")
Back to Journals » Patient Preference and Adherence » Volume 17
Factors Influencing Utilization of Assistive Devices by Tibetan Seniors on the Qinghai-Tibet Plateau: Based on Research Strategy of Triangulation
Authors Luo J, Liu Q, Gama Z, Gesang D, Zhu Y, Yang L, Bai D, Zhao Q, Xiao M
Received 6 December 2022
Accepted for publication 9 February 2023
Published 15 February 2023 Volume 2023:17 Pages 401—411
DOI https://doi.org/10.2147/PPA.S400346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Jun Luo,1 Qing Liu,2 Zhujizhaba Gama,3 Deji Gesang,3 Ying Zhu,2 Lining Yang,2 Dingqun Bai,2 Qinghua Zhao,4 Mingzhao Xiao1
1Department of Urology, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Rehabilitation Medicine, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 3Department of Rehabilitation Medicine, Tibet Autonomous Region People’s Hospital, Tibet, People’s Republic of China; 4Department of Nursing, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Mingzhao Xiao, 1st Youyi Road, Chongqing, 400016, People’s Republic of China, Tel +86 13608399433, Email [email protected]
Purpose: To investigate the current situation of assistive device (AD) usage among seniors in Tibet, China, and explore its influencing factors.
Methods: A mixed-methods design was used. Cognition, attitude, behavior, and preference toward ADs were assessed by a self-designed questionnaire. Additionally, participants responded to the open-ended questions. Anderson’s behavior model analyzed the impacts of the prerequisite factors, enabling factors, and demand factors influencing the utilization of ADs by Tibetan seniors.
Results: Of the 211 Tibetan seniors, 149 (70.6%) Tibetan seniors expressed the willingness to utilize ADs. Binary Logistic regression analysis showed that one prerequisite factor: age; one enabling factor: care situation, and one demand factor: dysfunctional condition were factors influencing the utilization of ADs. Qualitative comments described: psychological, physical environment, and social support factors were the main influencing factors.
Conclusion: This study presents the current situation to utilize ADs by Tibetan seniors on the Qinghai-Tibet Plateau, incorporates Anderson’s behavioral model for quantitative analysis, and combines qualitative research to explore the facilitating and hindering factors, to provide reference and basis for the development of ADs for seniors and policy formulation. The sample size of this study is relatively small and limited to ethnic groups, and we plan to increase the sample size and include more ethnic groups in the future study.
Keywords: assistive devices, seniors, Qinghai-Tibet Plateau, mixed-methods research
Introduction
Disability can occur at any age, but the elderly are at high risk.1 Along with aging, the physiological function of the elderly declines, with a high prevalence of cerebrovascular, osteoarticular, and other diseases2 and a corresponding increase in the risk of disability.3 In recent years, the increase in the number of seniors with dysfunction is a major demographic feature of an aging society and has increased the medical and care burden on society.4 Assistive devices (ADs) are defined as tools that assist individuals to maintain or improve their function and independence,5 and utilizing ADs can help seniors overcome physical dysfunction,6 such as limitations in mobility and vision, to enable them to seek medical treatment, care for their families, and participate in social activities.7
Tibet is located on the Qinghai-Tibet Plateau, with an average altitude of more than 4000 meters (13,123 feet).8 The high altitude, low oxygen level, and harsh climate, combined with the local population’s preference for high-purine foods such as beef, mutton, and butter tea, have made Tibet a region with a high incidence of stroke in China,9 with a higher prevalence among the elderly who have lived there for a long time. Restricted by local economic and medical conditions,10 the prognosis of the disease is poor and the disability rate is high.11 The economic development of high-altitude areas is more backward,12 so most of the local young people tend to choose to leave their hometowns for employment in more developed plain areas, leaving the elderly to take up the tasks of farming and caring for their families.13,14 In addition, the region is dominated by animal husbandry, and the elderly follow the traditional way of production and labor, which makes joints bear weight for a long time. As a result, they often suffer from osteoarthritis and have a high rate of joint deformity and disability.15 Poor living conditions and economic status in high-altitude areas exacerbate the vulnerability of the elderly to functional impairment, which also leads to the expansion of the application of ADs.
Tibet is a place inhabited by ethnic minorities, and Tibetans account for more than 90% of the total population.16 Assessing the prevalence of ADs among Tibetan seniors is a critical step in determining the current the utilization of ADs.17 In addition, it is essential to determine the proportion of older adults who need appropriate ADs but are unable to obtain or utilize them, and to understand the unmet need for ADs by Tibetan seniors. Most previous studies on ADs have focused on plain areas,18 with attention to young disabled groups19 and non-minority populations,20 and there is a lack of research on vulnerable populations in the plateau areas, including older disabled groups and ethnic minorities. Welfare policies cover people with disabilities who are already functionally disabled,21 while the elderly who can make the most of ADs are neglected in the face of an aging society where the burden of social care is becoming more and more serious.22 These are not conducive to achieving the overall goal of universal health coverage proposed by the World Health Organization.23 Therefore, this study was guided by a mixed research approach to understand the current situation and factors influencing the utilization of ADs by the Tibetan seniors on the Qinghai-Tibet Plateau. The results from this study will provide a reference for the development of AD services in the plateau region and help relevant government authorities with future strategies and policies.
