate family. In collectivist societies, individuals function in groups which take care of them in exchange for loyalty.38 Poland’s score in this dimension demonstrates that Polish society is an individualistic one, which means that individuals are expected to care only for themselves and their immediate families.2,39 By contrast, Japanese society displays many features of a collectivist society, in which people prioritize harmony with the group over expressing individual opinions or have a strong sense of shame about “losing face”. However, Japan is not as collectivist as most of its Asian neighbors. The most popular explanation for this is that Japanese society does not have an extended family system that forms the basis of more collectivist societies such as Chinese and Korean ones. In a strongly collectivist culture, people are loyal to their inner group of descent, such as the extended family and the local community. The Japanese are viewed as collectivist by Western standards and as individualist by Asian standards.40 Another dimension that distinguishes Polish and Japanese societies even more is the “long term orientation”. This dimension describes how society maintains ties with the past and how it deals with the challenges of the present and future. The Japanese see their lives as very short moments in the long history of mankind and are one of the most long-term oriented nations. This approach is particularly visible in Japanese corporations, which are managed with a focus on their long-term functioning. The management philosophy is that companies are not there to make money for their stockholders every quarter of the year, but to serve the stockholders and society at large for many generations to come. Poland’s low score in this dimension means that Polish society has a high respect for tradition and a relatively low inclination to save for the future, focusing instead on achieving quick results.41
The reactions of different societies to the threat caused by COVID-19 varied and affected the mental well-being of citizens in different ways.42 Of no small meaning were cultural differences, which had a significant impact on the degree to which citizens complied with the requirements set by health authorities.11,43,44 Japan, due to its geographical proximity to the epicenter of the epidemic in Wuhan, was in a different situation than Poland. Despite this, the COVID-19 regulations instituted in Japan imposed relatively lax restrictions on social activity. Unlike many parts of Europe, including Poland,45 Japan did not introduce a full lockdown.
The curbs imposed on direct social contact, despite the great variety of possibilities of communicating online, affected the well-being of citizens.24,46 The study of Turkish adolescents demonstrated that fear of COVID-19 is a significant individual difference factor that is associated with smartphone addiction and resilience.47 From an individual’s perspective, factors such as socio-economic status or the environment in which one lives are associated with experiencing loneliness.38 Loneliness negatively affects almost every aspect of human health, including physical and mental well-being and proper cognitive functioning. The study of examine the mediating role of self-esteem in university students in association with loneliness and psychological and subjective well-being. Results of the study showed that loneliness was significantly and negatively associated with self-esteem, psychological well-being, and subjective well-being. Self-esteem was significantly and positively related to psychological well-being and subjective well-being. “Mediation analysis revealed that loneliness was a significant and negative predictor of self-esteem, psychological and subjective well-being. Self–esteem partially mediated the association between loneliness and well-being outcomes; and it significantly and positively predicted psychological wellbeing and subjective wellbeing”.48 Some studies suggest that this effect is moderated by cultural individualism.49,50 The results of our study showed no cultural differences in the level of loneliness. Of course, it should be noted that our sample was quite specific in that it consisted of university students with an average age of less than 30 years. Research shows that the level of loneliness increases with age. It is possible that the effect of intercultural differences on loneliness was not observed in the surveyed group of university students because all of the participants were of a similar young age.51,52 Clear differences were observed in the relationship between loneliness and Mental Health between genders. We found that loneliness was statistically significantly correlated with the three dimensions of Mental Health, but only in the group of men. This relationship was similar in both populations. Our observation seems all the more interesting from the perspective of the relationship between loneliness and depression, which may manifest itself differently depending on gender.23,53 The largest cross-cultural difference in the studied variables concerned fear of COVID-19. The respondents’ gender did not correlate with the level of perceived fear. On the other hand, the level of fear in the group of women, regardless of the culture they came from, was not associated with any of the analyzed variables. In the Japanese sample, it was negatively associated with interdependent happiness, and in the Polish group – with the Social dimension of Mental Health. These results can be explained in terms of differences linked with the specific character of the cultures studied, especially differences in the Individualism–Collectivism. Despite the fact that the survey was conducted after the pandemic, the results clearly show that the Japanese participants had a higher fear of COVID-19. This result may be due to the geographical location of Japan and its proximity to China, where the pandemic has not yet been fully suppressed. Other variables that differentiated the two nationalities, though to a lesser extent, were the Social dimension of Mental Health, with higher scores in the Japanese sample, and the Psychological dimension of Mental Health, which higher scores in the Polish sample. This finding can be interpreted from the perspective of the specific character of collectivism, in which well-being is shaped, among others, in social interactions.54,55
