Back to Journals » ClinicoEconomics and Outcomes Research » Volume 14
Factors Influencing Willingness to Pay for Insecticidal Treated Bed Nets Among Rural Households of Bugina District North Wollo Zone, North-East Ethiopia
Authors Addis B, Akele W, Minyihun A ![]()
Received 21 December 2021
Accepted for publication 23 March 2022
Published 5 April 2022 Volume 2022:14 Pages 179—187
DOI https://doi.org/10.2147/CEOR.S353999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Banchlay Addis,1 Workye Akele,2 Amare Minyihun1
1Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Malaria Prevention & Control Program Officer, Bugina District Health Office, North Wollo Zone, Ayina, Ethiopia
Correspondence: Banchlay Addis, Email [email protected]
Background and Aim: Understanding potential demand and willingness to pay for the insecticide treated nets is important for sustainable insecticide-treated bed net intervention. However, there is limited evidence, and there is no study in this malarious area, so the study aimed to assess willingness to pay for insecticide-treated bed net and influencing factors.
Methods: A multi-stage community-based cross-sectional study was conducted by using an interview administered questionnaire with a total sample size of 711H.H from March 01 to 30, 2020. The data were entered into EPI data version 4.6.0 and exported to STATA SE version 14 for further analysis. The mean price of willingness to pay was presented as mean and median. Bivariable and multivariable Tobit economical model was used to identify factors associated with willingness to pay. Regression coefficient (ß), 95% CI, t-value and p-value were used to measure the strength and presence of a statistical association.
Results: A total of 683 study participants with a response rate of 96.1% were included in the study. Sixty-four percent of respondents were willing to pay for three types of an insecticide-treated bed net, and the mean price for blue rectangular medium size ITN was 46 (± 12.9) birr, for white circular medium size ITN was 44 (± 12.3) birr and for blue circular medium size ITN was 43 (± 11.8) birr. The factors influencing willingness to pay were sex, educational status, wealth status and knowledge toward malaria and ITN.
Conclusion: This study revealed that in the Bugina district majority of the households were willing to pay for the three types of ITN with a mean price of 55.6 ETB. Sex, educational status, knowledge and wealth index are factors affecting willingness to pay for ITN; further awareness needs to be created regarding the severity of malaria and the demand of ITN.
Keywords: ITN, willingness to pay, Tobit model
Introduction
Malaria remains a first-rate public health threat causing an unacceptable burden on the health and economic welfare of the world’s poorest communities.1,2 It is the most common public health problem in developing countries and imposes great health and socio-economic burden on humanity.3,4 Malaria is mainly associated with altitude and rainfall.5–7 Plasmodium falciparum and P vivax co-exist as major parasite species in Ethiopia.8,9
This epidemiologic feature makes malaria control more difficult than in most African countries where P. vivax has low or null prevalence.2,6,10 Overall, the malaria communicability pattern in the country is seasonal and unstable The disease has been frequently reported as the first leading cause of outpatient visits, hospitalization and death in health facilities across the country, but now the disease is the six leading causes of morbidity and mortality.8,10,11
WHO 2019 report showed that in 2018, an estimated 228million (213million are from the WHO Africa region) cases and 405,000 deaths of malaria occurred worldwide. From the total death, children under five account for 67% (272,000) death rate globally and 94% of child deaths are from the WHO Africa region, and 80% are from sub-Saharan Africa.12 In Ethiopia, 68% of the populations in the territory live in malarious areas covering 75% of the land, and the magnitude of malaria in pregnancy varies from 6.1% to 10.4%, which is a public health concern.13,14 Insecticide-treated nets are mosquito nets treated with insecticides that repel, disable or kill the vector mosquitoes that transmit malaria.15,16 The utilization of Insecticide Treated bed-Nets (ITNs) is one of the effective preventive strategies and cost-intervention against malaria recommended by the World Health Organization17 with the aim to provide one ITN for every two people for preventing malaria infection and its consequences during pregnancy.18–20 ITNs have proven to be a valuable and cost-effective method of protection against malaria, and it is effective in decreasing approximately 50% of malaria episodes among children under-five years of age and a 17% reduction in all-cause mortality.21,22 It also protects individuals who reside within a few meters of ITN using households. IRS can be combined with ITN in places where vectors become resistant to the insecticides used to impregnate net fabrics.23–25
