Back to Journals » Patient Preference and Adherence » Volume 20
Factors Influencing Transition Readiness in Adolescents with Systemic Lupus Erythematosus: A Qualitative Study
Authors Chen C ![]() , Gan S, Liu T, Xiong H, Tang J
, Gan S, Liu T, Xiong H, Tang J ![]() , Lu Y, Xiang Y, Yang X
, Lu Y, Xiang Y, Yang X
Received 19 December 2025
Accepted for publication 24 April 2026
Published 29 May 2026 Volume 2026:20 586211
DOI https://doi.org/10.2147/PPA.S586211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Cailin Chen,1 Shangquan Gan,1 Ting Liu,2 Huimin Xiong,1 Jiran Tang,1 Yongmei Lu,1 Yuxuan Xiang,3 Xiangwei Yang4
1School of Nursing, Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, People’s Republic of China; 2Department of Pediatrics, Second Ward, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, Guangdong, People’s Republic of China; 3Department of Geriatrics, The First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, People’s Republic of China; 4Department of Nursing, The First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, People’s Republic of China
Correspondence: Xiangwei Yang, Department of Nursing, The First Affiliated Hospital of Guangzhou University of Chinese Medicine, 16 Jichang Road, Guangzhou, Guangdong, 510405, People’s Republic of China, Tel +8613570919326, Email [email protected]
Objective: This study aimed to identify the factors influencing transition readiness among adolescents with systemic lupus erythematosus, thereby providing a foundation for the development of targeted intervention programs.
Methods: Guided by the Social-Ecological Model of Adolescent and Young Adult Readiness for Transition, a descriptive qualitative study was conducted from September 2024 to October 2025. Using purposive sampling, we recruited 17 adolescent patients with systemic lupus erythematosus, their respective caregivers, and 12 healthcare providers from a tertiary hospital in Guangdong Province, China. Semi-structured interviews were performed, and the data were analyzed using directed content analysis.
Results: Six themes and sixteen subthemes were identified: (1) knowledge, encompassing both the active acquisition of disease-related information and a general lack of transition awareness; (2) skills/efficacy, characterized by poor medication adherence and insufficient competence in navigating healthcare systems; (3) beliefs/expectations, reflecting recognition of the importance of transition preparation; (4) goals, primarily defined by the absence of clear transition objectives; (5) relationships, incorporating barriers such as communication challenges between patients and healthcare providers or caregivers, a lack of coordination between pediatric and adult care departments, as well as facilitators like support from healthcare providers, emotional support from caregivers, and peer encouragement; (6) psychosocial functioning, manifested as emotional distress, caregiver over-involvement, substantial family financial burdens, alongside experiences of social stigma and discrimination.
Conclusion: This study highlights that transition readiness in adolescents with systemic lupus erythematosus is influenced by multiple interacting factors. Healthcare providers should implement tailored interventions to improve treatment adherence and self-care during the transition process.
Keywords: adolescents, systemic lupus erythematosus, transition readiness, the social-ecological model of adolescents and young adults readiness for transition, qualitative research
Introduction
Systemic lupus erythematosus (SLE) is a complex systemic autoimmune disease that can be life-threatening in severe cases due to multi-organ failure, significantly reducing patients’ life expectancy.1 Globally, the annual incidence of SLE is approximately 5.14 per 100,000 individuals, corresponding to around 400,000 new cases annually, with adolescents accounting for roughly 20% of this population.2,3 Compared with adult-onset SLE, childhood-onset SLE typically exhibits a more aggressive clinical course, characterized by higher rates of organ involvement and an increased risk of mortality.4 Advances in medical management have improved the 10-year survival rate for adolescents with SLE to 94%-100%.5 Consequently, these patients face the critical process of transitioning from caregiver-directed pediatric care to self-managed adult care, a period referred to as the healthcare transition.
Transition readiness refers to the perceived capacity of adolescents, their parents, and healthcare providers to prepare for, initiate, and complete the transfer to the adult healthcare system, encompassing the acquisition of essential health self-management knowledge and skills.6 Adequate preparation for this transition can enhance adolescents’ disease management capabilities, thereby improving long-term outcomes and quality of life.7 However, existing studies indicate that transition readiness among adolescents with SLE remains suboptimal, with more than half experiencing substantial challenges, such as lapses in follow-up, poor medication adherence, and increased disease activity, during this period.8,9 An unsuccessful transition not only heightens the risk of severe complications and disease flares but also increases the caregiving burden on families and the utilization of healthcare resources, ultimately leading to a markedly diminished quality of life for patients.10 Successful healthcare transition requires adolescents to gradually develop autonomy and the ability to make independent health decisions.11 This requires adolescents to acquire necessary disease knowledge and possess the intrinsic motivation and behavioral skills to maintain regular treatment behaviors.12 At the same time, this process is fundamentally a shared decision-making process involving patients, caregivers, and healthcare providers, and research has confirmed that this collaborative approach can enhance treatment satisfaction and follow-up adherence among chronic disease patients.13,14 Therefore, identifying key factors associated with transition readiness is essential for developing and implementing effective, targeted interventions.
Existing research has begun to elucidate the factors influencing transition readiness among adolescents with SLE. For instance, Roberts et al reported a positive correlation between patient age and transition readiness.15 Similarly, qualitative findings from Ciosek et al16 identified health literacy as a significant determinant of successful transition. Additional evidence suggests that patients who attend medical appointments independently tend to exhibit higher levels of transition readiness.17 From a family perspective, Hong et al indicated that excessive parental protection may hinder the transition process for adolescents.18 Furthermore, Bitencourt et al found that maintaining continuous insurance coverage and receiving formal referrals from pediatric rheumatologists were associated with fewer delays in accessing adult care, thereby facilitating a more successful transition.19 Despite these contributions, the existing evidence has several limitations. Most studies adopt a unidimensional perspective, examining the experiences of patients, parents, or healthcare providers in isolation. Second, existing research often focuses on factors confined to a single level or a single domain, thereby limiting a comprehensive understanding of the principal barriers and facilitators to successful transition. Moreover, nearly all available data come from Western healthcare systems, while data from non-Western cultural contexts such as China are extremely scarce. In cultural contexts like China, family-centered decision-making, high parental involvement, and fragmented transition pathways may create unique challenges for adolescent autonomy and transition readiness.20,21 Consequently, existing studies cannot elucidate the full range of facilitators and barriers that shape transition readiness in adolescents with SLE, particularly from a multi-stakeholder, culturally grounded, and qualitative perspective.
Utilizing a theoretical framework can enhance qualitative research by providing a systematic approach to exploring and explaining behaviors, which is widely recognized as a rigorous strategy for understanding complex health phenomena. Among these frameworks, the Social-ecological Model of Adolescent and Young Adult Readiness for Transition (SMART), developed by Schwartz et al in 2011, is highly recommended for studies on healthcare transition. Compared with models that focus on single-level or unidimensional determinants, the SMART framework explicitly integrates individual, interpersonal, and healthcare system dimensions, and emphasizes the dynamic interactions among patients, caregivers, and providers.22 It is therefore particularly suitable for investigating transition readiness in adolescents with chronic conditions such as systemic lupus erythematosus. Moreover, the SMART model provides a theoretical foundation for developing evidence-based transition interventions and has been applied to various adolescent and young adult populations.23,24 However, to date, the SMART framework has not been used to qualitatively examine transition readiness in adolescents with SLE.
To address these gaps, this study employed a qualitative design using semi-structured interviews guided by the SMART model. By integrating the perspectives of patients, caregivers, and healthcare providers, we aimed to comprehensively examine the factors influencing transition readiness among adolescents with SLE in China. The findings are expected to provide an evidence-based foundation for developing practical and effective transition intervention programs, thereby improving patients’ treatment adherence and transition readiness.
Materials and Methods
Study Design
This study adopted a descriptive qualitative design to capture rich, context-grounded narratives in participants’ own words, which is particularly suited for exploring an underexplored issue and guiding the development of transition services.25,26 Accordingly, semi-structured interviews were conducted with 17 adolescent patients, their caregivers, and 12 healthcare providers to examine the factors influencing transition readiness from their respective viewpoints. The study adhered to the Standards for Reporting Qualitative Research (SRQR) to ensure methodological rigor and transparency throughout the research process.27
Study Setting and Participants
This study was conducted in the Department of Rheumatology of a tertiary hospital in Guangzhou, China. The study participants included adolescents diagnosed with SLE, their primary caregivers, and physicians and nurses working in the Department of Rheumatology at the First Affiliated Hospital of Guangzhou University of Chinese Medicine. Recruitment and data collection were carried out from September 2024 to October 2025. Participants were recruited through purposive sampling with a maximum variation strategy, intentionally including adolescent patients of different genders, ages, educational levels, and disease durations, as well as caregivers with varied relationships to the patients (eg., fathers, mothers), and healthcare providers from different professional roles (physicians and nurses) and years of experience. Data collection continued until thematic saturation was reached, indicating that additional interviews no longer generated new insights.28 After interviewing 15 adolescent patients, their 15 caregivers, and 10 healthcare providers, no new ideas emerged. To confirm saturation, the researcher continued to interview two patients and their respective caregivers; and continued to interview two more healthcare providers. Still, no new themes emerged, and saturation was confirmed.
Prior to data collection, ethical approval was obtained. The researcher contacted potential participants to provide a detailed explanation of the study objectives and procedures. Written informed consent was obtained from all participants before interviews were scheduled and conducted at a mutually agreed-upon time and location.
Inclusion criteria of patients: (1) A confirmed diagnosis of systemic lupus erythematosus based on the 2019 European League Against Rheumatism/American College of Rheumatology Systemic Lupus Erythematosus Classification Criteria,29 with a disease duration of ≥3 months; (2) Age 12–18 years; (3) Basic proficiency in Chinese listening and speaking, with normal comprehension and communication abilities enabling barrier-free interaction. Exclusion criteria: (1) Presence of severe cardiac, cerebral, renal, or other major organ injuries; (2) Presence of psychiatric disorders or cognitive impairment.
