Back to Journals » Risk Management and Healthcare Policy » Volume 19
Failure Mode and Effects Analysis in Reducing the Incidence of Sterilization Cycle Interruptions in Low-Temperature Hydrogen Peroxide Plasma Sterilizers
Authors Yi L ![]() , You L, Pan W, Wu K, Zhang H
, You L, Pan W, Wu K, Zhang H
Received 24 October 2025
Accepted for publication 29 January 2026
Published 17 February 2026 Volume 2026:19 576606
DOI https://doi.org/10.2147/RMHP.S576606
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Keon-Hyung Lee
Liangying Yi,1,2,* Ling You,3,* Wei Pan,1,2 Kaili Wu,2,4 Hongxia Zhang1,2
1Department of Sterile Processing Nursing, West China Second University Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 2Key Laboratory of Birth Defects and Related Diseases of Women and Children (Sichuan University), Ministry of Education, Chengdu, Sichuan, People’s Republic of China; 3Lung Cancer Center/Lung Cancer Institute, West China Hospital, Sichuan University/West China School of Nursing, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 4Department of Pediatric Hematology and Oncology Nursing, West China Second University Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Pan, Email [email protected] Kaili Wu, Email [email protected]
Background: This study aimed to investigate the efficacy of failure mode and effects analysis (FMEA) in optimizing the sterilization process for low-temperature hydrogen peroxide plasma sterilizers.
Methods: Purposive sampling was used to select low-temperature hydrogen peroxide plasma sterilizers from a hospital in China as the study objects. The operational data for 1551 sterilization cycles in the low-temperature hydrogen peroxide plasma sterilizers, from May 2024 to November 2024, were classified into the control group. The operational data for 1492 sterilization cycles in the low-temperature hydrogen peroxide plasma sterilizers, from January 2025 to June 2025 following the implementation of the FMEA-based risk management scheme, were classified into the experimental group. The incidence of sterilization cycle interruptions, the risk priority number scores for high-risk failure modes, and the incidence of high-risk failure modes in both groups were investigated.
Results: After the optimization of the operating procedures, the incidence of sterilization cycle interruptions decreased from 5.48% (85/1551) to 0.87% (13/1492); the risk priority number scores and the incidence of high-risk failure modes were also decreased (P < 0.05).
Conclusion: The FMEA-based risk management scheme could optimize the sterilization process for low-temperature hydrogen peroxide plasma sterilizers and ensure the quality of medical device sterilization.
Keywords: failure mode and effects analysis, low-temperature hydrogen peroxide plasma sterilizers, sterilization interruptions, sterilization quality, risk management
Introduction
Low-temperature hydrogen peroxide plasma sterilizers use a specific dose of hydrogen peroxide as the sterilizing agent. Vaporized hydrogen peroxide is diffused into the sterilization chamber and converted into hydrogen peroxide plasma in a high-frequency electric field or a radio-frequency electromagnetic field under defined vacuum and low-temperature conditions.1 During plasma reactions, oxygen atoms generated from hydrogen peroxide interact with microbial cell walls and enzymes. Excited-state nitrogen oxides in air plasma can emit ultraviolet radiation with wavelengths ranging from 250 to 320 nm. Ultraviolet radiation with wavelengths of 220 to 270 nm is most effective at damaging the deoxyribonucleic acid of microbial cells, thereby enabling safe and rapid sterilization of medical devices without leaving toxic residues. Each step of the sterilization cycle is conducted in a low-temperature, dry environment, ensuring that compatible devices sensitive to moisture or heat are not damaged. Characterized by rapid sterilization, high sterilization efficiency, high device turnover rate, and decomposition into non-toxic end-products, hydrogen peroxide plasma sterilization has been widely adopted for low-temperature sterilization in central sterile supply departments (CSSDs).2,3
The low-temperature hydrogen peroxide plasma sterilizer is equipped with a sensitive and strict automatic identification control system. If sterilization conditions do not meet the requirements, this system will immediately trigger the sterilization cycle interruption mechanism.4 The sterilization efficacy of low-temperature hydrogen peroxide plasma sterilizers is influenced by multiple factors, including the structure, material, cleaning quality, drying quality, and loading method of the items to be sterilized. For example, CSSD staff may make incorrect judgments regarding the structure and material of medical devices awaiting sterilization. Devices unsuitable for low-temperature hydrogen peroxide plasma sterilization, such as lumen devices with blind ends, excessively long lumens, or lumens with diameters that are too small, may be incorrectly reprocessed using this method. In addition, packaging materials that absorb hydrogen peroxide, such as paper pouches or non-woven fabric that have not undergone sterilization validation, may be used. Inadequate cleaning can leave contaminants on device surfaces, preventing effective contact with the sterilizing agent. Incomplete drying allows residual moisture to absorb hydrogen peroxide, reducing its concentration within the sterilization chamber. Furthermore, item overloading or improper placement can obstruct the monitoring light at the chamber door, triggering alarms. These circumstances may interrupt the sterilization cycle and lead to equipment failure.5 Previous studies have reported sterilization failure rates of 3.18% to 6.47% for low-temperature hydrogen peroxide plasma sterilization, with operation failure rates as high as 9.46%.6,7 Common causes of sterilization failure include incomplete drying before sterilization, item overloading, and improper item placement.8 Sterilization failures can lead to the waste of resources and affect the implementation of clinical work. In severe cases, they can increase the incidence of nosocomial infections and seriously impact patient treatment outcomes. Therefore, identifying the weak links in the process of low-temperature hydrogen peroxide plasma sterilization is significant for improving sterilization quality and ensuring patient safety.
