Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Fat Compartment Gliding Theory – A Novel Technique for the Repositioning of Superficial Fat Compartments for Facial Rejuvenation
Authors Eid L, Mao X, Zhao B, Mao J, Qian S, Zhang Y, Zhang Y, Zhang L, Cheng L, Zhang Y, Sun X
Received 21 April 2023
Accepted for publication 3 October 2023
Published 26 October 2023 Volume 2023:16 Pages 3077—3090
DOI https://doi.org/10.2147/CCID.S415467
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Supplementary video of "Fat Compartment Gliding Theory" [ID 415467].
Views: 771
Loy Eid,* Xiyuan Mao,* Binfan Zhao, Jiayi Mao, Shutong Qian, Yuyu Zhang, Ying Zhang, Lu Zhang, Liying Cheng, Yuguang Zhang, Xiaoming Sun
Department of Plastic and Reconstructive Surgery, Shanghai Ninth People’s Hospital, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuguang Zhang; Xiaoming Sun, Department of Plastic and Reconstructive Surgery, Shanghai Ninth People’s Hospital, Shanghai, People’s Republic of China, Email [email protected]; [email protected]
Background: Facial fat compartments and their role in facial aging have gained increased recognition and are playing a significant role in facial rejuvenation. The superficial fat compartments glide inferiorly during the aging process, leading to the flattening and elongation of the face and the appearance of facial bulges, folds, and grooves.
Patients and Methods: Ultrasound imaging of the facial soft tissues was performed on nine female volunteers to demonstrate the change in superficial facial fat compartments from an upright to supine position. The net suture jowl and medial cheek fat compartment repositioning technique was operated on 165 Asian patients between September 2020 and July 2021. Volume and projection change of malar and jowl regions, as well as change in elevation of malar protrusion were measured 1, 3, and 6 months postoperatively using a three-dimensional imaging system.
Results: Ultrasound measurements confirmed the medial and middle cheek, nasolabial, and jowl fat compartments changed in thickness during positional changes with age-related differences. Postoperative three-dimensional imaging showed volume and projection increase in the malar region (2.23mL and 1.11mm) and decrease in the jowl region (− 0.18mL and − 0.52mm) by the 6-month follow-up date, and malar projection saw a superior displacement of 3.08mm.
Conclusion: The superficial fat glide inferiorly within their compartments under the force of gravity and naturally reposition themselves when the effect of gravity is reversed. The net suture technique offers a minimally invasive method for lifting the jowl fat, volumizing the mid-cheek and achieving facial rejuvenation by repositioning the superficial fat compartments.
Keywords: fat compartments, facial rejuvenation, face lift, facial aging
Introduction
The past few decades have seen a tremendous advancement in understanding the mechanism of facial aging, evolving from exclusively gravity’s effect on skin into a multifactorial, dynamic, and three-dimensional process involving changes in skin, soft tissue, and bone.1 Then, Rohrich and Pessa proposed the fat compartment theory, suggesting that facial aging does not occur in a confluent mass and is compartment specific, where deep fat is prone to atrophy, while superficial fat tends to redistribute inferiorly within its boundaries.2 This inferior displacement is thought to be the product of gravitational forces involving ligamentous laxity and pseudoptosis resulting from deep fat compartment volume loss, with no consensus as to which cause plays a greater role.3,4 The descent and separation of the fat compartments leads to the appearance of a deflated midface, V deformity at the lid-cheek junction, bulging jowl fat, and pronounced nasolabial folds, midcheek grooves, and marionette lines.5 This interestingly highlights the significance of facial fat in the aging process and its possibility to being the key to facial rejuvenation.
Traditional face lift and thread lift techniques have targeted the SMAS and/or cutaneous layers without specifically addressing facial fat.6,7 While these techniques have been effective in enhancing malar eminence and volumizing the lateral cheek, they have achieved little in correcting anterior midface deflation.8 Deeper understanding of the fat compartments has led to the advent of new techniques designed to reposition facial fat.9–13 However, lifting the fat at single points along single vectors may hinder results, as fat cannot be elevated across ligaments and often ligamentous release is required.14 While fat grafting in the deep fat compartments creates a lifting effect to a certain extent, injecting in the superficial compartments could lead to overfill and aggravate ptosis.15
A thorough understanding of the location, mobility, and behavior of the superficial fat compartments is essential for producing natural and effective repositioning.16–21 The effect of gravity on soft tissue ptosis has also been examined using photographs and three-dimensional imaging, which show that in supination, soft tissue placement and volume are reversed to their youthful state (Figure 1).22,23 However, the effect of gravity on the superficial fat alone is yet to be evaluated in a clinical setting.
