Back to Journals » Nature and Science of Sleep » Volume 17

Family Support Moderates the Relationship Between Pregnancy Stress, Depressive Symptoms, and Insomnia
Authors Liu S, Huang M, Zhang F, Tao J, Wen D, Deng W, Lin Y, Zhang P, Li M
Received 23 September 2024
Accepted for publication 5 February 2025
Published 6 February 2025 Volume 2025:17 Pages 261—270
DOI https://doi.org/10.2147/NSS.S496205
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Valentina Alfonsi
ShanYan Liu,1 Meijiao Huang,2 FengYing Zhang,2 Jing Tao,1 Dan Wen,1 WeiYuan Deng,1 YaoHua Lin,3 Ping Zhang,2 Min Li2
1The Affiliated Nanhua Hospital, Department of Obstetrics, Hengyang Medical College, University of South China, Hengyang, Hunan, 421002, People’s Republic of China; 2The Affiliated Nanhua Hospital, Department of Neurology, Hengyang Medical College, University of South China, Hengyang, Hunan, 421002, People’s Republic of China; 3The First Affiliated Hospital, Institute of Obstetrics, Hengyang Medical School, University of South China, Hengyang, Hunan, 421001, People’s Republic of China
Correspondence: Ping Zhang; Min Li, The Affiliated Nanhua Hospital, Department of Neurology, Hengyang Medical College, University of South China, Hengyang, Hunan, 421002, People’s Republic of China, Email [email protected]; [email protected]
Objective: Insomnia is a common issue that pregnant women often have to deal with. This study seeks to examine the connections between pregnancy stress, depressive symptoms, family support, and insomnia symptoms.
Methods: Convenience sampling was employed to recruit 1049 valid participants. The primary measurement tools utilized were the Pregnancy Stress Scale, the Family Support Subscale, and the Patient Health Questionnaire-2. Data analysis was conducted using SPSS 24.0 software. Using binary logistic regression to verify the independent effects of pregnancy stress, depression symptoms, and family support on insomnia symptoms. PROCESS macro Model 4 was applied to assess the mediating effect, while PROCESS macro Model 5 was used to evaluate the moderating effect.
Results: The overall prevalence of insomnia symptoms and depressive symptoms among pregnant women was 54% (n=572) and 20% (n=207) in this study. Pregnancy stress, depressive symptoms and family support positively affect insomnia symptoms. The indirect effect of depressive symptoms between pregnancy stress and insomnia symptoms was significant, with the mediator proportion of 45.16%. As moderator, family support weakens the impact of pregnancy stress on insomnia symptoms.
Conclusion: Increased pregnancy stress and increased depressive symptoms could trigger insomnia symptoms. Depressive symptoms mediated the path from between pregnancy stress and insomnia symptoms. Family support weakened the link between pregnancy stress and insomnia symptoms. These findings can assist pregnant women in managing stress more effectively and improving their mental well-being.
Keywords: depressive symptoms, family support, insomnia symptoms, pregnancy stress, pregnant woman
Introduction
Pregnant women experience substantial physiological and psychological changes, which can significantly impact their sleep patterns.1,2 Pregnancy-related sleep disorders refer to the decline in sleep quality that many pregnant individuals encounter.3 These disorders are primarily characterized by insomnia symptoms, such as increased difficulty maintaining sleep throughout the night and frequent early morning awakenings.4 Numerous studies have indicated that nearly half of pregnant women experience poor sleep quality.5–10 The sleep quality of these women is influenced by a myriad of factors, with social and psychological elements garnering significant attention.7 Pregnancy stress, which denotes the perception of various stressors encountered during pregnancy,11 encompasses navigating societal and familial expectations, apprehensions about assuming the maternal role, and coping with physical discomforts associated with pregnancy.12,13 These cumulative pressures can detrimentally affect sleep quality.14,15 Consequently, this study posits that increased pregnancy stress may precipitate insomnia symptoms in pregnant women.
From the perspective of path relationships, depressive symptoms as core psychological factors may mediate the relationship between pregnancy stress and insomnia. The prevalence of depressive symptoms, one of the most common psychological problems among pregnant women, ranges from 10 to 20%.16–18 Many evidences have shown that pregnancy stress is a major risk factor for depressive symptoms during trimester.18–23 Despite pregnancy stress and its negative influences, previous studies have shown that social support systems have a beneficial impact on mental health.24–26 Family support, as an integral component of social support, is closely intertwined with the mental well-being of pregnant women.24,25,27 Evidence suggested that family relationships and social support are negatively correlated with postpartum depression and sleep problems.28–31 Therefore, this study hypothesized that depressive symptoms as mediator and family as moderator affect the relationship between pregnancy stress and insomnia symptoms.
Overall, existing research provides fragmented evidence indicating that pregnancy stress is positively associated with depressive symptoms and sleep disturbances, while family support exhibits a protective effect, showing a negative correlation with sleep problems. However, to date, no comprehensive studies have integrated these factors to thoroughly examine the relationships among pregnancy stress, depressive symptoms, family support, and insomnia symptoms. To address this research gap, the current study aimed to test: 1) the prevalence of insomnia and depressive symptoms in pregnant women. 2) The effect of pregnancy stress, depressive symptoms, and family support on insomnia symptoms; 3) The mediating effect of depressive symptoms between pregnancy stress and insomnia symptoms; and 4) The moderating effect of family support between pregnancy stress and insomnia symptoms. The research model was showed in Figure 1. Based on findings, this study can offer valuable strategies to address stress during pregnancy, such as psychological support at the family level and conducting relaxation training to enhance sleep quality. The primary goal of this study is to assist pregnant women in managing stress more effectively and improving their mental well-being.