In Ethiopia, the two dominant malaria prevention strategies implemented are targeted IRS with the distribution of ITNs for universal coverage.26 Though ITN is currently distributed freely to rural communities through health posts and kebeles to prevent malaria and other diseases, the country faces problems on universal coverage and sustainability of ITN at the household level. Therefore to increase utilization habit and sustainability of the program, the Federal Ministry of Health has developed a national five-year strategic plan for the prevention and control of malaria in Ethiopia, which is a plan to be implemented by providing subsidies to those not able to pay and by charging fees for the remaining population. There are some Debates on ITN distribution making free or with payment for sustainability of the service most of the findings try to support freely distribution though till now there is no clear decision to freely distribute the service rather focus on subsidy.27,28
Introducing a Subsidized ITN market rather than the free distribution for all should be considered to ensure sustainability and Self-reliance in the prevention and control of malaria. Thus assessing the level of WTP is a method help to determine the contribution and subsidized amount. Previous finding in in northern and southern part of Ethiopia revealed that about that 68.5% and 86% of persons had willingness to buy Insecticide-Treated Nets if they have access to these Nets.29,30
In Ethiopia, there were limited studies on WTP for malaria control interventions, especially on ITN and in this malarious area. In addition, the model used to estimate the amount of willingness to pay was not advanced and considered censored; therefore, this study determined the level of WTP for ITN and identified factors affecting WTP with Tobit econometric model in the Bugina district. Which help policymakers and program planners generate relevant information for an evidence-based redesign of malaria control policies and strategies.
Methods
Study Area and Period
The study was conducted in the Bugina district, which is one of the 14 districts of North Wollo Zone, Amhara region. Ayina is the town of the district and is located at a distance of 354 km from regional town Bahir-Dar in the west direction. The total catchment area of the district is 1159.36 Km2. The climatic zone of the district is 16.2% Dega, 82.3% Woynadega and 1.5% kola. The town is situated between 18˚43ꞌ N latitude and 38˚40ꞌE longitude with an altitude of 1336–2827 meters above sea level. According to the 2016 census projection, currently, the district has a total population of 94,261 and 21,921 households. The district is one of the most malarious, drought-affected and food insecure areas in the region and targeted under Sekota declaration. Now a day, four health centres and 16 health posts are found in the district.31
A multi-stage Community-based cross-sectional study was conducted from February 21 to March 07, 2020. The source population were all household heads living in all Kebeles of Bugina District. During the study period, the study population were all households living in the four/4/ selected kebeles of Bugina district during the study period. Households living in the kebeles less than 6 months during the study period were excluded.
For estimating sample size of willingness to pay for three different types of ITN, calculating with using Mean formula based on a previous study done on Arba Minch Zuria district of SNNPR with a formula of (Za/2)2 *(SD)2/(d)2; 95% confidence interval (CI) (Z α/2=1.96), SD standard deviation and the 5% error margin. Therefore sample size of WTP for Blue rectangular ITN/711/ is greater than other types of ITN and their determinant factors, so 711 is the maximum sample size.30
From the total 16 malaria-endemic kebeles of Bugina District, four kebeles were selected by simple random sampling for the first stage. The study household was selected using systematic random sampling from the selected kebeles through the proportional allocation method in the second stage. Then, the first household was selected randomly by the lottery method for the interval of K=10. When the household owner was unavailable during the data collection period, it was skipped and went to the other households by keeping the pattern. The skipped households were considered again and, if not available, was registered as non – response rate.
Data Collection Tools and Procedure
The tool was a pre-tested interview administered structured questionnaire adapted from reviewing different literature, and it is prepared in English and translated to Amharic. For every respondent, one Medium size rectangular, white and blue conical ITN will be prepared for demonstration in order to elicit their preferences. The head of the household or one adult member representative of the study household were interviewed. The questionnaire has four parts: The first part would assess the respondent’s socio-demographic characteristics. The second part of the questionnaire would assess the wealth index; the third part dealt with malaria-related variables, including knowledge attitude on transmission and prevention, previous history of illness and previous source and possession of ITN. The fourth part of the questionnaire would assess the ability to pay of the respondent in terms of their wealth status and other variables. The bid contingent valuation method using binary with follow-up was used through household survey mechanisms to assess their willingness to pay. Then respondents were asked a yes or no question of their willingness to pay for the ITN at a certain price 21. If a respondent was unwilling to pay, he/she was asked the main reasons for the refusal. Whereas if the respondent is willing to pay a specific amount, the question is repeated using a higher or lower bid value depending on the response to the first question.
