Back to Journals » Clinical Ophthalmology » Volume 17
Factors Predictive of Refractive Error After Toric Lens Implantation
Authors Gauthier A ![]() , Awidi AA
, Awidi AA ![]() , Noble PM, Daoud YJ
, Noble PM, Daoud YJ
Received 16 February 2023
Accepted for publication 2 May 2023
Published 26 June 2023 Volume 2023:17 Pages 1813—1821
DOI https://doi.org/10.2147/OPTH.S407414
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Angela Gauthier,1 Abdelhalim A Awidi,1 Paige M Noble,2 Yassine J Daoud1
1Wilmer Eye Institute, Johns Hopkins Hospital, Baltimore, MD, USA; 2Department of Ophthalmology, University of Iowa, Iowa City, IA, USA
Correspondence: Yassine J Daoud, The Wilmer Eye Institute, Johns Hopkins Hospital, 600 North Wolfe Street, Baltimore, MD, 21287, USA, Tel +1 410-955-5080, Fax +1 410-583-2842, Email [email protected]
Purpose: To identify factors related to suboptimal refractive outcomes after toric intraocular lens implantation.
Patients and Methods: A retrospective case-control chart review of 446 eyes with toric lens insertion by the same surgeon at a university hospital from 2016 to 2020 was conducted. Pre-operative exam findings, biometry, and one month and three month post-operative vision and refraction were noted. Reviewed charts were considered cases if uncorrected distance visual acuity (UDVA) was worse than 20/40, spherical equivalent (SE) > 1 diopter (D) off target, or cylinder > 1 D off target.
Results: Overall, 93.7% (n = 343) of eyes achieved UDVA of 20/40 or better, 92.7% (n = 306) were within 1 D of target SE, and 90.9% (n = 300) were within 1 D of target cylinder. UDVA cases had more eyes with prior LASIK (21.7% vs 7.0%, p = 0.01) and keratoconus (8.7% vs 0.6%, p < 0.001) than controls. More SE cases had prior radial keratotomy (RK) (8.3% vs 0%, p < 0.001) and keratoconus (12.5% vs 0%, p < 0.001) than controls. More cylinder cases had prior LASIK (30.0% vs 8.7%, p < 0.001) and higher mean astigmatism (2.3 vs 1.5 D, p = 0.02) than controls. More cases in all three analyses had higher toric cylinder power (T5-T9) than controls. Age, sex, eye laterality, axial length, anterior chamber depth, lens power, dry eye, anterior basement membrane dystrophy, and Fuchs’ endothelial dystrophy differences were not significant.
Conclusion: Prior LASIK or RK, keratoconus, and higher astigmatism may increase the chance of a suboptimal outcome.
Keywords: cataract surgery, refractive surgery, astigmatism
Introduction
Cataract is a leading cause of reversible vision loss among adults in the United States.1 Approximately 24 million Americans are currently living with cataracts, and this number is expected to rise to 38.7 million by 2030.2 Due to advancements in cataract surgery techniques and intraocular lens (IOL) technology, many patients expect significant improvement in their visual acuity and spectacle independence after surgery. In patients undergoing cataract surgery, 22% have at least 1.5 diopters (D) and 8% have at least 2.0 D of corneal astigmatism.3,4 Treatment of corneal astigmatism during cataract surgery using clear corneal incisions at the steep meridian, limbal relaxing incisions, or a toric IOL, can help optimize final uncorrected visual acuity.5–8
Several studies have demonstrated the ability of toric IOLs to achieve excellent post-operative visual acuity outcomes, with 90–95% of patients attaining an uncorrected distance visual acuity (UDVA) of 20/40 or better.9–11 Post-operative residual refractive astigmatism is 0.5 D or less in 71–92% of patients.12–15 Toric lenses were able to provide spectacle independence for distance vision in 60–97% of patients.16
The purpose of this study is to investigate patient characteristics, comorbid eye pathology, and biometry factors that may lead to suboptimal UDVA or residual refractive error in patients undergoing cataract surgery with toric IOL implants. Understanding these factors may help manage visual outcome expectations in patients with astigmatism.
Materials and Methods
A single-center, retrospective case-control study of patients who underwent toric IOL implantation at the Johns Hopkins University Wilmer Eye Institute was conducted. This study adhered to the tenants of the Declaration of Helsinki and was approved by the Johns Hopkins Institutional Review Board (IRB), IRB00243897. A waiver for written informed consent was granted by the IRB for the purposes of this study. This study was deemed compliant with the Health Insurance Portability and Accountability Act (HIPAA) by the IRB.
An electronic chart review was conducted on all patients who received hydrophobic acrylic toric lens (AcrySof IQ toric IOLs; Alcon Laboratories, Inc., Fort Worth, Texas, USA) implantation by the same cataract surgeon between 2016 and 2020. Target refraction, best corrected distance visual acuity (CDVA), UDVA, and refraction at post-operative month one and three was collected. Pre-operative exam findings and comorbid conditions including dry eye (defined by the presence of punctate epithelial erosions on the pre-operative exam), Fuchs’ endothelial dystrophy (FED), anterior basement membrane dystrophy (ABMD), keratoconus (diagnosed by a corneal specialist based on Scheimpflug imaging), history of laser assisted in situ keratomileusis (LASIK), and history of radial keratotomy (RK) were noted. Only patients with stable keratoconus grade I–III according to the Global Consensus of Keratoconus and Ectatic Diseases were included in the study.17 Lastly, biometry data from the IOL master (IOLMaster 500, Zeiss, Jena, Germany) including axial length, anterior chamber depth, keratometry, and corneal astigmatism, as well as lens type and lens power were recorded. All lenses were chosen using the IOL master measurements in the Barrett Universal II formula except in cases of prior refractive surgery, where the American Society of Cataract and Refractive Surgeons (ASCRS) online IOL calculator was used to select the best IOL power.
Three separate analyses were used to find characteristics associated with suboptimal outcomes. In all three analyses, eyes were excluded if there was no data at the one-month and three-month postoperative visit. They were also excluded if CDVA was 20/40 or worse at one month and beyond, indicating additional eye pathology beyond refractive error.