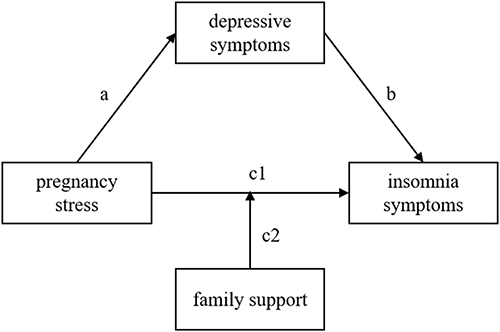 |
Figure 1 The research model. The path from pregnancy stress to depressive symptoms was denoted as path a, while the path from depressive symptoms to insomnia symptoms was represented as path b. The direct path from pregnancy stress to insomnia symptoms was labeled as path c1. The indirect effect of pregnancy stress on insomnia symptoms through mediator depressive symptoms was calculated by multiplying path a and path b. The total effect was the sum of the direct effect (c1) and the indirect effect (a*b). The moderation effect of family support between pregnancy stress and insomnia. |
Methods
Participant and Procedure
This study adopted a cross-sectional survey design and was conducted from July to August 2024. This study employed convenience sampling to recruit pregnant women attending obstetrics clinics at three tertiary hospitals in Hengyang, Hunan Province, China, as study participants. The research team contacted the obstetric leaders of three hospitals to explain the research objectives and procedures, and received support from the hospitals.
According to previous research,32,33 the sample size for a cross-sectional descriptive survey aimed at estimating a proportion can be determined using Equation (1). Prior studies have indicated that the prevalence of insomnia symptoms among pregnant women stands at approximately 45.7%.7 Assuming an acceptable error margin of 0.05 (e = 0.05) for this proportion, and with an anticipated population proportion of 0.6 (p = 0.6), the required sample size for the survey, at a significance level of 0.05 (α = 0.05) with Z1-α/2= 1.96, was calculated to be 381. In addition, previous study showed that the prevalence of depressive symptoms among pregnant women was about 38.2%,8 the required sample was calculated to be 363. Combining two variables, the minimum sample size required for this study is 744 participants.
The online questionnaire was meticulously designed and distributed via the Wenjuanxing platform, a widely-used online survey tool in China. Researchers introduced the reasons and purposes of this survey to pregnant women. After obtaining consent and signing the informed consent form, the pregnant women scanned the QR code to fill out the electronic questionnaire. During the filling process, one researcher used a unified guide to explain the items that were confused. The investigation followed guidelines to ensure that the research was voluntary and confidential. If the pregnant women experienced any discomfort during the filling process, they could withdraw from the survey at any time.
A total of 1226 questionnaires were distributed by the researcher across three hospitals, with 503, 379, and 344 questionnaires handed out at each respective hospital. The raw data were screened using the inclusion and exclusion criteria. This study included pregnant women who were 18 years of age or older. Pregnant women were excluded if they had fetal abnormalities, prior diagnosed mental health conditions, or concurrent organic diseases (ie, malignant tumors). This information was gathered via questionnaire. Pregnant women who respond affirmatively to these criteria will be excluded from the study. After data cleaning, this study obtained 1049 valid data, with an effective rate of 85.56%.
Measurement
Insomnia Symptoms (IS)
Insomnia symptoms in pregnant women were evaluated using three items: difficulty initiating sleep (DIS), difficulty maintaining sleep (DMS), and early morning awakening (EMA).34 Each item is scored with 5 grades, including 1=never, 2= less than once a week, 3= 1–2 times a week, 4= 3–5 times a week, 5= 6–7 times a week. Participants were considered to have insomnia symptoms if they experienced any symptom on three or more occasions (response ≥ 4).34 In this study, the Cronbach’s α for the IS was 0.77.
Pregnancy Stress (PP)
The Pregnancy Stress Scale (PSS) is a self-reported assessment tool used in Taiwan to measure stress levels during pregnancy.12 This study adopted a sub-scale of “seeking safe passage for mother and child”, consisting of eight items like “I worry about abnormal or difficult birth”, “I worry about premature labor”, and “I worry about unbearable labor pain”.12 The items rated on a 4-point scale (0=none, 1=mild, 2=moderate, 3=severe). It considers China’s cultural background during its development. The higher the PPS score, the higher is the level of stress experienced during pregnancy. In this study, Cronbach’s α of the PSS was 0.92.
Family Support (FS)
This study used the Family Support sub0scale (FSS) of the Perceived Social Support Scale35 to evaluate family support in pregnant women. This sub-scale consists of four items, such as “My family really tries to help me”, all of which are scored on a four-point Likert 4-level scoring method. The scores ranged from “strongly disagree“ to ”strongly agree”, with 1–4 points. The higher the score, the higher the individual’s understanding of the family support. In this study, Cronbach’s α of the FSS was 0.96.
Depressive Symptoms (DS)
This study adopted 2 items from the Patient Health Questionnaire-2 (PHQ-2)36 to measure depressive symptoms of pregnant woman. Pregnant women need to answer questions “Over the past 2 weeks, how often have you been bothered by any of the following problems?” with 4-point Likert scale ranging from 0= “not at all” to 3= “nearly every day”. Item 1 was “Little interest or pleasure in doing things”, while Item 2 was “feeling down, depressed or hopeless”. A total score greater than or equal to 3 indicates that an individual has clinical depressive symptoms.36 The higher the total item score, the higher the total level of depressive symptoms. In this study, Cronbach’s α for the PHQ-2 was 0.78.
