")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Factors Influencing the Uptake of Voluntary Medical Male Circumcision Among Boda-Boda Riders Aged 18–49 Years in Hoima, Western Uganda
Authors Tusabe J, Muyinda H , Nangendo J, Kwesiga D, Nabikande S, Muhoozi M, Agwang W, Okello T , Rutebemberwa E
Received 22 July 2022
Accepted for publication 16 September 2022
Published 23 September 2022 Volume 2022:14 Pages 437—449
DOI https://doi.org/10.2147/HIV.S382219
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Joan Tusabe,1 Herbert Muyinda,2 Joanita Nangendo,3 Doris Kwesiga,4 Sherifah Nabikande,4 Michael Muhoozi,1 Winnie Agwang,4 Tom Okello,3 Elizeus Rutebemberwa4
1Department of Epidemiology and Biostatistics, School of Public Health, Makerere University, Kampala, Uganda; 2Child Health and Development Center, School of Medicine Makerere University, Kampala, Uganda; 3Clinical epidemiology Unit, School of Medicine, Makerere University, Kampala, Uganda; 4Department of Health Policy, Planning and Management, School of public health, Makerere University, Kampala, Uganda
Correspondence: Joan Tusabe, Email [email protected]
Introduction: We asseSssed factors influencing the uptake of voluntary medical male circumcision (VMMC) among boda-boda riders aged 18– 49 years in Hoima, western Uganda. Despite high levels of awareness about availability and benefits of VMMC, uptake was still low.
Methods: We employed the convergent parallel mixed methods design among boda-boda riders in Hoima district between August and September 2020. We administered a structured questionnaire to 316 boda-boda riders to determine factors associated with uptake of VMMC. We also conducted eight focus group discussions (FGDs) and six key informant interviews (KIIs) to explore perceptions of VMMC. To determine factors associated with VMMC, we conducted modified Poisson regression analysis at 5% level of significance. We identified sociocultural barriers and facilitators for VMMC using thematic content analysis.
Results: Uptake of VMMC was at 33.9% (95% CI 28.6– 39.1) and was associated with higher level of education, adjusted prevalence ratio (APR) 1.63, (95% CI 1.12– 2.40); concern about being away from work, APR 0.66 (95% CI 0.49– 0.88); and the belief that VMMC does not diminish sexual performance, APR 1.78 (95% CI 1.08– 2.9). Facilitators of uptake of VMMC were health education and awareness creation, improved penile hygiene, and perceived sexual functioning; and reduced chances of HIV and sexually transmitted infections (STIs). On the other hand, the barriers to uptake were fear of pain and compulsory HIV testing, healing duration, financial loss during the healing period, fear of sexual misbehavior after circumcision, interruption of God’s creation, and fear of loss of male fertility.
Conclusion: Although VMMC is largely perceived as protective against HIV and other STIs, deliberate measures using multiple strategies should be put in place to address the barriers to its uptake among this key population.
Keywords: voluntary medical male circumcision, men aged 18– 49 years, Western Uganda
Introduction
In Uganda, transport workers such as boda-boda riders (term commonly used to describe motorcycle and bicycle taxis) and long-distance truckers are known to be at risk of HIV acquisition and transmission.1 This is attributed to the transactional sex that occurs due to prolonged time away from partners and failure to use HIV-preventive measures.2,3 Conceptually, uptake of voluntary medical male circumcision (VMMC) among these key populations is vital in reducing the burden of HIV acquisition and transmission.4,5 However, research in Uganda indicates VMMC uptake levels ranging between 8.4% and 33.2%.1,6,7 Social demographic factors, concerns, and misconceptions about VMMC have been found to influence the uptake of VMMC.7–12 Further, research in other parts of East Africa among key populations of transport workers and fishermen found that men were reluctant to take up VMMC due to the physical demands of their jobs and relying on daily earnings.8,11
Hoima is one of the rapidly growing towns in Uganda because of the commercially viable oil resources and has observed a rapid increase in HIV incidence.13 With the increasing influx of individuals into the district, the boda-boda business has attracted a number of individuals as a lucrative business. Regardless of the age and education level, the business has attracted many; yet there are hardly any particular HIV-preventive measures targeting them as a key population. A survey conducted in Hoima in 2019 showed a relatively high prevalence of 7.0%,13 and the contribution of boda-boda riders to the HIV prevalence is known to be significant.1 In fact, evidence from Central and Western Uganda indicates prevalence of HIV among boda-boda riders to range between 7.5% and 9.9%.1,14 This is higher than the HIV district-specific (4.1%–6.1%) and national prevalence rates (5.7%) for surveys conducted between 2011 and 2020.1,14 This puts the entire population at a higher risk of acquiring HIV. Evidence from systematic review on VMMC in 10 of the 14 priority countries revealed the need for more research among sub-populations that were not adequately reached.15 Moreover, studies have shown that boda-boda riders involve themselves in high-risk behaviors such as having multiple sexual partners, non-use or low condom use with non-regular sexual partners, and alcohol and drug abuse.1,3 The risk is even higher among uncircumcised boda-boda riders since VMMC reduces the chances of acquiring HIV by 60%.1,4
Strategies for scaling up and increasing the uptake of VMMC in Uganda include: adoption of a VMMC policy, contextualization and implementation of VMMC among HIV/AIDS implementation bodies, VMMC media campaigns, social mobilization, and outreach services.16 In the rural setting, VMMC is conducted at both facility and community level through outreach services, mainly under the support and supervision of NGOs and other implementing partners. However, there is paucity of literature regarding the uptake of VMMC among boda-boda riders; yet this understanding is key in the development of population-specific interventions. This study therefore analyzed the factors influencing the uptake of VMMC among a key population of boda-boda riders aged 18–49 years in Hoima Municipality, Western Uganda.
Materials and Methods
Study Setting
This study was conducted between August and September 2020 among boda-boda riders aged 18–49 years in the municipality of Hoima district, Western Uganda. Within the district, the boda-boda business has attracted a number of individuals as a lucrative business. Currently, the district has over 1000 registered boda-boda riders,17 each transporting an average of 10–20 passengers a day. More importantly, anecdotal evidence indicates a sharp rise in new HIV cases from 1689 in 2012 to 3004 in 2017 in Hoima district, which saw the launch of an HIV/AIDS sensitization campaign in the district including VMMC.13 As an HIV-preventive measure, VMMC is carried out both at health facilities and at community level during outreaches supported by NGOs especially the Infectious Diseases Institute (IDI). However, by 2016, only 10,919 men were circumcised, achieving 50% of the district target.18
Study Design and Participants
We conducted a cross-sectional study employing a convergent parallel mixed methods study approach among boda-boda riders, women in the municipality, and KIs. This study adopted and modified the Andersen’s Behavioral model (Andersen, 1995) and the Health Behavioral (HB) model to study the factors influencing uptake of VMMC among boda-boda riders (Supplementary Figure 1).