The American National Standards Institute/Association for the Advancement of Medical Instrumentation emphasizes that risk management is crucial for ensuring the safety of medical devices.9 The standards for low-temperature hydrogen peroxide plasma sterilization released by the Chinese government focus on the technical requirements for sterilizer hygiene and performance testing, and rarely address the operational procedures and risk management of the sterilizers. Moreover, equipment management for low-temperature hydrogen peroxide plasma sterilizers focuses on “post-event correction” rather than “pre-event prevention”, lacking a proactive and systematic risk management scheme to control potential risks effectively.
Failure Mode and Effects Analysis (FMEA) is a proactive and systematic risk management tool endorsed by The Joint Commission International. It can be used to systematically quantify healthcare risk events, analyze the causes of failures and the failure modes, and provide a scientific basis for adjusting plans and optimizing processes.10 FMEA has been widely utilized in healthcare risk management, yielding significant reductions in the incidences of healthcare accidents and disputes.11 Wang et al applied FMEA to equipment performance management and maintenance strategies for low-temperature hydrogen peroxide plasma sterilizers.12 However, studies examining the application of FMEA to process management in low-temperature hydrogen peroxide plasma sterilization remain scarce.
Methods
Sampling
Purposive sampling was used to select low-temperature hydrogen peroxide plasma sterilizers (STERRAD™ 100NX) from the Central Sterile Supply Department of West China Second University Hospital, Sichuan University as the study objects. The volume of the sterilization chamber was 152 L. Each hydrogen peroxide cassette contained 10 capsules, with a volume of 5400μL ± 216μL and a hydrogen peroxide concentration ranging from 53% to 59.6%. The sterilizers were equipped with a hydrogen peroxide purification function, achieving a post-purification concentration of 90% to 95%. The standard sterilization temperature was 50°C, the sterilization pressure ranged from 3.9 to 25.9 Torr, and the total sterilization time was 16 minutes. The sterilizers were equipped with an automatic monitoring system that could monitor and record parameters such as pressure, temperature, humidity, and hydrogen peroxide concentrations in real time during the sterilization process. The data concerning the sterilizer operation was exported by an equipment engineer through an open-ended information connection port. The operational data for 1551 sterilization cycles in the low-temperature hydrogen peroxide plasma sterilizers, from May 2024 to November 2024 (before the implementation of the FMEA-based risk management scheme), were classified into the control group. The operational data for 1492 sterilization cycles in the low-temperature hydrogen peroxide plasma sterilizers, from January 2025 to June 2025 (following the implementation of the FMEA-based risk management scheme), were classified into the experimental group.
Study Design
Control Group
The conventional operating procedures for low-temperature hydrogen peroxide plasma sterilizers were used in the control group. The cleaning quality and dryness levels of the items to be sterilized, packaging quality, and item loading were strictly checked. Sterilizer maintenance was performed once every two weeks.
Experimental Group
A FMEA-based risk management scheme was implemented for lower-temperature hydrogen peroxide plasma sterilizers in the experimental group.
Build an FMEA-Based Risk Management Team
Operating low-temperature hydrogen peroxide plasma sterilizers is a specialized task. Sterilization quality is closely associated with the prevention and control of nosocomial infections. A multidisciplinary team was created to comprehensively analyze and optimize the operating procedure for low-temperature hydrogen peroxide plasma sterilizers. The inclusion criteria for team members were: (1) familiar with the operating procedure for low-temperature hydrogen peroxide plasma sterilizers and possessing relevant theoretical knowledge; (2) having a bachelor’s degree or above and strong research capabilities; (3) having 5 years or more of work experience. The team consisted of 10 people. Of them, 1 was a manager in the Equipment Department, 2 were engineers, 6 were CSSD nurses, and 1 was an infection control expert. The details of the team members are shown in Table 1.
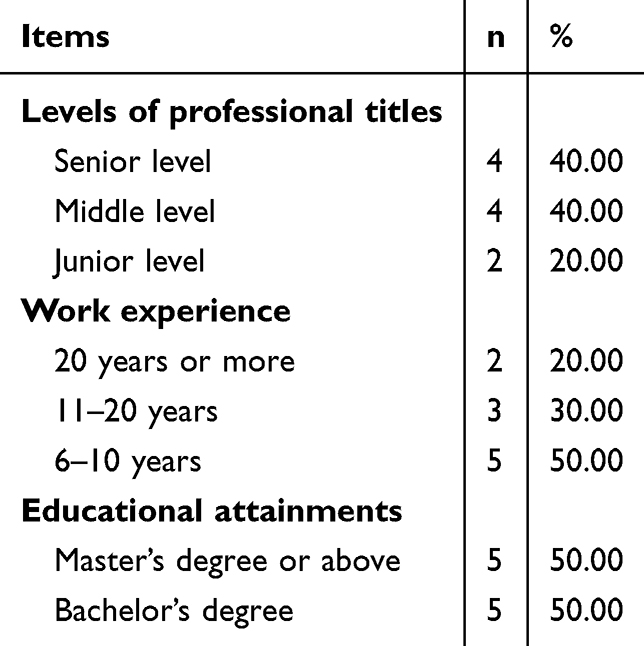 |
Table 1 Details of FMEA-Based Risk Management Team Members |
Identify Risks
Focusing on reducing the incidence of sterilization cycle interruptions in low-temperature hydrogen peroxide plasma sterilizers, the FMEA-based risk management team analyzed the causes of sterilization cycle interruptions that occurred from May 2024 to November 2024. Based on the analysis results, literature review, team discussions, and brainstorming, the causes of sterilization cycle interruptions were determined to involve a total of 22 main factors across 4 steps: (1) pre-treatment; (2) packaging; (3) loading; and (4) equipment management, as shown in Figure 1.
