Back to Journals » Clinical Ophthalmology » Volume 15
Factory-Made Elastic Silicone Sheet as an Alternative for the Posterior Capsule of the Lens During Phacoemulsification for Dislocated/Subluxated Lenses
Authors Akamine R, Miyamoto N, Kiritoshi S, Kusaka M, Akimoto M ![]()
Received 7 November 2020
Accepted for publication 27 January 2021
Published 23 February 2021 Volume 2021:15 Pages 769—774
DOI https://doi.org/10.2147/OPTH.S287462
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Supplementary video of "Alternative capsule for dislocated lens" [ID 287462].
Views: 35670
Rinko Akamine, Naomi Miyamoto, Shoko Kiritoshi, Mami Kusaka, Masayuki Akimoto
Osaka Red Cross Hospital, Osaka, Japan
Correspondence: Masayuki Akimoto
Osaka Red Cross Hospital, 5-30 Fudegasakicho, Tennojiku, Osaka, 543-8555, Japan
Email [email protected]
Background: We previously reported a novel technique using an elastic silicone bowl, which was handmade from a phaco test chamber, to salvage dislocated lenses and perform phacoemulsification and aspiration (PEA) on the bowl. However, creating the bowl was challenging.
Methods: A factory-made elastic silicone sheet (ESS), a ready-to-use alternative for the posterior capsule of the lens, was prepared. We used this sheet to salvage and support the dislocated/subluxated lenses in 11 eyes of nine patients.
Results: We could use a sheet immediately after we opened the package. In all the cases, we could insert a sheet beneath the lens and PEA performed at the center of the operative field. There was only one incident where the lens could not be placed onto the disc at the first attempt, but the lens was eventually salvaged. There was no risk of rupture during PEA, and the ESS could be removed completely without any complications.
Conclusion: The factory-made ESS described here can be used for salvaging dislocated/subluxated lenses and safely performing PEA.
Keywords: lens dislocation, perfluorocarbon, alternative posterior capsule of the lens
Introduction
In patients with lens dislocation, the use of vitreous cutters is not sufficient to remove large lens fragments. Several techniques for treating a dislocated lens have been reported, such as the fragmatome, phaco without sleeve, bimanual techniques, and use of perfluorocarbon liquid (PFCL).1–8
In cases of lens subluxation, a capsular expander able to sustain the dialyzed zonule may be useful once a continuous curvilinear capsulorhexis is completed. Previously, we reported a new technique using an elastic silicone bowl handmade from the phaco test chamber,9 which is inserted into the vitreous cavity through a corneoscleral incision. Then, the dislocated lens is salvaged with the bowl acting as a fish net. Phacoemulsification and aspiration (PEA) is performed in the bowl after pulling it up to the iris plane.
The bowl acts not only as a fish net but also as a posterior lens capsule substitute. PEA is performed at the center of the bowl under a stronger power setting, as the silicone bowl is too hard to be broken. The technique is useful; however, the bowl must be handmade. Instead, we introduced a designed laser-cut silicone sheet, made from a plain silicone sheet, comprising a dish and three arms. We present a case series in which this factory-made elastic silicone sheet (ESS) was used for salvage and PEA for dislocated/subluxated lenses.
Surgical Technique
The Supplementary video shows a shortened version of the procedures used in this study.
The ESS was made of silicone and composed of two parts: the central disc and three arms (Figure 1). The central part is round, with a diameter of about 13 mm. There are small holes at the center of this part, improving operability. Each of the three arms that are evenly placed on the edge of the central part have an equal length of approximately 20 mm, with each arm having a bulge in the middle to ensure non-slip.