Anderson’s behavioral model with a multi-dimensional theoretical analysis framework and a comprehensive and systematic index system24 had been widely tested all over the world,25–29 and has been usually used to explain the influencing factors of care and medical decision-making behavior in the elderly.30–32 In this study, we intend to describe the current condition of ADs for Tibetan seniors in Tibet, China. We were especially interested in the ability of different variables to explain the willingness of Tibetan seniors to utilize ADs by Andersons’ model. Based on data from the National Key Research and Development Program’s survey on the Tibetan Assistive Devices Demonstration Project, this study further analyzes the willingness to utilize ADs and its influencing factors among ethnic minority seniors in the border areas of China by introducing Anderson’s behavioral model as an analytical framework, to providing some reference and basis for the development of the elderly AD and policy formulation in the plateau area.
Methods
Study Population and Design
A triangulation mixed methods design was used to conduct this study. Using convenience sampling, quantitative data were collected from September to December 2021. Tibetan seniors included in this survey, are from three communities in Tibet, China. These three communities represent different levels of economic development, including urban, rural, and pastoral areas. To supplement the quantitative research, we conducted qualitative studies to interview 8 Tibetan seniors. The inclusion criteria were as follows: (a) aged ≥ 60 years old, (b) Tibetan nationality, (c) communicate independently or communicate with the help of investigators (the elderly with cognitive impairment, severe hearing loss, obvious language difficulties, and other communication disorders were excluded), and (d) willingness to take part in the survey.
Instrument
Based on the literature review at home and abroad and expert consultation in the research group, a self-made questionnaire was created. Researchers deeply studied the history, culture, and regional disease spectrum of Tibet, inquired about the geriatric and AD-related Specialists of a tertiary class A hospital in Tibet, and conducted face-to-face interviews with two Tibetan seniors. After the completion of the initial questionnaire draft, 10 experts in this research field were invited to evaluate the validity of the questionnaire. Inclusion Criteria: (a) bachelor’s degree or above, intermediate or above professional title; (b) clinical or management experience in tertiary class A hospitals with geriatric major and AD-related services for more than 10 years; (c) volunteer to participate in this study. The proportion of experts giving opinions is 60%, and the expert authority coefficient Cr is 0.925, indicating that the questionnaire had good content validity. Finally, the researchers carried out a pre-validation survey in the pilot area to find out the inadequacies of the questionnaire and improve it to form the final version of the questionnaire: “Cognition, attitude, and behavior towards ADs in Tibetan seniors”, including the following 3 parts: (a) Basic information and demographics of participants; (b) Cognition and attitude towards ADs (Whether the elderly are knowing the functions of the ADs, the application population, the acquisition channels and the attitude towards ADs); (c) Behavioral performance towards ADs.
This study took various factors that may affect the utilization of ADs by Tibetan seniors as independent variables and introduced Anderson’s behavioral model as the theoretical analysis framework. The model classified the factors of the willingness to utilize ADs into three categories: prerequisite factors, enabling factors, and demand factors.33 (a) Prerequisite factors referred to the characteristics of people who tend to choose elderly care and health services before they become ill (disabled), including two variables: demographic characteristics (gender, age, marital status) and social structure (occupational status, education level). (b) Enabling factors referred to the ability of individuals to acquire health services, which were indirect influences on individual health service needs, including three aspects: economic status (financial status), care resource (care situation), and availability of community health services and care resources (accessibility of Barrier-free facilities and environment in the community). (c) Demand factors reflected the demand for medical and health services arising from individual physical health or functional status, which was the direct and prerequisite factor for individual demand for health services. It included health status and perception of self-care status (dysfunctional condition, disability certificate and grade, cognition and perception of ADs, willingness to utilize ADs, preference for ADs, and behavioral performance).
Additionally, 8 Tibetan seniors were invited to participate in the interview to answer the following open-ended questions: (a) How do you think about assistive devices? (b) What do you think about the use of assistive devices for seniors? (c) What factors influence your choice of assistive devices? (d) Specifically, what are your requirements or needs for assistive devices? (e) Do you have anything to add to the above discussion on the topic of assistive devices?
Data Collection
The surveys (via a questionnaire website platform) were completed either by self-reported, by a caregiver or representative of participants, or by investigators trained specifically for this study. The investigator initially explained to the participants the purpose and significance of this study and stated that they would remain anonymous and keep the information confidential. After the informed consent of the participants, scanned the quick response code and entered their responses into the answer interface. A total of 240 questionnaires were collected by December 7, 2021, of which 211 were valid, with an effective rate of 88%. The collection of qualitative data, undertaken through semi-structured in-depth interviews with 8 Tibetan seniors in Lhasa took place in September and December 2021. The interview framework was structured to explore the cognition, attitude, behavior, and factors influencing the utilization of ADs by Tibetan seniors. A pre-interview was Conducted before the formal interview, and the interview outline based on the results of the pre-interview was revised. Within 24 hours of the interview, the transcript was transcribed word for word, and then reviewed by another researcher.