This study also collected demographic information on pregnant women, including age (years), educational level, monthly family income, residence, medical insurance, and trimester (1st = [0, 13 weeks], 2nd= [14 weeks, 27 weeks], 3rd= [28 weeks, 40 weeks]).6,23
Data Analysis
The survey data was used SPSS 24.0 software to the main analysis. This study used n (%) to represent the count data and performed the χ2 tests. This study used M±SD to represent metric data with normal distribution and homogeneity of variance and performed a T-test or ANOVA. This study tested the relationship between pregnancy stress, depressive symptoms, family support, and insomnia symptoms using Pearson’s correlation and binary logic regression analyses. The bias-corrected percentile bootstrap method was used to analyze the mediating effect of depressive symptoms, and the PROCESS MODEL was used to test the mediation and moderation models. p<0.05, indicating that the difference in the data was statistically significant. The PROCESS macro, developed by Andrew F. Hayes for SPSS, is a specialized tool designed to handle a wide range of mediation and moderation analyses.37 It enables researchers to examine models with single or multiple mediators, moderators (including moderated mediation), and provides comprehensive output including bootstrap confidence intervals and effect size estimates for mediated effects.
Model 4 from the PROCESS Macro is simple mediation. By default, PROCESS employed bootstrapped confidence intervals to estimate the indirect effect. The ratio of the indirect effect (a*b) and total effect (a*b + c) represents the mediator proportion.37 Based on Model 4, Model 5 added a moderator of direct independent variable-dependent variable path only. In this study, family support was the moderator between pregnancy stress and insomnia symptoms. If the moderation effect (the multiply of pregnancy stress and family support) is significant, then it is necessary to conduct simple slope tests. Simple slope tests are conditional hypothesis tests of whether the relationship between independent variable and dependent variable is significant at a particular value of the moderator, usually one standard deviation above and below the mean (M±SD).37
Results
Sample Characteristics