 |
Figure 1 A 39-year-old female patient. (a) Patient in upright position exhibiting flat malar mound, greater lid-cheek distance (yellow line), prominent nasolabial folds, mid-cheek grooves, and jowl fat; (b) Patient in supine position showing a fuller malar mound, shortened lid-cheek distance, and improvement in the mid-cheek grooves and nasolabial folds. The distance from the pupil to the most projected point of the mid-face is shorter (red lines), indicating elevation and augmentation of malar mound. |
In our study, we first verified the gliding characteristic of the superficial fat compartments under the effect of gravity, as well as the influence of age on fat mobility by measuring the change in fat thickness in the upright and supine positions using ultrasound imaging. Then, based on this theory, we introduced our novel net-shaped suturing technique to reposition the superficial jowl and mid-cheek fat compartments and restore mid-facial volume to present a more youthful appearance. Three-dimensional photography was used for objective evaluation of surgical results.
Patients and Methods
Volunteer Population for Ultrasound Imaging
To showcase the gliding displacement of the superficial facial fat compartments, facial fat thickness was measured using B-mode ultrasound in the upright and supine positions. The study included nine female volunteers (18 hemifaces) categorized into two age groups: Group A (<35 years, n=5, mean age 26.4 years) and Group B (≥35 years, n=4, mean age 43.8 years). All subjects had a normal body mass index (BMI), and volunteers with a history of craniofacial deformities, facial surgery, and hormonal therapy were excluded.
Fat Compartment Changes by Ultrasound Imaging
The volunteers were first positioned sitting upright, and seven facial points representing the superficial medial and middle cheek, nasolabial, and jowl fat compartments were identified bilaterally in relation to fixed and bony landmarks, and thin metallic decals were glued onto the chosen points as markers for better precision (Figure 2).
 |
Figure 2 Metal decals on measurement points: A. Medial cheek (interior) B. Medial cheek (exterior) C. Nasolabial (superior) D. Nasolabial (inferior) E. Middle cheek (superior) F. Middle cheek (inferior) G. Jowl. |
To measure facial subcutaneous fat, ultrasound imaging (GE Logiq e) was chosen due its reliability, accuracy, non-invasiveness, and postural flexibility.24,25 Measurements were performed using a 15-MHz linear transducer applied to the predesignated points. To limit compression of the underlying soft tissues, a thick layer of ultrasound gel was applied to the skin, avoiding probe to skin contact. All examinations were conducted by one investigator for consistency, and the thickness of the superficial fat at each site was measured three times to reduce error. The volunteers were then positioned in a supine position facing straight upwards, and after re-identifying the pre-determined points, fat thickness was again measured.
Patient Population for Surgery
Between September 2020 and July 2021, 165 patients exhibiting loss of midface volume, flat or ptotic malar region, prominent jowl fat, and/or prominent nasolabial folds, midcheek groove, and marionette lines underwent our fat repositioning procedure. Patients included 159 women and 6 men, aged between 24 and 66 years, with a mean age of 42.3 years. We asked patients to come in for surgical evaluations at 1, 3, and 6 months post-operatively, and only those who completed all three visits were included in the statistical analysis (Table 1). Written informed consent was obtained from each patient, and all surgeries were performed by one single senior surgeon (ZYG). Institutional review board approval was obtained from Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine.
 |
Table 1 Patient Demographics |
Three-Dimensional Imaging Analysis
For objective assessment of post-surgical changes in the mid-cheek and jowl areas, three-dimensional photographs were recorded prior to surgery and during the 1, 3, and 6-month follow-ups. Image acquisition was completed under same conditions (lighting, distance, position, neutral facial expression) using a structured light scanner (CASZM MVS-600; Shenzhen Zhongke Zhimei Technology Co., People’s Republic of China) and analyzed using the corresponding virtual simulation software.26 For comparison, the post-surgical 3D image at each follow-up was superimposed onto the baseline pre-operative one after identifying fixed surface references such as the nasal tip, inner canthus, brow, and forehead.
Volume of Mid-Cheek and Jowl
Net volumetric changes in the mid-cheek and jowl areas were calculated and measured in milliliters. To standardize measured regions, the perimeter of the malar zone is defined as the inferior orbital rim, nasolabial fold, horizontal line connecting the cheilon to the subaurale, and vertical extension from the lateral orbital rim. The jowl zone falls within the cheilon-subaurale line superiorly, lateral orbital rim extension laterally, vertical line from cheilon to jawline medially, and the jawline inferiorly (Figure 3A).
 |
Figure 3 (A) Color map of chosen areas for volumetric measurement of the mid-cheek and jowl regions. Yellow and Orange represent relative volume gain, blue represents relative volume loss, green represents no change. (B) Comparison of height of malar prominence before and after surgery. Green dotted line represents level of pre-operative malar prominence; red dotted line represents level of post-operative malar prominence; white arrow represents height difference. |
Projection of Mid-Cheek and Jowl
Malar and jowl projection changes were recorded in millimeters at chosen fixed points on the frontal overlapped images. The malar point was selected at the intersection of the pupil and alar crease, while that of the jowl at the midpoint between the cheilon and jawline at the level of the lateral limbus.