Ethical Approval
The investigation scheme was approved by the ethics committee of the First Affiliated Hospital of Chongqing Medical University (No.2020–622), and all participants provided oral or written consent included publication of anonymized responses. The study complies with the Declaration of Helsinki.
Data Analysis
SPSS 26.0 was used for data analysis. Data were expressed as mean ± standard deviation or frequency and percentage; The χ2 test was used to compare the categorical variables between groups. An analysis of the influencing factors was conducted using binary logistic regression. P < 0.05 was considered statistically significant.
The qualitative data were analyzed by the Colaizzi seven-step analysis method after reviewing unanimously. We strived to discover latent themes and ensured that all relevant text segments were assigned to a category. The two researchers coded independently, and the inconsistencies were verified with the study subjects until a consensus was reached. Additionally, a peer debriefing was conducted to enhance the validity and credibility of the qualitative content analysis.
Results
Quantitative Findings
Demographic Characteristics
Among the 211 respondents, 129 were females (61.1%) and 82 were males (38.9%). Participants comprised 141 aged 60–69 (66.8%), 57 aged 70–79 (27.0%), and 13 aged over 80, accounting for 6.2%. 85.3% were primary and below (n=180). Most subjects were married (n=147, 69.7%), 25.6% (n=54) were windowed. 71.6% (n=151) of participants were still working; 28.4% (n=60) retired at home. In this group, 43.6% suffered from an income lower than 1000 yuan/month. The majority of the participants were dysfunctional34 (Generalized terms for impairment, activity limitation, and participation restriction, n=154, 73%), but 93.4% did not have disability certificates, and among the elderly with disability certificates (6.6%, n = 14), 42.9% of them were tertiary disabled (disability grade, grade 3 is moderate). 57.8% of the participants lived alone and took care of themselves, and 39.8% of them were cared for by specialized caregivers. 7.1% of these participants had a history of safety accidents (such as accidental falls). Most of the elderly (60.7%, n = 128) lived in communities that could provide barrier-free environments and facilities for AD use. More details were outlined in Table 1.
 |
Table 1 Univariate Analysis Results of Willingness to Use ADs |
Cognition, Attitude, Behaviour and Preference Toward ADs
Table 1 showed the status of participants regarding cognition, attitude, behaviour, and preference toward ADs. Of those surveyed, 61.6% (n = 177) of the participants understood the function of ADs, 53.2% (n = 101) learned about ADs adapted to the population, but only 37.9% (n = 72) knew the channels to source ADs. Overall, the attitude of most participants toward ADs was positive (76.3%). The agreement with the opinion that “ADs have limited help to the elderly” was 11.6%. Other subjects held a negative attitude, with 12.1% believing “ADs do not have any effects”. The history of ADs use was 24.2% (n=51), most of them (72.5%) purchased or manufactured ADs by themselves, and 78.4% of the participants thought that ADs were suitable Considering the cultural and linguistic differences in Tibet, 61.6% of the elderly hoped to use the Tibetan language to configure instructions and use guidance, 22.8% of the elderly expressed a tendency to rely on ADs in daily life, and 70.6% were willing to utilize and accept ADs.
Univariate Analysis results of Willingness to Utilize ADs
The multi-collinearity test between the variables showed that the differential expansion factor (VIF) of the model was less than 10, which indicated no multi-collinearity between the variables. Age, dysfunctional condition, care situation, history of ADs use, language preference of ADs, and dependence degree, the differences were statistically significant (P< 0.05). No significant difference was seen in gender, education level, marital status, occupational status, financial condition, disability certificate and grade, safety issues, barrier-free facilities in living environment, cognition and attitude toward ADs, suitability and access source (P > 0.05, see Table 1).
Binary Logistic Analysis Results of Willingness to Utilize ADs
Taking whether the Tibetan seniors were using ADs as the dependent variable (no = 0, yes = 1) and the variables with statistical differences in the univariate analysis as the independent variable, binary logistic regression analysis was carried out to test the goodness of fit and Hausman test of the model χ2 = 74.013, P < 0.001, indicating that the model fitting is good. The model was able to correctly classify 80.6% of the cases. The analysis results showed that age, dysfunctional condition, and care situation were the influencing factors of willingness to utilize ADs among the Tibetan seniors (P < 0.05, see Table 2).
