Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Fatty Acid Degradation (FAD) Subtype-Informed Treatment Allocation in Unresectable Hepatocellular Carcinoma (FAD-HCC-01): Protocol for a Prospective Multicentre Proof-of-Concept Study
Received 11 March 2026
Accepted for publication 24 April 2026
Published 15 May 2026 Volume 2026:13 608436
DOI https://doi.org/10.2147/JHC.S608436
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Gerber
Yuan Cheng,1 Binghua Li,2 Decai Yu2
1Department of Medical Oncology, Jinling Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China; 2Division of Hepatobiliary and Transplantation Surgery, Department of General Surgery, Nanjing Drum Tower Hospital, The Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China
Correspondence: Decai Yu, Email [email protected]
Background: Hepatocellular carcinoma (HCC) exhibits substantial biological and metabolic heterogeneity, contributing to variable therapeutic responses in unresectable disease. Although immune checkpoint inhibitors combined with anti-angiogenic agents have improved outcomes, treatment selection remains largely empirical because validated predictive biomarkers are lacking. Recent multi-omics studies have identified fatty acid degradation (FAD)-related transcriptional signatures that classify HCC into distinct metabolic subtypes with different immune microenvironment characteristics and therapeutic vulnerabilities. Retrospective analyses suggest that F1/F2 subtypes may derive greater benefit from immune checkpoint inhibitor-based systemic therapy, whereas F3 tumours may be more responsive to transarterial chemoembolisation (TACE). However, whether FAD-based metabolic stratification can prospectively inform treatment allocation remains unknown.
Methods: FAD-HCC-01 is a prospective, multicentre, open-label proof-of-concept Phase II study designed to evaluate the feasibility and preliminary clinical activity of FAD-informed treatment allocation in patients with unresectable HCC. Eligible patients with Barcelona Clinic Liver Cancer stage B or C disease and no prior systemic therapy will undergo baseline tumour transcriptomic profiling to determine FAD subtype. Patients with F1/F2 tumours will receive camrelizumab plus rivoceranib, whereas patients with F3 tumours will receive TACE combined with camrelizumab and rivoceranib. Eighty-six patients will be enrolled, with 43 in each biomarker-defined cohort. The primary endpoint is objective response rate according to RECIST version 1.1. Secondary endpoints include objective response rate by mRECIST, disease control rate, progression-free survival, overall survival, duration of response, conversion to curative treatment, and safety. Exploratory analyses will assess concordance between MRI-derived proton density fat fraction and transcriptomic FAD classification.
Conclusion: This proof-of-concept study will prospectively assess whether FAD-based metabolic subtyping can inform treatment allocation in unresectable HCC. The results may provide early evidence supporting metabolism-informed precision therapy and the design of future biomarker-guided clinical trials.
Keywords: hepatocellular carcinoma, fatty acid degradation, metabolic subtype, biomarker-informed treatment allocation, precision oncology
Introduction
Hepatocellular carcinoma (HCC) remains one of the leading causes of cancer-related mortality worldwide and represents a major global health burden.1 Despite improvements in surveillance and therapeutic strategies, a considerable proportion of patients are diagnosed at intermediate or advanced stages when curative treatments are no longer feasible. In recent years, systemic therapy for unresectable HCC has evolved rapidly, particularly with the introduction of immune checkpoint inhibitor (ICI)–based combination regimens. Treatments such as atezolizumab plus bevacizumab and camrelizumab combined with rivoceranib have significantly improved clinical outcomes and have become important first-line options for advanced disease.2,3 However, treatment responses remain heterogeneous, and only a subset of patients derives durable benefit from these therapies.