Quantitative Data Collection Techniques
For the quantitative component, a boda-boda rider was eligible if he: 1) was aged 18–49 years, 2) worked within the municipality, 3) had been in the boda-boda business for at least six months, and 4) was willing to consent to join the study. An individual was excluded if they had participated in the qualitative study and was unable to speak Runyoro.
We estimated the sample size of 316 boda-boda riders using both the Leslie Kish and finite population formulae. This was done under the following assumptions: 39.2%1 uptake of VMMC among boda-boda riders, a 5% level of precision and 95% confidence intervals, and a finite population of 1260 boda-boda riders.17 We employed multilevel sampling technique to obtain the study participants. For purposes of representation, about half of the boda-boda stages from each division were selected using computer-generated random numbers. From each selected stage, simple random sampling using a ballot box was employed to obtain five or six study participants.
Quantitative Data Collection Procedure
We collected quantitative data to determine factors associated with the uptake of VMMC among boda-boda riders. Data were collected using a structured questionnaire (Supplementary Figure 2) administered in face-to-face interviews. The study team included the first author, boda-boda stage chairpersons (these register boda-boda riders and manage the rider activities), and four research assistants (RAs) who were experienced in community work and had at least degree-level training in nursing. Prior to the start of data collection, RAs were trained for three days on all study procedures to clarify their responsibilities and pre-test the study questionnaire. The boda-boda stage chairpersons helped in identifying the registered boda-boda riders at their respective stages from which a sampling frame was created. The RAs individually administered the questionnaires to each recruited participant. At the end of each day, all collected data were reviewed for accuracy and completeness.
Quantitative Data Management and Analysis
In our quantitative analysis, we summarized continuous variables using mean and standard deviation, and used percentages for the categorical variables. We defined the outcome (uptake of VMMC) as getting circumcised under the VMMC program by a trained medical worker,6,19 which we measured on a binary scale as a proportion. Information on perceptions on VMMC, fears associated with VMMC, and misconceptions about VMMC were assessed using a Likert scale and later collapsed into binary responses. We used modified Poisson regression analysis to assess for factors associated with uptake of VMMC and measured associations as prevalence ratios (PR) and their 95% CI. At bivariate analysis, we considered variables with P <0.20 as significant for multivariate analysis. We also added to the multivariable model variables reported as confounders in literature even if they were not significant at bivariate analysis. Modified Poisson regression model was used because data were cross-sectional and PR are more conservative in magnitude than prevalence odds ratios (POR) for a relatively common outcome, ie, >10%.20,21 We checked for correlation and multi-collinearity by conducting a correlation coefficient matrix and a variance inflation factor (VIF) test. We conducted likelihood ratio tests to identify the best fitting model. Adjusted prevalence ratios with P-value <0.05 were considered statistically significant. We presented the findings using strengthening the reporting of observational studies in epidemiology (STROBE) guidelines for reporting cross-sectional studies (Supplementary Figure 3).
Qualitative Data Collection Techniques
Selection for FGDs and KIs
For the qualitative component, a boda-boda rider was eligible if he: 1) was aged 18–49 years, 2) worked within the municipality, 3) had been in the boda-boda business for at least six months, and 4) was willing to consent and talk about VMMC. Exclusion criteria were inability to speak Runyoro or English. We also conducted FGDs among women and KIIs for triangulation of the qualitative data. A woman was eligible if she was: 1) aged 18–49 years, 2) engaged in any form of work within the municipality, 3) willing to consent, and 4) willing to talk about VMMC. The exclusion criterion was inability to speak Runyoro or English. A key informant (KI) was eligible if he/she: 1) did VMMC-related work, 2) had worked at their respective offices for at least six months, 3) was willing to consent, and 4) was willing to talk about VMMC. A KI was excluded if he/she did not speak either Runyoro or English.
We selected two boda-boda riders per stage to take part in the FGDs with the help of the Hoima district boda-boda riders association (HDBRA) chairperson and the respective boda-boda stage chairperson. Boda–boda riders were selected from stages in Kahora division, where the majority of the stages are. For the FGDs among women, we identified one woman from Hoima central market who served as our mobilizer with the help of the HDBRA chairperson. Selection of FGD participants was done purposively using the homogeneous sampling strategy. The required minimum number of FGDs was set depending on saturation of data. This was determined when there was no new information emerging from subsequent data collection and after attaining maximum variation by age, education, and marital status.22 We conducted a total of eight FGDs, six among men and two among women. We then identified KIs and conducted interviews at their respective offices. KIs were selected based on their cultural, religious, or technical role in uptake of VMMC. Six KIs were identified and purposively selected using the “maximum variation” strategy. This ensured maximization of the diversity dynamics surrounding VMMC uptake through recruitment of a range of personalities in different settings.
Qualitative Data Collection Procedure
The data were collected by two RAs, who were nurses with experience in qualitative data collection. The RAs were trained for two days on the current study and qualitative study procedures by the PI. During the discussions, one acted as a moderator and the other a note taker. We conducted the FGDs at the HDBRA offices where participants gathered. Each FGD had 8–9 members; the discussions were held in Runyoro and lasted one hour on average. The discussions were guided by a trained moderator fluent in both English and Runyoro using a pre-tested FGD guide (Supplementary Figure 4). Details of the FGDs including body language were captured by a note taker and were later used to enrich the coding at analysis.
In addition, six KI interviews were conducted for triangulation. These included a Catholic Church priest, an Anglican Church reverend, the “Katikiro” (cultural leader) of Bunyoro kingdom, a Muslim circumciser, and the two VMMC coordinators. All KIIs lasted 30–45 minutes and were conducted in English except one interview which was conducted in Runyoro using a pre-tested KII guide (Supplementary Figure 5) and later translated to English. These interviews obtained perceptions of VMMC from a religious, cultural, or medical point of view. With permission from the participants, all the qualitative conversations were recorded using a digital audio recorder for subsequent analysis.
Qualitative Data Management and Analyses
All audio recordings were transcribed verbatim by two independent RAs skilled in qualitative research and translated to English for analysis by the first author. Before analysis, the first author reviewed the translated transcripts to assess accuracy and completeness. The first and fourth author then read through the transcripts to familiarize themselves with the data and then imported it to Atlas ti version 6.0 software for analysis. Where inconsistences existed during analysis, consensus was reached in meetings with all the other research team members. Thematic content analysis following prior themes from similar studies was applied.9,10,12,23–25 We presented the findings following standards for reporting qualitative research (SRQR) guidelines for reporting qualitative research (Supplementary Figure 6).
Results
In our survey, we included a total 316 participants; the participants’ mean age was 30.5 (STD 7.2 years), with 161 (50.9%) aged 25–34 years. The majority (235; 74.4%) were married. A total of 147 (46.5%) had attained primary education. Most boda-boda riders (232; 73.4%) were engaged in other income-generating activities. Of those, more than half (132; 56.9%) were engaged in farming, followed by 54 (23.3%) who were engaged in sales and services (Table 1).