Principal components analysis was used to analyze wealth index status based on each household’s ownership of various assets, and each household was assigned a socio-economic quintile rank as poor, medium and rich.
Data were collected by four clinical nurses working at the health center level using a structured and pre-tested questionnaire with face to face interviews.
Data Quality Control
Data quality was controlled by providing two-day training to the data collectors and supervisors (3 BSc Nurses) about the study’s overall objective, the definition of terms and concepts, the approach of respondents, data collection tools, and techniques of interviewing.
After training, a pre-test was done to assess the applicability of procedures and tools on 5% of participants in “Lasta woreda” near Bugina Woreda, which has the same socio-demographic and economic status. Finally, the necessary revision or corrective modifications was done on the questionnaire depending on the pre-test result. The principal investigator and supervisors performed close site supervision during the whole data collection period. The collected data was also checked for completeness, consistency, accuracy, and clarity on a daily basis.
Data Processing and Analysis
The data was entered using EPI data version 4.6.0 and cleaned, recoded and exported to STATA SE version 14 software packages for analysis. For descriptive part frequency, mean and standard deviation were used to show the distribution of the outcome variables and associated factors. The Tobit Econometric model was used to analyze the determinants of willingness to pay and the maximum amount of money individuals was willing to pay. The maximum amount of money the respondent will be paid is given by Y = 1 if MWTP =β0 + βiXi + ԑ>0, and Y=0, if MWTP≤0.
Where Y=outcome of WTP for ITN, MWTP= maximum willingness to pay, Xi= Explanatory variable, β0= slope, βi=coefficient, ԑ= error term, 1= success/yes, 0= failure /No.
The model also estimates the marginal effect of an explanatory variable on the expected value of the dependent variable. To be free from serious data error, the assumptions of the Tobit model like independence, normality and equal variance were tested. Variables with a p-value of less than 0.2 during bivariate analysis were considered for the multiple regression analysis. 95% CI, regression coefficient (ß-coefficient), t-value and p-value were used to measure the strength and presence of statistical association.
Operational Definition
ITN;- Insecticide-treated nets are mosquito nets treated with insecticides that repel, disable or kill the vector mosquitoes which transmit malaria.
Willingness to pay: is the maximum amount a person or household would be willing to pay for a good or service and will be measured by using, Bid contingent valuation method, where the respondent is first asked whether they would be willing to pay a specific amount and then the question is repeated using a higher or lower bid value depending on the response to the first question.
Wealth status: The wealth status of households will be computed by Principal Component Analysis (PCA) and will be divided into equal parts (three tires) as poor, medium and rich wealth status.
Knowledge about malaria: Awareness of respondents about basic information of malaria transmission as well as the prevention of malaria and supported by a Yes/No or a one specific response type of question and supported by 16 questions. If an individual answer 50% of questions correctly, he or she is considered knowledgeable.
Attitude towards malaria and ITN: Is feelings of respondents towards different aspects of ITN. And its question is designed by more than one response type and weights up to 25. If an individual answers 50% of questions correctly, he or she is considered to have a good attitude.
Ethical Consideration
Ethical approval was obtained from the Ethical Review Board of the Institute of Public Health, College of Medicine and Health Science, University of Gondar. Permission letters were obtained from the University of Gondar comprehensive specialized hospital. All study participants were oriented on the objectives and purpose of the study before study participation. Confidentiality and anonymity were explained. Patients at health facilities and sick individuals were informed that participation had no impact on their health care provision. Written informed consent was obtained, and study team members safeguarded the confidentiality and anonymity of study participants throughout the entire study. To ensure participant privacy, interviews were conducted in quiet areas, enclosed whenever possible. To protect the identities of the study participants, each participant was given a unique identification number (ID). Participation in the study was voluntary, and individuals were free to withdraw or stop the interview at any time.
Result
Socio-Demographic and Economic Characteristics of the Respondents
A total of 683 study participants with a response rate of 96.1% were included in the study. The respondents’ mean age (SD) was 42 (±14) years. The majority of respondents were male 512 (75.29%), Orthodox Christian followers 670 (98.5%) and 75.7% (515) were Farmers in occupation status. The mean (SD) family size of the respondent is 4.5 (±1.7) see (Table 1).