Current treatment algorithms for hepatocellular carcinoma, including the Barcelona Clinic Liver Cancer (BCLC) staging system, primarily guide therapeutic decision-making according to tumour burden, liver function and performance status.4 While these frameworks provide practical clinical guidance, tumour-intrinsic biological heterogeneity is not fully incorporated into treatment selection. As a consequence, patients with similar clinical characteristics may experience markedly different responses to systemic or locoregional therapies. Compared with several other malignancies in which molecular alterations directly inform therapeutic strategies, clinically validated predictive biomarkers for treatment selection remain limited in hepatocellular carcinoma.5,6
Metabolic reprogramming has emerged as a fundamental hallmark of cancer and plays a central role in tumour progression, immune regulation and therapeutic resistance.7 In hepatocellular carcinoma, metabolic alterations are particularly relevant because hepatocytes function as key regulators of systemic metabolism and metabolic dysregulation frequently accompanies chronic liver disease and hepatocarcinogenesis. Recent multi-omics studies have identified fatty acid degradation (FAD)–related transcriptional signatures that classify hepatocellular carcinoma into distinct metabolic subtypes.8 These subtypes, commonly designated as F1, F2 and F3, demonstrate differences in metabolic activity, immune microenvironment characteristics and vascular biology.8,9 Retrospective analyses suggest that these metabolic phenotypes may be associated with differential therapeutic sensitivity: tumours corresponding predominantly to F1 and F2 subtypes appear more responsive to immune checkpoint inhibitor–based systemic therapy, whereas the F3 subtype may exhibit greater sensitivity to locoregional interventions such as transarterial chemoembolisation (TACE).8,10
However, current evidence supporting FAD-based therapeutic stratification is largely derived from retrospective analyses, and prospective clinical validation remains lacking. The FAD-HCC-01 study was therefore designed as a prospective multicentre proof-of-concept trial to evaluate whether metabolic stratification based on fatty acid degradation signatures can inform treatment allocation in patients with unresectable hepatocellular carcinoma. By assigning therapy according to predefined metabolic subtypes, this study aims to generate early clinical evidence supporting metabolism-informed precision therapy and to inform the design of future biomarker-guided clinical trials in hepatocellular carcinoma. Importantly, this study is designed to explore feasibility and generate preliminary efficacy signals, rather than to establish predictive value or demonstrate treatment superiority.
Methods and Analysis
Study Design
The FAD-HCC-01 study is a prospective, multicentre, open-label proof-of-concept phase II trial designed to evaluate the feasibility and preliminary clinical activity of FAD-informed treatment allocation in patients with unresectable hepatocellular carcinoma.
Eligible patients with unresectable hepatocellular carcinoma will undergo baseline tumour transcriptomic profiling to determine FAD metabolic subtype. According to predefined biomarker stratification, patients will be allocated to treatment cohorts based on their metabolic classification. Patients with F1 or F2 tumours will receive systemic therapy consisting of camrelizumab combined with rivoceranib, whereas patients with F3 tumours will receive TACE in combination with camrelizumab and rivoceranib.
The study adopts a biomarker-stratified parallel-cohort design rather than a comparative randomised design. This approach allows the evaluation of treatment activity within biologically defined patient populations without requiring direct comparisons between metabolic subtypes. Such a design is appropriate for early translational studies in which the predictive value of a biomarker has not yet been prospectively validated.
A total of 86 patients will be enrolled across participating centres, with 43 patients included in each biomarker-defined cohort. The primary endpoint is objective response rate (ORR) according to RECIST version 1.1. Secondary endpoints include ORR by modified RECIST (mRECIST), disease control rate, progression-free survival, overall survival, duration of response, conversion to curative treatment and safety.
An exploratory component of the study will evaluate the concordance between magnetic resonance imaging–derived proton density fat fraction (PDFF) and transcriptomic FAD classification. This analysis aims to explore whether imaging-based metabolic assessment may complement transcriptomic classification in future studies (Figure 1).