Among the participants (Table 1), the overall prevalence of insomnia symptoms and depressive symptoms among pregnant women was 54.5% (n=572) and 19.7% (n=207). 75.1% pregnant women were aged 25–34 (n=788); 74.2% pregnant women had a bachelor’s degree (n=778); 42.8% pregnant women had a monthly family income of 3000–10000 yuan (n=449), while 51.9% pregnant women had a monthly income greater than 1000 yuan (n=544); 72.2% pregnant women residing in the city (n=757); 86.8% pregnant women with medical insurance (n=911); 10.4% pregnant women were in 1st trimester (n=109), 27.5% pregnant women were in 2nd trimester (n=288), and 62.2% pregnant women were in 3rd trimester (n=652).
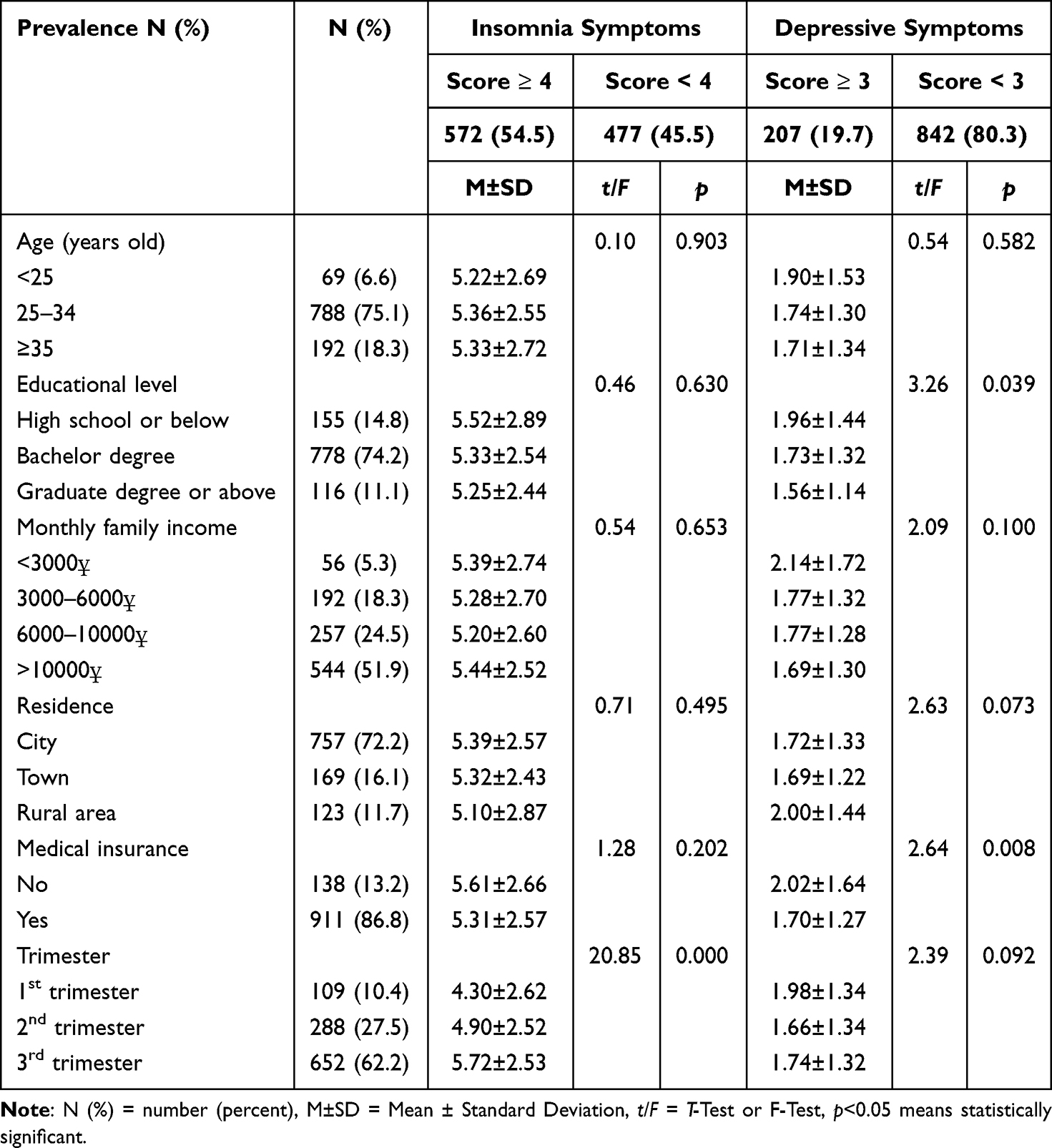 |
Table 1 Demographic characteristics Among Pregnant Women |
The Binary Logistic Regression Model
In the unadjusted model (Table 2), higher levels of pregnancy stress are associated with an increased likelihood of insomnia symptoms in pregnant women (OR=1.49, 95% CI= [1.28, 1.74]). Similarly, more severe depressive symptoms also correlate with a greater propensity for insomnia symptoms during pregnancy (OR=1.50, 95% CI= [1.29, 1.75]). Conversely, pregnant women are less likely to have insomnia symptoms with higher levels of family support (OR=0.88, 95% CI= [0.77, 0.99]). After controlling for the effect of trimester, although the coefficients decreased slightly, the relationships remained significant. These results indicate that pregnancy stress and depressive symptoms are risk factors for insomnia symptoms, whereas family support is a protective factor for having insomnia symptoms.
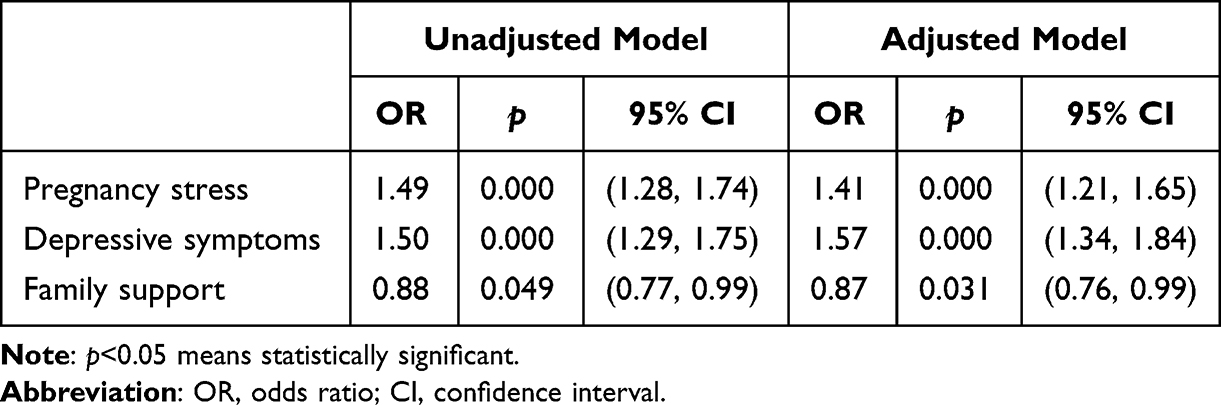 |
Table 2 The Effect of Pregnancy Stress, Depressive Symptoms, and Family Support on Insomnia Symptoms |
The Mediating Effect of Depressive Symptoms
According to correlation analysis, the relation between pregnancy stress and insomnia symptoms (r=0.33, p<0.01), pregnancy stress and depressive symptoms (r=0.48, p<0.01), family support and insomnia symptoms (r=−0.07, p<0.05), and depressive symptoms and insomnia symptoms (r=0.36, p<0.01) were significant.
Next, this study used PROCESS MODEL 4 to test the mediating effect of depressive symptoms on the relationship between pregnancy stress and insomnia symptoms. As shown in Table 3 and Figure 2, increased pregnancy stress was significantly associated with increased depressive symptoms (β=0.50, 95% CI= [0.44, 0.55]) and increased insomnia symptoms (β=0.16, 95% CI= [0.10, 0.23]); increased depressive symptoms significantly influenced increased insomnia symptoms (β=0.28, 95% CI= [0.22, 0.35]). The indirect effect of depressive symptoms between pregnancy stress and insomnia symptoms was significant (β=0.14, 95% CI= [0.11, 0.18]), with mediator proportion of 45.16%.
