Back to Journals » Clinical Interventions in Aging » Volume 17
Factors Influencing Post-Stroke Cognitive Impairment in Patients with Type 2 Diabetes Mellitus
Authors Ma ZY, Wu YY ![]() , Cui HY
, Cui HY ![]() , Yao GY, Bian H
, Yao GY, Bian H
Received 15 January 2022
Accepted for publication 11 April 2022
Published 29 April 2022 Volume 2022:17 Pages 653—664
DOI https://doi.org/10.2147/CIA.S355242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Zhao-Yin Ma,1,* Yong-Ya Wu,2,* Hong-Yin-Long Cui,3 Guang-Yan Yao,3 Hong Bian3,4
1Department of Diagnostic, Medical Integration and Practice Center, Shandong University, Jinan, Shandong, People’s Republic of China; 2Department of Emergency Critical Care Medicine, The Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, Shandong, People’s Republic of China; 3Department of Neurology, Central Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, People’s Republic of China; 4Department of Neurology, Jinan Central Hospital, Shandong University, Jinan, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hong Bian, Department of Neurology, Central Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, People’s Republic of China, Tel +86-15318816109, Fax +86-053188382085, Email [email protected]
Objective: Type 2 diabetes mellitus (T2DM) and ischemic stroke, which are common diseases among older people, are closely related to cognitive impairment. This study aims to investigate the influencing factors of post-stroke cognitive impairment (PSCI) in patients with T2DM.
Methods: We enrolled 161 patients with T2DM who experienced acute ischemic stroke and were hospitalized in the Department of Neurology, Jinan Central Hospital, Shandong, China. Cognitive function was evaluated with the Montreal Cognitive Assessment scale. According to the results, patients were divided into three groups—the cognitively normal group, mild cognitive impairment group, and severe cognitive impairment group. We analyzed general demographic data, laboratory information, imaging data, the results of neuropsychological evaluation, and clinical features as well as influencing factors of PSCI in these patients and established a prediction model.
Results: The three groups of patients were significantly different in terms of age, education level, course of diabetes mellitus (DM), recurrent cerebral infarction (RCI), and other factors. RCI, course of DM, and glycated hemoglobin (HbA1c) were independent risk factors of PSCI in patients with T2DM, with odds ratio (95% confidence interval): 7.17 (2.09, 30.37), 5.39 (2.40, 14.59), and 3.89 (1.66, 10.04), respectively, whereas female, senior high school, serum albumin were protective factors: 0.28 (0.07, 0.95), 0.05 (0.01, 0.21), 0.20 (0.08, 0.42), respectively. Furthermore, we constructed a prediction model using sex, age, education level, RCI, DM course, HbA1c and serum albumin and obtained a receiver operating characteristic (ROC) curve. The area under the ROC curve is 0.966, suggesting the significant association of these influencing factors with PSCI in patients with T2DM.
Conclusion: In this study, the occurrence of PSCI in patients with T2DM was related to RCI, course of DM, and HbA1c, among other factors. Attention to influencing factors is needed in these patients for early diagnosis and timely intervention of cognitive impairment.
Keywords: blood glucose, cognitive impairment, ischemic stroke, risk factor
Introduction
Recent years have seen an increasing incidence of type 2 diabetes mellitus (T2DM), acute ischemic stroke (AIS), and cognitive impairment (CI). Characterized by high rates of disability and mortality, these diseases tend to place huge life pressure and a heavy economic burden on families as well as society. There is increased prevalence of brain damage and mental illness in patients with T2DM. Cognitive impairment, depression, and stroke, which are considered to be complications of diabetic microangiopathy,1 are likely caused by hyperglycemia, obesity, and insulin resistance. Motor dysfunction, speech impairment, sleep disorders, epilepsy, emotional disorders, and CI can remain to varying degrees after the onset of ischemic stroke. Recent studies have shown that vascular risk factors are related to CI, and cerebrovascular disease is the second most common cause of dementia.2 Post-stroke cognitive impairment (PSCI) is not only an important factor leading to slow physical recovery and a decline in the work capacity and social ability of patients with stroke but also a risk factor for recurrence of stroke and severe stroke.3,4 Studies have shown that patients with stroke develop dementia 10 years earlier than those without stroke.5 According to statistics, the incidence of PSCI is as high as 20%–80%.6 PSCI mainly includes two phases, post-stroke cognitive impairment with no dementia and post-stroke dementia.
To investigate the influencing factors of PSCI, researchers have used different methods based on their respective interests,7–12 including demographic information (advanced age and low education level), chronic brain injury (white matter hyperintense signal and temporal lobe atrophy), clinical data (hypertension, diabetes, and large artery occlusion), and biological information (apolipoprotein E, neuroinflammation, and intestinal flora). However, there are a great variety of factors affecting cognitive function, and it is difficult to completely cover the baseline data in specific practice, so opinions vary regarding the research results. Cognitive impairment does not have typical early symptoms, which often encompass a wide range. Older people with mild cognitive impairment (MCI) may experience cognitive dysfunction whereas those with severe CI may progress to dementia or Alzheimer’s disease without effective treatment and intervention measures.13 Thus, early diagnosis and prevention play critical roles in delaying the occurrence of CI. Identifying effective indicators to predict the occurrence of PSCI can provide clinicians with important information to conduct early diagnosis and cognitive rehabilitation, improve cognition through proper management, delay disease progression, and reduce early mortality.14 Overall, this study has explored the relationship of influencing factors with PSCI in patients with T2DM, which can provide insights into the early diagnosis and intervention treatment.
Methods
Study Population
The research participants in this study comprised 161 patients with T2DM who had experienced AIS and were hospitalized in the Department of Neurology, Jinan Central Hospital Affiliated to Shandong University between September 2017 and February 2020.
The inclusion criteria were as follows: 1) patients with the onset form and symptoms suspicious for acute stroke and onset time within 72 hours were examined using brain magnetic resonance imaging (MRI); patients determined to have AIS were hospitalized (met the criteria for AIS stated in the 2014 Guidelines for Diagnosis and Treatment of Acute Ischemic Stroke in China15); 2) patients who had been previously diagnosed with T2DM or who had venous plasma fasting glucose ≥7.0 mmol/L on the second day after hospital admission (met the diagnostic criteria for T2DM stipulated in the China Guidelines for the Prevention and Treatment of Type 2 Diabetes (2017)16); 3) patients aged ≤85 years; and 4) right-handed.
The exclusion criteria were as follows: 1) patients with massive cerebral infarction or severe cerebral infarction with obvious disorder of consciousness; 2) patients with obvious apraxia, aphasia, and acute complications of diabetes mellitus (such as diabetic ketoacidosis) who were unable to complete the questionnaire; 3) patients complicated with diseases affecting cognitive function, eg, cerebral trauma, brain tumor, intracranial infection; 4) patients with degenerative diseases of the nervous system such as Parkinson’s syndrome and frontotemporal dementia; 5) patients with mental diseases such as schizophrenia and severe depression, as well as drug and alcohol abuse; 6) patients with severe cardiopulmonary diseases, liver and kidney diseases, and malignant tumors; 7) patients complicated with severe stress response-related diseases such as acute infection and trauma; and 8) patients with previous hypoglycemia.