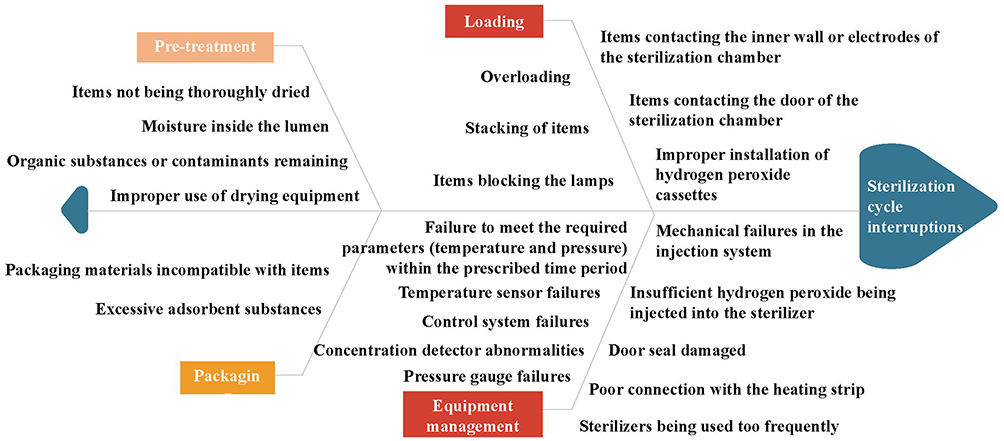 |
Figure 1 Fishbone diagram for failure modes of low-temperature hydrogen peroxide plasma sterilization. |
Analyze and Evaluate Risks
The risk priority number (RPN) was used to quantitatively evaluate the risks associated with each failure mode and its impact on sterilization cycle interruptions in low-temperature hydrogen peroxide plasma sterilizers. Each failure mode was quantitatively analyzed in three aspects: severity (S), occurrence (O), and detection (D).12 The scoring criteria are shown in Table 2. The formula for calculating the RPN is: RPN = S × O × D. The risks were classified into five levels based on the range of RPN values: high risk, medium-high risk, medium risk, medium-low risk, and low risk, with the 20th, 40th, 60th, and 80th percentiles, respectively, for classification. Further risk management was performed on the high-risk failure modes,13 as shown in Tables 3 and 4.
