Back to Journals » Cancer Management and Research » Volume 18

Factors Influencing Survival After Curative Gastrectomy in Oligometastatic Gastric Cancer: A Single-Center Study
Authors Yumak M, Deniz A ![]() , Gursoy G
, Gursoy G
Received 23 January 2026
Accepted for publication 5 May 2026
Published 13 May 2026 Volume 2026:18 594098
DOI https://doi.org/10.2147/CMAR.S594098
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Yong Teng
Merve Yumak,1 Abdulkadir Deniz,1 Gokturk Gursoy2
1Department of Gastroenterological Surgery, Van Training and Research Hospital, Van, Türkiye; 2Department of Surgical Oncology, Van Training and Research Hospital, Van, Türkiye
Correspondence: Merve Yumak, Department of Gastroenterological Surgery, Van Training and Research Hospital, Van, Türkiye, Email [email protected]
Background: Gastric cancer remains a major global health burden. Oligometastatic gastric cancer (OMGC) represents an intermediate disease state with limited metastatic spread and potential eligibility for multimodal treatment.
Objective: To evaluate clinicopathological factors associated with overall survival (OS) and progression-free survival (PFS) in patients undergoing curative-intent surgery for OMGC.
Methods: This retrospective study included 38 patients with de novo OMGC who underwent curative-intent gastrectomy between 2011 and 2023. Oligometastatic disease was defined according to OMEC/Bertinoro 2024 criteria: solitary liver metastasis (Group A), para-aortic lymph node metastasis (Group B), or limited peritoneal dissemination (Group C, PCI ≤ 6). Survival was analyzed using Kaplan-Meier and Cox regression.
Results: Median follow-up was 28 months; 32 patients (84.2%) died. Median OS was 18.0 months. Female sex and age ≥ 65 years were associated with longer OS (p=0.003 and p=0.001). Adjuvant chemotherapy (HR=0.24; p< 0.001) and adjuvant chemoradiotherapy (p=0.039) improved OS. R0 resection rates varied: liver 85.7%, para-aortic 62.5%, peritoneal 12.5%. Five-year OS was 41% for liver metastases vs 0% for peritoneal disease. Harvest of ≥ 30 lymph nodes was independently associated with improved OS (HR=0.45; p=0.028).
Conclusion: Survival in OMGC is strongly influenced by metastatic pattern, adequacy of lymphadenectomy, and adjuvant therapy. Liver metastases have the most favorable prognosis; peritoneal involvement requires highly selective criteria for surgery.
Keywords: oligometastatic gastric cancer, survival analysis, lymphadenectomy
Introduction
Gastric cancer remains a leading cause of cancer-related mortality worldwide, with approximately one million new cases annually.1,2 Despite advances in systemic therapies, metastatic disease continues to portend a poor prognosis, with 35–50% of patients presenting with metastases at diagnosis.3 Accurate staging relies on endoscopic evaluation with deep biopsies for histopathological confirmation, complemented by cross-sectional imaging.4–6
The oligometastatic disease (OMD) concept describes an intermediate state with limited metastatic burden.7 In gastric cancer, this defines oligometastatic gastric cancer (OMGC), where aggressive local therapies combined with systemic treatment may offer curative potential.8 Management requires a multidisciplinary approach incorporating nutritional support,9 neoadjuvant chemotherapy,10 and innovative local therapies.11,12 Complex management pathways achieve superior outcomes in high-volume centers.13
While current NCCN and Japanese guidelines lack standardized OMGC algorithms, radical surgery may be considered for solitary liver metastases or para-aortic lymph node involvement.3,14 ESMO and Bertinoro 2024 guidelines define OMGC eligibility based on limited liver metastases, specific nodal stations, or peritoneal carcinomatosis with Peritoneal Cancer Index (PCI) ≤6.15–17 The RENAISSANCE trial demonstrated potential survival benefit in patients with isolated retroperitoneal lymph node metastases.18 Japanese and Korean data indicate OMGC accounts for 20–30% of gastric cancer cases.19,20
Identifying prognostic markers such as lymphadenectomy extent and adjuvant therapy use remains crucial.21,22 However, real-world data from high-incidence regions like Eastern Turkey remain scarce.23 This study aims to evaluate clinical and pathological predictors of overall survival and progression-free survival in patients undergoing curative surgery for OMGC at a tertiary center in Eastern Turkey, with focus on surgical technique, adjuvant therapy, and metastasis patterns.
It should be noted that treatment strategies for OMGC have evolved considerably over the past decade. During the earlier years of the study period, neoadjuvant chemotherapy was not uniformly adopted in our region, and upfront surgery followed by adjuvant therapy was frequently considered for highly selected patients with limited metastatic burden. Therefore, the present study reflects a real-world, single-center experience over a long time span.
Materials and Methods
Study Design and Setting
This retrospective observational study was conducted at Van Training and Research Hospital, a tertiary care referral center in Eastern Turkey. The study aimed to evaluate the clinicopathological features and survival outcomes of patients undergoing curative-intent surgery for histologically confirmed OMGC. This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was granted by the Van Training and Research Hospital Ethics Committee (approval number: GOKAEK/2025-05-13, date: 04.07.2025).