This study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the Research and Ethics Committee of Jinan Central Hospital (AF/SC-08/04.0). All participants were informed about the purpose of the study. Written informed consent was obtained from all participants, or from informants in the case of participants with severe cognitive impairment.
Demographic and Clinical Characteristics
We collected patients’ demographic data (sex, age, and education level), lifestyle information (smoking history and drinking history), influencing factors of cardiovascular and cerebrovascular diseases (hypertension, coronary artery disease, atrial fibrillation, history of cerebral infarction, total cholesterol, triglyceride, low-density lipoprotein, glycated hemoglobin [HbA1c], uric acid, fibrinogen, and serum albumin; the peripheral blood samples were taken by automatic biochemical analyzer [cs-600b, Changchun Dirui, China]), blood pressure on admission to the hospital, and the course of DM. Patients with hypertension were defined as those with systolic blood pressure ≥140 mmHg and diastolic blood pressure ≥90 mmHg measured three times using an electronic sphygmomanometer (hem-7127j, OMRON, Kyoto, Japan) on different days in the clinic without antihypertensive drugs, as well as those who had been diagnosed with hypertension in the past and were currently taking antihypertensive drugs. Coronary artery disease was determined according to a history of myocardial infarction, angina pectoris, or dynamic changes on an electrocardiogram (CM300, Shenzhen Branch, China) related to symptoms, as reported by patients. Cerebral infarction and atrial fibrillation were determined according to the medical history provided by patients. The course of DM spanned from the first time when the patient was diagnosed with diabetes to the time of this study, according to the patient’s self-reported medical history or existing medical records. Patients with a smoking history were defined as those who had smoked at least 100 cigarettes or 100 g of tobacco leaves in the past, and who were smoking within 1 month before this study was carried out. Patients with a drinking history were defined as those who had consumed alcohol for more than 1 year and who drank more than 30 mL of liquor or more than 150 mL of beer every day.
Imaging Examination
All participants underwent brain MRI after admission. All MR scans were performed using a standard 3.0 T scanner (GE Discovery750, Milwaukee, WI, USA) in a standard manner. The sequence included T1-weighted imaging (T1WI), T2-weighted imaging (T2WI), T2-weighted axial fluid-attenuated inversion recovery (FLAIR) images, diffusion-weighted imaging (DWI), and apparent diffusion coefficient (ADC) sequences. The infarcted tissue showed isointense or hypointense signals on T1WI and hyperintense signals on T2WI, with hyperintense signals found in the DWI phase of the corresponding parts. According to the results of brain MRI, we recorded the location of cerebral infarction (anterior circulation, posterior circulation, and anterior circulation + posterior circulation), the number of infarct lesions (single cerebral infarction and multiple cerebral infarction), TOAST classification–a system for categorization of subtypes of ischemic stroke mainly based on etiology–(atherosclerosis type, arteriole occlusion type, cardiogenic embolism, other cause type, and unexplained type), and OCSP classification-a simple clinical stroke classification system that has been associated with size and location of the infarct- (partial anterior circulation infarction, lacunar infarction, and posterior circulation infarction).
Chronic Brain Injury
Cerebral small vessel disease refers to a pathological process involving intracerebral arterioles and venules caused by chronic diseases. Cerebral small vessel disease has diverse pathological mechanisms. Its neuroimaging features include white matter hyperintensity (WMH), new subcortical infarction, lacuna, cerebral microbleeds, brain atrophy, and perivascular space. Patients with WMH, lacuna, perivascular space, and temporal lobe atrophy were included in this study. WMH was evaluated using the Fazekas scale, which gives a score ranging from 0 to 3 each for periventricular white matter hyperintense (PVH) and deep white matter hyperintense (DWMH); these two scores can be summed to give a total score from 0 to 6, with lower scores indicating less WMH burden. Lacuna refers to a round or oval subcortical hole with diameter 3–15 mm (the signal is close to that of cerebrospinal fluid), which originates from an acute subcortical small infarction or hemorrhage in the perforating artery. Perivascular space refers to a circular or linear lacuna with a diameter less than 3 mm and the same signal as cerebrospinal fluid. 4) Temporal lobe atrophy refers to a decrease in temporal lobe brain volume unrelated to visible focal injury, which is determined according to medical imaging.
Neuropsychological Evaluation
A professionally trained neurologist measured the cognitive function of patients using the Montreal Cognitive Assessment (MoCA) scale, administered within 10 minutes. The total score is 30 points. Patients with a score ≥26 points are considered to have normal cognitive function, those with a score <26 points are considered to have MCI, and those with a score <20 points are classified as having severe CI. To correct for errors, 1 point was added to the total score in patients with less than 12 years of education.
Statistical Analysis
The data were preprocessed and analyzed using R, version 4.0.1 (The R Project for Statistical Computing, Vienna, Austria). Number (n) and percentage (%) are used to report the data. χ2 test and Fisher’s exact test were used for comparisons among groups. Measurement data conforming to a normal distribution and satisfying the homogeneity test of variance are expressed using mean ± standard deviation. One-way analysis of variance was applied for intergroup comparison. Measurement data with a non-normal distribution are denoted using median and interquartile range. The Kruskal–Wallis H-test was used for intergroup comparison. Logistic regression analysis was carried out as multivariate regression analysis. We considered P<0.05 to indicate statistical significance. The backward stepwise regression method was used to analyze influencing factors. The optimal model was selected based on the Akaike information criterion (AIC). Once the model was determined, a prediction model was built based on the logistic regression model and a receiver operating characteristic (ROC) curve was drawn. The area under the ROC curve (AUC) was calculated to evaluate the predictability of each index. The Youden index of the most predictive index was calculated, and the critical point, sensitivity, and specificity were determined.
Results
Demographic and Imaging Characteristics
As shown in Table 1, 94 (58.39%) were identified with CI. Thereinto 61 (37.89%) of CI was characterized as MCI and 33 (20.50%) as severe CI. Compared with CN group, the patients in both of MCI and severe CI groups had the significant increase at age, the lower education level, the longer course of DM, the higher mRS and NIHSS scores. Moreover, the significant differences between CN and MCI or severe CI were observed in RCI, multiple cerebral infarction and TOAST classification (P<0.05).