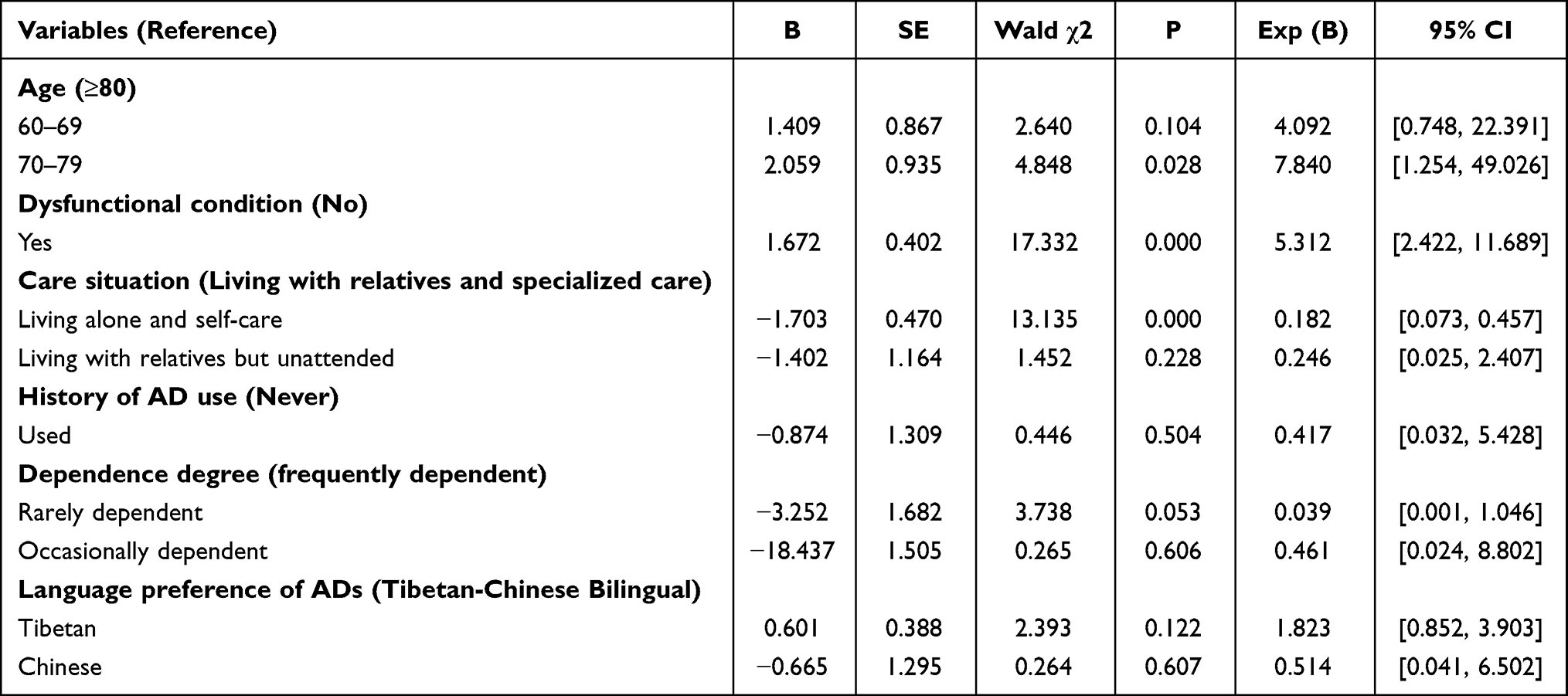 |
Table 2 Binary Logistic Analysis Results of Willingness to Use ADs |
Qualitative Findings
To gain a deeper understanding of the factors influencing the utilization of ADs by Tibetan seniors, this study added a qualitative study to the quantitative study. Eight Tibetan seniors (half male and female) responded to the interview framework structure. Ages ranged from 60 to 80, with details shown in Table 3. Three themes were identified: psychological factors, physical environment, and social support.
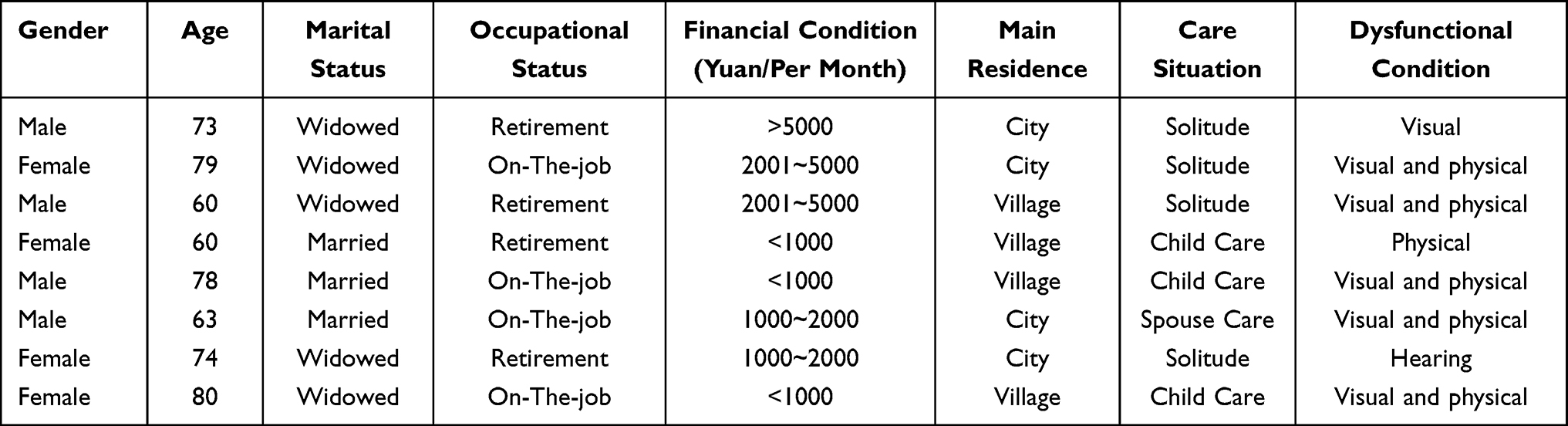 |
Table 3 Demographic Data for Interviewees |
Psychological Factors
Some respondents felt that they experienced significant psychological stress when using ADs, apparently due to the “stigma” of ADs. Another group of respondents expressed uncertainty and insecurity about wearing or using a “new” item.