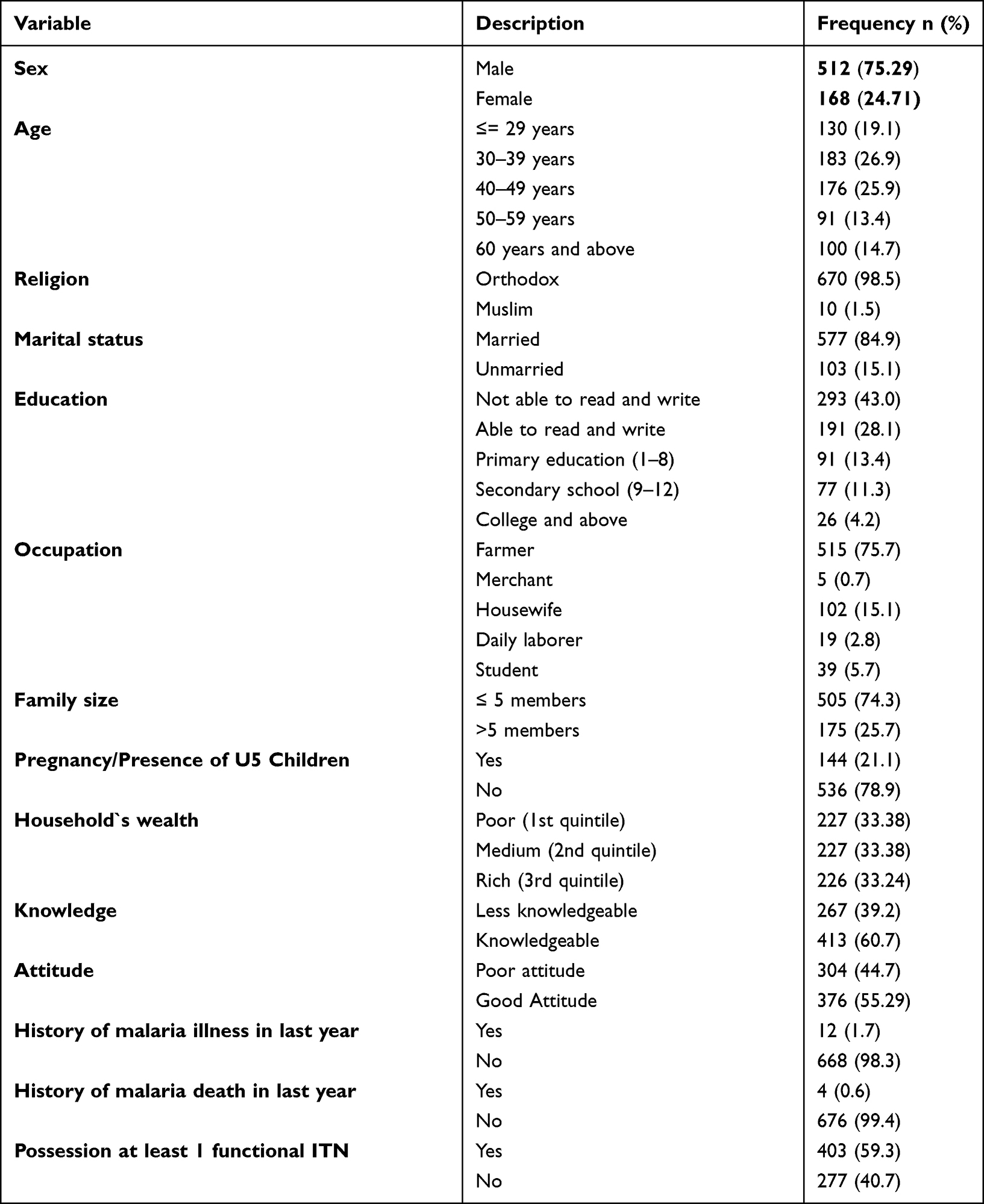 |
Table 1 Socio- Demographic, Economic and Individual Factors of Study Participants in Bugina District Northeast Ethiopia, 2020 (n=683) |
Willingness to Pay Characteristics of Study Participants
Among all the respondents, 435 (64%) were willing to pay, whereas 245 (36%) were unwilling to buy any of the three types of ITN if supplied by the market. The common and frequently replied reasons for their unwillingness were being the inability to afford 170 (69.4%) and says they do not bother much for the disease 72 (29.4%) and the rest 3 (1.2%) says we have not confidence on it.
