Back to Journals » Risk Management and Healthcare Policy » Volume 19
Family-Centered Psychosocial Interventions for Disaster-Affected Children Across Developmental Stages: A Scoping Review
Authors Rhamelani P ![]() , Cahaya AP
, Cahaya AP ![]() , Yunita S, Wijayanti R, Nirwana JP, Nasution N, Widiawati A
, Yunita S, Wijayanti R, Nirwana JP, Nasution N, Widiawati A ![]() , Oktaviani R, Sijabat YS, Febrian N
, Oktaviani R, Sijabat YS, Febrian N ![]() , Rahayu R, Rohnenti O, Priambodo AP
, Rahayu R, Rohnenti O, Priambodo AP ![]()
Received 7 May 2026
Accepted for publication 24 June 2026
Published 11 July 2026 Volume 2026:19 622846
DOI https://doi.org/10.2147/RMHP.S622846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Keon-Hyung Lee
Putri Rhamelani,1,* Annisa Putri Cahaya,1,* Sri Yunita,1,* Restu Wijayanti,1,* Jelita Puspa Nirwana,1,* Nando Nasution,1,* Aninda Widiawati,1,* Rima Oktaviani,1,* Yunihar Susilawaty Sijabat,1,* Nurul Febrian,1,* Rahayu Rahayu,1,* Onis Rohnenti,1,* Ayu Prawesti Priambodo2,*
1Master of Nursing Program, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Critical Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia
*These authors contributed equally to this work
Correspondence: Ayu Prawesti Priambodo, Email [email protected]
Abstract: Children are highly vulnerable in disaster settings due to developmental, physiological, and psychosocial limitations, increasing their risk of long-term mental health and psychosocial problems. Although disasters cause both physical and psychological consequences, psychosocial difficulties often persist longer and may hinder children’s developmental recovery. Therefore, family-centered psychosocial interventions are essential for post-disaster recovery. However, the integration of Family-Centered Care (FCC) principles into disaster mental health and psychosocial support systems remains fragmented and insufficiently tailored to children’s developmental stages. This scoping review mapped and synthesized evidence on family-centered psychosocial interventions for disaster-affected children across developmental stages. Following PRISMA-ScR guidelines, articles published between 2016 and 2026 were searched in PubMed, MEDLINE, Scopus, ScienceDirect, and SAGE. Studies were selected using PCC criteria (Population: children aged 0– 18 years; Concept: family-centered psychosocial interventions, including caregiver-mediated, play-based, cognitive-behavioral, resilience-building, and family support approaches; Context: disaster settings). Eleven studies (randomized controlled trials, quasi-experimental, and mixed-methods) from multiple countries were included. Findings indicate that interventions are developmentally differentiated and predominantly family-based; however, evidence remains limited for preschool children, adolescents, and long-term psychosocial outcomes. Play-based and dyadic caregiver child interventions were primarily used for younger children, while cognitive behavioral and resilience-focused approaches were more common among school-aged children and adolescents. Across studies, improvements in caregiver wellbeing and family functioning were consistently associated with better child emotional and behavioral outcomes, highlighting an interconnected recovery pathway across developmental stages. Family-centered psychosocial interventions should be tailored to developmental needs and strengthen caregiver wellbeing and family functioning. The findings support integrating family-centered approaches into disaster mental health systems to strengthen resilience and long-term recovery, particularly in disaster-prone and resource-limited settings.
Keywords: disaster, family-centered care, pediatrics, psychosocial interventions, resilience
Introduction
A disaster is an event or a series of events that threatens an disrupts the lives of communities, caused by natural, non-natural, or human factors, resulting in human casualties, environmental damage, property loss, and psychological impacts.1 Globally, literature classifies these crises into two main categories that both have massive destructive power on populations: natural disasters (such as earthquakes, tsunamis, and extreme climate events) and human-made/man-made disasters (such as armed conflicts, technological failures, and terrorism).2 The increasing frequency and intensity of disasters have become a major global public health and risk management concern, particularly for vulnerable populations such as children. A UNICEF report in 2023 estimates that more than 400 million children live in areas with extreme disaster vulnerability.3 In Indonesia, the National Disaster Management Agency (BNPB) also records thousands of disaster events annually, placing children as the population with the largest percentage of those affected.4 In the context of any form of disaster, children are not merely “miniature adults.” They constitute a highly vulnerable population anatomically, physiologically, and psychologically. Limited physical mobility to save themselves, high dependence on parental protection, and immature cognitive coping mechanisms put children at a much higher risk of physical morbidity and psychosocial trauma, including a high prevalence of Post-Traumatic Stress Disorder (PTSD) and depression, compared to the adult population when facing disaster agents.5
This vulnerability is further intensified by children’s ongoing developmental processes and limited capacity to understand and regulate traumatic experiences. Psychological trauma in children may persist long after physical recovery and contribute to long-term public health burdens, including impaired psychosocial functioning, educational disruption, and increased mental health service needs. These impacts vary across developmental stages: in early childhood, disasters may disrupt attachment and emotional security; in school-aged children, they may impair academic performance and social interactions; and in adolescents, who are in the stage of identity vs role confusion, disasters may trigger identity disturbances, social withdrawal, and prolonged mental health problems such as depression and anxiety.5,6
Understanding these developmental vulnerabilities highlights that children’s recovery cannot be addressed in isolation. Instead, the family serves as the primary system of emotional regulation and recovery and plays a critical role in strengthening community resilience and post-disaster recovery outcomes.7 However, despite the large number of children affected by disasters globally, psychosocial interventions remain largely generalized and often fail to adequately integrate the family as the primary support system.
These developmental vulnerabilities indicate that children’s post-disaster recovery is closely influenced by the family context in which they live and develop. Families provide emotional support and stability that facilitate children’s psychosocial recovery. This understanding is consistent with Family Systems Theory, which views individual wellbeing as inseparable from the functioning of the family unit. According to Family Systems Theory, disasters affect not only individual children but also caregiver wellbeing, parenting practices, family relationships, and communication patterns, which collectively influence children’s emotional responses and recovery trajectories following disaster exposure.8 Recent evidence suggests that family resources, social support, and family strengths contribute to better caregiver wellbeing and improved psychosocial outcomes among children.9
Children’s developmental stages may also influence both their psychosocial needs and the ways they respond to intervention. Preschool children often require emotional reassurance from caregivers and may benefit from play-based strategies that facilitate the expression of distress. School-aged children are generally more capable of participating in structured coping and resilience-building activities, while adolescents may benefit from approaches that address emotional regulation, identity development, family communication, and increasing autonomy. These developmental differences suggest that family-centered psychosocial interventions should be adapted to children’s cognitive, emotional, and social capacities to ensure effectiveness across developmental stages.
Parents play a critical role in minimizing the short- and long-term impacts of disasters on children. By providing emotional support, guidance, and preparedness education, parents help children adaptively respond to crisis situations.10 Within disaster and emergency healthcare settings, Family-Centered Care (FCC) has emerged as an important strategy to strengthen psychosocial support, improve continuity of care, and enhance adaptive coping among disaster-affected children. Previous studies have shown that parental involvement in psychosocial interventions improves emotional regulation, reduces trauma symptoms, and enhances resilience among children, supporting the view that strengthening caregiver capacity and family functioning indirectly improves child psychosocial outcomes through family support, communication, and coping processes.9,11
The implementation of FCC positions families as active partners in healthcare decision-making and psychosocial recovery, contributing to more responsive and developmentally appropriate disaster care services. This collaboration helps strengthen children’s resilience in facing disasters and supports the fulfillment of their holistic developmental needs after experiencing a disaster.12 Although psychosocial interventions are highly crucial, their implementation during the emergency response and recovery phases remains suboptimal. Despite strong evidence supporting Family-Centered Care (FCC) in routine clinical settings, its application in disaster contexts remains fragmented and inconsistently implemented. Most existing psychosocial interventions in disaster settings continue to adopt a one-size-fits-all approach, limiting the effectiveness of disaster mental health responses for children with diverse developmental needs.
The specific context of a disaster presents unique and complex challenges for FCC. During acute emergencies, healthcare systems and humanitarian responses typically prioritize physical triage, basic logistical needs (shelter and food), and infectious disease control, often sidelining structured mental health support. Furthermore, disasters frequently result in family separation, displacement, and severe concurrent trauma among parents. Implementing FCC becomes challenging when caregivers themselves experience psychological distress, caregiver burden, and resource scarcity. This concurrent parental trauma is a critical contextual barrier that is frequently overlooked in disaster management.13
Currently, previous studies have extensively explored general post-disaster mental health responses. For instance, systematic reviews have highlighted the utility of school-based mental health and psychosocial support interventions for children and adolescents, including those with specific developmental vulnerabilities in low- and middle-income countries.14 Other relevant studies have critically evaluated the limited empirical evidence surrounding the efficacy of Psychological First Aid (PFA) and mass trauma healing programs on general mental health and well-being.15 While these previous studies provide valuable insights into pediatric psychosocial support, they predominantly reflect a one-size-fits-all approach. Furthermore, these approaches overlook the specific psychosocial needs associated with children’s developmental stages, resulting in interventions that are not developmentally appropriate or optimally effective.6,15
To overcome these barriers, FCC-based psychosocial interventions tailored to children’s developmental stages serve as a strategic solution. Several previous studies indicate that parent-involved interventions, such as emotion regulation psychoeducation for mothers of preschool children or family-based cognitive behavioral therapy for adolescents, are significantly more effective in reducing PTSD scores and accelerating resilience compared to individual interventions.16 Aligning interventions with children’s developmental tasks ensures that the methods used, whether play therapy for preschoolers or structured discussions for adolescents, can be cognitively accepted and processed by the child together with their family.