Since the 1990s, issues of social disparities and their impact on mental health have been receiving more and more attention. Research on socioeconomic status shows that this variable is positively associated with well-being, including mental health.44,45 Some authors warned the scientific and clinical community about this risk by pointing out that especially psychiatric, psychological, and social factors could interact with each other to create a vicious cycle. The increased suicide risk affected people more during the pandemic following phases. The reasons for this phenomenon may be a persistent state of insecurity regarding the economic crisis, financial debt, home loss, and poverty.56 In our study, the relationship between subjectively assessed economic status and the psychological well-being variables was strongly dependent on the respondents’ culture and gender. In the group of men, economic status was positively associated with Psychological Mental Health but also with fear of COVID-19. No such relationship was observed in the group of Polish women. In the Japanese sample, similar, but much stronger correlations were found. Economic status was positively related to the three dimensions of Mental Health and the Interdependent Happiness Scale. Negative associations were found with loneliness and fear of COVID-19. It is worth noting that in the Japanese sample, higher economic status was associated with lower fear, while in the Polish sample an opposite relationship was observed (the higher the economic status, the higher the fear). An explanation can be looked for in the previously mentioned cultural differences regarding long-term orientation. Japanese society, despite the higher fear of COVID-19, is focused on long-term functioning without falling into excessive fatalism.41 The decline in income due to the pandemic is not a large problem from a long-term In the Polish economy, which has relatively young companies, established after the transformation of the political system in 1989, the fear of losing one’s possessions, additionally stimulated by quite strong negative thinking, may manifest itself in a higher level of fear of COVID-19 and its various effects.2
Research shows that loneliness among students of all education levels has increased since the start of the pandemic.9,57 By contrast, seniors were characterised by greater resilience to the mental disorders associated with living in the pandemic, which was linked to their use of better emotion regulation strategies and lower stress vulnerability, as well as more frequent experiences of being alone and having to cope with health problems.58,59 Young adults, who need social contact with peers for their well-being, did not endure situations of social isolation as well as older adults. Older age and more social contacts were associated with less loneliness.13 When analyzing the loneliness of people during the COVID-19 pandemic, it should be emphasised that loneliness as such is a normal state. It is experienced by many people at different stages of life and cannot be immediately perceived as threatening to well-being or mental health.25
The research results presented above have a practical aspect, pointing to the need to provide support for university students and to prepare programs to promote the creation of support groups. Facilitating access to social networks and creating teams of competent specialists to provide professional support can be one way of counteracting loneliness and social isolation, which particularly affects people who live on their own.
Limitations
The main limitation of the present study is the size of the investigated groups of university students in Poland and Japan and the different gender distribution in the study groups. The failure to control for variables such as the students’ field of study or students’ background may also be viewed as a limitation. Therefore, the results should be interpreted with caution and only in relation to the study participants who experienced social isolation resulting from COVID-19. The present investigation has limitation. First, our Japan students samples were limited to participate online. Second, the sample used in in this investigation covered the time of young adulthood and early midlife. Second, the sample used in this study spanned early adulthood and early middle age. A more heterogeneous sample may help explain individual differences between developmental periods. Third, the samples included in the present study is admittedly not large and represents only small part population of polish and Japanese students. Therefore, this study is not fully reproducible as the time since the end of the covid-19 pandemic is increasing. Finally, in our studies, only self-report measures were used, which may be susceptible to effects of response sets and social desirability.
Conclusion
The present data characterizing university students from the distinct cultures of Japan and Poland indicate that societies have become accustomed to the effects of the pandemic. Regardless of the level of fear of this threat in the two cultures, the examined mental resources are positively associated with well-being and the return to normal functioning after the pandemic. This confirms the vital role of mental resources in returning to stable functioning after a crisis or a period of struggle with traumas and difficulties. It is particularly important to note that the power of mental resources, although it may vary among individuals, is independent of culture. Future research should examine other factors that may influence the happiness and mental health of Polish and Japanese students in the years following the end of the covid-19 pandemic.