Height of Malar Prominence
The most prominent point of the midcheek in the lateral view was pinpointed on both the pre- and post-operative images, followed by calculation of vertical height difference between the two positions (Figure 3B).
Surgical Procedure
Jowl Fat Compartment Repositioning
The lowest and most prominent point of the descended jowl fat is marked in an upright position. Then, in the supine position, a specially designed adhesive is placed onto the surgical area for reference (Figure 4).
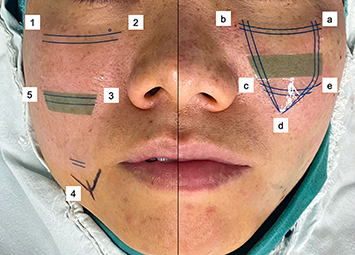 |
Figure 4 Patient’s right hemiface shows the reference adhesive for jowl fat compartment repositioning. The superior border of the adhesive sits at the level of the inferior orbital rim, the medial border at the level of the medial limbus and a distance of 5mm from the nasolabial fold, and the inferior end at the lowest point of the jowl (marked with methylene blue dye). Points 1 to 5 refer to entry and exit points of the needle in sequential order. Patient’s left hemiface shows reference adhesive for medial cheek fat compartment repositioning. The superior border of the adhesive sits at the level of the inferior orbital rim and the medial border at the level of the medial limbus and 5mm from the nasolabial fold. Points a to e refer to entry and exit points of the needle in sequential order. |
The principle of the adhesive is as follows: The midfacial deep fat compartments are located medial to the vertical line of ligaments (Figure 5), and upon their deflation, the superficial compartments found on this side of the line lose their support and redistribute inferiorly.27,28 On the other hand, descent of the superficial fat compartments in the mid and lower face lateral to the line is not as obvious due to the absence of deep compartments in this area.29 For this reason, the lateral edge of our reference adhesive is designed to coincide with the line of ligaments, and the operated area is limited to the medial mobile portion of the face.
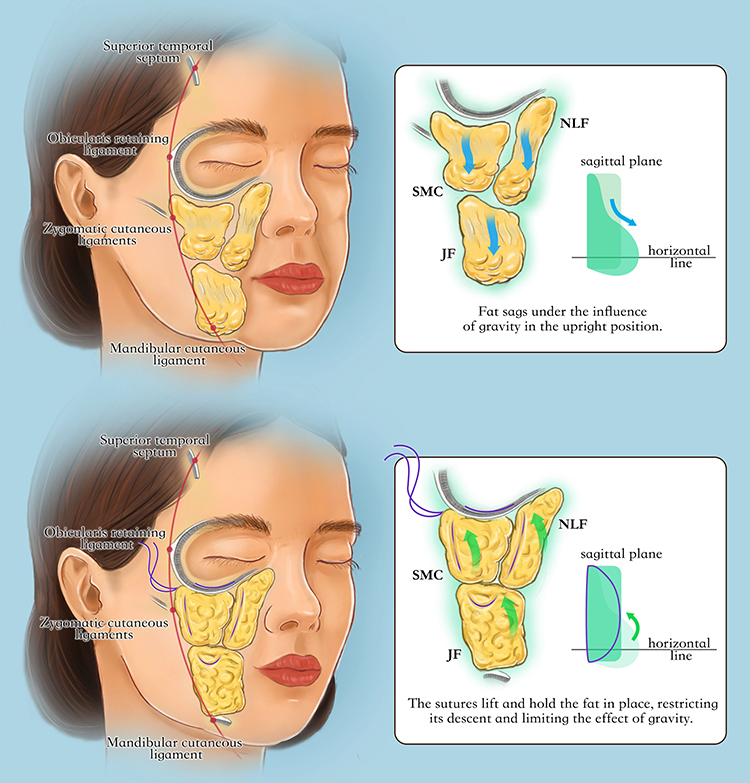 |
Figure 5 Illustration of the principle behind our fat repositioning technique. The nasolabial, medial cheek, and jowl fat compartments are located medial to the line of ligaments. (Top) With age and under the influence of gravity, the fat in each compartment glides inferiorly to take a water droplet form in the sagittal plane, and the compartments are separated, which manifests in bulging of the jowl and nasolabial areas and the appearance of facial lines and grooves. (Bottom) After fat compartment repositioning, the fat compartments are reconnected and restored into their original state, recovering a semi-spherical shape in the sagittal plane. NLF: nasolabial fat compartment; SMC: superficial medial cheek fat compartment; JF: jowl fat compartment. |
Around 20mL of 1% lidocaine with epinephrine (1:100,000) is injected at the infraorbital foramen and subcutaneously along the borders of the adhesive. A graduated hollow double-ended curved needle is used in this technique. The needle end of a 2-0 polyester non-absorbable suture is anchored into one end of the hollow needle.