Inclusion criteria of caregivers: (1) Family caregivers of patients aged 12 to 18 years who meet the diagnostic criteria of SLE; (2) Caregivers who are relatives and bear the primary responsibility for patient care; (3) Caregiving duration ≥3 months without financial compensation; (4) Basic proficiency in Chinese listening and speaking, with normal comprehension and communication abilities enabling barrier-free interaction. Exclusion criteria: (1) Presence of serious physical or mental illnesses; (2) Inability to participate in interviews or communication barriers.
Inclusion criteria of healthcare providers: (1) Possession of professional qualification certificates of a physician or nurse; (2) More than 3 years of experience in the treatment or nursing care of patients with systemic lupus erythematosus. Exclusion criteria: Visiting physicians, intern physicians, and intern nurses.
Date Collection
Data were collected through individual, face-to-face, semi-structured interviews conducted by a graduate nurse trained in qualitative research to ensure confidentiality. Interviews were held in a quiet, private hospital setting to create a comfortable environment free from interruptions. Prior to each interview, the researcher explained the study’s purpose and significance, assured participants of their right to withdraw at any time without penalty, and guaranteed the confidentiality and anonymity of their data. After receiving a detailed explanation, all participants provided written informed consent.
With participants’ permission, interviews were audio-recorded using a pre-prepared digital recorder to capture verbal responses accurately. Concurrently, detailed field notes were taken to document non-verbal cues, including changes in tone, facial expressions, and behaviors. Data collection continued until thematic saturation was reached, defined as the point at which no new concepts or themes emerged. Each interview lasted between 20 and 60 minutes. No participants withdrew from the study or declined to answer any questions during the interviews.
To collect the data, the researcher and the research team developed a semi-structured interview outline based on the study objectives and the SMART model. The SMART model is an internationally recognized theoretical framework for identifying the factors influencing transition readiness from pediatric to adult care.22 It comprises 6 key subjective domains: knowledge, skills/efficacy, beliefs/expectations, goals, relationships, and psychosocial functioning.30 Within this framework, the 6 domains are conceptually defined as follows: knowledge refers to understanding SLE, its treatment and related medications. Skills/efficacy relates to the competence and confidence in managing one’s own health and navigating the transition process. Beliefs/expectations denote attitudes and anticipations regarding the transition process or adult care. Goals involve the objectives established for the transition process. Relationships encompass the interactions between patients, parents and healthcare providers, including both pediatric and adult caregivers. Psychosocial functioning includes psychological status, family support, coping strategies for acute crises affecting both the patient and the family, and emotions specifically related to the transition process.
Six key concepts guided the design of the interview outline: knowledge, skills/efficacy, beliefs/expectations, goals, relationships, and psychosocial functioning. Subsequently, the formal interview outline was refined and finalized based on the findings of pre-interviews with three patients, caregivers, and healthcare providers. The finalized version of the interview outline is presented in Figure 1.
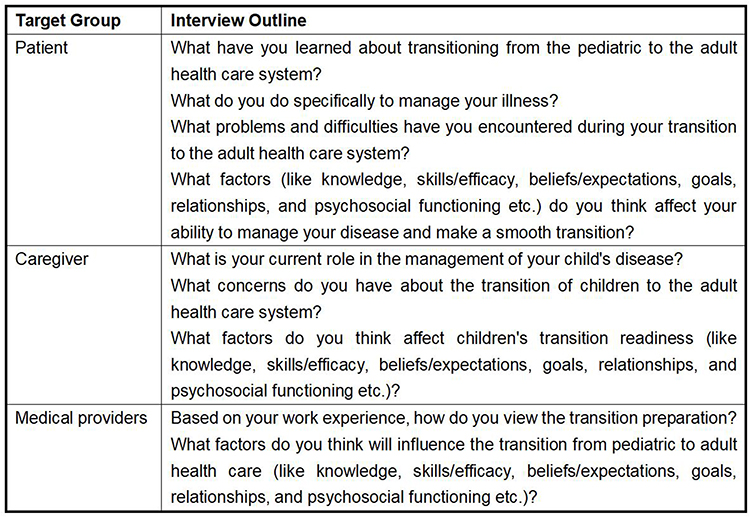 |
Figure 1 Final version of the interview outline. |
Data Analysis
After each interview, within 48 hours, two researchers transcribed the audio recordings verbatim. The transcripts were cross-checked against field notes and reflective journals. When clarification or confirmation was needed, the researchers contacted the participants to clarify meaning. The transcripts were proofread twice to ensure accuracy, and the verified text files were imported into NVivo (version 11) for data storage, analysis, and coding. Directed content analysis was employed to examine the factors influencing patients’ transition readiness because this method enables a systematic, objective, and theory-driven analysis using a top-down coding approach and deductive reasoning.31 It is particularly suitable when the theoretical foundation of the research phenomenon, the SMART model, is well established, allowing researchers to focus the analysis within the existing framework while still permitting new insights to emerge, thereby validating or extending the conceptual framework. The specific analytical steps are as follows: (1) Based on the SMART model and relevant literature, key concepts and variables were extracted to establish initial coding categories, each with a clear operational definition; (2) Interview transcripts were read line by line to identify and categorize statements pertinent to the SMART model; (3) New codes were assigned to uncategorized data and existing coding schemes were refined as necessary; (4) Codes were grouped into categories and sub-categories according to their conceptual relationships; (5) Categories were organized and conceptualized to derive overarching themes.
To enhance the reliability of the findings, analyst triangulation was conducted. Two researchers independently conducted open coding of the relevant transcripts. When disagreements arose, the two coders re-examined the original transcripts and field notes, revisiting the context of the coded segments. The research team then discussed any inconsistencies to reach a consensus. If consensus could not be achieved through discussion, a third senior researcher (experienced in qualitative analysis and not involved in data collection) was consulted to help resolve the disagreements. Additionally, the third senior researcher undertook to review a subset of the transcripts, the codebook, and the thematic structure, examined the fit between the raw data and the coded themes, and provided feedback on the clarity and distinctiveness of the themes.
Quality Control
The rigor of this qualitative study was assessed based on the established criteria of credibility, transferability, dependability, and confirmability.32 To enhance credibility, the researcher conducted a thorough review of the relevant literature prior to data collection to ensure accurate interpretation of participants’ narratives. All interviews were conducted by the first author, who had previously established rapport with SLE patients, caregivers, and healthcare providers during an internship in the rheumatology department, thereby fostering trust. The interviewer maintained a neutral, non-judgmental stance throughout each interview, and all sessions were audio-recorded in their entirety. Given her prior role as an intern nurse for some participants, the research team acknowledged the potential for social desirability bias and expectancy effects. Therefore, before data collection, she undertook reflexive preparation, including bracketing her preconceptions related to her clinical experience with SLE patients. Through self-reflection and team discussions, she identified and consciously set aside her personal assumptions about patients’ transition behaviors to minimize bias in data generation and interpretation. Reflexive awareness was maintained throughout the study to ensure authentic representation of participants’ perspectives. To strengthen transferability, a maximum variation sampling strategy was employed to capture a broad range of experiences and characteristics within the study population. To ensure dependability and confirmability, all audio recordings were transcribed verbatim within 48 hours of completion, and the research team employed triangulation along with repeated team discussions. The entire study was supervised by the corresponding author. Furthermore, the research team held regular discussions to examine the coherence of coding and the appropriateness of emerging themes, making revisions through consensus to minimize researcher bias throughout the analytical process.
Ethics Approval
The study was conducted in accordance with the principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of the First Affiliated Hospital of Guangzhou University of Chinese Medicine (No. k-2024-129). All participants provided written informed consent prior to participation and agreed to the audio recording of their interviews, as well as to the publication of anonymized responses and direct quotes. In addition, informed consent was obtained from the legal guardians of all underage participants before the study. To ensure confidentiality and anonymity, each participant was assigned an alphanumeric ID code.
Results
A total of 17 adolescent patients with SLE, their respective caregivers, and 12 healthcare providers were recruited for this study. The demographic and clinical characteristics of the participants are presented in Table 1 and Table 2. The analysis identified six themes and sixteen subthemes related to transition readiness in adolescents with SLE: (1) knowledge, (2) skills/efficacy, (3) beliefs/expectations, (4) goals, (5) relationships, (6) psychosocial functioning, as summarized in Table 3 and Figure 2.