In the first analysis, cases were defined as eyes achieving UDVA worse than 20/40 at one month after cataract surgery. Controls achieved an UDVA of 20/40 or better one month after cataract surgery. Eyes with UDVA worse than 20/40 at one month that improved to better than 20/40 at their three month post-operative visit were also included in this group. Eyes were excluded from this analysis if target vision was aimed for near (spherical equivalent (SE) ≥ −1.00 D).
The second and third analyses measured residual SE and cylindrical error, respectively. Eyes were excluded if there was no refraction at 1 month and 3 months after surgery, or if there was no clearly defined target refraction. In each analysis, the proportion of eyes achieving a SE or cylinder within 0.25, 0.5, 1.0, 1.5, and 2.0 D of the target at one month (or three months if no one-month data were available) was calculated. Cases were defined as achieving a SE or cylinder error of more than 1.0 D, whereas controls achieved a SE or cylinder error of 1.0 D or less.
Microsoft excel (Mac, Version 16.71, Microsoft, Redmond, Washington) was used to run statistical analyses. In all analyses, Welch’s t-test was used to compare the difference of means between groups due to unequal variance. Chi-square testing was used for differences in proportions of categorical variables. For the purposes of our statistical analysis, significance was defined as p < 0.05.
Results
There were 518 eyes that received a toric IOL implant between 2016 and 2020. Seventy-two eyes were excluded for not meeting the above inclusion criteria. The remaining 446 eyes were analyzed in the study.
UDVA Outcomes
In the UDVA analysis, 80 eyes were excluded for being aimed for near, resulting in 23 cases and 343 controls.
Baseline demographics and biometry data results are demonstrated in Table 1. There were no significant differences between the two groups in sex, eye laterality, age, axial length, anterior chamber depth, astigmatism, or lens power.
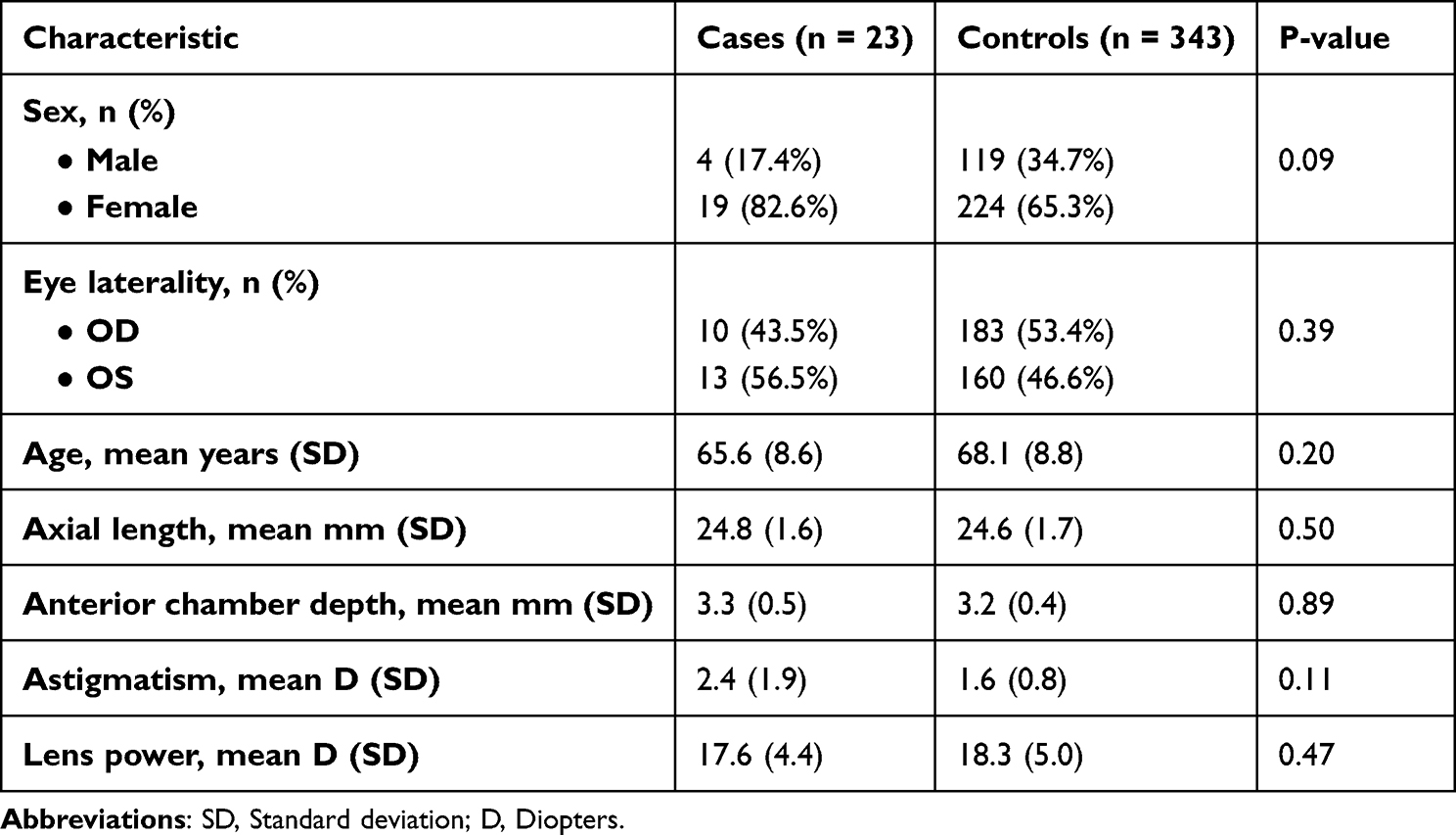 |
Table 1 Baseline Demographics and Biometry Data in the Uncorrected Distance Visual Acuity Analysis |
Pre-operative exam findings and ocular comorbidities in the UDVA analysis are presented in Figure 1. Compared to controls, cases had a significantly higher percentage of eyes with prior LASIK (21.7% vs 7.0%, p = 0.01) and keratoconus (8.7% vs 0.6%, p < 0.001). There was no significant difference between cases and controls in the percentage of eyes with dry eye (43.5% vs 26.2%, p = 0.07), ABMD (13.0% vs 8.5%, p = 0.45), FED (0% vs 14.0%, p = 0.05), and prior RK surgery (0% vs 1.2%, p = 0.60). Although most eyes overall received lower cylinder power toric lenses (T3 and T4), a greater percentage of cases had higher (T5 – T9) cylinder power lenses (39.1%) than controls (17.9%, p < 0.001).