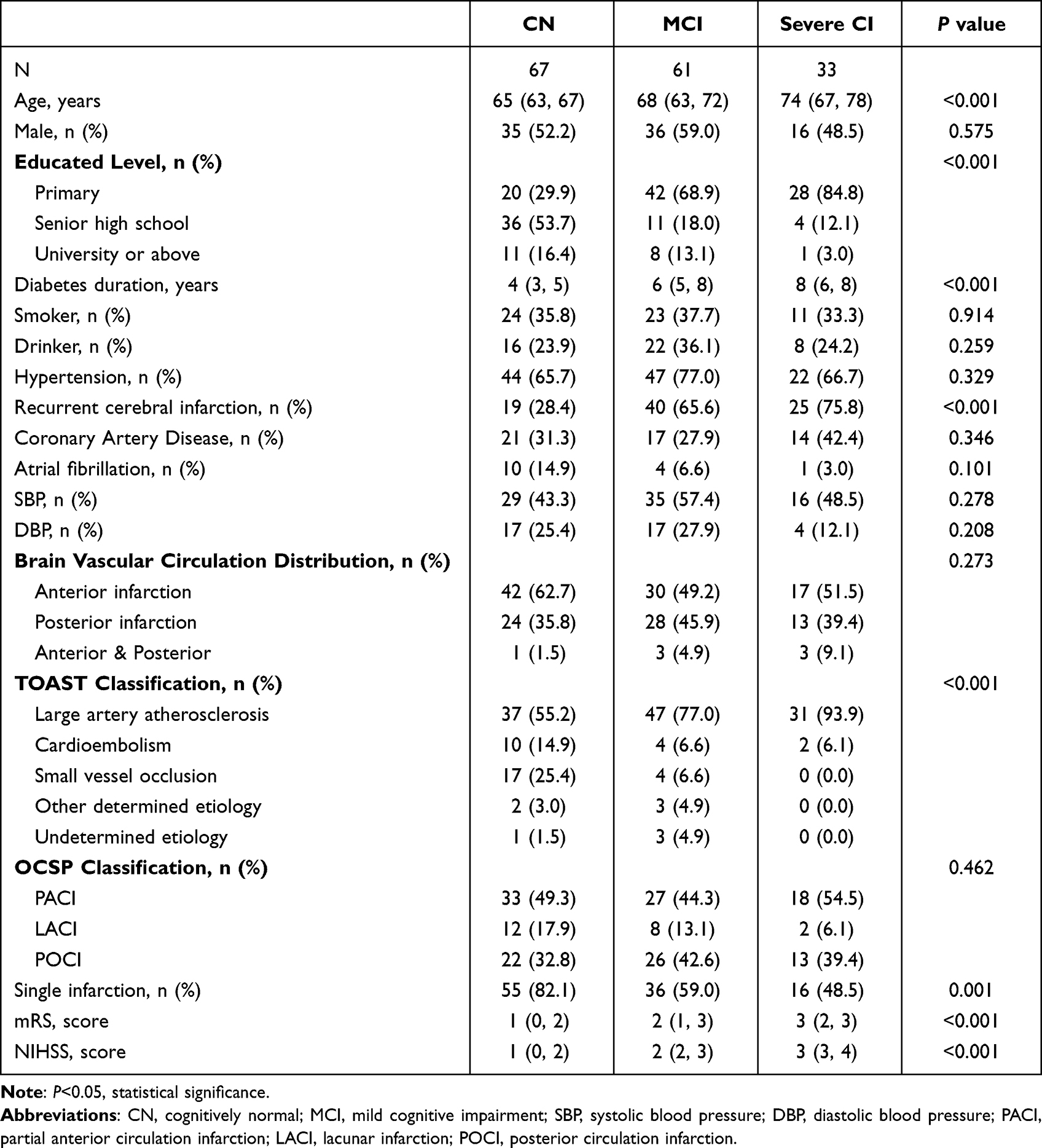 |
Table 1 Demographic and Clinical Characteristics by Cognition Groups |
Laboratory Data
The collected laboratory data were compared among the three groups of patients. As shown in Table 2, the levels of HbA1c and serum albumin in MCI and severe CI groups were higher than CN group (P<0.05). There were no significant differences in triglyceride, total cholesterol, low density lipoprotein, fibrinogen and uric acid among the three groups (P > 0.05).
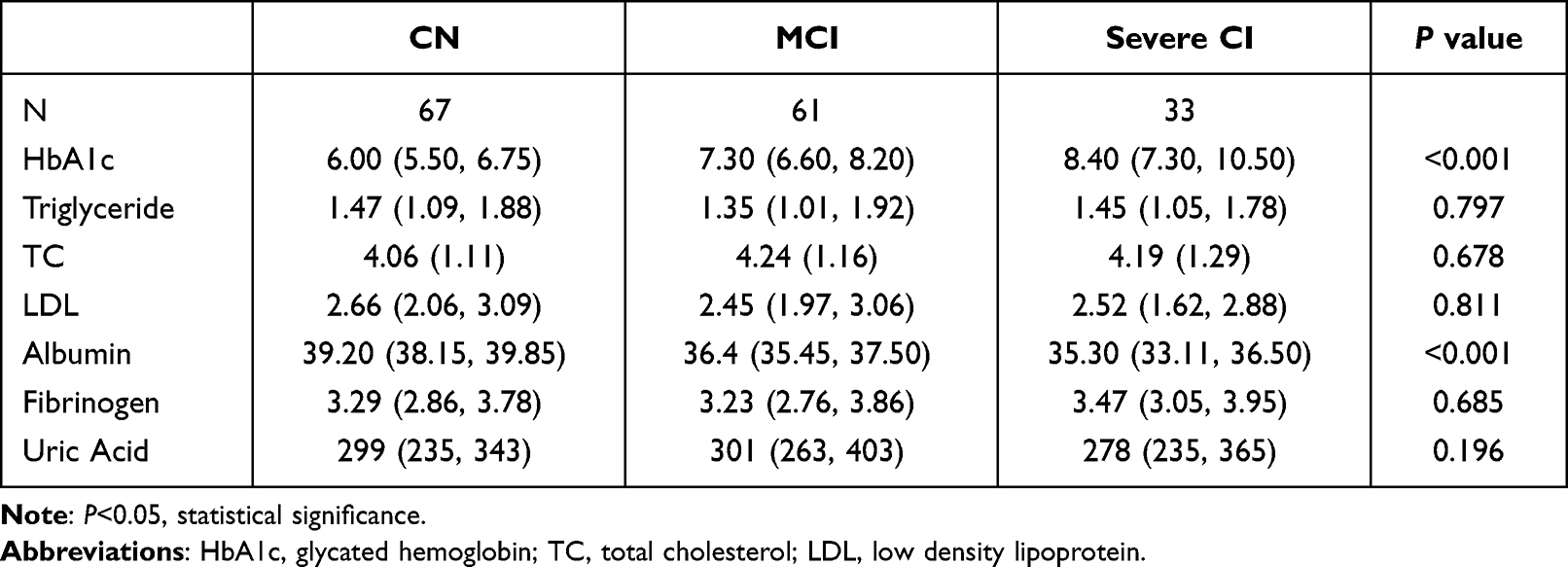 |
Table 2 Biochemical Criterion by Cognition Groups |
Chronic Brain Injury and Neurocognitive Characteristics
Table 3 shows the characteristics of chronic brain dysfunction. There were significant differences among the three groups in terms of each index. As shown in Table S1, compared with cognitively normal (CN) patients, those with CI had poorer performance in all cognitive domains ranging from visual space to naming, attention, language, abstraction, memory, and orientation (P<0.05).