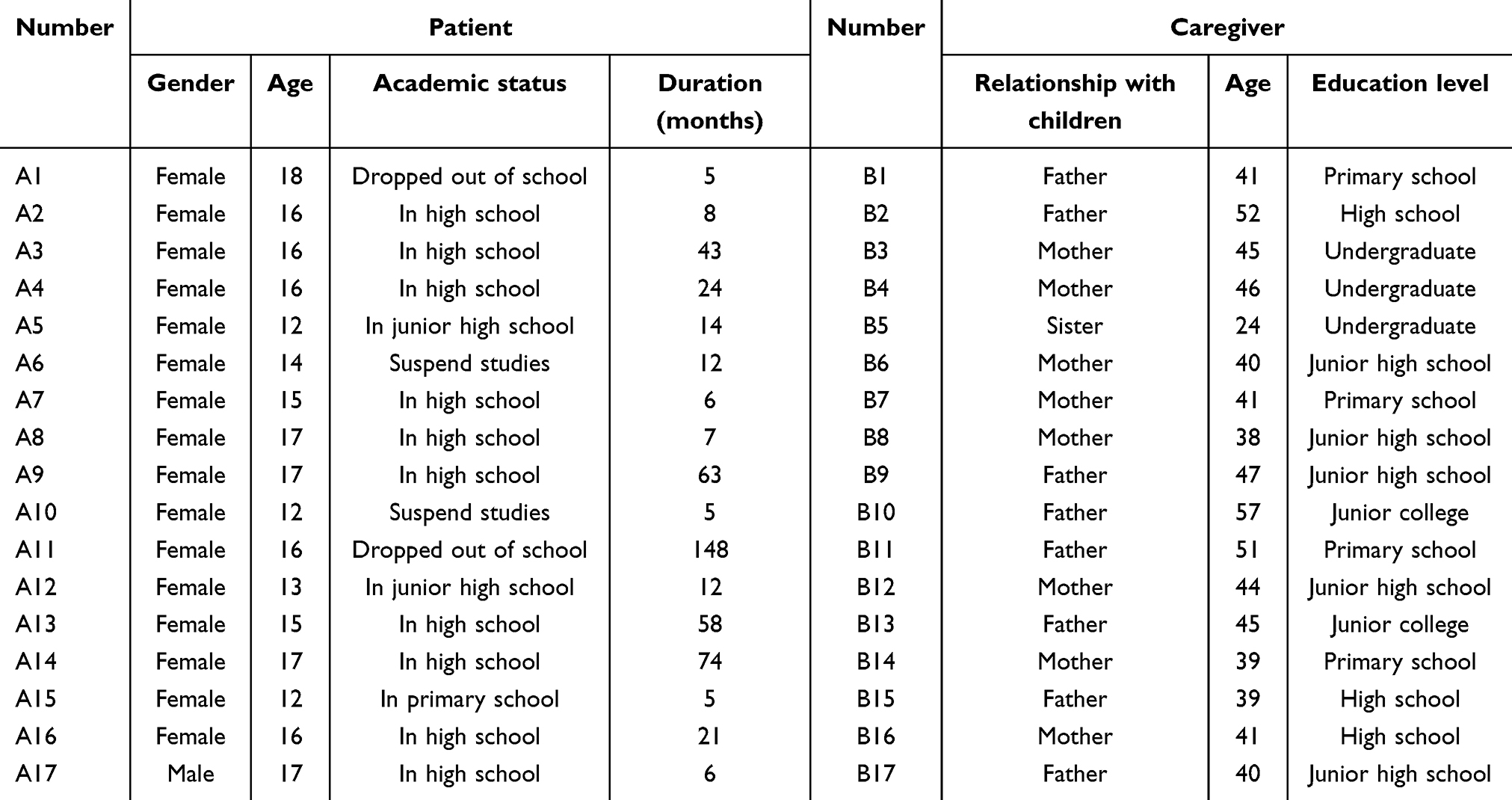 |
Table 1 Sociodemographic Characteristics of SLE Patients and Caregivers (n=17) |
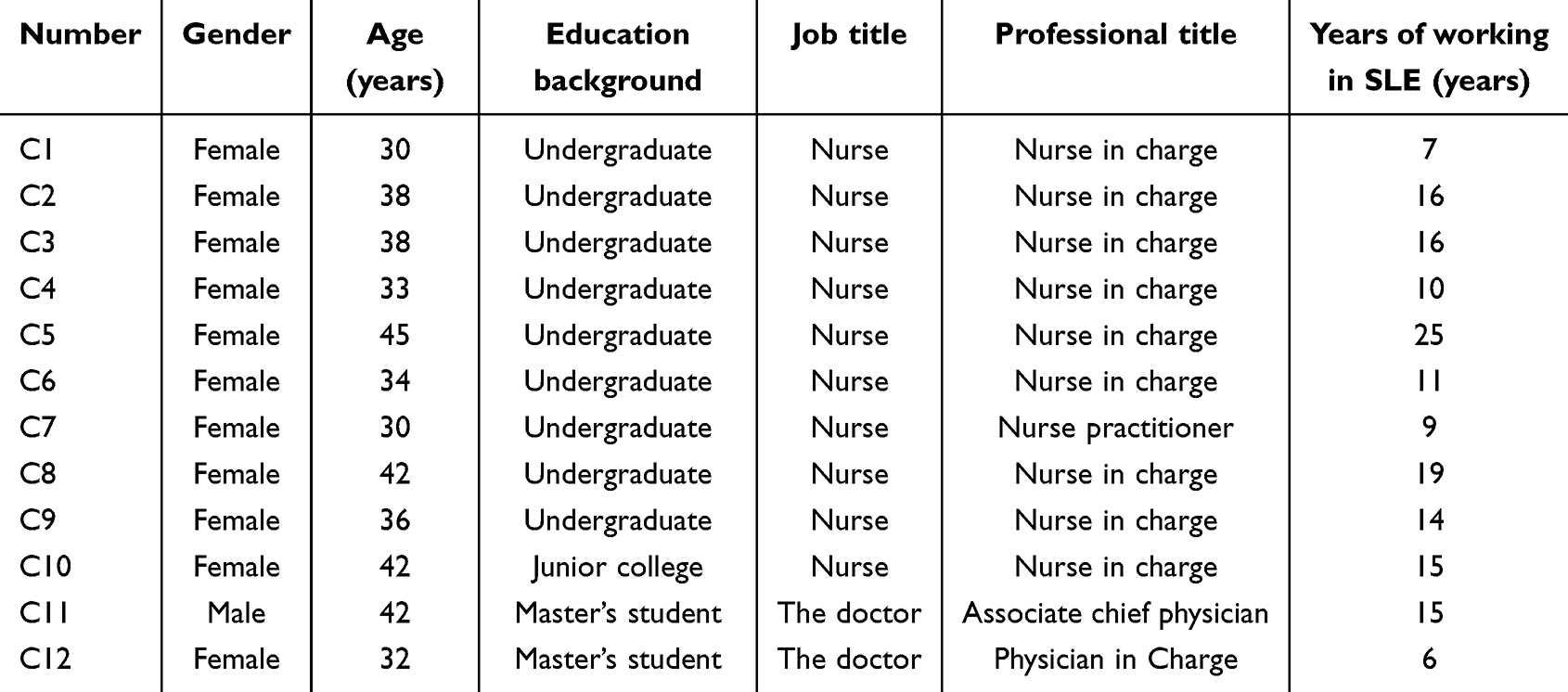 |
Table 2 Sociodemographic Characteristics of Health Care Workers (n=12) |
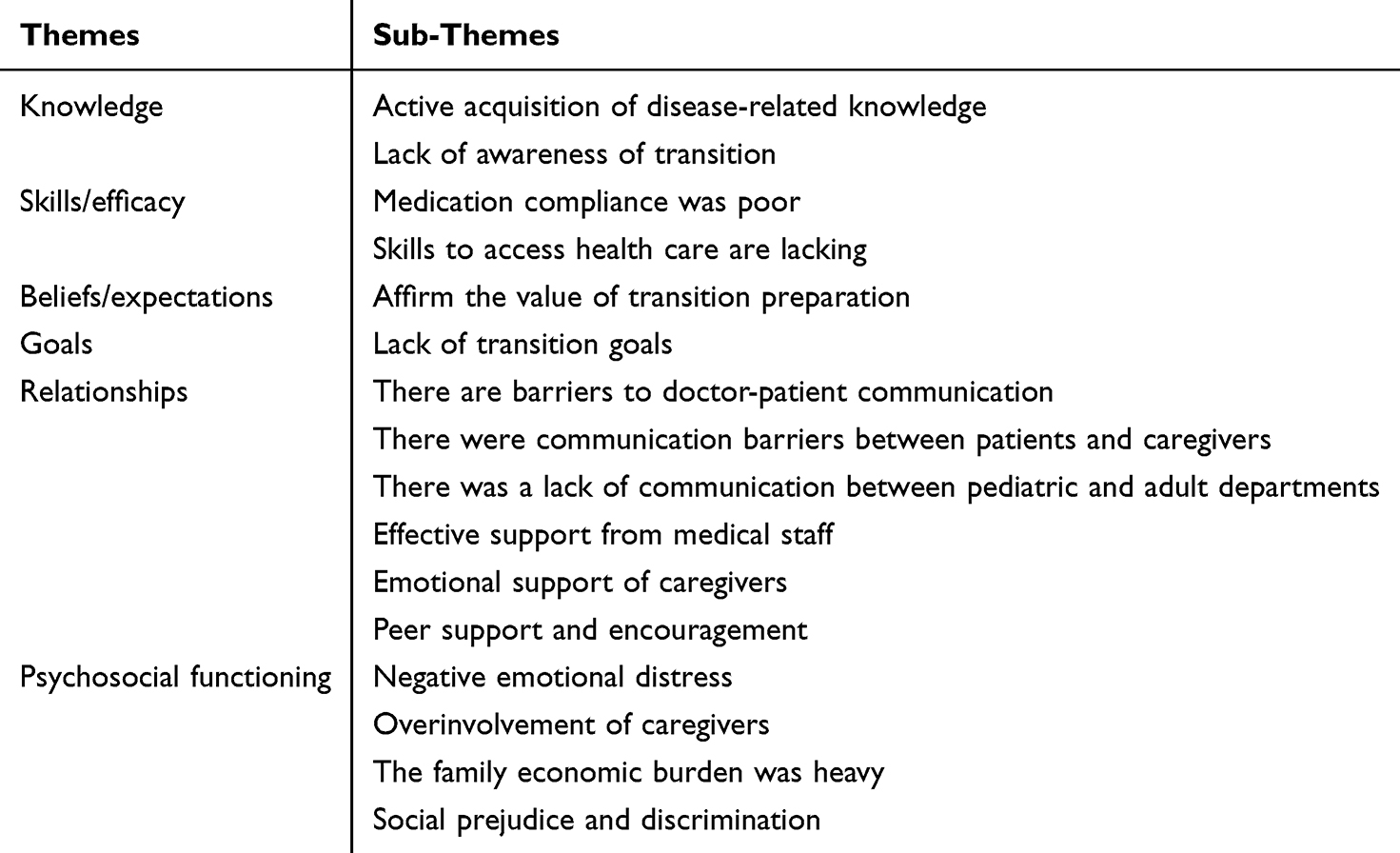 |
Table 3 Themes and Sub-Themes Identified in the Analysis |
 |
Figure 2 Themes and Subthemes of Qualitative Research Findings. |
Theme 1: Knowledge
Active acquisition of disease-related knowledge
Adolescents with SLE are required to adopt specific lifestyle measures for self-management, including avoiding sun exposure, limiting photosensitive foods, and moderating vigorous exercise. Most adolescents with SLE reported actively acquiring knowledge and skills related to SLE to enhance their self-management abilities and transition readiness. Healthcare providers similarly emphasized that patient knowledge of SLE is essential for a successful transition.