After determining the entry point at the upper lateral end of the adhesive at the level of the orbital retaining ligament (ORL) at point 1 (Figure 6A), the needle is inserted perpendicular to the skin to reach the periosteum, then guided horizontally through the ORL. Once the needle reaches point 2, it is partially extracted leaving 4–5mm of the tip within the tissues, and it is then rotated and guided downwards through the nasolabial fat compartment (NLF) towards point 3 (Figure 6B). The needle is pulled out leaving 6–8mm under the skin, then turned and navigated through the NLF towards the jowl fat compartment (JF). Lightly pinching the segment that the needle is traveling through helps ensure its passage through the correct plane. The needle is partially withdrawn at point 4 leaving the tip at a depth of 8–10 mm and is redirected to aim upwards and travel cranially on the lateral side of the adhesive into the superficial medial cheek fat compartment (SMC), penetrating the skin at point 5. With 6–8mm of the needle tip left under the skin, it is brought upwards through the SMC towards the first point of insertion, in which a catheter needle is inserted to guide the suture needle out of the original entry point (Figure 6C). Partially extracting the needle at every point and using the catheter needle to exit from the first point of insertion are both imperative for avoiding skin dimpling. At point 1, the needle is again not fully withdrawn leaving 4–5mm buried, and the previous steps are repeated to complete a second round of the suture net. Upon return to point 1, the needle is pulled out completely, and after slight pulling to achieve the desired elevation, the two ends of the suture are knot together and buried under the skin.
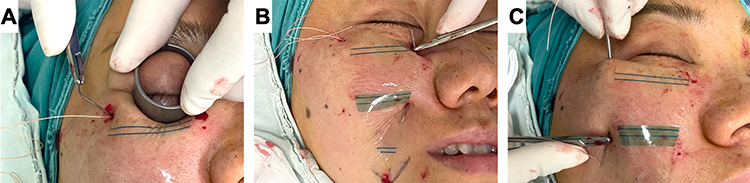 |
Figure 6 Jowl fat compartment repositioning. (A) The suture needle is inserted perpendicular to the skin at point 1. A metal ring is used to ensure eyeball protection while guiding the needle through the ORL. (B) The needle passes through the nasolabial fat compartment and exits at point 3. (C) The suture needle is guided into the catheter needle for extraction. |
Medial Cheek Fat Compartment Repositioning
To further elevate malar prominence, repositioning of the medial cheek fat is performed. A reference adhesive marking the SMC is placed on the malar area (Figure 4).
The procedure is done in the same netting fashion as jowl fat repositioning. The needle is navigated through points a to e twice, passing through the ORL superiorly, NLF medially, and SMC laterally. Depth of needle at partial extraction is 4–5mm at points a and b and 6–8mm at points c, d, and e (Supplementary Video).
Statistical Analysis
Ultrasound measurements at each point were statistically analyzed using a two-tailed paired t-test for each age group, while an unpaired t-test was used to compare both age groups. As for surgical evaluation, the distribution of variables was calculated using the Shapiro–Wilk test. Paired t-test and Wilcoxon signed-rank test were applied to determine the mean difference of volume, projection, and elevation change between baseline and each of the follow-up periods. The independent t-test and the Mann–Whitney U-test were used for age group comparisons. A value of p < 0.05 was considered statistically significant.