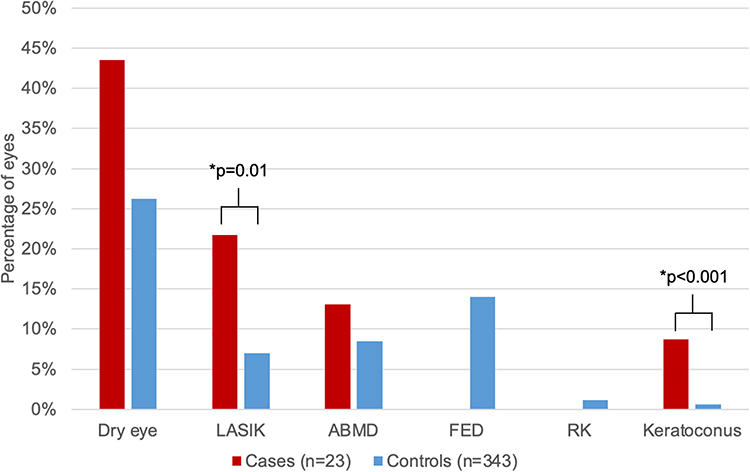 |
Figure 1 Pre-operative exam findings and ocular comorbidities in the uncorrected distance visual acuity analysis. *Denotes statistical significance at the p < 0.05 level. Abbreviations: LASIK, laser assisted in situ keratomileusis; ABMD, Anterior basement membrane dystrophy; FED, Fuchs endothelial dystrophy; RK, Radial keratectomy. |
SE Analysis
In the SE analysis, 57 eyes were excluded for having no clear documented target refraction and 59 patients were excluded for not having a refraction at 1 month or 3 months, leaving 24 cases and 306 controls. Of the 116 excluded eyes, UDVA was 20/15, 20/20, 20/25, 20/30, and 20/40 in 7.8%, 46.6%, 13.8%, 9.5% and 10.3% of eyes, respectively. Of the included eyes, post-operative refraction showed that 46.1%, 73.0%, 92.7%, 96.7%, and 99.4% of eyes were within 0.25, 0.5, 1.0, 1.5, and 2.0 D of target SE, respectively.
Baseline demographics and biometry data results are demonstrated in Table 2. There was a trend towards higher astigmatism in cases (mean 2.4 D, SD 2.0 D) compared to controls (mean 1.5 D, SD 0.7 D, p = 0.05). There were no significant differences between the two groups in sex, eye laterality, age, axial length, anterior chamber depth, Kmean, or lens power.
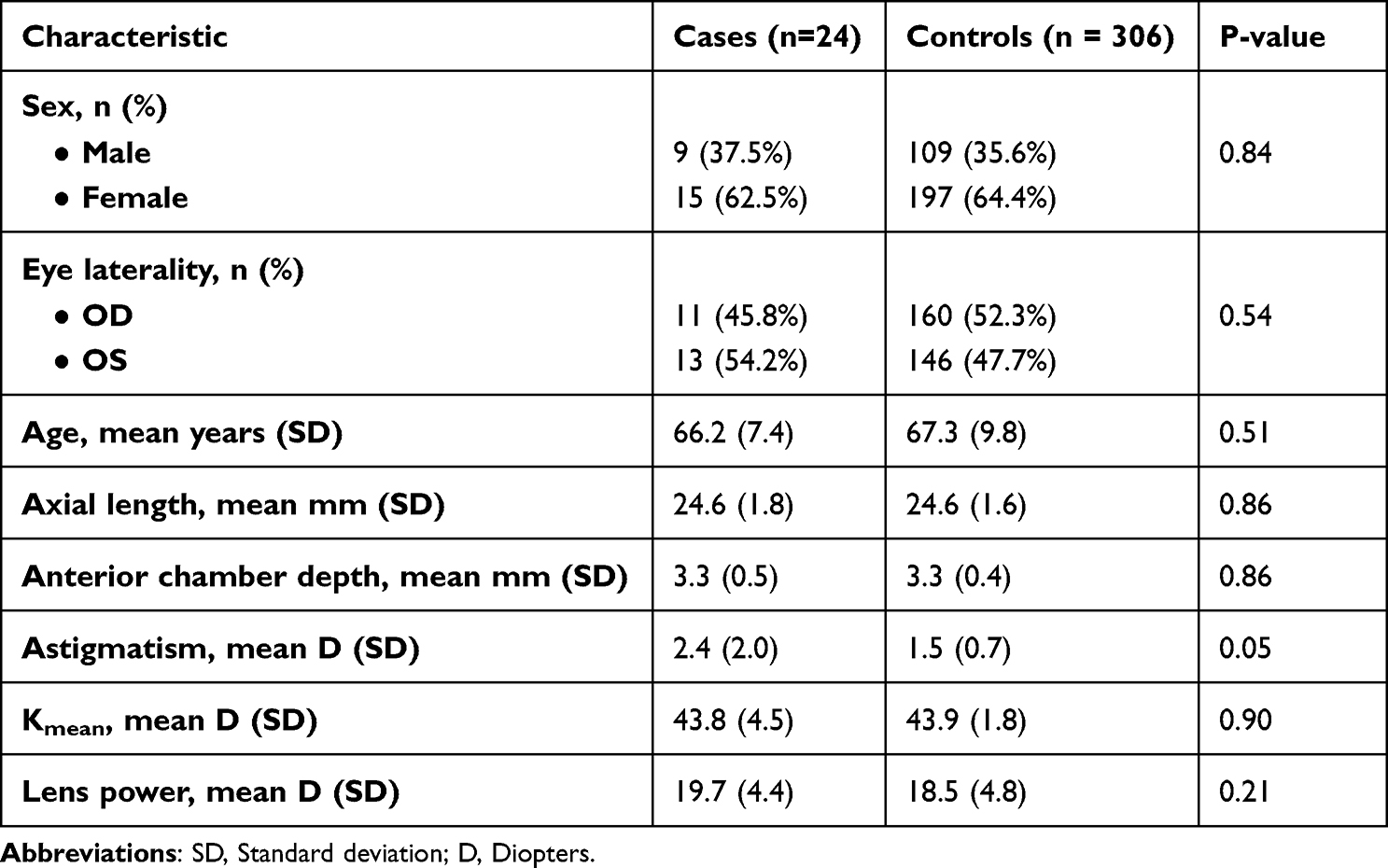 |
Table 2 Baseline Demographics and Biometry Data in Spherical Equivalent Analysis |
Pre-operative exam findings and ocular comorbidities in the SE analysis are presented in Figure 2. Compared to controls, cases had a higher percentage of prior RK (8.3% vs 0%, p < 0.0001) and keratoconus (12.5% vs 0%, p < 0.0001). Cases and controls had a similar percentage of dry eye (20.8% vs 25.2%, p = 0.64), FED (12.5% vs 12.1%, p = 0.95), ABMD (4.2% and 9.5%, p = 0.38), and prior LASIK (20.8% vs 9.8%, p = 0.09). A greater proportion of cases had higher (T5 – T9) cylinder power lenses (37.5%) than controls (17.3%, p = 0.01).