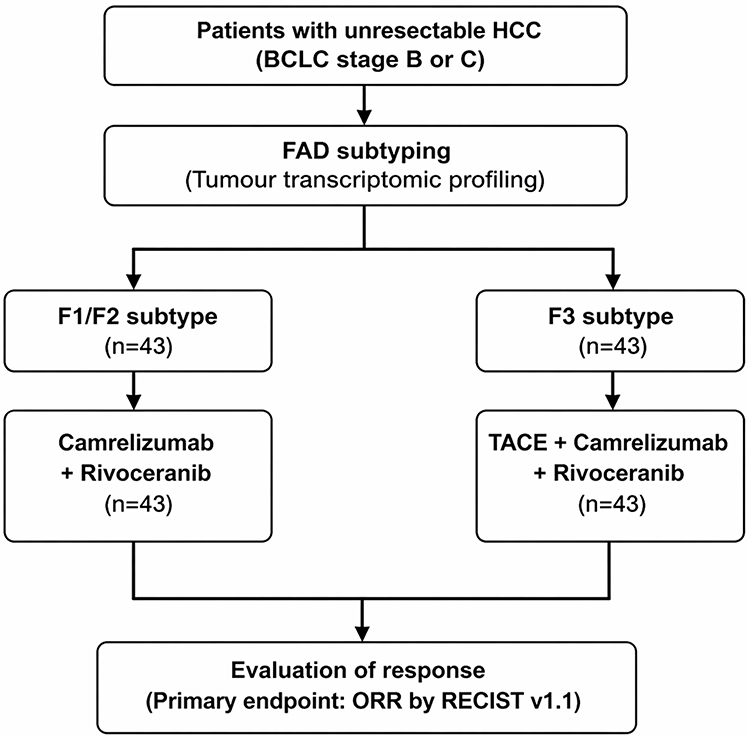 |
Figure 1 Study design of the FAD-HCC-01 trial. |
Patient Eligibility
Inclusion Criteria
Eligible patients must meet the following criteria:
- Age ≥18 years.
- Histologically or clinically confirmed hepatocellular carcinoma.
- BCLC B or C disease not amenable to curative treatment.
- At least one measurable lesion according to RECIST v1.1.
- No prior systemic therapy for HCC.
- Child–Pugh class A or B (≤7).
- Eastern Cooperative Oncology Group (ECOG) performance status 0–1.
- Adequate haematologic, hepatic and renal function.
- Availability of tumour tissue for molecular analysis or imaging-based assessment.
Patients with hepatitis B virus infection must receive antiviral therapy according to clinical guidelines.
Exclusion Criteria
Major exclusion criteria include:
- Non-HCC histology (eg, cholangiocarcinoma or mixed tumours).
- Clinically significant ascites or uncontrolled pleural effusion.
- Active autoimmune disease requiring systemic treatment.
- Active interstitial lung disease or pneumonitis.
- Recent major cardiovascular events.
- Significant bleeding risk or gastrointestinal haemorrhage.
- Uncontrolled hypertension.
- Active severe infection.
- Known HIV infection or immunodeficiency.
- Any other condition that may interfere with study participation or evaluation.
FAD Subtyping and Biomarker Assessment
Baseline tumour tissue will be obtained from either fresh biopsy or archived formalin-fixed paraffin-embedded samples RNA will be extracted and subjected to transcriptomic profiling according to standardised laboratory procedures.
FAD subtype will be determined using a predefined fatty acid degradation gene signature. Single-sample gene set enrichment analysis (ssGSEA) will be used to calculate individual FAD scores.11
ssGSEA scoring will be performed using the GSVA package (version 1.42.0) in R (version 4.2.0), with predefined gene sets and default parameters unless otherwise specified. FAD classification will be performed using a predefined gene signature and a standardized ssGSEA-based scoring approach with a uniform data processing and normalization pipeline. To minimize inter-sample variability, transcriptomic analyses will be conducted using a centralized analytical workflow, and batch effect correction methods will be applied where appropriate. Tumours will be classified as F1, F2 or F3 based on prespecified thresholds. For treatment allocation, F1 and F2 subtypes will be grouped into a single cohort, while F3 will constitute a separate cohort. This grouping was based on prior evidence suggesting that F1/F2 tumours may share relatively similar immune-related characteristics and potential sensitivity to immunotherapy-based systemic treatment. PDFF will be evaluated as an exploratory imaging biomarker to assess its potential association with transcriptomic FAD classification.12 Concordance between PDFF and transcriptomic subtype classification will be evaluated in exploratory analyses.