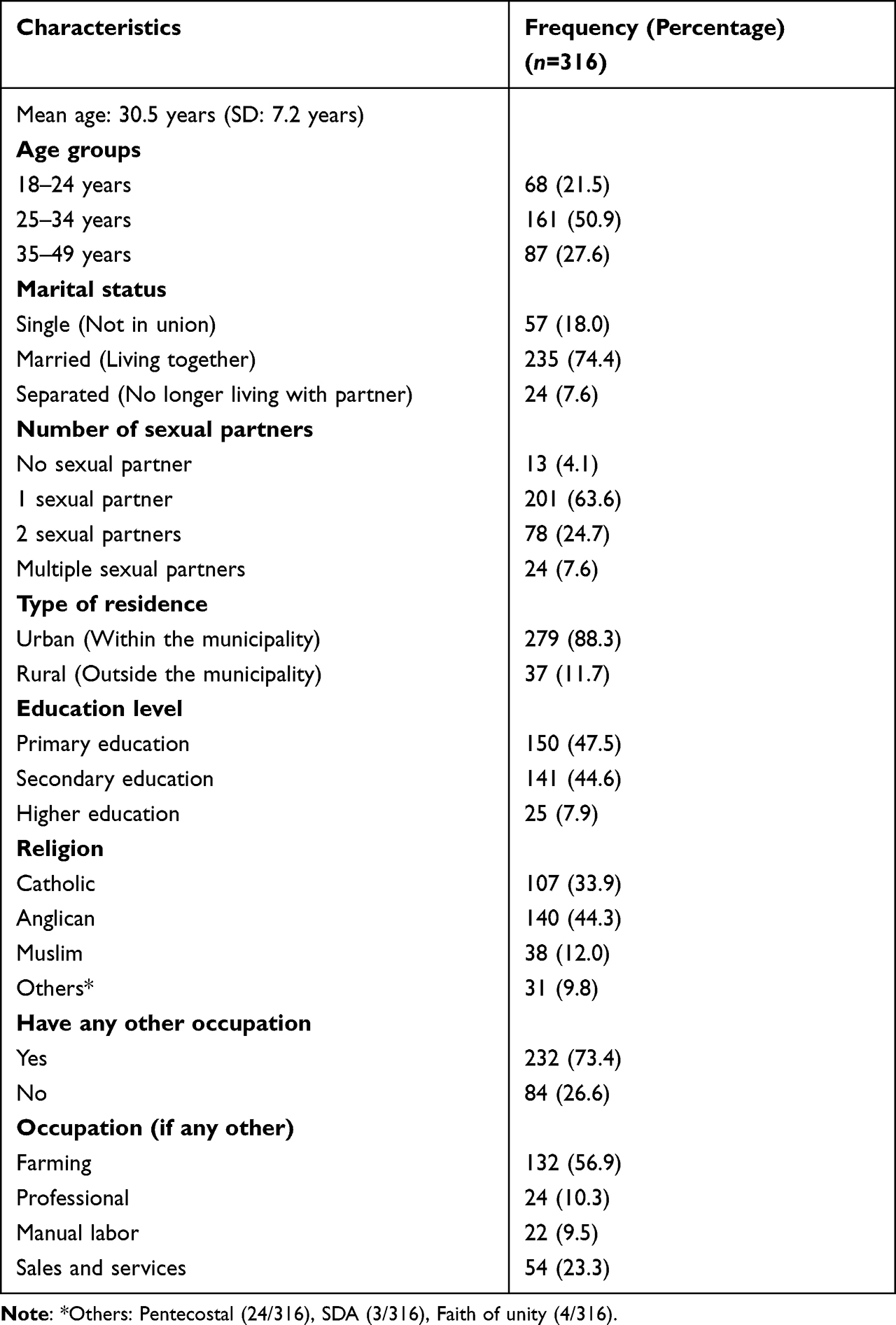 |
Table 1 Social Demographic Characteristics of the Boda-Boda Riders |
For the qualitative study, a total of eight FGDs were conducted, six of the FGDs among boda-boda riders and two among women who ran different businesses in the municipality. In addition, we conducted six KIIs: two with VMMC providers, two with religious leaders, one with a Muslim circumciser, and one with a cultural leader. The results are summarized under three themes of local understanding of circumcision, facilitators for VMMC, and barriers for VMMC.
Factors Associated with Uptake of VMMC Among Boda-Boda Riders
Thirty-four percent (107/316) of the participants reported having taken up VMMC. The other forms of circumcision taken up were religious and traditional circumcision taken up by 75 (23.7%) and 5 (1.6%) participants, respectively (Table 2).
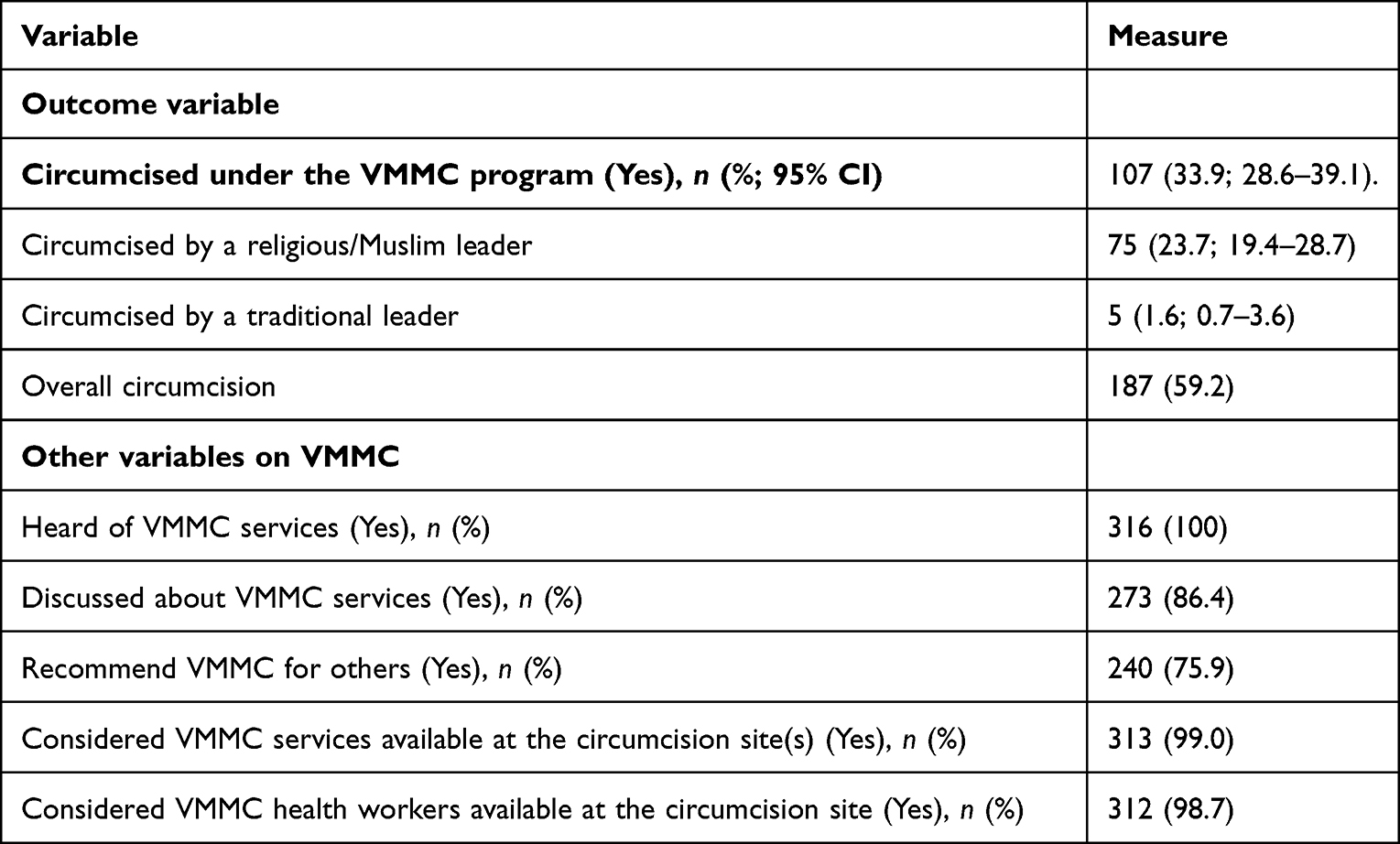 |
Table 2 Uptake of VMMC Among Boda-Boda Riders (N=316) |
Boda-boda men were more likely to take up VMMC if they had attained secondary and higher education (APR 1.36; 95% CI 1.01–1.84 and APR 1.63; 95% CI 1.12–2.40) and if they did not believe that circumcision reduces a man’s sexual performance (APR 1.78; 95% CI 1.08–2.90). On the other hand, boda-boda men were less likely to take up VMMC if they were concerned about being away from work for long (APR 0.66; 95% CI 0.49–0.88) (Table 3).