Patient Selection and Multidisciplinary Evaluation
We included 38 consecutive patients with de novo OMGC who underwent curative-intent surgery between January 2011 and December 2023. Inclusion criteria were age ≥18 years, histologically confirmed gastric adenocarcinoma, and radiologically defined oligometastatic disease according to ESMO/Bertinoro 2024 criteria. Eligible metastatic patterns included solitary liver metastasis (Group A), para-aortic lymph node involvement at stations 16a2/16b1 (Group B), or peritoneal dissemination with PCI ≤6 (Group C).
Radiological and Pathological Assessment
Oligometastatic status was confirmed using contrast-enhanced computed tomography (CT) and, when indicated, 18F-FDG PET-CT. Staging laparoscopy with peritoneal cytology was performed in all patients with suspected peritoneal disease. Quantitative response to preoperative chemotherapy was defined as >50% reduction in target lesions per RECIST 1.1.
In patients with peritoneal metastases, curative-intent surgery was considered only in highly selected cases (PCI ≤6 and favorable response to systemic chemotherapy). No patients underwent hyperthermic intraperitoneal chemotherapy (HIPEC). Patients with positive peritoneal cytology were excluded.
All patients underwent curative-intent gastrectomy with metastasectomy and had complete clinical records with a minimum follow-up of 6 months. All cases were evaluated by a multidisciplinary team (MDT) comprising gastrointestinal surgeons, medical oncologists, radiation oncologists, radiologists, pathologists, and nutrition specialists. Exclusion criteria included incomplete records, unresectable metastatic disease, palliative surgery only, metastatic patterns outside OMGC criteria, or unsuitability for aggressive resection based on MDT consensus.
Data Collection
Data were collected retrospectively from electronic medical records, pathology databases, and MDT reports. Variables included: demographic data (age, sex), clinical parameters (preoperative chemotherapy regimens/cycles, response), surgical procedures, pathological characteristics (tumor size, lymph node harvest/involvement, margin status, histology, Lauren classification, differentiation grade, lymphovascular invasion, perineural invasion), treatment details (adjuvant chemotherapy/radiotherapy regimens, cycles), and outcomes (postoperative mortality, OS, PFS).
Surgical Approach
Experienced gastrointestinal surgeons performed all procedures. Standard surgery involved total/subtotal gastrectomy with D2 lymphadenectomy, defined as removal of perigastric nodes (stations 1–7) plus nodes along the left gastric artery (station 9), common hepatic artery (station 8), celiac artery (station 12a), and splenic artery (stations 11p, 11d). For patients in Group B (para-aortic metastases), D2 lymphadenectomy was performed in all cases, with additional para-aortic lymph node dissection (stations 16a2/16b1) when indicated.
Metastasectomy techniques varied by group:
- Group A (Liver): Anatomical (segmentectomy) or non-anatomical wedge resections with ≥1 cm margins when possible.
- Group B (Para-aortic): Dissection of stations 16a2/16b1.
- Group C (Peritoneal): Complete omentectomy with peritonectomy in affected regions documented by PCI.
The primary surgical goal was R0 resection (no microscopic residual tumor at primary or metastatic sites).
All patients were managed following standardized Enhanced Recovery After Surgery (ERAS) principles.
Adjuvant Therapy Protocols
Adjuvant Chemotherapy
Patients received doublet/triplet regimens based on performance status:
- FLOT regimen (5-FU, leucovorin, oxaliplatin, docetaxel): 4 cycles every 2 weeks.
- XELOX regimen (capecitabine, oxaliplatin): 6–8 cycles every 3 weeks.
Adjuvant Chemoradiotherapy (CRT)
Administered to high-risk patients (node positivity, close margins). Radiation delivered 45–50.4 Gy in 25–28 fractions (1.8–2.0 Gy/fraction) to the tumor bed and regional lymph nodes. Concurrent chemotherapy used capecitabine (825 mg/m2 twice daily on treatment days) or 5-FU.
Follow-Up and Outcomes
Follow-up included scheduled outpatient visits, CT scans (every 3–6 months for the first 2 years, then annually), and telephone interviews. Overall survival (OS) was defined as the time from diagnosis to death from any cause. Progression-free survival (PFS) was defined as the time from diagnosis to first documented recurrence (locoregional/distant) or death. A sensitivity analysis using surgery date as the start point yielded similar results (data not shown).
Statistical Analysis
Analyses used SPSS 25.0. Continuous variables were reported as mean ± SD or median (range), categorical variables as frequencies/percentages. Normality was assessed with the Kolmogorov–Smirnov test. Group comparisons used the Chi-square/Fisher’s exact tests (categorical) and Student’s t-test/Mann–Whitney U-test (continuous). Survival curves used the Kaplan-Meier method with the Log rank test for comparisons. The minimal clinically important difference (MCID) for OS was predefined as 3 months. Variables with p<0.1 in univariate analysis entered multivariate Cox proportional hazards regression (backward stepwise) to identify independent prognostic factors. The following variables were included in the multivariate model: age, sex, metastasis type, adjuvant chemotherapy, R0 resection status, lymph node harvest (categorized as ≥30 vs <30), and Lauren classification. Model assumptions (proportional hazards) were tested and satisfied. Hazard ratios with 95% confidence intervals are reported, with p<0.05 considered statistically significant.