 |
Table 2 Risk Scoring Criteria for Severity, Occurrence, and Detection |
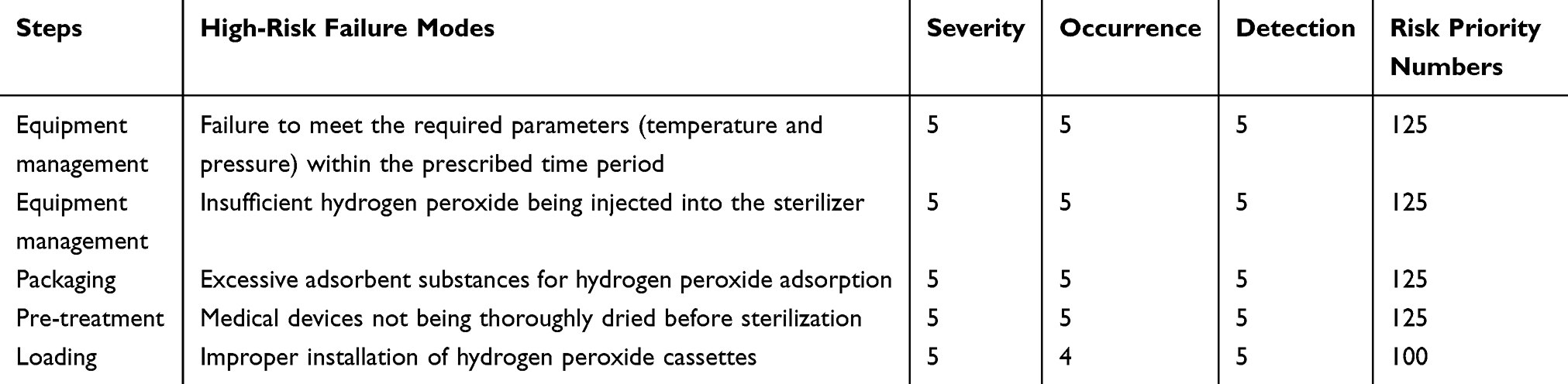 |
Table 3 High-Risk Failure Modes and Risk Priority Numbers for Sterilization Cycle Interruptions in Low-Temperature Hydrogen Peroxide Plasma Sterilizers |
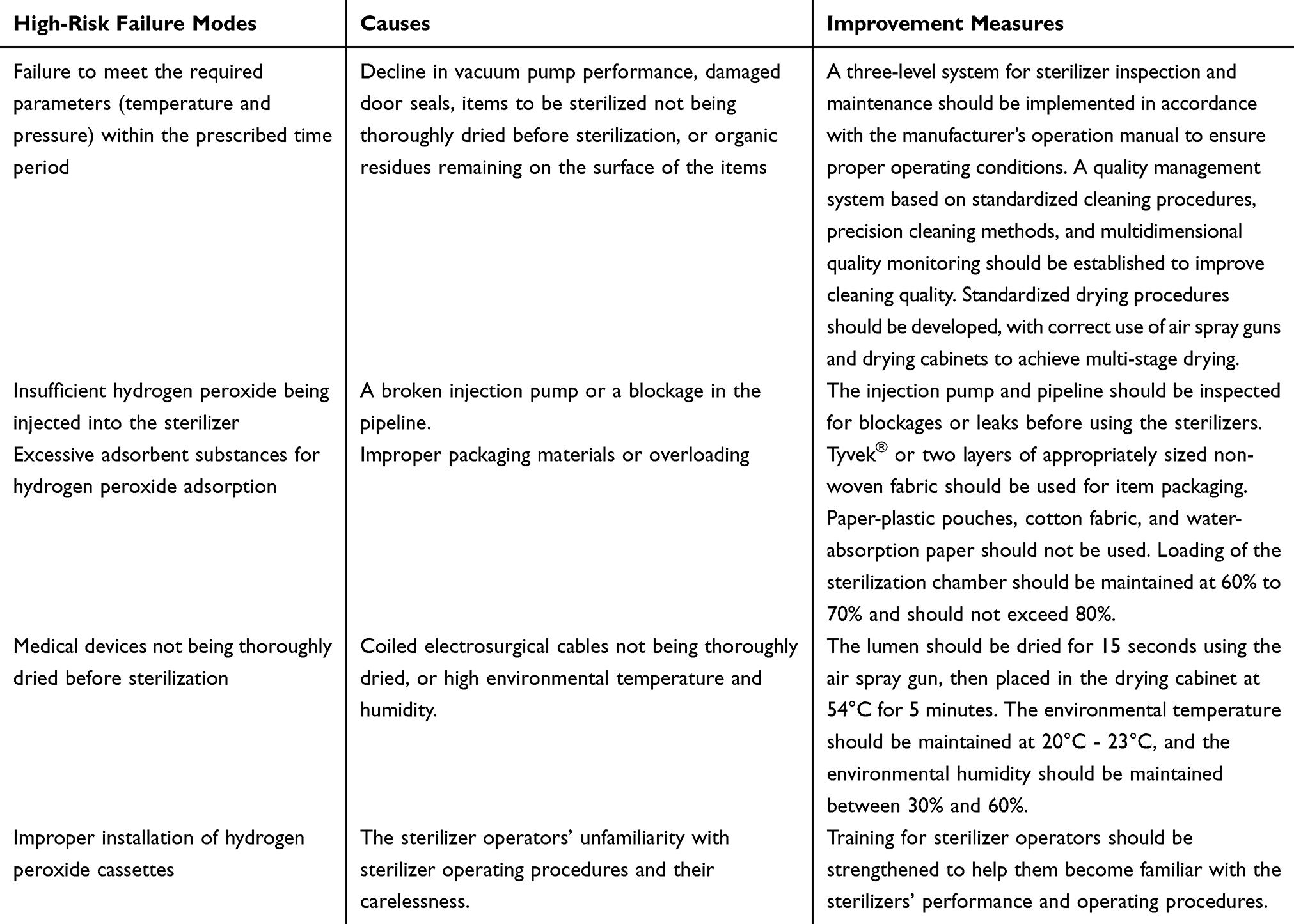 |
Table 4 Causes of High-Risk Failure Modes and Improvement Measures |
Optimization of Operating Procedures for Low-Temperature Hydrogen Peroxide Plasma Sterilizers Based on FMEA
Guided by the FMEA, a flowchart was developed to optimize the operating procedures for low-temperature hydrogen peroxide plasma sterilizers, based on the five high-risk failure modes identified in this study, a literature review, brainstorming, and team discussions. This flowchart was used to guide the implementation of the FMEA-based risk management scheme, ensuring continuous improvement of quality, as shown in Figure 2.