Although the literature on the importance of Family-Centered Care (FCC) and the impacts of disasters on children is growing, there remains a critical gap in systematically mapping and synthesizing FCC-based psychosocial interventions that are explicitly tailored across different developmental stages. Previous reviews have examined psychosocial interventions for disaster-affected children, school-based mental health programs, or family involvement in child mental health recovery; however, none have synthesized family-centered psychosocial interventions across developmental stages in disaster contexts. Consequently, evidence remains fragmented, limiting the development of targeted and developmentally appropriate psychosocial interventions. Therefore, this scoping review aims to systematically map and synthesize the existing evidence on family-centered psychosocial interventions for disaster-affected children across developmental stages, with particular attention to implications for disaster preparedness, psychosocial risk management, and child-centered healthcare practice.
Methods
Study Design
This study used a scoping review research design that maps various relevant research findings.17 This review was conducted following the methodological framework proposed by Arksey & O’malley (2005),18 further refined by the Joanna Briggs Institute (JBI), and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR).19 The article review process is carried out through various stages including identifying research questions, formulating keywords for the article search process, determining inclusion and exclusion criteria, identifying various sources of information, selecting relevant literature that meets the criteria, extracting and mapping results from selected articles, and compiling a report on the results of the article analysis. The primary research question guiding this review was: “What are the characteristics and effectiveness of family-centered psychosocial interventions for children across different developmental stages in disaster contexts?”
Eligibility Criteria
The research questions and eligibility criteria in this review use the PCC (Population, Concept, Context) approach as follows:
P (Population): children aged 0–18 years affected by disasters
C (Concept): family-centered psychosocial interventions involving parents
C (Context): disaster contexts, including natural disasters and human-made or social disasters
In the article search process, the authors applied selection criteria consisting of inclusion and exclusion criteria. Inclusion criteria for the population included articles with the subject of children aged 0–18 years affected by disasters or displacement; for the concept included articles that focused on discussing family-centered psychosocial interventions; for the context included articles on context of natural or human-made disasters; and original English-language research published between 2016–2026. Exclusion criteria for this review included articles with review study types and research protocols.
Data Collection and Analysis
Search Strategy
Based on the JBI methodology, there are three stages of the search strategy. In the first stage, researchers conducted an initial search limited to three databases (PubMed, Scopus, and ScienceDirect). In the second stage, researchers conducted a keyword search across all available databases. Each keyword was expanded using MeSH (Medical Subject Headings) terms and synonyms to find potentially all relevant articles using the Boolean operators “AND” and “OR” on each syllable. An example of the PubMed search string used was: (vulnerable pediatric populations OR pediatrics OR infant OR child OR adolescent) AND (family centered psychosocial intervention OR psychosocial interventions) AND (disaster situations across developmental stages OR disasters OR disaster nursing OR natural disasters OR child development). A simplified Boolean search strategy was also applied using key terms such as: (“family-centered care” OR “family intervention”) AND “psychosocial support” AND “disaster” AND “children”. The literature used in this review was obtained from these primary databases: PubMed/MEDLINE, Scopus, ScienceDirect, and SAGE. The last search was conducted on April 5, 2026.
The resulting inclusion and exclusion criteria were applied to the article search process. The authors used structured queries and specific search parameters to search literature databases such as Scopus, PubMed/MEDLINE as well as publisher platforms such as Sage Journals and ScienceDirect. All identified articles were independently screened by two reviewers based on titles and abstracts for relevance to the research objectives. Any disagreements between reviewers were resolved through discussion or consultation with a third reviewer. In the third stage, researchers conducted a bibliography search of the found articles for additional references.
Study Selection
After the literature search was completed, all articles found were selected based on the established inclusion and exclusion criteria. The literature selection and screening process in this review is presented in the PRISMA-ScR flowchart (Figure 1).19 During the identification stage, 2,722 records were retrieved from PubMed/MEDLINE, Scopus, ScienceDirect, and SAGE databases. After removing 660 duplicate records, 2,062 articles underwent title and abstract screening. During the eligibility stage, 171 full-text articles were assessed against the PCC-based inclusion and exclusion criteria. Of these, 160 articles were excluded because of unsuitable study designs (n=32), non-child populations (n=71), or lack of focus on family-centered psychosocial interventions in disaster settings (n=57). Finally, 11 studies met all eligibility criteria and were included in the review.
The screening process involved duplicate removal, title and abstract screening, and full-text eligibility assessment. Articles that did not meet the predefined PCC-based criteria were excluded at each stage of the review process. All articles obtained from the various databases used were then screened through title, abstract, and full-text review to ensure their suitability to the focus and objectives of this review. Articles that were irrelevant and did not meet the inclusion criteria were excluded from further analysis. In line with scoping review methodology, critical appraisal of included studies was not conducted, as the aim of this review was to map the existing evidence rather than to assess methodological quality.
Data Extraction and Analysis
In this review, the authors analyzed 11 articles that met the established criteria. The extraction and analysis of articles in this review were conducted using a matrix table that included information on the author’s name, year of article, country, research purposes, sample, study design, family-centered psychosocial interventions (type of intervention, description, outcomes), and results. Data charting was performed by one author using a standardized extraction matrix and independently checked by a second reviewer to ensure accuracy and consistency. All articles reviewed were original research, observational or exploratory studies, and development studies.
This review ensured that all research articles reviewed were relevant and supported the review’s objective, which was to map, identify, and analyze the available literature on family-centered psychosocial interventions for vulnerable child populations in disaster situations, highlighting the appropriateness of the interventions to the child’s developmental stages. Developmental stages were categorized based on standard pediatric age group classifications. When studies included broader age ranges spanning multiple developmental stages, classification was based on the predominant age group or as reported in the original study. The authors conducted data analysis through a process of identifying findings, which were then presented in a matrix table Next, the authors compiled findings on family-centered interventions to improve children’s psychosocial well-being in disaster situations according to the child’s developmental stage.
Results
Study Selection
The initial literature search process began with the identification of articles from several databases, resulting in a total of 2,722 articles. The article selection stage was visually illustrated using a PRISMA 2020 flow diagram presented as a figure (Figure 1). Following title and abstract screening, 171 articles were retained for full-text eligibility assessment. The inclusion and exclusion criteria were then applied in the full-text screening stage, resulting in 11 articles that met the eligibility criteria and were included in this review (Table 1).