I remember what the doctor told me. This disease is mainly controlled by taking medicine. If you suddenly have joint pain, oral ulcers, or facial erythema at home, you need to come to the hospital as soon as possible. (A8)
Combined with my own experience and online research, I know that this is a disease of the immune system, and the clinical manifestations and lifestyle precautions are very clear. (A13)
I have noticed that children who know more about the disease learn to manage it faster when they move to the adult side, and their disease control is better. (C6)
Lack of awareness of transition
In China, transitional care for adolescents with chronic diseases is still in exploratory and developmental stages. There is limited knowledge regarding the transition period and inadequate preparation for transition care. Consequently, most participants were unclear about the concept of transition readiness, which may create obstacles for a smooth transition of SLE patients.
Transition readiness (frowning)? No one ever told me that. (A4)
I do not understand (medical transition) at all. Do not I just take my child to another department? (B14)
If you had not told me about the transition today, I would not have heard about it before.(C3)
Theme 2: Skills/Self-Efficacy
Medication compliance was poor
During the transition period, adolescents with SLE often require long-term, regular administration of multiple medications to control the disease. However, due to limited understanding of drug efficacy and potential side effects, some patients experienced difficulty adhering to prescribed regimens, which might negatively impact the outcome of the transition.
Eating is exhausting for a few months, I don’t want to eat, it’s so annoying, and I don’t take my medication on time in the morning. (A6)
The medication instructions list a long series of side effects, including the possibility that my child may develop deformities in the future, which scared me to death, so terrible, I didn’t dare take the medicine. (A8)
If they are not reminded, they may not take the medicine, and most children need to take Chinese medicine, but Chinese medicine is very bitter, he refused to take this medicine. (C7)
Lack of skills to access healthcare
Proficiency in healthcare-related skills is essential for a successful transition to adult care. However, during interviews, many patients expressed concerns regarding their ability to navigate the healthcare system independently, including scheduling outpatient appointments and managing hospital admissions.
I feel lonely seeing a doctor by myself. I do not know what to do after coming to the clinic. (A8)
I don’t dare come to the hospital alone, because I am unfamiliar with the whole process, especially where the payment is made. (A17)
Children are usually accompanied by their parents when obtaining medications or attending hospital visits, and their ability in this area is still limited. (C9)
Theme 3: Beliefs/Expectations
Affirming the value of transition readiness
The majority of patients and healthcare providers regarded the transition to the adult healthcare system as a critical period that requires careful preparation, and they acknowledged the importance of transition readiness. Some caregivers also recognized that their role should shift from being the primary manager of the disease to serving as a supporter, allowing adolescents sufficient time to develop and enhance self-management skills for a smooth transition.
I feel that preparing in advance not only allows me to know my body better and managel my condition more effectively, but also helps me learn independence more quickly. (A3)
I think (transition readiness) is very important, because you can’t rely on your parents forever, and one day you will need to face it on your own. (A16)
Now I’m starting to let go and let her to learn to visit the adult department and obtain her medications independently. (B13)
Because patients with an earlier age of onset have to face the transition from child to adult, moving from parent-led management to self-management, it is necessary to plan the transition in advance. (C2)
Theme 4: Goals
Lack of transition goals
Most patients were not adequately prepared for the transition period. Current preparation primarily focused on medication adherence and regular follow-up, with limited attention to detailed and comprehensive planning for the broader transition period.
I think I just need to learn how to register and remember the time of picking up my medications. (A1)
Feel Like I Do Not Need to Set Goals or Make Plans. I Can Just Take My Medication on Time. (A11)
Many children don’t have clear self-management goals after they transition, and they are unsure of the next steps, so we need to establish goals with the children and then have parents supervise their implementation. (C5)
Theme 5: Relationships
Barriers to doctor-patient communication
In the adult healthcare system, adolescents with SLE are required to communicate directly with healthcare professionals. However, many adolescents with SLE experienced difficulties in this process due to a lack of confidence and insufficient communication skills, which hindered effective interactions with physicians.
When the doctor asked me how I’ve been recently, I really can’t explain clearly. It would be easier if there were multiple-choice options for me to select from. (A3)
I cannot talk in front of people I do not know well, I am afraid to answer the doctor’s questions. (A6)
I get nervous in front of the doctor. I do not know how to communicate or what to ask or say. (A7)
Children usually do not talk to me much, and sometimes they do not quite understand what we are saying. (C2)
Communication barriers between patients and caregivers
Most caregivers reported difficulties in maintaining effective communication with their children. They expressed concerns that inappropriate words or attitudes might increase the psychological burden of their children, thereby creating barriers to parent-child communication. Meanwhile, some adolescent patients also reported resistance to engaging in conversations with their caregivers, which might hinder effective transition readiness.
After I got sick, my parents often quarrel with each other, and they are usually busy with work, so I don’t take the initiative to contact them and don’t want to talk to them. (A12)
I tell her to rest early and take her medicine every day, but she never listens. How dare I let her be independent? (B5)
Every time I say something about her, she immediately loses her temper, so we rarely communicate, and I especially avoid mentioning the illness. (B8)
Lack of communication between pediatric and adult departments
According to several patients and caregivers, the transition process should involve collaborative participation from both pediatric and adult healthcare providers. Effective communication between these departments, particularly when pediatric healthcare providers introduce the child’s health history and treatment details to their adult counterparts, can effectively facilitate a smoother transition and help prevent unnecessary medical issues.
When transferring from children’s hospital to this side, I have to repeat my situation to the doctor again, it feels so troublesome. (A6)
I wish there could be an exchange of medical records between hospitals, so that adult doctors could better understand more about the child’s condition from pediatrics. (B3)
After being transferred to the adult department, my child has to repeat blood tests and undergo all kinds of examinations again, which is quite a torment of the child. It would be much more convenient if the results from the previous hospital could be directly accessed. (B15)
We’re doctors in the adult department, but in fact, we can communicate more with pediatricians, such as about children’s medication experience and the handover of treatment from pediatric care. Ideally, a designed physician should oversee this transition process. (C11)
Effective support from healthcare providers
Interviews revealed that adolescents with SLE regarded healthcare providers as key facilitators in the transition to adult healthcare. They believed that these professionals not only provided medical services and a sense of security, but also offered emotional support that helped them to adapt to the adult care model. In addition, healthcare providers also reported that they actively encouraged patients to participate in disease self-management.
Whenever I want to know something, the doctor will explain it to me, treat me kindly, and show genuine care. (A12)
I like the doctors and nurses in the adult department because they communicate directly with me, speak gently, and maintain a good attitude. (A14)
Doctors and nurses will carefully remind me not to eat photosensitive foods and not to get too tired. (A15)
During ward rounds, we will actively ask the children where they feel uncomfortable, mainly to foster their awareness of active participation in disease management. (C12)
Emotional support of caregivers
Most patients emphasized the crucial role of family support in managing their illness, daily life, and transition to the adult healthcare system. In particular, the emotional encouragement and psychological support provided by family members were viewed as key factors that enhanced patients’ confidence during this critical period.
My family protects me very well. They remind me to take medicine in the morning. They also tell me not to eat snacks. (A10)
I usually tell her that her illness is not a big deal, the medicine is well-developed now, and doctors are highly skilled. With the right treatment, the disease can be controlled, and she can grow up as healthy as other people. (B1)
She’s coming of age, and this transition period is quite challenging for us. But as her mom, I will try to make her happy, encourage her, and help her feel that her family truly cares about her. (B4)
Peer support and encouragement
SLE is a chronic and difficult-to-cure disease, making it important for adolescents to connect with peers who share similar experiences to facilitate a smooth transition to adult care. Some adolescents reported that sharing experiences with other patients not only alleviated feelings of isolation but also improved their ability to cope with the disease. Healthcare providers also emphasized that establishing peer connections allows patients to gradually assume more responsibility in a supportive environment, thereby enhancing transition readiness.
I like communicating with other patients because everyone has similar experiences and can empathize with each other. (A3)
I added a sister on WeChat. We usually don’t chat much, but she reminds me of many things I need to pay attention to, which makes me feel very supported. (A11)
I think we could establish peer groups or exchange meetings because peer communication is very effective. This way, they can encourage each other and learn transition-related knowledge and skills together. (C1)
Theme 6: Psychosocial Functioning
Negative emotional distress
Due to the rapid progression and its incurable nature of SLE, most adolescents and their caregivers are prone to negative emotions, including pessimism and denial. In addition, healthcare providers also observed that caregivers’ emotional states influence patients’ motivation for treatment, which may hinder patient engagement with the healthcare system and delay the transition to adult care.
At that time, I knew this disease could not be cured, I felt very negative, and even feel that life was not interesting. (A8)
After taking the medication, my hair fell out badly, and I felt very uncomfortable. I was too ill to attend school, felt very unhappy, and couldn’t help it. (A11)
She is only 16 years old. I really can’t accept that she has to live with this disease for the rest of her life. It’s very sad. (B2)
Parents’ negative mood will directly affect their children. The children will also act unhappy, worry excessively about the disease, and may resist treatment. (C10)
Overinvolvement of caregivers
Caregivers’ understanding and support are invaluable in helping adolescents develop life skills and build confidence in managing SLE. However, in Chinese-style families, caregivers often overlook adolescents’ enthusiasm for self-management, interfere with their independence and autonomous participation in disease management, hinder the development of adolescents’ self-management skills, and consequently affect the transition process.
