Back to Journals » Advances in Medical Education and Practice » Volume 17
Factors Influencing the Clinical Research Behavior Among Physicians: A Qualitative Study
Authors Rastegari F, Soleymani MR ![]() , Nouri R, Alavi M
, Nouri R, Alavi M
Received 21 December 2025
Accepted for publication 2 May 2026
Published 18 May 2026 Volume 2026:17 590739
DOI https://doi.org/10.2147/AMEP.S590739
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Fatemeh Rastegari,1 Mohammad Reza Soleymani,2 Rasool Nouri,2 Mousa Alavi3
1School of Health Management and Information Sciences, Isfahan University of Medical Sciences, Isfahan, Iran; 2Health Information Technology Research Center, Isfahan University of Medical Sciences, Isfahan, Iran; 3Nursing and Midwifery Care Research Center, Isfahan University of Medical Sciences, Isfahan, Iran
Correspondence: Mohammad Reza Soleymani, Email [email protected]
Purpose: Conducting research by physicians plays a pivotal role in enhancing the quality of education, clinical practice, and knowledge production within the healthcare system. Despite several studies conducted in this domain, the process underlying clinical research behavior among physicians has not yet been fully elucidated. Therefore, this study aimed to provide a theoretical explanation of the research behavior of physicians at medical universities.
Methods: This qualitative study employed a thematic analysis approach to explore and explain the research behavior of physicians in Iranian medical universities from March 2024 to March 2025. Twenty-two physicians were selected through purposive sampling. Semi-structured interviews were conducted, and the data were analyzed using Strauss and Corbin’s (1998) grounded theory approach, supported by MAXQDA 20 software.
Results: The data analysis resulted in the emergence of five main categories: (1) individual factors, (2) organizational factors, (3) research-related factors, (4) factors related to the process of conducting research activities, and (5) environmental factors. The core category identified in this study was conducting clinical research, which was present throughout all stages of the clinical research behavior process.
Conclusion: The research behavior of physicians is a multifaceted phenomenon influenced by various individual, organizational, research-related, and environmental factors. Hence, adopting a comprehensive and multidimensional approach is essential. The insights gained from this study can inform institutional and national policymaking aimed at improving the quantity and quality of physicians’ research behavior, thereby enhancing physicians’ professional contributions and advancing the research capacity of the healthcare sector.
Keywords: research behavior, physicians, clinical research, medical universities
Introduction
Clinical research is critically important because it directly affects patient health and treatment outcomes. Drugs, therapeutic interventions, and innovative medical technologies are systematically tested on patients to evaluate their efficacy and safety, highlighting the central role of research in improving care quality.1 Moreover, clinical research represents a cost-effective long-term strategy for strengthening health systems in developing countries by promoting equitable access, affordability, and overall service improvement.2
Physicians play a pivotal role in shaping research agendas, formulating relevant questions, and conducting studies that facilitate rapid translation of evidence into practice.3 Empirical data indicate that healthcare centers with higher physician research engagement demonstrate lower mortality rates and greater organizational efficiency.4 Despite this, global investment in research remains uneven: UNESCO reports that industrialized countries allocate 2–24% of GDP to research and researcher training, whereas many developing countries allocate 0.5% or less.5 In Iran, national initiatives have been launched to promote clinical research, yet their success heavily depends on active physician participation and adequate incentives, as high-quality, impactful studies are often undervalued in practice.
Existing literature on medical faculty research behavior, both in Iran and internationally, largely focuses on identifying barriers and facilitators.3,6–10 Strategies proposed include strengthening research infrastructure, defining national priorities, providing formal training, and fostering interdisciplinary collaboration.11,12 Analytical frameworks, such as SWOT, have been employed to assess systemic pressures affecting research engagement.13 Leadership structures and research translation processes have also been highlighted as key factors in promoting productive clinical research environments.14,15 Positive outcomes associated with physician research involvement include enhanced self-confidence, greater learning opportunities, improved clinical competencies, quality assurance, elevated professional standards, and expanded scientific networks.16,17
However, much of the existing evidence predates the systemic transformations triggered by the COVID-19 pandemic. The pandemic accelerated digitalization in clinical research through decentralized and adaptive trial models, remote data collection, telemedicine integration, regulatory flexibility, and global collaboration, while simultaneously increasing clinicians’ workload, psychological distress, and burnout.18–20 Concurrently, the rapid expansion of artificial intelligence (AI) technologies has begun to reshape research workflows by enabling advanced analytics, machine learning–based prediction, automated evidence synthesis, and enhanced data management.21–26 Although these developments offer efficiency and innovation, they introduce new challenges regarding digital literacy, governance, equity, and research integrity. Collectively, these structural and technological shifts suggest that physicians’ research behavior is now situated within a more complex, technology-mediated professional environment. In the context of Evidence-Based Medicine (EBM), understanding these barriers is now more critical than ever.27 Addressing the challenges physicians face in research is essential not only for academic advancement but for the immediate sustainability of healthcare systems.28 As the pressure to integrate rapidly evolving evidence into practice intensifies, identifying and resolving these behavioral obstacles is vital to ensure that health systems can adapt and thrive amidst current technological and clinical demands.29
Despite extensive quantitative research on physician engagement, no qualitative study has yet explored the contextual, experiential, and motivational dimensions of their research behavior in this evolving environment. Accordingly, the present study adopts a qualitative approach to examine and interpret physicians’ research behavior, aiming to generate context-sensitive insights that can inform institutional policy, capacity-building initiatives, and the design of effective incentive systems to strengthen clinical research outcomes.