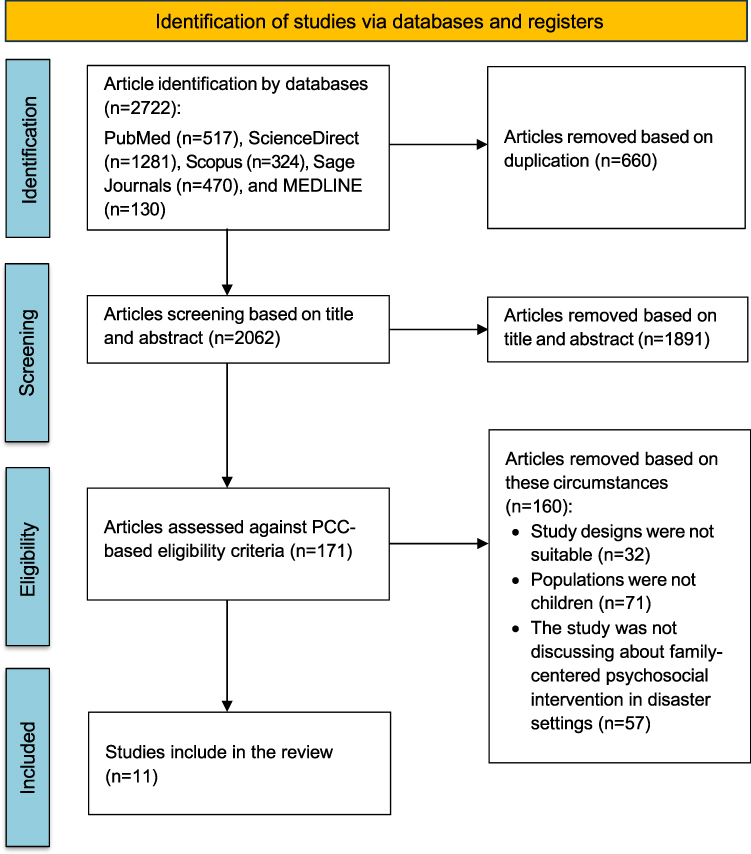 |
Figure 1 PRISMA-ScR Flow Diagram of Study Identification, Screening, Eligibility Assessment, and Inclusion Process. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM et al The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372: n71. Creative Commons.20. |
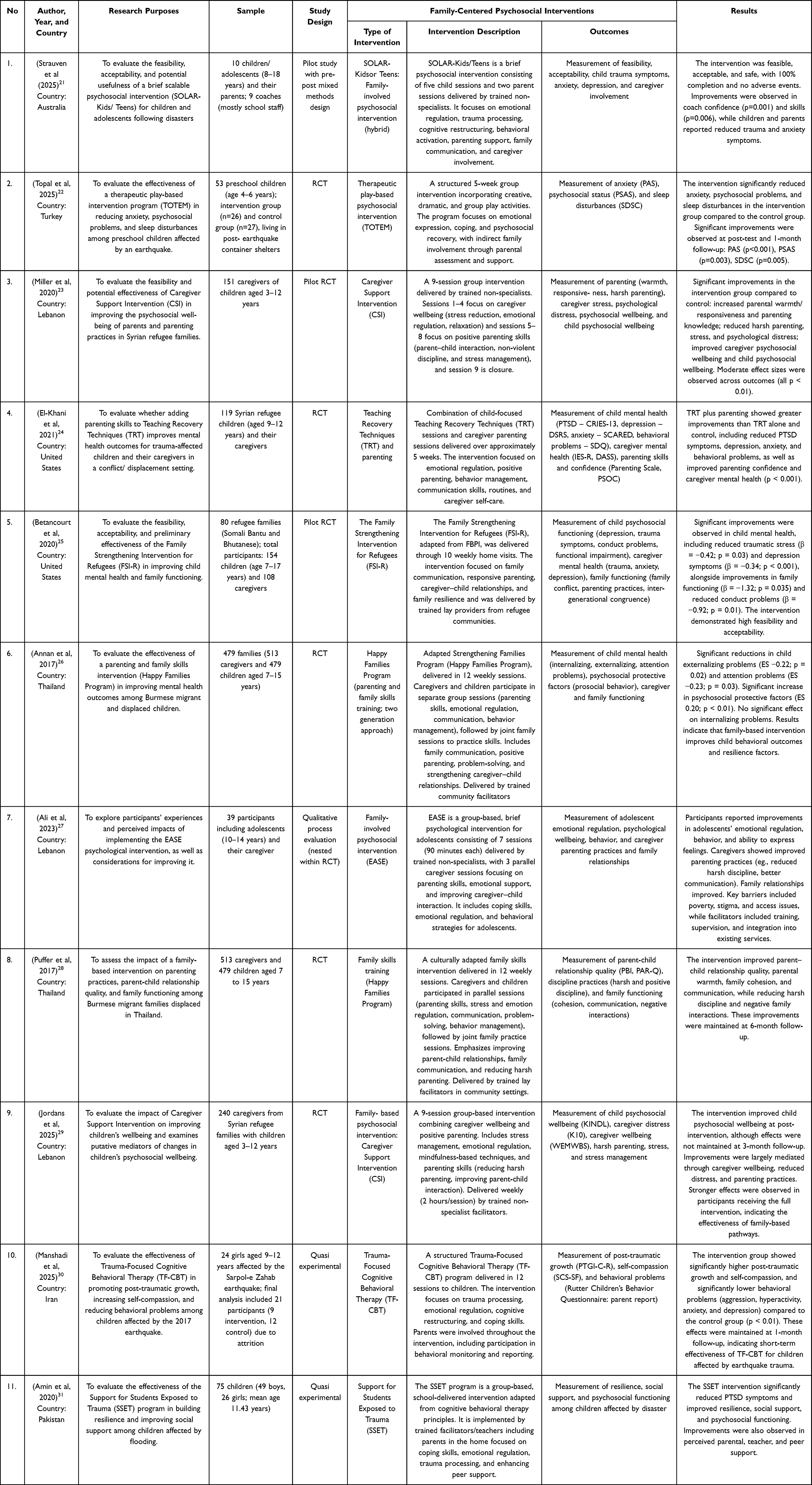 |
Table 1 Results of Article Analysis |
Study Characteristic
Of the 11 articles included in this review, the majority were quantitative experimental studies, comprising 5 randomized controlled trials (RCTs) and 2 pilot RCTs. In addition, 2 quasi-experimental studies, 1 qualitative study, and 1 mixed-methods study were identified. Most studies were conducted in low- and middle-income countries and humanitarian settings, reflecting the growing global concern regarding psychosocial risk management among vulnerable pediatric populations affected by disasters and displacement, including Lebanon (n=3), Thailand (n=2), the United States (n=2), Australia (n=1), Turkey (n=1), Iran (n=1), and Pakistan (n=1), as summarized in Table 1, which details study characteristics including country of origin, disaster type, and intervention characteristics.
The study populations mainly consisted of children affected by disasters and their caregivers. Across the included studies, participants involved children and adolescents (aged approximately 3–18 years) as well as parents or caregivers from disaster-affected or refugee populations. The largest sample size was reported in the study by Annan et al (2017), which included 479 families (513 caregivers and 479 children), while the smallest sample size was found in the study by Strauven et al (2025), involving 10 children and their parents Overall, the included studies demonstrate a predominance of family-based interventions that simultaneously target child psychosocial recovery and caregiver wellbeing, highlighting the importance of family systems in disaster mental health responses.
Thematic Synthesis of Family-Centered Psychosocial Interventions Across Developmental Stages
Eleven studies examined family-centered psychosocial interventions across different developmental stages and types of disasters. A detailed mapping of interventions by country, disaster type, and developmental stage (infants, preschool, school-age children, and adolescents) is presented in Tables 2 and 3. Overall, most interventions were implemented across mixed-age populations rather than being developmentally tailored, indicating a persistent gap in developmentally specific psychosocial strategies within disaster response systems.
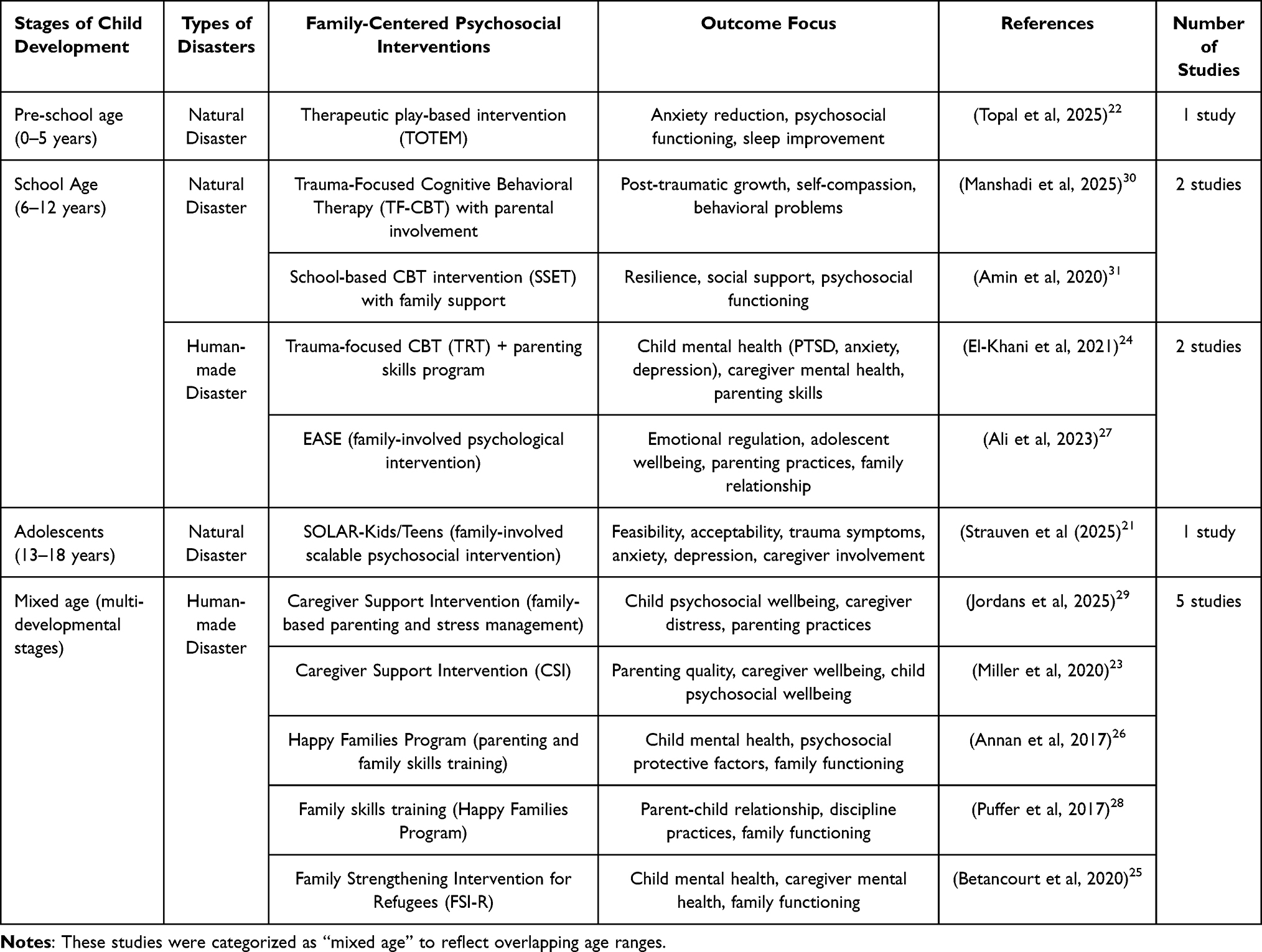 |
Table 2 Mapping of Family-Centered Psychosocial Interventions for Pediatric in Disaster Situations |
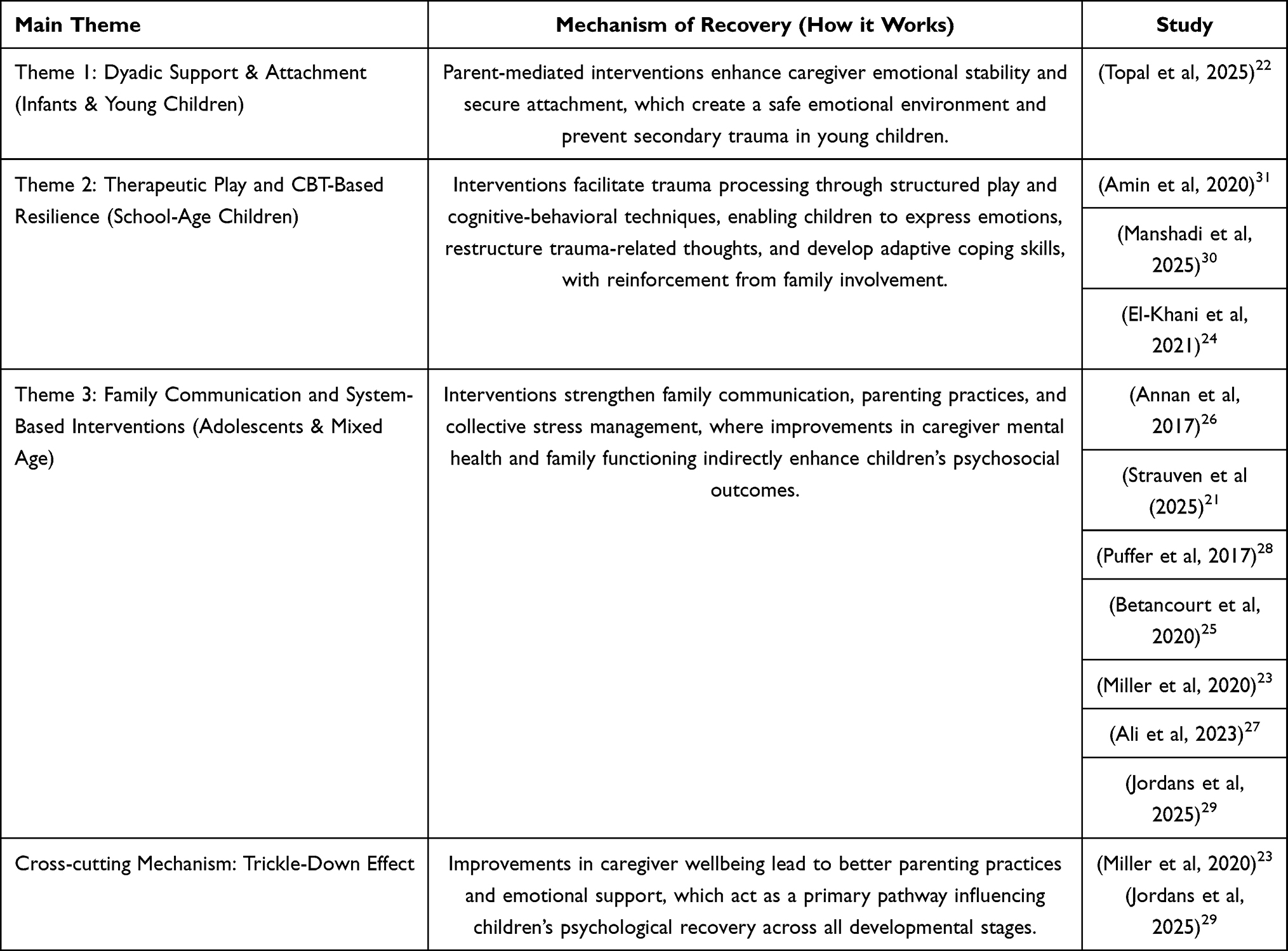 |
Table 3 Thematic Synthesis |
Theme 1: Dyadic Support in Infants and Young Children
Interventions targeting infants and young children are predominantly parent-mediated, as children in this developmental stage have limited verbal and cognitive capacities to process trauma independently. Interventions for infants and young children primarily utilize structured play to facilitate emotional expression. These interventions primarily operate by strengthening caregiver–child attachment, emotional regulation, and perceived safety, which are critical protective factors in post-disaster psychosocial recovery. For instance, the therapeutic play-based intervention (TOTEM) utilizes structured play to facilitate emotional expression, significantly reducing anxiety, psychosocial problems, and sleep disturbances.22 The limited number of studies targeting infants and young children indicates an important evidence gap in early childhood disaster mental health interventions and suggests insufficient prioritization of developmentally appropriate psychosocial care within disaster preparedness and response frameworks.
Theme 2: Therapeutic Play and Resilience in School-Age Children
For school-age children (6–12 years), family-centered psychosocial interventions emphasize therapeutic play and structured resilience-building programs. At this stage, children are better able to express emotions and engage in guided activities that facilitate trauma processing. Interventions such as Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) and Support for Students Exposed to Trauma (SSET) demonstrate positive outcomes, particularly when parents are actively involved in reinforcing coping strategies at home.30,31 These interventions demonstrated improvements in post-traumatic growth, resilience, behavioral adjustment, and psychosocial functioning, suggesting their potential contribution to strengthening long-term child mental health outcomes in disaster-affected communities. In human-made disaster contexts, only a small number of interventions specifically focused on this age group, including trauma-focused interventions combined with parenting skills.24 These interventions facilitate trauma processing through cognitive restructuring, emotional expression, and family reinforcement mechanisms, thereby supporting adaptive coping within the broader family and community environment.