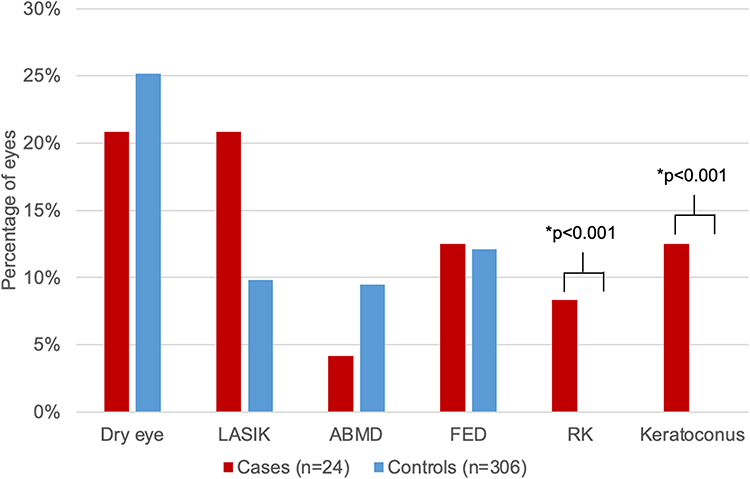 |
Figure 2 Pre-operative exam findings and ocular comorbidities in the spherical equivalent analysis. *Denotes statistical significance at the p < 0.05 level. Abbreviations: LASIK, laser assisted in situ keratomileusis; ABMD, Anterior basement membrane dystrophy; FED, Fuchs endothelial dystrophy; RK, Radial keratectomy. |
Cylinder Analysis
After excluding the same 116 patients for not having a clear target refraction or no refraction at 1 month or 3 months, there were 30 cases and 300 controls in the cylinder analysis. Post-operative refraction showed that 40.6%, 66.4%, 90.9%, 97.9%, and 99.4% of eyes were within 0.25, 0.5, 1.0, 1.5, and 2.0 D of target cylinder, respectively.
Baseline demographics and biometry data results are demonstrated in Table 3. Cases had higher astigmatism (mean 2.3 D, SD 1.6 D) than controls (mean 1.5 D, SD 0.8 D, p = 0.02). There was a difference between cases and controls in the flat K (mean 41.7, SD 2.6 vs mean 43.2, SD 2.0, p = 0.003). There was no difference in the steep K (mean 44.0, SD 2.6 vs mean 44.8, SD 2.2, p = 0.13). There were no significant differences between the two groups in sex, eye laterality, age, axial length, anterior chamber depth, or lens power.
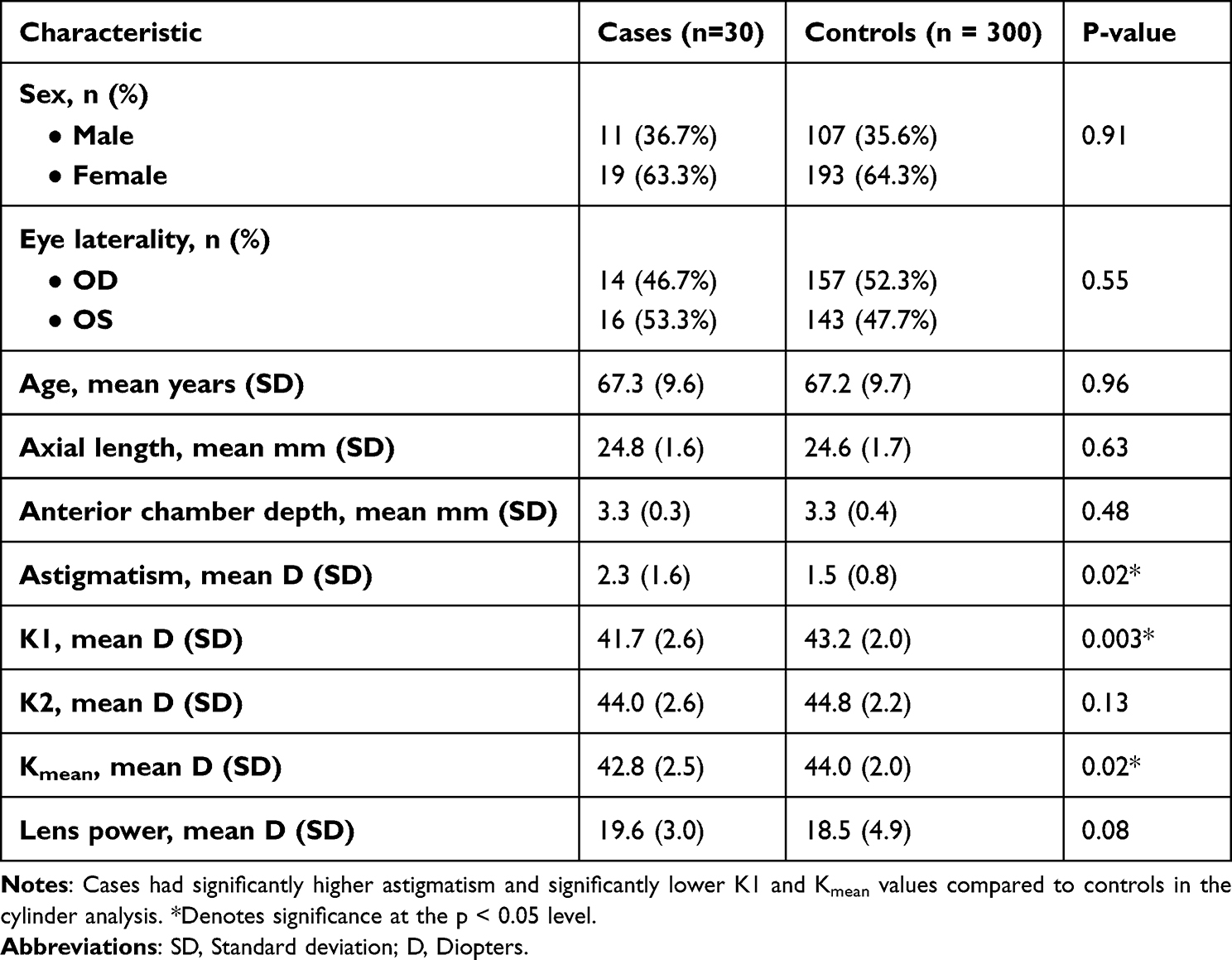 |
Table 3 Baseline Demographics and Biometry Data in Cylinder Analysis |
Pre-operative exam findings and ocular comorbidities in the cylinder analysis are presented in Figure 3. Compared to controls, cases had a higher percentage of prior LASIK (30.0% vs 8.7%, p = 0.0003). Cases and controls had a similar percentage of ABMD (10.0% vs 9.0%, p = 0.86), prior RK (0% vs 0.6%, p = 0.65), keratoconus (0% vs 1%, p = 0.58), dry eye (16.7% vs 25.7%, p = 0.28), and FED (6.7% vs 12.7%, p = 0.34). A greater percentage of cases had higher (T5 – T9) cylinder power lenses (46.7%) than controls (16.0%, p < 0.0001).
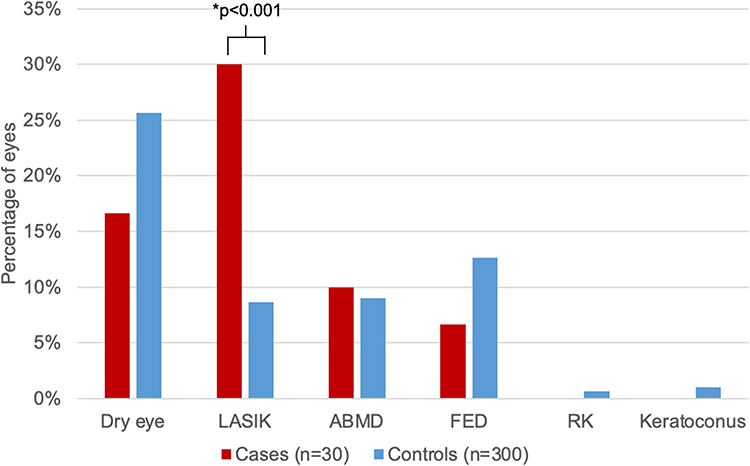 |
Figure 3 Pre-operative exam findings and ocular comorbidities in the cylinder analysis. *Denotes statistical significance at the p < 0.05 level. Abbreviations: LASIK, laser assisted in situ keratomileusis; ABMD, Anterior basement membrane dystrophy; FED, Fuchs endothelial dystrophy; RK, Radial keratectomy. |
IOL master measurements were used to select the lens in 28 of the 30 cases. Pentacam (Oculus, Wetzlar, Germany) or Orbscan II (Orbtek, Bausch and Lomb, Odessa, Florida) measurements were also taken in 22 of those cases, and the measurements agreed with the IOL master measurements (defined as within 0.6 D difference in K1 and K2 values and axis within 10 degrees) in 14 (64%) cases. Using measurements obtained by Pentacam or Orbscan likely would have resulted in a residual cylinder of < 1 D in 4 cases (18%).