…I feel like this is only for people with disabilities and I’m embarrassed to use it…I’m just afraid that people around me will discriminate, so I don’t want to use it, even if I can’t stand for long periods.
…This has never been used before. I’m afraid of the side effects of wearing it…I would wonder if I would get dizzy and woozy after wearing reading glasses.
I would worry about… its quality, such as whether it is harmful to my body and how it works.
Physical Environment
Physical environment factors for the availability of ADs included cumbersome adaptation processes, inconvenient transportation, and environmental barriers to use. Most respondents reported a preference for external devices (ADs) to improve their quality of life due to age and decreased mobility. Because of this, they would like to have a better-configured environment.
I would prefer to go to the (grocery) store…I hate the complicated adaptation process of professional institutions. I am an elderly person. I am willing to go to the (grocery) store for convenience…I mind the trouble of the process.
If I need to buy crutches, I have to walk to a resort far away from the neighborhood committee, and from there take a bus, and then transfer once in the middle and take more than 20 stops to get to Barkhor Street. (main city)
Even if I had a wheelchair…the road is potholes, which obviously doesn’t help…you know I have a leg with dysfunction…I want to go outside in my wheelchair and take a walk with my friends…
Social Support
The theme of social support reflected individuals’ concerns about formal government and organization-led support, professional and technical support from professionals, and support from personal networks, including family and friends.
I am mainly concerned about the price…It would be great if I could be subsidized!
My family… is a low-income household and cannot afford it. The government will help us for free and donate ADs to us.
…I would like to be assessed by a professional before ADs adaptation…and provide me with professional guidance after adaptation and teach us how to use.
My friend and I were both getting older and were experiencing varying degrees of muscle atrophy, which was causing mobility problems. Suddenly one day I saw my friend using a cane. He told me where to go to configure ADs and considerations…It made my life better.
I have…no financial income now…everything depends on my children…if my family agrees then I will go and try… if my children are against it, I think I may not do it.
Discussion
The results of this study showed that 149 (70.6%) of the Tibetan seniors had the willingness to use ADs, and this data set also indicated that the willingness of seniors to accept ADs is universal, which is consistent with the study by Wilkowska et al35 The reasons for this are mainly related to the functional decline in the elderly and the need for ADs to maintain their basic self-care ability. China’s population is developing from a pyramid to an inverted pyramid, and the “421 family model” (ie, 2 adults will be responsible for supporting 4 seniors and 1 child) has become the basic family structure in China, and the burden of pension is getting heavier. At the same time, the “empty-nest” phenomenon is disintegrating the traditional family model, especially in the frontier and remote areas of China. Without reliable support, seniors have to resort to ADs. Therefore, in this study, the willingness of seniors to utilize ADs is high, whether they are forced to use ADs due to the real situation or voluntarily to participate in social life, and in general, ADs are playing an increasingly important role in the healthcare and daily lives of seniors.
Prerequisite Factors
This study found that age is the main factor influencing the utilization of ADs for seniors and that increasing age makes the willingness to utilize ADs stronger. Some researchers indicated that along with aging, seniors are facing problems such as mobility disability and disabilities, and ADs are helping them address the conundrum.36 It is worth noting that the acceptance of ADs varies among the elderly at different ages, with a general trend of gradual decline. This may be related to the fact that when the age exceeds 80, the function of the elderly body declines rapidly plus they suffer from multiple chronic diseases at the same time, resulting in a limited range of motion and no use of ADs.
Enabling Factors
Caregiving resources are an important enabling factor in the choice of ADs.37 Seniors who live alone and take care of themselves are more likely to utilize ADs because they often have to take care of themselves due to the “empty-nest” and ADs become a tool for self-care, providing convenience, and meeting social needs. To investigate more deeply how care status affects the willingness to utilize ADs, this study further describes qualitatively that the acceptance of ADs is higher among the elderly who live with relatives and have a specified person to take care of them, mainly due to two reasons: the support from caregivers38 and a strong sense of family responsibility of seniors. In the traditional Tibetan family structure, the culture of “filial piety and respect for parents” prevails and the elderly are highly respected in the family. Children choose to purchase ADs for their parents out of concern for their safety and to ease their caregiving burden. The willingness to use ADs is generally higher among the elderly who are sponsored by their children. Moreover, the traditional family culture, which is more pronounced in the remote areas of western China, is that seniors are more willing to take responsibility than to be a “burden”. As a result, seniors who live with relatives and have a specified person to care for them tend to be active caregivers who are more than willing to take on some of the responsibilities of caring for their families. Despite their limited mobility, they take the initiative to look after their grandchildren, cook, do housework and do whatever they can to lighten the load of their children.