Theme 3: Family Communication and Cognitive Behavioral Approaches in Adolescents
Among adolescents (13–18 years), family-centered interventions focus on improving communication patterns and collective stress management within the family while supporting the adolescent’s need for autonomy. Cognitive Behavioral Therapy (CBT)-based approaches, such as SOLAR-Kids/Teens, are particularly effective in addressing trauma symptoms, emotional regulation, and depressive symptoms.21 These interventions operate through family-system mechanisms in which improvements in caregiver wellbeing, parenting practices, and family communication collectively strengthen psychosocial resilience and recovery among adolescents.
A substantial proportion of studies involved mixed-age populations and were therefore categorized as multi-developmental stage interventions. These studies were predominantly conducted in human-made disaster contexts and included caregiver-focused and family-based programs such as the Caregiver Support Intervention (CSI), Happy Families Program, family skills training interventions, and the Family Strengthening Intervention for Refugees (FSI-R).23,25–29 These interventions emphasized parenting practices, caregiver wellbeing, stress management, and family functioning as integral components of disaster mental health support, reflecting the growing recognition of family-centered approaches within humanitarian and public health responses. These findings highlight that, although adolescents seek autonomy, supportive family communication remains essential in promoting adaptive coping and psychological recovery.
Across all themes, family-centered psychosocial interventions consistently addressed interconnected child and caregiver outcomes, reinforcing the importance of family systems in disaster mental health recovery and psychosocial risk reduction. Common outcome domains include child mental health (such as anxiety, PTSD, and depression), psychosocial functioning, resilience, and behavioral outcomes, alongside caregiver-related outcomes such as stress, wellbeing, parenting practices, and family relationships. Importantly, several studies demonstrated a “trickle-down effect,” in which improvements in caregiver wellbeing were associated with subsequent improvements in children’s psychosocial outcomes.23,29 Across developmental stages, this pattern suggests that family-centered interventions may exert their effects through shared family processes, including caregiver support, family communication, emotional regulation, and strengthened family functioning.
These findings suggest that caregiver wellbeing may function as a central mechanism influencing child recovery outcomes, underscoring the interdependent nature of psychosocial resilience within family systems. Collectively, the findings indicate that although family-centered psychosocial interventions demonstrate promising outcomes, substantial gaps remain in the availability of developmentally tailored interventions, implementation consistency, and integration into disaster preparedness and mental health response systems. Taken together, these findings informed the development of a conceptual framework synthesizing the pathways through which family-centered interventions support psychosocial recovery in disaster-affected children and adolescents.
Conceptual Framework of Family-Centered Psychosocial Recovery
The thematic synthesis further revealed a conceptual pathway linking caregiver well-being, parenting practices, family functioning, and child psychosocial recovery across developmental stages (Figure 2). Family-centered psychosocial interventions appeared to enhance caregiver emotional well-being, stress management, and coping capacities, which subsequently strengthened parenting practices and overall family functioning. These family-level improvements were associated with positive child outcomes, including reduced trauma-related symptoms, improved emotional regulation, enhanced resilience, and better psychosocial functioning. Across the included studies, this mechanism was reflected in a cross-cutting “trickle-down effect,” whereby improvements in caregiver well-being indirectly promoted child psychosocial recovery through strengthened family processes. The conceptual framework synthesizes these relationships and highlights potential pathways through which family-centered interventions support psychosocial recovery in disaster-affected children and adolescents.