Discussion
This study aimed to analyze toric refractive outcomes in a large cohort of patients and determine which factors may lead to suboptimal results. Overall, a majority of patients experienced favorable outcomes, with 93.7% of eyes achieving UDVA of 20/40 or better, 92.7% of eyes refracting to within 1 D of target SE, and 90.9% of eyes refracting to within 1 D of target cylinder 1 month or 3 months after surgery. These results are similar to other published studies, in which 90–95% of patients attain UDVA of 20/40 or better.9–11 In the literature, 81–100% of patients achieve a SE within 1D of target.11,18–22 Eighty-eight percent of patients fall within 1D of target cylinder,10 and 71–92% of patients fall within 0.5 D of target cylinder.12–15
Despite these good results, our study found that certain factors, including prior LASIK and RK surgery, keratoconus, higher astigmatism, and higher toric cylinder power lenses (T5-T9) were each associated with suboptimal outcomes.
Eyes with prior LASIK made up a higher proportion of cases than controls in the UDVA and cylinder analyses. A review and expert opinion paper by Wang et al found that 80% of eyes with previous myopic LASIK or PRK and 84% of previous hyperopic LASIK or PRK that received toric lenses attained 0.5 D or less postoperative astigmatism.23 LASIK changes the central corneal steepness and the relationship between the anterior and posterior corneal curvature, making measurement of corneal power less accurate.24 Myopic ablation causes IOL calculation formulas to predict a shallower anterior chamber depth and more anterior effective lens position, leading to an underestimated IOL power and hyperopic surprise.24 The opposite phenomenon occurs with hyperopic ablations. Traditional formulas like the SRK/T and Holladay 1 will recommend inaccurate IOL power for these patients.24,25 Many surgeons will try to obtain pre-refractive data, generate IOL prediction with several different formulas, or shift their target refraction in the direction of the LASIK ablation.24 Despite the measurement inaccuracies introduced by LASIK, one study found that 84% of eyes with toric implants had a refractive astigmatism of less than 0.5 D.26 We recommend using Scheimpflug imaging measurements for astigmatism and the anterior and posterior corneal power in the ASCRS online IOL calculator to select the best IOL power.27 In our cylinder analysis, using Scheimpflug measurements instead of IOL master measurements could have eliminated significant cylinder refractive error in 18% of cases. Interoperative aberrometry may also help refine outcomes.
