")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Family and Social Support Among Patients on Anti-Retroviral Therapy in West Wollega Zone Public Hospitals, Western Ethiopia: A Facility-Based Cross-Sectional Study
Authors Desalegn M , Gutama T, Merdassa E , Kejela G , Benti W
Received 5 February 2022
Accepted for publication 2 April 2022
Published 13 April 2022 Volume 2022:14 Pages 167—179
DOI https://doi.org/10.2147/HIV.S360431
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Markos Desalegn, Tokuma Gutama, Emiru Merdassa, Gemechu Kejela, Wase Benti
Department of Public Health, Wollega University, Nekemte Town, West Ethiopia
Correspondence: Markos Desalegn, Department of Public Health, Wollega University, Nekemte Town, West Ethiopia, Tel +251927619190, Email [email protected]
Background: Poor family and social support is a problem for patients taking antiretroviral therapy (ART), but it protects them against the negative consequences of stress, reducing morbidity and mortality among peoples living with human immunodeficiency virus (PLWHIV).
Objective: This study aimed to assess family and social support and the associated factors among patients on antiretroviral therapy in West Wollega Public Hospitals.
Methods: A facility-based cross-sectional study design was conducted among 329 respondents attending antiretroviral therapy (ARV) clinics in West Wollega Public Hospitals from September 1– 30, 2020. Data were collected by simple random sampling methods using an interviewer-administered questionnaire. Bivariate and multivariate logistic regression analysis was used. The strength and presence of statistical association were assessed using adjusted odds ratio with a 95% confidence interval.
Results: About 266 (66.4%) of the respondents had low family and social support. Being female sex [AOR (95% CI)=0.066 (0.013– 0.338)], failing to discuss with family or society [AOR (95% CI)=0.275 (0.100– 0.753)], lack of information on support [AOR (95% CI)=0.314 (0.104– 0.951)], and non-disclosure of HIV status to family [AOR (95% CI)=0.227 (0.084– 0.916)] were associated with family and social support.
Conclusion: In this study, family and social support to people living with HIV/AIDS is low. Being female sex, feelings of negative treatment, lack of discussion on support, lack of information about support, and failure to disclose HIV status were associated with low family and social support. Information, education, and communication should be intensified to increase the awareness of the community, family, and people living with HIV related to support for people living with HIV.
Keywords: family, social support, people living with HIV/AIDS
Introduction
Human immune deficiency virus/Acquired immune deficiency syndrome (HIV/AIDS) is one of the major global health burdens and has become the number one killer disease of human beings globally.1 Globally, 36.1 million [27.2–47.8 million] people were living with HIV, of these 1.7 million were children.1 African regions remain the most severely affected, with nearly two-thirds of the people living with HIV in the world.2,3 In Ethiopia, the prevalence of HIV/AIDS was estimated to be 0.9%, with a regional disparity ranging from 0.1% in Ethiopia Somali to 4.8% in Gambella.4
Social support is a type of social network in which all-around support is given to a recipient from different segments of society, including parents, relatives, and friends. It consists of emotional support, informational support, instrumental (tangible support), and appraisal support.5,6 Social support has a positive influence on HIV treatment, adherence, diagnosis disclosure, social isolation, immune functioning, and enhancing coping with the challenges, thereby improving quality-of-life.7,8 A study in Iran showed that information and personal motivation for people living with HIV had a proven advantage in reducing depression.9 In Ethiopia, studies have shown that a large proportion of people living with HIV/AIDS were experiencing stigma and discrimination, which ranged from 28.9% in Buta jira to 48.6% in Nekemte.10–13 Apart from this, the prevalence of depression among HIV/AIDS patients in Ethiopia was 38.93%.14 In the Oromia region, Nekemte town, the prevalence was 42.96,15 and in Jimma town 30.2%.16
The government of Ethiopia has taken several steps to increase accessibility to HIV care, treatment, and support for individuals living with HIV/AIDS. Furthermore, the national guidelines on HIV prevention, treatment, and care have identified social support as a key element of chronic care and support for people at risk of HIV infection or PLWHA.17 HIV/AIDS is a disease that is feared because of misinformation about the transmission routes.18 With only treatment services, we cannot attain the healthcare needs of patients living with HIV/AIDS, particularly challenging in developing countries where there is limited health facility or only a few trained healthcare providers.19 Therefore, provision of care, support, and treatment at the homes of those with HIV/AIDS is of paramount advantage.19 The methods of delivering social support needs to be focused, developed, and tested to improve the quality-of -life for PLWHA.20
Many studies were conducted in Ethiopia on the prevention, treatment, and care of HIV-positive patients, but few studies were conducted on the status of social support to people living with HIV in Ethiopia. Factors associated with social support in PLHA are not yet conducted in Ethiopia. The study aimed to assess the magnitude of social support and its associated factors among patients on ART in West Wollega Zone Public Hospitals, Ethiopia.
Methods
Study Area and Period
The study was conducted in West Wollega Zone Public Hospitals from September 1–30, 2020. There were 4,752 HIV positive patients ever started on ART, 2,000 currently on antiretroviral therapy (ART), and 233 new HIV infections in the Zone by the end of August 2019. West Wollega Zone has five governmental Hospitals, two NGO Hospitals, 67 Health Centers, and many medium clinics, primary clinics, drug stores, and drug vendors. Among these Health Facilities (HF), there were 25 health facilities providing ART services in the zone (of which there were four governmental Hospitals, two NGO Hospitals, and 19 public Health Centers).
Study Design and Population
A facility-based cross-sectional study design was used to assess family and social support to patients on ART in West Wollega Public Hospitals. The source population of this study was all patients on ART in West Wollega Public Hospitals, and PLWHA taking ART from the randomly selected hospitals in West Wollega were the study population of the study.
PLWHA on ART for at least 6 months or more before data collection, aged greater than or equal to 18 years and found in randomly selected Public Hospitals in West Wollega were included. Whereas, patients on ART who were seriously ill having auditory or visual problems, all to the extent of being unable to give a response to questions were excluded.