I think my family is too protective of me. In fact, it would be fine for me to go to the doctor by myself, but they request leave to accompany me every time, which is unnecessary. (A2)
I am almost an adult, yet my family always treats me like a child. I really wanted to come to the hospital to get the medication myself, but they thought I couldn’t manage it, so they didn’t let me. (A9)
I think she is too young to understand many things, so I communicate with the doctor and make decisions about her illness. (B10)
Some parents take fully charge of the child’s affairs, and overly protective, and believe the child should lie in bed to rest due to the illness. As a result,n the child learns very little about theire disease. (C4)
The family economic burden was heavy
Currently, there is no effective cure for SLE, and patients must rely on long-term medication to maintain disease stability. Most caregivers reported that the ongoing cost of treatment and regular follow-up appointments imposed a substantial financial burden. In addition, caregivers expressed particular concern that patients may be unable to obtain or maintain health insurance in adulthood, which could compromise treatment continuity and the stability of the transition process.
She is still on free health care, which is guaranteed until she is 18, but not when she becomes an adult. (B3)
Her illness requires long-term treatment, but the family’s income is limited. She now has to pay for the medication every month, which is really stressful. I don’t know if I can continue the treatment. (B9)
It took a long time at home for her condition to become so severe because the family’s money was all spent. I could only bring her to the hospital by borrowing money from relatives. (B11)
The cost of treatment is still significant, and some patients do not continue hospital treatment in adulthood because they cannot afford it. (C7)
Social prejudice and discrimination
Most participants reported that encountering negative perceptions and attitudes upon returning to school directly undermined their confidence in managing their illness, which made it more difficult for them to obtain social support and successfully transition to adult care.
I have become a celebrity at school now because the whole school knows about my illness. It makes me feel uncomfortable and excluded by everyone. (A5)
The child eat hormones, which caused her face to develop red spots. Classmates mistakenly think that she has an infectious disease, are avoided her, which made her feel very lonely. (B6)
Some children tell me that they are often teased by others, which makes them want to avoid treatment. (C8)
Discussion
To the best of our knowledge, this is the first qualitative study to investigate the factors influencing transition readiness among adolescents with SLE from the perspectives of adolescents with SLE, their parents, and healthcare providers using the SMART model as a guiding framework. The interview findings indicated that transition readiness is comprehensively shaped by multiple interrelated factors, which align closely with the factors outlined in the SMART theoretical framework. These included (1) knowledge, encompassing both the active acquisition of disease-related information and a general lack of transition awareness; (2) skills/efficacy, characterized by poor medication adherence and insufficient competence in navigating healthcare systems; (3) beliefs/expectations, reflecting recognition of the importance of transition readiness; (4) goals, primarily defined by the absence of clear transition objectives; (5) relationships, incorporating barriers such as communication challenges between patients and healthcare providers or caregivers, a lack of coordination between pediatric and adult care departments, as well as facilitators like support from healthcare providers, emotional support from caregivers, and peer encouragement; (6) psychosocial functioning, manifested as emotional distress, caregiver over-involvement, substantial family financial burdens, alongside experiences of social stigma and discrimination. Together, these factors illustrate the challenges that may affect adolescents with SLE during the transition period in the Chinese context. Based on these influencing factors, a transition intervention program tailored to the needs of Chinese adolescents with SLE can be developed.
The results of this study indicate that disease-related knowledge is a predictor of transition readiness, which aligns with the findings reported by Stewart et al33 Moreover, patients, parents and healthcare providers collectively acknowledged that the transition period plays a critical role in cultivating self-management abilities and achieving effective disease control. However, our study also revealed a widespread and profound problem: patients were completely unfamiliar with the term “transition readiness”; caregivers were confused and focused only on logistical matters such as changing departments; and healthcare providers also admitted having no prior knowledge of the transition process. This universal lack of awareness highlights a systemic educational gap in China’s current transitional care system, rooted in cultural and healthcare differences between China and the West. Western healthcare systems actively promote adolescent autonomy and encourage young people to gradually assume responsibility for their own health. In contrast, China’s family-centered decision-making model dominates, with parents playing a core role in medical decisions, which often delays the development of independent health behaviors in adolescents.34 Furthermore, unlike Western countries where well-established transition programmes exist, China lacks systematic, localised transition models, and the fragmentation between paediatric and adult rheumatology departments further exacerbates the inadequacy of transition readiness.35 Therefore, Western transition interventions cannot be simply transplanted.
From the perspective of the Capability, Opportunity, Motivation-Behaviour (COM-B) model, behaviour change requires capability (psychological and physical ability to perform the behaviour), opportunity (external factors that enable the behaviour), and motivation (automatic and reflective processes that drive behaviour).36 Therefore, at the patient level, drawing on international experience, a transition clinic led by advanced practice nurses can be established.37 Through standardised transition education modules, using methods such as educational booklets, video presentations, and online/offline lectures, patients can be taught the core concepts of healthcare transition, the implementation process, and disease-related knowledge, thereby strengthening their mastery of transition-related information, enhancing their reflective motivation, and building psychological capability. At the same time, peer support programmes such as lupus summer camps and simulation exercises (eg., booking adult appointments, refilling prescriptions, communicating with new providers) can be offered to create practical opportunities.38 At the caregiver level, healthcare providers can actively build a family network community for systemic lupus erythematosus. On the one hand, this community can be used to provide transition-related education and training; on the other hand, caregivers can be encouraged to freely exchange experiences and feelings within the community while receiving professional guidance, thereby helping them shift from a purely logistical understanding to a developmental perspective that supports adolescent autonomy, gradually relinquishing decision-making control, improving social opportunities, and alleviating financial and emotional burdens. At the healthcare system and provider level, given the current situation in China, a transition coordinator role (composed of nurses) should be established to bridge paediatric and adult rheumatology departments. Providers need to receive training in transition-specific communication and shared decision-making through appropriate resource allocation, staffing adjustments, continuing education, and systematic training. A localised transition protocol tailored to China’s family-centred and fragmented context should be developed to create systemic opportunities.
This study identified poor medication adherence and limited healthcare navigation skills as key challenges during the transition period for adolescents with SLE. According to Lawson et al, insufficient self-management abilities, such as frequent missed doses and difficulty in independently scheduling medical appointments, are major factors that impede the smooth transfer into the adult healthcare system,39 which is consistent with the findings of this study. However, our findings further reveal that these challenges manifest differently across stakeholder groups. Regarding medication adherence, patients frequently reported distress caused by medication side effects and the long duration of treatment, leading to intentional non-adherence. In contrast, healthcare providers reported that many adolescents refuse to take the bitter-tasting traditional Chinese medicine prescribed to them, which places a considerable supervisory burden on caregivers. These differences indicate that adherence interventions must simultaneously address the distinct needs of patients (alleviating fear of side effects, fostering intrinsic motivation for medication) and caregivers (reducing supervisory burden, designing phased strategies for relinquishing control). Regarding healthcare navigation skills, patients expressed anxiety and lack of confidence in independently completing tasks such as scheduling outpatient appointments and managing hospital admissions. Healthcare providers acknowledged that adolescents’ practical skills remain limited, as most are still accompanied by their parents. Beyond adherence and navigation skills, the lack of goal setting also deserves attention. Based on social cognitive theory,40 clearly defined goals can effectively stimulate individual self-regulatory behaviors. However, this study found that most adolescents lacked explicit transition goals, with many holding overly simplistic or passive views (eg., believing that simply learning to register for appointments or taking medication on time is sufficient). Healthcare providers confirmed this gap, noting that many adolescents have no clear self-management goals after the transition and are unsure of the next steps. The absence of structured, stage-specific goals directly weakens patients’ intrinsic motivation for adherence and self-management.
Therefore, to address poor medication adherence, it is recommended to establish a pharmacist-led home medication service team to proactively reach adolescent SLE patients. At discharge, medication assessment, detailed medication instructions, and home medication education should be provided. During follow-up, repeated education on medication knowledge is necessary to promptly identify and correct erroneous medication behaviors caused by excessive fear of side effects, thereby ensuring medication safety and treatment continuity. In addition, visualized, standardized medication tools such as smart pillboxes or smart bottles with recording and reminder functions should be promoted to help patients track remaining medication, identify missed doses, and explore reasons for non-adherence.41 For caregivers, a phased responsibility transfer plan should be developed, guiding them to gradually reduce direct reminders (eg., from daily reminders to weekly pillbox checks) and learn to use smart tools to track patients’ medication behavior, thereby reducing their own supervisory burden while enhancing patients’ autonomous medication motivation. Second, to address limited healthcare navigation skills, healthcare providers should adopt peer-interactive skill training methods such as role-play and situational simulation to help patients master practical skills including appointment booking and hospital admission procedures.42 Patients should also be directed to resources such as the MyLupusGuide website to access international treatment information, learn complete clinical visit processes, and perform self-monitoring of disease activity, thereby enhancing self-efficacy.43 For caregivers, the team should provide targeted training to clarify their critical role in fostering adolescents’ independent healthcare skills and guide them on how to gradually step back: for example, during the initial stage of a patient’s practice of scheduling an appointment, the caregiver should shift from full accompaniment to observing from the side, offering hints only when errors occur, rather than taking over the task. Third, to address the lack of goal setting, it is important to recognize that structured transition planning can significantly improve outcomes. Previous studies have shown that the development of targeted transition programs can improve disease outcomes and enhance quality of life among adolescent patients.44 Therefore, it is recommended that a transitional medical team develop a patient-centered preparation plan informed by comprehensive assessments of individual patients’ needs.45 To this end, a multidisciplinary transition team comprising family caregivers, specialized healthcare professionals, social workers, and school educators should be established, and a transition readiness instrument suitable for Chinese adolescents with SLE should be adapted or developed using validated international assessment tools to conduct comprehensive patient assessments.46 According to the assessment results, specific, measurable transition goals should be jointly set with patients and caregivers. For example, a patient should independently complete a clinic appointment within one month; the caregiver should shift from full accompaniment to only providing necessary support and document the specific steps of letting go. An empowerment-based motivational education model can then guide patients to reflect on their achievements and challenges during goal implementation, summarize coping strategies, and thereby strengthen their motivation to achieve goals.47 In addition, the multidisciplinary team should establish a regular dynamic evaluation mechanism to closely monitor patients’ disease status, psychological state, and transition readiness, optimizing the transition plan as needed to help patients progressively acquire transition skills.