Demand Factors
We found that the willingness of seniors to utilize ADs was primarily driven by their functional impairment status. Among those who responded positively to the selection of ADs, the proportion of those with functional impairment was as high as 85.2%, suggesting that seniors with dysfunction have a greater willingness to utilize ADs to meet the “challenges”. Although there are many factors influencing the choice of ADs for seniors, dysfunction condition remains the main influencing factor, which is in accordance with the findings of many researchers.39–41 In economically developed countries and regions with better medical resources, there always seems to be a way to compensate for body function, but in less economically developed countries and remote areas, especially for ethnic minorities, access to ADs for seniors is often very difficult. Therefore, it is important to strengthen the “talent pool” and promote the construction of AD professionals at the grassroots level, so that accessible and safe AT can cover remote, less developed areas and ethnic minority elderly groups.
Additional Findings
The qualitative findings complement the quantitative data, which will facilitate a more comprehensive and in-depth dissection of the key factors that influence the willingness to utilize ADs. Perhaps the most compelling observation in this study is that “stigma” and “fear” of ADs impede the willingness to utilize them. It is well known that religious culture profoundly influences the choice of health perceptions and performances of religious groups.42,43 However, in this study, we were surprised to find that in Tibet, where almost all people are religious, religious beliefs did not influence the choice of ADs, but rather the psychological resistance caused by the “stigmatization” of ADs led to a lower willingness to accept them, which has been confirmed in studies by foreign investigators.44,45 On the other hand, seniors developed uncertainty about ADs they had never used before, fearing that the ADs may cause falls and secondary injuries, thus creating a sense of fear to limit the use of ADs, as mentioned in the study by Gell et al.46
In addition, both professional support from healthcare professionals and informal support from relatives can impact the elderly’s willingness to utilize ADs. Most seniors expressed a preference to listen to the advice of doctors or other healthcare professionals,47 but there still exist some seniors who only want to receive advice from family members or friends, resulting in a single source of information for seniors which is not conducive to access to professional services for them, and this non-professional information support is a great safety risk,48 which may cause secondary harm to the elderly.
For a long time, official agencies and non-profit organizations have focused on the health and well-being of disabled people, but seniors do not benefit from it. At present, the global aging problem is getting more and more intense, and the risk of functional impairment and disability of the elderly increases accordingly with age. Aging-friendly ADs will usher in a golden era, but the supportive policies and regulations and financial subsidies are not backed, which makes seniors hesitant in utilizing ADs.
Limitations and Future Research
This study was conducted in the unique cultural context of Tibet, and the respondents were all ethnic minorities, which may limit the generalizability of the results. Secondly, the sample size of this study was small. In the future, we hope to include ethnic samples and non-ethnic minority groups from more regions to compare with the Tibetan sample and further explore the differences.
Conclusion
Increasing the proportion of ADs utilization for seniors plays an important role in actively coping with aging and greater attention to the health services of minority groups in plateau areas will facilitate the realization of a universal health program.23 Tibet has a lack of public health resources and certain regional prejudices, which have led to insufficient social attention to vulnerable groups. This study investigates the current situation of AD service based on research strategy of Triangulation and confirms the facilitating and impeding factors influencing the utilization of ADs by older minority adults on the Qinghai-Tibet Plateau. Promoting willingness to utilize ADs for seniors should be conducted in collaboration with various stakeholders, including government, non-profit organizations, professionals, family caregivers, and the elderly, to change the negative attitude toward ADs from society and value the business of customized ADs for seniors. It is hoped that the present study can provide a reference and basis for the development of AD business and policy formulation in frontier regions.
Acknowledgments
The authors would like to be grateful to the Tibet Autonomous Region People’s Hospital for their support of this study, and to all participants, researchers and staff.
Funding
This research was funded by The National Key Research and Development Program of China, grant number, 2020YFC2005900) and The Key Research and Development Program Jointly Implemented by Sichuan and Chongqing, grant number, cstc2020jscx-cylhX002).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Carmona-Torres JM, Rodríguez-Borrego MA, Laredo-Aguilera JA, et al. Disability for basic and instrumental activities of daily living in older individuals. PLoS One. 2019;26(14):0220157. doi:10.1371/journal.pone.0220157
2. Xie F, Li J, Song W, et al. Long-term care facility and its elderly chronic diseases in jishou: insights into underdeveloped area of China. Inquiry. 2022;2022(59):469580221128735. doi:10.1177/00469580221128735
3. Kim WH, Park YG, Shin HI, et al. The world report on disability and recent developments in South Korea. Am J Phys Med Rehabil. 2014;93(1Suppl 1):S58–62. doi:10.1097/PHM.0000000000000024
4. Mendonça JMB, Abigalil APC, Pereira PAP, et al. The meaning of aging for the dependent elderly. Cien Saude Colet. 2021;26(1):57–65. doi:10.1590/1413-81232020261.32382020
5. World Health Organization. Assistive Technology. Available from: https://www.who.int/zh/news-room/fact-sheets/detail/assistive-technology.