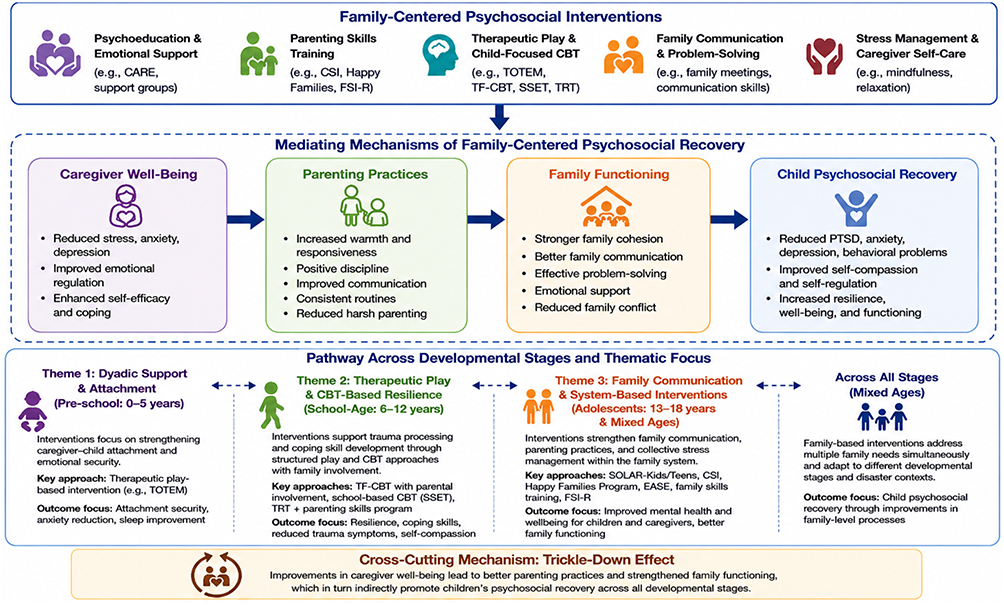 |
Figure 2 Conceptual Framework of Family-Centered Psychosocial Recovery Across Developmental Stages in Disaster Settings. Notes: Solid arrows represent the proposed directional pathway linking family-centered psychosocial interventions to child psychosocial recovery through caregiver well-being, parenting practices, and family functioning. Dotted double-headed arrows represent reciprocal relationships and thematic overlap across developmental stages and intervention approaches. |
Discussion
This scoping review highlights that family-centered psychosocial interventions are not merely an adjunct to disaster response but serve as a central component of psychosocial recovery and resilience-building among disaster-affected children. Across the eleven studies analyzed, a decisive theme emerges indicating that a child’s psychological recovery is inextricably linked to the stability and involvement of their primary caregivers. The findings suggest that developmentally tailored interventions are associated with more favorable psychosocial outcomes among disaster-affected children. For instance, the use of therapeutic play in the TOTEM program illustrates how vital it is to adapt to the limited verbal and cognitive capacities of preschool-aged children.22 This approach is effective because young children primarily process traumatic experiences through symbolic play rather than verbal expression, allowing them to externalize fear, regain a sense of control, and reconstruct meaning in a developmentally appropriate way.
In contrast, for school-aged children, structured programs such as TF-CBT and SSET demonstrate that involving parents as active co-therapists helps maintain long-term emotional regulation.30,31 This is because school-age children and adolescents have more advanced cognitive capacities, enabling them to engage in cognitive restructuring, trauma processing, and reflective thinking, which are core components of cognitive-behavioral approaches. Parental involvement further reinforces these skills in daily contexts. Broader family-based interventions, such as FSI-R, were typically applied across mixed-age populations, reflecting their focus on strengthening overall family functioning rather than targeting specific developmental stages.
Furthermore, the evidence underscores a critical “trickle-down effect” within the family system, where children’s psychological recovery is strongly dependent on the mental health and emotional stability of their caregivers. As evidenced by Jordans et al (2025) through the Caregiver Support Intervention (CSI), reducing caregiver distress directly leads to improvements in children’s behavioral and emotional outcomes. This indicates that trauma is not experienced in isolation, but within an interconnected family system in which caregiver wellbeing shapes the child’s recovery environment. Therefore, disaster mental health responses should move beyond child-focused models and adopt family-centered approaches that position the family as an integrated unit within psychosocial recovery systems. For healthcare professionals and disaster response teams, these findings emphasize the importance of system-oriented interventions that simultaneously support both children and caregivers.
Family-centered interventions appear applicable across diverse disaster and humanitarian contexts.21 This review highlights the “trickle-down effect” as a central mechanism through which caregiver wellbeing influences child recovery within an interconnected family system. Family-centered psychosocial interventions may be effective because they address not only children’s trauma symptoms but also the caregiver-child relationship, which serves as the primary context for emotional regulation, attachment, coping, and psychosocial development. By simultaneously strengthening caregiver wellbeing and family functioning, these interventions create supportive environments that facilitate children’s recovery across developmental stages. Consistent with Family Systems Theory, disasters disrupt family functioning as a whole, and recovery is facilitated when interventions strengthen caregiver support, attachment, communication, and coping capacities.32
An important contribution of this review is the identification of family-centered interventions as mechanisms not only for short-term psychosocial recovery but also for the development of long-term family resilience. Psychosocial recovery in the short term can be observed through reductions in anxiety, PTSD symptoms, emotional distress, behavioral problems, sleep disturbances, and social withdrawal, as reported across several interventions included in this review. However, the longer-term significance of these interventions lies in their ability to strengthen family resilience capacities, namely the ability of family systems to adapt, recover, and maintain functional relationships when confronted with future adversity.33 Examples identified in the reviewed studies include improved parent-child communication, increased parental warmth and responsiveness, reduced family conflict, enhanced emotional support within households, strengthened problem-solving abilities, and more effective collective coping strategies. These family-level changes create a protective environment that extends beyond the immediate disaster recovery period and may buffer children against future psychological stressors.
The findings also indicate that improvements in communication and family functioning may indirectly accelerate children’s psychosocial recovery. Communication serves as a critical mechanism through which caregivers recognize children’s emotional needs, validate their experiences, and provide reassurance following traumatic events.34 Positive family functioning, including family cohesion, emotional connectedness, supportive parenting practices, and shared problem-solving, may further enhance children’s sense of safety and predictability after disasters, thereby facilitating adaptive coping and psychosocial recovery.35 Taken together, these interpretations should be considered alongside several limitations of the present review, including restriction to English-language publications, the absence of formal critical appraisal inherent to scoping review methodology, and the predominance of short-term outcome measures across included studies, which are further elaborated in the Limitations of the Review section.
These findings further suggest that the effectiveness of family-centered interventions is closely linked to developmental processes. Younger children rely heavily on caregivers for emotional co-regulation and a sense of safety, whereas school-aged children and adolescents increasingly benefit from family communication, guidance, and collaborative coping. Consequently, family-centered care may support psychosocial recovery through different mechanisms across developmental stages while maintaining the family as the central recovery system.
Main Findings
The literature mapping in this scoping review confirms that family involvement is not merely a supporting factor, but an essential component determining the success of psychosocial interventions for children affected by disasters. These findings reinforce the conceptualization of families as active therapeutic agents within disaster mental health interventions, rather than passive recipients of support. Programs such as SOLAR-Kids/Teens,21 and Teaching Recovery Techniques (TRT) combined with parenting programs,24 systematically involve caregivers to enhance emotional regulation skills and behavioral support. These findings suggest that caregiver involvement functions not merely as an adjunct component of intervention delivery but as an active therapeutic mechanism that reinforces children’s coping skills and emotional recovery beyond formal intervention sessions. Interventions such as the Caregiver Support Intervention (CSI) further demonstrate that improvements in caregiver well-being are strongly associated with better child mental health outcomes, highlighting the central role of the family as a pathway of recovery.23,29
The findings also highlight the importance of adapting interventions to the child’s developmental stage, although important disparities remain in the availability of developmentally tailored evidence across age groups. Effective interventions are those aligned with how children process trauma, ranging from therapeutic play for preschool-aged children, such as the TOTEM program,22 to cognitive-behavioral approaches such as Trauma-Focused Cognitive Behavioral Therapy (TF-CBT),30 and school-based Support for Students Exposed to Trauma (SSET) for school-age children.31 For adolescents, communication-focused interventions such as SOLAR-Kids/Teens have been applied.21 However, most studies focus on school-age children, indicating a clear evidence gap for preschool and adolescent populations.36
Differences in intervention models further demonstrate variations in effectiveness and scope. School-based interventions, such as SSET, offer important advantages in scalability, accessibility, and rapid deployment within disaster response systems.31 In contrast, family-based interventions such as the Family Strengthening Intervention for Refugees (FSI-R), and the Happy Families Program are more effective in strengthening long-term protective factors and caregiver–child relationships, although their implementation may require greater resource allocation, sustained engagement, and interprofessional coordination.25,28 While many interventions, including EASE, utilize non-specialist providers through task-shifting approaches, professional supervision remains essential to ensure intervention quality and fidelity.27 Task-shifting approaches involving nurses, teachers, community health workers, and trained volunteers may improve the scalability and accessibility of psychosocial interventions in resource-constrained disaster settings.