Sample Size Determination and Sampling Procedure
A single population proportion formula was considered to estimate sample size using the
where
n = sample size,
P = The expected proportion of low social support to HIV positive patients (54.35%),21
level of significance (α) =5%,
confidence level at 5% level of significance (95% CI)=Z 1-α/2=1.96,
non-response rate=10%, and
margin of error (d) =5%.
Based on the above assumptions and formula the maximum possible sample size was 381 and, considering a 5% non-response rate, the final possible sample size was 400.
But, since the total target population (patients on ART in West Wollega Zone Public Hospitals) was less than 10,000, finite population correction was used. Therefore

nf=333.
Where nf = final sample size,
no = sample size from infinite population, and
N = finite population size.
Therefore the final estimated sample size was 333.
A simple random sampling technique was used to select study participants. West Wollega has four Public hospitals providing ART services. Two hospitals were selected using the lottery method. The sample was proportionally allocated to the selected hospitals based on the number of PLWHA who were taking ART in the respective hospitals. Based on this, a sample size of 242 was assigned to Nejo Hospital and 91 was assigned to Mendi Hospital. The respondents were selected by a simple random sampling method using a computer-generated random number and patient medical code from the registration logbook was used as a sampling frame.
Data Collection Instruments and Procedure
A structured, interviewer-administered, closed-ended questionnaire was developed and used after an extensive literature review.5,13,22 Initially, the questionnaire was developed in English language, then translated to regional language (Afaan Oromo), and then translated back to English by English language experts to check the consistency. Three BSc holder health professionals, two data collectors, and one supervisor were recruited for data collection. The questionnaire consists of socio-demographic factors, family-related factors, individual-related factors, knowledge, and awareness related, and multi-dimensional scales of social support sections. To determine the status of the family and social support, the Multi-Dimensional Scale of Social Support (MDSS) having 12 (items) was used. The MDSS scale has three sub-scales to measures perception of social support; namely family sub-scale, friends sub-scale, and significant others sub-scale. In MDSS, the Likert scale with scores ranging from 1=strongly disagree to 5=strongly agree was used. Patients on ART were interviewed at the time of their monthly follow-up at their respective hospitals.
Data Quality Control and Assurance
Before the actual data collection, the questionnaire was pretested on 5% of patients on ART in Mendi Health Center to ensure that the data collectors were familiar with the tools; the respondents were able to understand the questions, wording, and logic and order the questions in a sensible way to the respondents. Amendments were made accordingly after the pretest. One-day training on the objective of the study, confidentiality of information, and interviewing techniques was given to data collectors. Every day, the completeness and consistency of the collected data were reviewed and checked by data collectors and investigators. A discussion was made with data collectors at the end of the day and in the morning; the corrective measure was taken in a timely manner so that completeness and consistency of the data were assured.
Study Variables
Dependent Variable
Family and social support to patients taking antiretroviral therapy.
Independent Variables
Socio-demographic factors: Age, sex, educational status, marital status, average monthly income, religion, ethnicity, and occupational status.
Individual related factors: Duration of HIV diagnosis, duration of ART initiation, year, substance use (any of alcohol or chat), ability to perform any income-generating activities, daily eating pattern, being a beneficiary of Community Based Health Insurance (CBHI), perceived stigma, presence of feeling helpless, hopeless and continuous disturbance, whether HCP help disclosure, and disclosure of HIV status to family or society.
Family/Household factors: Educational level of father, educational level of mother, family size, and discussion on support with family or society.
Awareness about support to PLWHA: Media use, use of telephone, needs of PLWHA, thinks support can improve the wellbeing of PLWHA, and ever got support-related information.
Operational Definitions
Multi-Dimensional Scales of perceived social support (MDSPSS):A type of measurement of support that has 12 items to measure the level of social support that will be provided by family, friends, and significant others.22
Family sub-scales of MDSS: Sub-scale of MDSPSS that measures the status of support delivery by the family as perceived by the patients on ART. This sub-scale has four items to assess the perception of family-related support.22
Friends sub-scale of MDPSS: Another sub-scale of MDSPSS that measures the status of support delivery by the family as perceived by the patients on ART. This sub-scale has four items to assess the perception of friends-related support.22
Significant others sub-scale of MDSS: The third sub-scale of MDSPSS measures the status of support delivery by any person special to the patients on ART. This sub-scale has four items to measure the perception of support from any person significant to the patients attending ART.22
Family and social support: Support that family and society will provide to HIV-positive patients to enhance the wellbeing of those patients.
Good social support: Scores to multidimensional social support scales that respond to receiving social support above the mean score.
Poor social support: Scores to multidimensional social support scales that respond to receiving social support below the mean score.
Patients on ART: People that are diagnosed and known to live with HIV in their blood detected by HIV test according to the national algorithm and are taking antiretroviral therapy.
Perceived social support: Refers to an individual’s perception that support would be available to them whenever needed from their family or society.
Data Processing and Analysis
The collected data were cleaned, edited, coded, and entered into epi-data Version 3.1 and then exported to SPSS (Statistical Package for Social Science) Version 24. The data was also explored again for inconsistencies and missing values. Descriptive statistics such as frequencies, proportions, percentages, as well as mean and standard deviation were used to present the data in narration and figures. The data was re-checked for more errors by running frequency distributions. To summarize the support to PLWHA in this study, the response to an MDSS-SOCIAL SUPPORT SCALE was re-coded into a dichotomous variable (1 or 0). Accordingly, participants responses to strongly disagree (values=1), disagree (values=2) and neutral (Values=3) were all recoded to zero (0); whereas agree (values=4) and strongly agree (values=5) were re-coded into one. Then, the recorded score of Family and Social Support (FSS) was computed again to obtain mean values of FSS. After computing, the mean values of FSS were calculated to be 27.94 (SD=±27.46) (possible scores=1–60). Finally, values less than or equal to mean values were considered to have had poor support and those values above mean values were considered to have had good support.22
All relevant residual analyses, such as tests for multi-collinearity, linearity, normality, and homoscedasticity, were checked. Chi-square test was used for group comparisons of dependent variables (FSS) against independent categorical variables (age group, income category, family factors, individual factors, knowledge related factors, etc.). A binary logistic regression model was used to identify the determinant factors. Variables in the bi-variate analysis having a p-value <0.2 were considered for multivariate analysis to adjust the confounders. The strength and presence of statistical association were assessed using Adjusted Odds Ratio (AOR) with a 95% confidence interval (CI). Variables with a p-value <0.05 in the final model were considered as statistically significant factors associated with support to patients on ART.