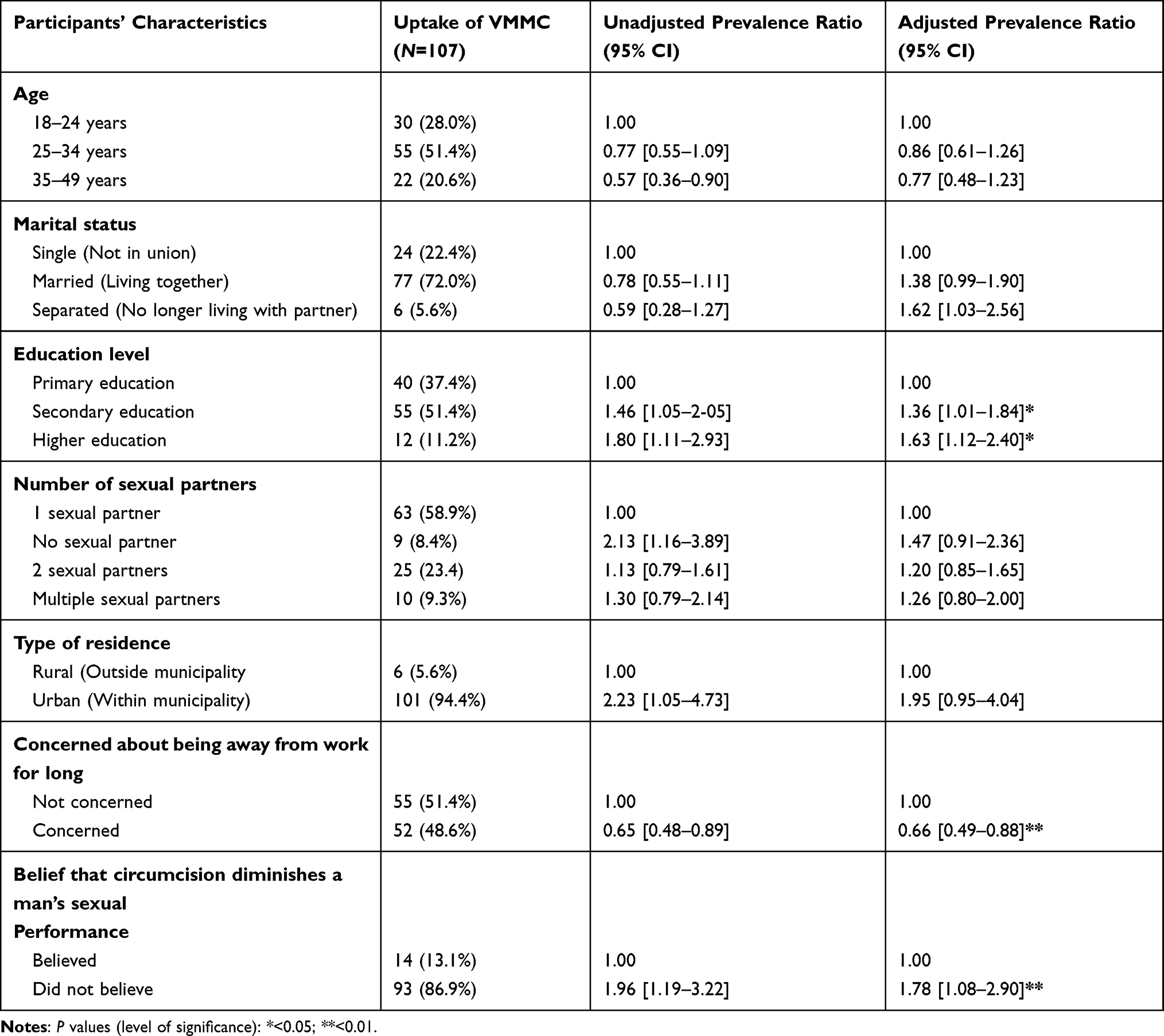 |
Table 3 Factors Associated with the Uptake of VMMC Among Boda-Boda Riders |
The Meaning of Circumcision Among Boda-Boda Riders
While circumcision was generally understood as the removal of the foreskin, one of the local phrases used to describe circumcision was “kusiramura”, literally meaning conversion to Islamic religion, which most of those in the Christian denominations were against. A related local term was “kusara”, literally meaning cutting of the foreskin, which was described as a painful process. Some people did not want to take up circumcision because they associated it with being Muslim. At the same time, a few pointed out that things had changed and circumcision was generally acceptable in all religious denominations.
In an FGD among married men, it was mentioned that:
… People used to know that getting circumcised is becoming a Muslim. But now since the ministry of health came in to educate the masses that is why now non-Muslim people associate with circumcision … (FGD, Men above 25 years FGD)
“Kutyekera” (sharpening) was another local term used to mean circumcision and was commonly used by married women. These would burst into laughter each time the term was mentioned. When probed further, one of the female participants related a circumcised penis to a sharp knife saying that the way a sharp knife cuts effectively, a circumcised penis is more enjoyable during sexual intercourse.