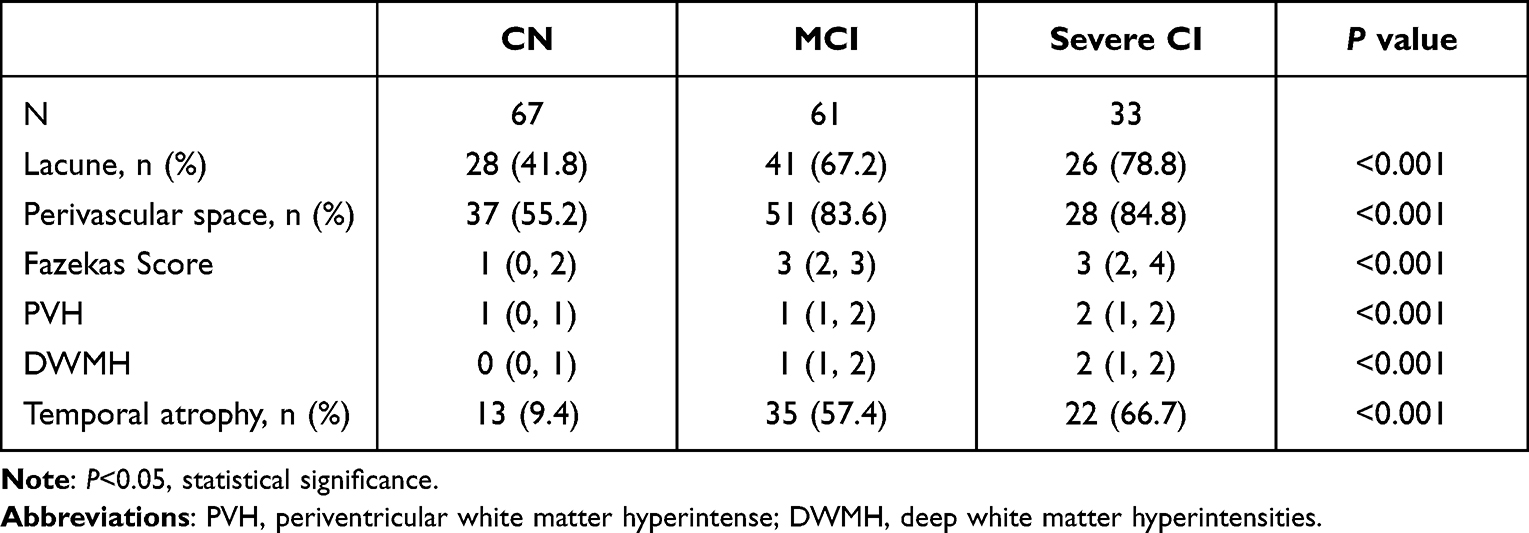 |
Table 3 Features of Small Vascular Lesions by Cognition Groups |
Age, Education Level, and HbA1c
As shown in Figures 1–3, cognitive levels gradually declined with increasing age and steadily improved with years of education. The cognitive level, which was negatively correlated with the level of HbA1c, showed an obvious downward curve.
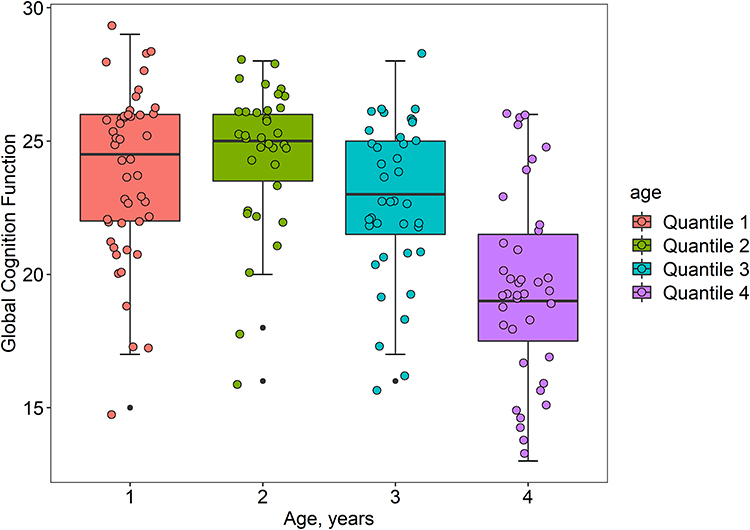 |
Figure 1 Distribution of cognitive function by age. The age of the enrolled patients was divided into four groups through the quartile interval, which increasing sequentially from left to right. The boxplot of the distribution of the four groups in the overall cognitive function was drawn by R analysis. The older patients had lower scores in cognitive function. |
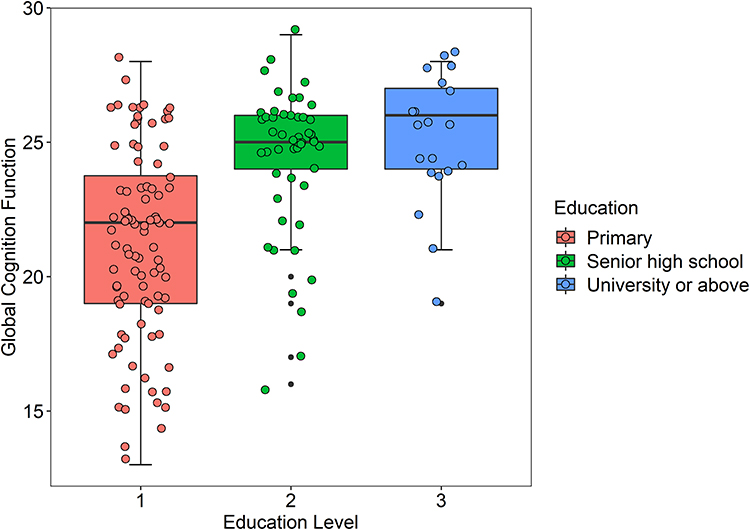 |
Figure 2 Distribution of cognitive function at educational level. Patients with less than 9 years of education were defined as primary, 9–11 years as Senior high school, and the patients with more than 11 years of education were defined as University or above. The boxplot of the distribution of the three groups in the overall cognitive function was drawn through R analysis. It can be seen that the cognitive function scores of patients with high education level are on the high side. |
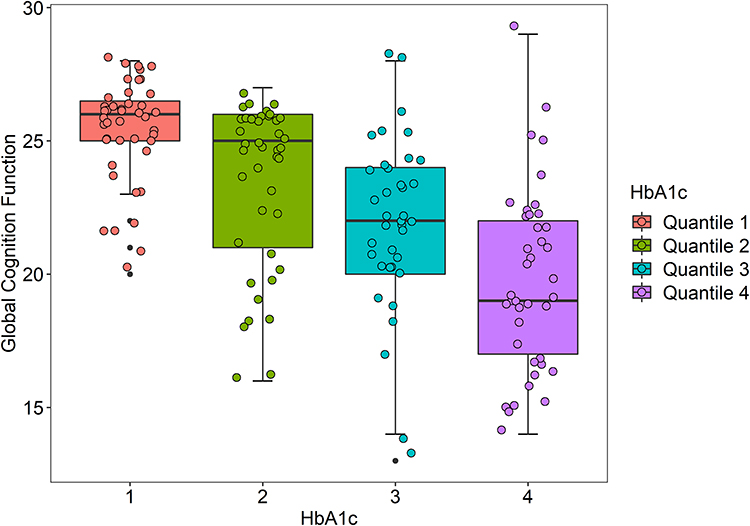 |
Figure 3 Distribution of cognitive function on HbA1c. The HbA1c were divided into four groups through the quartile interval, which increased from left to right. The boxplot of the distribution of HbA1c in the overall cognitive function was drawn by R analysis. Patients with high HbA1c scored lower in cognitive function. Abbreviation: HbA1c, glycated hemoglobin. |
Logistic Regression Analysis and Model Building
As shown in Figure S1, the Spearman correlation test was used to conduct correlation analysis on all variables. Fazekas score, PVH score, and other variables with high correlation were excluded to ensure the rationality of the model. Table 4 shows the results obtained using the optimal model of multivariate logistic regression. RCI, course of DM, and HbA1c were risk factors of CI, with OR (95% confidence interval) 7.17 (2.09, 30.37), 5.39 (2.40, 14.59), and 3.89 (1.66, 10.04), respectively. Female, senior high school education level, and serum albumin were protective factors of cognitive function, with OR (95% confidence interval) 0.28 (0.07, 0.95), 0.05 (0.01, 0.21), 0.20 (0.08, 0.42), respectively. We constructed a prediction model and drew a receiver operating characteristic (ROC) curve. As shown in Figure 4, the AUC of the model was 0.966, which indicates that the diagnosis was highly accurate. The optimal threshold was 0.511, with specificity 0.910, sensitivity 0.957, and Youden index 0.867.