Materials and Methods
This qualitative study employed a thematic analysis approach to explain the research behavior of physicians at medical universities in Iran from March 2024 to March 2025. Twenty-two physicians were selected through purposive sampling with maximum variation in terms of gender, medical specialty, academic rank, research experience, and university affiliation.
The inclusion criteria consisted of membership in a clinical department and willingness to participate in the interviews, while the exclusion criterion was withdrawal from participation at any stage of the study.
Data were collected through face-to-face semi-structured interviews. The interview guide was developed based on a review of the relevant literature and expert opinions. The interviews were conducted by a trained member of the research team and began with general questions such as, “What is the importance of research in the field of health?” and “What are your goals and motivations for engaging in research activities?” (Appendix 1). Three pilot interviews were conducted in the presence of the principal investigator to refine the interview process. To ensure reflexivity and minimize potential bias, the authors engaged in regular discussions throughout the research process to critically examine their own assumptions regarding physicians’ research behavior.
Interviews were conducted at locations mutually agreed upon with the participants after they had been fully informed about the study objectives, the confidentiality of their responses, the audio-recording process, and the voluntary nature of their participation. Each interview lasted approximately 50 minutes on average. Data collection continued until theoretical saturation was achieved. All interviews were transcribed verbatim using Microsoft Word.
Prior to the main study, the interview guide was pilot-tested with three physicians who met the inclusion criteria. These pilot interviews were conducted in the presence of the principal investigator to assess the clarity, flow, and relevance of the questions. Based on the feedback from this pilot phase, minor refinements were made to the wording of the questions to improve their comprehensibility.
Data analysis was carried out concurrently with data collection using MAXQDA version 20. Following the steps proposed by Graneheim,25 meaning units were first extracted from relevant sentences and paragraphs. These units were then condensed into shorter expressions, and initial coding was performed.
To ensure data trustworthiness, the four criteria proposed by Lincoln and Guba26—credibility, dependability, confirm ability, and transferability—were applied. Credibility was enhanced through maximum variation sampling to capture diverse experiences. Dependability was ensured by minimizing delays in data collection. The confirm ability and transferability of the findings were verified through external audits conducted by individuals not involved in the study.
The study protocol was approved by the Ethics Committee of Isfahan University of Medical Sciences with the code (IR.IUMS.REC.1401.145). All procedures were performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from all subjects involved in the study, which included permission to publish anonymized responses and quotes.
Results
A total of 22 physicians participated in this study. Their demographic characteristics are presented in Table 1. Based on the results of the interview analyses, five main categories—individual factors, organizational factors, research-related factors, factors related to the process of conducting research activities, and environmental factors—along with 20 subcategories were identified. The details of each category are discussed in the following sections. (Table 2).
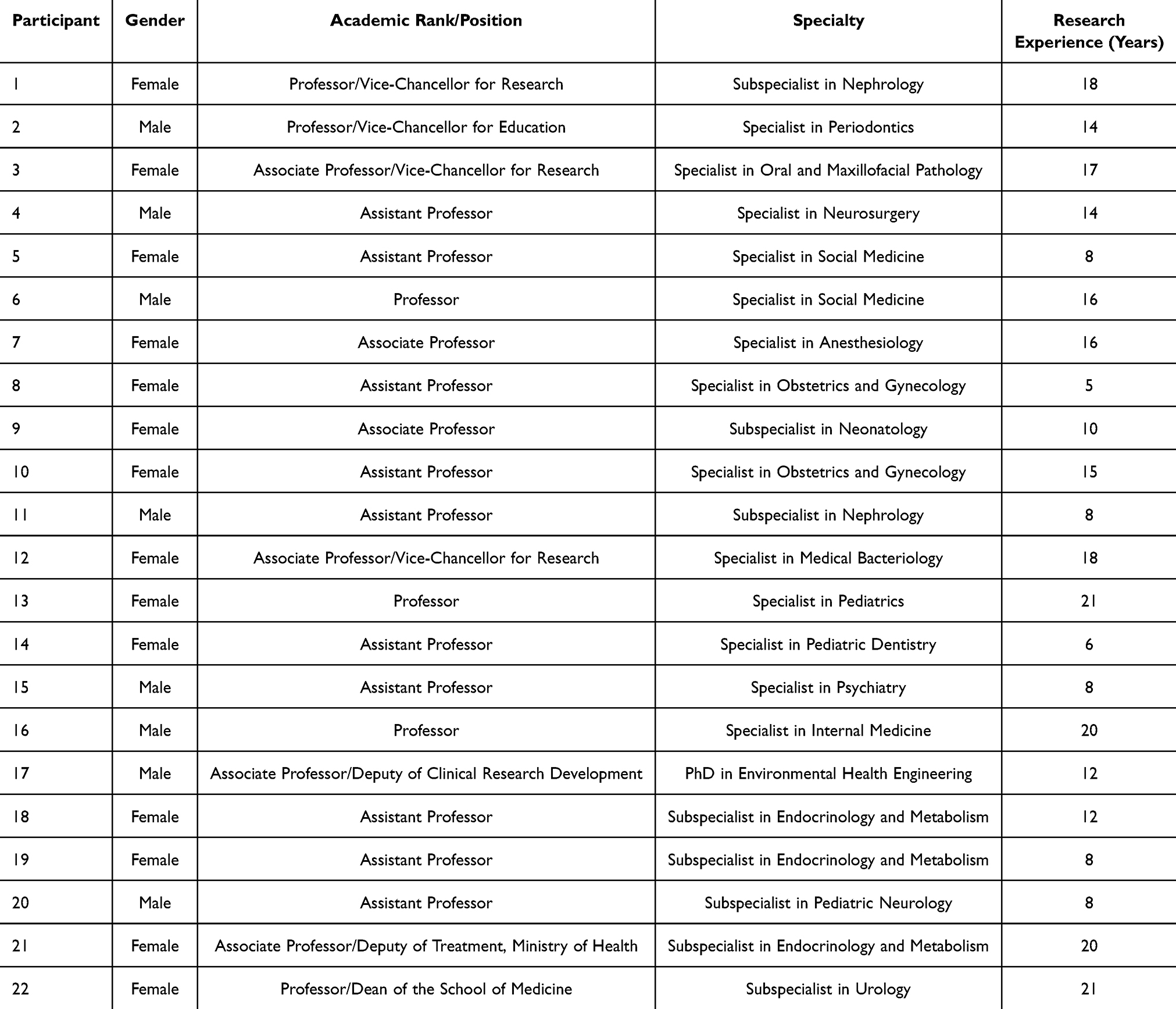 |
Table 1 Characteristics of the Interviewees |
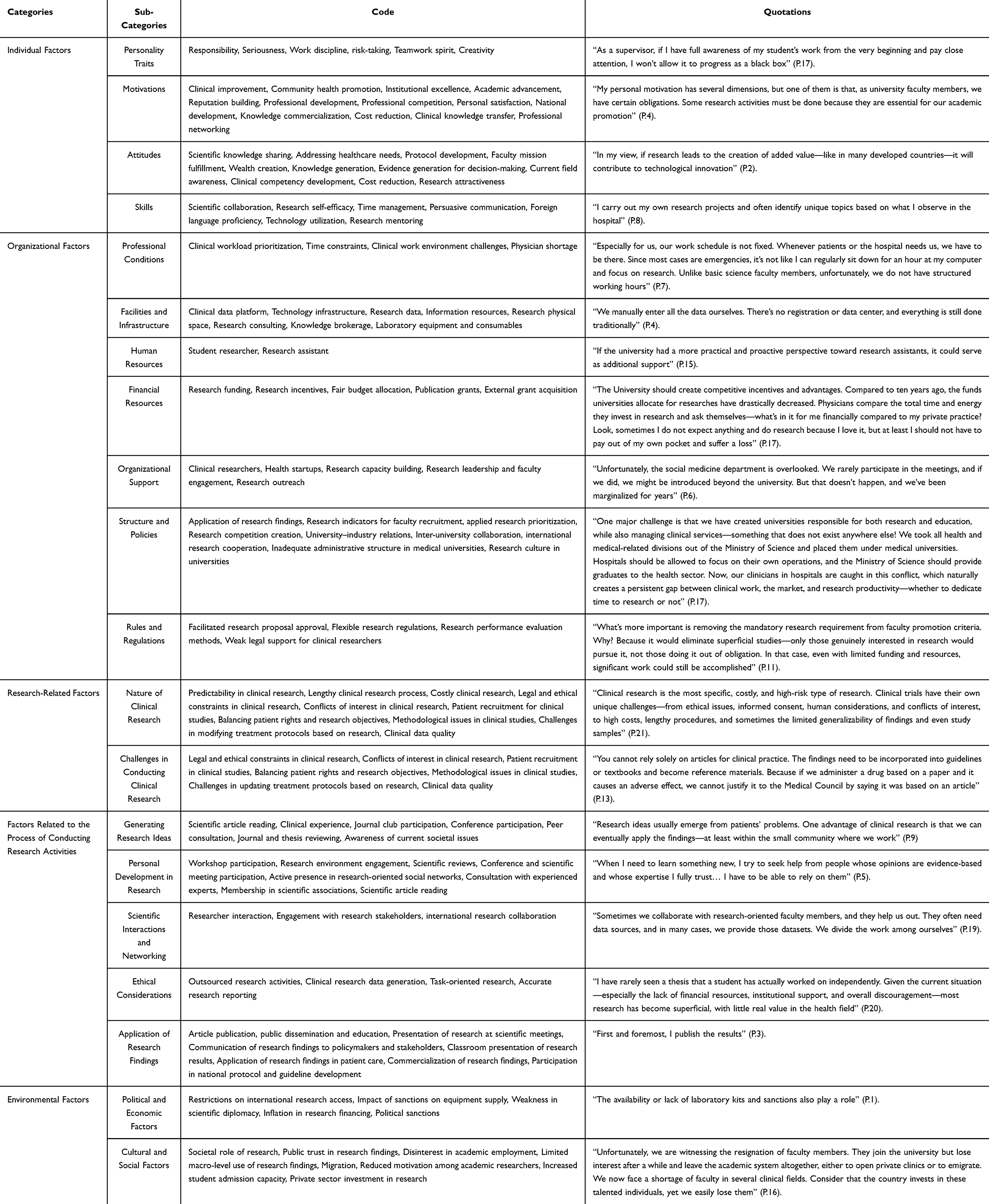 |
Table 2 Components and Subcomponents of Factors Related to Physicians’ Research Behavior |
Individual Factors
Personality Traits
Among the factors related to the research behavior of physicians, the most frequently mentioned in the interviews were personality traits such as diligence, responsibility, teamwork spirit, risk-taking, and creativity. Participant 21 stated:
I consider myself creative in conducting research. For example, if my study’s structure doesn’t allow me to continue in the same way, I don’t stop; instead, I modify the method or use alternative approaches. (P.21)
Similarly, another participant remarked:
As a supervisor, if I have full awareness of my student’s work from the very beginning and pay close attention, I won’t allow it to progress as a black box. (P.17)
Motivations
Research motivation was identified as one of the main driving forces behind faculty members’ engagement in research activities. Participant 15 explained:
Recognition is one of the reasons I do research. You see, the more research I do, the more I become connected to various institutions and professional networks. (P.15)
Another interviewee commented:
My personal motivation has several dimensions, but one of them is that, as university faculty members, we have certain obligations. Some research activities must be done because they are essential for our academic promotion. (P.4)
Attitudes
According to the findings, participants considered their attitude toward research as an important factor influencing their research engagement. For instance, Participant 2 stated:
In my view, if research leads to the creation of added value—like in many developed countries—it will contribute to technological innovation. (P.2)
Another participant emphasized the importance of knowledge sharing:
Sharing clinical knowledge among those working in the health sector happens mainly through research, and such sharing often leads to the discovery of issues that were previously unknown to us. (P.10)
Skills
Participants’ experiences indicated that research-related skills—such as scientific networking, familiarity with knowledge translation processes, and the use of modern technologies—significantly influence the quality of their research behavior. One participant explained:
I’ve tried to keep myself updated in these areas, such as artificial intelligence and research methodology. I make an effort to learn continuously and progress alongside my team. (P.18)
Another participant added:
I carry out my own research projects and often identify unique topics based on what I observe in the hospital. (P.8)
Organizational Factors
Occupational and Professional Conditions
In clinical environments, the prioritization of therapeutic activities, time constraints, working conditions, and the shortage of physicians were among the key issues raised by the participants. Supporting this point, Participant 7 stated:
Especially for us, our work schedule isn’t fixed. Whenever patients or the hospital needs us, we have to be there. Since most cases are emergencies, it’s not like I can regularly sit down for an hour at my computer and focus on research. Unlike basic science faculty members, unfortunately, we don’t have structured working hours. (P.7)
Facilities and Infrastructure
The existence of research centers, research development units, laboratory equipment, clinical data registration systems, technological infrastructures, research consultancy services, and knowledge brokerage services can all influence the quality of research behavior. In support of this view, Participant 4 stated:
We manually enter all the data ourselves. There’s no registration or data center, and everything is still done traditionally. (P.4)
Another participant added:
Advanced surgical devices or laboratory kits are expensive. We are currently negotiating with health benefactors to cover hospitals with advanced equipment and integrate them into the clinical and research systems. (P.22)
Research Human Resources
According to the physicians, clinical research requires effective collaboration and interaction among research team members. One participant mentioned:
I currently have a resident who’s about to graduate. The situation in the anesthesiology department is terrible because residents don’t join it anymore—there’s nothing in it for them. The new generation is smarter; they’re not like us who would stay in a field and keep working. (P.7)
Similarly, Participant 15 stated:
If the university had a more practical and proactive perspective toward research assistants, it could serve as additional support. (P.15)
Financial Resources
Participants emphasized the critical role of funding in providing specialized equipment, research rewards, publication subsidies, and ensuring equity in budget allocation. As participant 7 explained:
The research budget goes toward buying drugs or equipment, but in many cases, it doesn’t even reach that stage. The researcher’s compensation isn’t even considered. (P.7)
Participant 17 elaborated further:
The University should create competitive incentives and advantages. Compared to ten years ago, the funds universities allocate for researches have drastically decreased. Physicians compare the total time and energy they invest in research and ask themselves—what’s in it for me financially compared to my private practice? Look, sometimes I don’t expect anything and do research because I love it, but at least I shouldn’t have to pay out of my own pocket and suffer a loss. (P.17)
Organizational Support
In this regard, participants pointed to several issues. Participant 6 stated:
Unfortunately, the social medicine department is overlooked. We rarely participate in the meetings, and if we did, we might be introduced beyond the university. But that doesn’t happen, and we’ve been marginalized for years. (P.6)
Another participant noted:
I’ve never used university grants. The university claims to provide grants for faculty members, but it varies greatly from one university to another. Grants have become relationship-based and even individuals’ positions influence grant acquisition. (P.15)
Structure and Policies
Policies such as promoting the practical application of research findings, incorporating research competence into faculty recruitment criteria, prioritizing applied research, fostering healthy competition in research, strengthening university–industry collaboration, establishing inter-university agreements, and revising the administrative structure of medical universities can all enhance physicians’ motivation and research capabilities. Participant 17 explained:
One major challenge is that we’ve created universities responsible for both research and education, while also managing clinical services—something that doesn’t exist anywhere else! We took all health and medical-related divisions out of the Ministry of Science and placed them under medical universities. Hospitals should be allowed to focus on their own operations, and the Ministry of Science should provide graduates to the health sector. Now, our clinicians in hospitals are caught in this conflict, which naturally creates a persistent gap between clinical work, the market, and research productivity—whether to dedicate time to research or not. (P.17)
Rules and Regulations
Interviews with physicians revealed several key themes regarding rules and regulations, including research policies, performance evaluation procedures, and legal protections for researchers in clinical studies. Participant 11 stated:
What’s more important is removing the mandatory research requirement from faculty promotion criteria. Why? Because it would eliminate superficial studies—only those genuinely interested in research would pursue it, not those doing it out of obligation. In that case, even with limited funding and resources, significant work could still be accomplished. (P.11)
Research-Related Factors
Nature of Clinical Research
Given the human-centered nature of clinical research, Participant 21 described its characteristics as follows:
Clinical research is the most specific, costly, and high-risk type of research. Clinical trials have their own unique challenges—from ethical issues, informed consent, human considerations, and conflicts of interest, to high costs, lengthy procedures, and sometimes the limited generalizability of findings and even study samples. (P.21)
Challenges in Conducting Clinical Research
One of the major themes emerging from this study pertains to the numerous challenges faced by researchers in the process of conducting clinical studies. Participant 22 noted:
When it comes to patients, their rights must be respected. We need to ensure informed consent for those we include in our studies, maintain data confidentiality, and protect personal information. As you know, these are essential in clinical research. Most importantly, the study must pose no risk to our patients. (P.22)
Similarly, Participant 13 emphasized:
You can’t rely solely on articles for clinical practice. The findings need to be incorporated into guidelines or textbooks and become reference materials. Because if we administer a drug based on a paper and it causes an adverse effect, we can’t justify it to the Medical Council by saying it was based on an article. (P.13)
Factors Related to the Process of Conducting Research Activities
Generating Research Ideas
Participants identified several sources for generating research ideas, including reading academic papers, clinical experiences, attending scientific meetings, consulting with colleagues and students, peer reviewing, and identifying existing research gaps. One participant stated:
Research ideas usually emerge from patients’ problems. One advantage of clinical research is that we can eventually apply the findings—at least within the small community where we work. (P.9)
Another participant added:
I choose topics that haven’t been studied in Iran before, or at least have very limited prior research. (P.21)
Personal Development in Research
Findings from this study revealed that researchers enhance their capabilities through various means such as attending workshops, participating in peer review, joining scientific meetings, consulting experienced colleagues, joining academic associations, and engaging in self-study through scholarly resources. Participant 5 noted:
When I need to learn something new, I try to seek help from people whose opinions are evidence-based and whose expertise I fully trust… I have to be able to rely on them. (P.5)
Participant 14 further explained:
I teach research methodology workshops at the university, which has helped me evolve in this field and guide my students better. It has also allowed me to become recognized in the research community and establish connections with other faculty members. (P.14)
Scientific Interactions and Networking
The findings indicated that research team formation provides an effective platform for knowledge and skill sharing. Participant 21 remarked:
I’m a shareholder in a pharmaceutical company, and through that, I’ve built connections with other pharmaceutical firms, which helps me with team formation. (P.21)
Participant 19 added:
Sometimes we collaborate with research-oriented faculty members, and they help us out. They often need data sources, and in many cases, we provide those datasets. We divide the work among ourselves. (P.19)
Ethical Considerations
Participants raised several issues concerning research ethics, including outsourcing research activities, data fabrication in clinical studies, and mistrust in research findings. One participant stated:
Nowadays, we outsource our work to companies that handle everything—from proposal writing to article acceptance. It has become a common practice among physicians. You can find these companies online; they manage the entire process. I once didn’t have the time, so I gave my project to one of them. (P.7)
Another participant observed:
I’ve rarely seen a thesis that a student has actually worked on independently. Given the current situation—especially the lack of financial resources, institutional support, and overall discouragement—most research has become superficial, with little real value in the health field. (P.20)
Application of Research Findings
One of the most important indicators of success in clinical research is the practical application of its findings. The results of this study showed that research outcomes are applied through journal publications, presentations at scientific conferences, teaching, patient treatment, health-related decision-making, and the development of clinical protocols. Participant 21 stated:
We have a research team that develops endocrinology-related guidelines. Each member of the team is motivated and competent in their area. I also share my findings with the public through television and other media. (P.21)
Another participant added: “First and foremost, I publish the results” (P.3).