… It means becoming sharp, there is a difference for a circumcised man, the one who has been sharpened, he is more enjoyable during sexual intercourse. (FGD, Married women)
Circumcised men expressed personal experiences with sexual activity before and after circumcision. They discussed that circumcised men have more sexual feelings, enjoy sex more, and take longer to have orgasms (considered desirable in this context). They also expressed how circumcision improved their sexual prowess and confidence in convincing female sexual partners. Similarly, the survey component revealed that more than half (180; 57.0%) and the majority (256; 81.0%) of the respondents believed that circumcised men have more sexual feelings and enjoy sex more, respectively, than their counterparts (Table 4).
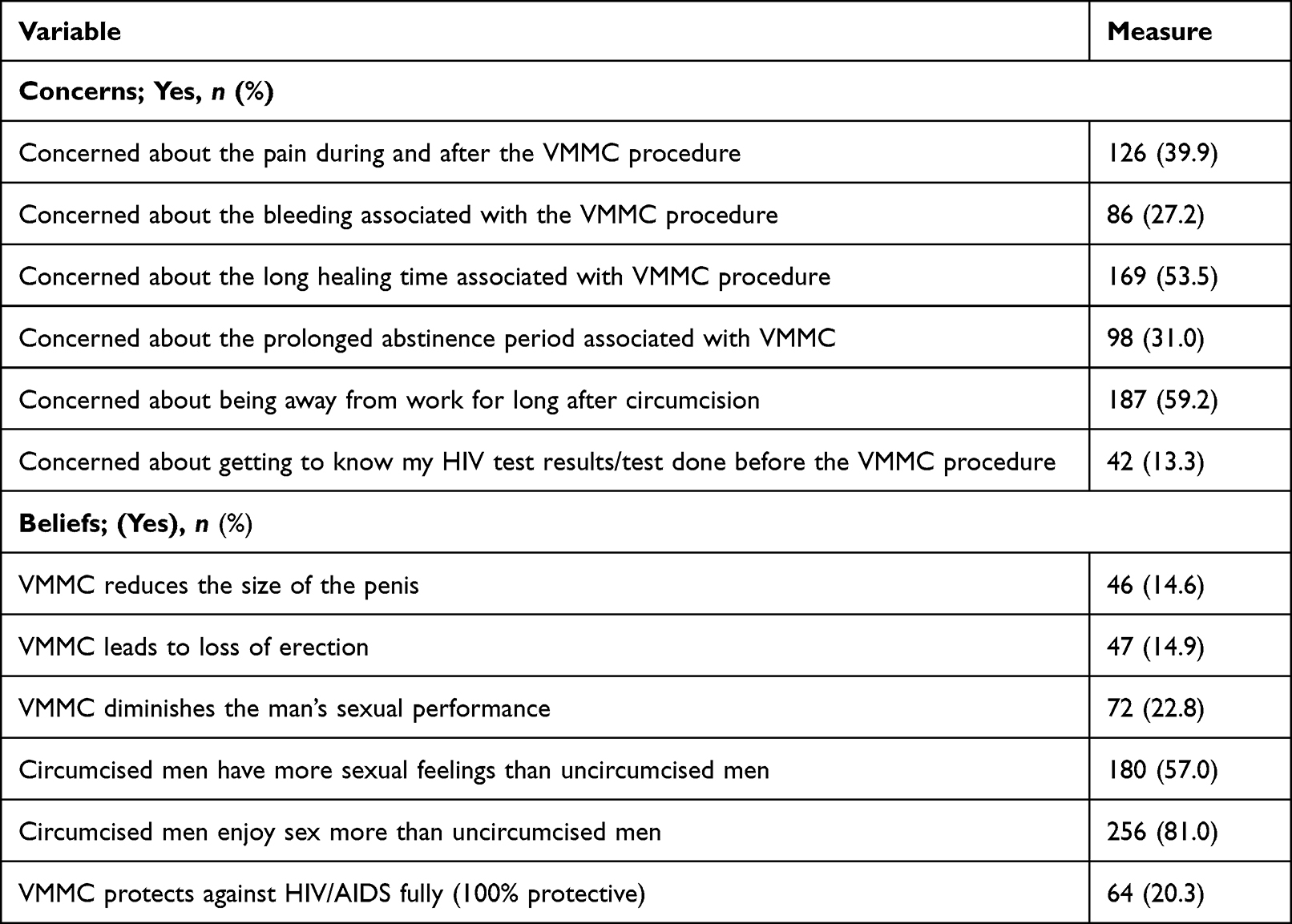 |
Table 4 Concerns and Misconceptions About VMMC |
Facilitators of VMMC Among Boda-Boda Riders Aged 18–49 Years in Hoima Municipality
A major factor that influenced uptake of VMMC was health education that increased levels of awareness about the importance of VMMC. Our survey showed that 316 (100%) study participants had heard about VMMC services and the majority (273; 86.4%) of whom had talked about these services among themselves (Table 2). Participants appreciated the efforts made by VMMC implementing partners in disseminating education on VMMC. This was done mainly through the media, facilities, and using mobile public address sound systems. From the professional health provider’s point of view, there was evidence that these activities were being done. A KI was quoted saying:
… We also have outreach activities, where we move the team and the entire theater to a nearby location where these boda-boda riders are or where the biggest number of clients are, station there and provide the service close to the people. (KI, VMMC Regional coordinator)
Thus, information sharing and bringing VMMC services closer to people through outreaches encouraged uptake.
Participants mentioned maintaining personal hygiene as one of the main reasons that encouraged men to go for circumcision. The perceived maintenance of personal hygiene was attributed to removal of the foreskin, which left no room for hiding dirt and made it easy to clean a circumcised penis. In one FGD, it was mentioned that,
… The first thing is personal hygiene even before we go far, a circumcised person is hygienic, you cannot compare him with one who is not circumcised. Even if, he doesn’t take a bath, he has no problem. (FGD, Men with Secondary level education)
Furthermore, participants described circumcision as a mechanism that reduces the risk of acquiring HIV and other sexually transmitted infections (STIs). In the survey, 64 (20.3%) participants erroneously believed that circumcision fully (100%) protects against acquisition of HIV/AIDS (Table 4). Participants attributed the reduction in risk to lower instances of bruising a circumcised penis during sexual intercourse. A circumcised penis develops a thicker inner skin which reduces the microscopic cuts that develop during intercourse, consequently reducing chances of acquiring HIV/AIDS and other STIs. However, study participants were not certain of what percentage of reduction VMMC offers. They often mentioned varying figures of 50%–99%, and others had no idea at all.