Results
Baseline Clinicopathological Characteristics
Baseline demographic and clinicopathological characteristics are summarized in Table 1. A total of 38 patients with de novo OMGC underwent curative-intent surgery. The median follow-up duration was 28 months (range: 6–132 months). During follow-up, 32 patients (84.2%) died, while 6 patients (15.8%) remained alive.
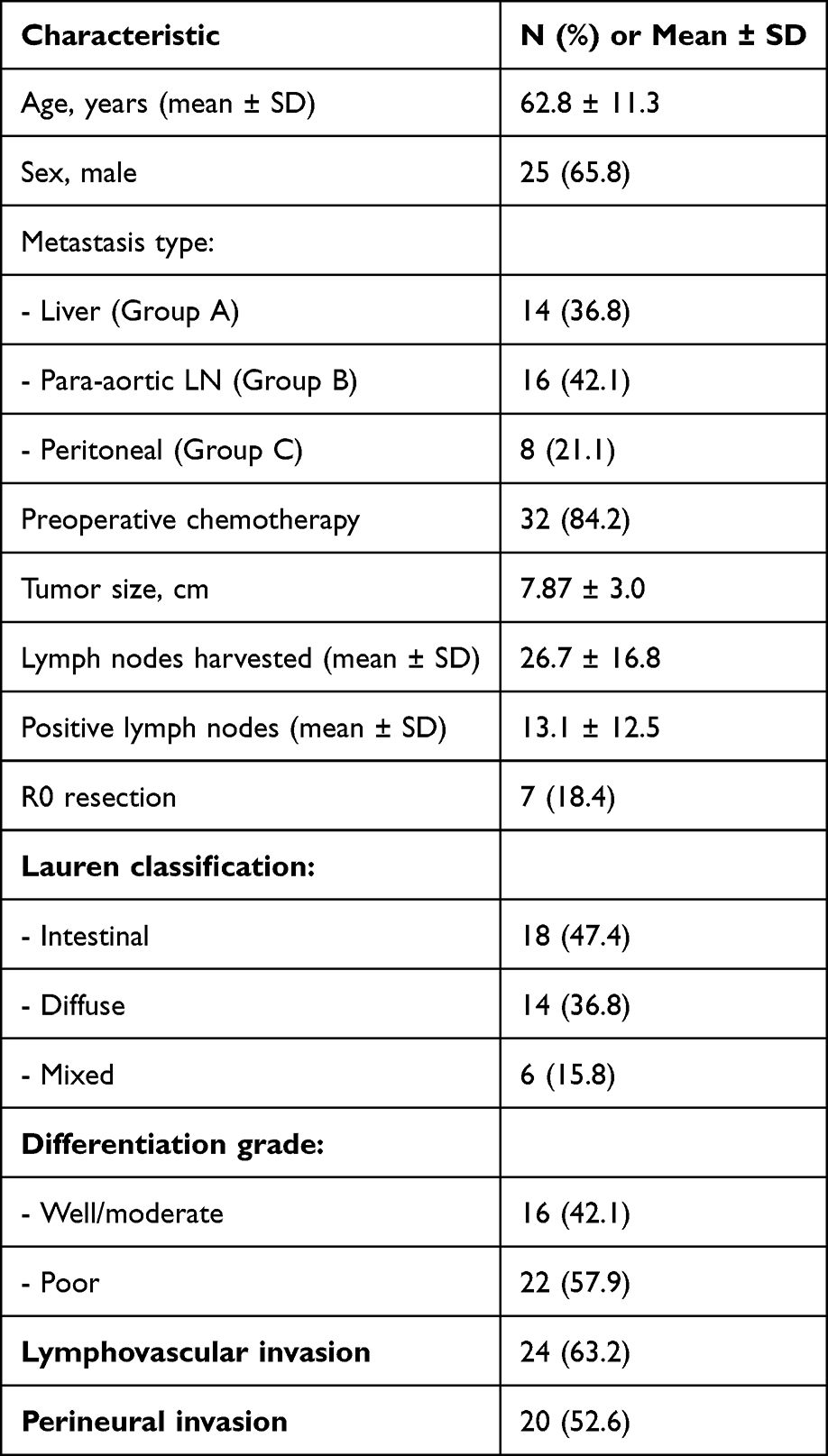 |
Table 1 Baseline Clinicopathological Characteristics of the Study Cohort (N=38) |
Neoadjuvant Treatment Details
Among the 32 patients who received preoperative chemotherapy, regimens included FLOT (n=18, 56.3%), XELOX (n=10, 31.3%), and other regimens (n=4, 12.5%). The median number of cycles was 4 (range: 2–6). A partial response (>50% reduction in target lesions) was observed in 21 patients (65.6%), stable disease in 8 (25.0%), and progression in 3 (9.4%). No patients received immunotherapy or targeted therapy in the neoadjuvant setting.