The willingness to pay for three different types of ITN was evaluated; 435 household owners were willing to buy ITN, the mean willingness to pay for the three/3/ different types of ITN is slightly different. For blue circular medium size ITN, households are willing to pay at a mean price of 43 (SD ±11.8) ranges from 10–75 ETB birr, for blue rectangular medium size ITN at a mean of 46 (SD ±12.9) ranges from 10–85 birr and for white circular medium size, ITN 44 (SD ±12.3) birr ranges from 10–80 Ethiopian birr.
More than 60% of the household owners were willing to buy also for other families members, and the preferred site to buy ITN was 286 (66.2%) from kebele/health post level/ 286 (66.2%), health center 134 (31%) and shops/other were 14 (2.8%). When we see the season of malaria, more than half of the respondents were willing to buy ITN at the beginning of the year, middle of the year 64 (14.8%) and the end of the year 148 (34%).
Factors Associated with the Willingness to Pay for ITNs
During Bivariable analysis, age, sex, educational status, knowledge, awareness, attitude and wealth index variables were significant with a p-value of less than 0.2, which were considered for the multiple regression analysis. In the multivariable Tobit econometrical regression, sex, educational status, wealth index, and knowledge about ITN and malaria were the factors associated with willingness to pay for insecticidal treated bed nets at a p-value ≤ 0.05 (Table 2).
 |
Table 2 Maximum Likelihood of Tobit Econometrical Analysis of Factors Associated with MWTP for Blue Rectangular ITN in Bugina District, 2020 |
4.34 Birr decreased the ITN WTP value of households for those female respondents than male respondents held other variables constant. The marginal effect result shows that when the household heads/respondents were male, it will increase the probability of willingness of a household to pay for ITN by 0.72 birrs from the average value ß= −4.34, probability of marginal effect=−0.72, (CI = −8.60, −0.076) and p-value=0.046).
Respondents who had formal education were 7.68 Birr more willing to pay than those who did not have formal education. The marginal effect of this variable reveals that If the respondents have formal education, the probability of paying for the ITN will increase by 3.58 birr from the average WTP value (ß=7.68, probability of marginal effect=3.58, (CI=−3.34, 12.02) and p-value=0.001).
Households with good knowledge about ITN and malaria prevention were 7.23 birr more willing to pay than those with poor knowledge about ITN. The marginal effect of this variable reveals that participants who have good knowledge about ITN increase the probability to pay by 3.84 birrs from the average WTP (ß=7.23, probability of marginal effect=3.84, (CI=3.64 10.81) and p-value=0.000).
Rich household heads were willing to pay 7.98 Birr more than their counterparts. The marginal effect of this variable reveals that rich participants increase the probability of paying for ITN by 3.84 birrs from the average WTP (ß=7.98 probability of marginal effect=3.84, (CI=3.92, 12.03) and p-value=0.001). See (Table 2).
Discussion
Determining willingness to pay for ITN helps to maximize the sustainability of distribution and better control of malaria. This study revealed that around 64% (95% CI= 60.36, - 67.64) of the respondents were willing to buy ITNs if supplied by the market at a reasonable price. This is consistent with similar studies conducted in Ethiopia that is Berehet district and lower than the study conducted at Arba Minch district, which is 86% of households are willing to pay for the three different types of ITN.29,30,32 The possible explanation may be attributed to differences in the study areas and time of study with the Arba Minch district. However, this study is greater than studies conducted in sub-Saharan Africa, which ranges from 0.8 to 32.7% and studies conducted in Tanzania, only 40% were willing to pay.13,33 The possible reason for their difference might be differences in economic status, time, and demographic situations of the source population and differences in malaria severity and prevention practice habit of the country.
The average MWT for the three different types of ITN were (43 ETB for blue circular ITN, 55.6 ETB for blue rectangular ITN and 46.7 ETB for white circular ITN). Which were greater than previous studies in Ethiopia Arba Minch district, for blue circular 26.4 ETB, for blue rectangular ITN, 13.6 ETB and for white circular ITN 25.6 ETB and studies were done at Berehet district, for blue circular ITN average MWT were 30 ETB, blue rectangular ITN, 20ETB and white for circular ITN 30 ETB.29,30,32
Blue rectangular ITN has higher prices than others, and this study is consistent with the Ethiopian national malaria indicator survey conducted in 2015;6 52% of households prefer rectangular shape ITN to a circular one. The possible reason is they are familiar with it, and it is comfortable when hanging with their sleeping beds. In contrast to this, in the previous studies conducted at Arba Minch and Berehet districts, blue rectangular ITN had a lower price rate when compared with other ITN types.30,32
This study has a higher price in all types of ITN compared with the Ethiopian national malaria indicator survey 2015; the average willingness to pay was also less than 10 ETB.6 The possible explanation might be the time difference with the current study.