Results
Socio-Demographic and Family Related Characteristics of Patients Taking ART in West Wollega Zone Public Hospitals, West Ethiopia, 2020
Three hundred and twenty participants responded to the questionnaire, makinga response rate of 96.1%. The mean age of the respondents was 35.50±10.47 years. The majority of the study participants (112; 35%) were in the age range of 21–30 years. Regarding sex composition, 164 (51.3%) of the respondents were male (Table 1).
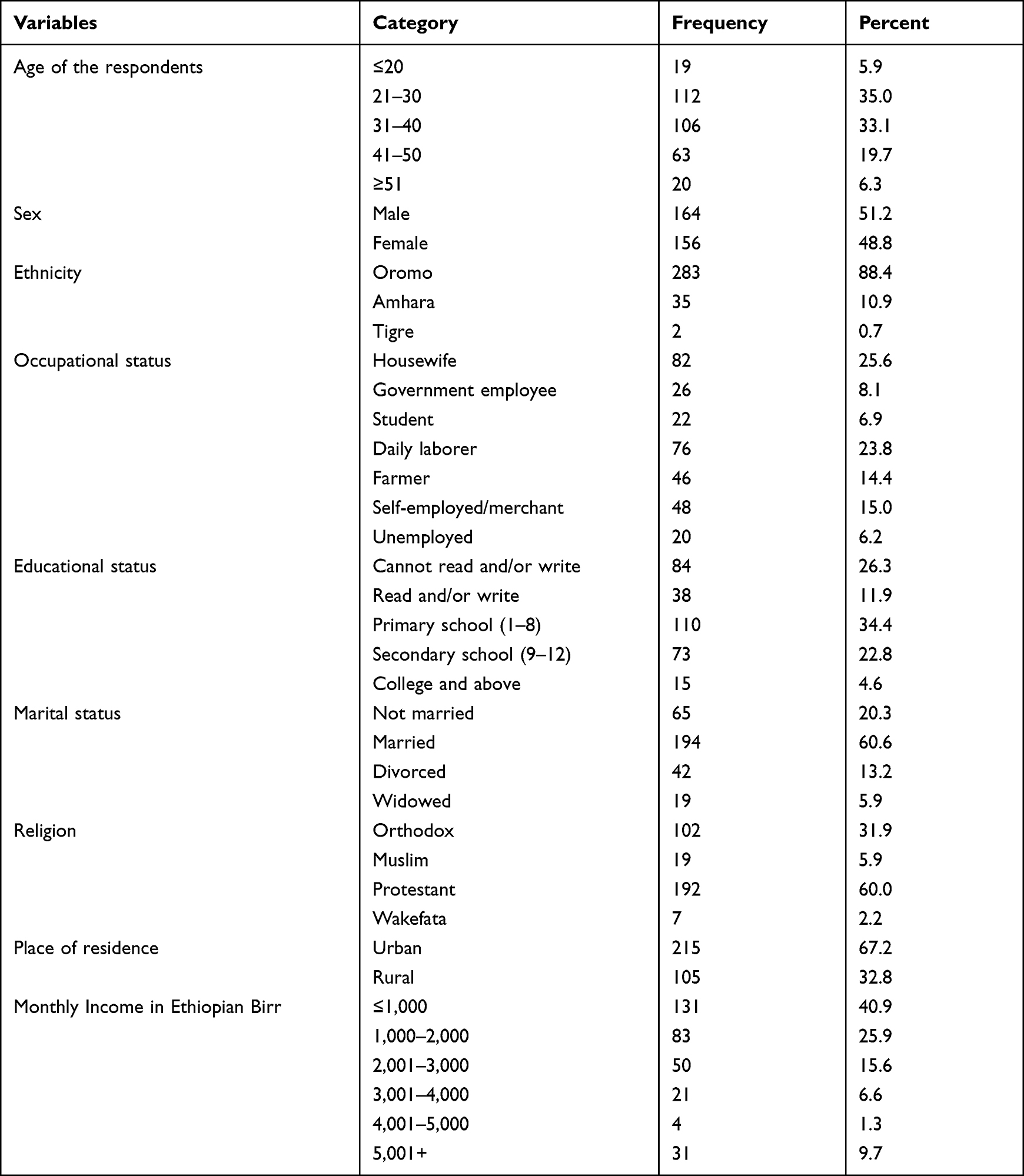 |
Table 1 Socio-Demographic Characteristics of Patients on ART in West Wollega Zone Public Hospitals, West Ethiopia, September 1–30 2020 (n=320) |
Regarding family characteristics, the majority (186; 58.1%) of the respondents were living with their spouse and only 22 (6.9%) of them were living alone. Regarding the educational status of the father and mother of the respondents, only 13 (4%) of either father or mother had completed or above secondary education (Grade 9 or more). The majority (227; 70.9%) of the respondents discussed the issues regarding support to PLWHA with their families or societies.
Awareness and Other Individual Related Characteristics of Patients Taking ART in West Wollega Zone Public Hospitals
The durations since the first HIV diagnosis and ART initiation for 217 (67.8%) and 233 (72.8%) of the respondents were both 2–10 years prior to the study period. The mean duration since the first HIV diagnosis and initiation of ART was 6.71 years (±3.653), and 6.32 (±3.33), respectively (Table 2).