Family-centered interventions may contribute to both psychosocial recovery and long-term family resilience by strengthening communication, caregiver coping capacities, and family functioning.37 These family-level improvements create a supportive recovery environment that indirectly facilitates children’s psychosocial adjustment.11 In the longer term, strengthening family relationships, caregiver coping capacities, and adaptive communication patterns may enhance the family’s ability to respond to future stressors and adversity, thereby fostering resilience across developmental stages.38
This review also identifies several implementation and contextual challenges. Caregiver burden following disasters can limit participation in interventions, and some programs demonstrate limited sustainability over time, as observed in CSI.29 In addition, there is a lack of evidence from disaster-prone regions such as Southeast Asia, including Indonesia, as well as limited exploration of the role of nurses as key facilitators. These findings highlight the need for contextually adapted, sustainable, and developmentally appropriate psychosocial interventions that can be integrated into disaster preparedness and community mental health systems.
Developmental-Stage Differences
Family-based psychosocial interventions for vulnerable children in disaster situations show varying patterns depending on the child’s developmental stage, the type of disaster, and the focus of the targeted outcome. The family-centered approach consistently involves parents or caregivers as an integral part of the intervention, whether through parallel sessions, home visits, or strengthening parenting skills, thereby supporting child resilience while reducing caregiver distress.39 These intervention variations reflect the specific developmental needs of children at different ages, ranging from play-based approaches in early childhood to cognitive-behavioral approaches and family skills training in older children.40
In the preschool age group (0–5 years), only one study met the inclusion criteria, namely the therapeutic play-based intervention (TOTEM) for earthquake victims in Turkey.22 This intervention focused on creative, dramatic, and group play tailored to the developmental stages of Piaget, Vygotsky, and Bandura, with indirect family involvement through parental assessment and support. These findings suggest that play-based interventions may be particularly suitable for preschool children due to their limited verbal capacity and reliance on symbolic expression. These effects persisted for up to 1 month post-intervention. These findings support the importance of a simple and enjoyable play-based approach for young children who are not yet able to express emotions verbally, and emphasize the role of families in creating a safe environment for children after a natural disaster.
At the school-age stage (6–12 years), the largest number of studies (8 studies out of a total of 11 articles analyzed) were found, covering both natural and human-made disasters. For natural disasters, there are two main interventions: Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) with parent involvement,30 and school-based Support for Students Exposed to Trauma (SSET) with family support.31 Both interventions showed increases in post-traumatic growth, self-compassion, resilience, and social support, as well as decreases in behavioral problems, PTSD, and anxiety symptoms. Meanwhile, in human-made disasters (especially for Syrian and Burmese refugees), the dominant interventions are caregiver-based, such as Caregiver Support Intervention (CSI),23,29 Teaching Recovery Techniques (TRT) and parenting skills,24 Emotional Approach to Safety and Empowerment (EASE),27 and the Happy Families Program/family skills training.26,28 These interventions consistently improve children’s psychosocial well-being, such as reducing PTSD, depression, and externalizing problems. Furthermore, these interventions also improve parenting quality (decreased harsh parenting, increased warmth and communication), and family functioning (cohesion, reduced conflict). The mediating effect of caregiver distress and parenting practices reached 77% on improving children’s well-being, confirming the strong family-centered mechanism in this age group.29
In adolescents (13–18 years), two main studies were conducted: SOLAR-Kids/Teens for natural disasters,21 and Family Strengthening Intervention for Refugees (FSI-R) for refugees.25 Among adolescents, interventions primarily focused on strengthening family communication, resilience, and emotional regulation. These findings suggest that supportive family relationships remain essential during a developmental period characterized by increasing autonomy and identity formation.
The family-centered psychosocial intervention approach across developmental stages positions the family as the primary system in children’s psychological recovery.11 Disasters impact children not only individually but also affect their emotional interactions with parents and other family members. Recent research shows that interventions involving families can improve the quality of care, particularly in reducing symptoms of stress and trauma in children.39 Furthermore, according to research by Çimke et al (2024), the family-centered care approach also increases children’s sense of security and involvement in the recovery process because families are actively involved in decision-making.41
Overall, the mapping in Table 2 shows that family-centered interventions are mostly developed for school-age children and those affected by human-made disasters (especially refugees). Meanwhile, evidence for preschoolers and adolescents is still limited. The outcomes that are the primary focus of these articles consistently demonstrate improvements in children’s mental health, reduced caregiver distress, and strengthened family functioning, in line with the principles of family-centered care, which positions families as active partners in post-disaster recovery. These findings should be interpreted in light of several limitations, including language restrictions, the absence of formal quality appraisal, and the geographical concentration of studies in specific regions, which may affect the generalizability of the findings.
Implications for Nursing Practice
The findings of this scoping review highlight several practical implications for pediatric nurses in disaster settings. Nurses should adopt a FCC approach by not only addressing the child’s psychological needs but also actively assessing and supporting caregiver mental health as a primary pathway to improving child outcomes. Active assessment of caregiver mental health may include screening for psychological distress, anxiety, depression, traumatic stress, sleep problems, and caregiver burden. Support strategies may involve psychological first aid, psychoeducation, stress-management interventions, and referral to specialized mental health services when needed.42 For example, nurses may conduct caregiver screening, provide psychoeducation, facilitate stress-management activities, and refer caregivers requiring more specialized support.
However, the implementation of FCC in disaster settings in Indonesia may face several cultural and contextual barriers. Hierarchical family structures, common across many Indonesian communities, may discourage children from openly expressing emotions or participating in family decision-making, thereby limiting the effectiveness of communication-based interventions.43 Mental health stigma remains another significant barrier, as psychological distress is often perceived as a personal weakness or a matter to be managed privately within the family, which can reduce caregivers’ willingness to seek psychosocial support.44 Additionally, disaster response systems in Indonesia often prioritize basic needs (eg., food, shelter, and physical health), with limited integration of structured psychosocial and family-based approaches.
Overcrowded evacuation settings and limited trained personnel further constrain the delivery of developmentally tailored and family-centered interventions. Through a task-shifting approach, nurses can collaborate with teachers, community health workers, or local cadres to deliver family-centered interventions. For example, nurses can adapt therapeutic play interventions such as TOTEM into low-resource group activities using locally available materials while engaging caregivers through psychoeducation and positive parenting support to accommodate unstable disaster settings.22 Nurses can train community cadres or volunteers to facilitate these sessions while simultaneously engaging caregivers through brief psychoeducation on emotional support and positive parenting. This aligns with the principles of family-centered care, which position families as active partners in the child’s recovery process. These challenges highlight the need for culturally sensitive, community-based adaptation of FCC models in Indonesian disaster contexts. In practice, nurses can involve community leaders or respected family figures to facilitate communication with caregivers, helping to reduce resistance related to hierarchical family structures and mental health stigma.45
At the practice level, family-centered interventions emphasize that caregivers are not merely mediators but core therapeutic agents within an interconnected family system. Supporting caregiver mental health should therefore be considered a primary clinical target, as improvements at the caregiver level will cascade into better psychosocial outcomes for children. Nurses can implement brief caregiver support strategies in evacuation settings, such as group relaxation exercises, stress management sessions, and short psychoeducation modules on how to respond to children’s emotional distress. Evidence from interventions such as the Caregiver Support Intervention (CSI) demonstrates that improvements in caregiver wellbeing are closely associated with better child mental health outcomes, including reduced psychological distress and improved emotional regulation.29 This indicates that addressing caregiver stress is not only beneficial for adults but also serves as an indirect pathway for improving children’s recovery. However, limitations in sustainability remain a concern, as some studies report that these effects are not consistently maintained over time, highlighting the need for long-term follow-up and continuous support systems.
From an implementation perspective, scalable intervention models such as SOLAR-Kids/Teens offer promising opportunities, particularly in disaster contexts with limited mental health professionals. These programs can be delivered by trained non-specialists, increasing accessibility and feasibility in large-scale emergencies.21 However, these approaches tend to focus primarily on the individual child and may not sufficiently address the broader family environment. In contrast, family-based interventions demonstrate stronger effects on long-term outcomes, including improvements in family functioning, parent-child relationships, and emotional support systems.25 This suggests that integrating both approaches may provide a more comprehensive and sustainable strategy for psychosocial recovery.
In the context of disaster management systems, the effectiveness of psychosocial interventions is strongly influenced by contextual factors, including stigma, socioeconomic conditions, and cross-sectoral coordination.27 While integrating interventions into existing service systems can enhance relevance and sustainability, these same factors may also act as barriers to participation and program success. Therefore, disaster response strategies should adopt adaptive, context-sensitive approaches that combine family-centered care, scalable delivery models, and strong health system and policy-level support. At the practice level, nurses should integrate psychosocial care into daily routines in evacuation settings, such as incorporating play-based activities, caregiver check-ins, and family communication support into routine health assessments and outreach services. Overall, these findings highlight that pediatric nurses should implement developmentally appropriate, family-centered psychosocial interventions that integrate caregiver support, scalable delivery strategies, and continuous follow-up to ensure sustainable recovery outcomes in disaster-affected children.