Comparative Analysis: Survivors vs Non-Survivors
Comparative analysis between survivors and non-survivors revealed several significant differences (Table 2). All surviving patients were female, whereas 78.1% of non-survivors were male (p=0.001). Survivors were significantly older (75.1 vs 60.5 years; p=0.001). Survivors had a higher mean number of lymph nodes removed (33.5 vs 25.4; p=0.035) and larger tumor sizes (9.0 vs 7.67 cm; p=0.044). Adjuvant chemotherapy was administered to all survivors vs 59.4% of non-survivors (p=0.064).
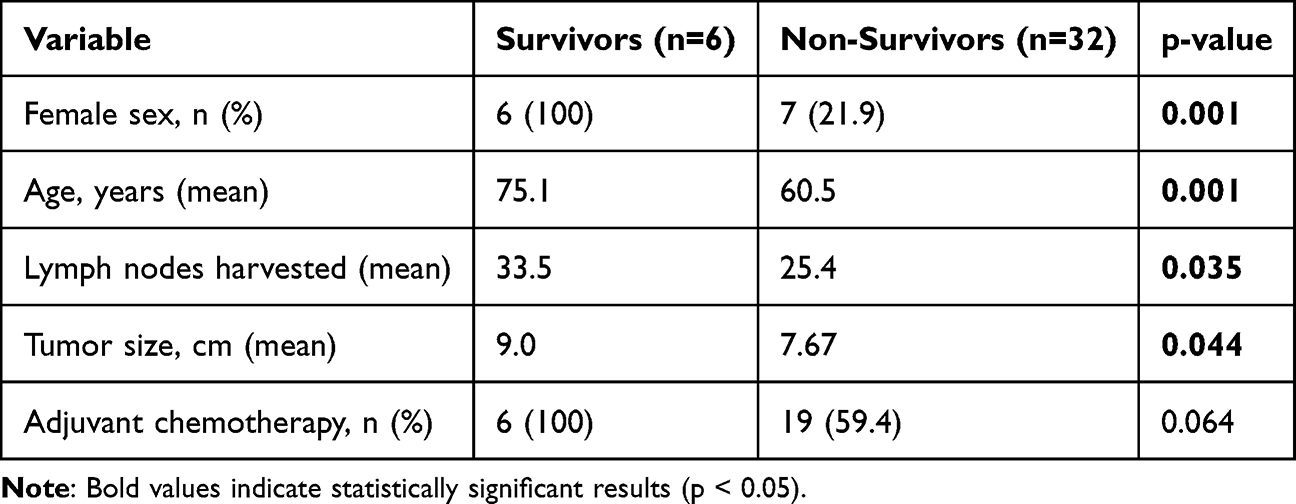 |
Table 2 Comparison of Survivors vs Non-Survivors |
Overall Survival Analysis
The mean OS for the entire cohort was 34.2 ± 8.3 months (median: 18.0 months; 95% CI: 18.0–50.4). Significant predictors of OS are shown in Table 3. Female sex (75.6 vs 12.7 months; p=0.003), age ≥65 years (62.5 vs 11.3 months; p=0.001), adjuvant chemotherapy (48.2 vs 7.2 months; p<0.001), and adjuvant CRT (58.3 vs 17.1 months; p=0.039) were associated with longer OS. Preoperative chemotherapy, surgical approach, and R0 resection status did not significantly influence OS (p>0.05) (Figure 1).