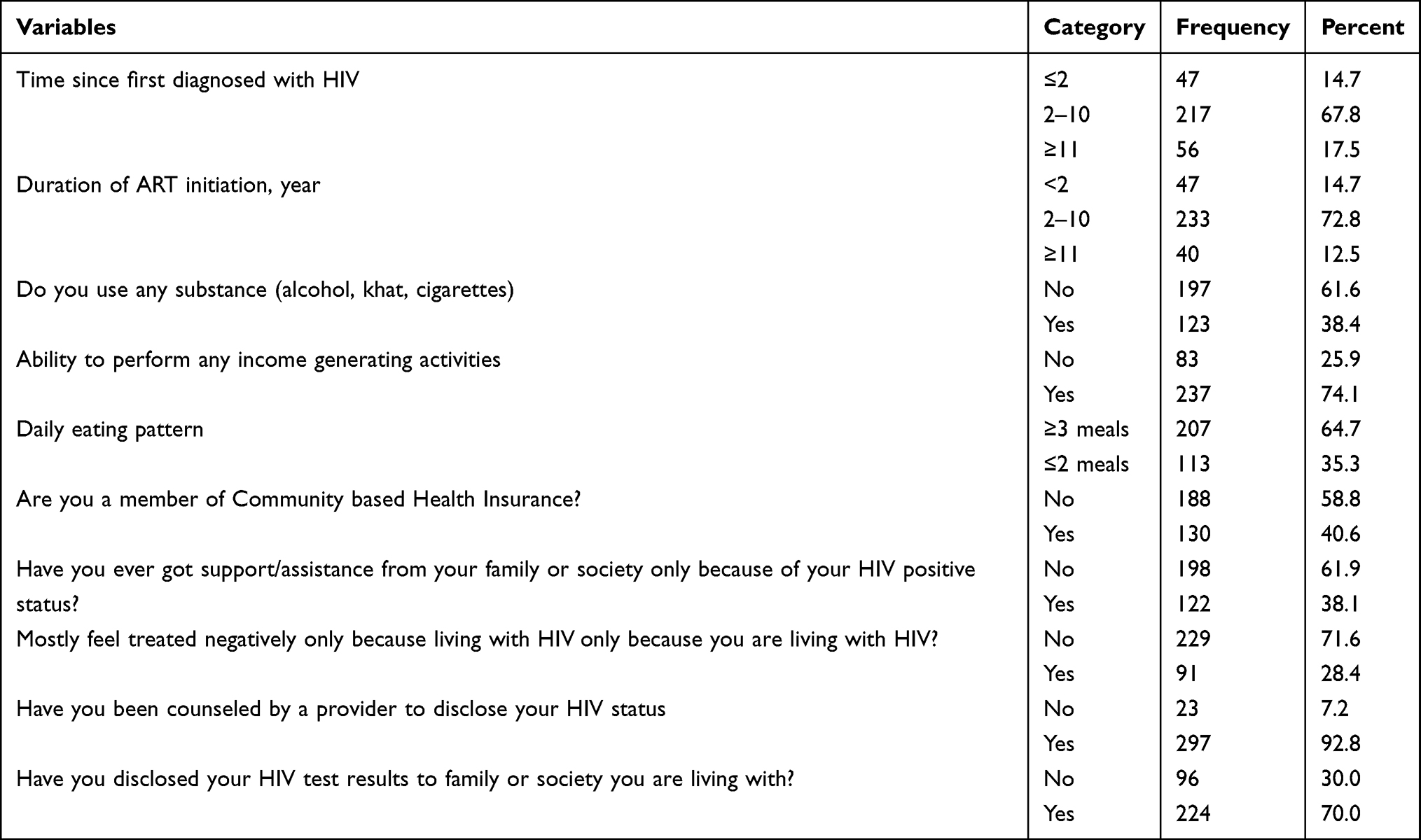 |
Table 2 Individual Related Characteristics of PLWHA on ART in West Wollega Zone Public Hospitals, West Ethiopia, September 2020 (n=320) |
Only 122 (38.1%) of the respondents ever got any level of family and social support because they were living with HIV virus, and the remaining 198 (61.9%) did not get any. Respondents were asked whether their family or society ever treated them negatively because they were living with HIV and 91 (28.4) of them responded 'yes'. Two hundred and ninety-seven (92.8%) of the respondents said they were counseled to disclose their HIV status to their family or society. However, only 224 (70%) of them did so (Table 3).
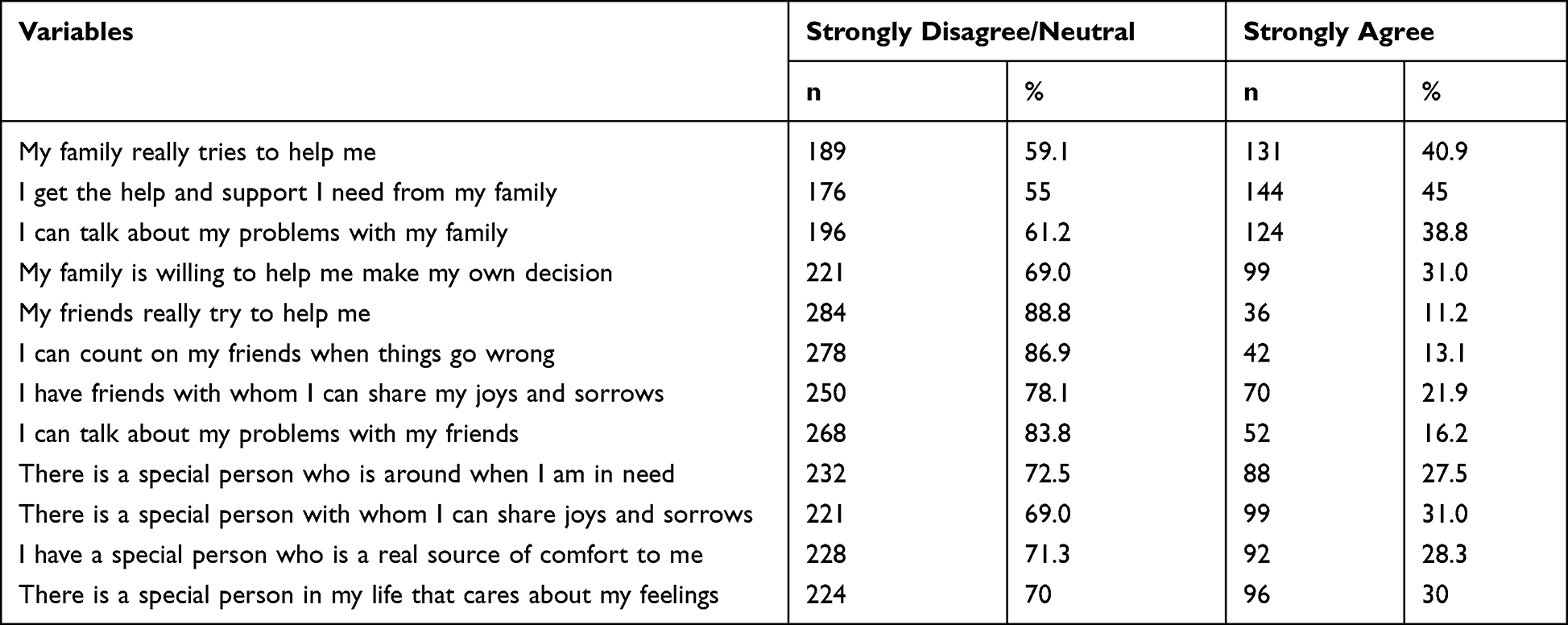 |
Table 3 Respondents Attitude About Support to Patients on ART in West Wollega Zone Public Hospitals, West Ethiopia, September 2020 (n=320) |
Regarding knowledge and awareness of patients about family and social support, the majority of respondents (207; 64.6%) used media (any of TV, radio, or internet), 196 (61.3%) used telephone, and 177 (55.3%) believed that support can improve the wellbeing of PLWHA.