Environmental Factors
Political and Economic Factors
Clinical research, as one of the key pillars of knowledge advancement and healthcare system improvement, is inevitably influenced by environmental factors beyond the academic domain. Participant 2 stated: “Lately, whenever I submit an article to a journal, they respond that we are under sanctions and therefore unable to accept your paper” (P.2). Another participant mentioned: “The availability or lack of laboratory kits and sanctions also play a role” (P.1).
Cultural and Social Factors
Clinical research is also profoundly shaped by cultural and social conditions. Participant 17 noted:
We currently have an imbalance here. With the rising inflation, the income of faculty members has become much lower compared to those working privately or running their own clinics. This gap keeps widening. After a few years, a clinical faculty member may reach the rank of assistant professor but then decide they can no longer continue and instead spend their mornings working in private practice. (P.17)
Similarly, Participant 16 remarked:
Unfortunately, we are witnessing the resignation of faculty members. They join the university but lose interest after a while and leave the academic system altogether, either to open private clinics or to emigrate. We now face a shortage of faculty in several clinical fields. Consider that the country invests in these talented individuals, yet we easily lose them. (P.16)
Discussion
The present study reveals that physicians’ research behavior is a multifaceted construct operationalized through the dynamic interplay of individual, organizational and social factors. Rather than being a linear sequence of activities, our findings suggest that research behavior emerges from a complex negotiation between clinical responsibilities and academic aspirations within the Iranian healthcare context. At the individual level, the data indicate that physicians perceive research as a high-stakes endeavor requiring specialized ethical and technical competencies. This aligns with Estapé-Garrastazu et al who noted that clinical researchers must possess strong ethical skills. However, our analysis deepens this by highlighting that in the Iranian context, the complexity of obtaining legal approvals and the high costs involved often act as deterrents. Consequently, physicians may retreat to safe, low-cost projects to avoid bureaucratic friction. This behavior is not merely a lack of motivation but a rational response to a system that lacks differentiated support structures.30 As Aguayo et al suggested, involving patients in ideation could foster innovation, yet our findings imply that without first reducing the administrative burden on physicians, such engagement remains difficult to achieve.31 Furthermore, the emphasis on collaboration by Moradi et al and Sonstein et al is corroborated by our data; however, we found that the quality of interpersonal relationships is often strained by a competitive rather than cooperative academic culture, hindering the trust necessary for enduring partnerships. A critical contribution of this study is the identification of a profound structural and cultural gap that impedes the transition from clinical roles to research roles.32,33 While previous literature, such as Talla et al has discussed the utility of knowledge brokers in bridging the gap between knowledge production and application, our findings suggest that the primary barrier lies earlier in the process: the disconnect between the clinical workflow and the research infrastructure. The structural gap refers to the misalignment between heavy clinical workloads and the rigid, resource-scarce research environment. The cultural gap pertains to a prevailing ethos where clinical practice is undervalued compared to publication metrics, creating an environment where research is often performed for promotion rather than genuine inquiry. This dual gap explains why the application of research results remains sporadic; physicians are structurally discouraged from integrating research into their daily routine, as the system lacks the facilitative structures called for by policy experts.34 Furthermore, our analysis underscores that environmental factors are not merely a backdrop but active shapers of research behavior. Weaver and Afshari correctly identify international collaboration as a driver of impact, yet our study reveals that the weak research-oriented culture in Iran acts as a ceiling for these ambitions.1,35 The findings by Merwin et al and Mansuri and Ebrahimi regarding the need for supportive policies and cultural evaluation are particularly pertinent here.36,37 We interpret these findings as evidence that individual capacity is insufficient without a corresponding ecosystem of support. The current environment, characterized by limited international connections and a lack of teamwork, forces physicians into a survival mode where research behavior is fragmented rather than systematic. In conclusion, this study argues that enhancing physicians’ research behavior requires more than individual training; it demands a systemic overhaul of the research culture. Policymakers must move beyond generic incentives and address the specific structural and cultural barriers identified here.
By bridging the gap between clinical and research roles through targeted support—such as streamlining ethical approvals and fostering a culture of collaboration—the healthcare system can better leverage its clinical workforce for high-quality research. Limitations This study faced certain limitations that should be acknowledged. The participants were clinical physicians who were often engaged in intensive treatment-related responsibilities, which at times posed challenges in terms of accessibility and scheduling for data collection.