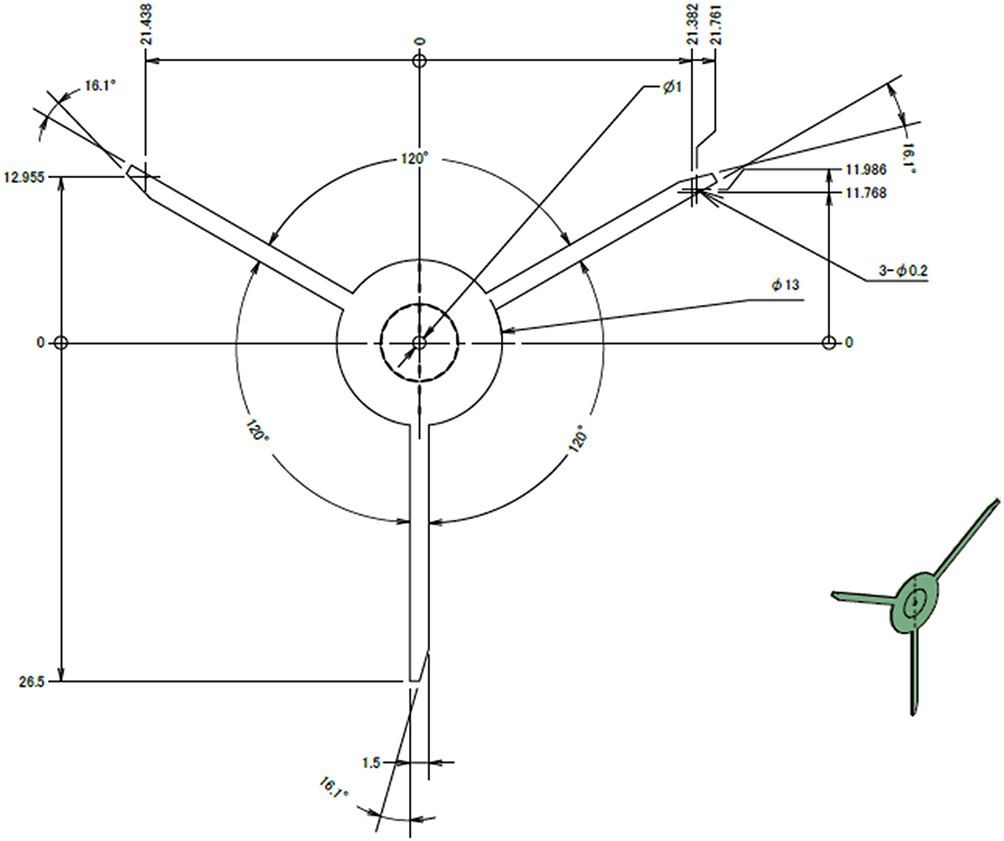 |
Figure 1 Drawing of the elastic silicone sheet. |
We placed three trocars at 3.5 mm from the limbus and performed pars plana vitrectomy using a 25-gauge cutter, after retrobulbar anesthesia induction. We then created three corneal side-ports at approximately 2ʹ, 6ʹ, and 10ʹ using a 20-gauge microvitreoretinal blade, and then, a 3-mm corneoscleral incision using a slit knife.
The ESS was inserted into the eye through a 3-mm corneoscleral incision. For cases of subluxated lens, one arm was inserted and pulled out through the corneal port at 6ʹ (Figure 2A). After the sheet was folded, it was inserted into the eye behind the subluxated lens (Figure 2B). The other two long arm was pulled out through one of the corneal side ports using forceps (Figure 2C). We performed PEA on the ESS after pulling it up to the iris plane (Figure 2D). After the PEA, we cut every arm out of the eye (Figure 2E) and removed the ESS via the corneoscleral incision using forceps (Figure 2F–H). For cases of dislocated lens (Not shown in figure), after all three arms were set, the sheet was pushed into the vitreous near the bottom. The dislocated lens was put onto the sheet by vitreous cutter. If it is unstable, Ophthalmic viscoelastic device (OVD) was placed on the sheet as glue.
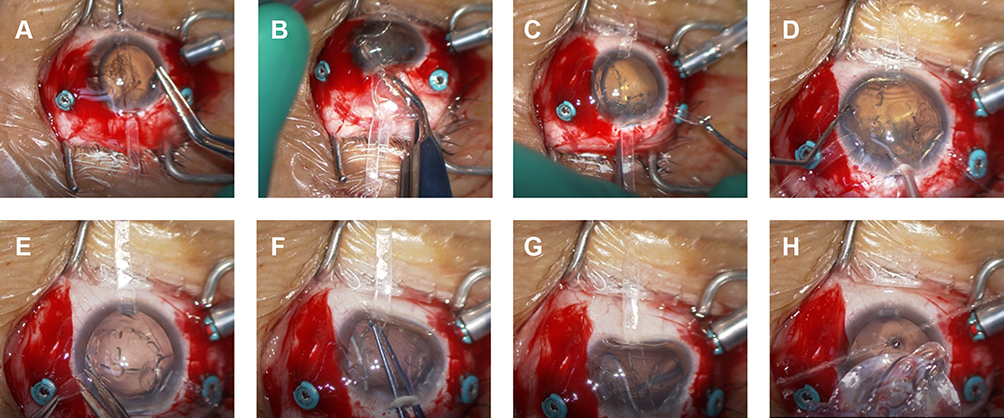 |
Figure 2 Surgical procedure of a case with a subluxated lens. (A) One arm was inserted into the corneal side port using forceps. (B) The elastic silicone sheet (ESS) was inserted into the eye behind the subluxated lens through a 3-mm corneoscleral incision and zonular dialysis. (C) The other two ends of the arms were inserted through the corneal side ports. (D) Phacoemulsification and aspiration (PEA) was performed on the ESS. (E) After the PEA was completed, the two arms were dissected. (F, G) The remaining arm was caught and pulled out. (H) The ESS was easily removed through the corneoscleral incision. |
A foldable 3-piece IOL was then fixed intrasclerally.10,11 Scleral incisions were sutured with 8–0 vicryl, but corneoscleral incision was not sutured.