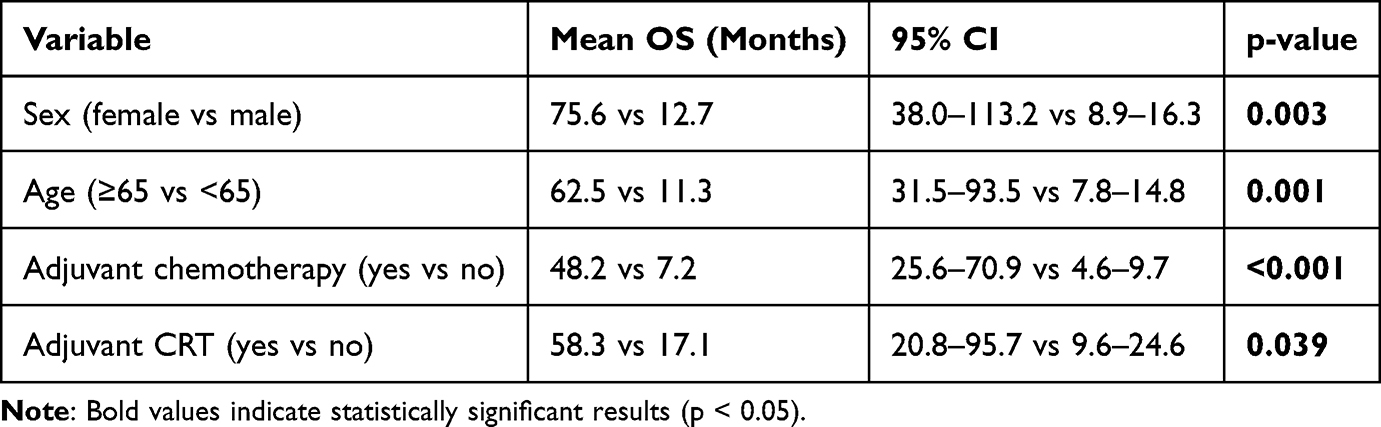 |
Table 3 Univariate Analysis of Overall Survival |
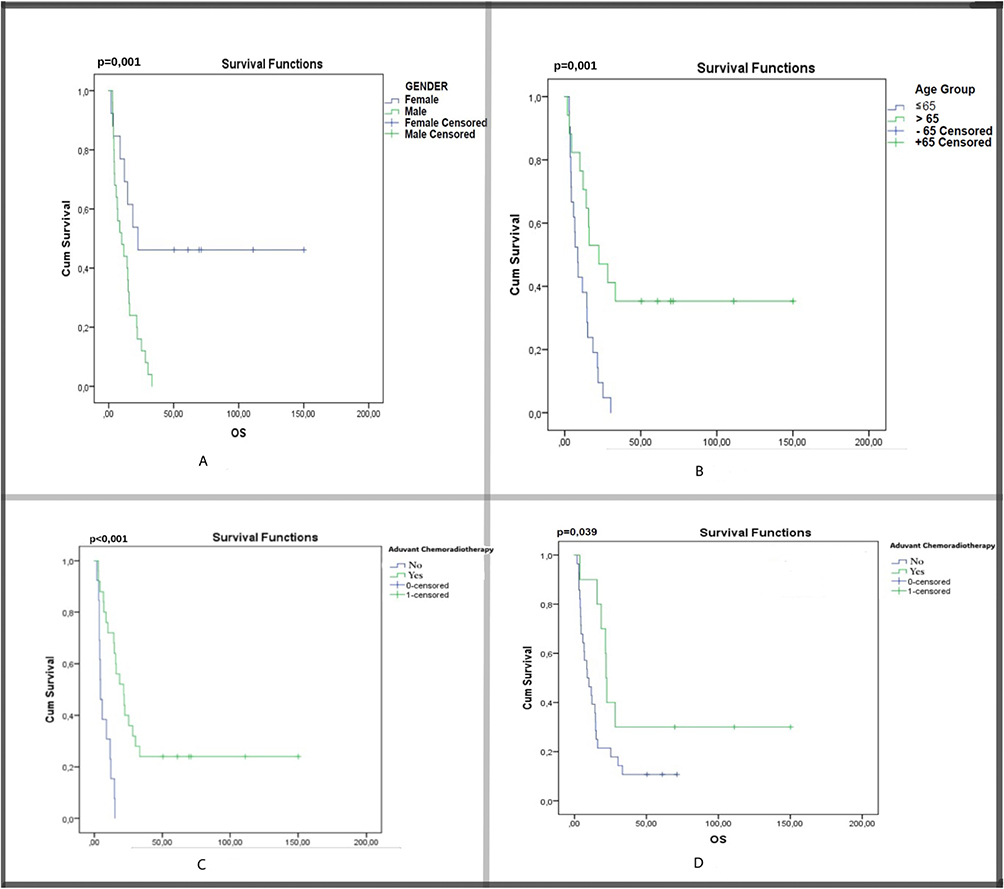 |
Figure 1 Kaplan-Meier survival curves for overall survival (OS). (A) Survival according to sex (log-rank p=0.003). (B) Survival according to age group, <65 vs ≥65 years (log-rank p=0.001). (C) Survival according to receipt of adjuvant chemotherapy (log-rank p<0.001). (D) Survival according to receipt of adjuvant chemoradiotherapy (log-rank p=0.039). |
Progression-Free Survival Analysis
The mean PFS was 9.99 ± 1.5 months (median: 8.0 months; 95% CI: 7.08–12.9). PFS was significantly longer in patients who received adjuvant chemotherapy (13.4 ± 2.1 vs 5.0 ± 1.1 months; p<0.001) (Figure 2). Adjuvant CRT showed a non-significant trend toward longer PFS (15.9 ± 2.6 vs 8.3 ± 1.6 months; p=0.149).