The Tobit econometrical regression analysis revealed that male respondents were willing to pay a higher amount than female respondents, which is supported by studies conducted elsewhere in Tanzania,34 Arba Minch district in Ethiopia.30,33 The possible explanation might be due to the huge financial resources and decision-making process relying on the hands of males than females. However, apart from studies done in the Berehet district, females have higher WTP.32
The educational status of the respondents was found to be another factor contributing to the increase in the amount of payment willing to pay for ITN. This is supported by a systematic review of low- and middle-income countries Nigeria, Bugina, Ethiopia and Bangladesh.31,35–37
The respondent’s marital status was also found to be contributing factor to increasing the amount of payment willing to pay for ITN. This is consistent with a study done in Bangladesh.35 The possible explanation might be respondent’s knowledge about ITN as malaria prevention had a positive and significant association with willingness to pay for ITN. This finding is consistent with the study conducted in Ethiopia and Tanzania.33,38
The wealth status of the families had a positive and strong significant association with willingness to pay. This is consistent with other studies conducted in Bangladesh.35 The possible explanation may be having more wealth is associated with high asset losses if an unexpected event occurs that leads households to be more willing to pay for the community insurance than the poorer.
The strengths of this study were able to differentiate people’s preference in the different types of ITN regarding shape colour and season of more willing to buy ITN and using the contingent valuation the binary with follow-up method to minimize bias. On the other hand, using self-reporting measures might overestimate or underestimate the results of the wealth index variable and willingness to pay value, and in addition, we have limited our sample selection to four kebeles within the zone that might overestimate or underestimate the result.
Conclusion
The study revealed that about 64% of households in the Bugina district were willing to pay ITN.
The result also showed that the household heads in the study area were willing to pay an average mean of 55.6 (SD±12.9) birr, which is greater than the current market price of 50 birrs for blue medium size rectangular ITN, 43 (SD ±11.8) birr. Which is less than the current market price of 60 birrs for blue circular medium size and 46.7 (SD±12.3) birr, which is less than the current market price of 80 birrs for white circular medium size ITN per household. Households have a good preference and high price for blue medium size rectangular ITN than the other two, as their WTP belonged to their lower bid dichotomous price. Respondent sex, Educational status, knowledge about ITN and malaria, and wealth status influenced WTP for ITN and the amount of WTP.
The FMOH and regional health bureau should focus on awareness creation and providing education for households to scale up willingness and amount of WTP for ITN. Also, the government should subside the poor households with some amount of premium for increasing universal coverage and avail ITNS in the market for those who cannot afford and are willing to pay to sustain the program.
Abbreviations
ARHB, Amhara Regional Health Bureau; CBA, cost-benefit analysis; CVM, contingent valuation method; FMoH, federal ministry of health; HH, households; IRS, indoor residual spraying; ITN, insecticidal treated bed net; LLIN, long lasting insecticidal bed net; MWTP, maximum willingness to pay; NGOs, Non-Governmental Organizations; PV, Plasmodium vivax; SNNP, South Nation Nationalities People; WHO, World Health Organization; WTP, willingness to pay.
Data Sharing Statement
The datasets supporting the conclusions of this article are available upon request to the corresponding author.
Ethics Statement
The manuscript complies with the Helsinki declaration.