Gaps and Future Research
Despite strong evidence supporting the effectiveness of family-centered psychosocial interventions, several critical gaps and limitations remain. One of the primary challenges lies in the feasibility of implementing family-based approaches in post-disaster contexts.46 Caregivers, who are expected to act as active partners in intervention delivery, often experience significant psychological distress, displacement, and economic hardship, which may limit their capacity to engage consistently in structured programs.23,24 In some cases, this may increase caregiver burden and contribute to higher attrition rates in interventions such as Teaching Recovery Techniques (TRT) and SOLAR-Kids/Teens.21,24 Furthermore, family-based interventions tend to be more resource-intensive than school-based models, requiring trained facilitators, sustained engagement, and ongoing supervision, which can be difficult to maintain in emergency settings.29
Another key limitation concerns the sustainability and consistency of intervention outcomes. Although programs such as the Caregiver Support Intervention (CSI) demonstrate significant short-term improvements in caregiver wellbeing and child psychosocial outcomes, these effects are not always sustained over time.29 Similarly, non-specialist delivery models such as the Family Strengthening Intervention for Refugees (FSI-R) and EASE have shown feasibility and acceptability, but concerns remain regarding variability in facilitator competence and the need for ongoing supervision to maintain intervention fidelity.25,27 These findings highlight the need for future research focusing on long-term follow-up, intervention sustainability, and implementation quality.
In addition, substantial heterogeneity exists in intervention components, delivery methods, and theoretical approaches. Trauma-focused interventions such as TF-CBT and TRT have demonstrated effectiveness in reducing PTSD symptoms; however, questions remain regarding their cultural adaptability across diverse settings.24,30 Likewise, play-based interventions such as TOTEM have shown positive outcomes for preschool children, but their scalability in resource-limited settings remains uncertain.22 Broader evidence also indicates variability in program content and outcomes, suggesting that while CBT-based approaches are effective, they may require adaptation when implemented in different cultural and contextual environments.36
The American Academy of Pediatrics emphasizes that children often experience long-term adjustment difficulties after disasters, including PTSD, depression, and anxiety, and that many do not access mental health services due to stigma or cost.47 This highlights the importance of integrating family-based approaches with professional triage systems. Similarly, evidence from China shows that survivors of man-made disasters often experience more complex and persistent psychological problems compared to natural disasters, including higher rates of PTSD, depression, and stigma.48 This underscores the need for culturally sensitive adaptations when interventions are applied in contexts of conflict or technological accidents.
A significant gap is also evident in the distribution of studies across developmental stages. Most interventions focus on school-aged children or mixed-age populations, while preschool children and adolescents remain underrepresented.31 This imbalance is concerning given the distinct developmental needs of these groups, where younger children require play-based and attachment-focused interventions, and adolescents require support related to identity development and emotional regulation.47 The lack of developmentally tailored interventions indicates that age-specific psychosocial needs are not being adequately addressed.
Geographical and contextual gaps further limit the generalizability of current evidence. Most studies have been conducted in Middle Eastern contexts, particularly among refugee populations, or in high-income countries, while evidence from disaster-prone regions such as Southeast Asia, including Indonesia, remains limited.36 This geographical imbalance raises important concerns regarding the cultural adaptability, contextual relevance, and transferability of existing intervention models. In addition, the role of nurses as key providers or facilitators of psychosocial interventions remains largely unexplored, despite their critical position within disaster response systems.
Finally, although both school-based and family-based interventions demonstrate distinct strengths, their integration remains underexplored. School-based models offer advantages in scalability and rapid access to children, whereas family-based interventions provide more sustained and relational benefits.26,28,31 However, current evidence suggests that neither approach alone is sufficient to address the complex and multidimensional needs of children affected by disasters. Future research should prioritize the development and evaluation of integrated, multi-level psychosocial intervention models that combine school, family, community, and healthcare system components while addressing sustainability, cultural adaptation, and implementation feasibility across diverse disaster settings.
Strengths of The Review
Regarding the merits of this review, the utilization of a rigorous PRISMA-ScR protocol ensures that the synthesized evidence meets high standards of methodological validity. One of the primary strengths is the comprehensive mapping of interventions across the entire pediatric age spectrum, providing practitioners with nuanced insights rather than a universal approach. By categorizing strategies based on developmental needs, including play-based models for toddlers and communication-focused programs for adolescents, this review offers a practical roadmap for healthcare providers. Moreover, the inclusion of studies from various global regions, such as Europe, the Middle East, and Asia, enhances the breadth of the findings and reflects the universal relevance of family-centered care in crisis settings.
Limitations of The Review
This scoping review has several limitations that should be considered when interpreting the findings. First, the literature search was restricted to articles published in English, which may have excluded relevant studies published in local languages, particularly from disaster-prone regions such as Southeast Asia. This language restriction introduces the potential for publication bias and may limit the comprehensiveness of the evidence base.
Second, in accordance with the methodological framework of scoping reviews, this study did not conduct a formal critical appraisal of the quality of included studies. As a result, the findings primarily reflect the breadth and mapping of available evidence rather than the methodological rigor of individual studies. Therefore, conclusions regarding the effectiveness of interventions should be interpreted with caution.
Additionally, the included studies showed geographical and contextual imbalances, with a predominance of research conducted in the Middle East and high-income countries, which may limit the generalizability of findings to other settings, including Indonesia. Most studies also focused on short-term outcomes, making it difficult to assess the long-term sustainability of intervention effects. Furthermore, limited evidence was available for specific vulnerable subgroups, such as children with disabilities or pre-existing mental health conditions.
Conclusions
In conclusion, this review confirms that family-centered psychosocial interventions are effective in supporting psychosocial recovery and strengthening resilience among disaster-affected children by actively engaging caregivers as key partners in the recovery process. The findings indicate that psychosocial interventions should be developmentally tailored, as children’s cognitive, emotional, and social needs vary substantially across developmental stages. By empowering caregivers and integrating them into the therapeutic process, these interventions improve family communication, caregiver wellbeing, emotional regulation, and adaptive coping, thereby creating a supportive recovery environment for children. Overall, the findings underscore that caregiver wellbeing and family functioning represent key mechanisms through which family-centered psychosocial interventions improve children’s emotional recovery, resilience, and psychosocial outcomes in disaster settings. An important advantage of family-centered interventions is their ability to simultaneously address child and caregiver needs, generating benefits that extend beyond short-term symptom reduction toward long-term family resilience and psychosocial adaptation.
Moving forward, disaster management policies should integrate family-centered psychosocial support into early disaster response phases and recovery frameworks by providing structured training and guidance for parents and caregivers immediately after the emergency phase, alongside physical, logistical, and emergency healthcare responses. Healthcare professionals, including pediatric nurses and mental health practitioners, should play an active role in implementing and advocating for developmentally appropriate family-centered psychosocial interventions within disaster response systems. Future research should prioritize the development and evaluation of culturally adapted, scalable, and sustainable family-centered psychosocial interventions, particularly in disaster-prone and resource-limited settings such as Indonesia.
Acknowledgments
This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/ B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Amelia M, Fitriyani N. Psychosocial-Based Trauma Recovery in Children After Flood Disasters. Jurnal Hawa. 2023;5(1):96–21.
2. Xie Y, Zhu X, Wang L, et al. A network meta-analysis of psychological interventions for children and adolescents after natural and man-made disasters. BMC Psychiatry. 2024;24(1):468. doi:10.1186/s12888-024-05924-8
3. UNICEF. Children Displaced in a Changing Climate, United Nations Children’s Fund (UNICEF). 2023.
4. BNPB. Indonesian Disaster Data for 2024. 2025.
5. Pfefferbaum B, Nitiéma P, Newman E. A meta-analysis of intervention effects on depression and/or anxiety in youth exposed to political violence or natural disasters. Child Youth Care Forum. 2019;48(4):449–477. doi:10.1007/s10566-019-09494-9
6. Danese A, Smith P, Chitsabesan P, Dubicka B. Child and adolescent mental health amidst emergencies and disasters. Br J Psychiatry. 2020;216(3):159–162. doi:10.1192/bjp.2019.244
7. Safitri M, Alnov KA, Apriansah E, Seftiyani E, Afriyanti D. The Impact of Disaster on Children’s Mental. Jurnal Hawa. 2024;6(2):196–202.
8. Gibson M, Johnson S, Field K. The Relationship Between Parent and Child Mental Health: Taking a Family Systems Perspective in Support Services. 2022.
9. Dunst CJ. Meta-analyses of the relationships between family systems practices, parents’ psychological health, and parenting quality. Int J Environ Res Public Health. 2023;20(18):6723. doi:10.3390/ijerph20186723
10. Rhamelani P, Rakhmawati W, Fitri SYR, Mujar NMM. Factors Associated with Parental Involvement in Efforts to Prevent Drug-Resistant Tuberculosis in Children: a Scoping Review. Infect Drug Resist. 2026;Volume 19:1–21. doi:10.2147/IDR.S573094
11. Prime H, Wade M, Browne DT. Pandemic-related disruption and positive adaptation: profiles of family function at the onset of the pandemic. Advers Resil Sci. 2022;3(4):321–333. doi:10.1007/s42844-022-00077-7
12. Rohmaniah R, Yudianto A, Ulfa AF. The Relationship between the Role of Parents in the Implementation of Family Centered Care (FCC) and the Anxiety Level of Preschool Children (3-6 Years) Who Experienced Hospitalization in the Children’s Ward of the Muslimat Hospital, Jombang. Educational Journal. 2026;1(2):247–260.