In cases of subluxated lenses, we performed anterior vitrectomy under the infusion through the anterior chamber maintainer in advance and inserted the ESS under the lens through the gap where the lens was off. We then repeated the procedure.
Patients
This study was a hospital-based, single-center case series. We obtained written informed consent from each patient for the original surgery, the case details and any accompanying images published. The procedures used were approved by the Ethics Committee of the Osaka Red Cross Hospital. The study adhered to the tenets of the Declaration of Helsinki.
The technique was used in 11 eyes of nine patients with dislocated/subluxated lenses. A summary of the patient characteristics is shown in Table 1. All patients in the current study underwent comprehensive ophthalmologic examinations prior to surgery.
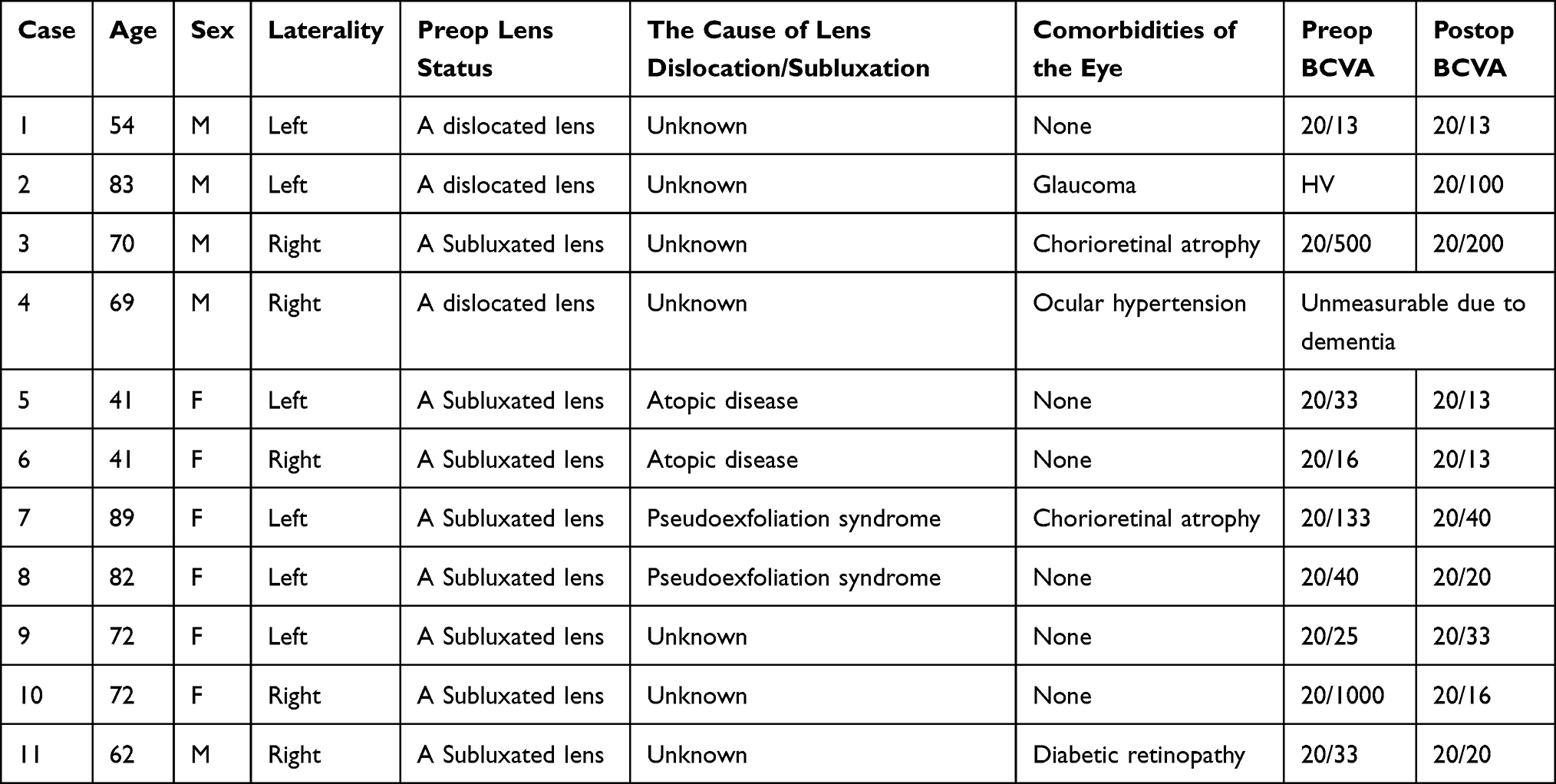 |
Table 1 A Summary of the Patients |
Results
The ESS was safely introduced in all 11 eyes with dislocated/subluxated lenses. After the dislocated/subluxated lenses were salvaged and lifted to the iris plane, PEA was performed on the sheet at the center without sheet-rupture. Large lens fragments were not dispersed and were located in the sheet during PEA. The ESS was then removed via the corneoscleral incision using forceps. After ESS removal, particles of lens fragments remained on the fundus. These fragments were easily cleared using a 25-gauge cutter, without cutting. In one case, the lens could not be placed onto the disc at first attempt. This was due to the fact that the silicone sheet was unable to hold the lens on the sheet, in contrast to the bowl, where the lens was dropped by current of vitreous infusion. The dropped lens was salvaged after OVD was placed on the sheet thus stopping the vitreous infusion.
We did not have to use a pupil expander, as the three arms expanded the pupil in the form of a triangle.
Each one case of hypotony (<5 mmHg) and hypertony (>30 mmHg) were recorded but soon recovered on the next consultation day without any treatment. IOL deviation was seen with two patients and one got operation to correct its position. No endophthalmitis, retinal detachment and hemorrhage were observed. The preoperative mean corneal astigmatism was 1.07 diopter (D), and postoperative one was 1.25 D. The mean corneal endothelial cell density decreased from 2369 cells/mm2 before surgery to 1862 cells/mm2 after surgery.
Discussion
Here, we presented a case series in which a factory-made ESS was successfully used for salvage and PEA in 11 cases of dislocated/subluxated lenses.