Conclusion
The findings of this study revealed that the research behavior of physicians is a multifaceted phenomenon influenced by a dynamic interplay of individual, organizational, and environmental factors. Specifically, our analysis identified a critical “structural and cultural gap” that acts as a primary barrier to research engagement. Therefore, improving and enhancing the research behavior of physicians requires moving beyond generic calls for increased funding; it demands targeted interventions that bridge this specific gap. In addition to strengthening motivation and research competencies, it is essential to foster a supportive and research-oriented culture within universities. Practically, this means operationalizing cultural change by restructuring reward systems to value clinical research as highly as patient care, and creating formal mentorship programs that mitigate the isolation physicians often feel in research endeavors. Moreover, the unique nature, complexity, and specific characteristics of clinical research necessitate differentiated approaches to both the facilitation and evaluation of such studies. Policymakers should therefore move away from “one-size-fits-all” metrics and adopt flexible evaluation frameworks that account for the specific constraints of clinical workflows. In direct response to the research questions, this study confirms that while individual barriers exist, they are exacerbated by a rigid infrastructure that fails to integrate research into the clinical role. The insights derived from this research can serve as a foundation for institutional and national policy-making aimed at dismantling the structural silos between clinical practice and research. By addressing these specific disconnects, universities can enhance physicians’ contribution to academic inquiry and advance the overall research capacity of the healthcare sector. Conducting future intervention studies and examining the specific mechanisms through which each of these factors exerts its influence would provide policymakers with more detailed and nuanced information to guide evidence-based decisions.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The ethics committee of Isfahan University of Medical Sciences approved the study with the ID Number IR.MUI.NUREMA.REC.1401.145. All authors demonstrate that they have adhered to the accepted ethical standards of a genuine research study and that all study is conducted with integrity, fidelity, and honesty.
Consent for Publication
Authors hereby give my full consent for the publication of the above-mentioned work in journal of Advances in Medical Education and Practice. We confirm that this work is our original creation and that we hold the intellectual property rights. We grant permission to the journal to publish the work in both print and digital formats. This consent is given voluntarily and without any coercion.
Acknowledgments
This study was conducted as part of a PhD thesis at Isfahan University of Medical Sciences (Code: 3401615) and was supported academically and administratively.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Afshari M. Research challenges in Iranian Universities of Medical Sciences. J Culture Health Promot Acad Medical Sci. 2024.
2. Kabirpanthi V, Gupta V, Chavan P. Barriers perceived by researchers in pursuing medical research in an evolving medical college of tribal Madhya Pradesh, India. J Family Med Prim Care. 2022;11(2):701–13. doi:10.4103/jfmpc.jfmpc_1706_21
3. Brandenburg C, Noble C, Wenke R, et al. Relationship between research culture and research activity of medical doctors: a survey and audit. J Multidisciplin Healthcare. 2021;14:2137–2150. doi:10.2147/JMDH.S319191
4. Kaiser F, Schmid A, Schlüchtermann J. Physician-leaders and hospital performance revisited. Soc Sci Med. 2020;249.
5. Anderson BJ, Kligler B, Taylor B, et al. Faculty survey to assess research literacy and evidence-informed practice interest and support at pacific college of oriental medicine. J AlternComplementary Med. 2014;20(9):705–712. doi:10.1089/acm.2014.0138
6. Conradie A, Duys R, Forget P, et al. Barriers to clinical research in Africa: a quantitative and qualitative survey of clinical researchers in 27 African countries. Br J Anaesth. 2018;121:813–821. doi:10.1016/j.bja.2018.06.013
7. Fournier I, Stephenson K, Fakhry N, et al. Barriers to research among residents in Otolaryngology-Head & Neck Surgery around the world. Eur Ann Otorhinolaryngol Head Neck Dis. 2019;136(3):S3–7. doi:10.1016/j.anorl.2018.06.006
8. Embi PJ, Tsevat J. Commentary: the relative research unit: providing incentives for clinician participation in research activities. Acad Med. 2012;87(1):11–14. doi:10.1097/ACM.0b013e31823a8d99
9. Seyyedmajidi M, Khafri S, Sohanian S, et al. Evaluation of the viewpoints of faculty members regarding to research barriers at Babol dental school. Biannual Med Educ Babol Univ Med Sci. 2018;6(1):27–32.
10. Rashid KA, Gomathy S, Manan A. The involvement of doctors in research activities in two major hospitals in Penang, Malaysia. Malaysian J Public Health Med. 2012;24–30.