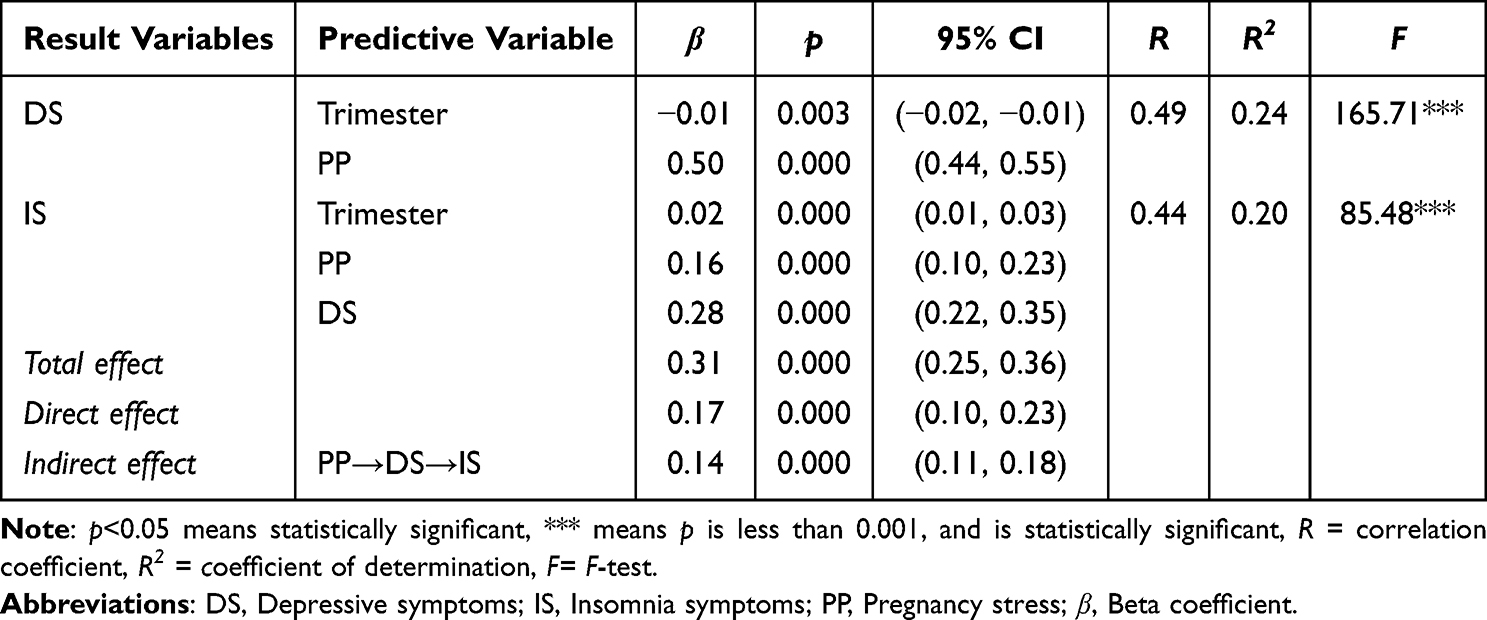 |
Table 3 The Mediating Effect of Depressive Symptoms on the Relationship Between Pregnancy Stress and Insomnia Symptoms |
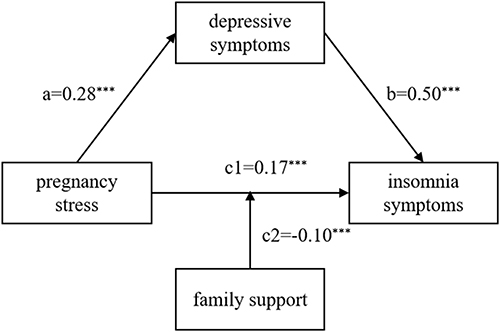 |
Figure 2 The test model. *** means p is less than 0.001, and is statistically significant. Increased pregnancy stress was significantly associated with increased depressive symptoms and increased insomnia symptoms. Increased depressive symptoms significantly influenced increased insomnia symptoms. The interaction effect of pregnancy stress and family support negatively affected insomnia symptoms. |
The Moderating Effect Test
Taking the trimester as the control variable, this study adopted PROCESS MODEL 5 to test the moderating effect of family support on the relationship between pregnancy stress and insomnia symptoms. As shown in Table 4 and Figure 3, the interaction effect of pregnancy stress and family support negatively affected insomnia symptoms (β=−0.10, p < 0.001, 95% CI= [−0.15, −0.04]). Next, this study divided the values of family support into high and low groups and selected the high family support group (SD+1) and low family support group (SD-1) for a simple slope test. As shown in Figure 3, when family support was low, pregnancy stress positively affected insomnia symptoms (β_simple=0.23, p<0.001, 95% CI= [0.16, 0.30]), whereas when family support was high, pregnancy stress did not significantly affect insomnia symptoms (β_simple=0.06, p>0.05, 95% CI= [−0.02, 0.14]). This result indicated that family support weakens the impact of pregnancy stress on insomnia symptoms.