Ethic
The study was approved by the Bioethics Committee of Institute of Psychology, Cardinal Stefan Wyszynski University in Warsaw, evidence #: 22/2021. Participation in the study was voluntary. All respondents were informed that they could discontinue their participation at any time without any consequences. The study procedure was conducted in accordance with the Declaration of Helsinki. All participants received research information, fully understood the study purpose, and gave signed informed consent to participate in the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Public health and social measures in response to COVID-19; 2023. Available from: https://phsm.euro.who.int.
2. Okruszek Ł, Aniszewska-Stańczuk A, Piejka A, Wiśniewska M, Żurek K. Safe but lonely? Loneliness, anxiety, and depression symptoms and COVID-19. Front Psychol. 2020;11. doi: 10.3389/fpsyg.2020.579181.
3. Costanza A, Sarasin FP, Khan RA. Prevention of Suicide at Emergency Room: from the Interpersonal Theory of Suicide to the Connectedness [Prévenir Le Suicide Aux Urgences: de La «Théorie Interpersonnelle Du Suicide]. Revue medicale suisse. 2018;14:335–338.
4. Costanza A, Macheret L, Folliet A, et al. COVID-19 related fears of patients admitted to a psychiatric emergency department during and post-lockdown in Switzerland: preliminary findings to look ahead for tailored preventive mental health strategies. Medicina. 2021;57(12):1360. doi:10.3390/medicina57121360
5. Ambrosetti J, Macheret L, Folliet A, et al. Psychiatric emergency admissions during and after COVID-19 lockdown: short-term impact and long-term implications on mental health. BMC Psychiatry. 2021;21(1):465. doi:10.1186/s12888-021-03469-8
6. Costanza A, Vasileios C, Ambrosetti J, et al. Demoralization in suicide: a systematic review. J Psychosom Res. 2022;157:110788. doi:10.1016/j.jpsychores.2022.110788
7. Mandryk RL, Frommel J, Armstrong A, Johnson D. How passion for playing world of Warcraft predicts in-game social capital, loneliness, and wellbeing. Front Psychol. 2020;11:11. doi:10.3389/fpsyg.2020.02165
8. Killgore WDS, Cloonan SA, Taylor EC, Dailey NS. Loneliness: a signature mental health concern in the era of COVID-19. Psychiatry Res. 2020;290:113117. doi:10.1016/j.psychres.2020.113117
9. Labrague LJ. Psychological resilience, coping behaviours and social support among health care workers during the COVID‐19 pandemic: a systematic review of quantitative studies. J Nurs Manag. 2021;29(7):1893–1905. doi:10.1111/jonm.13336
10. Babore A, Lombardi L, Viceconti ML, et al. Psychological effects of the COVID-2019 pandemic: perceived stress and coping strategies among healthcare professionals. Psychiatry Res. 2020;293:113366. doi:10.1016/J.PSYCHRES.2020.113366
11. Sinanovi O, Mufti M, Sinanovi S. COVID-19 pandemia: neuropsychiatric comorbidity and consequences. Psychiatr Danub. 2020;32(2):236–244. doi:10.24869/PSYD.2020.236
12. Gregório MJ, Santos A, Graça P. Obesity and COVID-19: present and future. Acta Med Port. 2021;34(5):329–331. doi:10.20344/amp.15921
13. Rumas R, Shamblaw AL, Jagtap S, Best MW. Predictors and consequences of loneliness during the COVID-19 pandemic. Psychiatry Res. 2021;300:113934. doi:10.1016/J.PSYCHRES.2021.113934
14. Shin DC, Johnson DM. Avowed happiness as an overall assessment of the quality of life. Soc Indic Res. 1978;5(1–4):475–492. doi:10.1007/BF00352944/METRICS
15. Ryff CD, Keyes CLM. The structure of psychological well-being revisited. J Pers Soc Psychol. 1995;69(4):719–727. doi:10.1037//0022-3514.69.4.719
16. Diener E, Diener M, Diener C. Factors predicting the subjective well-being of nations. J Pers Soc Psychol. 1995;69(5):851–864. doi:10.1037/0022-3514.69.5.851
17. Diener E. Subjective well-being. Psychol Bull. 2009;11–58. doi: 10.1007/978-90-481-2350-6_2
18. Diener E, Diener M. Cross-cultural correlates of life satisfaction and self-esteem. J Pers Soc Psychol. 1995;68(4):653–663. doi:10.1037/0022-3514.68.4.653
19. Ji LJ, Nisbett RE, Su Y. Culture, change, and prediction. Psychol Sci. 2016;12(6):450–456. doi: 10.1111/1467-9280.00384