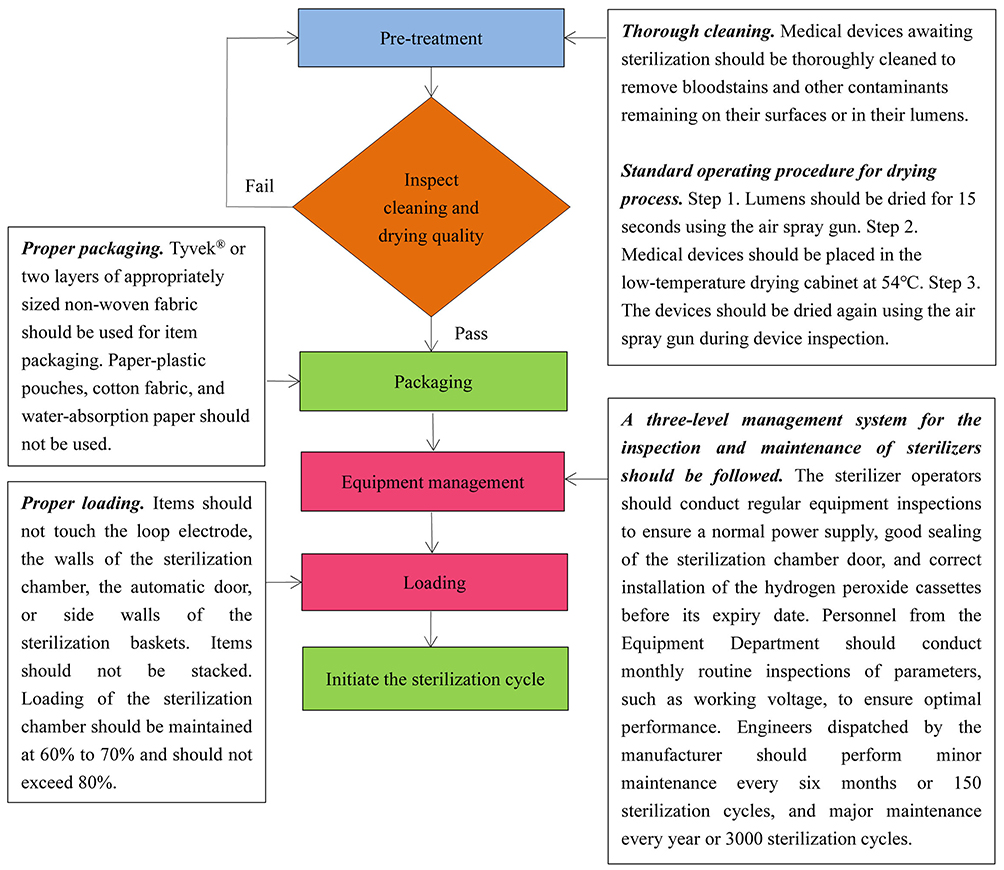 |
Figure 2 Flowchart of optimization process for low-temperature hydrogen peroxide plasma sterilization. |
Training
To ensure that every CSSD nurse could proficiently implement the FMEA-based risk management scheme for low-temperature hydrogen peroxide plasma sterilizers, a one-week training program was provided to all CSSD nurses before the implementation of the risk management scheme. The training employed a combination of theoretical knowledge explanations and practical skills training, delivered through offline lectures, group sessions, and hands-on demonstrations. A three-level quality control system was formed by the head nurse, nursing group leaders, and the nurses. The head nurse was responsible for supervising the training progress, analyzing the problems that occurred during the training, and proposing solutions and improvement suggestions. The nursing group leaders urged the nurses to complete the operating procedures stipulated in the FMEA-based risk management scheme. CSSD nurses were allowed to operate the sterilizers only after passing the training assessment.
Quality Control
The risk management team established a dynamic supervision mechanism to ensure the effective implementation and continuous optimization of the FMEA-based risk management scheme. They conducted irregular on-site inspections to monitor the implementation of the FMEA-based risk management scheme in real time. The implementation progress was analyzed monthly to summarize experiences and identify weak links, thereby enhancing the professionalism and problem-focused coping skills of CSSD nurses.
Observation Indicators
The incidence of sterilization cycle interruptions, the RPN values of high-risk failure modes, and the incidence of high-risk failure modes in both groups were investigated.
Statistical Methods
SPSS 26.0 (SPSS Inc, Armonk, NY, USA) was used for data analysis. The normality of the measurement data was tested using the Kolmogorov–Smirnov test. Measurement data that were normally distributed were expressed as the mean ± standard deviation ( ), and comparisons between the two groups were conducted using the independent samples t-test. Measurement data that were not normally distributed were expressed as the median and interquartile range [M (P25, P75)], and comparisons between the two groups were conducted using the Mann–Whitney U-test. Enumeration data were expressed as frequencies or percentages, and comparisons between the two groups were conducted using the chi-square test. A statistically significant difference was identified by P < 0.05.
), and comparisons between the two groups were conducted using the independent samples t-test. Measurement data that were not normally distributed were expressed as the median and interquartile range [M (P25, P75)], and comparisons between the two groups were conducted using the Mann–Whitney U-test. Enumeration data were expressed as frequencies or percentages, and comparisons between the two groups were conducted using the chi-square test. A statistically significant difference was identified by P < 0.05.
Results
Incidence of Sterilization Cycle Interruptions
The incidence of sterilization cycle interruptions in low-temperature hydrogen peroxide plasma sterilizers decreased from 5.48% (85/1551, before the optimization of the operating procedures) to 0.87% (13/1492, after the optimization of the operating procedures), with a statistically significant difference (χ2 = 51.831, P < 0.001).
RPN Values for High-Risk Failure Modes
After the operating procedures were optimized based on the FMEA, the RPN values for failure to meet the required parameters (temperature and pressure) within the prescribed time period, insufficient hydrogen peroxide being injected into the sterilizer, excessive adsorbent substances for hydrogen peroxide adsorption, medical devices not being thoroughly dried before sterilization, and improper installation of hydrogen peroxide cassettes decreased significantly, with a statistically significant difference (P < 0.05), as shown in Table 5. This demonstrates that the FMEA-based risk management scheme is effective in improving sterilization quality.