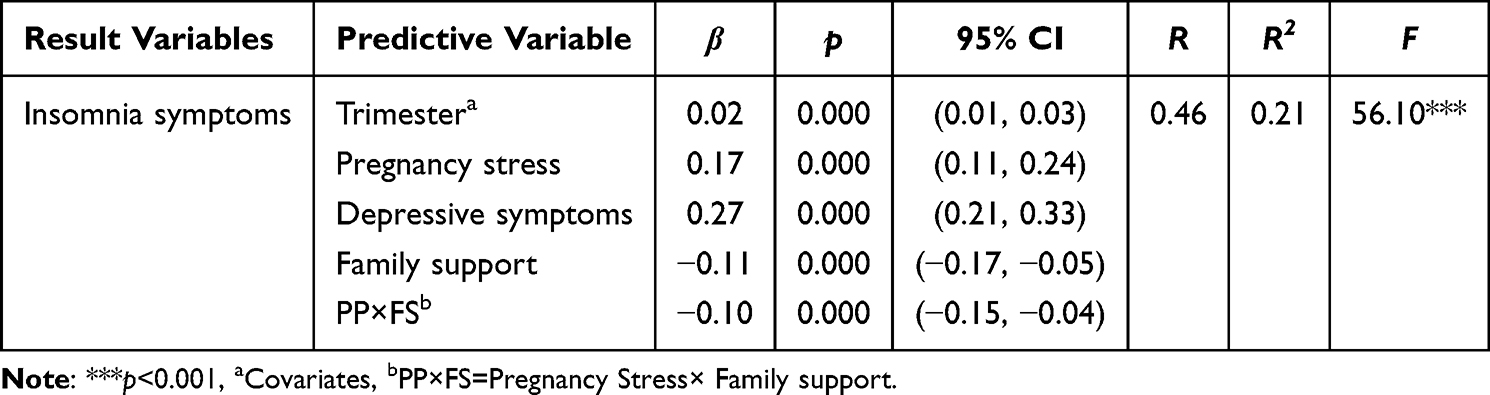 |
Table 4 The Moderating Effect of Family Support Between Pregnancy Stress and Insomnia Symptoms |
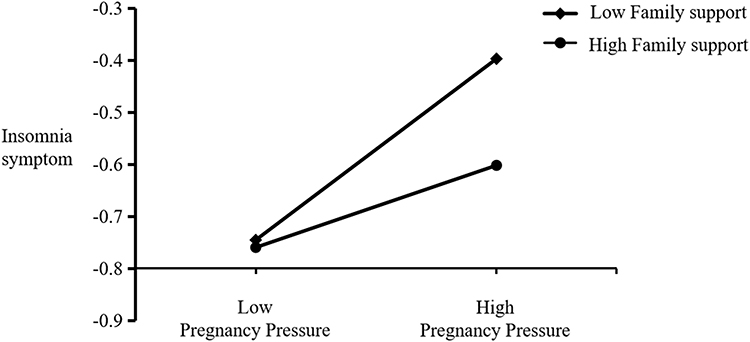 |
Figure 3 The simple slope plot of moderating effect. When family support was low (M-SD), pregnancy stress positively affected insomnia symptoms, whereas when family support was high (M+SD), pregnancy stress did not significantly affect insomnia symptoms. |
Discussion
First, this study found that the prevalence of insomnia symptoms among pregnant women was 54% and the prevalence of depressive symptoms was 20%. The prevalence of insomnia symptoms in this study was higher than that in a recent meta-analysis, which found that the prevalence of insomnia symptoms in pregnant women was 38.2%.8 Furthermore, this study revealed that 20% of pregnant women experienced depressive symptoms, which is consistent with previous research. Evidence indicates that the prevalence of depressive symptoms in pregnant women ranges between 10% and 20%.16–18
Second, this study found that pregnancy stress was a risk factor for insomnia symptoms among pregnant women. This finding echo previous studies such as those by Gao et al and Mei et al, which reported that poor sleep quality in pregnant women is affected by pregnancy stress.14,15 The Stress Response Model explains how people respond to stressors and how their actions affect physical and mental health.38 From a physiological perspective, stress hormones such as cortisol may increase during pregnancy. Increased hormone levels may result in activation of the arousal system, increased alertness, and consequently, sleep. In addition, stress reactions may lead to physiological discomfort,38 such as increased heart rate, muscle tension, frequent urination, and heartburn, which may increase pressure on pregnant women and affect sleep quality. From the perspective of behavioral responses, pregnant women may adopt inappropriate coping strategies to cope with pregnancy stress and insomnia,39 such as excessive use of mobile phones or irregular sleep habits, which may exacerbate sleep problems.
Third, this study illustrates that depressive symptoms mediated the relationship between pregnancy stress and insomnia symptoms in pregnant women. Previous studies have shown that pregnancy stress alone affect depressive symptoms, while depressive symptoms trigger insomnia.21–23 This study provides direct evidence of the relationship between pregnancy-related stress and insomnia symptoms, with depressive symptoms acting as a mediating factor. According to Stress-Emotion Theory, individuals exposed to high-pressure environments—such as the stress associated with childbirth—may experience psychological and physiological responses that lead to negative emotions, including depressive symptoms.40 These emotional states can subsequently impact physiological functions, notably sleep. Depressive symptoms are known to induce significant physiological changes, such as reduced physical activity and heightened nighttime distress, both of which are directly associated with insomnia.34 Therefore, it is crucial to conduct early screening for depressive symptoms during pregnancy and evaluate pregnant women who exhibit these symptoms. Implementing effective interventions, such as psychological counseling and education on healthy sleep practices, can help alleviate psychological pressure and negative emotions during pregnancy, ultimately improving sleep quality.
Fourth, this study reveals that family support weakens the relationship between pregnancy stress and insomnia symptoms. Women often rely on family support during pregnancy.24 Previous studies have confirmed that family support plays a crucial role in the mental health of pregnant women.24,25,28 This study extends this relationship to the sleep health of pregnant women. According to the buffering model, comprehending family support can mitigate the effects of stressful conditions or situations on an individual’s physical and mental health.41 Previous studies have found that individuals with better family support, such as an understanding from family members and support from friends and peers, are less likely to experience mental health problems.27 For pregnant women, strong family support can substantially ease psychological stress and mitigate its influence on sleep disturbances. When these women perceive low levels of family support, their insomnia symptoms tend to increase markedly with rising stress levels. Conversely, as stress escalates, the rate of increase in insomnia symptoms slows down if pregnant women feel they have good family support. Therefore, it is necessary to improve pregnant women’s understanding of family support levels, promote family and important relatives to provide more care and attention to pregnant women during pregnancy, and enhance family support levels, thereby reducing the occurrence of insomnia and promoting good maternal and infant outcomes.