In one of the FGDs, it was stated that:
… When you are circumcised … you still have the chances of getting HIV only that out of 100, you might have protection of 99% … (FGD, Men less than 25 years FGD)
Barriers to VMMC Among Boda-Boda Riders Aged 18–49 Years in Hoima Municipality
Participants in all FGDs discussed fear of pain during and after circumcision. From the survey, 126 (39.9%) participants were concerned about pain during and after the VMMC procedure (Table 4). Pain was feared after the surgical procedure when anesthesia has worn off and during wound healing. One of the participants confessed running away from a circumcision site without being circumcised due to fear of pain.
… The truth is I was number two in the line for circumcision, … but as I was hearing, when they circumcised the first person and he shouted in pain, I said eh, it seems these people are causing a lot of pain, I decided go back because of fear. (FGD, Men above 25 years)
Also discussed was fear of the mandatory HIV testing done before VMMC. Findings from the survey showed that 42 (13.3%) participants reported concern about the mandatory HIV testing. In all the two female FGDs, participants pointed out that men are poor at seeking health services and always fear to find out their HIV/AIDS status which discourages them from seeking circumcision services. However, there was a mixture of perceptions on this among men. Some men felt it would be embarrassing to test HIV-positive and then be denied the service, while others considered this as an opportunity to know their HIV status. It was mentioned that:
Most men do not want to know their HIV statuses, when they reach circumcision centers and they are told about the need for HIV testing, they just decide to go away without being circumcised. (FGD, Single women)
Long healing time which reduces one’s ability to smoothly resume work was cited as barrier to circumcision. More than half (169; 53.5% and 187; 59.2%) of the participants were concerned about the long healing time associated with VMMC and being away from work for long, respectively. Participants discussed financial constraints during the wound healing time. Income from boda-boda business is based on daily earnings and being employed by other people, and being away from work for more than a week can cause significant financial constraints to the circumcised man. In some scenarios, participants revealed how they bought their motorcycles on loan and therefore would not afford to miss paying back the loan because of the missed income due to the wound healing process. It was also reported that some men would be forced to return to work before they fully healed due to financial constraints, which actually prolongs the healing period. To such a category of people, monetary or food subsidy would be necessary after circumcision to allow them enough time for full recovery. Also related to the healing time was long abstinence period. It was reported that the majority of the married men were unlikely to wait for complete healing before resuming sexual intercourse, which impacted on the healing process.
In one of the FGDs it was suggested that:
… may be if you can come out and say when we circumcise you, government will give us like 10 kg of posho, so that one can first rest and heal completely. (FGD, Men above 25 years)
In some instances, circumcision was perceived as an interruption of God’s creation as a whole. There was a different view that there is a reason as to why God left the foreskin on the penis and may not be a good idea to disrupt God’s plan by removing it.
… A person is created whole. So if I am created in the image and likeness of God and he has wished for me to be as I am … why should I make myself lame, if it is not really a health issue and surely it is not giving danger to my life then I shouldn’t cut it. (KI, Catholic priest)
The prophetic understanding is that circumcised men will be asked where they put the foreskin after reaching heaven. In a different way, one of the religious leaders explained that the Catholic Church neither discourages nor encourages circumcision, but gives basic information and leaves individuals to make personal choices.
Another barrier was the belief that VMMC may lead to loss of male fertility especially when performed by inexperienced personnel. The belief was that the anesthesia given before conducting circumcision causes loss of male fertility. The understanding was that a man circumcised from the hospital would produce fewer children due to the anesthesia injection.
… In the hospital, they first give an injection which makes some of them end up lose their male fertility if someone intended to have like five or six children, he can find himself producing only three or two. (FGD, Married men)
Additionally, the VMMC provider explained that VMMC is perceived as a form of family planning method through making men impotent.
The KI was quoted saying:
… others think it is a family planning method, we just hide it … we are circumcising them so that we reduce the number of children they can produce. (KI, VMMC Regional coordinator)
VMMC was thought to be conducted by inexperienced health workers, trainees, and women whose work participants did not trust. They trusted Muslim circumcisers who they said have experience because they have been conducting circumcision for long. The understanding was that this is a new concept among the health workers who tend to lack the experience the Muslim circumcisers have. More so, in situations where VMMC is performed by female health workers, especially the older men shy away.
The problem is coming to circumcise me when you are female, yet even in labour wards of women it is midwives that work there, so this must be left for men. (FGD Men with Primary level education)
This is linked to the mistaken view that maternal and child health services are offered by female health workers, therefore VMMC should be left for male health workers.
Discussion
Factors influencing the uptake of VMMC included both biomedical and social cultural factors. Uptake of VMMC was at 33.9%, comparable to a study conducted in similar contexts among boda-boda riders.1 This is below national target of 80% set to be achieved by 2020.26 Six years later, with the current communication and sensitization about VMMC, one would expect the uptake of VMMC among boda-boda riders to have increased. However, this is not the case and can be attributed to the fact that knowledge alone is not sufficient for demand creation of VMMC services.11,27 More so, there are no particular interventions targeting boda-boda riders, even when the VMMC policy advocates for equitable access for all.16 Ensuring provision of a comprehensive package of the VMMC information coupled with other strategies targeting population-specific social and behavioral aspects is vital for the success of the program.28,29
VMMC was associated with higher level of education, concern about being away from work, and not believing that VMMC diminishes sexual performance. Facilitating factors included awareness creation about VMMC, reduced risk of infection, improved penile hygiene, and perceived improvement in sexual performance. On the other hand, barriers were fear of pain and compulsory HIV testing, long healing time, financial constraints, perceived interruption of God’s plan, loss of male fertility, and the non-experienced and female health workers.
Our findings show that the widespread health education can facilitate uptake of VMMC. Another factor was level of formal education. Secondary and higher education were significantly associated with uptake of VMMC, similar to findings elsewhere in Africa.7,30,31 It is therefore imperative to implement VMMC interventions targeting out-of-school youths with higher levels of school drop-outs such as boda-boda riders.
The findings further show that improved knowledge of the importance for personal hygiene and protection from HIV and other STIs were facilitators for VMMC. Other studies have shown comparable levels of knowledge of health benefits of VMMC between the general population and a key population of boda-boda riders.24,32 However, we found varied incorrect information regarding VMMC. One of the commonest misconceptions was that VMMC reduces chances of HIV acquisition among women. This is against the scientific evidence and can be misleading,33 resulting in higher unfulfilled expectations which might eventually discourage future uptake of VMMC among boda-boda riders and the general population. More health education interventions aimed at addressing these knowledge gaps and misconceptions about VMMC are imperative.
The fear of pain was emphasized in our findings as one of the barriers to VMMC mainly among older men. However, fear of pain was not significantly associated with uptake of VMMC. Similar studies found that individuals were scared of pain due to injections when giving anesthesia and the pain of the wound during and after the circumcision procedure.10,23 The use of analgesics during and after circumcision was reported as a relief to pain and encouraged men to take up the VMMC services,34 but it was perceived to be a cause of male infertility. In order to increase uptake of VMMC, it is important to package the VMMC message properly to inform boda-boda riders about the pain during and after the procedure and how it can be managed.