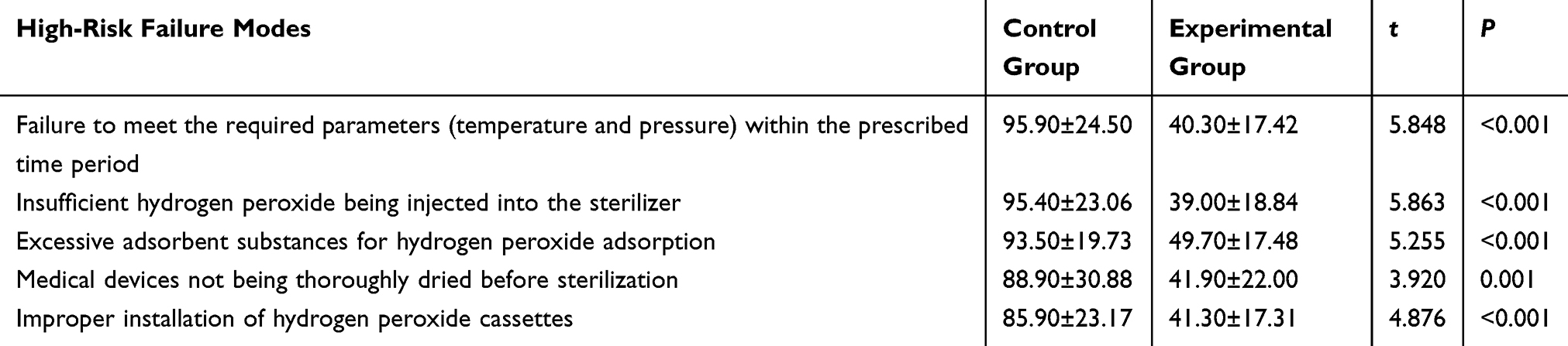 |
Table 5 Risk Priority Numbers for High-Risk Failure Modes |
Incidence of High-Risk Failure Modes
Following optimization of the operating procedures based on the FMEA, the incidences of the following high-risk failure modes decreased significantly: failure to meet the required parameters (temperature and pressure) within the prescribed time period, insufficient hydrogen peroxide being injected into the sterilizer, excessive adsorbent substances for hydrogen peroxide adsorption, and medical devices not being thoroughly dried before sterilization, with a statistically significant difference (P < 0.05). No statistically significant difference was found in the incidence of improper installation of hydrogen peroxide cassettes between the control and experimental groups, as shown in Table 6.
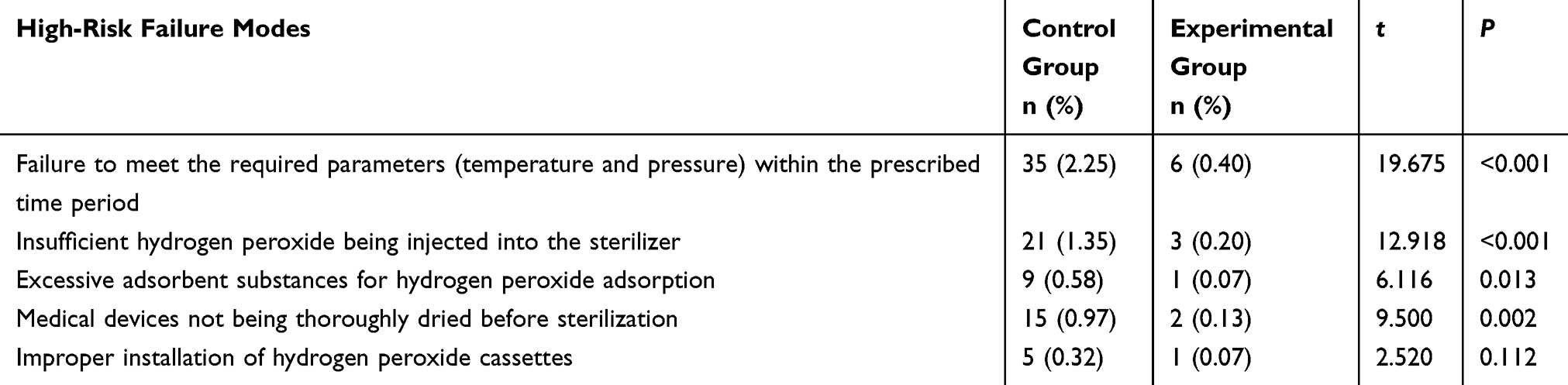 |
Table 6 Incidence of High-Risk Failure Modes in Control and Experimental Groups |
Discussion
FMEA Could Optimize the Operating Procedures for Low-Temperature Hydrogen Peroxide Plasma Sterilizers
FMEA is a scientific management tool that identifies weak links in process management in advance and facilitates standardized improvements to the process. This study employed FMEA to analyze the operating procedures for low-temperature hydrogen peroxide plasma sterilizers and identify potential failure modes. The RPN values of the five high-risk failure modes decreased after the implementation of the FMEA-based risk management scheme. This demonstrates that the FMEA-based risk management scheme can effectively improve the quality of low-temperature hydrogen peroxide plasma sterilization and can serve as a reference for other healthcare institutions in managing low-temperature hydrogen peroxide plasma sterilization.