Use of PFCL is a current standard technique for the treatment of a dislocated lens.1–3 Since PFCL is heavier than water, it enables the use of PEA around the iris plane, which prevents retinal damage. However, there are several issues. Lens fragments tend to avoid staying at the center of the operative field because of the surface tension of PFCL. Bubbles of PFCL may remain in the eye at the end of the surgery, and lead to patient discomfort or secondary glaucoma. It is difficult to use PFCL for the treatment of a subluxated lens without pars plana vitrectomy.
We hypothesized that for treating a dislocated/subluxated lens, a bowl-like device to catch the lens would be necessary as a substitute for the posterior capsule, thus enabling us to remove the lens fragments safely and effectively. Since the silicone bowl does not wrinkle and break by the change of fluid, we could only use anterior irrigation during PEA without posterior infusion. We have not seen surge nor globe collapse. Although the new silicone bowl technique is effective, its production is slightly complicated and time consuming. We collaborated with a company that makes sterile ESSs to avoid having to manufacture the material by hand. As in most cases, the use of an ESS helped us not only retain the lens fragments at the center of the field during PEA but also keep dilating pupil, although in one case, the lens fragment was dropped into the vitreous. It was possible to place the dislocated lens fragment back onto the sheet through a lens-salvation operation; however, the vitreous infusion flow dislocated the lens. After OVD was placed onto the sheet, the lens was returned onto the sheet and was salvaged after the vitreous infusion was stopped.
As shown in Table 1, postoperative BCVA was more than 20/40 with 8 patients, and this is comparable to PFCL use.8 Other patients did not show such improvement because their comorbidities such as glaucoma, chorioretinal atrophy and diabetic retinopathy. Although we made 3 corneal side port and corneoscleral incision, there was no obvious increase of corneal astigmatism. There was 21% loss of corneal endothelial cells. That was higher than with custom made bowl to our experience. The difference of the shape may make the lens position nearer the cornea with the sheet than with the bowl.
In cases of subluxated lens, it was easier to insert the ESS in case of zonular rupture at the upper and lateral sides of lens. Nevertheless, a potential lower side rupture made the insertion difficult. Therefore, it was necessary to enable the lens to deliberately drop to render the processes that followed easier and safer.
Although the ESS is a flat sheet, it is possible to remove the lens fragments safely from the ESS in a completely controlled manner. The remaining fragments at the fundus were small pieces that could be easily cut using a vitreous cutter. The ESS can be removed in its entirety using forceps. Therefore, there is no risk of the ESS remaining in the eye after surgery.