11. Wenke RJ, Mickan S, Bisset L. A cross sectional observational study of research activity of allied health teams: is there a link with self-reported success, motivators and barriers to undertaking research? BMC Health Serv Res. 2017;17. doi:10.1186/s12913-017-1996-7
12. Squires A, Chitashvili T, Djibuti M, et al. Health research capacity building in Georgia: a case-based needs assessment. Public Health. 2017;147:1–7. doi:10.1016/j.puhe.2017.01.024
13. George JF, Chen H. Developing research programs that align with the clinical mission. Surgery. 2024;175(4):1244–1246. doi:10.1016/j.surg.2023.11.021
14. Lavis JN, Guindon GE, Cameron D, et al. Bridging the gaps between research, policy and practice in low- and middle-income countries: a survey of researchers. CMAJ. 2010;182(9):E350–E361. doi:10.1503/cmaj.081164
15. Tabatabaie HAF, Ansarinia A. Investigating some obstacles in applying research results in clinical practice from the perspective of faculty members of Yazd Dental School in 2016. J Res Dent Sci. 2019;16:141–152.
16. Wenke R, Weir KA, Noble C, Mahoney J, Mickan S. Not enough time for research? Use of supported funding to promote allied health research activity. J Multidisciplin Healthcare. 2018;11:269–277. doi:10.2147/JMDH.S157034
17. Jonker L, Fisher SJ, Dagnan D. Patients admitted to more research-active hospitals have more confidence in staff and are better informed about their condition and medication: results from a retrospective cross-sectional study. J Eval Clin Pract. 2019;26:203–208. doi:10.1111/jep.13118
18. Park JJ, Mogg R, Smith GE, et al. How COVID-19 has fundamentally changed clinical research in global health. Lancet Glob Health. 2021;9(5):e711–e20. doi:10.1016/S2214-109X(20)30542-8
19. Angus DC. Optimizing the trade-off between learning and doing in a pandemic. JAMA. 2020;323(19):1895–1896. doi:10.1001/jama.2020.4984
20. Shanafelt TD, West CP, Sinsky C, Trockel M, Tutty M, editor. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2020. In:
21. Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nature Med. 2019;25(1):44–56. doi:10.1038/s41591-018-0300-7
22. Esteva A, Robicquet A, Ramsundar B, et al. A guide to deep learning in healthcare. Nature Med. 2019;25(1):24–29. doi:10.1038/s41591-018-0316-z
23. Liu X, Rivera SC, Moher D, et al. Reporting guidelines for clinical trial reports for interventions involving artificial intelligence: the CONSORT-AI extension. Lancet Digital Health. 2020;2(10):e537–e48. doi:10.1016/S2589-7500(20)30218-1
24. I. C. Organisation For Economic Co-Operation And Development—OECD. The Europa Directory of International Organizations 2022. Routledge. 694–701; 2022.
25. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
26. Lincoln YS, Guba EG. But is it rigorous? Trustworthiness and authenticity in naturalistic evaluation. New Dir Eval. 1986;30:73–84.
27. Djulbegovic B, Guyatt G. Evidence base medicine 2.0: a new paradigm for evidence-based medicine in the 21st century. J Clin Epidemiol. 2020;123.
28. Swinkels A AJ. The state of evidence-based practice: a review of the literature. Worldviews Evid Based Nurs. 2022;19(1):6–14. doi:10.1111/wvn.12560
29. Muhamedagic B. Evidence based medicine - new approaches and challenges. Mater Sociomed. 2021;33(1):71–75.
30. Estapé-Garrastazu ES, Noboa-Ramos C, De Jesús-Ojeda L, et al. Clinical and translational research capacity building needs in minority medical and health science hispanic institutions. Clin Transl Sci. 2014;7(5):406–412. doi:10.1111/cts.12165
31. Aguayo GA, Goetzinger C, Scibilia R, et al. Methods to generate innovative research ideas and improve patient and public involvement in modern epidemiological research: review, patient viewpoint, and guidelines for Implementation of a Digital Cohort Study. J Med Internet Res. 2021;23:e25743. doi:10.2196/25743
32. Moradi R, Zargham-Boroujeni A, Soleymani MR, et al. Factors related to the international research collaboration in the health area: a qualitative study. J Educ Health Promot. 2020;9. doi:10.4103/jehp.jehp_497_20
33. Sonstein SA, Silva H, Jones CT, Bierer BE. Education and training of clinical research professionals and the evolution of the Joint Task Force for Clinical Trial Competency. Front Pharmacol. 2024;15. doi:10.3389/fphar.2024.1291675
34. Kengne Talla P, Robillard C, Ahmed S, et al. Clinical research coordinators’ role in knowledge translation activities in rehabilitation: a mixed methods study. BMC Health Serv Res. 2023;23:124. doi:10.1186/s12913-023-09027-0
35. Weaver SP. Increasing residency research output while cultivating community research collaborations. Fam Med. 2018;50(6):460–464. doi:10.22454/FamMed.2018.734196
36. Merwin SL, Fornari A, Lane LB. A preliminary report on the initiation of a clinical research program in an orthopaedic surgery department: roadmaps and tool kits. J Surg Educ. 2014;71(1):43–51. doi:10.1016/j.jsurg.2013.06.002
37. Mansouri A, Ebrahimi Dorche E. Success factors in research activities based on the experiences of top researchers. Scientometrics Res J. 2024;10(1):115–121.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.