Acknowledgments
First, we would like to thank the University of Gondar for the approval of the ethical issue and its technical and financial support. Next, our gratitude goes to the North Wollo zone Bugina district health office for letting us conduct this research. Finally, we would like to thank our study participants for their volunteer participation and also data collectors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Delil RK, Dileba TK, Habtu YA, et al. Magnitude of malaria and factors among febrile cases in low transmission areas of Hadiya zone, Ethiopia: a facility based cross sectional study. PLoS One. 2016;11(5):e0154277. doi:10.1371/journal.pone.0154277
2. Goshu YA, Yitayew AE, Fischer F. Malaria knowledge and its associated factors among pregnant women attending antenatal clinic of Adis Zemen Hospital, North-western Ethiopia, 2018. PLoS One. 2019;14(1):e0210221. doi:10.1371/journal.pone.0210221
3. Atieli HE, Zhou G, Afrane Y, et al. Insecticide-treated net (ITN) ownership, usage, and malaria transmission in the highlands of western Kenya. Parasit Vectors. 2011;4(1):1–10. doi:10.1186/1756-3305-4-113
4. Barber BE, Rajahram GS, Grigg MJ, et al. World Malaria Report: time to acknowledge Plasmodium knowlesi malaria. Malar J. 2017;16(1):1–3. doi:10.1186/s12936-017-1787-y
5. Biadgilign S, Reda A, Kedir H. Determinants of ownership and utilization of insecticide-treated bed nets for malaria control in eastern Ethiopia. J Trop Med. 2012;2012:45.
6. Hwang J, Graves PM, Jima D, et al. Knowledge of malaria and its association with malaria-related behaviors—results from the malaria indicator survey, Ethiopia, 2007. PLoS One. 2010;5(7):e11692. doi:10.1371/journal.pone.0011692
7. Muchie KF, Alemu K, Tariku A, et al. Rural households at risk of malaria did not own sufficient insecticide treated nets at Dabat HDSS site: evidence from a cross sectional re-census. BMC Public Health. 2017;17(1):1–9. doi:10.1186/s12889-017-4906-3
8. Institute, E.p.h. Ethiopian National malaria indicator survey 2015; 2016.
9. Nega D, Dana D, Tefera T, et al. Prevalence and predictors of asymptomatic malaria parasitemia among pregnant women in the rural surroundings of Arbaminch Town, South Ethiopia. PLoS One. 2015;10(4):e0123630. doi:10.1371/journal.pone.0123630
10. Taffese HS, Hemming-Schroeder E, Koepfli C, et al. Malaria epidemiology and interventions in Ethiopia from 2001 to 2016. Infect Dis Poverty. 2018;7(1):1–9. doi:10.1186/s40249-018-0487-3
11. Tegegne Y, Asmelash D, Ambachew S, et al. The prevalence of malaria among pregnant women in Ethiopia: a systematic review and meta-analysis. J Parasitol Res. 2019;2019:8396091. doi:10.1155/2019/8396091
12. World Health Organisation. World malaria report 2019; 2020:40.
13. Asante A, Price J, Hayen A, et al. Equity in health care financing in low-and middle-income countries: a systematic review of evidence from studies using benefit and financing incidence analyses. PLoS One. 2016;11(4):e0152866. doi:10.1371/journal.pone.0152866
14. Woday A, Mohammed A, Gebre A, et al. Prevalence and associated factors of malaria among febrile children in Afar region, Ethiopia: a health facility based study. Ethiop J Health Sci. 2019;29(5). doi:10.4314/ejhs.v29i5.12
15. Loha E, Lunde TM, Lindtjørn B. Effect of bed nets and indoor residual spraying on spatio-temporal clustering of malaria in a village in south Ethiopia: a longitudinal study; 2012.
16. Tassew A, Hopkins R, Deressa W. Factors influencing the ownership and utilization of long-lasting insecticidal nets for malaria prevention in Ethiopia. Malar J. 2017;16(1):1–9. doi:10.1186/s12936-017-1907-8
17. World Health Organization. WHO malaria report; 2018.
18. Kanmiki EW, Awoonor-Williams JK, Phillips JF, et al. Socio-economic and demographic disparities in ownership and use of insecticide-treated bed nets for preventing malaria among rural reproductive-aged women in northern Ghana. PLoS One. 2019;14(1):e0211365. doi:10.1371/journal.pone.0211365
19. Kilian A, Koenker H, Baba E, et al. Universal coverage with insecticide-treated nets–applying the revised indicators for ownership and use to the Nigeria 2010 malaria indicator survey data. Malar J. 2013;12(1):1–12. doi:10.1186/1475-2875-12-314
20. Loha Shumbullo E, Lunde TM, Lindtjørn B. Effect of bed nets and indoor residual spraying on spatio-temporal clustering of malaria in a village in South Ethiopia: a Longitudinal Study. Variation in malaria transmission in Southern Ethiopia. The impact of prevention strategies and a need for targeted intervention; 2012.