We refer to the ESS as “The Tripus” because of its octopus-like three arms that are located on the sheet. To our experience, a bowl-shaped ESS is much better than a sheet design. We are still looking for a realistic shape that can be cost-effective in terms of production and useful for all surgeons.
Although we have achieved good outcome and have not seen critical complications in case series study, the ESS is still not available commercially. Further evaluation will be needed in multicenter study with larger samples and longer periods.
What Was Known
- The standard technique for performing phacoemulsification and aspiration (PEA) of dislocated/subluxated lenses employs perfluorocarbon liquid, but as previously shown, an elastic silicone bowl made from the phaco test chamber can be used for salvaging a dislocated/subluxated lens and performing PEA.
What This Paper Adds
- A factory-made flat silicone sheet with three arms can be used for salvaging dislocated/subluxated lenses and safely performing PEA.
Acknowledgment
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. The 42nd Annual Meeting of the Japanese Society of Ophthalmic Surgery, Yokohama, Japan, February 2019.
Funding
Materials were provided by Kono Seisakusho Co., Ltd, Tokyo.
Disclosure
M. Akimoto is a consultant for Kowa Co. Ltd. The authors report no other conflicts of interest in this work.
References
1. Girard LJ, Canizales R, Esnaola N, Rand WJ. Subluxated (ectopic) lenses in adults. Long-term results of pars plana lensectomy-vitrectomy by ultrasonic fragmentation with and without a phacoprosthesis. Ophthalmology. 1990;97(4):462–465. doi:10.1016/S0161-6420(90)32560-5
2. Yata K, Tanikawa A, Hori K, Nakamura A, Yamada H, Horiguchi M. Intravitreal bimanual surgery for residual lens fragments and displaced crystalline lenses. Ophthalmic Surg Lasers Imaging. 2009;40:331–335. doi:10.3928/15428877-20090430-22
3. Arroyo JG, You T, Bossi KE. Illuminated lens fixator for bimanual pars plana lensectomy. Ophthalmic Surg Lasers. 2001;32:438–440.
4. Chiang A, Garg SJ, Alshareef RA, et al. Removal of posterior segment retained lens material using the OZil phacoemulsification handpiece versus Fragmatome during pars plana vitrectomy. Retina. 2012;32:2119–2126. doi:10.1097/IAE.0b013e31825a89c3
5. Shapiro MJ, Resnick KI, Kim SH, Weinberg A. Management of the dislocated crystalline lens with a perfluorocarbon liquid. Am J Ophthalmol. 1991;112:401–405. doi:10.1016/S0002-9394(14)76247-6
6. Lee SJ, Kim IG, Park JM. Management of posteriorly dislocated crystalline lens with perfluorocarbon liquid and fibrin glue-assisted scleral-fixated intraocular lens implantation. J Cataract Refract Surg. 2013;39:334–338. doi:10.1016/j.jcrs.2013.01.022
7. Millar ER, Steel DH. Small-gauge transconjunctival vitrectomy with phacoemulsification in the pupillary plane of dense retained lens matter on perfluorocarbon liquids after complicated cataract surgery. Graefes Arch Clin Exp Ophthalmol. 2013;251:1757–1762. doi:10.1007/s00417-013-2293-8
8. Jang HD, Lee SJ, Park JM. Phacoemulsification with perfluorocarbon liquid using a 23-gauge transconjunctival sutureless vitrectomy for the management of dislocated crystalline lenses. Graefes Arch Clin Exp Ophthalmol. 2013;251:1267–1272. doi:10.1007/s00417-012-2170-x
9. Kiritoshi S, Kusaka M, Akimoto M. Elastic silicone bowl to salvage dislocated lenses and substitute for the substitutive posterior lens capsule during phacoemulsification. Retina. 2019;39(1):S58–S61. doi:10.1097/IAE.0000000000002267
10. Akimoto M, Taguchi H, Takayama K, Nagasawa S, Hiroi K. Intrascleral fixation technique using catheter needles and 30-gauge ultrathin needles: lock-and-lead technique. J Cataract Refract Surg. 2015;41:257–261. doi:10.1016/j.jcrs.2014.08.030
11. Takayama K, Akimoto M, Taguchi H, Nagasawa S, Hiroi K. Transconjunctival sutureless intrascleral intraocular lens fixation using intrascleral tunnels guided with catheter and 30-gauge needles. Br J Ophthalmol. 2015;99:1457–1459. doi:10.1136/bjophthalmol-2014-306579
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.