The Implementation of the FMEA-Based Risk Management Scheme Could Reduce the Incidence of Sterilization Cycle Interruptions
Sterilization cycle interruptions in low-temperature hydrogen peroxide plasma sterilizers can directly affect the quality of medical device sterilization and patient safety.14 The results of this study show that the incidence of sterilization cycle interruptions significantly decreased after the implementation of the FMEA-based risk management scheme. The three high-risk failure modes identified in our study—excessive adsorbent substances for hydrogen peroxide adsorption, medical devices not being thoroughly dried before sterilization, and improper installation of the hydrogen peroxide cassettes—confirmed the results of Peng et al15 and Wang et al.16 Based on the three identified high-risk failure modes, this study developed and implemented a structured closed-loop control scheme to block risk transmission pathways. To manage and control materials with hydrogen peroxide-adsorbing properties, a visualized item access list was created to explicitly prohibit the use of materials with high adsorption capacity, such as linen, wood products, powders, and items that were inadequately dried or contained cotton strips, for hydrogen peroxide sterilization. This list was posted in both the packaging inspection and sterilization areas.
To ensure adequate instrument drying, a dual inspection system combining visual inspection and quantitative random inspection of high-risk instruments was mandatorily implemented for items processed by low-temperature hydrogen peroxide plasma sterilizers, in addition to standard drying procedures. This approach effectively reduced the risk of sterilization failure caused by residual moisture.
To prevent improper installation of hydrogen peroxide cassettes, a standardized instructional chart for cassette installation was posted at the sterilization chamber door, clearly outlining installation steps, positioning marks, and key points for status verification. A mandatory two-person inspection system was also implemented, requiring two operators to jointly confirm each installation, verify that the correct cassette type was properly installed, and sign off on the inspection.
Previous relevant studies focused on medical device packaging and loading, compatibility of medical devices to be sterilized, and staff training.17 Our study found that failure to meet the required parameters (temperature and pressure) within the prescribed time period was also a significant cause of sterilization cycle interruptions in low-temperature hydrogen peroxide plasma sterilizers. The range of temperature fluctuation and the error in indicating pressure are important indicators for evaluating the performance of sterilizers. If a sterilizer fails to meet the required parameters for temperature or pressure within the prescribed time period, it will be unable to effectively kill bacterial spores and other microorganisms, resulting in sterilization failure. For high-risk failure modes, we formulated improvement measures for low-temperature hydrogen peroxide plasma sterilization through a literature review and brainstorming. These measures included the following: A three-level system for sterilizer inspection and maintenance should be implemented in accordance with the manufacturer’s operation manual to ensure proper operating conditions. A quality management system based on standardized cleaning procedures, precision cleaning methods, and multidimensional quality monitoring should be established to improve cleaning quality. Standardized drying procedures should be developed, with correct use of air spray guns and drying cabinets to achieve multi-stage drying. Packaging material selection should be clearly defined, with preference given to Tyvek® or two layers of appropriately sized non-woven fabric for item packaging. Paper-plastic pouches, cotton fabric, and water-absorbing paper should not be used. Loading of the sterilization chamber should be maintained at 60% to 70% and should not exceed 80%. In addition, staff training should be strengthened to ensure that operators can skillfully operate the sterilizers in accordance with standard operating procedures. An FMEA-based risk management scheme was developed after team discussions on these improvement measures. The incidence of sterilization cycle interruptions decreased from 5.48% (data before the implementation of the FMEA-based risk management scheme) to 0.87% (data after the implementation of the FMEA-based risk management scheme). This indicates that FMEA can effectively identify weak links in the operating process and provide a scientific basis for quality improvement.
The Implementation of the FMEA-Based Risk Management Scheme Could Reduce the Incidence of High-Risk Failure Modes
In this study, the incidence of high-risk failure modes significantly decreased after the implementation of the FMEA-based risk management scheme. Equipment failures, medical devices not being thoroughly dried before sterilization, item overloading, and sterilizer operators’ unfamiliarity with sterilizer operating procedures were the root causes of the failure modes. Therefore, when formulating improvement measures, we implemented a three-level management system for the inspection and maintenance of sterilizers, in addition to strictly standardizing processes such as instrument drying and item loading. The time points and frequencies for the inspection and maintenance of sterilizers were clearly specified, and specific personnel were assigned relevant responsibilities. This was done to enhance the professional knowledge and skills of sterilizer operators, standardize sterilizer operating procedures, and conduct quality control and supervision, ensuring that high-risk failure modes were addressed.18 To address sterilizer operators’ unfamiliarity with sterilization procedures, systematic measures were implemented, including standardized training, visual guidance, and continuous supervision. These measures aimed to ensure long-term standardization and consistency of the sterilization process, thereby fundamentally safeguarding sterilization safety and quality.
Limitations
This study has some limitations. First, this was a single-center study with a small sample size and a short study period. The generalizability of the study results is restricted. Second, FMEA is subjective in evaluating severity, occurrence, and detection, and the evaluation results largely depended on the professional knowledge and clinical experience of the FMEA team members. A multicenter study with a large sample size is need, and the sterilization process should be optimized based on actual circumstances to achieve better results.