6. Sehgal M, Jacobs J, Biggs WS. Mobility assistive device use in older adults. Am Fam Physician. 2021;103(12):737–744.
7. Yu HW, Chen DR, Chiang TL, et al. Disability trajectories and associated disablement process factors among older adults in Taiwan. Arch Gerontol Geriatr. 2015;60(2):272–280. doi:10.1016/j.archger.2014.12.005
8. Ministry of Commerce of the People’s Republic of China. Tibet autonomous region overview; 2022. Available from: http://cdtb.mofcom.gov.cn/article/shangwubangzhu/fazzn/201201/20120107918581.shtml.
9. Wang LD, Wang JH, Peng B, et al. Brief report on stroke prevention and treatment in China, 2016. Chin J Cerebrovasc Dis. 2017;(14):217–224. doi:10.3969/j.issn.1672-5921.2017.04.010
10. Zhou LX, Ci Y, Hu YX, et al. Preliminary study on the optimization effect of intravenous thrombolysis in acute ischemic stroke in Lhasa. Med J Pek Uni Med Col Hos. 2022;(13):888–894. doi:10.12290/xhyxzz.2022-0041
11. Katan M, Luft A. Global burden of stroke. Semin Neurol. 2018;38(2):208–211. doi:10.1055/s-0038-1649503
12. Zhu FB, Fang YP, Yang XT, et al. Effects of altitude on county economic development in China. J Mt Sci. 2018;15(2):406–418. doi:10.1007/s11629-017-4393-0
13. National Bureau of Statistics. Per capita disposable income of Tibetan residents. Available from: https://data.stats.gov.cn/easyquery.htm?cn=E0103&zb=A0201®=540000&sj=2021.
14. National Bureau of Statistics. National per capita disposable income. Available from: https://data.stats.gov.cn/easyquery.htm?cn=C01&zb=A0A01&sj=2021.
15. Tian DC, Zhang C, Yuan M, et al. Incidence of multiple sclerosis in China: a nationwide hospital-based study. Lancet Reg Health West Pac. 2020;1(1):100010. doi:10.1016/j.lanwpc.2020.100010
16. Central People’s Government of the People’s Republic of China. The fact that Tibetans are the main ethnic group in Tibet remains unchanged. Available from: http://www.gov.cn/jrzg/2009-03/25/content_1268044.htm.
17. Ishigami Y, Jutai J, Kirkland S. Assistive device use among community-dwelling older adults: a profile of Canadians using hearing, vision, and mobility devices in the Canadian longitudinal study on aging. Can J Aging. 2021;40(1):23–38. doi:10.1017/S0714980819000692
18. Rolland JP, Myrberget MA, Meisingset TW. The assistive device situation for ALS patients in Norway. Occup Ther Int. 2021;2021:5563343. doi:10.1155/2021/5563343
19. Nordstrom B, Prellwitz M. A pilot study of children and parents experiences of the use of a new assistive device, the electro suit Mollii. Assist Technol. 2021;33(5):238–245. doi:10.1080/10400435.2019.1579267
20. Jiménez-Arberas E, Díez E. Psychosocial impact of assistive devices and other technologies on deaf and hard of hearing people. Int J Environ Res Public Health. 2021;18(14):7259. doi:10.3390/ijerph18147259
21. World Health Organization. Disability and health. Available from: https://www.who.int/zh/news-room/fact-sheets/detail/disability-and-health.
22. Chakravarti D, LaBella KA, DePinho RA. Telomeres: history, health, and hallmarks of aging. Cell. 2021;184(2):306–322. doi:10.1016/j.cell.2020.12.028
23. World Health Organization. Universal health coverage (UHC). Available from: https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc).