Family and Social Support Among Patients on ART in West Wollega Zone Public Hospitals, 2020
To determine the status of family and social support, Multidimensional Scale of Perceived Social Support (MDPSS) having 12 (items) was used to measure attitude. Accordingly, among 320 study participants, only 107 (33.4%) achieved good social support, whereas the remaining 213 (66.6%) were found to achieve low support (Figure 1).
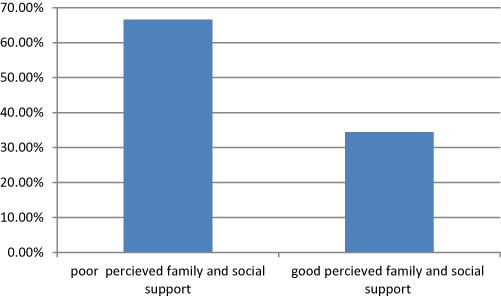 |
Figure 1 Status of family and social support among patients taking ART (antiretroviral therapy) in West Wollega Zone Public Hospitals, West Ethiopia September 2020. |
The family sub-scales revealed the majority of the respondents, 189 (59.1%), 176 (55%), 196 (61.2%), and 221 (69.0%), responded strongly disagree/disagree/neutral to the items their family really tried to help them, they get help and support they need from their family, they can talk about their problems with their familie,s and their family is willing to help them make their own decision, respectively. With the friends sub-scale of MDPSS, 284 (88.8%) and 278 (86.9%) strongly disagreed/disagreed/neutral to the items that their friends really tried to help them and they can count on friends when things go wrong, respectively; whereas 250 (78.1%) and 268 (83.8%) strongly disagreed/disagreed/neutral to the item they have friends with whom they can share their joys and sorrows and they can talk about their problems with their friends, respectively.
Additionally, 228 (71.3%) and 224 (70%) of the respondents were strongly disagreed/ disagreed/neutral respectively, that they have special persons who are a real source of comfort to them and there are special persons in their life who care about their feelings (Table 3).
Bivariate and Multivariate Logistic Regression of Family and Social Support and Associated Factors Among Patients on ART in West Wollega Zone Public Hospitals, West Ethiopia, September 2020
The result of binary logistic regression revealed that age, sex, current occupation, educational status, average monthly income educational status of the family (mother), disclosure of HIV test result, having discussion about support to PLWHA with family and society, and having a job for generating income were candidate variables with a p-value of less than 0.20.
The multivariate logistic regression analysis result showed that female respondents had about 93% less odds of having social support and family support [AOR (95% CI)=0.066 (0.013–0.338)]. Respondents unable to read and write had about 93% less odds of family and social support [AOR (95 CI)=0.067 (0.003–0.719)] compared to their counterparts.
The study also showed that average monthly income had a significant association with family and social support in this study. Participants having a monthly income of 5,001 ETB (USD 97.78) and greater were about 12-times more likely to have family and social support compared to those who earn less than 1,000 ETB (USD 19.55) per month [AOR (95% CI)=11.6 (1.06–12.45)].
Regarding discussion with family or society about the issues related to family and social support, the odds of patients on ART who did not discuss support had 73% less odds getting family and social support compared to their counterparts [AOR (95% CI)=0.275 (0.100–0.753)].
This study also depicted that respondents who had not ever heard issues related to family and social support for PLWHA had 69% less odds of getting family and social support [AOR (95% CI)=0.314 (0.104–0.951)].
Respondents having perceived stigma only because they were HIV positive had 87% less odds of having family and social support [AOR (95% CI)=0.127 (0.041–0.393)]. PLWHA who had not disclosed his/her HIV status to their family or society had about 77% less odds of accessing family and social support [AOR (95% CI)=0.227 (0.084–0.916)] (Table 4).