Finally, this study validated the impact of demographic and pregnancy factors on insomnia symptoms in pregnant women. Unlike previous studies,5,9,10 this study did not find significant differences in insomnia symptoms among pregnant women in terms of age, education level, monthly family income, residence, or medical insurance. This study found that the trimester is a symptom of insomnia in pregnant women; the later the pregnancy, the more severe the insomnia symptoms of pregnant women. This finding is consistent with those of most studies.6,23 This may be because the uterus significantly enlarges during late pregnancy, leading to increased nocturia, restricted respiratory function (shortness of breath, difficulty breathing), and other discomfort, thereby reducing the quality of nighttime sleep. In addition, most pregnant women in their third trimester are more concerned about the safety of their mother and baby during vaginal or cesarean delivery, which also leads to increased sleep problems. To prevent negative consequences for both mothers and babies, it is recommended that relevant institutions conduct early screening and interventions for sleep disorders in pregnant women.
This study has several limitations. For one thing, the data were derived from a cross-sectional survey conducted in three hospitals in a southern Chinese city, with participants being conveniently selected pregnant women. This sampling method may limit the generalizability of findings. For another, while this study examined both mediation and moderation effects, it did not delve into in-depth causal relationships, which should be addressed in future research. This study did not classify pregnant women and failed to consider internal heterogeneity, such as a lack of attention to unmarried pregnant women.
Conclusion
This study revealed that increased pregnancy stress and increased depressive symptoms can lead to insomnia symptoms. Specifically, depressive symptoms act as a mediator in the relationship between pregnancy stress and insomnia. Moreover, family support plays a crucial role in weakening the impact of pregnancy stress on insomnia. For future research, longitudinal tracking surveys are recommended to further examine the causal relationships among these variables. Such studies could provide more comprehensive insights and allow for refinements and expansions of the current findings.
IRB Statement
The study protocol has been approved by the Research Ethics Committee of The Affiliated Nanhua Hospital, under the code 2024-ky-095, as laid out in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Consent to Participate
Informed consent was obtained from all the participants.
Funding
This study was supported by Foundation of Health Commission of Hunan Province (No.2021105011370, No.202203074999).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Lagadec N, Steinecker M, Kapassi A, et al. Factors influencing the quality of life of pregnant women: a systematic review. BMC Pregnancy Childb. 2018;18:455. doi:10.1186/s12884-018-2087-4
2. Widelock T, Denney J, Brost B. Pregnancy and parturition: the physical and physiological changes and their pathologies. In: Gomes-Ferreira M, Olivas-Menayo J, editors. Post-Maternity Body Changes: Obstetric Fundamentals and Surgical Reshaping. Cham: Springer International Publishing; 2023:25–47.
3. Wong PF, D, Cruz R, Hare A. Sleep Disorders in Pregnancy. Breathe. 2022;18:220004. doi:10.1183/20734735.0004-2022
4. Sedov I, Anderson N, Dhillon A, Tomfohr-Madsen LM. Insomnia symptoms during pregnancy: a meta-analysis. J Sleep Res. 2021;30:e13207. doi:10.1111/jsr.13207
5. Lu Q, Zhang X, Wang Y, et al. Sleep disturbances during pregnancy and adverse maternal and fetal outcomes: a systematic review and meta-analysis. Sleep Med Rev. 2021;58:101436. doi:10.1016/j.smrv.2021.101436
6. Zhang H, Li P, Fan D, et al. Prevalence of and risk factors for poor sleep during different trimesters of pregnancy among women in China: a cross-sectional study. Nat Sci Sleep. 2021;13:811–820. doi:10.2147/NSS.S303763
7. Sedov I, Cameron E, Madigan S, Tomfohr-Madsen LM. Sleep quality during pregnancy: a meta-analysis. Sleep Med Rev. 2018;38:168–176. doi:10.1016/j.smrv.2017.06.005
8. Meers JM, Nowakowski S. Sleep during pregnancy. Curr Psychiat Rep. 2022;24:353–357. doi:10.1007/s11920-022-01343-2
9. Li H, Li H, Zhong J, et al. Association between sleep disorders during pregnancy and risk of postpartum depression: a systematic review and meta-analysis. Arch Women’s Mental Health. 2023;26:259–267. doi:10.1007/s00737-023-01295-3
10. Yang Z, Zhu Z, Wang C, Zhang F, Zeng H. Association between adverse perinatal outcomes and sleep disturbances during pregnancy: a systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2022;35:166–174. doi:10.1080/14767058.2020.1711727
11. Traylor C, Johnson JD, Kimmel M, Manuck TA. Effects of psychological stress on adverse pregnancy outcomes and nonpharmacologic approaches for reduction: an expert review. Am J Obstet Gynecol MFM. 2020;2:100229.