Results
A total of nine female volunteers (18 hemifaces) were included in our ultrasound study. The mean age for Group A was 26.4 years and that for Group B was 43.8 years. Shifting from an upright to a supine position, an increase in fat thickness was seen at the interior and exterior medial cheek and superior middle cheek points, while a decrease was seen at the superior and inferior nasolabial, inferior middle cheek, and jowl points in both age groups, p < 0.05. The changes in the medial cheek, nasolabial and superior middle cheek compartments of Group B were significantly greater than those of Group A, indicating that the degree of fat mobility may be affected by age (Figures 7 and 8).
 |
Figure 7 (A) Comparison of superficial facial fat thickness in the upright and supine positions for Group A. (B) Comparison of superficial facial fat thickness in the upright and supine positions at for Group B. (C) Comparison of change in fat thickness between Group A and Group B. *P < 0.05. |
 |
Figure 8 Ultrasound images of a 55-year-old volunteer depicting the increase in fat thickness from upright to supine at the interior and exterior medial cheek and superior middle cheek compartments and a decrease in the superior and inferior nasolabial, inferior middle cheek, and jowl compartment points. Yellow dashed lines represent upper and lower borders of superficial facial fat; white vertical lines represent thickness of superficial facial fat; red arrow points at metallic decal at point of measurement. |
Of the 165 patients who underwent both jowl and medial cheek fat compartment repositioning, 53 patients (all female, mean age 41.5 ± 9.0 years) completed all three follow-ups and were included in the statistical analysis. Table 2 describes volume and projection changes in the malar and jowl regions and the height changes in malar projection at each of the 1, 3, and 6-month follow-ups (p < 0.05). The malar zone showed a positive change in volume and projection by the final 6-month follow-up (mean changes, 2.23mL and 1.11mm, respectively), while a negative volume and projection change occurred in the jowl region (−0.18mL and −0.52mm respectively). Malar projection height demonstrated a positive change at 6 months (mean, 3.08mm), indicating an elevation in the position of the most projected point of the mid-cheek (Figure 3B). Three-dimensional images and volumetric color maps of 3 patient cases are shown in Figures 9–11. Additionally, patients were divided into three age groups: Group 1, <35 years; Group 2, 35 ~ 45 years; and Group 3, >45 years. Final check-in revealed significant differences in malar volume, projection, and height between Group 1 and Group 3, while no differences were found in the jowl region (Figure 12).
 |
Table 2 Volume, Projection, and Height Change of 53 Patients at 1, 3, and 6 Months Post- Operation Follow-Ups |
 |
Figure 9 A 40-year-old female presenting sagging jowl fat, flat malar mound, and prominent midcheek grooves underwent the two-step fat repositioning procedure. (A) Preoperative 3D photograph; (B) 6 months post-operative photograph; (C) 3-dimensional color map of the mid-cheek and jowl regions representing volume change at 6 months. |
 |
Figure 10 A 49-year-old female whose main complaint was mid-facial ptosis and the appearance of jowl fat. The two-step fat repositioning procedure was performed. (A) Preoperative 3D photograph; (B) 3 months post-operative photograph; (C) 3-dimensional color map of the mid-cheek and jowl regions depicting volume change at 3 months. |
 |
Figure 11 A 36-year-old female whose main complaint was mid-facial ptosis and a flat anterior mid-cheek. The two-step fat repositioning technique was performed. (A) Preoperative 3D photograph; (B) 6 months post-operative photograph; (C) 3-dimensional color map of the mid-cheek and jowl regions representing volume change at 6 months. |
 |
Figure 12 Comparison of volume, projection, and height change between age groups at 6-month follow-up (*P < 0.05; **P < 0.01). |
No major complications were reported. Patient complaints were limited to mild swelling and bruising, skin dimpling, and pigmentation at the site of needle insertion which resolved spontaneously without the need of intervention in all cases. Two patients (1.2%) developed an infection within one month after surgery which was resolved by the removal of the suture threads followed by irrigation of the wound with iodine and a prescription of oral antibiotics.
Discussion
The fat compartments of the face play different roles in determining facial shape and contour and contribute to age-related volume loss and facial ptosis.30 While several studies have stressed the role of deep fat deflation as the primary cause of midfacial volume loss, we believe that the inferior shift of superficial fat volume within each compartment is responsible for the aging characteristics of the anterior midface.4,31,32 Therefore, vertical repositioning of the ptotic superficial fat compartments proves to be an appropriate approach for reversing this volume displacement and regaining fullness to the midface.
Results of our ultrasound study demonstrated increased superficial fat thickness superiorly and laterally and decreased thickness inferiorly and medially. These results are in line with previous studies related to the mobility of superficial fat compartments and suggest their gliding tendency under the effect of gravity.18,21 This indicates that in supination, the superficial fat glides craniocaudally to naturally reposition itself to its youthful state, hinting that what was thought as volume loss may, in fact, be an inferior redistribution of fat tissue within each compartment.23 The theory behind this is that the superficial fat is loosely adherent to the SMAS relative to its attachment to the skin.29,33 Hence, fat descent within individual compartments can be depicted as a downward gliding motion posteriorly along the SMAS to form a thin upper portion and thick inferior portion “water droplet” shape (Figure 5).