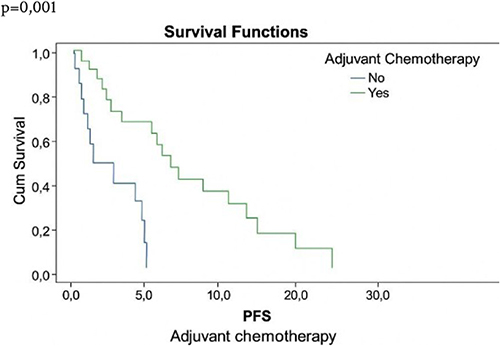 |
Figure 2 Kaplan-Meier survival curves for progression-free survival (PFS) according to receipt of adjuvant chemotherapy (log-rank p<0.001). |
Stratification by Metastasis Type
Among patients with liver metastases (Group A, n=14), the R0 resection rate was 85.7%, mean OS was 41.3 ± 6.2 months, and 5-year OS was 41%. In Group B (para-aortic, n=16), R0 rate was 62.5%, mean OS was 29.1 ± 4.8 months. In Group C (peritoneal, n=8), R0 rate was 12.5%, mean OS was 11.2 ± 2.1 months, and there were no 5-year survivors.
Multivariate Cox Regression Analysis
Variables with p<0.1 in univariate analysis (age, sex, adjuvant chemotherapy, metastasis type, lymph node harvest ≥30, R0 status, and Lauren classification) were included in the multivariate model. Table 4 presents the independent predictors of mortality.
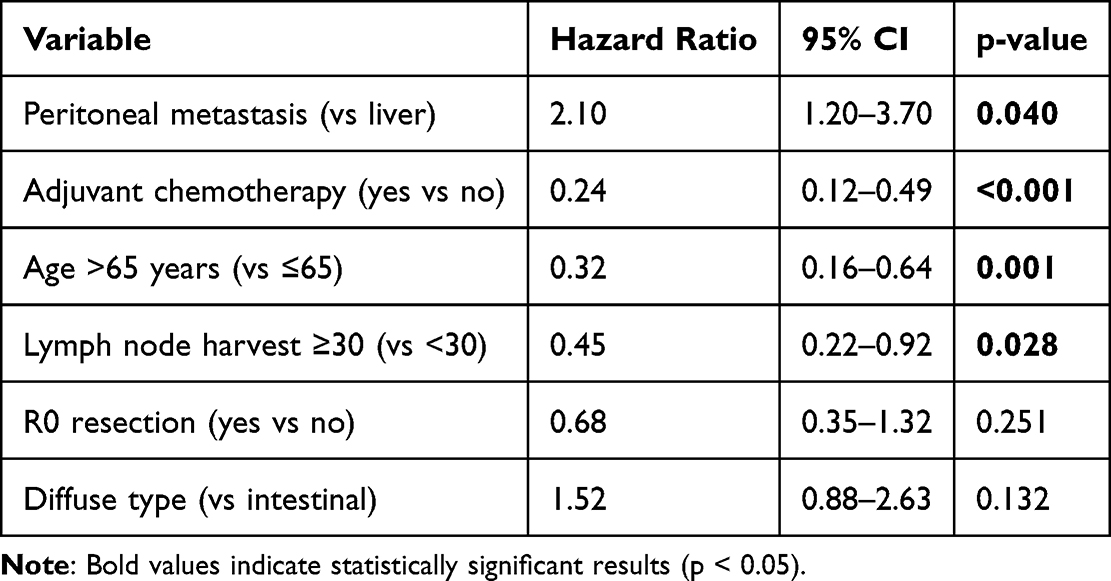 |
Table 4 Multivariate Cox Regression Analysis for Overall Survival |
Discussion
This study presents a metastasis-stratified analysis of outcomes in OMGC from Eastern Türkiye. The findings support key principles in the management of oligometastatic disease. One of the most striking findings was the clear survival hierarchy based on metastasis type. Patients with liver metastases had an R0 resection rate of 85.7%, translating to a 41% five-year OS, while patients with peritoneal disease had only a 12.5% R0 resection rate and 0% five-year OS. This pattern is consistent with subgroup analyses of the RENAISSANCE trial.18
Adjuvant therapy emerged as a critical determinant of survival. Adjuvant chemotherapy reduced mortality by 76% (HR=0.24; p<0.001), corroborating the CLASSIC and ACTS-GC trials.24 Adjuvant CRT offered a notable OS benefit (58.3 vs 17.1 months; p=0.039), consistent with the ARTIST-II trial.25
The extent of lymphadenectomy also played a significant role. In multivariate analysis, harvesting ≥30 lymph nodes was independently associated with improved OS (HR=0.45; p=0.028). This finding supports evidence from Korean studies indicating that harvesting more than 30 lymph nodes during D2 lymphadenectomy independently improves survival.26 However, given the retrospective design and small sample size, this threshold should be considered exploratory rather than definitive.
Interestingly, we observed that larger tumor size did not correlate with worse outcomes. This paradoxical finding likely reflects significant selection bias. Larger tumors may cause earlier symptom onset, prompting timely intervention, whereas smaller, more infiltrative tumors (eg, linitis plastica) often present with extensive unresectable disease, precluding surgical candidacy.27 This limitation of our retrospective design is explicitly acknowledged.