This study found that communication barriers are a major factor affecting the smooth transition of adolescents with SLE to the adult healthcare system. These barriers manifest at three levels: doctor-patient communication, communication between patients and caregivers, and communication between pediatric and adult departments. Each level negatively affects patients’ self-management abilities and the process of patient empowerment. At the doctor-patient communication level, many adolescents lack confidence and communication skills, making it difficult for them to clearly describe their condition. Healthcare providers also report that children often have difficulty understanding adult expressions. This barrier excludes patients from decision-making, hinders their active participation in their own health management, and delays patient empowerment. At the patient-caregiver communication level, patients distance themselves from their parents due to family conflicts or emotional resistance. Caregivers find that their children ignore advice or lose their temper when illness is mentioned. As a result, parents dare not let go and become overly involved in healthcare arrangements, which impedes the development of adolescents’ autonomous self-management abilities. At the communication level between pediatric and adult departments, patients have to repeat their medical history and undergo repeated examinations after transfer. Medical records are not shared, and there is a lack of effective coordination between pediatric and adult departments. This leaves patients feeling confused and distrustful, reduces continuity of care, and weakens their confidence in managing their own health.
The reason can be attributed to the developmental characteristics of adolescence, a critical period marking the transition from childhood to adulthood. During this stage, physical and psychological development is often unbalanced, and the coexistence of a chronic serious disease can easily lead adolescents to experience various emotional and behavioral problems.48,49 These developmental features may hinder their ability to communicate and express their needs effectively. Meanwhile, inadequate communication skills among caregivers and healthcare providers may further intensify patients’ psychological burden and exacerbate communication barriers. Interdepartmental communication barriers are largely associated with substantial differences between the pediatric and adult healthcare systems, insufficient coordination of care, and a lack of continuity during the transition process.50 To address the differentiated barriers faced by different stakeholder groups in the local Chinese healthcare context, the following specific and actionable recommendations are proposed. For patients, healthcare providers should actively use visual communication aids (eg., simple symptom checklists and emotional expression scales) in outpatient settings to help adolescents with communication difficulties describe their condition more clearly, and a dedicated adolescent consultation period of 5–10 minutes should be established during which the adolescent is encouraged to speak with the doctor first before the parent is invited in, so as to gradually develop self-advocacy skills. For caregivers, hospitals should regularly organize transition family communication workshops led by psychotherapists to guide parents in using non-blaming communication techniques, including how to discuss disease and transition-related topics in a gentle and open manner, how to recognize and respond to the adolescent’s emotional cues, and how to remain calm in conflict situations. For the healthcare system, previous studies have pointed out that involving pediatric and adult specialists in transition teams can enhance transition outcomes and promote patient health.51 Therefore, a designated physician should be assigned to follow the entire transition process, responsible for compiling the patient’s medical summary before transfer and organizing a three-party joint meeting (involving the pediatrician, adult physician, patient, and parent) after transfer; moreover, efforts should be made to promote the sharing of electronic medical records between hospitals or to develop a standardized “transition passport” handbook that the patient can carry with them, recording key medical information to avoid repeated examinations and information gaps.
Furthermore, this study found that the support and encouragement of healthcare providers, caregivers and peers plays an essential role in facilitating a successful transition for adolescents with SLE, which is consistent with the findings of Hovde et al.52 Healthcare providers offer professional guidance, gentle communication, and active encouragement for self-management. This direct, respectful interaction helps adolescents build confidence to take initiative in their own care, directly promoting self-management and patient empowerment. Caregivers provide daily reminders, emotional reassurance, and normalization of the illness. This support enhances patients’ emotional security and confidence during the transition period. Peers offer shared experiences and mutual encouragement, reducing feelings of isolation and enhancing intrinsic motivation. Peer support uniquely fosters a sense of belonging, which strengthens self-management and adherence. Therefore, it is recommended that healthcare providers integrate brief empowerment conversations and emotional encouragement into routine clinical encounters. For example, during each outpatient visit, providers should actively motivate and encourage patients to engage in their own disease management, while also attending to their life and psychological well-being. For caregivers, they should create a supportive and emotionally encouraging home environment by establishing simple, positive daily routines, such as spending more time with the adolescent, using affirming language to acknowledge the adolescent’s independent efforts, and allowing the adolescent to safely express concerns in a non-judgmental atmosphere. Regarding peer support, structured and safe opportunities for peer interaction should be promoted. For instance, the hospital could establish a “SLE peer support WeChat group” moderated by a nurse or psychotherapist, where adolescents can ask questions, share experiences, and receive encouragement. Monthly themed discussions may also be organized to keep the group active and focused on transition-related skills.
The results indicate that most adolescents with SLE experience negative emotions such as despair, low self-esteem, and depression, which adversely affect their transition process. These findings are consistent with previous studies.53 One possible explanation is that there is currently no definitive cure for SLE, and adolescents with SLE often exhibit a more acute onset, more severe disease activity, a longer disease course, and a greater likelihood of major organ involvement compared with adults. In addition, adolescence is a critical stage for the formation of self-identity. Changes in physical appearance (eg., erythema and alopecia) and medication-associated side effects (eg., weight gain) can lead to intense emotional distress, as reflected in patients’ reports of feeling that “life was not interesting” and being “too ill to attend school.” It is noteworthy that the emotional state of family caregivers differs significantly from that of patients. Caregivers primarily experience sadness and disbelief that their child must live with a lifelong illness. Evidence suggests that the negative emotions of caregivers are a key factor in successful transition and positive developmental outcomes in children.54 Caregivers’ psychological distress may further aggravate patients’ emotional burden, which is consistent with the findings of this study. Moreover, healthcare providers observed that caregivers’ negative emotions directly affect patients, causing adolescents to act unhappy, worry excessively about the disease, and even resist treatment. This bidirectional emotional contagion means that caregiver distress does not merely add to the patient’s burden but actively undermines the adolescent’s motivation for self-management and adherence. Consequently, patient empowerment-the process of gaining confidence and control over one’s own health-is severely hindered when both parties are trapped in a cycle of negativity.
Therefore, healthcare providers should offer emotional support and provide training in emotion regulation and coping strategies tailored to adolescents. Specific measures include establishing adolescent mental health service stations, disseminating mental health knowledge via WeChat public platforms, and organizing regular psychological education sessions. Rheumatology nurses or psychotherapists should conduct periodic group counseling on disease acceptance, and joint workshops with dermatology and nutrition departments can offer image management support (eg., cosmetic coverage, wig selection, weight control). Hospitals should collaborate with educational institutions to provide bedside schools or online tutoring to address schooling disruptions. At the same time, caregivers’ psychological status should be assessed. They should be encouraged to express their feelings and communicate negative emotions. Specific measures include regular psychological assessment and interviews for disease acceptance, followed by individualized counseling or cognitive restructuring. Joint parent-child emotion management workshops can teach caregivers to communicate calmly and avoid transmitting anxiety. For caregivers experiencing long-term emotional distress, online psychological interventions and positive psychology-based treatment programs may be offered, while also helping them share coping strategies and reinforce their positive role during the transition period.55
In addition, the present study found that caregiver over-involvement is a major barrier to transition readiness, but its impact differs notably across stakeholders. Patients expressed a desire for more autonomy, feeling that family members are overprotective, for example, by accompanying them to clinic visits unnecessarily or preventing them from performing simple healthcare tasks such as picking up medication independently. In contrast, caregivers themselves perceived their over-involvement as necessary protection, believing that the adolescent is too young to understand many things and therefore taking full charge of communication with doctors and treatment decisions. Healthcare providers confirmed this pattern, noting that some parents take complete control and even believe the child should rest in bed at all times, leaving the adolescent with very little knowledge about their own disease. This finding aligns with previous studies.56 A potential explanation is that, influenced by traditional Chinese family values, caregivers (particularly parents) tend to view children as fully dependent and often adopt overprotective behaviors, neglecting the ongoing development of adolescents’ disease knowledge and self-care abilities. For such caregivers, it is essential to help them understand their evolving role from “leader” to “supporter” and to provide guidance on gradually transferring responsibility for health management to adolescents. To achieve this, cognitive behavioral therapy can be used to help caregivers recognize the negative impact of overprotection on transition readiness, thereby reducing their excessive worry about letting go and alleviating caregiving burden.57 At the same time, caregivers should be encouraged to optimize responsibility sharing by sharing medical information and gradually returning communication and decision-making power to the adolescent, thereby transforming family interactions during clinical encounters from a dominant role to a supervisory and coordinating role, which promotes the development of the adolescent’s self-management skills.
During the interviews, participants also expressed concerns that the heavy financial burden on families may interrupt transition readiness. It is therefore recommended that relevant authorities should strengthen drug price monitoring, standardize diagnostic procedures, appropriately reduce the costs of medications and examinations, and develop corresponding medical policies to ensure continuous and stable medical insurance coverage for adolescents with SLE during the transition period. Moreover, efforts should be made to promote the establishment of dedicated support organizations for adolescents with SLE and to leverage public welfare and fundraising platforms to provide financial assistance to affected families, thereby alleviating their economic burden.