Treatment Procedures
Treatment allocation will be determined according to FAD subtype.
Patients with F1 or F2 tumours will receive:
- Camrelizumab 200 mg intravenously every 3 weeks.
- Rivoceranib 250 mg orally once daily.
Patients with F3 tumours will receive:
- Transarterial chemoembolisation (TACE).
- Camrelizumab 200 mg every 3 weeks.
- Rivoceranib 250 mg once daily.
TACE will be performed according to institutional standards. To enhance consistency across centres, key procedural principles, including treatment indications, embolisation endpoints, and retreatment criteria, will be guided by predefined recommendations. Repeat TACE procedures may be administered based on tumour response and liver function.
Treatment in both cohorts will continue until radiographic disease progression, unacceptable toxicity, withdrawal of consent, or investigator decision.
In the F3 cohort, systemic therapy was retained as the treatment backbone, while TACE was incorporated on the basis of prior evidence suggesting that this metabolic subtype may derive additional benefit from locoregional treatment. The treatment strategy was designed to explore whether such a locoregional-augmented combination approach could achieve activity exceeding historical benchmark outcomes.
Study Endpoints
Primary Endpoint
The primary endpoint is ORR, defined as the proportion of patients achieving complete response (CR) or partial response (PR) according to RECIST version 1.1.
ORR will be calculated separately for the F1/F2 cohort and the F3 cohort.
Secondary Endpoints
- ORR according to modified RECIST (mRECIST)
- Disease control rate (DCR)
- Progression-free survival (PFS)
- Overall survival (OS)
- Duration of response (DoR)
- Conversion rate to curative-intent therapy
- Incidence of treatment-related adverse events
Exploratory Endpoints
- Concordance between MRI-derived PDFF and transcriptomic FAD classification.
- Association of molecular biomarkers with treatment response.
- Characterisation of immune and metabolic tumour features.
Follow-Up and Assessments
Baseline evaluation includes medical history, physical examination, ECOG performance status, laboratory tests and imaging assessments.
Tumour imaging using contrast-enhanced CT or MRI will be performed every 6 weeks during the first 24 weeks and every 9 weeks thereafter until disease progression.
Tumour response will be assessed according to RECIST v1.1 and mRECIST.13,14
Safety will be monitored continuously throughout the study. Adverse events will be graded according to NCI-CTCAE version 5.0.
Statistical Analysis
The study consists of two independent single-arm phase II cohorts defined by FAD subtype.
The null hypothesis assumes an objective response rate of 25%, based on historical data from the CARES-310 study.3 The anticipated ORR under FAD-informed treatment allocation is 45%. These assumptions were used for signal detection within each biomarker-defined single-arm cohort, rather than for direct comparison between cohorts.
Using an exact binomial design with a two-sided significance level of 0.05 and 80% power, 41 evaluable patients per cohort are required. Allowing for potential dropout, 43 patients per cohort will be enrolled, resulting in a total planned sample size of 86 patients.
ORR will be reported with 95% confidence intervals using the exact binomial method. Time-to-event outcomes, including progression-free survival and overall survival, will be estimated using the Kaplan–Meier method.
Safety analyses will include all patients receiving at least one dose of study treatment.
Ethics and Trial Registration
The study will be conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines.15 The protocol has been approved by the Ethics Committee of Nanjing Drum Tower Hospital (approval number 2025–1044-02). Written informed consent will be obtained from all participants before enrolment.
The study is registered at ClinicalTrials.gov (NCT07314372).