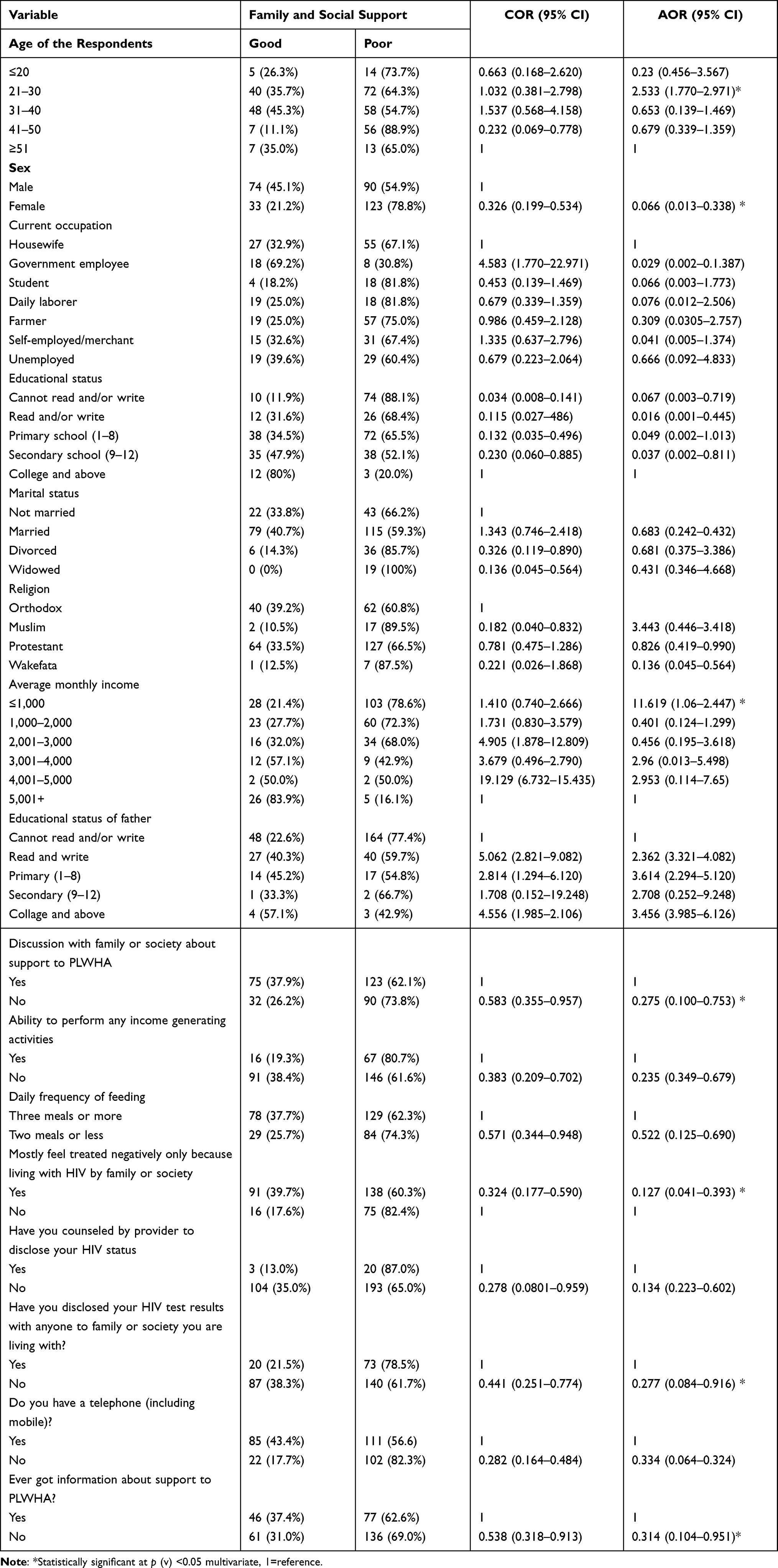 |
Table 4 Bivariate and Multivariate Logistic Regression Analysis of Support and Associated Factors Among Patients on ART in West Wollega Zone Public Hospitals, West Ethiopia, September 2020 |
Discussion
The study showed that the majority of patients taking ART in this study area, 213 (66.6%), had FSS below the mean score and were considered in this study as poor families, and the rest (33.4%) got good social support. In this study family and social support was influenced by respondents’ sociodemographic and other characteristics. Accordingly, sex, educational status, average monthly income, discussion about FSS with family or society, ever having access to information about support to PLWHA, and perceived stigma because they were living with HIV and disclosing HIV status.
The status of family and social support in this study is higher compared to a study conducted in Dublin, Ireland, where 54% of participants got a low PSS score and only 13% had a high PSS.21 The observed disparity might be due to differences in socio-economic status and culture of the population in this study area and Dublin. On the other hand, the current finding is in line with the study conducted in Nepal where the majority of PLWHA scored low or no social support score,22 but much lower than the longitudinal cohort study conducted in China where 90.4% of patients received family support at baseline or initiation of ART, 91.8% received family support 6 months into ART, 95.5% at 12 months, and 94.3% at 24 months.23 The possible reason might be due to differences in socio-economic status and awareness of society about HIV or PLWHA in this study area and the Chinese.
In this study female respondents had about 93% less odds of accessing family and social support. This is similar with the study conducted in Aksum town, which shows perceived social support was higher for males (with males having higher PSS (Perceived social support) scores.24 Educational status of the respondents was another factor that showed a statistically significant association with FSS in this study. Those unable to read and write had about 93% less odds of getting family and social support compared to those who have an educational status of college and above. This finding is in line with a study conducted in Aksum town and Arbaminch town which showed that lower education had less perceived social support.24,25 Lower educational attainment among PLWH has been associated with poorer social support, poorer linkage to care, treatment default, and greater HIV mortality in Ethiopia and other African countries. This might be due to the fact that lower educational attainment may reflect lower socioeconomic status, with fewer resources and information to meet health and HIV care needs.5,26
Average monthly income also showed a significant association with family and social support. Surprisingly respondents having higher monthly income were more likely to have family and social support than their counterparts. Respondents earning an average monthly income of greater than 5,001 ETB (USD 97.78) were about 12-times more likely to have family and social support than those who earn less than 1,000 ETB (USD 19.55) per month. This will be due to the fact that the peoples with the higher economic status may not have access to media or social media as a source of information regarding the family and social support they need to get from their family or society as a whole. Because in this study the respondents having less exposure to information about family and social support for PLWHA were less likely to have family and social support.