24. Luppa M, Luck T, Weyerer S, et al. Prediction of institutionalization in the elderly. A systematic review. Age Ageing. 2010;39(1):31–38. doi:10.1093/ageing/afp202
25. Freidoony L, Ranabhat CL, Kim CB, et al. Predisposing, enabling, and need factors associated with utilization of institutional delivery services: a community-based cross-sectional study in far-western Nepal. Women Health. 2018;58(1):51–71. doi:10.1080/03630242.2016.1267689
26. Houle LG, Salmoni AW, Pong RW, et al. Predictors of family physician use among older residents of Ontario and an analysis of the Andersen-Newman behavior model. Can J Aging-Rev Can Vieil. 2001;20(20):233–249. doi:10.1017/S071498080001299X
27. Nivestam A, Westergren A, Petersson P, et al. Factors associated with good health among older persons who received a preventive home visit: a cross-sectional study. BMC Public Health. 2020;20(1):688. doi:10.1186/s12889-020-08775-6
28. Pianori D, Maietti E, Lenzi J, et al. Sociodemographic and health service organizational factors associated with the choice of the private versus public sector for specialty visits: evidence from a national survey in Italy. PLoS One. 2020;15(5):e0232827. doi:10.1371/journal.pone.0232827
29. Tolera H, Gebre-Egziabher T, Kloos H. Using Andersen’s behavioral model of health care utilization in a decentralized program to examine the use of antenatal care in rural western Ethiopia. PLoS One. 2020;15(1):e0228282. doi:10.1371/journal.pone.0228282
30. Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995;36(1):1–10. doi:10.2307/2137284
31. Sunil TS, Rajaram S, Zottarelli LK. Do individual and program factors matter in the utilization of maternal care services in rural India?: a theoretical approach. Soc Sci Med. 2006;62(62):1943–1957. doi:10.1016/j.socscimed.2005.09.004
32. Fields NL, Richardson VE, Schuman D. Marital status and persons with dementia in assisted living: an exploration of length of stay. Am J Alzheimers Dis. 2017;32(2):82–89. doi:10.1177/1533317516688299
33. Yuee L, Shan L. Development, application and enlightenment of Anderson model in medical and health field. Res Health Policy in Chin. 2017;(11):77–82. doi:10.3969/j.issn.1674-2982.2017.11.013
34. ISO 9999: 2011, Rehabilitation assistive devices classification and terminology. National Standards of the People’s Republic of China; 2011.
35. Wilkowska W, Offermann-van Heek J, Laurentius T, et al. Insights into the older adults’ world: concepts of aging, care, and using assistive technology in late adulthood. Front Public Health. 2021;9(9):653931. doi:10.3389/fpubh.2021.653931
36. Bradley SM, Hernandez CR. Geriatric assistive devices. Am Fam Physician. 2011;84(4):405–411.
37. Sriram V, Jenkinson C, Peters M. Informal carers’ experience of assistive technology use in dementia care at home: a systematic review. BMC Geriatr. 2019;19(1):160. doi:10.1186/s12877-019-1169-0
38. Tuazon JR, Jahan A, Jutai JW. Understanding adherence to assistive devices among older adults: a conceptual review. Disabil Rehabil Assist Technol. 2019;14(5):424–433. doi:10.1080/17483107.2018.1493753
39. Grimmer M, Riener R, Walsh CJ, et al. Mobility related physical and functional losses due to aging and disease - a motivation for lower limb exoskeletons. J Neuroeng Rehabil. 2019;16(1):2. doi:10.1186/s12984-018-0458-8
40. Connors K, Mahony L, Morgan P. Variation in assistive technology use in motor neuron disease according to clinical phenotypes and ALS functional rating scale - revised score: a prospective observational study. NeuroRehabilitation. 2019;44(2):303–313. doi:10.3233/NRE-182511
41. Lo K, Stephenson M, Lockwood C. Effectiveness of robotic assisted rehabilitation for mobility and functional ability in adult stroke patients: a systematic review. JBI Database System Rev Implement Rep. 2017;15(12):3049–3091. doi:10.11124/JBISRIR-2017-003456
42. Hassan SM, Leavey C, Rooney JS, et al. A qualitative study of healthcare professionals’ experiences of providing maternity care for Muslim women in the UK. BMC Pregnancy Childbirth. 2020;20(1):400. doi:10.1186/s12884-020-03096-3
43. Vu M, Azmat A, Radejko T, et al. Predictors of delayed healthcare seeking among American Muslim women. J Womens Health. 2016;25(6):586–593. doi:10.1089/jwh.2015.5517
44. Fraser SA, Kenyon V, Lagacé M, et al. Stereotypes associated with age-related conditions and assistive device use in Canadian media. Gerontologist. 2016;56(6):1023–1032. doi:10.1016/j.dhjo.2008.12.002
45. Resnik L, Allen S, Isenstadt D, et al. Perspectives on use of mobility aids in a diverse population of seniors: implications for intervention. Disabil Health J. 2009;2(2):77–85. doi:10.1016/j.dhjo.2008.12.002
46. Gell NM, Wallace RB, LaCroix AZ, et al. Mobility device use in older adults and incidence of falls and worry about falling: findings from the 2011–2012 national health and aging trends study. J Am Geriatr Soc. 2015;63(5):853–859. doi:10.1111/jgs.13393
47. Mortenson WB, Pysklywec A, Fuhrer MJ, et al. Caregivers’ experiences with the selection and use of assistive technology. Disabil Rehabil Assist Technol. 2018;13(6):562–567. doi:10.1080/17483107.2017.1353652
48. Williams E, Hurwitz E, Obaga I, et al. Perspectives of basic wheelchair users on improving their access to wheelchair services in Kenya and Philippines: a qualitative study. BMC Int Health Hum Rights. 2017;17(1):22. doi:10.1186/s12914-017-0130-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.