21. Jima D, Getachew A, Bilak H, et al. Malaria indicator survey 2007, Ethiopia: coverage and use of major malaria prevention and control interventions. Malar J. 2010;9(1):1–12. doi:10.1186/1475-2875-9-58
22. Nkoka O, Chuang T-W, Chuang K-Y, et al. Factors associated with insecticide-treated net usage among women of childbearing age in Malawi: a multilevel analysis. Malar J. 2018;17(1):1–16. doi:10.1186/s12936-018-2522-z
23. Animut A, Negash Y, Kebede N. Distribution and utilization of vector control strategies in a malarious village of Jabi Tehnan District, north-western Ethiopia. Malar J. 2014;13(1):1–6. doi:10.1186/1475-2875-13-356
24. Babalola S, Ricotta E, Awantang G, et al. Correlates of intra-household ITN use in Liberia: a multilevel analysis of household survey data. PLoS One. 2016;11(7):e0158331. doi:10.1371/journal.pone.0158331
25. Wanzira H, Yeka A, Kigozi R, et al. Long-lasting insecticide-treated bed net ownership and use among children under five years of age following a targeted distribution in central Uganda. Malar J. 2014;13(1):1–8. doi:10.1186/1475-2875-13-185
26. Watiro AH, Awoke W. Insecticide-treated net ownership and utilization and factors that influence their use in Itang, Gambella region, Ethiopia: cross-sectional study. Risk Manag Healthc Policy. 2016;9:101. doi:10.2147/RMHP.S104311
27. Lengeler C, et al. Quick wins versus sustainability: options for the upscaling of insecticide-treated nets. Am J Trop Med Hygiene. 2007;77(6):45.
28. Curtis C, Maxwell C, Lemnge M, et al. Scaling-up coverage with insecticide-treated nets against malaria in Africa: who should pay? Lancet Infect Dis. 2003;3(5):304–307. doi:10.1016/S1473-3099(03)00612-1
29. Biadgilign S, Reda AA, Kedir H. Determinants of willingness to pay for the retreatment of insecticide treated mosquito nets in rural area of eastern Ethiopia. Int J Equity Health. 2015;14:99. doi:10.1186/s12939-015-0249-9
30. Gebresilassie FE, Mariam DH. Factors influencing people’s willingness-to-buy insecticide-treated bed nets in Arbaminch Zuria District, southern Ethiopia. J Health Popul Nutr. 2011;29(3):200–206. doi:10.3329/jhpn.v29i3.7867
31. Minyihun A, Gebregziabher MG, Gelaw YA. Willingness to pay for community-based health insurance and associated factors among rural households of Bugna District, Northeast Ethiopia. BMC Res Notes. 2019;12(1):1–7. doi:10.1186/s13104-019-4091-9
32. Aleme A, Girma E, Fentahun N. Willingness to pay for insecticide-treated nets in Berehet District, Amhara Region, Northern Ethiopia: implication of social marketing. Ethiop J Health Sci. 2014;24(1):75–84. doi:10.4314/ejhs.v24i1.10
33. Gingrich CD, Ricotta E, Kahwa A, et al. Demand and willingness-to-pay for bed nets in Tanzania: results from a choice experiment. Malar J. 2017;16(1):1–15. doi:10.1186/s12936-017-1929-2
34. Gingrich CD, Hanson KG, Marchant TJ, et al. Household demand for insecticide-treated bed nets in Tanzania and policy options for increasing uptake. Health Policy Plan. 2011;26(2):133–141. doi:10.1093/heapol/czq027
35. Ahmed S, Hoque ME, Sarker AR, et al. Willingness-to-pay for community-based health insurance among informal workers in urban Bangladesh. PLoS One. 2016;11(2):e0148211. doi:10.1371/journal.pone.0148211
36. Olapeju B, Choiriyyah I, Bertram K, et al. Who buys nets? Factors associated with ownership and use of purchased mosquito nets in sub-Saharan Africa. Malar J. 2019;18(1):1–10. doi:10.1186/s12936-019-3020-7
37. Onwujekwe O, Hanson K, Ichoku H, et al. Financing incidence analysis of household out‐of‐pocket spending for healthcare: getting more health for money in Nigeria? Int J Health Plann Manage. 2014;29(2):e174–e185. doi:10.1002/hpm.2166
38. Legesse Y, Tegegn A, Belachew T, et al. Households willingness to pay for long-lasting insecticide treated nets in three urban communities of Assosa Zone, western Ethiopia. Ethiop Med J. 2007;45(4):353–362.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.