Traditional rhytidectomy adopts a two-dimensional approach in which the skin and soft tissues are pulled obliquely upwards, which can produce exceptional lifting results but tend to flatten and widen the face. More recent face lift procedures have incorporated fat grafting34–36 or the repositioning of superficial fat through SMAS techniques8 to target volume augmentation of the malar and zygomatic area. However, Asian facial anatomy features a wider bizygomatic distance and a flatter midface, therefore, an anterior and central mid-face lift and fill may be preferable over traditional techniques.37 Furthermore, we observed that most patients exhibited ample facial fat that was simply displaced. We aimed to address these issues through our novel superficial fat compartment repositioning technique.
Based on the gliding theory of superficial fat, our surgical procedure repositions the superficial fat compartments to their supinated state by suspending and reconnecting the separated jowl, medial cheek, and nasolabial fat. This procedure differs from traditional thread lifting techniques; the latter uses multiple barbed sutures with vectors placed in a superior-lateral direction which results in volume augmentation of the lateral face.7,38 Contrarily, our technique adopts a purse-string-like suture which vertically repositions lower face volume to the anterior mid-cheek with the firm support of the ORL superiorly. The previously described aging “water droplet” shaped facial fat is reshaped into its youthful semi-spherical form. This simultaneously reduces the jowl fat, corrects sub-malar hollowing, and increases midface projection and three-dimensionality with no need for fat grafting. The produced net-like structure also reduces fat mobility and delays its inferior migration. Additionally, this structure encloses the fat tissue without placing excess tension along a single point or axis, reducing the possibility of cheese-wiring.
The results of our study suggest our fat compartment repositioning technique is effective in restoring a youthful facial contour by redistributing volume superiorly (Figures 13–15). In the early stage, volume change is partly due to post-operative edema, however results tend to become stable around 3 to 6 months after surgery, with a mean malar volume increase of 2.23mL and a mean jowl volume decrease of −0.18mL at the 6-month follow-up. This demonstrates that a sufficient amount of tissue is present to produce a natural result. The Patients in group 3 showed a more significant change in malar volume and height than those in group 1, while the opposite was true for malar projection. The greater degree of fat ptosis in the older group, as well as the initial higher position and firmness of fat in the younger group may have contributed to this trend. These findings provide further evidence to support the importance of superficial fat in midface volume loss.
 |
Figure 13 Preoperative (A–C) and 6 months postoperative (D–F) digital photographs of female patient from Figure 9 who underwent jowl and medial cheek fat repositioning. Major improvement is seen in the mid-cheek grooves, midcheek volume, nasolabial folds, and jowl area. |
 |
Figure 14 Preoperative (A–C) and 6 months postoperative (D–F) photographs of a 52-year-old female patient with remarkable improvement in the midcheek grooves and nasolabial folds. |
 |
Figure 15 Preoperative (A–C) and 3 months postoperative (D–F) photographs of a 48-year-old female patient showing increased malar volume, elevated malar position, and decreased jowl volume. |
The procedure is minimally invasive which is the preferred option for Asian patients who are concerned about scarring and longer post-operative downtime. While the entirety of the procedure is performed without direct visual observation of the operative plane, no severe complications such as hematoma and nerve injury were observed; however, a good understanding of the anatomy and a learning curve are required. To achieve optimal results, appropriate patient selection is necessary. The procedure is indicated in young and middle-aged patients who mainly exhibit signs of fat ptosis with no to minimal redundant skin. In older patients with skin laxity, superficial fat repositioning can be performed in conjunction with a facelift for improved outcomes.
Some limitations are present in this study. First, the volume and thickness of subcutaneous fat are closely linked to body mass index (BMI), which was not considered in this study. Another limitation was the short follow-up period and poor patient adherence, the latter possibly due to post-operative satisfaction, travel costs, and haste to undergo further facial aesthetic procedures during the follow-up period. Nevertheless, patients who visited after 12 months reported lasting results. Further studies are required to determine long-term outcomes of our technique.
Conclusion
In the present study, we first verified the gliding characteristic of the superficial fat compartments by means of ultrasound imaging, demonstrating their ability to naturally restore facial volume and contour in supination. We subsequently introduced our novel method of mid-facial rejuvenation which successfully repositions the superficial fat compartments, prevents fat from moving inferiorly within the compartments, and restores youthful midfacial projection. Overall, our technique is safe and effective for achieving natural rejuvenative results.
Ethical Approval
All procedures performed in this study were in accordance with the ethical standards of the national laws of clinical practice and the Declaration of Helsinki and were approved by the ethics committee of Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine.
Informed consent
Written informed consent was obtained from all participants for use of their images in publications.