Prior RK was more common in cases than controls in the SE analysis. According to Wang et al, only 69% of eyes with prior RK implanted with a toric lens achieved 0.5 D or less postoperative astigmatism.23 Like LASIK, prior RK has the potential to disrupt IOL calculations. Corneas destabilized by RK may also develop hyperopic drift and irregular astigmatism over time.24 Cataract surgery with any type of IOL is more risky in these eyes as RK incisions may open during surgery, causing leakage requiring additional sutures and worsened astigmatism.24 Specific and detailed informed consent should be obtained from these patients.
Keratoconus was more prevalent in cases than controls in the UDVA and SE analyses. A study of 32 eyes with keratoconus implanted with toric IOLs found that 71.9% of cases achieved UDVA of at least 20/40.28 A meta-analysis revealed that the percentage of eyes with keratoconus and a toric lens implant achieving within 1 D of target SE was between 57% and 100% for stage I keratoconus and 50 to 100% in stage II keratoconus.29 Irregular corneal astigmatism in keratoconus can increase the chance of inaccurate keratometry measurements.30 Conventional biometry often will overestimate corneal power, leading to an underpowered IOL and hyperopic surprise.30,31 These effects, as well as decreased replicability between measurements, are most pronounced in eyes with a Kmax > 55 D.30 Luckily, the Barrett Universal II formula can decrease the amount of error in mild to moderate keratoconus patients.30–32 Toric IOLs may be appropriate for patients with stable topography, no apical scarring, and no highly irregular astigmatism. We recommend using Scheimpflug imaging values for true corneal power, astigmatism, and axis at the 4 mm zone if these measurements are significantly different from those obtained by optical aberrometry.
Finally, cases tended to have higher pre-operative corneal astigmatism and higher toric lens cylinder power than controls. These outcomes are likely due to issues with rotational instability of the toric IOL.33,34 It is known that misalignment from the intended axis decreases the cylindrical corrective power of a toric IOL.35,36 These changes disproportionately affect higher cylinder lens powers. Unfortunately, due to our study’s retrospective nature, post-operative toric rotation was not documented and therefore could not be included in the analysis. Interestingly, greater axial length and anterior chamber depth, which may provide more room for lens rotation to occur, were not associated with worse UDVA or higher SE or cylindrical error.
Several comorbidities were not associated with poorer outcomes. Dry eye was present in a similar proportion of cases and controls in all three analyses. Dry eye disrupts the ocular surface, which can affect IOL calculations, toric IOL axis, keratometry, and topography.37 Cataract surgery itself can exacerbate dry eye, as prolonged operation time and light exposure both lead to a diminished mean goblet cell density and tear break up time.37 Eye drops prescribed post-operatively may reduce goblet cell density.37 Worsened dry eye after surgery may lead to decreased post-operative UDVA. Our favorable outcomes may stem from aggressive treatment of dry eye disease for at least four weeks before obtaining pre-operative measurements, instilling artificial tears on the eye right before measurements are taken, and even delaying surgery until the dry eye is under optimal control.
ABMD eyes also made up similar proportions of cases and controls in all three analyses. The surface irregularities found in ABMD may induce irregular astigmatism, causing errors in keratometry and IOL calculations.38 Severe or central ABMD may warrant treatment with epithelial debridement and bandage contact lens placement before cataract surgery.38 Stable refraction and topography can reassure the surgeon that this condition will not significantly affect post-operative outcomes. Our favorable outcomes may be due to excluding patients with severe ABMD or pre-treating these patients with superficial keratectomy three months before their pre-operative measurements. We also use a minimum of three different modalities to measure their pre-operative corneal power, including Scheimpflug, IOL master, autorefractor, and manual K measurements.
There was no statistically significant difference in the proportion of FED eyes between cases and controls in all analyses. Admittedly, the number of FED patients in this study is low. Cataract surgery in patients with FED can cause the cornea to decompensate, leading to edema and cloudy vision. Eyes with FED also have a flatter and more spherical posterior cornea, reducing negative power.39 These findings increase the chance of a hyperopic shift after endothelial keratoplasty surgery, so surgeons often aim these patients more myopic in case they need future endothelial keratoplasty. The axes of anterior and posterior corneal astigmatism may change after toric IOL implantation due to FED progression or subsequent endothelial keratoplasty, affecting the ability of the toric IOL to correct the patient’s astigmatism.39 In eyes that undergo concurrent toric lens implantation and DMEK, only 61.5% achieve UDVA better than 20/40.40 However, in our study, eyes with FED generally had favorable outcomes, perhaps because they were milder cases.
We suggest obtaining IOL master and Pentacam imaging on all potential toric candidates. IOL master measurements may be used with the Barrett Universal II formula to select the IOL lens power and toric power if they are within 0.6 D of those obtained by Pentacam imaging. However, if significant differences exist, certain factors like dry eyes may need to be optimized and repeat imaging obtained to get the most accurate measurements. In cases of keratoconus, we recommend using Scheimpflug imaging values for true corneal power, astigmatism, and axis at the 4 mm zone if measurement differences persist. Lastly, Scheimpflug imaging measurements for astigmatism and the anterior and posterior corneal power in the ASCRS online IOL calculator should be used for post-refractive eyes.
Our study had several key strengths that help it contribute to the field of cataract surgery research. It involved a large cohort of 446 eyes, making it adequately powered to help find differences between the two comparison groups. In addition, because every patient was operated on by the same surgeon, differences in outcomes due to surgical technique are unlikely.