12. Chen C. Revision and validation of a scale to assess pregnancy stress. J Nurs Res. 2015;23(1):25–32. doi:10.1097/jnr.0000000000000047
13. Husain N, Cruickshank K, Husain M, Khan S, Tomenson B, Rahman A. Social stress and depression during pregnancy and in the postnatal period in British Pakistani mothers: a cohort study. J Affect Disord. 2012;140:268–276. doi:10.1016/j.jad.2012.02.009
14. Gao M, Hu J, Yang L, et al. Association of sleep quality during pregnancy with stress and depression: a prospective birth cohort study in China. BMC Pregnancy Child. 2019;19:444. doi:10.1186/s12884-019-2583-1
15. Mei X, Du P, Li Y, et al. Fear of childbirth and sleep quality among pregnant women: a generalized additive model and moderated mediation analysis. BMC Psychiatry. 2023;23:931. doi:10.1186/s12888-023-05435-y
16. Austin M. Marcé international society position statement on psychosocial assessment and depression screening in perinatal women. Best Pract Res Cl Ob. 2014;28:179–187. doi:10.1016/j.bpobgyn.2013.08.016
17. El-Den S, Pham L, Anderson I, et al. Perinatal depression screening: a systematic review of recommendations from member countries of the organisation for economic co-operation and development (OECD). Arch Women’s Mental Health. 2022;25:871–893. doi:10.1007/s00737-022-01249-1
18. Tang X, Lu Z, Hu D, Zhong X. Influencing factors for prenatal stress, anxiety and depression in early pregnancy among women in Chongqing, China. J Affect Disord. 2019;253:292–302. doi:10.1016/j.jad.2019.05.003
19. Farren J, Jalmbrant M, Falconieri N, et al. Differences in post-traumatic stress, anxiety and depression following miscarriage or ectopic pregnancy between women and their partners: multicenter prospective cohort study. Ultrasound Obst Gyn. 2021;57:141–148. doi:10.1002/uog.23147
20. Gokoel AR, Abdoel Wahid F, Zijlmans WC, et al. Influence of perceived stress on prenatal depression in Surinamese women enrolled in the CCREOH study. Reprod Health. 2021;18:136. doi:10.1186/s12978-021-01184-x
21. Okun ML, Kline C, Roberts JM, Wettlaufer B, Glover K, Hall MH. Prevalence of sleep deficiency in early gestation and its associations with stress and depressive symptoms. J Women’s Health. 2013;22(12):1028–1037. doi:10.1089/jwh.2013.4331
22. Bao C, Wang Y, Le T, et al. Relationship between depressive symptoms and sleep quality and cognitive inhibition ability in prenatal pregnant women. BMC Psychiatry. 2023;23:522. doi:10.1186/s12888-023-04976-6
23. Zhang L, Wang L, Cui S, Yuan Q, Huang C, Zhou X. Prenatal depression in women in the third trimester: prevalence, predictive factors, and relationship with maternal-fetal attachment. Front Public Health. 2021;8: 602005.
24. Battulga B, Benjamin MR, Chen H, Bat-Enkh E. The impact of social support and pregnancy on subjective well-being: a systematic review. Front Psychol. 2021;12:710858.
25. Sun S, An S. Associations between patterns of social support and perinatal mental health among Chinese mother: the mediating role of social trust. J Psychosom Obstet Gynaecol. 2024;45(1). doi:10.1080/0167482X.2024.2325451
26. Ailshire JA, Burgard SA. Family relationships and troubled sleep among U.S. Adults: examining the influences of contact frequency and relationship quality. J Health Soc Behav. 2012;53:248–262. doi:10.1177/0022146512446642
27. Bouzari Z, Abdi S, Faramarzi M, Chehrazi M, Esfandyari M, Darzipoor Baboli M. Family functioning as a predictor of maternal mental health during pregnancy. Women’s Reprod Health. 2022;2022:1–14.
28. Qi W, Liu Y, Lv H, et al. Effects of family relationship and social support on the mental health of Chinese postpartum women. BMC Pregnancy Child. 2022;22:65. doi:10.1186/s12884-022-04392-w
29. Pauley AM, Moore GA, Mama SK, Molenaar P, Symons Downs D. Associations between prenatal sleep and psychological health: a systematic review. J Clin Sleep Med. 2020;16(4):619–630. doi:10.5664/jcsm.8248
30. Lee MS, Lee JJ, Park S, Kim S, Lee H. Is social support associated with postpartum depression, anxiety and perceived stress among Korean women within the first year postpartum? J Psychosom Obstet Gynaecol. 2023;44(1):2231629. doi:10.1080/0167482X.2023.2231629
31. Wang D, Li YL, Qiu D, Xiao SY. Factors influencing paternal postpartum depression: a systematic review and meta-analysis. J Affect Disord. 2021;293:51–63. doi:10.1016/j.jad.2021.05.088
32. Faries DE, Obenchain R, Haro JM, Leon AC. Analysis of Observational Health Care Data Using SAS. SAS Institute; 2014.
33. Wang X, Ji X. Sample size estimation in clinical research: from randomized controlled trials to observational studies. CHEST. 2020;158:S12–20. doi:10.1016/j.chest.2020.03.010
34. Ma Z, Wang D, Chen X, et al. Network structure of insomnia and depressive symptoms among shift workers in China. Sleep Med. 2022;100:150–156. doi:10.1016/j.sleep.2022.08.010
35. Zimet G, Dahlem NW, Zimet S, Farley G. The Multidimensional Scale of Perceived Social Support. Us: Lawrence Erlbaum; 1988:30–41.
36. Kroenke K, Spitzer RL, Williams JBW. The patient health questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284–1292. doi:10.1097/01.MLR.0000093487.78664.3C
37. Hayes AF. Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. 2013.
38. Lu S, Wei F, Li G. The evolution of the concept of stress and the framework of the stress system. Cell Stress. 2021;5:76–85. doi:10.15698/cst2021.06.250
39. Guardino C, Dunkel Schetter C. Coping during pregnancy: a systematic review and recommendations. Health Psychol Rev. 2014;8:70–94. doi:10.1080/17437199.2012.752659
40. Flores-Kanter P, Moretti L, Medrano L. A narrative review of emotion regulation process in stress and recovery phases. Heliyon. 2021;7(6):e07218. doi:10.1016/j.heliyon.2021.e07218
41. Bekiros S, Jahanshahi H, Munoz-Pacheco J. A new buffering theory of social support and psychological stress. PLoS One. 2022;17:e0275364. doi:10.1371/journal.pone.0275364
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.