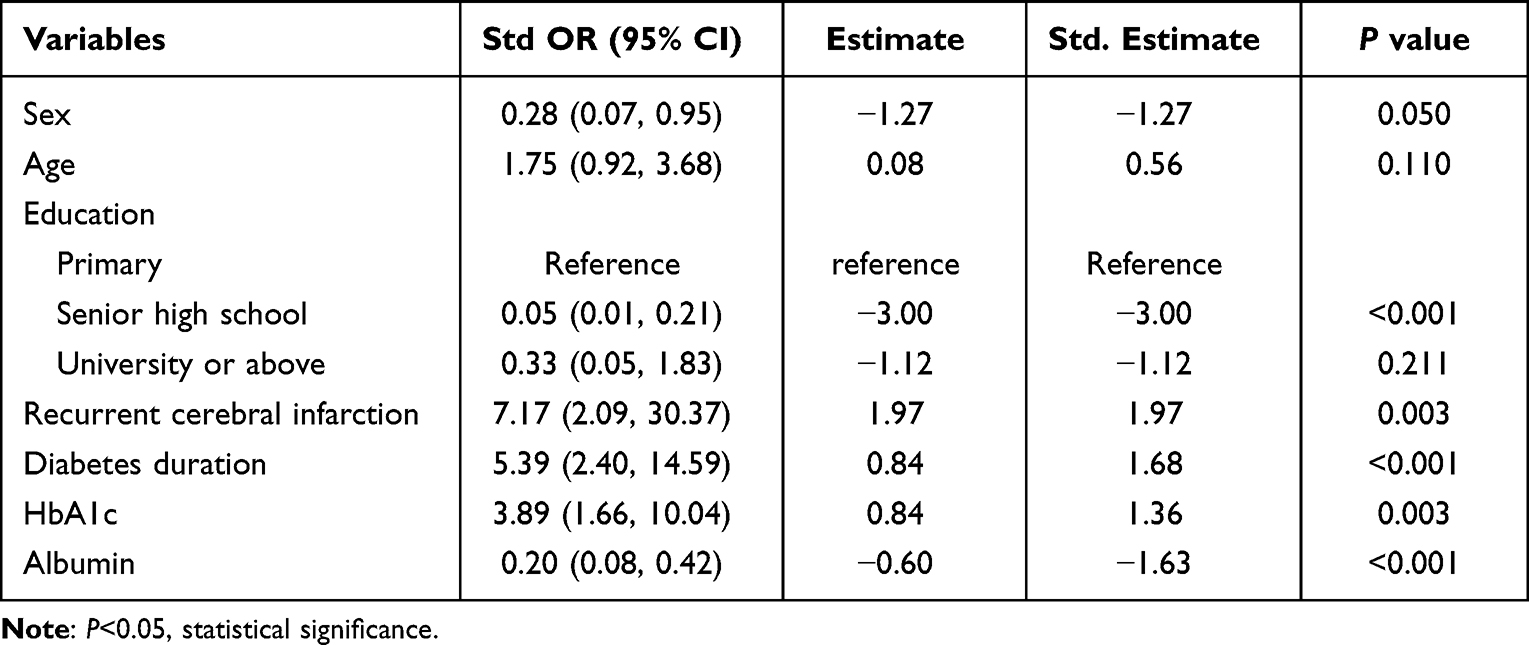 |
Table 4 Demographic, Clinical Characteristics and Laboratory Data Adjusted for PSCI in Patients with T2DM Predictive Model Using Binary Logistic Regression |
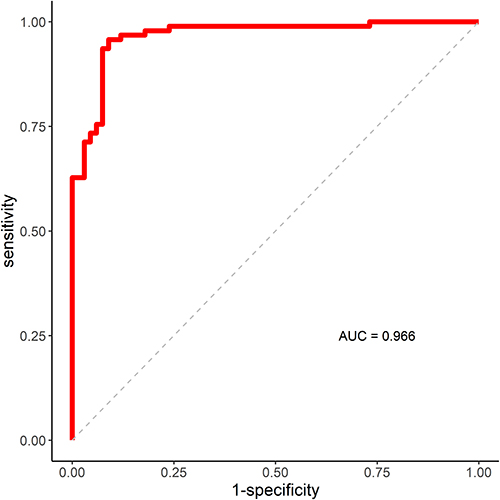 |
Figure 4 The receiver operating characteristic curve and area under the curve of the cognition function prediction model. Area under the curve of PSCI in patients with T2DM was predicted by the optimal model, including sex, age, education level, recurrent cerebral infarction, course of diabetes and serum albumin. The AUC of the model was 0.966, the optimal threshold was 0.511, with specificity 0.910, sensitivity 0.957, and Youden index 0.867. |
Discussion
In this study, we included patients with T2DM who experienced AIS and were hospitalized in the Department of Neurology, Jinan Central Hospital affiliated to Shandong University. Using cognitive assessment, the patients were divided into a CN group, MCI group, and severe CI group. According to the analyses of medical history, clinical examination, neuropsychological questionnaire, laboratory tests, and imaging examinations, we found that RCI, course of DM, and HbA1c were independent risk factors of PSCI in patients with T2DM, whereas female, senior high school, serum albumin were protective factors. We constructed a prediction model using sex, age, education level, RCI, DM course, HbA1c and serum albumin and obtained a receiver operating characteristic (ROC) curve, suggesting the significant association of these influencing factors with PSCI in patients with T2DM.