Discussion about support to PLWHA with family or society was another statistically significant factor in this study. The odds of those patients on ART who did not discuss support were less likely to have family and social support compared to those who discussed with family or society. A study conducted in Brazil on psychosocial support to PLWHA also showed that social discussion and relationships showed a highly significant correlation with social support.27 This could be due to the fact that discussion about support to PLWHA with family and society may improve social relations and hence make them able to know and try to help PLWHA.27
This study revealed that respondents who have ever exposed information about support for PLWHA were more likely to have family and social support. Those respondents who had not ever got information related to support to PLWHA got 69% lesser odds than those who had ever got information. This will be due to the fact that families and close socials are important caregivers, providing social (emotional and instrumental) support for members infected with HIV, with mothers and close friends being the most important caregivers.9 The benefits of informational support are that it buffers stress and improves the quality-of-life (meanwhile, informational support may also help the family member infected with HIV to restore their reason for being and increase their self-esteem.26,28,29
Feeling mostly treated negatively only because of living with HIV was also another significantly associated factor to support. Those who mostly feel treated negatively only because of living with HIV got 87% lesser odds of support than those who did not compared to their counterparts. In this study the magnitude of those who mostly feel treated negatively only because of living with HIV was 71.6%. This finding will be due to the probability that most people who mostly feel treated negatively only because of living with HIV will be isolated from the family and society due to perceived stigma so that they lose a chance to reflect their wishes and problems to others. Cultural beliefs about HIV and AIDS around contamination, sexuality, and religion have played a crucial role in the development of HIV-related discrimination. Studies also report perceived social support negatively associated with perceived internal stigma. HIV stigma includes distancing, exclusion, or social isolation.30
Disclosure of HIV status to the family or society was found to be associated with family and social support. Despite this, the significant proportion of PLWHA in this study area did not disclose their HIV status. This finding was lower than the study conducted in Addis Ababa, where more than three fourths (82.5%) of PLWHA had disclosed their HIV status to their most recent sexual partner.31 This difference could be due to a socio-demographic difference or difference in level of awareness which could be better in Addis Ababa and low in the current study area. Studies also showed that the intensified stigma associated with HIV/AIDS in African countries and in Eastern Europe made people more reluctant to disclose their HIV status to others.31,32 Finding identified that PLWHA taking ART who did not disclose their status had a statistically significant association with poor family and social support. WHO also concluded that women that disclose their HIV status have increased social support.24,25
Despite its interesting findings, this study had limitations. Firstly the study was cross-sectional which can be considered as an inherent design limitation where a causal relationship between the independent and dependent variables cannot be established. Secondly, family and society were not assessed to reflect their attitude towards PLWHA and qualitative data was not used which could explore the perception or beliefs of the family and society.
Conclusions
The study revealed that a significant proportion of the PLWHA attending ART clinic in West Wollega Public Hospitals had low family and social support. The finding of this study made clear about the advantage of information, and disclosing ones own HIV status to have better family and social support, while once perceived stigma and gender related issues negatively affect family and social support for PLWHA. Also, educational level, monthly income and discussion about support to PLHA with family or society were found to have an effect on the family and social support for PLWHA. Therefore, west Wollega health department and the respective hospitals ART clinic officer should trace and promote the family and social support of the PLWHA attending ART clinic. The responsible stakeholders should also intensify health information and awareness creation for the community or the family of the PLWHA about the importance and the type of care needed for people living with HIV. People living with HIV should opt to disclose their HIV status to at least their sexual parents or to the person close to them, which could improve the family and social support. Further research should be conducted to assess the effect of family and social support on patient adherence to ART and viral suppression.
Abbreviations
AIDS, acquired immuno-deficiency syndrome; ANC, antenatal care; ART, antiretroviral therapy; CI, confidence interval; CBHI, community based health insurance; EDHS, Ethiopian Demographic and Health Survey; EFY, Ethiopian fiscal year; ETB, Ethiopian Birr; FSS, family and social support; FMOH, Federal Ministry of Health; GC, Gregorian Calender; HC, health center; HEW, health extension workers; HIV, human immunodeficiency virus; JCF, Joint Consultative Forum; NCD, non-communicable diseases; OVC, orphans and vulnerable children; PHCUD, Primary Health Care Unit Director; PLWHA, peoples living with HIV AIDS; PSS, perceived social support; ORHB, Oromia Regional Health Bureaus; SSA, Sub-Saharan Africa; SS, social support; TB, tuberculosis; UNAIDS, United Nations Program on HIV/AIDS; UNICEF, United Nations Children Fund; USD, United State Dollar; WHO, World Health Organization.
Data Sharing Statement
The data used to support the findings of this study is available from the corresponding author upon request.
Ethical Consideration
This study was conducted in line with the Helsinki Declaration of health research.33 Ethical clearance was obtained from Wollega University, School of graduate studies Ethical Review committee. Permission for conducting the study was secured from the district health office. Written consent was obtained from all the studies after they had been briefed about the objectives and the aim of the research.
Acknowledgments
First, we would like to thank Wollega University for providing ethical permission to undertake this study. We also acknowledge the administrators and staff of the west Wollega Health Office, the respective Hospitals, their cooperation in providing me necessary baseline data of the study area and for their great support in the overall data collection process. Finally, our great full appreciation would be for all respondents and data collectors during data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. HIV/AIDS; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids.
2. UNAIDS. Communities at the center. Available from: 2019-global-AIDS-update_en.pdf.
3. Federal Democratic Republic of Ethiopia. Federal Ministry of Health .National consolidated guidelines for comprehensive HIV prevention, care and; 2018.
4. Central Statistical Agency - CSA/Ethiopia and ICF. Ethiopia demographic and health survey 2016. Addis Ababa, Ethiopia: CSA and ICF; 2017. Available from: http://dhsprogram.com/pubs/pdf/FR328/FR328.pdf.
5. Lifson AR, Workneh S, Hailemichael A, Demissie W. Perceived social support among HIV patients newly enrolled in care in rural Ethiopia. AIDS Care. 2015. doi:10.1080/09540121.2015.1098765
6. Matsumoto S, Yamaoka K, Takahashi K, et al. Social support as a key protective factor against depression in HIV-infected patients: report from large HIV clinics in Hanoi, Vietnam. Sci Rep. 2017;7(1):1–12. doi:10.1038/s41598-017-15768-w
7. Global report: UNAIDS report on the global AIDS epidemic 2013. “UNAIDS/JC2502/1/E”- Revisedandreissued; 2013. Available from: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_Global_Report_2013_en_1.pdf.
8. da Silva LMS, Campos Tavares JS. A família como rede de apoio às pessoas que vivem com HIV/AIDS: uma revisão na literatura Brasileira. Cien Saude Colet. 2015;20(4):1109–1118.