Conclusions
This study demonstrates that FMEA can be used to systematically review each step of low-temperature hydrogen peroxide plasma sterilization, accurately identify potential failure modes, and formulate feasible improvement measures. Application of FMEA can efficiently optimize work processes for low-temperature hydrogen peroxide plasma sterilization and effectively reduce or eliminate factors that trigger failures. As a result, the incidence of sterilization cycle interruptions and high-risk failure modes can be reduced, ensuring smooth implementation of sterilization procedures and maintaining the quality of medical device sterilization.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Funding
No funding was obtained for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. National Health Commission of the People’s Republic of China. Hygienic Requirements for Low-Temperature Hydrogen Peroxide Gas Plasma Sterilizer: GB 27955-2020. Beijing: Standards Press of China; 2020.
2. Ding L, Yao Z, Geng J, et al. Construction of quality evaluation index system for hydrogen peroxide low-temperature plasma sterilization in hospitals. J Nurs. 2024;31(20):60–10. doi:10.16460/j.issn1008-9969.2024.20.060
3. Chen H, Liu J, Zeng A, Qin N. Analysis of sterilization efficiency and application cost of three low temperature sterilization methods. Rev Sci Instrum. 2024;95(4):045112. doi:10.1063/5.0175121
4. He S. Study on the influence of PDCA cycle management method on the sterilization effect of hydrogen peroxide low-temperature plasma in disinfection and supply center. Clin Res. 2022;30(8):188–191. doi:10.12385/j.issn.2096-1278(2022)08-0188-04
5. Wang J, Zhang B, Sun H, et al. Monitoring the effective sterilization of low-temperature hydrogen peroxide gas plasma sterilizers in 58 hospitals - 22 PLADs, China, June 2015-December 2019. China CDC Wkly. 2021;3(29):624–626. doi:10.46234/ccdcw2021.152
6. Qiao L, Zheng H, He Y. Analysis of the causes and countermeasures of ASP100NX hydrogen peroxide low-temperature plasma sterilization Cycle Interruption. China Med Device Inf. 2023;29(21):159–161. doi:10.3969/j.issn.1006-6586.2023.21.050
7. Dai Y, Wang L, Luo M. Investigation and analysis of running faults in low-temperature hydrogen peroxide plasma sterilizers. Chin J Disinfect. 2016;33(11):1109–1110. doi:10.11726/j.issn.1001-7658.2016.11.026
8. Zhao Y, Zhao Y, Wang X, Sun X, Yang J. Analysis of adverse events of hydrogen peroxide low temperature plasma sterilizers. Chin Med Equip. 2022;19(1):161–164. doi:10.3969/J.ISSN.1672-8270.2022.01.037
9. Farlow CS, Jump ML, Seeberger MS, Fitzgerald BJ. ANSI/AAMI SW96: raising the bar for medical device security risk management. Biomed Instrum Technol. 2023;57(2):40–43. doi:10.2345/0899-8205-57.2.40
10. Liu L, Li X, Jiang M, Cai Y. Epidemiological characteristics of occupational exposure of medical personnel and intervention effect of failure mode and effects analysis (FMEA). Mod Hosp. 2023;23(4):637–640, 651. doi:10.3969/j.issn.1671-332X.2023.04.041
11. Cui Y, Wang Y, Liu H, Xu S, Zhang X. Exploring the correlation between patient safety culture and adverse medical events using failure mode and effect analysis (FMEA). Risk Manag Healthc Policy. 2025;18:1367–1376. doi:10.2147/RMHP.S502725
12. Wang D, Zhang M, Xu F. Application of FMEA in improving safety of hydrogen peroxide low-temperature plasma sterilizer. Hosp Manag Forum. 2021;38(2):18–21. doi:10.3969/j.issn.1671-9069.2021.02.005
13. Cai L, Zhang Y, Hu L, et al. Application of FMEA in prevention and control of device-related infection in intensive care unit. Chin J Infect Control. 2021;20(6):494–498. doi:10.12138/j.issn.1671-9638.20211055
14. Li L, Li Y, Chen X, Zhou X. Study on application effect of fine management in quality control of low temperature plasma sterilizer. China Med Device Inf. 2022;28(10):171–173. doi:10.3969/j.issn.1006-6586.2022.10.056
15. Peng Y, Lei Y, Shi H. Reasons and control measures for the interruption of the sterilization cy-cle of instruments in hydrogen peroxide low-temperature plasma sterilization system. China Mod Med. 2021;28(36):183–185, 189. doi:10.3969/j.issn.1674-4721.2021.36.052
16. Wang J, Ma H, Liu J. Influencing factors for interrupt of circulation of low-temperature hydrogen peroxide plasma sterilization system and process control. Chin J Nosocomiol. 2014;24(12):3105–3106, 3114. doi:10.11816/cn.ni.2014-141063
17. Fan Y, Qiao S, Cao T, Zhang J, Wang M. Application of PDCA cycle management in quality management of low-temperature hydrogen peroxide plasma sterilization. Chin Gen Pract Nurs. 2022;20(5):660–662. doi:10.12104/j.issn.1674-4748.2022.05.024
18. Pan W, Yi L, Hu T, Huang J, Huang Y. An action research study of quality improvement in instrument packaging procedures for the central sterile supply department. Sci Rep. 2024;14(1):3764. doi:10.1038/s41598-024-54237-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.