The main limitations of our study are due to its retrospective nature. Some patients were excluded from the SE and cylindrical analysis for not having a listed target refraction or post-operative refraction at one month or three months. A majority of patients without post-operative refraction had an UDVA of 20/20 or better. However, even with their exclusion, our numbers were still high enough to find significant differences between the study and control groups.
Conclusion
Our study found that most patients undergoing toric lens implantation have favorable outcomes as measured by UDVA, residual SE, and residual cylinder. Prior LASIK or RK surgery, keratoconus, and higher astigmatism may increase the chance of a suboptimal outcome. By recognizing these factors, surgeons can better counsel patients about expectations after surgery. Future studies taking a prospective approach to affirm or find new factors related to suboptimal toric outcomes are warranted.
Funding
This work was funded by the Medical Student Training in Aging Research (MSTAR) Program and by an unrestricted grant from the Rosenthal Family.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Congdon N, O’Colmain B, Klaver CCW, et al.; Eye Diseases Prevalence Research Group. Causes and prevalence of visual impairment among adults in the United States. Arch Ophthalmol. 2004;122(4):477–485.
2. Vision Problems in the U.S. Prevent blindness America and National Eye Institute; 2012. Available from: http://www.visionproblemsus.org.
3. Hoffmann PC, Hütz WW. Analysis of biometry and prevalence data for corneal astigmatism in 23,239 eyes. J Cataract Refract Surg. 2010;36(9):1479–1485. doi:10.1016/j.jcrs.2010.02.025
4. Mohammadi M, Naderan M, Pahlevani R, Jahanrad A. Prevalence of corneal astigmatism before cataract surgery. Int Ophthalmol. 2016;36(6):807–817. doi:10.1007/s10792-016-0201-z
5. Wolffsohn JS, Bhogal G, Shah S. Effect of uncorrected astigmatism on vision. J Cataract Refract Surg. 2011;37(3):454–460. doi:10.1016/j.jcrs.2010.09.022
6. Mohammad-Rabei H, Mohammad-Rabei E, Espandar G, et al. Three methods for correction of astigmatism during phacoemulsification. J Ophthalmic Vis Res. 2016;11(2):162–167. doi:10.4103/2008-322X.183924
7. Carvalho M, Suzuki S, Freitas L, Branco B, Schor P, Lima A. Limbal relaxing incisions to correct corneal astigmatism during phacoemulsification. J Refract Surg. 2007;23(5):499–504. doi:10.3928/1081-597X-20070501-14
8. Kessel L, Andresen J, Tendal B, Erngaard D, Flesner P, Hjortdal J. Toric intraocular lenses in the correction of astigmatism during cataract surgery: a systematic review and meta-analysis. Ophthalmology. 2016;123(2):275–286. doi:10.1016/j.ophtha.2015.10.002
9. Roensch MA, Charton JW, Blomquist PH, Aggarwal N, McCulley J. Resident experience with toric and multifocal intraocular lenses in a public county hospital system. J Cataract Refract Surg. 2012;38(5):793–798. doi:10.1016/j.jcrs.2011.11.043
10. Holland E, Lane S, Horn JD, Ernest P, Arleo R, Miller K. The AcrySof toric intraocular lens in subjects with cataracts and corneal astigmatism; a randomized, subject-masked, parallel-group, 1-year study. Ophthalmology. 2010;117(11):2104–2111. doi:10.1016/j.ophtha.2010.07.033
11. Dardzhikova A, Shah CR, Gimbel HV. Early experience with the AcrySof toric IOL for the correction of astigmatism in cataract surgery. Can J Ophthalmol. 2009;44(3):269–273. doi:10.3129/i09-048
12. Ahmed IIK, Rocha G, Slomovic AR, et al.; Canadian Toric Study Group. Visual function and patient experience after bilateral implantation of toric intraocular lenses. J Cataract Refract Surg. 2010;36(4):609–616. doi:10.1016/j.jcrs.2009.10.044
13. Poll JT, Wang L, Koch DD, Weikert M. Correction of astigmatism during cataract surgery: toric intraocular lens compared to peripheral corneal relaxing incisions. J Refract Surg. 2011;27(3):165–171. doi:10.3928/1081597X-20100526-01
14. Ernest P, Potvin R. Effects of preoperative corneal astigmatism orientation on results with a low-cylinder-power toric intraocular lens. J Cataract Refract Surg. 2011;37(4):727–732. doi:10.1016/j.jcrs.2010.11.026
15. Davison JA, Potvin R. Refractive cylinder outcomes after calculating toric intraocular lens cylinder power using total corneal refractive power. Clin Ophthalmol. 2015;19(9):1511–1517.
16. Kaur M, Shaikh F, Falera R, Titiyal J. Optimizing outcomes with toric intraocular lenses. Indian J Ophthalmol. 2017;65(12):1301–1303. doi:10.4103/ijo.IJO_810_17
17. Gomes JAP, Tan D, Rapuano J, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359–369. doi:10.1097/ICO.0000000000000408
18. Xue K, Jolly JK, Mall SP, Haldar S, Rosen P, MacLaren R. Real-world refractive outcomes of toric intraocular lens implantation in a United Kingdom national health service setting. BMC Ophthalmol. 2018;18(30):30. doi:10.1186/s12886-018-0692-7
19. Naripthaphan P, Pachimkul P, Chantra S. Comparison of visual outcomes for aspheric and spherical toric intraocular lens implantation in cataract patients with pre-existing corneal astigmatism: a randomized control trial. J Med Assoc Thai. 2014;97:S102–S110.