Fear of undergoing mandatory HIV testing before circumcision was another barrier, as has been documented in other studies conducted in Africa.23,35 This was linked with the failure to circumcise those found HIV-positive, which was deemed stigmatizing and made individuals shy away in fear of being tested HIV-positive and denied the service.
Economic factors, particularly disruption of livelihoods, were among the barriers. This is worse among boda-boda riders where the majority rely on daily earnings to support themselves, their families, and perhaps pay their bosses or loans. Moreover, boda-boda riding is an exhausting job that requires a lot of energy, with higher chances of causing injury to the wound; hence there is a need for a longer healing time. Circumcised boda-boda riders faced financial constraints during the healing time. In fact, boda-boda riders who were concerned about being away from work for long were less likely to take up VMMC. Similar observations were made elsewhere.8,11,36 Therefore, offering financial support to such a population after circumcision may be of great importance to the VMMC programming.
Religious beliefs also contributed to the barriers. George et al and Chiringa et al also asserted that circumcision is sinful and no one has the authority to change what God has created.9,23 Engaging religious institutions therefore when passing on information about VMMC is crucial to improve the uptake.
With the improved awareness and sensitization about VMMC, expectations would increase and the uptake of VMMC would potentially increase among boda-boda riders. However, it has been documented that knowledge alone is not sufficient for demand creation of VMMC services.11,27 It was noted that there were no particular interventions targeting boda-boda riders, even when the VMMC policy advocates for equitable access for all.16 Ensuring provision of a comprehensive package of the VMMC information coupled with other strategies targeting population-specific health information needs is vital for the success of the intervention. Using static and mobile services as well as population-specific interventions led to an increase in uptake in both urban and rural areas.28,29,37 Multiple interventions such as the provision of financial support, continuous education and sensitization, and targeted counseling may be warranted to improve uptake of VMMC in this key population. In fact, a systematic review conducted in demand creation interventions recommended financial incentives and education programs.38
Study Limitations
The main limitation of this study is the fact that the circumcision status of the boda-boda riders was not medically/physically confirmed but the study entirely depended on the respondents’ report. This could have been subject to social desirability bias. However, interviews were conducted maintaining utmost confidentiality and in a conducive environment for participants to provide an honest view.
Conclusion
Understanding of the availability and health benefits of VMMC was largely adequate; however, uptake of VMMC was generally low at 33.9%. This can be explained by the diffuse perceptions regarding VMMC. Although there were high levels of awareness about availability and benefits of VMMC, there were considerable concerns and beliefs that discouraged boda-boda riders from taking up VMMC. While formal education is an important ingredient in the uptake of VMMC, it is important to have interventions that target those outside the formal education sector with characteristics similar to those of boda-boda riders in Hoima.
Data Sharing Statement
All data supporting the results and conclusions of this manuscript are fully available without restriction and are included within the manuscript and its supporting information files.
Ethics Approval and Consent to Participate
We obtained ethical approval to conduct the study from the Higher Degree Research and Ethics Committee at Makerere University School of Public Health and a student waiver from Uganda National Council of Science and Technology (UNCST). We also obtained administrative permission to conduct the study from HDBRA. We obtained written informed consent from all study participants (who either provided a signature or a thumbprint after receiving explanation of the purpose of the study), including publication of anonymized responses and the participants’ rights. All boda-boda riders were left with a copy of the written informed consent form. All signed or thumb-printed consent forms, audio recordings, and filled tools were stored securely in a locked file cabinet, with access limited to only authorized personnel on the study team. All procedures in this study were applied in accordance with the standards and regulations of the Declaration of Helsinki.
Acknowledgment
The authors would like to thank the management of Hoima district boda-boda riders' association for their support and collaboration. We would also like to thank the research assistants, namely John Vianney Alinda, Albert Muhumuza, and Edward Mbabazi, and study participants for their efforts during the data collection exercise.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Research reported in this publication was supported by the Fogarty International Center, National Institute of Alcohol Abuse and Alcoholism, National Institute of Mental Health, of the National Institutes of Health under Award Number D43 TW011304. The content is solely the responsibility of the authors and does not necessarily represent the official views of the “National Institutes of Health”.
Disclosure
The authors declare that they have no competing interests.
References
1. Lindan CP, Anglemyer A, Hladik W, et al. High-risk motorcycle taxi drivers in the HIV/AIDS era: a respondent-driven sampling survey in Kampala, Uganda. Int J STD AIDS. 2015;26(5):336–345. doi:10.1177/0956462414538006
2. Morris CN, Morris SR, Ferguson AG. Sexual behavior of female sex workers and access to condoms in Kenya and Uganda on the Trans-Africa highway. AIDS Behav. 2009;13(5):860–865. doi:10.1007/s10461-008-9431-z
3. Delany-Moretlwe S, Bello B, Kinross P, et al. HIV prevalence and risk in long-distance truck drivers in South Africa: a national cross-sectional survey. Int J STD AIDS. 2014;25(6):428–438. doi:10.1177/0956462413512803
4. Auvert B, Taljaard D, Lagarde E, Sobngwi-Tambekou J, Sitta R, Puren A. Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: the ANRS 1265 trial. PLoS Med. 2005;2(11):e298. doi:10.1371/journal.pmed.0020298
5. Bailey RC, Moses S, Parker CB, et al. Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. Lancet. 2007;369(9562):643–656. doi:10.1016/S0140-6736(07)60312-2
6. Lubogo M, Anguzu R, Wanzira H, et al. Utilization of safe male circumcision among adult men in a fishing community in rural Uganda. Afr Health Sci. 2019;19(3):2645–2653. doi:10.4314/ahs.v19i3.40
7. Nanteza BM, Serwadda D, Kankaka EN, Mongo GB, Gray R, Makumbi FE. Knowledge on voluntary medical male circumcision in a low uptake setting in northern Uganda. BMC Public Health. 2018;18(1):1278. doi:10.1186/s12889-018-6158-2
8. Evens E, Lanham M, Hart C, Loolpapit M, Oguma I, Obiero W. Identifying and addressing barriers to uptake of voluntary medical male circumcision in Nyanza, Kenya among men 18–35: a qualitative study. PLoS One. 2014;9(6):e98221. doi:10.1371/journal.pone.0098221
9. Chiringa IO, Ramathuba DU, Mashau NS. Factors contributing to the low uptake of medical male circumcision in Mutare Rural District, Zimbabwe. Afr J Prim Health Care Fam Med. 2016;8(2). doi:10.4102/phcfm.v8i2.966
10. Tapera R, Kebofe T, Tumoyagae T, January J. Factors associated with uptake of voluntary medical male circumcision among University of Botswana undergraduate male students. Int J Health Promot Educ. 2017;55(5–6):333–342. doi:10.1080/14635240.2017.1394796
11. Nevin PE, Pfeiffer J, Kibira SP, Lubinga SJ, Mukose A, Babigumira JB. Perceptions of HIV and safe male circumcision in high HIV prevalence fishing communities on Lake Victoria, Uganda. PLoS One. 2015;10(12):e0145543. doi:10.1371/journal.pone.0145543
12. Ahinkorah BO, Hagan JE Jr, Seidu -A-A, Torgbenu E, Budu E, Schack T. Understanding the linkages between male circumcision and multiple sexual partnership among married Ghanaian men: analysis of data from the 2014 Ghana demographic and health survey. SSM-Popul Health. 2020;11:100622. doi:10.1016/j.ssmph.2020.100622
13. Mugerwa F. Uganda: CNOOC launches HIV/AIDS sensitisation campaign in oil-rich areas; increase in incidence attributed to labour-related emigration. Daily Monit Uganda. 2019;16:1.