Discussion
The FAD-HCC-01 study represents an initial prospective effort to translate metabolic classification into therapeutic decision-making in hepatocellular carcinoma. By integrating fatty acid degradation–based metabolic subtypes into treatment allocation, this proof-of-concept trial evaluates whether FAD-informed treatment allocation can be implemented in clinical practice for patients with unresectable disease. Emerging evidence suggests that tumour metabolic states may influence immune microenvironment, vascular biology and therapeutic sensitivity.7–9 The prospective evaluation of FAD-informed treatment allocation therefore provides an opportunity to generate early clinical evidence supporting metabolism-informed precision oncology in hepatocellular carcinoma. However, grouping F1 and F2 into a single cohort may obscure potential biological and therapeutic differences between these subtypes, which should be further evaluated in future studies.
An additional strength of the FAD-HCC-01 study lies in its biomarker-stratified parallel-cohort design. Rather than directly comparing treatments across heterogeneous patient populations, this design enables the evaluation of treatment activity within biologically defined metabolic subtypes. Such an approach is particularly suitable for early translational studies in which the predictive value of a biomarker has not yet been prospectively validated.16 By allocating therapy according to predefined FAD metabolic classifications, the study provides an opportunity to explore whether metabolic phenotypes may inform differential therapeutic sensitivity.8,10 If encouraging signals are observed, this strategy could support the development of subsequent biomarker-guided clinical trials designed to formally test the predictive role of metabolic stratification in hepatocellular carcinoma. Therefore, the findings from this study should be interpreted as hypothesis-generating rather than confirmatory.
Several limitations of the present study should be acknowledged. First, the non-randomized design precludes definitive conclusions regarding the predictive value of FAD metabolic subtypes or the comparative efficacy of different treatment strategies. Second, the relatively modest sample size and the proof-of-concept nature of the trial prioritize response-based endpoints rather than long-term survival outcomes. Third, the implementation of transcriptomic profiling for metabolic classification may not yet be routinely available across all clinical settings, which could limit the immediate applicability of this approach. In addition, the turnaround time for transcriptomic profiling may delay treatment initiation in certain patients, which may limit its applicability in time-sensitive clinical settings. In addition, the reproducibility and standardization of transcriptomic-based FAD classification require further prospective validation. At present, PDFF should not be considered a validated surrogate for transcriptomic metabolic classification. In the F3 cohort, the addition of TACE to systemic therapy was intended to explore whether a locoregional-augmented strategy could improve activity beyond historical outcomes observed with systemic therapy alone. Accordingly, treatment effects in this cohort should be interpreted as reflecting the activity of a combination strategy, and the contribution of individual components cannot be isolated. Furthermore, the non-randomized design may limit the generalizability of the findings to broader patient populations. Nevertheless, the prospective evaluation of FAD-informed treatment allocation in a multicenter setting may provide important preliminary insights and inform the design of future biomarker-driven studies in hepatocellular carcinoma. Importantly, the present study is designed to explore feasibility and generate preliminary signals rather than to establish the predictive value of FAD subtypes or demonstrate treatment superiority.
If metabolism-informed treatment allocation demonstrates feasibility and encouraging clinical activity in this study, it may provide the basis for subsequent biomarker-driven clinical trials designed to prospectively validate the predictive role of metabolic stratification in hepatocellular carcinoma.17 More broadly, metabolism-informed precision oncology may represent a promising framework for moving beyond conventional stage-based treatment algorithms. The FAD-HCC-01 study therefore represents an important early step toward translating metabolic classification into clinically applicable strategies for hepatocellular carcinoma.
In addition to metabolic subtypes, a range of emerging biomarkers, including molecular, transcriptomic, and immune-related markers, have been investigated for their potential roles in prognostic stratification and therapeutic decision-making in hepatocellular carcinoma.18–21 These studies highlight the growing complexity of biomarker-driven research in HCC. Integrating these biomarkers with metabolic phenotyping may further refine patient selection and therapeutic decision-making in future studies.