In addition to the internal barriers discussed above, this study found that adolescents with SLE are vulnerable to social prejudice and discrimination, which significantly undermines their transition readiness. The impact of such prejudice, however, differs across stakeholders. Patients reported that negative perceptions from peers at school directly damaged their confidence in managing their illness, making them feel excluded and uncomfortable. Caregivers observed that disease-related changes in appearance (eg., facial spots caused by hormone therapy) led classmates to mistakenly believe the condition was infectious, resulting in avoidance and social isolation for the adolescent. Healthcare providers confirmed that adolescents who are teased or stigmatized often develop a desire to avoid treatment altogether. These findings indicate that social prejudice not only harms the adolescent’s emotional well-being but also directly weakens their motivation for self-management and treatment adherence. When patients feel rejected by their social environment, they are less likely to engage in active disease management or seek necessary care, thereby delaying patient empowerment and a smooth transition. Therefore, for patients, interventions should focus on cognitive restructuring to help adolescents reframe negative peer reactions and reduce the emotional impact of discrimination. This includes guiding patients to identify automatic negative thoughts triggered by stigmatizing encounters, challenging the validity of these thoughts, and developing more balanced, self-affirming interpretations of social situations. For caregivers, healthcare providers should issue official medical certificates and clear written explanations of the disease characteristics, emphasizing that SLE is non-communicable and that patients can participate normally in school activities. These documents can be shared with schools to correct misconceptions and foster a more inclusive environment. For healthcare providers, they should take an active role in disseminating accurate disease-related knowledge to schools and communities by organizing school-based health education lectures, distributing easy-to-understand brochures about SLE, and collaborating with school nurses to correct myths. At the policy level, hospitals and public health agencies should use government and media platforms (eg., WeChat public accounts, short videos) to launch public awareness campaigns about SLE, highlighting that the disease is not infectious and that patients deserve full social inclusion. These targeted, multi-level interventions addressing the needs of patients, caregivers, providers, schools, and the broader public can help reduce stigma, strengthen self-management and adherence in adolescents with SLE, and ultimately support a more successful transition to adult care.
Conclusion
Drawing upon the SMART theoretical framework, this study explored the factors influencing transition readiness among adolescents with SLE through qualitative interviews integrating perspectives from patients, caregivers, and healthcare providers. Six themes were identified: knowledge, skills/efficacy, beliefs/expectations, goals, relationships, and psychosocial functioning. The findings reveal that transition readiness is a complex, multidimensional process shaped by interacting factors at the individual, familial, peer, and healthcare system levels. This insight fills a gap in the existing literature, which has largely focused on single‑stakeholder or Western-centric perspectives, and provides a clear theoretical basis and practical direction for clinical healthcare professionals to implement targeted interventions. At the clinical level, healthcare providers can implement targeted interventions addressing the six SMART themes to enhance transition readiness in adolescents with SLE. For knowledge, providers should offer standardised education to improve disease and transition awareness. For skills/efficacy, training should be provided to strengthen medication adherence and healthcare navigation abilities. For beliefs/expectations, misconceptions should be corrected and positive attitudes toward transition should be fostered. For goals, specific, measurable transition objectives should be co-created with patients and caregivers, with regular progress evaluations. For relationships, communication among patients, caregivers, and providers should be improved, peer support facilitated, and paediatric-adult care coordination strengthened. For psychosocial functioning, emotional distress, overprotection, financial burden, and social stigma should be addressed through psychological support, family guidance, and policy advocacy. This approach aims to meaningfully improve transition readiness for adolescents with SLE in China by operationalising the six themes through provider-led, patient-centred actions.
Strengths and Limitations
A major strength of this study is the adoption of the SMART model as its theoretical framework. Respondents discussed relevant facilitators and barriers in detail across the various levels of the framework. This also suggests that interventions developed in accordance with these influencing factors hold substantial potential to support a smooth transition into the adult healthcare system.
However, several limitations must be critically examined. First, regarding transferability, all participants were recruited from a single tertiary hospital in Guangzhou, China. This convenience sampling approach, combined with a relatively small and demographically homogeneous sample, significantly limits the generalizability of our findings to other geographic regions, healthcare settings, or patient populations with different socioeconomic and cultural backgrounds. The results should therefore be interpreted as context-specific rather than broadly representative. Second, concerning cultural specificity, the study was conducted within a Chinese healthcare and family environment characterized by strong family-centered decision-making, high parental involvement, and fragmented pediatric-adult transition pathways. While these features reflect the local context, they also mean that our findings may not directly apply to Western or other non-Chinese settings where healthcare systems and family dynamics differ substantially. Conversely, the cultural specificity is also a strength, as it provides novel insights into an underexplored population. Third, with respect to selection bias, participants were recruited voluntarily, which may have introduced self-selection bias. Families who agreed to participate might have been more motivated, better educated, or more concerned about transition issues than those who declined. This could have led to an overestimation of certain barriers or an underestimation of others. Additionally, caregivers who were overburdened or less engaged may have been less likely to participate, potentially skewing the findings toward more proactive families. To address transferability, cultural specificity, and selection bias limitations, future research should expand the sample size, recruit participants from different regions and hospitals across China as well as from diverse cultural backgrounds, and adopt strategies to minimize self-selection bias. These measures would enhance the representativeness of the sample and the general applicability of the results.
Acknowledgment
The authors would like to thank the people who participated in this study for their valuable feedback.
Author Contributions
All authors made a significant contribution to the work reported, whether in conception, study design, execution, data acquisition, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval to the version to be published; have reached a consensus on the journal to which the article was submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was supported by research grants from Guangdong Medical Science and Technology Research Foundation (A2024401).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ameer MA, Chaudhry H, Mushtaq J, et al. An overview of systemic lupus erythematosus (SLE) pathogenesis, classification, and management. Cureus. 2022;14(10):e30330. doi:10.7759/cureus.30330
2. Charras A, Smith E, Hedrich CM. Systemic lupus erythematosus in children and young people. Curr Rheumatol Rep. 2021;23(3):20. doi:10.1007/s11926-021-00985-0
3. Tian J, Zhang D, Yao X, Huang Y, Lu Q. Global epidemiology of systemic lupus erythematosus: a comprehensive systematic analysis and modelling study. Ann Rheum Dis. 2023;82(3):351–20. doi:10.1136/ard-2022-223035
4. Hersh A, von Scheven E, Yelin E. Adult outcomes of childhood-onset rheumatic diseases. Nat Rev Rheumatol. 2011;7(5):290–295. doi:10.1038/nrrheum.2011.38
5. Ambrose N, Morgan TA, Galloway J, et al. Differences in disease phenotype and severity in SLE across age groups. Lupus. 2016;25(14):1542–1550. doi:10.1177/0961203316644333
6. McKenzie RB, Sanders L, Bhattacharya J, Bundorf MK. Health care system factors associated with transition preparation in youth with special health care needs. Popul Health Manag. 2019;22(1):63–73. doi:10.1089/pop.2018.0027
7. Conti F, Pontikaki I, D’Andrea M, Ravelli A, De Benedetti F. Patients with juvenile idiopathic arthritis become adults: the role of transitional care. Clin Exp Rheumatol. 2018;36(6):1086–1094.