20. Kim MH, Chung TY, Chung ES. Long-term efficacy and rotational stability of AcrySof toric intraocular lens implantation in cataract surgery. Korean J Ophthalmol. 2010;24(4):207–212. doi:10.3341/kjo.2010.24.4.207
21. Mendicute J, Irigoyen C, Ruiz M, Illarramendi I, Ferrer-Blasco T, Montes-Mico R. Toric intraocular lens versus opposite clear corneal incisions to correct astigmatism in eyes having cataract surgery. J Cataract Refract Surg. 2009;35(3):451–458. doi:10.1016/j.jcrs.2008.11.043
22. Mendicute J, Irigoyen C, Aramberri J, Ondarra A, Montes-Mico R. Foldable toric intraocular lens for astigmatism correction in cataract patients. J Cataract Refract Surg. 2008;34(4):601–607. doi:10.1016/j.jcrs.2007.11.033
23. Wang L, Koch D. Intraocular lens power calculations in eyes with previous corneal refractive surgery: review and expert opinion. Ophthalmol. 2021;128(11):e121–e131. doi:10.1016/j.ophtha.2020.06.054
24. Patel R, Karp CL, Yoo SH, Amescua G, Galor A. Cataract surgery after refractive surgery. Int Ophthalmol Clin. 2016;56(2):171–182. doi:10.1097/IIO.0000000000000106
25. Mori Y, Shimizu K, Minami K, Kamiya K, Shoji N, Miyata K. Relationship of corneal asphericity to intraocular lens power calculations after myopic laser in situ keratomileusis. J Cataract Refract Surg. 2016;42(5):703–709. doi:10.1016/j.jcrs.2016.01.050
26. Cao D, Wang L, Koch DD. Outcome of toric intraocular lenses implanted in eyes with previous corneal refractive surgery. J Cataract Refract Surg. 2020;46(4):534–539. doi:10.1097/j.jcrs.0000000000000089
27. Mustafa O, Prescott C, Alsaleh F, Dzhaber D, Daoud Y. Refractive and visual outcomes and rotational stability of toric intraocular lenses in eyes with and without previous ocular surgeries: a longitudinal study. J Refract Surg. 2019;35(12):781–788. doi:10.3928/1081597X-20191021-03
28. Ton Y, Barrett G, Kleinmann G, Levy A, Assia E. Toric intraocular lens power calculation in cataract patients with keratoconus. J Cataract Refract Surg. 2021;47(11):1389–1397. doi:10.1097/j.jcrs.0000000000000638
29. Yahalomi T, Achiron A, Hecht I, et al. Refractive outcomes of non-toric and toric intraocular lenses in mild, moderate, and advanced keratoconus: a systematic review and meta-analysis. J Clin Med. 2022;11(9):2456. doi:10.3390/jcm11092456
30. Allard K, Zetterberg M. Implantation of toric intraocular lenses in patients with cataract and keratoconus: a case series. Int Med Case Rep J. 2018;11:185–191. doi:10.2147/IMCRJ.S174315
31. Wang KM, Jun AS, Ladas JG, Siddiqui A, Woreta F, Srikumaran D. Accuracy of intraocular lens formulas in eyes with keratoconus. Am J Ophthalmol. 2020;212:26–33. doi:10.1016/j.ajo.2019.11.019
32. Nanavaty MA, Lake DB, Daya SM. Outcomes of pseudophakic toric intraocular lens implantation in keratoconic eyes with cataract. J Refract Surg. 2012;28(12):884–889. doi:10.3928/1081597X-20121106-02
33. Chang DF. Comparative rotational stability of single-piece open-loop acrylic and plate-haptic silicone toric intraocular lenses. J Cataract Refract Surg. 2008;34(11):1842–1847. doi:10.1016/j.jcrs.2008.07.012
34. Till JS, Yoder PR Jr, Wilcox TK, Spielman JL. Toric intraocular lens implantation: 100 consecutive cases. J Cataract Refract Surg. 2002;28(2):295–301. doi:10.1016/S0886-3350(01)01035-5
35. Novis C. Astigmatism and toric intraocular lenses. Curr Opin Ophthalmol. 2000;11(1):47–50. doi:10.1097/00055735-200002000-00007
36. Alpins NA. Vector analysis of astigmatism changes by flattening, steepening, and torque. J Cataract Refract Surg. 1997;23(10):1503–1514. doi:10.1016/S0886-3350(97)80021-1
37. Chuang J, Shih KC, Chan TC, Wan K, Jhanji V, Tong L. Preoperative optimization of ocular surface disease before cataract surgery. J Cataract Refract Surg. 2017;43(12):1596–1607. doi:10.1016/j.jcrs.2017.10.033
38. Yeu E, Cuozzo S. Matching the patient to the intraocular lens: preoperative considerations to optimize surgical outcomes. Ophthalmology. 2021;128(11):e132–e141. doi:10.1016/j.ophtha.2020.08.025
39. Kaup S, Pandey SK. Cataract surgery in patients with Fuchs’ endothelial corneal dystrophy. Community Eye Health. 2019;31(104):86–87.
40. Yokogawa H, Sanchez PJ, Mayko ZM, Straiko M, Terry M. Astigmatism correction with toric intraocular lenses in descemet membrane endothelial keratoplasty triple procedures. Cornea. 2017;36(3):269–274. doi:10.1097/ICO.0000000000001124
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Photorefractive Keratectomy Enhancement (PRK) After Small-Incision Lenticule Extraction (SMILE)
Moshirfar M, Parsons MT, Chartrand NA, Lau CK, Stapley S, Bundogji N, Ronquillo YC, Hoopes PC
Clinical Ophthalmology 2022, 16:3033-3042
Published Date: 12 September 2022
Prospective, Randomized, Fellow Eye-Controlled Study of Postoperative Pain and Inflammation Control with an Intracanalicular Dexamethasone 0.4 mg Ophthalmic Insert Following Small Incision Lenticule Extraction
Jee KJ, Ling J, Bafna S, Chester T, Augustine J, Wiley WF
Clinical Ophthalmology 2022, 16:3895-3904
Published Date: 22 November 2022
Visual Outcomes of a Second-Generation, Enhanced UV Protected Light Adjustable Lens in Cataract Patients with Previous LASIK and/or PRK
Wong JR, Folden DV, Wandling GR, Schaefer S, Stephens J, Boots C, Nichols CJ, Everson MH, Johnson R
Clinical Ophthalmology 2023, 17:3379-3387
Published Date: 6 November 2023
A Comprehensive Retrospective Analysis of EVO/EVO+ Implantable Collamer Lens: Evaluating Refractive Outcomes in the Largest Single Center Study of ICL Patients in the United States
Albo C, Nasser T, Szynkarski DT, Nguyen N, Mueller B, Libfraind L, Parkhurst G
Clinical Ophthalmology 2024, 18:69-78
Published Date: 9 January 2024