Funding
No funding was received for this article.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Boehm LM, Morgan A, Hettinger P, Matloub HS. Facial aging: a quantitative analysis of midface volume changes over 11 years. Plast Reconstr Surg. 2021;147(2):319–327. doi:10.1097/PRS.0000000000007518
2. Rohrich RJ, Pessa JE. The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007;119(7):2219–2227. doi:10.1097/01.prs.0000265403.66886.54
3. Kretlow JD, Hollier LH Jr, Hatef DA. The facial aging debate of deflation versus attenuation: attenuation strikes back. Plast Reconstr Surg. 2012;130(1):180e–181e. doi:10.1097/PRS.0b013e318254f619
4. Rohrich RJ, Pessa JE, Ristow B. The youthful cheek and the deep medial fat compartment. Plast Reconstr Surg. 2008;121(6):2107–2112. doi:10.1097/PRS.0b013e31817123c6
5. Swift A, Liew S, Weinkle S, Garcia JK, Silberberg MB. The facial aging process from the “Inside out”. Aesthet Surg J. 2021;41(10):1107–1119. doi:10.1093/asj/sjaa339
6. Wan D, Small KH, Barton FE. Face lift. Plast Reconstr Surg. 2015;136(5):676e–689e. doi:10.1097/PRS.0000000000001695
7. Halepas S, Chen XJ, Ferneini EM. Thread-lift sutures: anatomy, technique, and review of current literature. J Oral Maxillofac Surg. 2020;78(5):813–820. doi:10.1016/j.joms.2019.11.011
8. Stuzin JM, Rohrich RJ, Dayan E. The facial fat compartments revisited: clinical relevance to subcutaneous dissection and facial deflation in face lifting. Plast Reconstr Surg. 2019;144(5):1070–1078. doi:10.1097/PRS.0000000000006181
9. Divaris M, Sabri E, Cancemi G, Daury R. LCL: (Locked Cheek Lift) three-dimensional cheek lift and inferior palpebral rejuvenation. Aesthetic Plast Surg. 2018;42(3):825–838. doi:10.1007/s00266-018-1086-1
10. Zou C, Liu Y, Wang X, Wang T, Wang J. Vertical midface lifting: an improved technique for Asians. Dermatol Surg. 2020;46(11):e88–e95. doi:10.1097/DSS.0000000000002341
11. Askeroglu U, Kayadibi T, Pilanci O. Trinity lift: a unique technique for endoscopic midface and lower periorbital unit lift. Aesthetic Plast Surg. 2021;45(3):992–1001. doi:10.1007/s00266-021-02126-5
12. Myung Y, Jung C. Mini-midface lift using polydioxanone cog threads. Plast Reconstr Surg Glob Open. 2020;8(6):e2920. doi:10.1097/GOX.0000000000002920
13. Bellity P, Bellity J. Facial rejuvenation enhancing cheek lift. Arch Plast Surg. 2017;44(6):559–563. doi:10.5999/aps.2016.01858
14. Jacono AA, Malone MH, Talei B. Three-dimensional analysis of long-term midface volume change after vertical vector deep-plane rhytidectomy. Aesthet Surg J. 2015;35(5):491–503. doi:10.1093/asj/sju171
15. Cotofana S, Gotkin RH, Frank K, Lachman N, Schenck TL. Anatomy behind the facial overfilled syndrome: the transverse facial septum. Dermatol Surg. 2020;46(8):e16–e22. doi:10.1097/DSS.0000000000002236
16. Gosain AK, Klein MH, Sudhakar PV, Prost RW. A volumetric analysis of soft-tissue changes in the aging midface using high-resolution MRI: implications for facial rejuvenation. Plast Reconstr Surg. 2005;115(4):1143–1152. doi:10.1097/01.PRS.0000156333.57852.2F
17. Cevik Cenkeri H, Sarigul Guduk S, Derin Cicek E. Aging changes of the superficial fat compartments of the midface over time: a magnetic resonance imaging study. Dermatol Surg. 2020;46(12):1600–1605. doi:10.1097/DSS.0000000000002646
18. Schenck TL, Koban KC, Schlattau A, et al. The functional anatomy of the superficial fat compartments of the face: a detailed imaging study. Plast Reconstr Surg. 2018;141(6):1351–1359. doi:10.1097/PRS.0000000000004364
19. Wen LH, Zhong PH, Wang XL, et al. Analysis of age-related changes in midfacial fat compartments in Asian women using computed tomography. J Plast Reconstr Aesthet Surg. 2019;72(11):1839–1846. doi:10.1016/j.bjps.2019.05.035