14. Tumwebaze M, Otiam EO, Rukindo KM, Mwesigwa J. Prevalence and predisposing factors of human immunodeficiency virus infection among the boda-boda riders in Mbarara municipality-Uganda. Open J Epidemiol. 2020;10(03):235. doi:10.4236/ojepi.2020.103021
15. Carrasco MA, Wilkinson J, Kasdan B, Fleming P. Systematic review of barriers and facilitators to voluntary medical male circumcision in priority countries and programmatic implications for service uptake. Glob Public Health. 2019;14(1):91–111. doi:10.1080/17441692.2018.1465108
16. Minisrty of Health. Safe Male Circumcision Policy. Kampala: Government of Uganda; 2010:14.
17. Mani S. Registered Number of Boda Boda Rider Cyclists in Hoima District. Hoima: Hoima district boda-boda rides association; 2019.
18. Francis WL, Tumuramye J, Muganzi A. Voluntary Medical Male Circumcision Program Data for Hoima District. Hoima: Infectious diseases institute; 2020.
19. UNAIDS. Voluntary medical male circumcision report - 4.1 million performed in 2018; 2019. Available from: https://www.unaids.org/en/resources/presscentre/featurestories/2019/october/20191021.vmmc.
20. Bastos LS, Oliveira RDVCD, Velasque LDS. Obtaining adjusted prevalence ratios from logistic regression models in cross-sectional studies. Cad Saude Publica. 2015;31:487–495. doi:10.1590/0102-311x00175413
21. Behrens T, Taeger D, Wellmann J, Keil U. Different methods to calculate effect estimates in cross-sectional studies. Methods Inf Med. 2004;43(05):505–509. doi:10.1055/s-0038-1633907
22. Corbin J, Strauss A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. Sage publications; 2014.
23. George G, Strauss M, Chirawu P, et al. Barriers and facilitators to the uptake of voluntary medical male circumcision (VMMC) among adolescent boys in KwaZulu–Natal, South Africa. Afr J AIDS Res. 2014;13(2):179–187. doi:10.2989/16085906.2014.943253
24. Kibira SP, Daniel M, Atuyambe LM, Makumbi FE, Sandøy IF. Exploring drivers for safe male circumcision: experiences with health education and understanding of partial HIV protection among newly circumcised men in Wakiso, Uganda. PLoS One. 2017;12(3):e0175228. doi:10.1371/journal.pone.0175228
25. Tian Y, Liu W, Wang J-Z, Wazir R, Yue X, Wang K-J. Effects of circumcision on male sexual functions: a systematic review and meta-analysis. Asian J Androl. 2013;15(5):662. doi:10.1038/aja.2013.47
26. Cork MA, Wilson KF, Perkins S, et al. Mapping male circumcision for HIV prevention efforts in sub-Saharan Africa. BMC Med. 2020;18(1):189. doi:10.1186/s12916-020-01635-5
27. Kong X, Ssekasanvu J, Kigozi G, et al. Male circumcision coverage, knowledge, and attitudes after 4-years of program scale-up in Rakai, Uganda. AIDS Behav. 2014;18(5):880–884. doi:10.1007/s10461-014-0740-0
28. Grund JM, Chetty-Makkan CM, Ginindza S, et al. Effectiveness of an ”exclusive intervention strategy” to increase medical male circumcision uptake among men aged 25–49 years in South Africa. BMC Public Health. 2018;18(1):868. doi:10.1186/s12889-018-5729-6
29. Kaufman ZA, DeCelles J, Bhauti K, et al. A sport-based intervention to increase uptake of voluntary medical male circumcision among adolescent male students: results from the MCUTS 2 cluster-randomized trial in Bulawayo, Zimbabwe. J Acquir Immune Defic Syndr. 2016;72(Suppl 4):S292–298. doi:10.1097/QAI.0000000000001046
30. Mangombe K, Kalule-Sabiti I. Knowledge about male circumcision and perception of risk for HIV among youth in Harare, Zimbabwe. South Afr J HIV Med. 2019;20(1):1–9. doi:10.4102/sajhivmed.v20i1.855
31. Spees LP, Ledikwe JH, Kleinman NJ, et al. Immediate motivators to seeking voluntary medical male circumcision among HIV-negative adult men in an urban setting in Botswana. AIDS Educ Prev. 2019;31(2):136–151. doi:10.1521/aeap.2019.31.2.136
32. Ssekubugu R, Leontsini E, Wawer MJ, et al. Contextual barriers and motivators to adult male medical circumcision in Rakai, Uganda. Qual Health Res. 2013;23(6):795–804. doi:10.1177/1049732313482189
33. Baeten JM, Donnell D, Kapiga SH, et al. Male circumcision and risk of male-to-female HIV-1 transmission: a multinational prospective study in African HIV-1 serodiscordant couples. AIDS. 2010;24(5):737. doi:10.1097/QAD.0b013e32833616e0
34. Kitara DL, Ocero A, Lanyero J, Ocom F. Roll-out of Medical Male Circumcision (MMC) for HIV prevention in non-circumcising communities of Northern Uganda. Pan Afr Med J. 2013;15(1). doi:10.11604/pamj.2013.15.100.2338
35. Hatzold K, Mavhu W, Jasi P, et al. Barriers and motivators to voluntary medical male circumcision uptake among different age groups of men in Zimbabwe: results from a mixed methods study. PLoS One. 2014;9(5):e85051. doi:10.1371/journal.pone.0085051
36. Plotkin M, Castor D, Mziray H, et al. “Man, what took you so long?” Social and individual factors affecting adult attendance at voluntary medical male circumcision services in Tanzania. Sci Pract. 2013;1(1):108–116.
37. Atkins K, Yeh PT, Kennedy CE, et al. Service delivery interventions to increase uptake of voluntary medical male circumcision for HIV prevention: a systematic review. PLoS One. 2020;15(1):e0227755. doi:10.1371/journal.pone.0227755
38. Ensor S, Davies B, Rai T, Ward H. The effectiveness of demand creation interventions for voluntary male medical circumcision for HIV prevention in sub-Saharan Africa: a mixed methods systematic review. J Int AIDS Soc. 2019;22:e25299. doi:10.1002/jia2.25299
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.