A particularly notable finding was the poor prognosis associated with younger age (<65 years) and male sex. Younger patients had markedly shorter OS (11.3 vs 62.5 months; p=0.001), and 78.1% of deaths occurred in male patients. This trend aligns with studies showing that aggressive histological subtypes (diffuse-type, signet-ring) are more prevalent in younger patients.28 The higher male mortality may reflect hormonal factors affecting the tumor microenvironment or delays in healthcare access.29
Our finding that older age was independently associated with better survival challenges conventional wisdom but underscores the importance of meticulous patient selection. The integration of geriatric assessment tools could further refine selection.30
From a surgical perspective, hepatic metastasectomy was associated with excellent R0 resection rates and prolonged survival, supporting Japanese guidelines.14 Para-aortic lymph node dissection showed a moderate but meaningful survival benefit (62.5% R0 rate).
Limitations
This study has several limitations. The retrospective, single-center design and limited sample size (n=38) restrict statistical power and generalizability. The absence of molecular biomarker data (HER2, MSI, PD-L1, CLDN18.2) represents a critical limitation, as these are essential for personalized medicine.6 Furthermore, postoperative complications and detailed performance status were not systematically recorded, which may have influenced adjuvant therapy allocation. The lack of routine comprehensive nutritional assessment and geriatric evaluation limits our ability to fully evaluate these factors.9 The MDT decision-making process was not fully standardized, and the long study period (2011–2023) introduces temporal heterogeneity in treatment paradigms. Therefore, our findings should be interpreted cautiously and require prospective validation.
Conclusion
Our study suggests that metastatic pattern, administration of adjuvant therapy, and adequacy of lymphadenectomy are important factors influencing survival in patients with OMGC undergoing curative-intent gastrectomy. Patients with liver metastases achieved more favorable outcomes, whereas peritoneal dissemination was associated with poor prognosis, requiring highly selective criteria for surgical intervention. Harvesting ≥30 lymph nodes may be considered a quality benchmark, but this requires prospective validation. Prospective, multicenter studies integrating molecular profiling and standardized decision algorithms are warranted to further refine personalized treatment strategies in OMGC.
Data Access Statement
The data supporting the findings are available from the corresponding author upon reasonable request.
Ethics Approval
The study protocol was reviewed and approved by the Non-Interventional Clinical Research Ethics Committee of Van Training and Research Hospital (Decision No: GOKAEK/2025-05-13). The study was conducted in accordance with the Declaration of Helsinki. As this was a retrospective study based on anonymized data, the requirement for informed consent was waived by the Institutional Review Board, but patient confidentiality was strictly maintained.
Author Contributions
All authors made a significant contribution to the work reported, whether in conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was not supported by a foundation.
Disclosure
The authors declare no potential conflicts of interest.
References
1. Smyth EC, Nilsson M, Grabsch HI, van Grieken NC, Lordick F. Gastric cancer. Lancet. 2020;396(10251):635–9. doi:10.1016/S0140-6736(20)31288-5
2. Torre LA, Siegel RL, Ward EM, Jemal A. Global cancer incidence and mortality rates and trends-an update. Cancer Epidemiol Biomarkers Prev. 2016;25(1):16–27. doi:10.1158/1055-9965.EPI-15-0578
3. Chau I, Norman AR, Cunningham D, et al. Multivariate prognostic factor analysis in locally advanced and metastatic esophago-gastric cancer. J Clin Oncol. 2004;22(12):2395–2403. doi:10.1200/JCO.2004.08.154
4. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2021 (6th edition). Gastric Cancer. 2023;26(1):1–25. doi:10.1007/s10120-022-01331-8
5. Smyth EC, Tarazona N, Peckitt C, et al. Challenges in the treatment of gastric cancer: the role of the multidisciplinary team and molecular biomarkers. Eur J Cancer Prev. 2024;33(2):89–97.
6. Pietrantonio F, Raimondi A, Lonardi S, et al; IMMUNOREG-GC Investigators. Margetuximab plus pembrolizumab in patients with previously treated, metastatic HER2-positive gastroesophageal adenocarcinoma. Cancer Drug Resist. 2024;7:102–115.
7. Izmailov T, Ryzhkin S, Borshchev G, Boichuk S. Oligometastatic disease (OMD): the classification and practical review of prospective trials. Cancers. 2023;15(21):5234. doi:10.3390/cancers15215234
8. Yasufuku I, Tsuchiya H, Fujibayashi S, et al. Oligometastasis of gastric cancer: a review. Cancers. 2024;16(3):673. doi:10.3390/cancers16030673
9. Bozzetti F, Mariani L, Nardone V. Perioperative nutritional support in patients undergoing gastrectomy for gastric cancer. Nutrients. 2025;17(1):188. doi:10.3390/nu17010188
10. Al-Batran SE, Homann N, Pauligk C, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, Phase 2/3 trial. Lancet. 2019;393(10184):1948–1957. doi:10.1016/S0140-6736(18)32557-1
11. Rovers KP, Lurvink RJ, Rijken A, et al. The current and future role of pressurized intraperitoneal aerosol chemotherapy in the treatment of peritoneal metastases from gastric cancer. Br J Surg. 2023;110(8):1001–1010.