20. Gierloff M, Stöhring C, Buder T, Wiltfang J. The subcutaneous fat compartments in relation to aesthetically important facial folds and rhytides. J Plast Reconstr Aesthet Surg. 2012;65(10):1292–1297. doi:10.1016/j.bjps.2012.04.047
21. Schelke L, Velthuis PJ, Lowry N, et al. The mobility of the superficial and deep midfacial fat compartments: an ultrasound-based investigation. J Cosmet Dermatol. 2021;20(12):3849–3856. doi:10.1111/jocd.14374
22. Mally P, Czyz CN, Wulc AE. The role of gravity in periorbital and midfacial aging. Aesthet Surg J. 2014;34(6):809–822. doi:10.1177/1090820X14535077
23. Ramesh S, Johnson P, Sarcu D, Wulc AE. Gravity in midfacial aging: a 3-dimensional study. Aesthet Surg J. 2021;41(2):143–151. doi:10.1093/asj/sjaa021
24. Störchle P, Müller W, Sengeis M, et al. Standardized ultrasound measurement of subcutaneous fat patterning: high reliability and accuracy in groups ranging from lean to obese. Ultrasound Med Biol. 2017;43(2):427–438. doi:10.1016/j.ultrasmedbio.2016.09.014
25. Cotofana S, Hexsel D, Avelar LE, et al. Calculating the thickness of the superficial fatty layer of the body using age, gender, and body mass index. J Drugs Dermatol. 2020;19(1):36–44. doi:10.36849/JDD.2020.4619
26. Ye Y, Song Z, Guo J, Qiao Y. SIAT-3DFE: a high-resolution 3D facial expression dataset. IEEE Access. 2020;8:48205–48211. doi:10.1109/ACCESS.2020.2979518
27. Cotofana S, Lachman N. Anatomy of the facial fat compartments and their relevance in aesthetic surgery. J Dtsch Dermatol Ges. 2019;17(4):399–413.
28. Wan D, Amirlak B, Giessler P, et al. The differing adipocyte morphologies of deep versus superficial midfacial fat compartments: a cadaveric study. Plast Reconstr Surg. 2014;133(5):615e–622e. doi:10.1097/PRS.0000000000000100
29. Fundarò S, Mauro G, Di Blasio A, Di Blasio C, Schembri-Wismayer P. Anatomy and aging of cheek fat compartments. Med Dent Res. 2018;1(3):1–7.
30. Ramanadham SR, Rohrich RJ. Newer understanding of specific anatomic targets in the aging face as applied to injectables: superficial and deep facial fat compartments--an evolving target for site-specific facial augmentation. Plast Reconstr Surg. 2015;136(5 Suppl):49s–55s. doi:10.1097/PRS.0000000000001730
31. Cotofana S, Gotkin RH, Frank K, et al. The functional anatomy of the deep facial fat compartments: a detailed imaging-based investigation. Plast Reconstr Surg. 2019;143(1):53–63. doi:10.1097/PRS.0000000000005080
32. Divaris M, Sabri E, Ohana S. ”Mirror Face Lift”: concept, description, and evaluation 1 year postoperatively. Plast Reconstr Surg Glob Open. 2020;8(3):e2697. doi:10.1097/GOX.0000000000002697
33. Rohrich RJ, Pessa JE. The retaining system of the face: histologic evaluation of the septal boundaries of the subcutaneous fat compartments. Plast Reconstr Surg. 2008;121(5):1804–1809. doi:10.1097/PRS.0b013e31816c3c1a
34. Schreiber JE, Terner J, Stern CS, et al. The boomerang lift: a three-step compartment-based approach to the youthful cheek. Plast Reconstr Surg. 2018;141(4):910–913. doi:10.1097/PRS.0000000000004251
35. Rohrich RJ, Afrooz PN. Finesse in face lifting: the role of facial fat compartment augmentation in facial rejuvenation. Plast Reconstr Surg. 2019;143(1):98–101. doi:10.1097/PRS.0000000000005165
36. Rohrich RJ, Ghavami A, Constantine FC, Unger J, Mojallal A. Lift-and-fill face lift: integrating the fat compartments. Plast Reconstr Surg. 2014;133(6):756e–767e. doi:10.1097/01.prs.0000436817.96214.7e
37. Wong CH, Hsieh MKH, Mendelson B. Asian face lift with the composite face lift technique. Plast Reconstr Surg. 2022;149(1):59–69. doi:10.1097/PRS.0000000000008686
38. Kwon HH, Choi SC, Park GH, Jung JY. Clinical evaluations of a novel thread lifting regimen using barbed polyglyconate suture for facial rejuvenation: analysis using a 3-dimensional imaging system. Dermatol Surg. 2019;45(3):431–437. doi:10.1097/DSS.0000000000001642
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.