In this study, PSCI was significantly correlated with age and education level, and the risk of PSCI was higher in patients with older age and low education level, which is consistent with previous research results.5,17,18 With increased age, brain atrophy is aggravated, and synaptic connections between neurons are reduced in older individuals. Older patients often have accompanying cerebral arteriosclerosis and decreased cerebral blood flow, which increase the risk of CI. Older people with a low education level are more likely to develop age-related cognitive decline. Studies have shown that older individuals with an education background of junior high school or below are 3.03 times more likely to have PSCI than those with senior high school education level. Stroke survivors with higher education levels tend to have a larger cognitive reserve capacity, which can make up for brain damage.19–21
We also found that patients with a long course of DM are at higher risk for PSCI. Previous studies have shown that the course of DM is a risk factor for CI.18 Patients with a long course of DM have severe microangiopathy, longer exposure to glycolipid metabolic disorders, and severer oxidative stress responses.22 All of the above factors play a critical role in the development of atherosclerosis and CI in patients with T2DM.23,24 We found an increased risk of PSCI in patients with recurrent cerebral infarction, which is verified in previous research results.5,25 Studies have shown that the probability of dementia in patients with a previous stroke history is similar to that in patients who are 10 years older but without a stroke history.
By analyzing the differences between patients in the three subgroups classified using TOAST, we found that patients with large artery atherosclerosis and small artery occlusion had an increased risk of CI. According to a previous study, patients with stroke caused by cardiac cerebral embolism are prone to aphasia whereas patients with stroke owing to other causes are associated with executive function, memory, and emotional disorders. However, large artery atherosclerosis and small vessel occlusion can lead to nearly all types of CI.26 This also indicates the importance of monitoring cognition in specific stroke subtypes, so as to provide a warning of early stages of neurological impairment. Many studies have shown that the severity of infarction and low score for activities of daily living are effective in predicting PSCI.17,27 Patients with PSCI have a higher NIHSS score and a lower Barthel index. This study included the NIHSS score and mRS score, which were significantly different in single-factor analysis. It should be pointed out that our study findings were not in agreement with the results of previous studies when it comes to the relationship between the number of infarcts and CI.17,28 We found a significant correlation between multiple infarcts and the risk of CI, and the volume of cerebral infarction was non-significantly correlated with cognitive function.
The results of analysis of laboratory indexes, HbA1c was found to be a risk factor for the development of PSCI. HbA1c represents the average blood glucose level of patients in the past 8–12 weeks. Most researchers believe that hyperglycemia represented by increased HbA1c is negatively correlated with cognitive function because it can accelerate brain damage and aging.25,29 Nevertheless, a few researchers hold the opposite view, believing that cognitive function improves with increased HbA1c.30 Moreover, we found that high serum albumin was a protective factor for cognitive function, which has been verified in previous studies.31–33 This may be related to nutritional status, blood volume, and oxidative stress reflected in serum albumin. We did not find any significant correlation between lipids and CI, which is inconsistent with previous data.34,35 This is probably because some patients were taking oral lipid-lowering drugs before the onset of stroke.
It has been found that microvascular lesions, vascular endothelial damage, and insulin resistance caused by diabetes are related to WMH, and an increased load of WMH will lead to CI.12,36 Cerebral small vessel disease is an important influencing factor of CI. In this study, WMH, lacuna, perivascular space, and temporal lobe atrophy were included as representative types of chronic brain injury in cerebral small vessel diseases; cerebral microbleeds were not included because most research participants were not scanned with susceptibility-weighted imaging during hospitalization. Univariate analysis revealed significant differences among the three groups in terms of chronic brain injury. However, this variable with relatively high correlation was excluded in the final regression analysis; chronic brain injury caused by cerebral small vessel diseases is very common in patients with CI. In future research, we can further increase the sample size and quantitatively analyze chronic brain injuries such as lacuna and perivascular space. Our study shows a comparison of neuropsychological evaluations conducted among the different groups. Significant differences were found among the three groups in terms of each cognitive domain.
We entered the abovementioned influencing factors into the regression model and selected the optimal model according to the AIC. Once the model was determined, we predicted the occurrence of PSCI in patients with T2DM based on the logistic regression model. RCI, the course of DM, and HbA1c were risk factors of PSCI. For every unit of increased course of DM, the risk of PSCI increased by 5.39 times, and the risk of PSCI in patients with recurrent cerebral infarction was 7.17 times that of patients with a first cerebral infarction. However, sex (female), senior high school and serum albumin were protective factors of cognitive function. There are differences between men and women when it comes to cognitive status and the prevalence of many mental diseases, which involves many aspects such as sex hormones, brain neuroanatomy, neurotransmitters, and sleep disorders. According to most studies, men have more serious cognitive deficits than women.37–39 Women perform well in speech and episodic memory whereas men have better visual spatial abilities. Given the same estrogen level, women outperform men in terms of memory and speech,40–44 and women with acute cerebrovascular diseases have stronger cognitive reserve abilities than men.41 In addition, the volume of brain regions related to cognitive functions such as learning and memory has been proven to be significantly different between men and women. The volume of the hippocampus, caudate nucleus, dorsolateral prefrontal cortex, and anterior cingulate gyrus is larger in women than in men.45–47 Our study showed that female was a protective factor of cognitive function. Nonetheless, some researchers hold differing opinions,48–51 believing that women are more likely to have CI than men or that the incidences of CI are quite similar between men and women. Through stepwise regression, we finally determined that recurrent cerebral infarction, the course of DM, and HbA1c were the most effective in predicting PSCI in patients with T2DM. The AUC of the model was 0.966, which indicates that the diagnostic accuracy is high. These clinical variables provide the basis for early screening of CI. In future clinical work, clinicians should suggest that patients at high risk for CI manage their lifestyle and control vascular risk factors, such as through smoking cessation, alcohol restriction, diet management, exercise, and control of blood pressure and blood glucose. If necessary, patients should receive cognitive rehabilitation training and drug intervention, such as with cholinesterase inhibitors and N-methyl-D-aspartate (NMDA) receptor antagonists,52,53 which will help to improve patients’ cognitive function and delay the progression of disease.
Currently, only a small number of researchers have studied the cognitive function of patients with T2DM after stroke. Compared with the other research, this study included more detailed information about demographic data, imaging, laboratory data, stroke types, nerve injury, and recovery evaluation. We used the MoCA Scale,54 which has relatively high sensitivity and specificity for CI caused by vascular factors, to screen the cognitive function of patients. We excluded patients with major diseases like depression and hypoglycemia that may affect cognitive function, as well as patients with severe brain injury, many complications, and aphasia who could not complete the scale. However, because of this, the research participants in this study had mild symptoms of nerve damage (median NIHSS 2), with the corresponding cognitive performance being better than expected. Hence, these research participants cannot represent all patients with T2DM who have PSCI.