13. Panneer S, Kumar S, Raka K, Balu KRA, Rose GJS, Akkayasamy VS. Impact of Disaster on Children and the Need for Child Centric Disaster Risk Reduction. In: Child Centric Disaster Risk Reduction, Priorities, Preparedness and Resilience. Bloomsbury India; 2023:87–103.
14. de Lille MJA, da Silva RT, Smythe T. School-based mental health and psychosocial support interventions for children and adolescents with developmental disabilities in low-and middle-income countries: a systematic review. Tropical Medicine and International Health. 2025;30(8):763–781. doi:10.1111/tmi.70000
15. Hermosilla S, Forthal S, Sadowska K, Magill EB, Watson P, Pike KM. We need to build the evidence: a systematic review of psychological first aid on mental health and well-being. J Trauma Stress. 2023;36(1):5–16. doi:10.1002/jts.22888
16. Goodrum NM, Prinz RJ. Family-based prevention of child traumatic stress. Pediatr Clin North Am. 2022;69(4):633–644. doi:10.1016/j.pcl.2022.04.011
17. Peterson J, Pearce PF, Ferguson LA, Langford CA. Understanding scoping reviews: definition, purpose, and process. J Am Assoc Nurse Pract. 2017;29(1):12–16. PubMed PMID: 27245885. doi:10.1002/2327-6924.12380
18. Arksey H, O’malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
19. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and Explanation. Ann Intern Med. 2018;169(7):467–473. PubMed PMID: 30178033. doi:10.7326/M18-0850
20. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
21. Strauven S, Dennison MJ, O’donnell ML, et al. A pilot study of a brief and scalable psychosocial intervention for children and adolescents following disasters. Br J Clin Psychol. 2025;64(1):6–35. doi:10.1111/bjc.12484
22. Topal S, Çaka SY, Uysal G, Alabay E, Demir Y, Arslan SC. The effect of therapeutic play-based intervention programme applied to earthquake victim preschool children on psychosocial well-being: a randomised controlled trial. BMC Psychol. 2025;13(1):981. doi:10.1186/s40359-025-03317-4
23. Miller KE, Koppenol-Gonzalez GV, Arnous M, et al. Supporting Syrian families displaced by armed conflict: a pilot randomizedcontrolled trial of the Caregiver Support Intervention. Child Abuse Negl. 2020;106:104512. PubMed PMID: 32408022. doi:10.1016/j.chiabu.2020.104512
24. El-Khani A, Haar K, Stojanovic M, Maalouf W. Assessing the feasibility of providing a family skills intervention, “strong families”, for refugee families residing in reception centers in Serbia. Int J Environ Res Public Health. 2021;18(9):4530. doi:10.3390/ijerph18094530
25. Betancourt TS, Berent JM, Freeman J, et al. Family-Based Mental Health Promotion for Somali Bantu and Bhutanese Refugees:Feasibility and Acceptability Trial. J Adolesc Health. 2020;66(3):336–344. PubMed PMID: 31699604. doi:10.1016/j.jadohealth.2019.08.023
26. Annan J, Sim A, Puffer ES, Salhi C, Betancourt TS. Improving Mental Health Outcomes of Burmese Migrant and Displaced Children inThailand: a Community-Based Randomized Controlled Trial of a Parenting and Family Skills Intervention. Prev Sci. 2017;18(7):793–803. PubMed PMID: 27858282. doi:10.1007/s11121-016-0728-2
27. Ali R, Brown FL, Stevenson K, et al. Implementing a non-specialist delivered psychological intervention for young adolescents in a protracted refugee setting: a qualitative process evaluation in Lebanon. J Behav Health Serv Res. 2023;51(3):377. doi:10.1007/s11414-023-09870-3
28. Puffer ES, Annan J, Sim AL, Salhi C, Betancourt TS. The impact of a family skills training intervention among Burmese migrantfamilies in Thailand: a randomized controlled trial. PLoS One. 2017;12(3):e0172611. PubMed PMID: 28350809. doi:10.1371/journal.pone.0172611
29. Jordans MJD, Bakolis I, Arnous M, et al. Effectiveness of the caregiver support intervention on child psychosocialwellbeing among Syrian refugees in Lebanon: mediation and secondary analysis of a Randomized Controlled Trial. Child Abuse Negl. 2025;162(Pt 2):106335. PubMed PMID: 37400323. doi:10.1016/j.chiabu.2023.106335
30. Manshadi ZD, Doost HTN, Talebi H, Vostanis P. TF-CBT for child earthquake survivors: promoting self-compassion, PTG, and reducing behavioral problems. J Loss Trauma. 2025;30(2):218–241. doi:10.1080/15325024.2024.2396130
31. Amin R, Nadeem E, Iqbal K, Asadullah MA, Hussain B. Support for students exposed to trauma (SSET) program: an approach for building resilience and social support among flood-impacted children. School Ment Health. 2020;12(3):493–506. doi:10.1007/s12310-020-09373-y
32. Priest JB. The Science of Family Systems Theory: Foundations for Effective Clinical Practice. Routledge; 2025.
33. Cameranesi M, Theron L, Höltge J, Jefferies P, Ungar M. Understanding the mechanisms through which family risk affects adolescent mental health: a model of multisystemic resilience in context. Children. 2022;9(4):546. doi:10.3390/children9040546
34. Ye Y, Li Y, Jin S, et al. Family function and post-traumatic stress disorder in children and adolescents: a meta-analysis. Trauma Violence Abuse. 2023;24(5):3151–3169. doi:10.1177/15248380221126182
35. Arega NT. Mental health and psychosocial support interventions for children affected by armed conflict in low-and middle-income countries: a systematic review. Child Youth Care Forum. 2023;52(6):1431–1456. doi:10.1007/s10566-023-09741-0
36. Gibbs L, Marinkovic K, Nursey J, et al. Child and adolescent psychosocial support programs following natural disasters—A scoping review of emerging evidence. Curr Psychiatry Rep. 2021;23(12):82. doi:10.1007/s11920-021-01293-1
37. Shabahang R, Arena AS, Navis I, Kuhls D, Newton C, Burke RV. Factors associated with resilience in children during a disaster: a scoping review. Disaster Med Public Health Prep. 2025;19:e52. doi:10.1017/dmp.2024.341
38. Ivéus K, Holm M, Årestedt K, et al. The Family Talk Intervention Improves Family Communication and Psychosocial Health Among Families in Pediatric Palliative Care: a Pre-Post Evaluation Study. Children. 2026;13(4):471. doi:10.3390/children13040471
39. Akhtar TN, Maiorano N, Cosma A, Hadfield K. A review of early childhood psychosocial interventions following extreme weather events in low-and middle-income countries. Perspect Public Health. 2025;145(6):332–342. doi:10.1177/17579139251371589
40. Álvarez-Pérez Y, Duarte-Díaz A, Rivero-Santana A, et al. Effectiveness of psychological interventions for parents of children eligible for paediatric palliative care: a systematic review and meta-analysis. Front Psychol. 2026;17:1775937. doi:10.3389/fpsyg.2026.1775937
41. Çimke S, Gürkan DY, Polat S. Research on family-centered care in pediatric patients: a bibliometric analysis. J Pediatr Nurs. 2024;76:199–206. doi:10.1016/j.pedn.2024.02.017
42. Brymer M, Taylor M, Escudero P, et al. Psychological first aid for schools: field operations guide. Natl Child Traumatic Stress Netw. 2012;2012:1.
43. Riany YE, Haslam DM, Sanders M. Parental mood, parenting style and child emotional and behavioural adjustment: australia-Indonesia cross-cultural study. J Child Fam Stud. 2022;31(9):2331–2343. doi:10.1007/s10826-021-02137-5
44. Subu MA, Dias JM, Mottershead R, et al. Exploring mental health stigma among Indonesian healthcare students towards individuals with mental illnesses: a qualitative study. Int J Qual Stud Health Well-Being. 2024;19(1):2327103. doi:10.1080/17482631.2024.2327103
45. Kohrt BA, Ojagbemi A, Luitel NP, et al. An app-based WHO mental health guide for depression detection: a cluster randomized clinical trial. JAMA Network Open. 2025;8(5):e2512064. doi:10.1001/jamanetworkopen.2025.12064
46. Bunn M, Zolman N, Smith CP, et al. Family-based mental health interventions for refugees across the migration continuum: a systematic review. SSM-Mental Health. 2022;2:100153. doi:10.1016/j.ssmmh.2022.100153
47. Schonfeld DJ, Demaria T, Krug SE, et al. Providing psychosocial support to children and families in the aftermath of disasters and crises. Pediatrics. 2015;136(4):e1120–30. doi:10.1542/peds.2015-2861
48. Zhengkui L, Yue L, Richu W. Crisis intervention and psychological assistance after sudden man-made disasters. Bulletin of Chinese Academy of Sciences. 2017;32(2):166–174.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.