9. Morowatisharifabad MA, Movahed E, Farokhzadian J, et al. Antiretroviral therapy adherence based on information, motivation, and behavioral skills model and its association with depression among HIV-positive patients: health promotion strategy towards the 909090 target. J Educ Health Promot. 2019;8:192.
10. Melis T, Fikadu Y, Lemma L. Perceived stigma and associated factors among HIV positive adult patients attending antiretroviral therapy clinics at public facilities of Butajira Town, Southern Ethiopia, 2020. HIV AIDS. 2020;12:717–724. PMID: 33204172; PMCID: PMC7665444. doi:10.2147/HIV.S280501
11. Adane B, Yalew M, Damtie Y, Kefale B. Perceived stigma and associated factors among people living with HIV attending art clinics in public health facilities of Dessie City, Ethiopia. HIV AIDS. 2020;12:551–557. doi:10.2147/HIV.S274019
12. Chekole YA, Tarekegn D. HIV-related perceived stigma and associated factors among patients with HIV, Dilla, Ethiopia: a cross-sectional study. Ann Med Surg. 2021;71:102921. PMID: 34691447; PMCID: PMC8515236. doi:10.1016/j.amsu.2021.102921
13. Turi E, Simegnew D, Fekadu G, et al. High perceived stigma among people living with HIV/AIDS in a resource limited setting in Western Ethiopia: the effect of depression and low social support. HIV AIDS. 2021;13:389–397. doi:10.2147/HIV.S295110
14. Weldesenbet AB, Kebede SA, Tusa BS. The effect of poor social support on depression among HIV/AIDS patients in Ethiopia: a systematic review and meta-analysis. Depress Res Treat. 2020;2020:8. doi:10.1155/2020/6633686
15. Abdisa E, Tolesa T, Abadiga M. Prevalence of depressive symptoms and its associated factors among people living with HIV attending public hospitals of Nekemte Town, Western Ethiopia, 2021. Behav Neurol. 2021;2021:8854791. PMID: 34306251; PMCID: PMC8270704.. doi:10.1155/2021/8854791
16. Girma D, Assegid S, Gezahegn Y. Depression and associated factors among HIV-positive youths attending antiretroviral therapy clinics in Jimma town, southwest Ethiopia. PLoS One. 2021;16(1):e0244879. doi:10.1371/journal.pone.0244879
17. EFDRE Federal ministry of health. National consolidated guidelines for comprehensive HIV prevention, care and treatment; 2018. Available from: https://www.afro.who.int/sites/default/files/201904/National%20Comprehensive%20HIV%20Care%20%20Guideline%202018.pdf.
18. Global information and education on HIV and AIDS. HIV stigma and discrimination. Available from: https://www.avert.org/professionals/hiv-social-issues/stigma-discrimination.
19. Moradi G, Mohraz M, Gouya MM, et al. Health needs of people living with HIV/AIDS: from the perspective of policy makers, physicians and consultants, and people living with HIV/AIDS. Iran J Public Health. 2014;43(10):1424–1435.
20. Mark H, David C, Vincent L, Munoz SH, Vimla N, Semigina Tetyana SV. Getting to zero; global social work responds to HIV. Sex Health. 2014;11(2):107–118.
21. Okonkwo NO, Larkan F, Galligan M. An assessment of the levels of perceived social support among older adults living with HIV and AIDS in Dublin. Springerplus; 2016.
22. Zimet G. Multidimensional Scale of Perceived Social Support (MSPSS) - scale items and scoring information; 2016: 28–30.
23. Mao Y, Qiao S, Li X, Zhao Q, Zhou Y, Shen Z. Depression, social support, and adherence to antiretroviral therapy among people living with HIV in Guangxi, China : a Longitudinal Study. AIDS Edu Prevent. 2019;31(1):38–50. doi:10.1521/aeap.2019.31.1.38
24. Psychiatry G, Duko B, Geja E, Zewude M, Mekonen S. Prevalence and associated factors of depression among patients with HIV/AIDS in Hawassa, Ethiopia, cross ‑ sectional study. Ann Gen Psychiatry. 2020;2018:4–9. doi:10.1186/s12991-018-0215-1
25. Tefera B, Kondale T. Subjective quality of life and perceived adequacy of social support among the Elderly in Arbaminch Town. Ethiop J Soc Sci Humanit. 2014;10:1–26.
26. Cummings B, Gutin SA, Jaiantilal P, Rose CD, Francisco S. The role of social support among people living with HIV in rural Mozambique. AIDS Patient Care and STDs. 2014. doi:10.1089/apc.2014.0193
27. Calvetti PÜ, Giovelli GRM, Gauer GJC, Moraes JFDD. Psychosocial factors associated with adherence to treatment and quality of life in people living with HIV/AIDS in Brazil. J Bras Psiquiatr. 2014;63(1):8–15. doi:10.1590/0047-2085000000002
28. Joseph BN, Dapar MPL, Nyam N. Impact of stigma, health belief and social support in predicting adherence to antiretroviral medicines in Jos, Nigeria Impact of stigma, health belief and social support in predicting adherence to antiretroviral medicines in Jos, Nigeria; 2018.
29. Çevik GB. The roles of perceived social support, coping, and loneliness in predicting internet addiction in adolescents. J Edu Pract. 2017;8(12):64–73.
30. Shrestha S, Poudel KC, Poudel-Tandukar K, et al. Perceived family support and depression among people living with HIV/AIDS in the Kathmandu Valley, Nepal. J Int Assoc Provid AIDS Care. 2014;13(3):214–222. doi:10.1177/1545109712456741
31. Id NGD, Hailemichael RG, Shewa-amare A, Hillman J. HIV disclosure : HIV-positive status disclosure to sexual partners among individuals receiving HIV care in Addis Ababa, Ethiopia; 2019: 1–17.
32. Nanfuka EK, Kyaddondo D, Ssali SN, Asingwire N. Sustaining social support for lifelong HIV treatment : practices of patients on antiretroviral therapy in Uganda. JIAPAC. 2019. doi:10.1177/2325958219859654
33. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.