Owing to some limitations, these results must be carefully interpreted. First, the sample size was not sufficiently large and this was a single-center study. The results of this study were in-sample results, lacking external verification. Second, the severity and extent of CI among the included patients might be underestimated as a single administration of the MoCA scale was used to evaluate the cognition of patients at specific time points.55,56 Third, no data were collected regarding the cognitive status of research participants before stroke (1 year earlier or longer), which may affect our research results to some extent. Therefore, as a preliminary study, this study was initially aimed at screening the influencing factors of CI after T2DM ischemic stroke with the aim to establish a prediction model. More prospective, longitudinal, and multicenter studies will be needed in the future to confirm the results of this study, so as to better diagnose and intervene CI in such patients.
Conclusion
This study screened for factors affecting cognitive function after ischemic stroke in patients with T2DM. RCI, course of DM, and HbA1c were independent risk factors of PSCI in patients with T2DM, whereas female, senior high school, serum albumin were protective factors. We constructed a prediction model using sex, age, education level, RCI, DM course, HbA1c and serum albumin. It showed the significant association of these influencing factors with PSCI in patients with T2DM. Our study emphasized the importance of a patient’s history, laboratory testing, and imaging examination for patients with type 2 diabetes after stroke. After further external validation, the predictive model results of this study may serve as a potential tool to identify high-risk patients with CI, provide a basis for early management strategies for patients with PSCI, help delay disease progression, and improve the quality of life of post-stroke patients.
Ethical Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the Research and Ethics Committee of Jinan Central Hospital (AF/SC-08/04.0). All participants were informed about the purpose of the study. Written informed consent was obtained from all participants, or from informants in the case of participants with severe cognitive impairment.
Acknowledgments
We thank all participants of this study! We thank Yanlin Qu for statistical analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. van Sloten TT, Sedaghat S, Carnethon MR, et al. Cerebral microvascular complications of type 2 diabetes: stroke, cognitive dysfunction, and depression. Lancet Diabetes Endocrinol. 2020;8(4):325–336. doi:10.1016/S2213-8587(19)30405-X
2. OBrien JT, Erkinjuntti T, Reisberg B, et al. Vascular cognitive impairment. Lancet Neurol. 2003;2(2):89–98. doi:10.1016/S1474-4422(03)00305-3
3. Kwon HS, Lee D, Lee MH, et al. Post-stroke cognitive impairment as an independent predictor of ischemic stroke recurrence: PICASSO sub-study. J Neurol. 2020;267(3):688–693.doi:10.1007/s00415-019-09630-4
4. Béjot Y, Duloquin G, Crespy V, et al. Influence of preexisting cognitive impairment on clinical severity of ischemic stroke. Dijon Stroke Registry Stroke. 2020;51:1667–1673. doi:10.1161/STROKEAHA.119.028845
5. Ronchi D, Palmer K, Pioggiosi P, et al. The combined effect of age, education, and stroke on dementia and cognitive impairment no dementia in the elderly. Dement Geriatr Cogn Disord. 2007;24(4):266–273. doi:10.1159/000107102
6. Ding MY, Xu Y, Wang Y, et al. Predictors of cognitive impairment after stroke: a prospective stroke cohort study. J Alzheimers Dis. 2019;71(4):1139–1151. doi:10.3233/JAD-190382
7. Chander RJ, Lam BY, Lin X, et al. Development and validation of a risk795 score (CHANGE) for cognitive impairment after ischemic796 stroke. Sci Rep. 2017;29:1–11.
8. Sivakumar L, Riaz P, Kate M, et al. 2017 white matter hyper-803 intensity volume predicts persistent cognitive impairment in804 transient ischemic attack and minor stroke. Int J Stroke. 2019;12:264–272. doi:10.1177/1747493016676612
9. Chen X, Duan L, Han Y, et al. Predictors for vascular cognitive792 impairment in stroke patients. BMC Neurol. 2016;16(1):115. doi:10.1186/s12883-016-0638-8
10. Kalaria RN, Akinyemi R, Ihara M. Stroke injury, cog-812 nitive impairment and vascular dementia. Biochim Biophys. 2016;1862:1–63.
11. Wei Y, Dapeng G, Wen J, et al. Intestinal flora dysbiosis aggravates cognitive dysfunction associated with neuroinflammation in heart failure. J Card Fail. 2020. doi:10.1016/j.cardfail.2020.02.002
12. Zhenjie T, Yanhong D, Dandan Z, et al. Cerebral small vessel disease and post-stroke cognitive impairment. Int J Neurosci. 2017;127(9):824–830.
13. Zhang Q, Wu Y, Han T, Liu E. Changes in cognitive function and risk factors for cognitive impairment of the elderly in China: 2005–2014. Int J Environ Res Public Health. 2019;16(16):2847. PMID: 31404951; PMCID: PMC6719934. doi:10.3390/ijerph16162847
14. Bejot Y, Jacquin A, Rouaud O, et al. One-year survival of demented stroke patients: data from the Dijon Stroke Registry, France (1985–2008). Eur J Neurol. 2012;19:712–717. doi:10.1111/j.1468-1331.2011.03613.x
15. Chinese Society of Neurology, Cerebrovascular Group of Chinese Society of Neurology. The guidelines for diagnosis and treatment of acute ischemic stroke in China 2014. J Zhong Hua Shen Jing Ke Za Zhi. 2015;48(4):246–257.
16. Diabetes Society of Chinese Medical Association. The guidelines for prevention and treatment of type 2 diabetes in China. J zhong huo shi yong nei ke za zhi. 2018;38(04):292–344.