20. Uchida Y. A holistic view of happiness: belief in the negative side of happiness is more prevalent in Japan than in the United States. Psychologia. 2010;53(4):236–245. doi:10.2117/PSYSOC.2010.236
21. Uchida Y, Ogihara Y. Personal or interpersonal construal of happiness: a cultural psychological perspective. Int J Wellbeing. 2012;2(4):354–369. doi:10.5502/ijw.v2.i4.5
22. Uchida Y, Kitayama S. Happiness and unhappiness in east and west: themes and variations. Emotion. 2009;9(4):441–456. doi:10.1037/A0015634
23. Cacioppo S, Grippo AJ, London S, Goossens L, Cacioppo JT. Loneliness: clinical import and interventions. Perspect Psychol Sci. 2015;10(2):238–249. doi:10.1177/1745691615570616
24. Coyle CE, Dugan E. Social isolation, loneliness and health among older adults. J Aging Health. 2012;24(8):1346–1363. doi:10.1177/0898264312460275
25. Ernst M, Niederer D, Werner AM, et al. Loneliness before and during the COVID-19 pandemic: a systematic review with meta-analysis. Am Psychol. 2022;77(5):660–677. doi:10.1037/amp0001005
26. King DL, Delfabbro PH, Billieux J, Potenza MN. Problematic online gaming and the COVID-19 pandemic. J Behav Addict. 2020;9(2):184–186. doi:10.1556/2006.2020.00016
27. Yıldırım M, Solmaz F. COVID-19 burnout, COVID-19 stress and resilience: initial psychometric properties of COVID-19 burnout scale. Death Stud. 2022;46(3):524–532. doi:10.1080/07481187.2020.1818885
28. Karaś D, Cieciuch J, Keyes CLM. The Polish adaptation of the Mental Health Continuum-Short Form (MHC-SF). Pers Individ Dif. 2014;69:104–109. doi:10.1016/J.PAID.2014.05.011
29. Sakano J, Langeland E, Sasahara S, Yamazaki Y, Yajima Y, Oi Y. Validity and reliability of the Japanese mental health continuum-short form (MHC-SF); 2013. Available from: https://www.webofscience.com/wos/woscc/full-record/WOS:000209359000353?SID=EUW1ED0CEAxczdUH464rlfDViEZ62.
30. Hughes ME, Waite LJ, Hawkley LC, Cacioppo JT. A short scale for measuring loneliness in large surveys: results from two population-based studies. Res Aging. 2004;26(6):655–672. doi:10.1177/0164027504268574
31. Hitokoto H, Uchida Y. Interdependent happiness: theoretical importance and measurement validity. J Happiness Stud. 2015;16(1):211–239. doi:10.1007/S10902-014-9505-8
32. Mosca O, Maricchiolo F, Krys K, Lauriola M. Two countries, one happiness? The interdependent happiness scale in Italy and Poland. TPM Test Psychom Methodol Appl Psychol. 2021;28(3):343–362. doi:10.4473/TPM28.3.5
33. Ahorsu DK, Lin CY, Imani V, Saffari M, Griffiths MD, Pakpour AH. The fear of COVID-19 scale: development and initial validation. Int J Ment Health Addict. 2022;20(3):1537. doi:10.1007/S11469-020-00270-8
34. Pisula E, Nowakowska I. Skala Lęku przed Koronawirusem FCV-19S (Ahorsu i in., 2020) – polskie tłumaczenie [Fear of COVID-19 ScaleFCV-19S (Ahorsuet al., 2020) –Polish translation]. Open Sci. 2020. doi:10.17605/OSF.IO/39JR8
35. Midorikawa H, Aiba M, Lebowitz A, et al. Confirming validity of the fear of COVID-19 scale in Japanese with a nationwide large-scale sample. PLoS One. 2021;16(2):e0246840. doi:10.1371/JOURNAL.PONE.0246840
36. Sawilowsky SS. New effect size rules of thumb. J Mod Appl Stat Methods. 2009;8(2):597–599. doi:10.22237/jmasm/1257035100
37. Struelens MJ, Irving AT, Maaravi Y, et al. “The Tragedy of the Commons”: how Individualism and Collectivism Affected the Spread of the COVID-19 Pandemic. Front Public Health. 2021;9. doi: 10.3389/fpubh.2021.627559
38. Yokoyama K, Birchley SL. Country comparisons. In: Transnational Entrepreneurship in South East Asia: Japanese Self-Initiated Expatriate Entrepreneurs. Springer; 2020. doi: 10.1007/978-981-32-9252-9_4
39. Geert H. Country comparison - Hofstede insights. Hofstede Insights. 2017.
40. Hofstede G. Compare countries - Hofstede insights. Cultures and Organizations, Software of the Mind; 1993.
41. York N, San C, Lisbon F, et al. Cultures and organizations SOFTWARE OFTHE MIND intercultural cooperation and its importance for survival |Mc IGrauu JHill. 2010.