12. Park SH, Kang MJ, Yun EH, Jung KW. Epidemiology of gastric cancer in Korea: trends in incidence and survival based on Korea central cancer registry data (1999-2019). Gastric Cancer. 2023;26(4):585–594.
13. Joshi SS, Badgwell BD. Current treatment and recent progress in gastric cancer. CA Cancer J Clin. 2021;71(3):264–279. doi:10.3322/caac.21657
14. Giovinazzo F, Vicenzo F, Baggio E, et al. The importance of high-volume centers in esophageal and gastric cancer surgery: a systematic review and meta-analysis. J Clin Med. 2023;12(7):2708. doi:10.3390/jcm12072708
15. Lordick F, Carneiro F, Cascinu S, et al. Gastric cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(10):1005–1020. doi:10.1016/j.annonc.2022.07.004
16. Rudy S, Gholami S, Shaghaghi M, et al. Oligometastatic gastric cancer: current landscape and future perspectives. Cancers. 2023;15(21):5234. doi:10.3390/cancers15215234
17. Smyth EC, Tarazona N, Peckitt C, et al. Current standards and future strategies in the treatment of oligometastatic gastric cancer. Cancers. 2024;16(3):673. doi:10.3390/cancers16030673
18. Al-Batran SE, Hofheinz RD, Pauligk C, et al. Histopathological regression after neoadjuvant docetaxel, oxaliplatin, fluorouracil, and leucovorin versus epirubicin, cisplatin, and fluorouracil or capecitabine in patients with resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4-AIO): results from the phase 2 part of a multicentre, open-label, randomised phase 2/3 trial. Lancet Oncol. 2016;17(12):1697–1708. doi:10.1016/S1470-2045(16)30531-9
19. Yoshida K, Kodera Y, Kochi M, et al. Addition of docetaxel to oral fluoropyrimidine improves efficacy in patients with stage III gastric cancer: interim analysis of JACCRO GC-07, a randomized controlled trial. J Clin Oncol. 2019;37(15_suppl):4001. doi:10.1200/JCO.18.01138
20. Park SH, Lim DH, Sohn TS, et al. A randomized Phase III trial comparing adjuvant single-agent S1, S-1 with oxaliplatin, and postoperative chemoradiation with S-1 and oxaliplatin in patients with node-positive gastric cancer after D2 resection: the ARTIST 2 trial. Ann Oncol. 2021;32(3):368–374. doi:10.1016/j.annonc.2020.11.017
21. Zheng Z, Liu Y, Bu Z, et al. Prognostic role of lymph node metastasis in early gastric cancer. Chin J Cancer Res. 2014;26(2):192–199. doi:10.3978/j.issn.1000-9604.2014.04.06
22. Komatsu S, Ichikawa D, Miyamae M, et al. Positive lymph node ratio as an indicator of prognosis and local tumor clearance in N3 gastric cancer. J Gastrointest Surg. 2016;20(9):1565–1571. doi:10.1007/s11605-016-3197-9
23. Özdemir Y, Yıldız R, Ekinci Ö, et al. Prognostic significance of lymphovascular invasion and perineural invasion in gastric cancer. Turk J Gastroenterol. 2021;32(6):489–496.
24. Noh SH, Park SR, Yang HK, et al. Adjuvant capecitabine plus oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): 5-year follow-up of an open-label, randomised Phase 3 trial. Lancet Oncol. 2014;15(12):1389–1396. doi:10.1016/S1470-2045(14)70473-5
25. Park SH, Sohn TS, Lee J, et al. Phase III trial to compare adjuvant chemotherapy with capecitabine and cisplatin versus concurrent chemoradiotherapy in gastric cancer: final report of the adjuvant chemoradiotherapy in stomach tumors trial, and survival update. J Clin Oncol. 2022;40(6):589–600.
26. Lu J, Wang W, Zheng CH, et al. Influence of total lymph node count on staging and survival after gastrectomy for gastric cancer. Ann Surg Oncol. 2017;24(2):486–493. doi:10.1245/s10434-016-5494-7
27. Rhodin KE, DeLaura IF, Horne E, et al. Impact of tumor size and management on survival in gastric cancer. J Gastrointest Surg. 2023;27(10):2076–2084. doi:10.1007/s11605-023-05779-6
28. Qu X, Zhao X, Liu Y, et al. The clinicopathological characteristics of early-onset gastric cancer and its evolutionary trends: a retrospective study. Am J Cancer Res. 2022;12(6):2757–2769.
29. Li H, Wei Z, Wang C, Chen W, He Y, Zhang C. Gender differences in gastric cancer survival: 99,922 cases based on the SEER database. J Gastrointest Surg. 2020;24(8):1747–1757. doi:10.1007/s11605-019-04304-y
30. Montroni I, Ugolini G, Saur NM, et al. Personalized management of elderly patients with rectal cancer: recommendations from the SIOG surgical task force. Eur J Surg Oncol. 2023;49(2):e84–e92. doi:10.1016/j.ejso.2022.11.003
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.