17. Zulkifly MF, Ghazali SE, Din NC, et al. A review of risk factors for cognitive impairment in stroke survivors. Sci World J. 2016:16. doi:10.1155/2016/3456943
18. Cai R, Han J, Sun J, et al. Plasma clusterin and the CLU gene rs11136000 variant are associated with mild cognitive impairment in type 2 diabetic patients. Front Aging Neurosci. 2016;8:179. doi:10.3389/fnagi.2016.00179
19. Duda B, Puente A, Miller L. Cognitive reserve moderates relation between global cognition and functional status in older adults. J Clin Exp Neuropsychol. 2014;36(4):368–378. doi:10.1080/13803395.2014.892916
20. Oh H, Park J, Seo W. A 2-year prospective follow-up study of temporal changes associated with post-stroke cognitive impairment. Int J Nurs. 2018;24(2):e12618. doi:10.1111/ijn.12618
21. Stern Y. Cognitive reserve and Alzheimer disease. Alzheimer Dis Assoc Disord. 2006;20(2):112–117. doi:10.1097/01.wad.0000213815.20177.19
22. Polidori MC, Mecocci P, Stahl W, et al. Plasma levels of lipophilic antioxidants in very old patients with type 2 diabetes. Diabetes Metab Res Rev. 2000;16:15–19. doi:10.1002/(SICI)1520-7560(200001/02)16:1
23. Mackness B, Hunt R, Durrington PN, et al. Increased immunolocalization of paraoxonase, clusterin, and apolipoprotein A-I in the human artery wall with the progression of atherosclerosis. Arterioscler Thromb Vasc Biol. 1997;17:1233–1238. doi:10.1161/01.atv.17.7.1233
24. Ahmad W. Overlapped metabolic and therapeutic links betweenAlzheimer and diabetes. Mol Neurobiol. 2013;47:399–424. doi:10.1007/s12035-012-8352-z
25. Albai O, Frandes M, Timar R, et al. Risk factors for developing dementia in type 2 diabetes mellitus patients with mild cognitive impairment Neuropsychiatr. Dis Treat. 2019;15:167–175. doi:10.2147/NDT.S189905
26. Hoffmann M, Schmitt F, Bromley E. Vascular cognitive syndromes: relation to stroke etiology and topography. Acta Neurol Scand. 2009;120(3):161–169. doi:10.1111/j.1600-0404.2008.01145.x
27. Renjen P, Gauba C, Chaudhar D. Cognitive Impairment After Stroke. Cureus. 2015;7(9):e335. doi:10.7759/cureus.335
28. Sundar U, Adwani S. Post-stroke cognitive impairment at 3 months. Ann Indian Acad Neurol. 2010;13(1):42. doi:10.4103/0972-2327.61276
29. Neumann KF, Rojo L, Navarrete P, et al. Insulin resistance and Alzheimer’s disease: molecular links & clinical implications. Curr Alzheimer Res. 2008;5(5):438–447. doi:10.2174/156720508785908919
30. Van den Berg,De E, Biessels GJ, Gussekloo J, et al. The impact of diabetes mellitus on cognitive decline in the oldest of the old: a prospective population-based study. Diabetologia. 2006;49(9):2015–2023. doi:10.1007/s00125-006-0333-1
31. Wang L, Wang F, Liu J, et al. Inverse relationship between baseline serum albumin levels and risk of mild cognitive impairment in elderly: a Seven-year retrospective cohort study. Tohoku J Exp Med. 2018;246:51–57. doi:10.1620/tjem.246.51
32. Yin ZX, Wang JL, Lyu YB. Association between serum albumin and cognitive performance in elderly Chinese. Zhonghua Liu Xing Bing Xue Za Zhi. 2016;37(10):1323–1326. doi:10.3760/cma.j.issn.0254-6450.2016.10.001
33. Llewellyn DJ, Langa KM, Friedland RP, et al. Serum albumin concentration and cognitive impairment. Curr Alzheimer Res. 2010;7:91–96. doi:10.2174/156720510790274392
34. Ying X, Le Z, Jingyi H, et al. Correlation of early cognitive dysfunction with inflammatory factors and metabolic indicators in patients with Alzheimer’s disease. Am J Transl Res. 2021;13(8):9208–9215.
35. Haoqiang Z, Wenwen Z, Tong N, et al. Inverted U-shaped correlation between serum low-density lipoprotein cholesterol levels and cognitive functions of patients with type 2 diabetes mellitus. Lipids Health Dis. 2021;20(1):103. doi:10.1186/s12944-021-01534-5
36. Tamura Y, Araki A. Diabetes mellitus and white matter hyperintensity. Geriatr Gerontol Int. 2015;15(Suppl. 1):34–42. doi:10.1111/ggi.12666
37. Mendrek A, Mancini-Marïe A. Sex/gender differences in the brain and cognition in schizophrenia. Neurosci Biobehav Rev. 2016;67:57–78. doi:10.1016/j.neubiorev.2015.10.013
38. Abel KM, Drake R, Goldstein JM. Sex differences in schizophrenia. Int Rev Psychiatry. 2010;22:417–428. doi:10.3109/09540261.2010.515205
39. Nussbaum NL. ADHD and female specific concerns. J Atten Disord. 2012;16:87–100. doi:10.1177/1087054711416909
40. Barel E, Tzischinsky O. Age and sex differences in verbal and visuospatial abilities. Adv Cogn Psychol. 2018;14:51–61. doi:10.5709/acp-0238-x
41. Sundermann EE, Mak PM, Rubin LH, et al. Female advantage in verbal memory evidence of sex-specific cognitive reserve. Neurology. 2016;87:1916–1924. doi:10.1212/WNL.0000000000003288
42. Grysman A. Gender differences in episodic encoding of autobiographical memory. J Appl Res Mem Cogn. 2017;6:51–59. doi:10.1016/j.jarmac.2016.07.012
43. Herlitz A, Rehnman J. Sex differences in episodic memory. Curr Dir Psychol Sci. 2008;17:52–56. doi:10.1111/j.1467-8721.2008.00547.x
44. Yonker JE, Eriksson E, Nilsson LG, et al. Sex differences in episodic memory: minimal influence of estradiol. Brain Cogn. 2003;52:231–238. PubMed: 12821106. doi:10.1016/S0278-2626(03)00074-5
45. Goldstein JM, Seidman LJ, Horton NJ, et al. Normal sexual dimorphism of the adult human brain assessed by in vivo magnetic resonance imaging. Cereb Cortex. 2001;11:490. doi:10.1093/cercor/11.6.490
46. Lenroot RK, Giedd JN. Sex differences in the adolescent brain. Brain Cogn. 2010;72(1):46–55. doi:10.1016/j.bandc.2009.10.008
47. Ruigrok AN, Salimi-Khorshidi G, Lai MC, et al. A meta-analysis of sex differences in human brain structure. Neurosci Biobehav Rev. 2014;39:34–50. doi:10.1016/j.neubiorev.2013.12.004
48. Janet S. Hyde.sex and cognition: gender and cognitive functions. Curr Opin Neurobiol. 2016;38:53–56. doi:10.1016/j.conb.2016.02.007
49. Kessler RC, Petukhova M, Sampson NA, et al. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int J Methods Psychiatr Res. 2012;21:169–184. doi:10.1002/mpr.1359
50. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198–210. doi:10.1177/1524838009334448
51. Tolin DF, Foa EB. Sex differences in trauma and posttraumatic stress disorder: a quantitative review of 25 years of research. Psychol Bull. 2006;132:959–992. doi:10.1037/0033-2909.132.6.959
52. Sun JH, Tan L, Yu JT. Post-stroke cognitive impairment: epidemiology, mechanisms and management. AnnTransl Med. 2014;2:80.
53. Mijajlovi´c MD, Pavlovi´c A, Brainin M, et al. Post-stroke dementia: a comprehensive review. BMC Med. 2017;15:11. doi:10.1186/s12916-017-0779-7
54. Lei X, Tao Z, Biao Z, et al. The associations of increased cerebral small vessel disease with cognitive impairment in neurosyphilis presenting with ischemic stroke. Brain Behav. 2021;11(6):e02187. doi:10.1002/brb3.2187
55. Chan E, Altendorff S, Healy C, et al. The test accuracy of the Montreal Cognitive Assessment (MoCA) by stroke lateralisation. J Neurol Sci. 2017;373:100–104. doi:10.1016/j.jns.2016.12.028
56. Chan E, Khan S, Oliver R, et al. Underestimation of cognitive impairments by the Montreal Cognitive Assessment (MoCA) in an acute stroke unit population. J Neurol Sci. 2014;343(1–2):176–179. doi:10.1016/j.jns.2014.05.005
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.