8. Chang JC, Knight AM, Lawson EF. Patterns of healthcare use and medication adherence among youth with systemic lupus erythematosus during transfer from pediatric to adult care. J Rheumatol. 2021;48(1):105–113. doi:10.3899/jrheum.191029
9. Felsenstein S, Reiff AO, Ramanathan A. Transition of care and health-related outcomes in pediatric-onset systemic lupus erythematosus. Arthritis Care Res. 2015;67(11):1521–1528. doi:10.1002/acr.22611
10. Varty M, Popejoy LL. A systematic review of transition readiness in youth with chronic disease. West J Nurs Res. 2020;42(7):554–566. doi:10.1177/0193945919875470
11. Zhu Y, Chen Y, Hu J, et al. Effectiveness of a remote intervention program for self-management behaviors in adolescents and young adults with inflammatory bowel disease based on the self-determination theory: randomized controlled trial across 2 centers. J Med Internet Res. 2025;27:e79370. doi:10.2196/79370
12. Karadag P, Taylor J, Burton A. Self-management and coping in young adults with chronic pain: a reflexive thematic analysis. J Health Psychol. 2025;30(12):3518–3534. doi:10.1177/13591053251344236
13. Hiratsuka K, Nakamura N. Process model for transitioning care responsibility to adolescents and young adults with biliary atresia: a secondary and integrative analysis. Nurs Rep. 2025;15(8):308. doi:10.3390/nursrep15080308
14. Stutzin Donoso F. From self-management to shared-management: a relational approach for equitable chronic care. Public Health Ethics. 2024;17(3):85–100. doi:10.1093/phe/phae007
15. Roberts JE, Halyabar O, Petty CR, et al. Longitudinal assessment of preparation for care transition among adolescents and young adults with rheumatologic disease: a single-center pilot study. Pediatr Rheumatol Online J. 2022;20:93. doi:10.1186/s12969-022-00751-1
16. Ciosek AL, Makris UE, Kramer J, et al. Health literacy and patient activation in the pediatric to adult transition in systemic lupus erythematosus: patient and health care team perspectives. ACR Open Rheumatol. 2022;4(9):782–793. doi:10.1002/acr2.11474
17. Kittivisuit S, Lerkvaleekul B, Soponkanaporn S, Ngamjanyaporn P, Vilaiyuk S. Assessment of transition readiness in adolescents in Thailand with rheumatic diseases: a cross-sectional study. Pediatr Rheumatol Online J. 2021;19(1):101. doi:10.1186/s12969-021-00602-5
18. Hong HS, Im Y. Factors associated with healthcare transition readiness for adolescents with chronic conditions: a cross-sectional study. J Child Health Care Prof Work Child Hosp Community. 2025;29(3):658–672. doi:10.1177/13674935241248859
19. Bitencourt N, Bermas BL, Makris UE, Wright T, Reisch J, Solow EB. Time to first completed visit and health care utilization among young adults transferring from pediatric to adult rheumatologic care in a safety-net hospital. Arthritis Care Res. 2021;73(12):1730–1738. doi:10.1002/acr.24409
20. Miao Y, Li J, Wang J, et al. The experience of transition preparation for children and adolescents with mental disorders in China: a qualitative study. Front Psychol. 2025;16:1638296. doi:10.3389/fpsyg.2025.1638296
21. Qi Y, Xia L, Chen Y, et al. Self-management needs of adolescents with type 1 diabetes on transition to adult health care: a qualitative study. Eur J Pediatr. 2025;184(9). doi:10.1007/s00431-025-06373-5
22. Schwartz LA, Tuchman LK, Hobbie WL, Ginsberg JP. A social-ecological model of readiness for transition to adult-oriented care for adolescents and young adults with chronic health conditions. Child Care Health Dev. 2011;37(6):883–895. doi:10.1111/j.1365-2214.2011.01282.x
23. Smith AW, Gutierrez-Colina AM, Roemisch E, et al. Modifiable factors related to transition readiness in adolescents and young adults with epilepsy. Epilepsy Behav. 2021;115:107718. doi:10.1016/j.yebeh.2020.107718
24. Heitzer AM, Ris D, Raghubar K, Kahalley LS, Hilliard ME, Gragert M. Facilitating transitions to adulthood in pediatric brain tumor patients: the role of neuropsychology. Curr Oncol Rep. 2020;22(10):102. doi:10.1007/s11912-020-00963-2
25. Kim H, Sefcik JS, Bradway C. Characteristics of qualitative descriptive studies: a systematic review. Res Nurs Health. 2017;40(1):23–42. doi:10.1002/nur.21768
26. Doyle L, McCabe C, Keogh B, Brady A, McCann M. An overview of the qualitative descriptive design within nursing research. J Res Nurs JRN. 2020;25(5):443–455. doi:10.1177/1744987119880234
27. O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med J Assoc Am Med Coll. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388
28. Kerr C, Nixon A, Wild D. Assessing and demonstrating data saturation in qualitative inquiry supporting patient-reported outcomes research. Expert Rev Pharmacoecon Outcomes Res. 2010;10(3):269–281. doi:10.1586/erp.10.30
29. Aringer M, Costenbader K, Daikh D, et al. 2019 european league against rheumatism/American college of rheumatology classification criteria for systemic lupus erythematosus. Arthritis Rheumatol Hoboken NJ. 2019;71(9):1400–1412. doi:10.1002/art.40930
30. Schwartz LA, Brumley LD, Tuchman LK, et al. Stakeholder validation of a model of readiness for transition to adult care. JAMA Pediatr. 2013;167(10):939–946. doi:10.1001/jamapediatrics.2013.2223
31. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
32. Lincoln YS, Guba EG. But is it rigorous? Trustworthiness and authenticity in naturalistic evaluation. New Dir Program Eval. 1986;1986(30):73–84. doi:10.1002/ev.1427
33. Stewart KT, Chahal N, Kovacs AH, et al. Readiness for transition to adult health care for young adolescents with congenital heart disease. Pediatr Cardiol. 2017;38(4):778–786. doi:10.1007/s00246-017-1580-2
34. Cui C, Zhou H, Chen W, Li S, Zheng X. Behavioral dilemmas and support requirements of self-management for Chinese adolescents with epilepsy during transition readiness: a mixed-methods study. Patient Prefer Adherence. 2023;17:2605–2619. doi:10.2147/PPA.S429890
35. Yulan H, Ying C, Tian L, Jinrui C, Mengyue W, Genzhen Y. Advances in transition care for adolescents with chronic illnesses. J Nurs Sci. 2023;38(2):112–116. doi:10.3870/j.issn.1001-4152.2023.02.112
36. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci IS. 2011;6:42. doi:10.1186/1748-5908-6-42
37. Dushnicky MJ, Fine C, Cellucci T, et al. Mind the gap: a longitudinal analysis of the experiences of adolescents and parents in a rheumatology transition clinic. J Clin Rheumatol Pract Rep Rheum Musculoskelet Dis. 2023;29(5):235–239. doi:10.1097/RHU.0000000000001988
38. Saez C, Nassi L, Wright T, et al. Therapeutic recreation camps for youth with childhood-onset systemic lupus erythematosus: perceived psychosocial benefits. Pediatr Rheumatol Online J. 2022;20(1):39. doi:10.1186/s12969-022-00702-w
39. Lawson EF, Hersh AO, Applebaum MA, Yelin EH, Okumura MJ, von Scheven E. Self-management skills in adolescents with chronic rheumatic disease: a cross-sectional survey. Pediatr Rheumatol Online J. 2011;9(1):35. doi:10.1186/1546-0096-9-35
40. Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol. 2001;52:1–26. doi:10.1146/annurev.psych.52.1.1
41. Sun W, Reeve R, Ouellette T, et al. Novel tool to monitor adherence to oral oncolytics: a pilot study. JCO Clin Cancer Inform. 2021;5:701–708. doi:10.1200/CCI.20.00151
42. Kwok G, Levonyan-Radloff K, Masterson M, et al. A randomized feasibility trial of managing your health: a self-management and peer mentoring intervention for young adult survivors of childhood cancer. J Pediatr Psychol. 2025;50(8):798–810. doi:10.1093/jpepsy/jsaf004
43. Fortin PR, Neville C, Julien AS, et al. Measuring the impact of MyLupusGuide in Canada: results of a randomized controlled study. Arthritis Care Res. 2023;75(3):529–539. doi:10.1002/acr.24871
44. Otto C, Tárnok A, Erős A, et al. Planned transition of adolescent patients with inflammatory bowel disease results in higher remission rates. J Pediatr Nurs. 2019;45:62–66. doi:10.1016/j.pedn.2019.02.003
45. Fanouriakis A, Kostopoulou M, Andersen J, et al. EULAR recommendations for the management of systemic lupus erythematosus: 2023 update. Ann Rheum Dis. 2024;83(1):15–29. doi:10.1136/ard-2023-224762
46. V V, M M, C G, et al. A COSMIN systematic review of transition readiness assessment tools for adolescents with type 1 diabetes. Healthc Basel Switz. 2026;14(5). doi:10.3390/healthcare14050639
47. Zhang Z, Bai X, Hao L, Wang Y. Barriers to home-based medication self-management among older adults with multimorbidity: a qualitative study guided by empowerment theory. Patient Prefer Adherence. 2025;19:3985–3998. doi:10.2147/PPA.S569526
48. Rubinstein TB, Dionizovik-Dimanovski M, Davis AM, et al. Multicenter study of utility and acceptability of depression and anxiety screening in adolescents and young adults with childhood-onset systemic lupus. Arthritis Care Res. 2023;75(4):724–733. doi:10.1002/acr.24825
49. Wi D, Palermo TM, Stevens A, Ward TM. Sleep deficiency and symptoms of pain, fatigue, and depressed mood in youth with and without childhood systemic lupus erythematosus. J Clin Sleep Med JCSM off Publ Am Acad Sleep Med. 2024;20(10):1607–1614. doi:10.5664/jcsm.11210
50. Sadak KT, Gemeda MT, Grafelman M, et al. Identifying metrics of success for transitional care practices in childhood cancer survivorship: a qualitative interview study of survivors. BMC Cancer. 2020;20(1):898. doi:10.1186/s12885-020-07360-9
51. Kreuzer M, Drube J, Prüfe J, Schaefer F, Pape L. Members of the ERKNet Taskforce ‘QoL & Transition.’ Current management of transition of young people affected by rare renal conditions in the ERKNet. Eur J Hum Genet EJHG. 2019;27(12):1783–1790. doi:10.1038/s41431-019-0460-z
52. Hovde AM, McFarland CA, Garcia GM, et al. Multi-pronged approach to enhance education of children and adolescents with lupus, caregivers, and healthcare providers in new Jersey: needs assessment, evaluation, and development of educational materials. Lupus. 2021;30(1):86–95. doi:10.1177/0961203320969975
53. DeCoste C, Moaf P, Mohamed I, et al. Adolescent health care needs and relationship to disease in patients with childhood-onset systemic lupus erythematosus. Arthritis Care Res. 2024;76(6):841–849. doi:10.1002/acr.25297
54. Peng B, Hu N, Yu H, Xiao H, Luo J. Parenting style and adolescent mental health: the chain mediating effects of self-esteem and psychological inflexibility. Front Psychol. 2021;12:738170. doi:10.3389/fpsyg.2021.738170
55. Liu J, Liu J, Wang R, MSN N, Wu X, Chen J. Positive living with dialysis: the effect of a positive psychology intervention in patients receiving maintenance hemodialysis. Appl Psychol Health Well-Being. 2025;17(5):e70078. doi:10.1111/aphw.70078
56. Bitencourt N, Kramer J, Bermas BL, Solow EB, Wright T, Makris UE. Clinical team perspectives on the psychosocial aspects of transition to adult care for patients with childhood-onset systemic lupus erythematosus. Arthritis Care Res. 2021;73(1):39–47. doi:10.1002/acr.24463
57. Chen Y, Yi S, Chen R, Zhang Q. The efficacy of psychosocial interventions in relieving family caregiver burden in older adults with disabilities: a systematic review and network meta-analysis. Age Ageing. 2025;54(6):afaf155. doi:10.1093/ageing/afaf155
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Adolescent Patients’experiences of Mental Disorders Related to School Bullying
Chu ZJ, Yin X, Zhu GY, Yu SS, Li HY
Journal of Multidisciplinary Healthcare 2024, 17:2911-2919
Published Date: 19 June 2024
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025