Funding
This study was supported by grants from the National Natural Science Foundation of China (No. U25A20104) and the Fundings for Clinical Trials from the Affiliated Drum Tower Hospital, Medical School of Nanjing University (2025-LCYJ-ZD-02).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–8. doi:10.3322/caac.21834
2. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
3. Qin S, Chan SL, Gu S, et al. Camrelizumab plus rivoceranib versus sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised, open-label, international phase 3 study. Lancet. 2023;402(10408):1133–1146. doi:10.1016/S0140-6736(23)00961-3
4. Reig M, Sanduzzi-Zamparelli M, Forner A, et al. BCLC strategy for prognosis prediction and treatment recommendations: the 2026 update. J Hepatol. 2026;84(3):631–654. doi:10.1016/j.jhep.2025.10.020
5. Vogel A, Meyer T, Sapisochin G, Salem R, Saborowski A. Hepatocellular carcinoma. Lancet. 2022;400(10360):1345–1362. doi:10.1016/S0140-6736(22)01200-4
6. Lu LC, Hsu CH, Hsu C, Cheng AL. Tumor heterogeneity in hepatocellular carcinoma: facing the challenges. Liver Cancer. 2016;5(2):128–138. doi:10.1159/000367754
7. Pavlova NN, Zhu J, Thompson CB. The hallmarks of cancer metabolism: still emerging. Cell Metab. 2022;34(3):355–377. doi:10.1016/j.cmet.2022.01.007
8. Li B, Li Y, Zhou H, et al. Multiomics identifies metabolic subtypes based on fatty acid degradation allocating personalized treatment in hepatocellular carcinoma. Hepatology. 2024;79(2):289–306. doi:10.1097/HEP.0000000000000553
9. Montironi C, Castet F, Haber PK, et al. Inflamed and non-inflamed classes of HCC: a revised immunogenomic classification. Gut. 2023;72(1):129–140. doi:10.1136/gutjnl-2021-325918
10. Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7(1):6. doi:10.1038/s41572-020-00240-3
11. Hänzelmann S, Castelo R, Guinney J. GSVA: gene set variation analysis for microarray and RNA-seq data. BMC Bioinformatics. 2013;14:7. doi:10.1186/1471-2105-14-7
12. Zhang L, Mai X, Li B, et al. Fat fraction quantification by MRI predicts diagnosis and prognosis of HBV-related steatohepatitic hepatocellular carcinoma. Eur Radiol. 2025;35(6):3144–3157. doi:10.1007/s00330-024-11151-2
13. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
14. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi:10.1055/s-0030-1247132
15. World Medical Association. World medical association declaration of helsinki: ethical principles for medical research involving human participants. JAMA. 2025;333(1):71–74. doi:10.1001/jama.2024.21972
16. Tsimberidou AM, Fountzilas E, Nikanjam M, Kurzrock R. Review of precision cancer medicine: evolution of the treatment paradigm. Cancer Treat Rev. 2020;86:102019. doi:10.1016/j.ctrv.2020.102019
17. Llovet JM, Castet F, Heikenwalder M, et al. Immunotherapies for hepatocellular carcinoma. Nat Rev Clin Oncol. 2022;19(3):151–172. doi:10.1038/s41571-021-00573-2
18. Chen XM, Liang YB, Zuo JX, et al. ZG16B: a key regulator of tumor progression and immune microenvironment modulation in cancer (Review). Int J Mol Med. 2026;57(3):58. doi:10.3892/ijmm.2026.5729
19. Xu W, Liao S, Hu Y, Huang Y, Zhou J. Upregulation of miR-3130-5p enhances hepatocellular carcinoma growth by suppressing ferredoxin 1: miR-3130-5p enhances HCC growth via inhibiting FDX1. Curr Mol Pharmacol. 2024;17:e18761429358008. doi:10.2174/0118761429358008250305070518
20. Gudivada IP, Amajala KC. Integrative bioinformatics analysis for targeting hub genes in hepatocellular carcinoma treatment. Curr Genomics. 2025;26(1):48–80. doi:10.2174/0113892029308243240709073945
21. Mu R, Chang M, Feng C, et al. Analysis of the expression of PRDX6 in patients with hepatocellular carcinoma and its effect on the phenotype of hepatocellular carcinoma cells. Curr Genomics. 2024;25(1):2–11. doi:10.2174/0113892029273682240111052317
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.