42. Gelfand MJ, Raver JL, Nishii L, et al. Differences between tight and loose cultures: a 33-nation study. Science. 2011;332(6033):1100–1104. doi:10.1126/SCIENCE.1197754
43. Chan HF, Moon JW, Savage DA, Skali A, Torgler B, Whyte S. Can psychological traits explain mobility behavior during the COVID-19 pandemic? Soc Psychol Personal Sci. 2020. doi:10.1177/1948550620952572
44. Jiang S, Wei Q, Zhang L. Individualism vs. collectivism and the early-stage transmission of COVID-19. SSRN Electronic J. 2021. doi:10.2139/SSRN.3646229
45. Inoue H. Japanese strategy to COVID-19: how does it work? Glob Health Med. 2020;2(2):131–132. doi:10.35772/GHM.2020.01043
46. Chou KL, Ho AHY, Chi I. Living alone and depression in Chinese older adults. Aging Ment Health. 2006;10(6):583–591. doi:10.1080/13607860600641150
47. Yıldırım M, Çiçek İ. Fear of COVID-19 and smartphone addiction Among Turkish adolescents: mitigating role of resilience. Fam J. 2022;106648072211395. doi:10.1177/10664807221139510
48. Çiçek İ. Mediating role of self-esteem in the association between loneliness and psychological and subjective well-being in university students. Int J Contemp Educ Res. 2021;8(2):83–97. doi:10.33200/ijcer.817660
49. Chou KL, Liang K, Sareen J. The association between social isolation and DSM-IV mood, anxiety, and substance use disorders: wave 2 of the National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry. 2011;72(11):1468–1476. doi:10.4088/JCP.10M06019GRY
50. Beller J, Wagner A. Loneliness and health: the moderating effect of cross-cultural individualism/collectivism. J Aging Health. 2020;32(10):1516–1527. doi:10.1177/0898264320943336/ASSET/IMAGES/LARGE/10.1177_0898264320943336-FIG1.JPEG
51. Somes J. The loneliness of aging. J Emerg Nurs. 2021;47(3):469–475. doi:10.1016/j.jen.2020.12.009
52. Ong AD, Uchino BN, Wethington E. Loneliness and health in older adults: a mini-review and synthesis. Gerontology. 2016;62(4):443–449. doi:10.1159/000441651
53. Hawkley LC, Cacioppo JT. Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann Behav Med. 2010;40(2):218–227. doi:10.1007/s12160-010-9210-8
54. Rajkumar RP. COVID-19 and mental health: a review of the existing literature. Asian J Psychiatr. 2020;52:102066. doi:10.1016/j.ajp.2020.102066
55. O’Sullivan R, Burns A, Leavey G, et al. Impact of the COVID-19 pandemic on loneliness and social isolation: a multi-country study. Int J Environ Res Public Health. 2021;18(19):9982. doi:10.3390/ijerph18199982
56. Costanza A, Amerio A, Aguglia A, et al. From “The Interpersonal Theory of Suicide” to “The Interpersonal Trust”: an unexpected and effective resource to mitigate economic crisis-related suicide risk in times of Covid-19? Acta Biomed. 2021;92(S6):e2021417. doi:10.23750/abm.v92iS6.12249
57. Phillips R, Seaborne K, Goldsmith A, et al. Student loneliness through the pandemic: how, why and where? Geogr J. 2022;188(2):277–293. doi:10.1111/geoj.12438
58. Luchetti M, Lee JH, Aschwanden D, et al. The trajectory of loneliness in response to COVID-19. Am Psychol. 2020;75(7):897–908. doi:10.1037/amp0000690
59. Palgi Y, Shrira A, Ring L, et al. The loneliness pandemic: loneliness and other concomitants of depression, anxiety and their comorbidity during the COVID-19 outbreak. J Affect Disord. 2020;275:109–111. doi:10.1016/j.jad.2020.06.036
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.